hrct protocols
TRANSCRIPT

Multidetector High-resolution ComputedTomography of the Lungs
Protocols and Applications
Baskaran Sundaram, MD, Aamer R. Chughtai, MD, and Ella A. Kazerooni, MD, MS
Abstract: Advances in computed tomography (CT) scanner techno-logy have made isotropic volumetric, multiplanar high-resolutionlung imaging possible in a single breath-hold, a significant advanceover the incremental high-resolution CT (HRCT) technique inwhich noncontiguous images sampled the lung, but lacked anatomiccontinuity. HRCT of the lungs is an established imaging techniquefor the diagnosis and management of interstitial lung disease,emphysema, and small airway disease, providing a noninvasivedetailed evaluation of the lung parenchyma, and providing infor-mation about the lungs as a whole and focally. In addition tohaving a high degree of specificity for diagnosing conditions such asemphysema, sarcoidosis, usual interstitial pneumonitis, Langer-hans cell histiocytosis, and small airway disease, there is a growingbody of medical evidence to support the use of HRCT findingsor diagnosis to predict patient prognosis. In this article, we reviewthe technique, advantages, and clinical applications of the currentHRCT technique.
Key Words: high-resolution computed tomography, lungs, interstitial
lung disease, technique, protocols
(J Thorac Imaging 2010;25:125–141)
Advances in multidetector computed tomography (CT)have made volumetric, high-resolution CT (HRCT)
possible in a single breath-hold, even for patients withshortness of breath, one of the most frequent symptoms inpatients undergoing lung evaluation. HRCT of the lungshas become the in vivo gold standard for evaluating thelung parenchyma and airways. Its superiority over conven-tional chest radiography and standard chest CT is wellestablished. Fortunately, imaging of the lung parenchymawith CT requires relatively fewer x-ray photons to generatediagnostic quality images compared with other parts of thebody, thus making ‘‘low-dose’’ thoracic CT more straight-forward. As with all applications of CT today, every effortshould be made to reduce radiation exposure following theALARA principle of ‘‘as low as reasonably achievable.’’1
The use of HRCT as part of a multidisciplinaryapproach by pulmonary medicine specialists, radiologists,and pathologists to evaluate patients with diffuse lungdisease (DLD) has been shown to be helpful in arriving atthe correct final diagnosis of DLD.2 It has also been shown
that the HRCT lung findings in interstitial lung diseasesmay have survival implications for patients.3,4
In this review, we aim to illustrate various aspects ofHRCT, including technical aspects, radiation exposure,lung anatomy relevant to HRCT, and clinical utility fordiagnosing and managing various lung diseases.
IMAGE ACQUISITION AND EVALUATIONThe primary objective of HRCT is to obtain optimal
spatial resolution for accurate anatomic depiction of thelung parenchyma and the evaluation of the extent anddistribution of lung abnormalities. This allows accuratedepiction of fine lung detail and also helps avoid manypitfalls of incremental scanning, such as difficulty in differ-entiating small lung nodules from vessels and bronchiecta-sis from true honeycombing. The technique used shouldbe reproducible for accurate comparison and follow-up.Although it is important to maintain optimal image quality,radiation exposure should be kept to the minimum necessaryto obtain images of sufficient diagnostic quality, throughmeticulous attention to the technical parameters used.
There are many different ways in which an HRCTexamination can be obtained, which can be tailored to thesuspected or known disease process. Common to all HRCTprotocols are thin collimation of 1.5mm or less, coupledwith a high spatial frequency reconstruction algorithm, tomaximize fine lung detail. The 2 most widely used methodsare the incremental acquisition technique, in which axial imagesare obtained at 1 to 2 cm increments throughout the lungs,and volumetric acquisition, in which the entire lungs areimaged helically in a continuous manner. The incrementalmethod was mostly used before CT scanners of 16 detectorsor more became widely available, permitting consistentsingle breath-hold imaging of the entire lungs at thincollimation and without tube cooling issues routinely due toincreased scanning speed.5
Data AcquisitionHRCT protocols usually consist of several acquisi-
tions, optimized to evaluate the lung parenchyma for DLDand airway disease by combining differences in breathholding and patient positioning. Our current standardHRCT protocol consists of a volumetric inspiratory supineacquisition, incremental expiratory supine acquisition, andincremental inspiratory prone acquisition, which permitsevaluation of both infiltrative and obstructive lung diseases.
CT Scanning ParametersGeneral technical parameters for HRCT include 100 to
120 kVp at 40 to 100mAs. The technique can be modifiedaccording to patient body habitus, using the body massCopyright r 2010 by Lippincott Williams & Wilkins
From the Department of Radiology, University of Michigan HealthSystem, Ann Arbor, MI.
Reprints: Baskaran Sundaram, MD, Department of Radiology,University of Michigan Health System, Cardiovascular Center#5481, 1500 East Medical Center Drive, Ann Arbor, MI 48109-5868 (e-mail: [email protected]).
SYMPOSIA
J Thorac Imaging � Volume 25, Number 2, May 2010 www.thoracicimaging.com | 125

index or circumference of the thorax. Higher milliampereseconds and kilovolt peak are used for larger patients andlower values for smaller-sized patients and for the pediatricpopulation, balancing image noise and radiation exposurewith sufficient diagnostic quality. Thin collimation of 1.5mmor less is important in HRCT to reduce the volume-averaging artifacts and increase the spatial resolution inthe images, enabling us to visualize subtle lung findings.Although thinner collimation of 0.5 to 0.6mm is availablecurrently on many CT scanners, it has not yet been shownto provide additional clinically relevant information over themore commonly used 1 to 1.5mm collimation for HRCT. Afast CT gantry rotation time, often sub-second, is also idealto reduce motion artifacts.6 Typically, the 360-degreerotation time for current CT scanners is of the order of350 to 500ms.7 Patients are comfortably able to hold theirbreath for that amount of short volumetric acquisitions,which reduces respiratory motion artifacts. Cardiac motionartifacts are also reduced, as a typical left ventriculardiastole lasts about 500ms.8
Patient Positioning and Respiratory PhaseMost thoracic imaging, including HRCT, is obtained
with the patient in a supine position, the standard anatomicposition for thoracic CT examinations. Prone images areimportant, both when the nondependent lung parenchymais normal on the supine images to distinguish betweendependent atelectasis versus mild lung disease and to elimi-nate superimposed atelectasis, which may make diseaseseem more severe than it really is, by exaggerating ground-glass opacity (GGO). Images are usually obtained followingseveral breaths in and out, with the patient holding his orher breath in deep inspiration to allow optimal tissue
contrast within the lung parenchyma between normalaerated tissue, normal anatomy, and disease. If the patientis not able to hold his or her breath and remain motionlessduring the scan, the images may be suboptimal for theevaluation of the lungs. In this situation, the scan can beobtained in 2 consecutive but shorter acquisitions to reducethe duration of breath-hold. The scan direction can also bemodified to scan in the caudal-to-cranial direction, thereverse of most examinations, so that the lower lung imagesare acquired first, in the event the patient exhales, as motionat the lung bases with the movement of the diaphragmcreates more artifacts than exhaling while scanning the lungapices. A less ideal solution is to increase the pitch or tablespeed to reduce the total imaging time, at the expense ofspatial resolution, as this results in an increase in effectiveslice thickness.8 Images can also be obtained duringdynamic expiration or at static end-expiration to evaluatefor air trapping in the lung parenchyma as evidence of smallairway disease and tracheobronchomalacia of the centralairway.
Image Reconstruction Plane, Interslice Gap,and Algorithm
Volumetric acquisitions are reconstructed using over-lapping or continuous increments with no interslice gaps.This is advantageous for detecting and comparing smalllung nodules or tracing small airways to, respectively,differentiate them from blood vessels and honeycombing(Fig. 1).9 The reconstruction algorithm is the filter appliedto the raw data set for image reconstruction. Conventionalimaging is obtained with low spatial frequency and lownoise algorithm for soft tissue reconstruction. A highspecial frequency algorithm is typically applied for HRCT
FIGURE 1. A and B, Volumetric HRCT. Focal thin-walled multiple cystic lesions in the right upper lobe on an axial HRCT image suggestcentrilobular emphysema or cystic lung disease or early honeycombing (arrow in A). Coronal reconstruction image from the volumetricHRCT examination clearly shows focal bronchiectasis (curved arrow in B).
