hospital practice
TRANSCRIPT
THE LANCBT I AUGUST 8, 1970
Hospital Practice
A STUDY OF CONSULTANTS N. F. CoGHILL F. M. ULYATT
R. W. RBvANS K. W. ULYATT
W.,t MidtlIu4Jt Hospital,lsUworth; Buropeon Association of Mancw""",t Trainm, eMtr." Bruss"', and Guy's Hospital
M«Iical School, London; Mayday Hospital, Croydon
THE speed of innovation today, alike in technology, economics, and social attitude, has brought every institution under stress. The Health Service is familiar with the effects such stress produces, but lacks insight into its causes.
At one very large factory several hundred araduare manaaen and their foremen joined in a largely selforpniaed study of their feelinp about four major topics 1: the rewards offered by the job; the information they had to do it; their view of themselves as persons; and their view of themselves as leaders. This survey auaeated that there is an institutional level of communication, common throushout the workiDI orpniaation, and hence better in lOme orpniaatiom than in others eopged in the same technology; and that there is around every individual in the orpniaation he serves a local or penonaJ network, of which the transparency or opacity is determined by that individual himself. In this C8Ie it was shown that, although the avenae quality of the several hundred local or penonal communication networks was significantly above the national avenae for individuals, the average quality of the overall information system was significantly below that of all other orpniaationa studied.
Another study' ahowed that the attitudes of factory workers to JIWlIIerB, and lIlII1qement problema, were c:Ioeely related to their views of the manqers as people and to the factory as a place to work in.
Hospitals are not industtial factories, nor are doctors and nurses the exact equivalents of managers and supervison in charge of squads of process and maintenance workers. But hospitals have their problems of communicating what others need to know, and in this respect they differ markedly among themselves. Indeed, a previous study • sugested that the variation between the averages of the hospitals perceived as the best and wont was several times as great as the variation between the individuals within them having most and least difficulty in communicating. Here the individuals sampled were ward sisters; it was their perceptions of the ease-of-contact with their superion and with their subordinates that was under review.
We do not know what determines the aenerallevel of transparency or opacity in a hospital communication system, although research in industry, as well as historical tradition, suggests that the influence of the key persons at the top is paramount. Where is the power in the hospital? What is it used for? Over two thousand yean ago, the writer of Ecclesiasticus (X, 2) observed: .. As the judge of the people is, so are his officers j and what manner of man the ruler of the city is, so are aU they that inhabit therein ". There may well be no judges and no rulen in a modern hospital, but there are individuals with power, and amODI these are the consultants. To what extent are we able to examine the nature and effects of consultant power, and, in particular, to trace its effects upon the quality of communications between those dependent on the
consultant--end between those on whom the consultant, in his turn, no less depends ?
The power exercised by consultants is such that only with their consent and active participation are we able to examine the effects of their iDfiuence on hospital communication systems, and so on the adaptation of the service to changes in general. A practical exercise designed to study the attitudes of consultants to their workina environment was included in the proaramme at the conference on management in medicine organised by the Royal College of Physicians in September, 1968.
A pilot study for this exercise was held among the consultants of a single hospital.· The results of this suggested that the consultants who thought t;Jle h0spital could be improved were those who were prepared to examine their own relations with it; those who were complacent about the hospital were complacent about themselves.
THB BXI.CISB The exercise was based on a twenty-item questionary
(see appendix) constructed after the experience of the pilot study.· The docton taldng part in this se1fexamination study were asked to express opinions that not only reflected their perception of their own reaponsibilities for the effectiveness of the hospital organisation, but that could be commented upon by others who knew them well. Consider, for example, item 7 and suppose that, say, fifty consultants, in conditions of anonymity, confidentiality, and independence were asked to make their responses to it-strong agreement (SA), tendency to agreement (A), uncertain (U), tendency to disagreement (D), or strong disagreement (SD). Suppose the series of responses ran 9 SA, 21 A. 8 U, 10 D, 2 SD, showing a trend towards qreeing with the opinion. But then, supposing that fifty persons who know consultants well by haviDI to work with them, such as matrons, sisters, hospital secretaries, officers of regional boards, registran, and so forth, also completed their entries apinst the same statement as if they were each a consultant whom they mew well, what series of results would one expect? If the statement is meaningful, if the non-consultants really understand the consultants, and if all in each sample give truthful responses, the second series should not be significantly different from the tint. In the event, the views expressed at the conference by the 63 consultants as themselves and those expressed by 100 colleques as if they were consultants were strongly correlated.
