hospice enrollment and hospitalization of dying nursing home patients
TRANSCRIPT

Hospice Enrollment and Hospitalization ofDying Nursing Home Patients
Susan C. Miller, PhD, Pedro Gozalo, PhD, Vincent Mor, PhD
PURPOSE: This study’s purpose was to evaluate whetherMedicare hospice care provided in nursing homes is associatedwith lower hospitalization rates.SUBJECTS AND METHODS: This retrospective cohort studyincluded nursing home residents in five states who enrolled inhospice between 1992 and 1996 (n 5 9202), and who died be-fore 1998. For each hospice patient, 3 nonhospice residents (2 in106 instances) were chosen (n 5 27,500). Medicare claims iden-tified hospice enrollment and acute care hospitalizations.RESULTS: Twenty-four percent of hospice and 44% of non-hospice residents were hospitalized in the last 30 days of life.Adjusting for confounders, hospice patients were less likely thannonhospice residents to be hospitalized (odds ratio 0.43; 95%confidence interval [CI]: 0.39 to 0.46). Considering all of non-hospice residents who died (n 5 226,469), those in facilities
with no hospice had a 47% hospitalization rate, whereas rateswere 41% in facilities with low hospice use and 39% in facilitieswith moderate hospice use (5%1 of patients in hospice). Hos-pitalization was less likely for nonhospice residents in facilitieswith low hospice use (odds ratio 0.82; 95% CI: 0.80 to 0.84) andmoderate hospice use (odds ratio 0.71; 95% CI: 0.69 to 0.74),compared with those in facilities with no hospice.CONCLUSIONS: When integrated into the nursing home careprocesses, hospice care is associated with less hospitalization forMedicare hospice patients. Additionally, possibly through dif-fusion of palliative care philosophy and practices, nonhospiceresidents who died in nursing homes having a hospice presencehad lower rates of end-of-life hospitalizations. Am J Med.2001;111:38 – 44. q2001 by Excerpta Medica, Inc.
Nursing homes are the site of death for more than 1in 5 older persons (1). Because legislation has al-lowed for the provision of Medicare hospice care in
nursing homes (Omnibus Budget Reconciliation Act of1985), palliative services in nursing homes can be providedby contracted hospice providers (2,3). A recent study ofnursing home Medicare beneficiaries in five states estimatedthat 24% of all Medicare hospice patients resided in nursinghomes (4). Nonetheless, although research supports the no-tion that pain and symptom management in the nursinghome may be less than optimal (5–7), we know little aboutthe care provided to dying nursing home patients and howthe presence of hospice may influence this care. Recent stud-
ies, however, suggest that hospice enrollment is associatedwith higher quality symptom assessment and management(8,9) and with prevention of hospitalizations (per families’perceptions; 8).
Hospitalization of nursing home patients is common(10 –16). Irrespective of the costs of these hospitaliza-tions, they include hazards that compromise the qualityof life (17) and are often inappropriate (18). Because hos-pice care philosophy discourages aggressive nonpalliativemedical care, the influence of hospice presence in thenursing home on hospitalization rates of dying nursinghome residents may substantially influence Medicare in-patient expenditures and the quality of life for dyingnursing home residents.
The goal of hospice is to ameliorate symptoms, to re-duce unneeded and unwanted medical intervention, andto attend to the psychosocial needs of patients and fami-lies. Early hospice studies focused on home and inpa-tient-based models of hospice care. This past researchfound home-based hospice to be associated with reduc-tions in hospitalization (19 –22). The purpose of ourstudy was to determine whether this benefit generalizedto the nursing home. We hypothesized that hospice careprovided in the nursing home would be associated withlower rates of acute care hospitalization in the last 30 daysof life.
MATERIAL AND METHODS
Study DataBrown University has assembled the Systematic Assess-ment of Geriatric Drug Use via Epidemiology database
From the Center for Gerontology and Health Care Research (SCM, PG,VM), Department of Community Health, Brown University, Provi-dence, Rhode Island.
Requests for reprints should be addressed to Susan C. Miller, PhD,Center for Gerontology and Health Care Research, Brown University,Box G-H3, Providence, RI 02912 [email protected]
Supported by Contract 100 –97– 0010 to The Urban Institute fromthe Office of Disability, Aging, and Long Term Care Policy in the Officeof the Assistant Secretary for Planning and Evaluation, U.S. Departmentof Health and Human Services. The Center for Gerontology and HealthCare Research subcontracted with The Urban Institute. Supported inpart by Grant 97–385 from the Retirement Research Foundation and bythe Retirement Research Foundation grant, “Decisions About Death inLong-Term Care: Development and Dissemination of Guidelines toEase the Death of a Resident in the Nursing Home,” by GrantAG11624 – 06s1 from the National Institute on Aging, Grant HS10549from the Agency for Healthcare Research and Quality, and by the JohnA. Hartford Foundation Institute for Geriatric Nursing at New YorkUniversity Division of Nursing. The opinions expressed in this manu-script are those of the researchers and do not necessarily reflect those ofthe sponsoring agencies.