Sundaram et al J Thorac Imaging � Volume 25, Number 2, May 2010
126 | www.thoracicimaging.com r 2010 Lippincott Williams & Wilkins

image reconstruction, which increases spatial resolution,providing edge enhancement and higher contrast, whichreduces image smoothing and increases image noise.10
Image EvaluationImages are usually reviewed on a picture archiving and
communication systems or image review workstation. Thechoice of window width and level settings is important,particularly when comparing examinations. Typically, thewindow level used ranges from �500 to �600HU, with awindow width of 1500 to 2000HU. The window settings canbe modified in individual cases to depict finer detail. Imagesmay be viewed in a 2-dimensional (axial, coronal, and sagittalplanes) and a 3-dimensional manner (volume-renderedimages, maximum and minimum intensity projections).11
Multiplanar viewing may help to better appreciate the exactand predominant distribution of parenchymal disease, withcoronal images mimicking a frontal chest radiographicimage, and sagittal images mimicking a lateral radiographicimage.12 Sliding slab maximum intensity projection imagesaid in the detection of small pulmonary nodules.13 Pulmo-nary micronodules and their orientation to the secondarypulmonary lobule anatomy may be better appreciated withvolumetric data sets that permit rotation of the anatomyunder review into the best plane.14,15 Similarly, even subtleemphysema may be better appreciated with sliding minimumintensity projection images than with routine HRCTviews.15,16
HRCT LUNG ANATOMYThe smallest functional unit displayed on HRCT
images is the secondary pulmonary lobule (Fig. 2).17,18
The secondary pulmonary lobule is a polygonal structure, 1
to 4 cm in diameter, and bounded by the interlobular septa.Interlobular septa contain pulmonary veins that collectoxygenated blood from the pulmonary acini. Each second-ary pulmonary lobule contains 3 to 24 acini clusteredtogether beyond the terminal bronchiole. The centralbronchovascular core of each lobule has several terminalbronchioles, each with an adjacent small pulmonary artery.The terminal bronchioles bifurcate into clusters of pulmonaryacini, each of which is a collection of alveoli. Lymphatics arepresent both around the central bronchovascular structuresand within the interlobular septae. Generally, in normalsecondary pulmonary lobules, it is difficult to visualize mostof these structures on HRCT, with the exception of theterminal pulmonary artery branches as a small nodule in thecentrilobular location. More specifically, Murata et al,19
using 4 inflation-fixed lungs obtained from autopsy, showedthat HRCT is capable of showing normal pulmonary arterybranches as small as 200mm in diameter, and noted that thedistance between these vessels and the lobule border rangesfrom 3 to 5mm.
Understanding the HRCT findings in relation to thesecondary pulmonary lobule architecture is important tocategorize interstitial lung disease for the purposes ofdifferential diagnosis. HRCT abnormalities in DLD maybe categorized as primarily linear, nodular, high- or low-attenuation lesions. On the basis of the distribution of theseabnormalities in relation to the secondary pulmonarylobule, lung nodules can be further subcategorized ascentrilobular, perilymphatic, or random. The predominantgroup of nodules and their distribution may suggest specificdiseases, such as acute hypersensitivity pneumonitis (HP)or respiratory bronchiolitis (centrilobular), sarcoidosis(perilymphatic), and military infections or tumors (ran-dom). HRCT abnormalities can be described in a standard-ized manner using the glossary of terms described by theFleischner society.20
RADIATION EXPOSURERadiation exposure from a CT examination is based
on many variables, including both patient-related factorsand CT technical parameters. Whether a helical ornonhelical technique is used, the goal is to obtain imagesof sufficient diagnostic quality using radiation exposuresthat are as low as reasonably achievable.1 Mayo et al21
reported that the skin radiation dose using specific scanningparameters of 120 kVp, 200mA, and 2 seconds of gantryrotation time and incremental HRCT technique with a 10-mm to 20-mm gap between HRCT slices results in muchlower radiation exposure than routine helical CT. Similarly,van der Bruggen-Bogaarts et al22 reported that the effectiveradiation exposure is 6.5 times lower for axial nonvolu-metric HRCT than helical CT. As radiation exposureduring CT scanning has a linear relationship with CTscanner tube current, many investigators have attempted toreduce the tube current and have now established the utilityof low-dose helical chest CT examinations.23,24
The inherent high contrast difference between the airwithin the alveoli of the lung and lung tissue has madelower-dose thoracic CT examinations possible, and at lowerexposure levels than possible for CT examinations of otherbody parts.25 Lowering tube current may degrade imagequality by decreasing the signal-to-noise ratio, probablymore so in helical volumetric HRCT than axial HRCT,leading to concerns about image quality.26 However,
FIGURE 2. Schematic illustration of secondary pulmonary lobule.Secondary pulmonary lobules are bounded by interlobular septa(arrows), which contain the pulmonary veins (red). The centralbronchovascular core is composed of a pulmonary artery (curvedarrow) and accompanying terminal airway (arrowhead). Theterminal bronchovascular core is surrounded by clusters ofpulmonary acini (A), where gas exchange takes place.
J Thorac Imaging � Volume 25, Number 2, May 2010 Multidetector HRCT of Lungs
r 2010 Lippincott Williams & Wilkins www.thoracicimaging.com | 127
Zwirewich et al25 evaluated a low radiation exposureHRCT examination technique (20mA, 2 s rotation speed,120 kVp, 1.5-mm collimation), showing equal diagnosticquality to a higher radiation exposure HRCT examinationtechnique (200mA, 2 s rotation speed, 120 kVp, 1.5-mmcollimation). Leswick et al26 compared radiation exposurebetween routine helical chest CT (1.25mm�8, 130mAs,120 kVp, and 0.875 pitch) and nonvolumetric HRCT(1.25mm�10, 170mAs, and 120 kVp) and a combinationCT acquisition (1.25mm�8, 225mAs, 120 kV, and 0.875pitch) that was used to generate contiguous 5-mm and 1.25-mm axial images. Initially, they established that 225mAshelical CT had a similar noise index to an axial nonvolu-metric HRCT after testing a female water phantom atvarious 10-mA increments. They reported that combinationCT acquisition resulted in higher radiation exposure to thecentral chest (33% higher; P=0.001), breast (25% higher;P<0.05), and total body (32% higher; P<0.001), andlower average radiation exposure to the ovaries (25%lower; P<0.01), which, presumably, was secondary toshorter scanning time.
CLINICAL APPLICATIONS
Diffuse Lung DiseaseHRCT is a well-established technique to evaluate for
DLD in advanced disease, early-stage disease, or evenpreclinical disease.27,28 As with almost all diagnostic tests,a normal HRCT may not exclude DLD.29 Although theremay be no major differences in diagnosing DLD usingeither an incremental HRCT scan at regular increments oreven fewer HRCT images, let alone helical technique incases of sufficient severity to warrant surgical biopsy, theimpact of incremental versus helical HRCT on sensitivityfor disease or specific diagnosis has not been evaluated.30 Itis important to understand that the information obtainedfrom HRCT is used for many different reasons, fromdifferential diagnosis to the evaluation of disease activity,
and evaluating temporal change in disease with treatment.In addition, many patients with DLD are at increased riskfor lung malignancy31–34; therefore, being able to consis-tently view and evaluate these nodules on the serial HRCTexaminations these patients may undergo over time is veryimportant.
DLD categorization has continued to evolve over theyears, as our understanding of these diseases improvesthrough the process of scientific inquiry. The internationalmultidisciplinary consensus statement from the AmericanThoracic Society and European Respiratory Societyclassifies DLD into discrete groups as follows: (a)idiopathic: idiopathic pulmonary fibrosis usual interstitialpneumonitis (UIP), desquamative interstitial pneumonitis(DIP), acute interstitial pneumonitis, nonspecific interstitialpneumonitis (NSIP), respiratory bronchiolitis-interstitiallung disease (RB-ILD), cryptogenic organizing pneumonia(COP), and lymphocytic interstitial pneumonits (LIP);(b) secondary (such as collagen vascular disease or drugs);(c) granulomatous disease (such as sarcoid); and (d) otherforms (cystic lung diseases).35
Idiopathic Interstitial PneumoniaDLDs with no identifiable etiology are considered
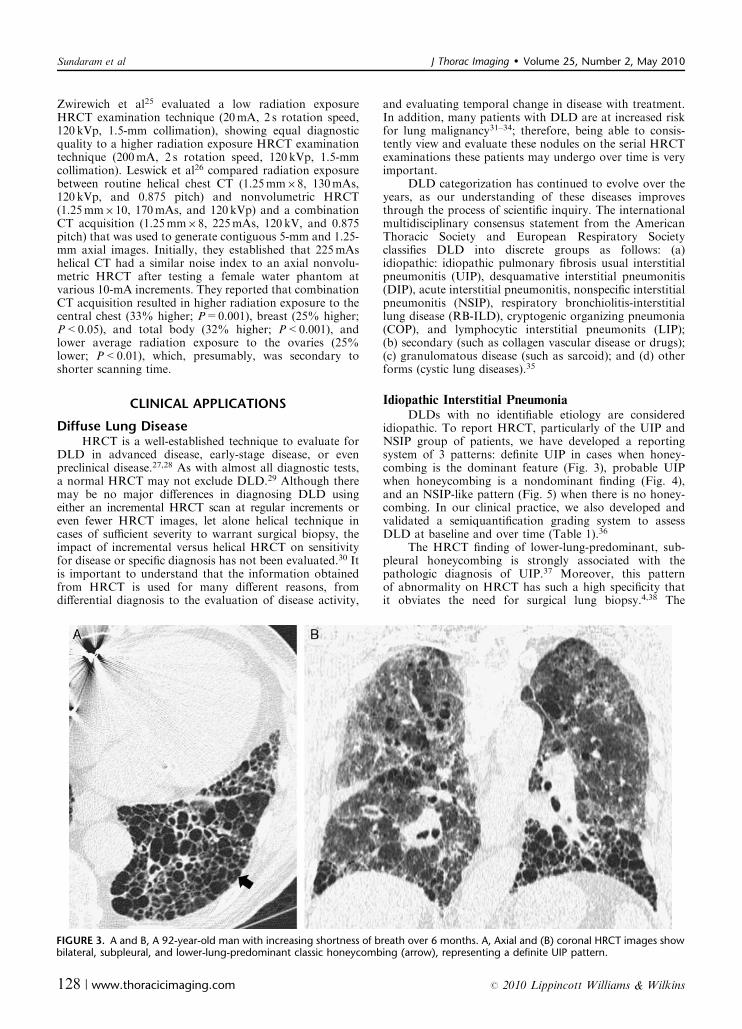
idiopathic. To report HRCT, particularly of the UIP andNSIP group of patients, we have developed a reportingsystem of 3 patterns: definite UIP in cases when honey-combing is the dominant feature (Fig. 3), probable UIPwhen honeycombing is a nondominant finding (Fig. 4),and an NSIP-like pattern (Fig. 5) when there is no honey-combing. In our clinical practice, we also developed andvalidated a semiquantification grading system to assessDLD at baseline and over time (Table 1).36
The HRCT finding of lower-lung-predominant, sub-pleural honeycombing is strongly associated with thepathologic diagnosis of UIP.37 Moreover, this patternof abnormality on HRCT has such a high specificity thatit obviates the need for surgical lung biopsy.4,38 The
FIGURE 3. A and B, A 92-year-old man with increasing shortness of breath over 6 months. A, Axial and (B) coronal HRCT images showbilateral, subpleural, and lower-lung-predominant classic honeycombing (arrow), representing a definite UIP pattern.