Of the 20 statements making up the exercise instrument, 10 were concerned with the consultants' view of themselves (P in appendix), and 10 were concerned with their views of conditions at their hospitals (H). Respondents identified themselves as doctor/consultant/administrator/nune/other. The 163 sets of 20 reaponses each were marked 10 as to suaeat confidence in communication (or openness of contact) as positive, remoteness or caution as neptive. Given a scale of markina on these lines, with opinions stroDlly expressed scoring double marb, we can calculate, for each class of respondent, the .venae score, positive or negative, for each statement in each of the 2 blocb of 10 statements. There were seven classes of reaponcients-clinical COl1Iultants, COl1Iultant admini ... traton, clinical docton, doctor administrators. nonmedical administraton, nurses, and other informed observers of the consultants' task, such u research
306
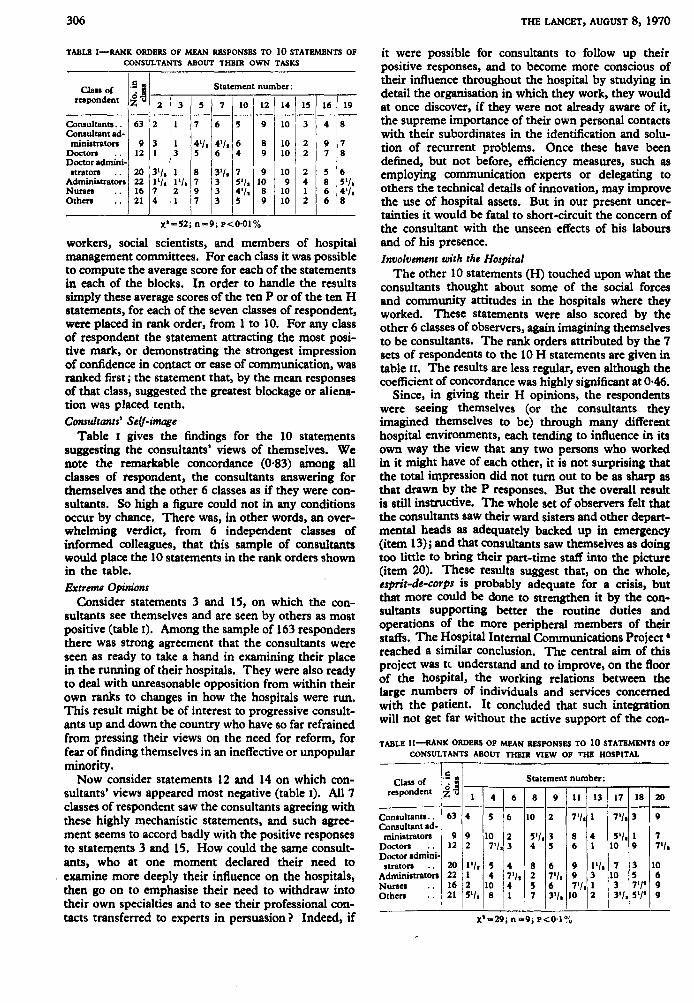
TABLE I-RANK ORDERS OF MEAN RllSPONSBS TO 10 STATEMENTS OF CONSULTANTS ABOUT THEIR OWN TASKS
Clan of '~j Statement number: respondent ~u 2 3 5 7 10 12 14 15 16 19
- - - - - - - - - -Consultants .. 63 2 1 7 6 5 9 10 3 4 8 Consultant ad-ministraton 9 3 1 4'1. 4'1. 6 8 10 2 9 7
Docton 12 1 3 5 6 4 9 10 2 7 8 Doctor adminl-straton 20 3'1. 1 8 3'1. 7 9 10 2 5 6
Administraton 22 1'1. 1'1. 7 3 5'/. 10 9 4 8 5'1. Nunes .. 16 7 2 9 3 4'/. 8 10 1 6 4'/. Othen .. 21 4 1 7 3 5 9 10 2 6 8
x' -52; n =9; p<O'OI %
workers, social scientists, and members of hospital management committees. For each class it was possible to compute the average score for each of the statements in each of the blocks. In order to handle the results simply these average scores of the ten P or of the ten H statements, for each of the seven classes of respondent, were placed in rank order, from 1 to 10. For any class of respondent the statement attracting the most positive mark, or demonstrating the strongest impression of confidence in contact or ease of communication, was ranked first; the statement that, by the mean responses of that class, suggested the greatest blockage or alienation was placed tenth. Consultants' Self-image
Table I gives the findings for the 10 statements suggesting the consultants' views of themselves. We note the remarkable concordance (0'83) among all classes of respondent, the consultants answering for themselves and the other 6 classes as if they were consultants. So high a figure could not in any conditions occur by chance. There was, in other words, an overwhelming verdict, from 6 independent classes of informed colleagues, that this sample of consultants would place the 10 statements in the rank orders shown in the table. Extreme Opinions