Manuscript submitted November 9, 2000, and accepted in revisedform March 27, 2001.
38 q2001 by Excerpta Medica, Inc. 0002-9343/01/$–see front matterAll rights reserved. PII S0002-9343(01)00747-1

(23–24), which links data from nursing facility residentassessments, Health Care Financing Administration(HCFA) claims data, and organizational data on nursinghome providers. All sources are universally available onall residents of all Medicare- and Medicaid-certified nurs-ing homes in the country (96% of all homes). In thisstudy, successful matching of residents across all datasources was 87%.
Nursing homes conduct standardized comprehensiveassessments of residents, and data from these assessmentsmake up the Minimum Data Set (25). The MinimumData Set includes cognitive function, communicationand hearing problems, physical functioning, continence,psychosocial status, diagnoses, health conditions andsymptoms, medications, and numerous other items. Inthe time period studied, standardized resident assess-ments were required upon admission (by 14 days fol-lowing), quarterly, and annually. Reassessments wererequired when a resident was readmitted following hos-pitalization and when significant change occurred, al-though not necessarily upon hospice enrollment (25).
With a data use agreement from the HCFA in place, wehad access to 1992–1996 Minimum Data Set data in thefive states of Kansas, Maine, Mississippi, New York, andSouth Dakota. These states were part of the Case-MixReimbursement and Quality Demonstration project con-ducted by the HCFA between 1989 and 1995, and, assuch, had all Minimum Data Set assessments computer-ized beginning in 1992. To identify hospice enrollment,hospitalization, and death, we linked these MinimumData Set data with 1991 through 1997 HCFA claims dataand with HCFA’s 1997 enrollment file.
Study SampleOur sample consisted of nursing home residents who hada Minimum Data Set assessment record between 1992and 1996 and who died before January 1998. Of these240,194 residents, 13,725 (5.7%) chose hospice at somepoint in time. Residents enrolling in hospice after nursinghome admission and receiving hospice in any of the last30 days of life were included, resulting in 10,425 hospicepatients for study. Of these, 616 (6%) had missing assess-ment data on one or more clinical variables to be used tocontrol for confounding. These patients were excluded,resulting in 9809 hospice patients for study. Comparisonsof hospice patients with and without missing data re-vealed no meaningful differences. Those with missingdata were more likely to have resided in Kansas than werethose with nonmissing data.
For each hospice patient, 3 nonhospice residents (2 of106 instances) with similar lengths of nursing home stay,time intervals from last Minimum Data Set to death, stateof nursing home residence, and 1 of 4 diagnosis groups(cancer with no dementia/Alzheimer’s disease, cancerwith dementia/Alzheimer’s disease, dementia/Alzhei-
mer’s disease without cancer, and diagnoses other thancancer or dementia/Alzheimer’s disease) were chosen.Diagnostic data came from the Minimum Data Set assess-ment and from Medicare inpatient claims 6 months be-fore and during the nursing home episode. Six hundredand seven hospice patients could not be matched to atleast 2 nonhospice residents and were excluded, resultingin 9,202 hospice patients and 27,500 nonhospice patientsfor study.
Hospitalization in the Last 30 Days of LifeBased on date information on Medicare acute care hos-pital claims, we determined whether hospitalization oc-curred in the 30 days before death. Although the hospicebenefit does have a hospice inpatient option, it was infre-quently used (it accounted for only 3% [$77 of $2296] ofall per patient hospice expenditures in the last 30 days oflife).
Independent VariableWe tested the effect of Medicare hospice care on Medi-care acute care hospitalization in the last 30 days of life.Nursing home residents who died were considered to behospice patients when dates on Medicare hospice claimsindicated that hospice began after nursing home admis-sion. Because we adopted an “intent to treat” approach,patients who withdrew from hospice before death werestill considered to be hospice patients. Also, we estimateda conservative hospice effect because we included 5848hospice patients (64%) who did not receive hospice carefor the entire 30-day period, primarily because of shorthospice stays.