Sundaram et al J Thorac Imaging � Volume 25, Number 2, May 2010
128 | www.thoracicimaging.com r 2010 Lippincott Williams & Wilkins

limitation of this pattern is that many patients with UIPhave an ‘‘NSIP-like’’ appearance, dominated by septal linesand GGO in the absence of honeycombing, such that thispattern has limited sensitivity for UIP. In fact, for patientswith an NSIP-like pattern on HRCT, it has been shownthat the diagnosis of NSIP versus UIP is almost equallylikely at surgical lung biopsy.4 Hence, in the absence oftypical HRCT findings of UIP, tissue diagnosis is advisedto confirm the diagnosis.4
Similarly, HRCT features of chronic HP could alsosignificantly overlap with UIP. A patchy distribution of the
same pattern of UIP HRCT findings should raise suspicionof chronic HP, particularly in the context of upper-lung-dominant distribution. Pathologically, a combination ofrelatively lesser cellularity, temporal heterogeneity, honey-combing, and fibroblastic foci suggests UIP and not chronicHP. Despite the large size of the pathologic specimensobtained during surgical lung biopsy, sampling error stillexists in diagnosing DLD. Hence, we emphasize incorpor-ating HRCT findings, clinical and lung functional informa-tion, and histopathologic information in a multidisciplinarymanner to arrive at the correct DLD diagnosis.2
FIGURE 5. A and B, A 60-year-old woman with lower-lung-dominant bilateral ground-glass attenuation lesion and tractionbronchiecatasis (arrow) and no honeycombing, suggesting an NSIP pattern. Subsequent surgical lung biopsy diagnosis was UIP.
FIGURE 4. A and B, A 75-year-old man with progressive declining pulmonary functions. His HRCT showed scattered subpleural patchesof minor foci of honeycomb (arrows) and lower-lung-dominant interlobular septal thickening, traction bronchiectasis, and minimalGGO, suggesting probable UIP pattern. Surgical lung biopsy confirmed UIP.
J Thorac Imaging � Volume 25, Number 2, May 2010 Multidetector HRCT of Lungs
r 2010 Lippincott Williams & Wilkins www.thoracicimaging.com | 129
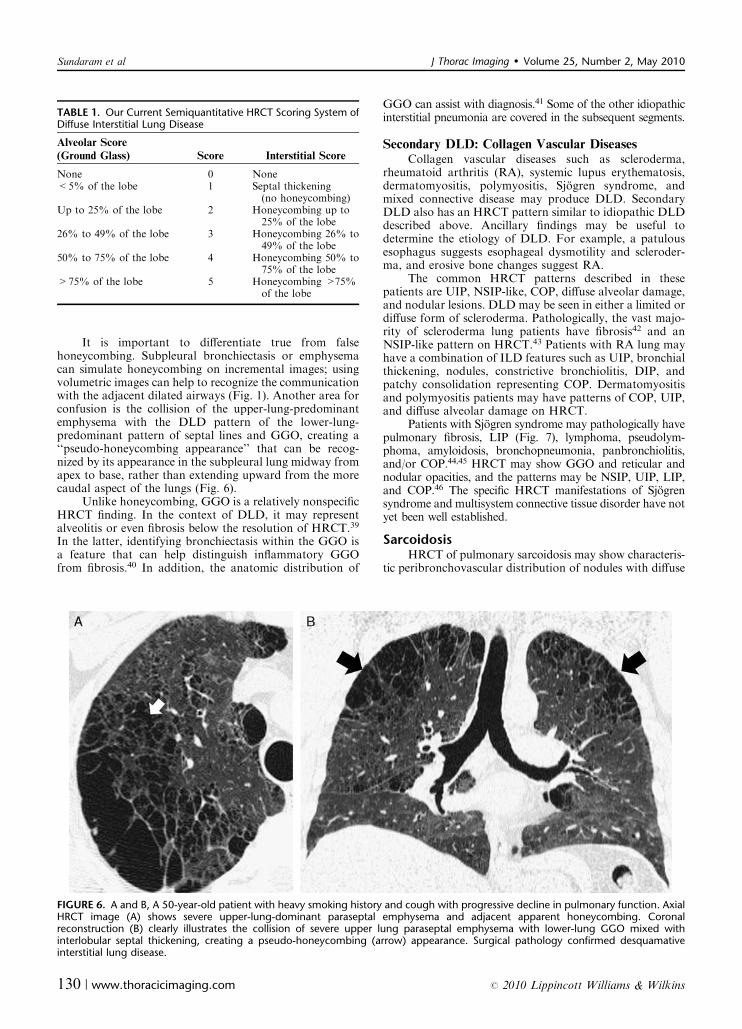
It is important to differentiate true from falsehoneycombing. Subpleural bronchiectasis or emphysemacan simulate honeycombing on incremental images; usingvolumetric images can help to recognize the communicationwith the adjacent dilated airways (Fig. 1). Another area forconfusion is the collision of the upper-lung-predominantemphysema with the DLD pattern of the lower-lung-predominant pattern of septal lines and GGO, creating a‘‘pseudo-honeycombing appearance’’ that can be recog-nized by its appearance in the subpleural lung midway fromapex to base, rather than extending upward from the morecaudal aspect of the lungs (Fig. 6).
Unlike honeycombing, GGO is a relatively nonspecificHRCT finding. In the context of DLD, it may representalveolitis or even fibrosis below the resolution of HRCT.39
In the latter, identifying bronchiectasis within the GGO isa feature that can help distinguish inflammatory GGOfrom fibrosis.40 In addition, the anatomic distribution of
GGO can assist with diagnosis.41 Some of the other idiopathicinterstitial pneumonia are covered in the subsequent segments.
Secondary DLD: Collagen Vascular DiseasesCollagen vascular diseases such as scleroderma,
rheumatoid arthritis (RA), systemic lupus erythematosis,dermatomyositis, polymyositis, Sjogren syndrome, andmixed connective disease may produce DLD. SecondaryDLD also has an HRCT pattern similar to idiopathic DLDdescribed above. Ancillary findings may be useful todetermine the etiology of DLD. For example, a patulousesophagus suggests esophageal dysmotility and scleroder-ma, and erosive bone changes suggest RA.
The common HRCT patterns described in thesepatients are UIP, NSIP-like, COP, diffuse alveolar damage,and nodular lesions. DLD may be seen in either a limited ordiffuse form of scleroderma. Pathologically, the vast majo-rity of scleroderma lung patients have fibrosis42 and anNSIP-like pattern on HRCT.43 Patients with RA lung mayhave a combination of ILD features such as UIP, bronchialthickening, nodules, constrictive bronchiolitis, DIP, andpatchy consolidation representing COP. Dermatomyositisand polymyositis patients may have patterns of COP, UIP,and diffuse alveolar damage on HRCT.
Patients with Sjogren syndrome may pathologically havepulmonary fibrosis, LIP (Fig. 7), lymphoma, pseudolym-phoma, amyloidosis, bronchopneumonia, panbronchiolitis,and/or COP.44,45 HRCT may show GGO and reticular andnodular opacities, and the patterns may be NSIP, UIP, LIP,and COP.46 The specific HRCT manifestations of Sjogrensyndrome and multisystem connective tissue disorder have notyet been well established.