Consider statements 3 and 15, on which the consultants see themselves and are seen by others as most positive (table I). Among the sample of 163 responders there was strong agreement that the consultants were seen as ready to take a hand in examining their place in the running of their hospitals. They were also ready to deal with unreasonable opposition from within their own ranks to changes in how the hospitals were run. This result might be of interest to progressive consultants up and down the country who have so far refrained from pressing their views on the need for reform, for fear of finding themselves in an ineffective or unpopular minority.
Now consider statements 12 and 14 on which consultants' views appeared most negative (table I). All 7 classes of respondent saw the consultants agreeing with these highly mechanistic statements, and such agreement seems to accord badly with the positive responses to statements 3 and 15. How could the same consultants, who at one moment declared their need to examine more deeply their influence on the hospitals, then go on to emphasise their need to withdraw into their own specialties and to see their professional contacts transferred to experts in persuasion? Indeed, if
THE LANCET, AUGUST 8, 1970
it were possible for consultants to follow up their positive responses, and to become more conscious of their influence throughout the hospital by studying in detail the organisation in which they work, they would at once discover, if they were not already aware of it, the supreme importance of their own personal contacts with their subordinates in the identification and solution of recurrent problems. Once these have been defined, but not before, efficiency measures, such as employing communication experts or delegating to others the technical details of innovation, may improve the use of hospital assets. But in our present uncertainties it would be fatal to short-circuit the concern of the consultant with the unseen effects of his labours and of his presence. Involvement with the Hospital
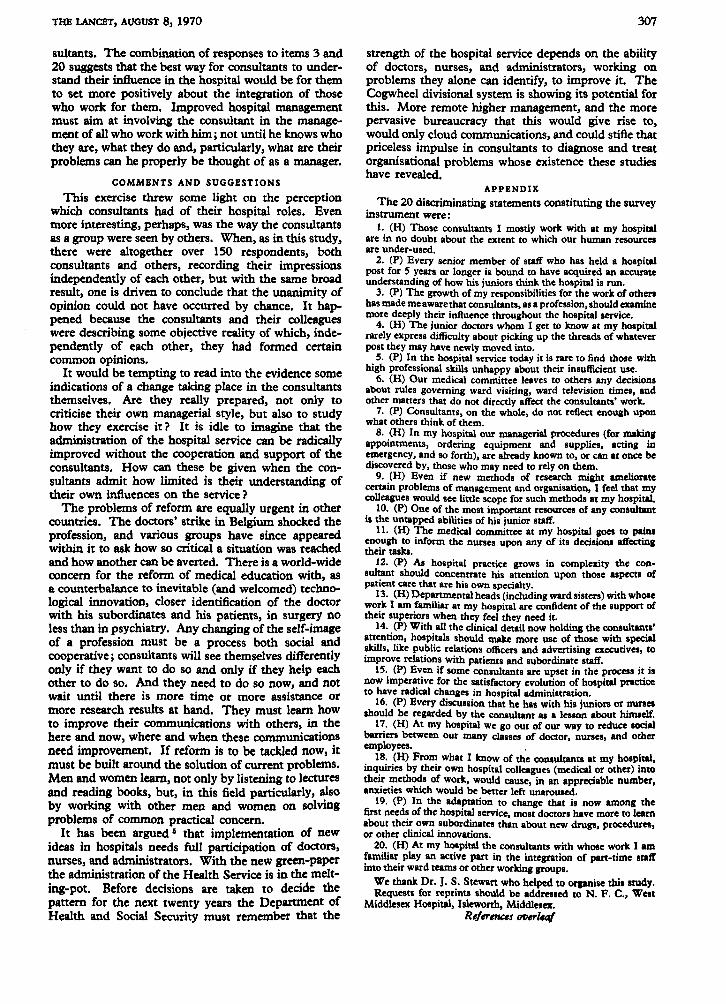
The other 10 statements (H) touched upon what the consultants thought about some of the social forces and community attitudes in the hospitals where they worked. These statements were also scored by the other 6 classes of observers, again imagining themselves to be consultants. The rank orders attributed by the 7 sets of respondents to the 10 H statements are given in table II. The results are less regular, even although the coefficient of concordance was highly significant at 0·46.