Analytic ApproachAnalysis of the dichotomous outcome measure, hospital-ization in the last 30 days of life, was performed usinglogistic regression with a generalized estimating equationin SAS GENMOD procedure (26). The generalized esti-mating equation adjusted for the correlation occurringbecause of patients residing in the same nursing facility.Because we had no evidence to the contrary, we assumedthat patient independent variables were similarly relatedto the outcomes across all facilities. Because we matchednonhospice residents to the hospice patient cohort onseveral variables, conditional logistic regression was themost appropriate analytic approach (27). Given the largesample size in many strata, however, we were unable toachieve convergence using conditional logistic regressionwith the matched variables as strata. Also, we could notuse a generalized estimating equation, and thus adjustedfor within-facility patient correlations, if we used the con-ditional logistic regression modeling required for 3–1 or2–1 matching. Because of our large sample size, we wereable to approximate conditional logistic modeling by in-cluding the matching variables as dummy variables in ourregression model. Additionally, we ran a conditional lo-
Hospice Enrollment and Hospitalization/Miller et al
July 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 111 39
gistic model without a generalized estimating equation inwhich each stratum consisted of each hospice patient andthe matched nonhospice residents. The results of thisanalysis are reported.
The multivariate model adjusted for confounding byincluding sociodemographic and case-mix variables thatwere chosen based on a systematic literature review andprevious related work performed by the authors and theircolleagues (3). These variables include sex, race (white,nonwhite), marital status (married, not married), age, a6-point activities of daily living index, the Cognitive Per-formance Scale (28), and the presence of congestive heartfailure or chronic obstructive pulmonary disease as re-corded on the Minimum Data Set. Scores from the6-point activities of daily living index range from 1 (min-imal oversight) to 6 (highly dependent). Scores on the cog-nitive performance scale range from 0 (intact) to 6 (verysevere impairment).
We included the diagnosis groups in our model asdummy variables. We also included dummy variables forthe states in the model. The multivariate model adjustedfor patient preferences by including variables represent-ing the presence of do not resuscitate and do not hospi-