SarcoidosisHRCT of pulmonary sarcoidosis may show characteris-
tic peribronchovascular distribution of nodules with diffuse
FIGURE 6. A and B, A 50-year-old patient with heavy smoking history and cough with progressive decline in pulmonary function. AxialHRCT image (A) shows severe upper-lung-dominant paraseptal emphysema and adjacent apparent honeycombing. Coronalreconstruction (B) clearly illustrates the collision of severe upper lung paraseptal emphysema with lower-lung GGO mixed withinterlobular septal thickening, creating a pseudo-honeycombing (arrow) appearance. Surgical pathology confirmed desquamativeinterstitial lung disease.
TABLE 1. Our Current Semiquantitative HRCT Scoring System ofDiffuse Interstitial Lung Disease
Alveolar Score
(Ground Glass) Score Interstitial Score
None 0 None<5% of the lobe 1 Septal thickening
(no honeycombing)Up to 25% of the lobe 2 Honeycombing up to
25% of the lobe26% to 49% of the lobe 3 Honeycombing 26% to
49% of the lobe50% to 75% of the lobe 4 Honeycombing 50% to
75% of the lobe>75% of the lobe 5 Honeycombing >75%
of the lobe
Sundaram et al J Thorac Imaging � Volume 25, Number 2, May 2010
130 | www.thoracicimaging.com r 2010 Lippincott Williams & Wilkins

thickening, GGO, bronchiectasis, focal consolidation, lungnodules, parenchymal distortion, lines, honeycombing, andmediastinal enlarged lymph nodes (Fig. 8). Typically, thecentral and upper lungs are involved. Depending upon thestage of the disease process, severity, activity, and therapy,
these patients may have a combination of the above-mentioned findings. Air trapping in sarcoidosis is common,seen in 95% of HRCT examinations in 1 series of21 patients, and correlates with small airway disease foundon pulmonary function tests. Furthermore, as shown in
FIGURE 7. A and B, A 59-year-old woman with scleroderma presenting with worsening exertional breathlessness. Axial (A) andcoronal reformatted images (B) from her HRCT illustrate lower-lung-dominant interstitial lung disease as evidenced by GGO,interlobular septal thickening, and traction bronchiectasis (arrow). There were also thin-walled pulmonary cysts (curved arrow). Herlower esophagus (arrowhead) also was dilated due to scleroderma-induced esophageal dysmotility. Appearances are felt to becharacteristic of LIP.
FIGURE 8. A and B, A 50-year-old man with chronic cough and abnormal hila on chest radiograph. HRCT shows (A) enlarged lymphnodes (arrow in A) in the mediastinum and bilateral hila with peribronchovascular nodules (arrowhead in B) and thickening (curvedarrow in B), characteristic of sarcoidosis. Transbronchial biopsy revealed multiple epithelioid granulomas in the alveolar parenchyma andbronchial wall, confirming sarcoidosis.
J Thorac Imaging � Volume 25, Number 2, May 2010 Multidetector HRCT of Lungs
r 2010 Lippincott Williams & Wilkins www.thoracicimaging.com | 131

one study of 29 patients with sarcoidosis, the mean extentof nodules and consolidation on HRCT reflects diseaseactivity, as quantified by 67 Gallium scintography, broncho-alveolar lavage, and serum angiotensin converting enzymeassay.47 In contrast, HRCT findings of GGO, nodularity,septal thickening, traction bronchiectasis, and parenchymaldistortion do not correlate well with lung function.48 Thesmall nodules seen on HRCT have been shown tocorrespond to granulomas on surgical lung biopsy, whereasresting lung function in these same patients correlatespoorly with the presence and extent of disease on HRCT.49
Patients with sarcoidosis, who predominantly have GGOand consolidation on their initial HRCT, may have a poorprognosis compared with other patients with sarcoidosiswith progressive decline in their lung function.50
Cystic Lung DiseaseSimple lung cysts are uniform, approximately 1 to
2 cm or less in diameter, thin-walled, air-containing lesionswith usually no mural nodules or wall thickening. Simplelung cysts are sometimes confused with emphysema,honeycombing, and cavitary lung disease within preexistingdisease such as cystic malignancy, infection, and granulo-ma. In contrast to cysts, emphysema has no perceptiblewall, and honeycombing lesions are thick and irregularlywalled. Lymphangiomyomatosis (LAM; Fig. 9) is a diseasecharacterized by the proliferation of smooth muscle in thewall of lymphatic channels, which occludes lymphatic flowresulting in rupture of these channels, hence the finding ofassociated chylous pleural effusions. Subsequently, cysticlung lesions develop because of obstruction of the terminalbronchioles that are surrounded by these abnormallymphatic vessels. The cysts in LAM are usually fairly
uniform in size and are uniformly distributed throughoutthe lungs, both apex to base, and axial to peripheral lung.Some patients may have associated enlarged lymph nodes.LAM is a disease that occurs mainly in women of child-bearing age.
Langerhans cell histiocytosis (LCH; Fig. 10) is anothercystic lung disease that can be differentiated from LAM inmany ways. The cysts in LCH are usually irregular in shapeand size, and associated with small irregular nodules thatare also of varying size and may be cavitary. LCH is one ofthe smoking-related lung diseases, all of which are morecommon in the upper lungs, where there is relatively lessventilation and perfusion, allowing for greater concentra-tion of the toxins from inhaled smoke and relatively lessmacrophage delivery.
A few other cystic lung diseases deserve mention,including lung cysts in the context of Sjogren disease orHIV infection, which represent LIP,51 and cysts in chronicPneumocytsis jiroveci pneumonia.52
Airway DiseaseCT is the noninvasive imaging of choice for diagnosing
both large and small airway disease. Multidetector HRCTcan both image the anatomy of the airways in multi-dimensional planes, which has eliminated diagnosticbronchography, and also identify secondary evidence ofairway disease in the form of air trapping (Fig. 11) onexpiratory images. Sometimes, the latter is the earliestevidence of small airway disease, at a stage when the smallairways appear morphologically normal.
The common manifestations of small airway diseaseare bronchiectasis, bronchial wall thickening, and airtrapping. Bronchiectasis is generally divided into 3 types:
FIGURE 9. A and B, A 83-year-old woman with clinical features of reactive airway disease and obstructive pulmonary function tests.HRCT shows multiple thin-walled lung cysts (arrow) that were evenly distributed from lung apex to base, and from center to peripheryof the lungs.
Sundaram et al J Thorac Imaging � Volume 25, Number 2, May 2010
132 | www.thoracicimaging.com r 2010 Lippincott Williams & Wilkins

cylindrical, varicose, and cystic. If one assumes that thepulmonary arteries are normal in size, a bronchus that islarger in cross-section than the adjacent artery is consideredabnormally dilated. This has been referred to as the signetring sign or pearl ring sign. Caution should be used whenapplying this criterion at high altitudes where there isnormally some degree of vasoconstriction, so that thearteries may be smaller than the bronchi in the normalstate.53
Large airway diseases include infection (bacterial,mycobacterial, viral, fungal), mucociliary dysfunction (cysticfibrosis, Kartagener syndrome) (Fig. 12), congenital dis-orders (Mounier-Kuhn syndrome, Williams-Campbell syn-drome, bronchopulmonary sequestration), immune disorders(AIDS, hypogammaglobulinemia), postobstructive (tumor,foreign body), collagen vascular disorders (RA, Sjogrensyndrome, ankylosing spondilitis, relapsing polychondritis),aspiration, asthma, and sarcoidosis.54 HRCT findings ofbronchiectasis, bronchial wall thickening, air trapping, andmucoid impaction may overlap among these. However, inmany conditions, the distribution of abnormalities and associa-ted features may narrow the differential diagnosis. Forexample, the central airway abnormalities with glove-fingerappearance of central mucous plugging abnormali-ties suggest allergic bronchopulmonary aspergillosis.55
Similarly, an upper lung distribution of bronchiectasis sug-gests cystic fibrosis.56 Mounier-Kuhn syndrome is tracheo-megaly, often associated with bronchiectasis.57
Small airway diseases may be primary or secondaryto the interstitial disease with bronchiolar involvement.58The primary bronchiolar diseases include constrictivebronchiolitis, acute bronchiolitis, diffuse panbronchiolitis,RB-ILD, and follicular bronchiolitis. Secondary bronchio-lar diseases due to interstitial lung disease include HP, RB,DIP, and COP. Among the primary bronchiolar diseases,the HRCT features overlap and include bronchiectasis,bronchiolectasis, airway wall thickening, mucoid impactionresulting in centrilobular nodules, tree-in-bud appearance,and air trapping.