Since, in giving their H opinions, the respondents were seeing themselves (or the consultants they imagined themselves to be) through many different hospital environments, each tending to influence in its own way the view that any two persons who worked in it might have of each other, it is not surprising that the total impression did not tum out to be as sharp as that drawn by the P responses. But the overall result is still instructive. The whole set of observers felt that the consultants saw their ward sisters and other departmental heads as adequately backed up in emergency (item 13); and that consultants saw themselves as doing too little to bring their part-time staff into the picture (item 20). These results suggest that, on the whole, esprit-de-corps is probably adequate for a crisis, but that more could be done to strengthen it by the consultants supporting better the routine duties and operations of the more peripheral members of their staffs. The Hospital Internal Communications Project • reached a similar conclusion. The central aim of this project was t<. understand and to improve, on the floor of the hospital, the working relations between the large numbers of individuals and services concerned with the patient. It concluded that such integration will not get far without the active support of the con-
TABLE II-RANK ORDERS OF MEAN RllSPONSBS TO 10 STATEMENTS OF CONSULTANTS ABOUT THEIR VIEW OF THE HOSPITAL
Class of .5 to Statement number: ol respondent zu 1 4 6 8 9 11 13 17 I~~ Consultant •.. 63 4 5 6 10 2 7'/. 1 7'1. 3 9
Consultant ad-ministraton 9 9 10 2 5'/.3 8 4 5'/. 1 7
Docton 12 2 7'/.3 4 5 6 1 10 9 7'1. Doctor admini-straton ., 20 1'/. 5 4 8 6 9 1'1. 7 3 10
Administrators 22 1 4 7'/. 2 7'/. 9 3 10 5 6 Nurses .. 16 2 10 4 5 6 7'/. 1 3 7'1' 9 Others .. 21 5'/. 8 1 7 3'/. 10 2 3'1. 5'1' 9
X'-29; n-9; P<O'I%
THE LANCET, AUGUST 8,1970
sultants. The combination of responses to items 3 and 20 suggests that the best way for consultants to understand their influence in the hospital would be for them to set more positively about the integration of those who work for them. Improved hospital management must aim at involving the consultant in the management of all who work with him; not until he knows who they are, what they do and, particularly, what are their problems can he properly be thought of as a manager.
COMMENTS AND SUGGESTIONS
This exercise threw some light on the perception which consultants had of their hospital roles. Even more interesting, perhaps, was the way the consultants as a group were seen by others. When, as in this study, there were altogether over 150 respondents, both consultants and others, recording their impressions independently of each other, but with the same broad result, one is driven to conclude that the unanimity of opinion could not have occurred by chance. It happened because the consultants and their colleagues were describing some objective reality of which, independently of each other, they had formed certain common opinions.
It would be tempting to read into the evidence some indications of a change taking place in the consultants themselves. Are they really prepared, not only to criticise their own managerial style, but also to study how they exercise it? It is idle to imagine that the administration of the hospital service can be radically improved without the cooperation and support of the consultants. How can these be given when the consultants admit how limited is their understanding of their own influences on the service?