talize orders, and for the influence of being a short-staynursing home patient, by including a variable represent-ing nursing home stays of ,90 days. Furthermore, themodel adjusted for previous hospital utilization (a reflec-tion of preferences and disease severity) by including acontinuous variable indicating the number of acute carehospital days experienced in the 6 months before hospiceadmission. For nonhospice patients this variable was cal-culated using a 6-month time period ending the samenumber of days before death as was the case for corre-sponding matched cases. (This variable and the do notresuscitate and do not hospitalize variables help to correctfor patient selection bias associated with hospice enroll-ment.) Because approximately 73% (25,549) of the hos-pice and nonhospice cohorts resided in nursing homes inNew York (Table 1), we repeated the analysis excludingNew York residents to ensure that the observed effect wasnot a phenomenon solely of nursing home hospice care inNew York. Last, we calculated predicted probabilities foreight subgroups (i.e., the four diagnosis groups by hos-pice or nonhospice status) by using average variable val-ues for each subgroup in a multivariate model identical tothe one described above.
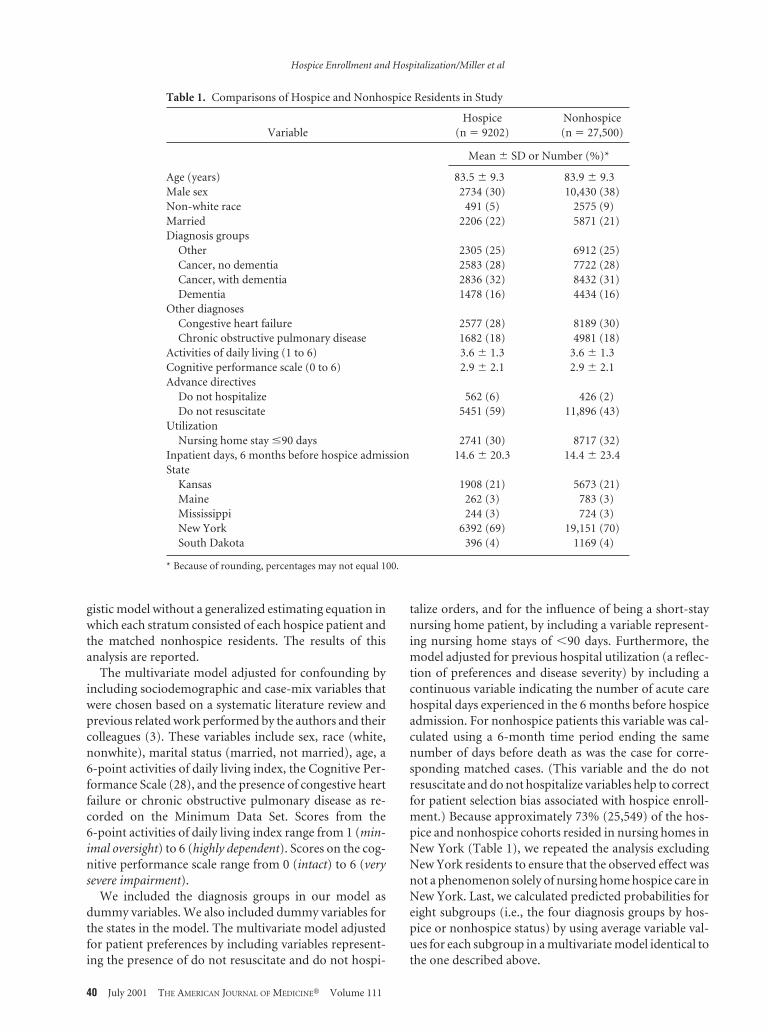
Table 1. Comparisons of Hospice and Nonhospice Residents in Study
VariableHospice
(n 5 9202)Nonhospice(n 5 27,500)
Mean 6 SD or Number (%)*
Age (years) 83.5 6 9.3 83.9 6 9.3Male sex 2734 (30) 10,430 (38)Non-white race 491 (5) 2575 (9)Married 2206 (22) 5871 (21)Diagnosis groups
Other 2305 (25) 6912 (25)Cancer, no dementia 2583 (28) 7722 (28)Cancer, with dementia 2836 (32) 8432 (31)Dementia 1478 (16) 4434 (16)
Other diagnosesCongestive heart failure 2577 (28) 8189 (30)Chronic obstructive pulmonary disease 1682 (18) 4981 (18)
Activities of daily living (1 to 6) 3.6 6 1.3 3.6 6 1.3Cognitive performance scale (0 to 6) 2.9 6 2.1 2.9 6 2.1Advance directives
Do not hospitalize 562 (6) 426 (2)Do not resuscitate 5451 (59) 11,896 (43)
UtilizationNursing home stay #90 days 2741 (30) 8717 (32)
Inpatient days, 6 months before hospice admission 14.6 6 20.3 14.4 6 23.4State
Kansas 1908 (21) 5673 (21)Maine 262 (3) 783 (3)Mississippi 244 (3) 724 (3)New York 6392 (69) 19,151 (70)South Dakota 396 (4) 1169 (4)
* Because of rounding, percentages may not equal 100.
Hospice Enrollment and Hospitalization/Miller et al
40 July 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 111

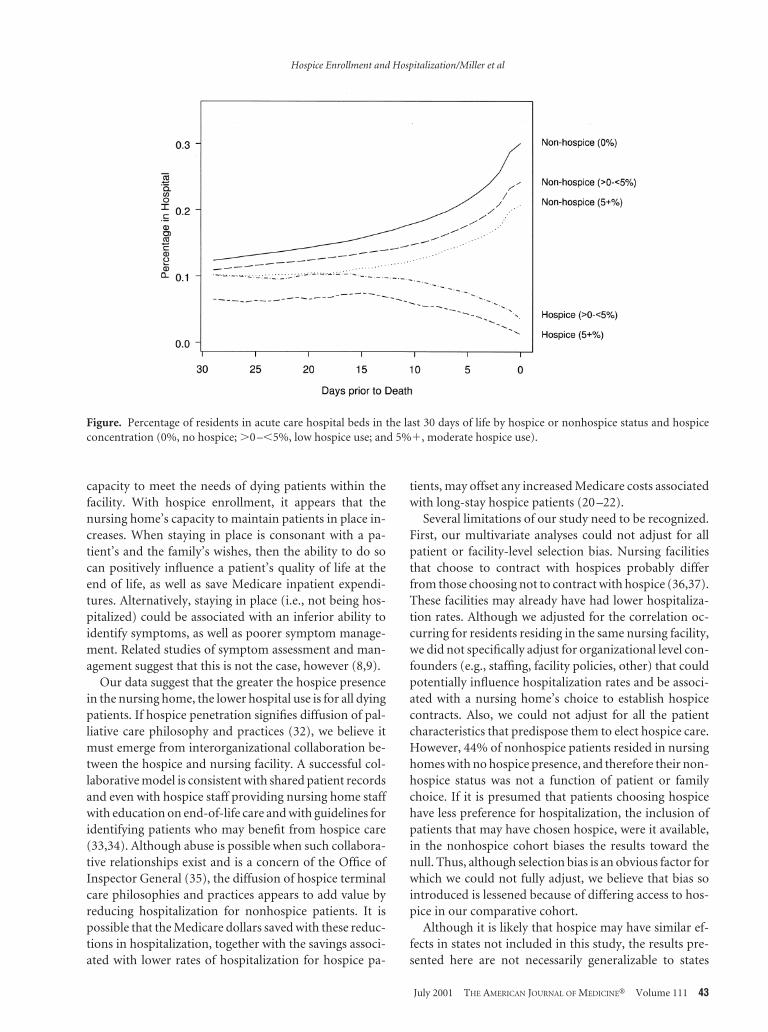
To observe differences in hospital use by hospice con-centration, we used the entire population of 240,194nursing home residents and their associated Medicare in-patient claims to calculate the percentage of residents inan acute care hospital bed on any given day in the last 30days of life. We stratified these percentages by patient’shospice status and, within these groups, by hospice con-centration levels for the nursing home in which patientsresided in their last month of life. Using the multivariatetechniques described above and adjusting for case-mixand state of residence, we examined differences in theprobability of hospitalization for nonhospice residents bycategories of hospice concentration. Hospice concentra-tion was calculated as the ratio of hospice patients to allpatients in a nursing home in a given calendar year.