The utility of a volumetric HRCT over nonvolumetricscans to diagnose bronchiectasis was shown as early as1994 by Engeler et al.59 More recently, Lucidarme et al60
reported the added benefit of volumetric HRCT overincremental HRCT in diagnosing bronchiectasis in 50consecutive patients. Incremental HRCT images (120 kV,175mAs, 1.5-mm collimation at 10-mm intervals of theentire lungs) and volumetric HRCT images (120 kV, and150mAs, 3-mm collimation, 4.8mm/s table increments witha pitch of 1.6; from 15mm above the carina down to thebases of the lung) were compared independently forbronchiectasis by 3 observers in both blinded and consensusmanner. The extent of bronchiectasis detected was moreextensive with volumetric HRCT in segments through thedistal bronchi (k=0.77; P<10�9) compared with incre-mental HRCT (k=0.27; P=not significant). It is impor-tant to note that in their study the measured skin radiation
FIGURE 10. A and B, A 35-year-old woman with a 30 pack-year smoking history and pituitary insufficiency underwent HRCT to evaluatefor possible sarcoidosis. Axial HRCT (A) showed upper- and central-lung-predominant innumerable centrilobular ground-glassattenuation nodules (arrow), cysts (curved arrow), and emphysema (arrowhead). Surgical lung biopsy suggested respiratorybronchiolitis-associated interstitial lung disease. She successfully stopped smoking. HRCT obtained 22 months later (B) showedsignificant resolution of nodules. Her pulmonary function test parameters had also significantly improved. The pituitary findings werepresumed to be due to pituitary eosinophilic granulomatosis.
J Thorac Imaging � Volume 25, Number 2, May 2010 Multidetector HRCT of Lungs
r 2010 Lippincott Williams & Wilkins www.thoracicimaging.com | 133

exposure was 3.4 times higher in volumetric than inincremental HRCT. Dodd et al61 also reported theimproved performance of volumetric HRCT imaging indetecting bronchiectasis in a series of 61 patients. Volu-metric HRCT (1-mm thickness, 15-mm table speed perrotation, 0.5-s gantry rotation time, 120 kVp, and 130mAs,reconstructed using bone algorithm) images at full inspira-tion from lung apex to base and simulated incrementalHRCT (1-mm slices at 10-mm intervals) images weregenerated from the volumetric HRCT, with the lattershowing a higher prevalence of bronchiectasis (P<0.0001;good consensus interobserver agreement values), greaterextent of bronchiectasis within a lobe (P<0.0001; verygood consensus interobserver agreement values), and higherseverity (P<0.0001; good consensus interobserver agree-ment values) of bronchiectasis. Using consensus volumetricHRCT findings as the gold standard, performance of incre-mental HRCT for detecting bronchiectasis was as follows:prevalence 42%; sensitivity 71% (95% confidence interval=64-78%); specificity 93% (95% confidence interval=90-96%); and positive and negative predictive values,88% and 81%, respectively.
Emphysema AnalysisBeyond medical therapy and pulmonary rehabilita-
tion, the treatment options for severe emphysema includelung transplantation and surgery designed to improve respi-ratory mechanics, including lung volume reduction surgery(LVRS), bullectomy, and endobronchial valve proce-dures.62 HRCT plays a key role in patient selection forthese procedures as the best in vivo tool to evaluate regionalemphysema severity and distribution and to evaluate forpotential comorbid conditions. LVRS has been shown tohave a short-term and long-term impact on clinical andfunctional parameters, with positive long-term outcomebeing debatable.63,64 Preoperative emphysema quantifica-tion by HRCT is shown to correlate with postoperativeoutcome. More specifically, patients with severe emphyse-ma homogenously distributed from lung apex to base havebeen identified to have high mortality after LVRS,65–69
whereas patients with upper-lung-predominant emphyse-ma, often referred to as heterogeneous emphysema, havethe best outcome. This is one of the most important criteriafor selecting patients to undergo LVRS.66,67,70,71 The roleof HRCT in emphysema in this setting is to evaluate the
FIGURE 11. A and B, A 50-year-old woman with proven sarcoidosis and a restrictive small airway disease pattern on pulmonary functiontests. HRCT images obtained at end inspiration (A) shows unremarkable lung parenchyma and an image during end expiration (B)shows alternative high-attenuating and low-attenuating lower-lung parenchyma, suggesting air trapping evident in the left lower lobe.
Sundaram et al J Thorac Imaging � Volume 25, Number 2, May 2010
134 | www.thoracicimaging.com r 2010 Lippincott Williams & Wilkins

severity and distribution of emphysema, and the presence ofbronchiectasis and related findings such as pulmonaryartery enlargement and potential lung malignancy.
Preoperative assessment of the degree and quantity ofemphysema may be performed easily with HRCT images(Fig. 13). HRCT quantification is a sensitive tool forassessing longitudinal changes in emphysema and followingspecific therapy.72–74 Using computer attenuation-basedanalysis, referred to as the density mask technique, therange of lung tissue that is abnormally low in attenuationvalues can be quantified as emphysema. This has beenshown to correlate well with the pathologic grade ofemphysema.75 Different HRCT reconstruction algorithmsimpact density mask-based emphysema quantification, asdoes slice thickness.76 Recently, lung texture-based quantifi-cation has been shown to correlate better with pulmonaryfunction tests than the density mask technique.77 Somehave suggested that a simple visual score may be just asreliable as sophisticated analysis in the quantitative analysisof emphysema78; however, this may be too gross to evaluatefor short-term changes in disease, as it lacks sufficientreliably reproducible detailed analysis. Recent studiessuggest that objective emphysema quantification withattenuation thresholds may perform better than subjectiveassessment.79,80 Although there may be some relationshipbetween the objective and subjective emphysema assess-ment for its severity and distribution, there is higher repeat-ability of the quantitative CT indices using volumetricimaging of the entire lungs.78,81,82 In addition, CT emphysemaquantification based on attenuation values seems to havea high predictability of gas transfer reduction; however, theelastic recoil has not been thought to be correlated.83
InfectionThe role of HRCT in diagnosing pulmonary infections
is well known, particularly atypical and typical infections inimmunocompromised patients.84–91 HRCT reliably diagno-ses Pneumocysitis jiroveci pneumonia based on certainfindings such as nodular or patchy GGO, diffuse GGO inthe upper lungs with or without reticulations, and lungcysts (Fig. 14).87,92 Patients with cytomegalovirus pneumo-nia after bone marrow transplantation have bilateralasymmetric GGO, air space opacities, and centrilobularnodules.89 Although the halo sign is most commonlyassociated with invasive pulmonary aspergillosis, otherinfections should be kept in mind, particularly Candida.90
HRCT has also been shown to be useful in early diagnosis ofeven unusual infections such as severe acute respiratorysyndrome-associated coronavirus pneumonia.85 HRCT find-ings may also have prognostic significance in patients withpulmonary infections. For example, a study reports thatHRCT findings such as atelectasis, cavities, and pleuralthickening are shown to predict responders to infectionamong patients with mycobacterium avium complex.93
Similarly, another study reported that HRCT findingspredict disease progression in patients with culture-positivenon-mycobacterial tuberculosis with underlying cysticfibrosis.94
Smoking-related Interstitial Lung DiseasesSmoking-related interstitial lung diseases include LCH,
RB, and DIP. LCH was discussed earlier in the sectionon cystic lung diseases. RB is characterized on HRCTas upper-lung-predominant centrilobular GGO nodules,similar to acute HP. When patients with an RB are
FIGURE 12. A and B, A 21-year-old man with a known history of cystic fibrosis was evaluated for bilateral lung transplantation. As part ofhis workup, HRCT was performed that showed bilateral upper-lung bronchiectasis of varying degrees (arrow) with mucoid impactedthick-walled bronchi (curved arrow). In addition, there were areas of mosaic attenuation and bilateral hyperinflated lungs due to fixedair trapping.
J Thorac Imaging � Volume 25, Number 2, May 2010 Multidetector HRCT of Lungs
r 2010 Lippincott Williams & Wilkins www.thoracicimaging.com | 135

symptomatic, usually dyspnea, the same finding is con-sidered to represent RB-ILD. Patients with DIP havelower-lung-predominant GGO. RB, RB-ILD, and DIP havea significant overlap in their HRCT features, suggesting thatthey reflect various time frames of the same disease process.95
Asymptomatic healthy smokers are known to haveabnormal lungs on HRCT.96 Similarly, patients with asecond-hand smoking exposure have been shown to havesubclinical DIP and RB-ILD, with GGO and irregular/linear opacities on HRCT (Figs. 6, 15).97 Low attenuationareas on HRCT significantly correlate with abnormalpulmonary function tests,98 and air trapping may evenprecede these abnormalities.99 HRCT measurements ofairway thickening inversely correlate with airflow limitationand cumulative smoking history.100 A 5-year longitudinalHRCT study of smokers showed that continued smoking
results in increasing upper lung disease, and that the rate ofdisease progression does not slow down in the first few yearsafter smoking cessation.101
Occupational Lung DiseasesChronic dust exposures are known to result in ILDs,
including silicosis, coal worker’s pneumoconiosis, graphitepneumoconiosis, asbestosis, talcosis, welder’s lung, beryl-liosis, aluminum lung, hard metal lung disease, HP, andchemical pneumonitis. In silicosis, small, less than 1 cm,discrete solid nodules are found predominantly in the upperlungs and may increase in size over time, or coalesce toform large, partly calcified, conglomerate masses witharchitectural distortion and upward retraction of lung hilarstructures, associated with enlarged thoracic lymph nodesthat may have eggshell calcifications. Coal workers with
FIGURE 13. A to D, A 71-year-old woman with prior significant smoking history undergoing evaluation for exertional breathlessness.Pulmonary function tests suggested severe emphysema. A, Coronal and (B) sagittal HRCT images show severe emphysema in the upper lungs(arrows) and mild emphysema in the lower lungs (arrowheads). Density mask technique using �920HU showed that (C) 84.6% of the upperlungs is emphysema and (D) 37.2% of the lower lungs, with an upper versus lower lung emphysema ratio of 2.3. She successfully underwentbilateral upper lobe LVRS.