The problems of reform are equally urgent in other countries. The doctors' strike in Belgium shocked the profession, and various groups have since appeared within it to ask how so critical a situation was reached and how another can be averted. There is a world-wide concern for the reform of medical education with, as a counterbalance to inevitable (and welcomed) technological innovation, closer identification of the doctor with his subordinates and his patients, in surgery no less than in psychiatry. Any changing of the self-image of a profession must be a process both social and cooperative; consultants will see themselves differently only if they want to do so and only if they help each other to do so. And they need to do so now, and not wait until there is more time or more assistance or more research results at hand. They must learn how to improve their communications with others, in the here and now, where and when these communications need improvement. If reform is to be tackled now, it must be built around the solution of current problems. Men and women learn, not only by listening to lectures and reading books, but, in this field particularly, also by working with other men and women on solving problems of common practical concern.
It has been argued 6 that implementation of new ideas in hospitals needs full participation of doctors, nurses, and administrators. With the new green-paper the administration of the Health Service is in the melting-pot. Before decisions are taken to decide the pattern for the next twenty years the Department of Health and Social Security must remember that the
307
strength of the hospital service depends on the ability of doctors, nurses, and administrators, working on problems they alone can identify, to improve it. The Cogwheel divisional system is showing its potential for this. More remote higher management, and the more pervasive bureaucracy that this would give rise to, would only cloud communications, and could stifle that priceless impulse in consultants to diagnose and treat organisational problems whose existence these studies have revealed.
APPENDIX
The 20 discriminating statements constituting the survey instrument were:
1. (H) Those consultants I mostly work with at my hospital are in no doubt about the extent to which Out human resoutces are under-used.
2. (P) Every senior member of staff who has held a hospital post for 5 years or longer is bound to have acquired an accurate understanding of how his juniors think the h08pital is run.
3. (P) The growth of my responsibilities for the work of others has made me aware that consultants, as a profession, should examine mote deeply their influence throughout the hospital service.
4. (H) The junior doctors whom I get to know at my hospital rarely express difficulty about picking up the threads of whatever post they may have newly moved into.
5. (P) In the hospital service today it is rare to find those with high professional skills unhappy about their insufficient use.
6. (H) Our medical committee leaves to others any decisions about rules governing ward visiting, ward television times, and other matters that do not directly affect the consultants' work.
7. (P) Consultants, on the whole, do not reflect enough upon what others think of them.
8. (H) In my hospital out managerial procedutes (fot makin; appointments, ordering equipment and supplies, acting in emergency, and so forth), are already known to, or can at once be discovered by, those who may need to rely on them.
9. (H) Even if new methods of research might ameliorate certain problems of management and organisation, I feel that my colleagues would see little scope for such methods at my hospital.
10. (P) One of the most important resources of any consultant is the untapped abilities of his junior staff.
11. (H) The medical committee at my hospital goes to pains enough to inform the nurses upon any of its decisions affecting their raska.
12. (P) As hospital practice grows in complexity the consultant should concentrate his attention upon those aspects of patient care that are his own specialty.
13. (H) Departmental heads (including ward sisters) with whose work I am familiar at my hospital are confident of the suppon of their superiors when they feel they need it.
14. (P) With all the clinical detail now holding the consultant.' attention, hospitals should make more use of those with special skills. like public relations officers and advertising executives, to improve relations with patients and subordinate staff.
15. (P) Even if some consultants are upset in the process it is now imperative for the satisfactory evolution of hospital practice to have radical changes in hospital administration.
16. (P) Every discussion that he has with his juniors or nurses should be regarded by the consultant as a lesson about himself.
17. (H) At my hospital we go out of out way to reduce social barriers between Out many classes of doctor, nurses, and other employees. .
18. (H) From what I know of the consultants at my hospital, inquiries by their own hospital colleagues (medical or other) into their methods of work, would cause, in an appreciable number, anxieties which would be better left unaroused.
19. (P) In the adaptation to change that is now among the first needs of the hospital service, most doctors have more to learn about their own subordinates than about new drugs, procedutes, ot other clinical innovations.
20. (H) At my hospital the consultants with whose work I am familiar play an active part in the integration of part-time staff into their ward teams or other working groups.
We thank Dr. J. S. Stewan who helped to organise this ltudy. Requests for reprints should be addressed to N. F. C., West
Middlesex Hospital, bleworth, Middlesex. Re/erenus OfJerlUl/