RESULTS
Descriptive Comparisons of Hospice andNonhospice PatientsHospice patients were clinically similar to nonhospice pa-tients except that they were more often women and moreoften white than were nonhospice patients (Table 1). Asanticipated, greater proportions of patients enrolled inhospice had advance directives documented than did pa-tients in the nonhospice cohort (Table 1).
Hospitalization at the End of LifeIn the 30 days before death, 24% (2208) of the hospicecohort and 44% (12,100) of the nonhospice cohort werehospitalized (Table 2). Differences between hospice andnonhospice hospitalization rates were even greater whenwe compared hospice patients who were enrolled in hos-pice for the entire last 30 days of life to their nonhospicecohort matches (Table 2). For these hospice patients, thehospitalization rate was 1% (34 of 3354), whereas it was42% (4209 of 10,021) for the nonhospice patients.
In a multivariate analysis that included the entire hospiceand nonhospice cohorts, hospice enrollment for any por-tion of the last 30 days of life was significantly associated witha reduced likelihood of hospitalization in the same time pe-riod (odds ratio 0.43; 95% confidence interval [CI]: 0.39 to
0.46) (Table 3). When New York residents were excluded,hospice enrollment continued to be significantly associatedwith a reduced likelihood of hospitalization in the last 30days of life (odds ratio 0.36; 95% CI: 0.32 to 0.40). Includingall states, using conditional logistic regression modelingwithout the generalized estimating equation, and consider-ing each stratum to be each hospice patient and the matchednonhospice patients, a similar hospice effect was observed(odds ratio 0.36; 95% CI: 0.34 to 0.38).
Predicted probabilities of being hospitalized in the last30 days of life are shown in Table 4. For both cohorts,patients with dementia (and no cancer) were least likelyto be hospitalized (Table 4).
Influence of Hospice Concentration onHospitalization at End of LifeThe figure reveals the percentages of residents occupyingan acute care hospital bed on any given day of the last 30days of life, stratified by hospice concentration for theentire population of hospice and nonhospice nursinghome patients who died (n 5 240,194). Higher and in-creasing percentages of nonhospice residents were in thehospital as they approached their last days of life, whereasthe reverse was true for hospice patients (Figure). In thelast 30 days of life, 47% (52,804 of 113,307) of nonhospiceresidents in facilities with no hospice were hospitalized,compared with 41% (40,859 of 98,650) in facilities with a0.1% to less than a 5% hospice concentration (i.e., lowuse) and 39% (5603 of 14,512) in facilities with a 5% andgreater hospice concentration (i.e., moderate use). Inmultivariate analyses, compared with residents in facili-ties with no hospice, hospitalization of nonhospice resi-dents was less likely in facilities with low hospice use(odds ratio 0.82; 95% CI: 0.80 to 0.84) and least likely infacilities with moderate hospice use (odds ratio 0.71; 95%CI: 0.69 to 0.74).
DISCUSSION
This study supports the hypothesis that hospice care de-livered in nursing homes is associated with lower rates ofhospitalization in the last 30 days of life. The predicted
Table 2. Hospitalization by Hospice Enrollment Status during Last 30 Days of Life
State
Some Hospice in Last 30 Days Hospice Throughout Last 30 Days
Hospice Nonhospice Hospice Nonhospice
Percent Hospitalized (number hospitalized/number in sample)
Kansas 23 (439/1908) 46 (2610/5673) 1 (7/705) 43 (900/2092)Maine 24 (63/262) 40 (313/783) 1 (1/98) 38 (111/292)Mississippi 39 (95/244) 63 (456/724) 5 (5/96) 64 (183/286)New York 23 (1470/6392) 43 (8235/19,151) 1 (23/2318) 41 (2847/6945)South Dakota 30 (119/396) 41 (479/1169) 1 (1/137) 35 (142/406)All states 24 (2208/9202) 44 (12,100/27,500) 1 (34/3354) 42 (4209/10,021)
Hospice Enrollment and Hospitalization/Miller et al
July 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 111 41

probabilities for hospitalization in the last 30 days of lifewere 19% to 20% lower for hospice patients than theywere for the nonhospice cohort. These findings are con-sistent with study of hospice care in the community donealmost 2 decades ago (19,29).