Sundaram et al J Thorac Imaging � Volume 25, Number 2, May 2010
136 | www.thoracicimaging.com r 2010 Lippincott Williams & Wilkins

rheumatoid disease may develop lung nodules even afterlow levels of dust exposures, known as Caplan syndrome.Similarly, systemic sclerosis is reported to occur more oftenin patients with silicosis, a condition known as Erasmussyndrome.102 The HRCT appearance of graphite pneumo-coniosis is similar to coal worker’s pneumoconiosis.
Asbestos exposure-related ILD is referred to asasbestosis, and is characterized by lower-lung-predominant,
peripheral interlobular septa thickening, subpleural bands,parenchymal lines, and honeycombing when severe. Asbes-tosis is often seen with asbestos-related calcified andnoncalcified pleural plaques (Fig. 16).
Intravenous drug abuse of oral medications containingmagnesium silicate, aluminum, and iron can producepulmonary talcosis, which appears on HRCT as diffusefine nodules and GGO. The inhalation of metallic iron
FIGURE 14. A and B, A 44-year-old woman with HIV and low CD4 cell count presents with 4 months of cough, dyspnea on exertion,and unintentional weight loss. Her HRCT showed bilateral upper- and central-lung-dominant central ground-glass attenuation (arrow)and minimal interlobular septal thickening, characteristic of Pneumocystis jiroveci pneumonia. She was successfully treated withsulfamethoxazole and trimethoprim.
FIGURE 15. A and B, A 25-year-old woman with significant smoking history had recent onset of breathlessness. Her HRCT showed fluffycentrilobular ground-glass nodules (arrow). Findings were considered to be characteristic of respiratory bronchiolitis.
J Thorac Imaging � Volume 25, Number 2, May 2010 Multidetector HRCT of Lungs
r 2010 Lippincott Williams & Wilkins www.thoracicimaging.com | 137

or iron oxide fumes along with other metallic dusts thathave a fibrogenic potential may result in welder’s lung,with centrilobular micronodules in the central mid-lungs.Berylliosis has many similarities to sarcoidosis, includingparenchymal nodules distributed along the bronchovascu-lar bundles in the upper lungs. Patients with aluminumtoxicity manifest on HRCT as a reticulonodular interstitialfibrosis pattern, mainly in the upper lungs.
Patients exposed to organic dust may develop HP.Depending on the etiology, this may be called farmer’slung, bird-fancier lung, mushroom worker’s lung, and
bagassosis. In the acute and subacute form of thedisease, HRCT shows upper-lung-dominant/ill-definedcentrilobular GGO nodules, whereas in the chronicphase, HRCT shows evidence of interstitial fibrosis,with irregular septal thickening, traction bronchiectasis,GGO, and honeycombing, the same findings seen withUIP, but in a patchy, geographic or mosaic-like distribu-tion, rather than the lower lung subpleural distribution ofUIP (Fig. 17). Often, the radiologist recognizing thispattern is the first to suggest chronic HP, and shouldrecommend that an extensive exposure history be taken.
FIGURE 17. A 50-year-old woman with progressive breathlessness and abnormal pulmonary function tests. Her axial (A) and coronal (B)HRCT images showed diffuse centrilobular ground-glass attenuation nodules (arrow). In addition, there were areas of lobular sparingand fixed air trapping (curved arrow). The appearances were thought to be characteristic of HP. Later, pathologic diagnosis of talcinhalation pneumonitis was made.
FIGURE 16. A and B, An 80-year-old veteran with significant occupational asbestos exposure during construction work. He hasprogressive dyspnea and increasing oxygen requirement. His pulmonary function tests revealed a restrictive pattern. His HRCT showsbilateral focal dense pleural calcified plaques (arrows) and lower-lung-dominant interstitial lung disease as evidenced by GGO,interlobular septal thickening (curved arrow), and traction bronchiectasis (arrowhead).
Sundaram et al J Thorac Imaging � Volume 25, Number 2, May 2010
138 | www.thoracicimaging.com r 2010 Lippincott Williams & Wilkins

Expiratory images may also show areas of air trapping inthese patients.
CONCLUSIONSIn conclusion, recent advancements in CT techniques
have made volumetric lung imaging possible in a reliableand reproducible manner in a single breath-hold. It isimportant to be cognizant of the radiation dose in HRCT,and appropriate clinical use of HRCT is recommended asper the ALARA principle. Current HRCT imaging hasbecome the noninvasive gold standard for the evaluation ofDLD, emphysema, and small and large airway disease.Using HRCT alone, a specific diagnosis can often be made.Even in cases in which the HRCT findings are atypical ornonspecific, it can direct surgical lung biopsy to the areas ofgreatest yield. HRCT features may also predict the surgicaland overall outcome in some DLDs. A multidisciplinaryapproach to the DLD is a critical element in arriving at thefinal correct diagnosis.
REFERENCES
1. Cascade PN, Webster EW, Kazerooni EA. Ineffective use ofradiology: the hidden cost. AJR Am J Roentgenol. 1998;170:561–564.
2. Flaherty KR, King TE Jr, Raghu G, et al. Idiopathicinterstitial pneumonia: what is the effect of a multidisciplinaryapproach to diagnosis? Am J Respir Crit Care Med. 2004;170:904–910.
3. Goh NS, Desai SR, Veeraraghavan S, et al. Interstitial lungdisease in systemic sclerosis: a simple staging system. Am JRespir Crit Care Med. 2008;177:1248–1254.
4. Flaherty KR, Thwaite EL, Kazerooni EA, et al. Radiologicalversus histological diagnosis in UIP and NSIP: survival impli-cations. Thorax. 2003;58:143–148.
5. Dawn SK, Gotway MB, Webb WR. Multidetector-row spiralcomputed tomography in the diagnosis of thoracic diseases.Respir Care. 2001;46:912–921.
6. Rubin GD, Leung AN, Robertson VJ, et al. Thoracic spiralCT: influence of subsecond gantry rotation on image quality.Radiology. 1998;208:771–776.
7. Remy-Jardin M, Tillie-Leblond I, Szapiro D, et al. CTangiography of pulmonary embolism in patients with under-lying respiratory disease: impact of multislice CT on imagequality and negative predictive value. Eur Radiol. 2002;12:1971–1978.
8. Remy-Jardin M, Dumont P, Remy J. High-resolution compu-ted tomography techniques in diffuse parenchymal lungdisease and their application to clinical practice. Semin RespirCrit Care Med. 2003;24:333–346.
9. Schoepf UJ, Bruening RD, Hong C, et al. Multislice helicalCT of focal and diffuse lung disease: comprehensive diagnosiswith reconstruction of contiguous and high-resolution CTsections from a single thin-collimation scan. AJR Am JRoentgenol. 2001;177:179–184.
10. Mayo JR, Webb WR, Gould R, et al. High-resolution CT ofthe lungs: an optimal approach. Radiology. 1987;163:507–510.
11. Beigelman-Aubry C, Hill C, Guibal A, et al. Multi-detectorrow CT and postprocessing techniques in the assessment ofdiffuse lung disease. Radiographics. 2005;25:1639–1652.
12. Remy-Jardin M, Campistron P, Amara A, et al. Usefulness ofcoronal reformations in the diagnostic evaluation of infiltra-tive lung disease. J Comput Assist Tomogr. 2003;27:266–273.
13. Kawel N, Seifert B, Luetolf M, et al. Effect of slab thicknesson the CT detection of pulmonary nodules: use of sliding thin-slab maximum intensity projection and volume rendering.AJR Am J Roentgenol. 2009;192:1324–1329.
14. Remy-Jardin M, Remy J, Artaud D, et al. Diffuse infiltrativelung disease: clinical value of sliding-thin-slab maximum
intensity projection ct scans in the detection of mild micro-nodular patterns. Radiology. 1996;200:333–339.
15. Bhalla M, Naidich DP, McGuinness G, et al. Diffuse lungdisease: assessment with helical CT—preliminary observationsof the role of maximum and minimum intensity projectionimages. Radiology. 1996;200:341–347.
16. Remy-Jardin M, Remy J, Gosselin B, et al. Sliding thin slab,minimum intensity projection technique in the diagnosis ofemphysema: histopathologic-CT correlation. Radiology. 1996;200:665–671.
17. Griffin CB, Primack SL. High-resolution CT: normal ana-tomy, techniques, and pitfalls. Radiol Clin North Am. 2001;39:1073–1090.
18. Webb WR. Thin-section CT of the secondary pulmonarylobule: anatomy and the image—the 2004 Fleischner lecture.Radiology. 2006;239:322–338.
19. Murata K, Itoh H, Todo G, et al. Centrilobular lesions of thelung: demonstration by high-resolution CT and pathologiccorrelation. Radiology. 1986;161:641–645.
20. Hansell DM, Bankier AA, MacMahon H, et al. Fleischnersociety: glossary of terms for thoracic imaging. Radiology.2008;246:697–722.
21. Mayo JR, Jackson SA, Muller NL. High-resolution CT ofthe chest: radiation dose. AJR Am J Roentgenol. 1993;160:479–481.
22. van der Bruggen-Bogaarts BA, Broerse JJ, Lammers JW,et al. Radiation exposure in standard and high-resolutionchest CT scans. Chest. 1995;107:113–115.
23. Jung KJ, Lee KS, Kim SY, et al. Low-dose, volumetric helicalCT: image quality, radiation dose, and usefulness forevaluation of bronchiectasis. Invest Radiol. 2000;35:557–563.
24. Yi CA, Lee KS, Kim TS, et al. Multidetector CT of bronchi-ectasis: effect of radiation dose on image quality. AJR Am JRoentgenol. 2003;181:501–505.
25. Zwirewich CV, Mayo JR, Muller NL. Low-dose high-resolution CT of lung parenchyma. Radiology. 1991;180:413–417.
26. Leswick DA, Webster ST, Wilcox BA, et al. Radiation cost ofhelical high-resolution chest CT. AJR Am J Roentgenol. 2005;184:742–745.
27. Afeltra A, Zennaro D, Garzia P, et al. Prevalence of intersti-tial lung involvement in patients with connective tissuediseases assessed with high-resolution computed tomography.Scand J Rheumatol. 2006;35:388–394.
28. Gochuico BR, Avila NA, Chow CK, et al. Progressive pre-clinical interstitial lung disease in rheumatoid arthritis. ArchIntern Med. 2008;168:159–166.
29. Orens JB, Kazerooni EA, Martinez FJ, et al. The sensitivityof high-resolution CT in detecting idiopathic pulmonaryfibrosis proved by open lung biopsy. A prospective study.Chest. 1995;108:109–115.
30. Sundaram B, Gross BH, Oh E, et al. Reader accuracy andconfidence in diagnosing diffuse lung disease on high-resolu-tion computed tomography of the lungs: impact of samplingfrequency. Acta Radiol. 2008;49:870–875.
31. Hubbard R, Venn A, Lewis S, et al. Lung cancer and crypto-genic fibrosing alveolitis. A population-based cohort study.Am J Respir Crit Care Med. 2000;161:5–8.
32. Daniels CE, Jett JR. Does interstitial lung disease predisposeto lung cancer? Curr Opin Pulm Med. 2005;11:431–437.
33. Lee HJ, Im JG, Ahn JM, et al. Lung cancer in patients withidiopathic pulmonary fibrosis: CT findings. J Comput AssistTomogr. 1996;20:979–982.
34. Kishi K, Homma S, Kurosaki A, et al. High-resolutioncomputed tomography findings of lung cancer associated withidiopathic pulmonary fibrosis. J Comput Assist Tomogr. 2006;30:95–99.
35. Demedts M, Costabel U. Ats/Ers International multidisci-plinary consensus classification of the idiopathic interstitialpneumonias. Eur Respir J. 2002;19:794–796.
36. Kazerooni EA, Martinez FJ, Flint A, et al. Thin-sectionCT obtained at 10-mm increments versus limited three-level
J Thorac Imaging � Volume 25, Number 2, May 2010 Multidetector HRCT of Lungs
r 2010 Lippincott Williams & Wilkins www.thoracicimaging.com | 139
thin-section CT for idiopathic pulmonary fibrosis: correlationwith pathologic scoring. AJR Am J Roentgenol. 1997;169:977–983.
37. Hunninghake GW, Lynch DA, Galvin JR, et al. Radiologicfindings are strongly associated with a pathologic diagnosis ofusual interstitial pneumonia. Chest. 2003;124:1215–1223.
38. Raghu G, Mageto YN, Lockhart D, et al. The accuracy of theclinical diagnosis of new-onset idiopathic pulmonary fibrosisand other interstitial lung disease: a prospective study. Chest.1999;116:1168–1174.
39. Leung AN, Miller RR, Muller NL. Parenchymal opacifica-tion in chronic infiltrative lung diseases: CT-pathologiccorrelation. Radiology. 1993;188:209–214.
40. Remy-Jardin M, Giraud F, Remy J, et al. Importance ofground-glass attenuation in chronic diffuse infiltrativelung disease: pathologic-CT correlation. Radiology. 1993;189:693–698.
41. Sundaram B, Gross BH, Martinez FJ, et al. Accuracy of high-resolution CT in the diagnosis of diffuse lung disease: effectof predominance and distribution of findings. AJR Am JRoentgenol. 2008;191:1032–1039.
42. Steen VD, Owens GR, Fino GJ, et al. Pulmonary involve-ment in systemic sclerosis (Scleroderma). Arthritis Rheum.1985;28:759–767.
43. Bouros D, Wells AU, Nicholson AG, et al. Histopathologicsubsets of fibrosing alveolitis in patients with systemicsclerosis and their relationship to outcome. Am J Respir CritCare Med. 2002;165:1581–1586.
44. Strimlan CV, Rosenow EC III, Divertie MB, et al. Pulmonarymanifestations of Sjogren’s syndrome. Chest. 1976;70:354–361.
45. Wright JL, Cagle P, Churg A, et al. Diseases of the smallairways. Am Rev Respir Dis. 1992;146:240–262.
46. Parambil JG, Myers JL, Lindell RM, et al. Interstitial lungdisease in primary Sjogren syndrome. Chest. 2006;130:1489–1495.
47. Leung AN, Brauner MW, Caillat-Vigneron N, et al. Sarco-idosis activity: correlation of HRCT findings with those of67ga scanning, bronchoalveolar lavage, and serum angioten-sin-converting enzyme assay. J Comput Assist Tomogr.1998;22:229–234.
48. Davies CW, Tasker AD, Padley SP, et al. Air trapping insarcoidosis on computed tomography: correlation with lungfunction. Clin Radiol. 2000;55:217–221.
49. Lynch DA, Webb WR, Gamsu G, et al. Computed tomo-graphy in pulmonary sarcoidosis. J Comput Assist Tomogr.1989;13:405–410.
50. Akira M, Kozuka T, Inoue Y, et al. Long-term follow-up CTscan evaluation in patients with pulmonary sarcoidosis.Chest. 2005;127:185–191.
51. Ryu JHSwensen SJ. Cystic and cavitary lung diseases: focaland diffuse. Mayo Clin Proc. 2003;78:744–752.
52. Boiselle PM, Crans CA Jr, Kaplan MA. The changing faceof pneumocystis carinii pneumonia in aids patients. AJR AmJ Roentgenol. 1999;172:1301–1309.
53. Ouellette H. The signet ring sign. Radiology. 1999;212:67–68.54. McGuinness G, Naidich DP. CT of airways disease and
bronchiectasis. Radiol Clin North Am. 2002;40:1–19.55. Kalil ME, Fernandes AL, Curzel AC, et al. Allergic broncho-
pulmonary aspergillosis presenting a glove-finger shadow inradiographic images. J Bras Pneumol. 2006;32:472–475.
56. Helbich TH, Heinz-Peer G, Eichler I, et al. Cystic fibrosis: CTassessment of lung involvement in children and adults.Radiology. 1999;213:537–544.
57. Katz I, Levine M, Herman P. Tracheobronchiomegaly. TheMounier-Kuhn syndrome. Am J Roentgenol Radium TherNucl Med. 1962;88:1084–1094.
58. Ryu JH, Myers JL, Swensen SJ. Bronchiolar disorders. Am JRespir Crit Care Med. 2003;168:1277–1292.
59. Engeler CE, Tashjian JH, Engeler CM, et al. Volumetric high-resolution CT in the diagnosis of interstitial lung disease andbronchiectasis: diagnostic accuracy and radiation dose. AJRAm J Roentgenol. 1994;163:31–35.
60. Lucidarme O, Grenier P, Coche E, et al. Bronchiectasis:comparative assessment with thin-section ct and helical CT.Radiology. 1996;200:673–679.
61. Dodd JD, Souza CA, Muller NL. Conventional high-resolution CT versus helical high-resolution Mdct in thedetection of bronchiectasis. AJR Am J Roentgenol. 2006;187:414–420.
62. Brasileiro FC, Vargas FS, Kavakama JI, et al. High-resolution CT scan in the evaluation of exercise-inducedinterstitial pulmonary edema in cardiac patients. Chest. 1997;111:1577–1582.