The observed association between hospice enrollmentand a lower probability of hospitalization is consistentwith previous research revealing hospice enrollment to besignificantly associated with reduced Medicare inpatient
expenditures in the last month of life (20 –22). At least forthe states in our study, our findings extend the generaliz-ability of this observed hospice effect to include hospicecare provided in the nursing home. Our hospitalizationfindings are also consistent with findings that closer med-ical management (by physicians or physician assistants)is associated with reductions in hospitalization (30,31).Reductions in hospitalization are a function of choice(patient and nursing home) and reflect a nursing home’s
Table 3. Effect of Hospice Enrollment on Hospitalization—Multivariate Analysis
Variable
Odds Ratio(95% Confidence Interval)
(n 5 36,702)
Hospice enrollment 0.43 (0.39, 0.46)Age (per 10-year increase) 0.99 (0.96, 1.02)Male sex 1.01 (0.96, 1.06)Non-white race 1.10 (1.01, 1.19)Married 1.05 (0.99, 1.11)Diagnosis group*Cancer, no dementia 0.90 (0.85, 0.96)Cancer, with dementia 1.05 (0.99, 1.12)Dementia 1.02 (0.95, 1.10)Other diagnoses
Congestive heart failure 1.08 (1.03, 1.14)Chronic obstructive pulmonary disease 0.98 (0.92, 1.03)
Activities of daily living (per unit increase) 0.90 (0.88, 0.92)Cognitive performance scale (per unit increase) 0.95 (0.93, 0.96)Advance directives
Do not hospitalize order 0.77 (0.65, 0.91)Do not resuscitate order 0.80 (0.76, 0.84)
UtilizationNursing home stay #90 days 1.16 (1.09, 1.23)
Inpatient days, 6 months before hospice admission(per day increase)
1.02 (1.02, 1.02)
States†
Kansas 1.40 (1.15, 1.69)Mississippi 2.09 (1.70, 2.56)New York 1.15 (0.98, 1.35)South Dakota 1.28 (1.07, 1.55)
* Reference group is “Other.”† Reference state is Maine.
Table 4. Predicted Probabilities of Hospitalization in Last 30 Days of Life by Diagnosis Groups and Hospice Enrollment Status*
Probability of Hospitalization (95% Confidence Interval)
Diagnosis Groups
Cancer, NoDementia
Cancer, withDementia Dementia
OtherDiagnoses
Hospice enrollment statusHospice 0.29 (0.27, 0.30) 0.23 (0.22, 0.25) 0.19 (0.17, 0.20) 0.27 (0.25, 0.28)Nonhospice 0.49 (0.48, 0.51) 0.42 (0.40, 0.43) 0.39 (0.37, 0.41) 0.47 (0.46, 0.49)
* Predicted probabilities reflect the probability of hospitalization based on the average of the values for the variables age, sex, race, marital status,congestive heart failure, chronic obstructive pulmonary disease, activities of daily living, cognitive performance scale, do not hospitalize order, do notresuscitate order, nursing home stay #90 days, inpatient days 6 months before hospice admission, and state of residence.
Hospice Enrollment and Hospitalization/Miller et al
42 July 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 111
capacity to meet the needs of dying patients within thefacility. With hospice enrollment, it appears that thenursing home’s capacity to maintain patients in place in-creases. When staying in place is consonant with a pa-tient’s and the family’s wishes, then the ability to do socan positively influence a patient’s quality of life at theend of life, as well as save Medicare inpatient expendi-tures. Alternatively, staying in place (i.e., not being hos-pitalized) could be associated with an inferior ability toidentify symptoms, as well as poorer symptom manage-ment. Related studies of symptom assessment and man-agement suggest that this is not the case, however (8,9).
Our data suggest that the greater the hospice presencein the nursing home, the lower hospital use is for all dyingpatients. If hospice penetration signifies diffusion of pal-liative care philosophy and practices (32), we believe itmust emerge from interorganizational collaboration be-tween the hospice and nursing facility. A successful col-laborative model is consistent with shared patient recordsand even with hospice staff providing nursing home staffwith education on end-of-life care and with guidelines foridentifying patients who may benefit from hospice care(33,34). Although abuse is possible when such collabora-tive relationships exist and is a concern of the Office ofInspector General (35), the diffusion of hospice terminalcare philosophies and practices appears to add value byreducing hospitalization for nonhospice patients. It ispossible that the Medicare dollars saved with these reduc-tions in hospitalization, together with the savings associ-ated with lower rates of hospitalization for hospice pa-
tients, may offset any increased Medicare costs associatedwith long-stay hospice patients (20 –22).