63. Flaherty KR, Kazerooni EA, Curtis JL, et al. Short-term andlong-term outcomes after bilateral lung volume reductionsurgery: prediction by quantitative CT. Chest. 2001;119:1337–1346.
64. Gelb AF, McKenna RJ Jr, Brenner M, et al. Lung function 4years after lung volume reduction surgery for emphysema.Chest. 1999;116:1608–1615.
65. Geddes D, Davies M, Koyama H, et al. Effect of lung-volume-reduction surgery in patients with severe emphysema.N Engl J Med. 2000;343:239–245.
66. National Emphysema Treatment Trial Research Group.Patients at high risk of death after lung-volume-reductionsurgery. N Engl J Med. 2001;345:1075–1083.
67. Fishman A, Martinez F, Naunheim K, et al. A randomizedtrial comparing lung-volume-reduction surgery with medicaltherapy for severe emphysema. N Engl J Med. 2003;348:2059–2073.
68. Pakhale SS, Gutierrez C. Lung-volume—reduction surgery.N Engl J Med. 2003;349:999–1000; author reply 1999–1000.
69. Ramsey SD, Berry K, Etzioni R, et al. Cost effectiveness oflung-volume-reduction surgery for patients with severeemphysema. N Engl J Med. 2003;348:2092–2102.
70. Algranti E, Mendonca EM, DeCapitani EM, et al. Non-malignant asbestos-related diseases in Brazilian asbestos-cement workers. Am J Ind Med. 2001;40:240–254.
71. McKenna RJ Jr, Brenner M, Fischel RJ, et al. Patientselection criteria for lung volume reduction surgery. J ThoracCardiovasc Surg. 1997;114:957–964; discussion 964–957.
72. Dowson LJ, Guest PJ, Stockley RA. Longitudinal changes inphysiological, radiological, and health status measurements inalpha(1)-antitrypsin deficiency and factors associated withdecline. Am J Respir Crit Care Med. 2001;164:1805–1809.
73. D’Andrilli A, Vismara L, Rolla M, et al. Computed tomogra-phy with volume rendering for the evaluation of parenchymalhyperinflation after bronchoscopic lung volume reduction.Eur J Cardiothorac Surg. 2009;35:403–407.
74. Dirksen A, Piitulainen E, Parr DG, et al. Exploring the role ofCT densitometry: a randomised study of augmentationtherapy in alpha-1 antitrypsin deficiency. Eur Respir J. 2009;33:1345–1353.
75. Muller NL, Staples CA, Miller RR, et al. ‘‘Density mask’’. Anobjective method to quantitate emphysema using computedtomography. Chest. 1988;94:782–787.
76. Boedeker KL, McNitt-Gray MF, Rogers SR, et al. Emphy-sema: effect of reconstruction algorithm on CT imagingmeasures. Radiology. 2004;232:295–301.
77. Park YS, Seo JB, Kim N, et al. Texture-based quantificationof pulmonary emphysema on high-resolution computedtomography: comparison with density-based quantificationand correlation with pulmonary function test. Invest Radiol.2008;43:395–402.
78. Zompatori M, Battaglia M, Rimondi MR, et al. Quantitativeassessment of pulmonary emphysema with computerizedtomography. Comparison of the visual score and high resolu-tion computerized tomography, expiratory density mask withspiral computerized tomography and respiratory functiontests. Radiol Med. 1997;93:374–381.
79. Hersh CP, Washko GR, Jacobson FL, et al. Interobservervariability in the determination of upper lobe-predominantemphysema. Chest. 2007;131:424–431.
Sundaram et al J Thorac Imaging � Volume 25, Number 2, May 2010
140 | www.thoracicimaging.com r 2010 Lippincott Williams & Wilkins
80. Stavngaard T, Shaker SB, Bach KS, et al. Quantitativeassessment of regional emphysema distribution in patientswith chronic obstructive pulmonary disease (COPD). ActaRadiol. 2006;47:914–921.
81. Hunsaker AR, Ingenito EP, Reilly JJ, et al. Lung volumereduction surgery for emphysema: correlation of CT and V/Qimaging with physiologic mechanisms of improvement in lungfunction. Radiology. 2002;222:491–498.
82. Gierada DS, Yusen RD, Pilgram TK, et al. Repeatability ofquantitative CT indexes of emphysema in patients evaluatedfor lung volume reduction surgery. Radiology. 2001;220:448–454.
83. Baldi S, Miniati M, Bellina CR, et al. Relationship betweenextent of pulmonary emphysema by high-resolution compu-ted tomography and lung elastic recoil in patients withchronic obstructive pulmonary disease. Am J Respir Crit CareMed. 2001;164:585–589.
84. Bayramoglu S, Cimilli T, Aksoy S, et al. The role of HRCTversus CXR in children with recurrent pulmonary infections.Clin Imaging. 2005;29:317–324.
85. Hui JY, Hon TY, Yang MK, et al. High-resolution computedtomography is useful for early diagnosis of severe acuterespiratory syndrome-associated coronavirus pneumonia inpatients with normal chest radiographs. J Comput AssistTomogr. 2004;28:1–9.
86. D’Arienzo P, Giampalma E, Lavecchia MA, et al. Role ofHRCT in the identification of atypical pulmonary myco-bacteriosis. Radiol Med. 2002;103:158–170.
87. Hidalgo A, Falco V, Mauleon S, et al. Accuracy of high-resolution CT in distinguishing between pneumocystis cariniipneumonia and non- pneumocystis carinii pneumonia in aidspatients. Eur Radiol. 2003;13:1179–1184.
88. Syrjala H, Broas M, Suramo I, et al. High-resolution com-puted tomography for the diagnosis of community-acquiredpneumonia. Clin Infect Dis. 1998;27:358–363.
89. Gasparetto EL, Ono SE, Escuissato D, et al. Cytomegaloviruspneumonia after bone marrow transplantation: high resolu-tion CT findings. Br J Radiol. 2004;77:724–727.
90. Althoff Souza C, Muller NL, Marchiori E, et al. Pulmonaryinvasive aspergillosis and candidiasis in immunocompromisedpatients: a comparative study of the high-resolution CTfindings. J Thorac Imaging. 2006;21:184–189.
91. Franquet T. High-resolution computed tomography (HRCT)of lung infections in non-aids immunocompromised patients.Eur Radiol. 2006;16:707–718.
92. Gruden JF, Huang L, Turner J, et al. High-resolution CT inthe evaluation of clinically suspected pneumocystis cariniipneumonia in aids patients with normal, equivocal, or non-specific radiographic findings. AJR Am J Roentgenol. 1997;169:967–975.
93. Kuroishi S, Nakamura Y, Hayakawa H, et al. Mycobacteri-um avium complex disease: prognostic implication of high-resolution computed tomography findings. Eur Respir J.2008;32:147–152.
94. Olivier KN, Weber DJ, Lee JH, et al. Nontuberculousmycobacteria. II: nested-cohort study of impact on cysticfibrosis lung disease. Am J Respir Crit Care Med. 2003;167:835–840.
95. Vassallo R, Jensen EA, Colby TV, et al. The overlap betweenrespiratory bronchiolitis and desquamative interstitial pneu-monia in pulmonary Langerhans cell histiocytosis: high-resolution CT, histologic, and functional correlations. Chest.2003;124:1199–1205.
96. Clark KD, Wardrobe-Wong N, Elliott JJ, et al. Patterns oflung disease in a ‘‘Normal’’ smoking population: are emphy-sema and airflow obstruction found together? Chest. 2001;120:743–747.
97. Vierikko T, Jarvenpaa R, Uitti J, et al. The effects ofsecondhand smoke exposure on HRCT findings amongasbestos-exposed workers. Respir Med. 2008;102:658–664.
98. Betsuyaku T, Yoshioka A, Nishimura M, et al. Pulmonaryfunction is diminished in older asymptomatic smokers andex-smokers with low attenuation areas on high-resolutioncomputed tomography. Respiration. 1996;63:333–338.
99. Verschakelen JA, Scheinbaum K, Bogaert J, et al. ExpiratoryCT in cigarette smokers: correlation between areas of decrea-sed lung attenuation, pulmonary function tests and smokinghistory. Eur Radiol. 1998;8:1391–1399.
100. Deveci F, Murat A, Turgut T, et al. Airway wall thickness inpatients with COPD and healthy current smokers and healthynon-smokers: assessment with high resolution computedtomographic scanning. Respiration. 2004;71:602–610.
101. Soejima K, Yamaguchi K, Kohda E, et al. Longitudinalfollow-up study of smoking-induced lung density changesby high-resolution computed tomography. Am J Respir CritCare Med. 2000;161:1264–1273.
102. Remy-Jardin M, Remy J, Farre I, et al. Computed tomo-graphic evaluation of silicosis and coal workers’ pneumoco-niosis. Radiol Clin North Am. 1992;30:1155–1176.
J Thorac Imaging � Volume 25, Number 2, May 2010 Multidetector HRCT of Lungs
r 2010 Lippincott Williams & Wilkins www.thoracicimaging.com | 141