Several limitations of our study need to be recognized.First, our multivariate analyses could not adjust for allpatient or facility-level selection bias. Nursing facilitiesthat choose to contract with hospices probably differfrom those choosing not to contract with hospice (36,37).These facilities may already have had lower hospitaliza-tion rates. Although we adjusted for the correlation oc-curring for residents residing in the same nursing facility,we did not specifically adjust for organizational level con-founders (e.g., staffing, facility policies, other) that couldpotentially influence hospitalization rates and be associ-ated with a nursing home’s choice to establish hospicecontracts. Also, we could not adjust for all the patientcharacteristics that predispose them to elect hospice care.However, 44% of nonhospice patients resided in nursinghomes with no hospice presence, and therefore their non-hospice status was not a function of patient or familychoice. If it is presumed that patients choosing hospicehave less preference for hospitalization, the inclusion ofpatients that may have chosen hospice, were it available,in the nonhospice cohort biases the results toward thenull. Thus, although selection bias is an obvious factor forwhich we could not fully adjust, we believe that bias sointroduced is lessened because of differing access to hos-pice in our comparative cohort.
Although it is likely that hospice may have similar ef-fects in states not included in this study, the results pre-sented here are not necessarily generalizable to states
Figure. Percentage of residents in acute care hospital beds in the last 30 days of life by hospice or nonhospice status and hospiceconcentration (0%, no hospice; .0 –,5%, low hospice use; and 5%1, moderate hospice use).
Hospice Enrollment and Hospitalization/Miller et al
July 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 111 43

other than the study states. Last, our logistic regressionwas not conditioned on the factors on which we matched,and this may have affected our analytic efficiency. None-theless, because this study was a retrospective cohortstudy rather than a case control study, use of conditionallogistic regression was not required to reduce bias intro-duced by matching (27).
In conclusion, hospice care provision in the nursinghome setting is associated with a reduced probability ofhospitalization for those dying residents enrolled in hos-pice. Additionally, through a possible diffusion effect(32), hospice presence in nursing homes appears also tobe associated with reductions in end-of-life hospitaliza-tions for nonhospice nursing home residents. Reductionsin hospitalizations associated with hospice care may po-tentially improve the quality of life at the end of life fornursing home residents as well as result in Medicare in-patient expenditure savings and perhaps in total Medi-care expenditure savings for nursing home residents. Re-search is needed to evaluate whether these associated ben-efits do indeed occur. Nonetheless, these findings, as wellas other related research (8,9), suggest that hospice refer-ral and presence can assist physicians in managing thecare of dying nursing home residents.
REFERENCES1. Brock DB, Foley DJ. Demography and epidemiology of dying in the
U.S. with emphasis on deaths of older persons. Hosp J. 1998;13:49–60.2. Keay TJ, Schonwetter RS. Hospice care in the nursing home. Am
Fam Physician. 1998;57:491– 493.3. Miller SC, Mor V, Coppola K, et al. The Medicare hospice benefit’s
influence on dying in nursing homes. J Palliat Med. 1998;1:367–376.4. Miller SC, Gozalo P, Mor V. Use of Medicare’s hospice benefit by
nursing facility residents. In: Synthesis and Analysis of Medicare’sHospice Benefit. Washington, DC: Office of Disability, Aging, andLong Term Care Policy in the Office of the Assistant Secretary forPlanning and Evaluation, US Department of Health and HumanServices; 2000.
5. Bernabei R, Gambassi G, Lapane K, et al. Management of pain inelderly patients with cancer. SAGE Study Group. Systematic Assess-ment of Geriatric Drug Use via Epidemiology. JAMA. 1998;279:1877–1882.
6. Ferrell BA. Pain evaluation and management in the nursing home.Ann Intern Med. 1995;123:681– 687.
7. Wagner AM, Goodwin M, Campbell B, et al. Pain prevalence andpain treatments for residents in Oregon nursing homes. GeriatricNursing. 1997;18:268 –272.
8. Baer WM, Hanson LC. Families’ perception of the added value ofhospice in the nursing home. J Am Geriatr Soc. 2000;48:879 – 882.
9. Miller SC, Gozalo P, Mor V. Outcome and utilization for hospiceand non-hospice nursing facility decedents. In: Synthesis and anal-ysis of Medicare’s Hospice Benefit. Washington, DC: Office of Dis-ability, Aging, and Long Term Care Policy in the Office of the As-sistant Secretary for Planning and Evaluation, U.S. Department ofHealth and Human Services; 2000.
10. Castle NG, Mor V. Hospitalization of nursing home residents: Areview of the literature, 1980 –1995. Medical Care Research and Re-view. 1996;53:123–148.
11. Densen PM. The elderly and the health care system: Another per-spective. Milbank Q. 1987;65:614 – 638.
12. Laliberte L, Mor V, Berg K, et al. Impact of the Medicare CatastrophicCoverage Act on nursing homes. Milbank Q. 1997;75:203–233.
13. Murtaugh CM, Freiman MP. Nursing home residents at risk ofhospitalization and the characteristics of their hospital stays. Ger-ontologist. 1995;35:35– 43.
14. Sekscenski ES. Discharges from nursing homes: 1985 NationalNursing Home Survey. Vital Health Stat. 1990;103:1– 87.
15. Smith WR, Kellerman A, Brown JS. The impact of nursing hometransfer policies at the end of life on a public acute care hospital.J Am Geriatr Soc. 1995;43:1052–1057.
16. Weissert WC, Scanlon WJ. Determinants of nursing home dis-charge status. Med Care. 1985;23:333–343.
17. Creditor MC. Hazards of hospitalization of the elderly. Ann InternMed. 1993;118:219 –223.
18. Saliba D, Raynard K, Buchanan J, et al. Appropriateness of thedecision to transfer nursing facility residents to the hospital. J AmGeriatr Soc. 2000;48:154 –163.
19. Greer DS, Mor V, Morris JN, et al. An alternative in terminal care:Results of the National Hospice Study. J Chronic Dis. 1986;39:9 –26.
20. Kidder D. The effects of hospice coverage on Medicare expendi-tures. Health Serv Res. 1992;27:195–217.
21. Lewin-VHI Inc. An Analysis of the Cost Savings of the Medicare Hos-pice Benefit. Arlington, VA: National Hospice Organization; 1995.
22. Mor V, Kidder D. Cost savings in hospice: final results of the Na-tional Hospice Study. Health Serv Res. 1985;20:407– 422.
23. Bernabei R, Gambassi G, Lapane K, et al. Characteristics of theSAGE database: A new resource for research on outcomes in long-term care. J Gerontol. 1998;53:M1–M9.
24. Gambassi G, Landi F, Peng L, et al. Validity of diagnostic and drugdata in standardized nursing home resident assessment: Potentialfor geriatric pharmacoepidemiology. Med Care. 1998;36:167–179.
25. Health Care Financing Administration. Minimum Data Set PlusMultistate Nursing Home Case Mix and Quality DemonstrationTraining Manual. Natick, MA: Eliot Press, 1991:17–38.
26. SAS Institute Inc. SAS/STAT Software. Changes and Enhancementthrough Release 6.12. Cary, NC: 1997.
27. Rothman, KJ, Greenland S. Modern Epidemiology. Philidelphia, PA:Lippincott-Raven Publishers; 1998:147–161.
28. Morris JN, Fries BE, Mehr DR, et al. MDS Cognitive PerformanceScale. J Gerontol. 1994;49:M174–M182.
29. Kane RL, Wales J, Bernstein L, et al. A randomized controlled trialof hospice care. Lancet. 1984;1:890 – 894.
30. Intrator O, Castle N, Mor V. Facility characteristics associated withhospitalization of nursing home residents: results of a nationalstudy. Med Care. 1999;37:228 –237.
31. Ackerman RJ, Kemle KA. Death in a nursing home with activemedical management. Ann Long-Term Care. 1999;7:313–318.
32. Rogers EM. Diffusion of innovation, 3rd ed. New York: Free Press, 1983.33. National Hospice and Palliative Care Organization. Medical Guide-
lines for Determining Prognosis in Selected Non-Cancer Diseases, 2nd
Edition. Alexandria, VA. 1996.34. National Hospice and Palliative Care Organization. Nursing Home
Task Force Report. Alexandria, VA. 1998.35. Office of Inspector General, U.S. Department of Health, and Hu-
man Services (Document OEI-05–95– 00251). Hospice and NursingHome Contractual Relationships. Washington, DC. November1997.
36. Castle NG, Mor V, Banaszak-Holl J. Special care hospice units innursing homes. Hosp J. 1997;12:59 – 69.
37. Petrisek A, Mor V. Hospice in nursing homes: A facility level anal-ysis of the distribution of hospice beneficiaries. Gerontologist. 1998;39:279 –290.
Hospice Enrollment and Hospitalization/Miller et al
44 July 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 111