hormone replacement therapy dr annice mukherjee consultant and lecturer in endocrinology salford...
TRANSCRIPT
Hormone Replacement Therapy
Dr Annice MukherjeeConsultant and Lecturer in Endocrinology
Salford Royal NHS
Definition of Menopause
Failure of steroid production and ovulation and the final cessation of menstruation
Average age 51 yrs Incidence of natural
premature ovarian failure before age 40 is estimated as 1%
Menopause facts
70% women suffer with symptoms
Symptoms may occur before menopause is biochemically or clinically evident
Symptoms spontaneously improve over 2-5 years

Symptoms of Menopause
Menstrual irregularity indicating failing ovulation
Vasomotor symptoms - hot flushes/flashes, night sweats
Sleep disturbance Vaginal symptoms Mood changes Joint pains Physical
Skin/body habitus/weight changes Sexual dysfunction
Eleanor
46, menopause began last year Has had fractured humerus and pelvis after
trivial injuries in past Otherwise very healthy BMI 19, FH osteoporosis Tolerating menopause well with few
symptoms
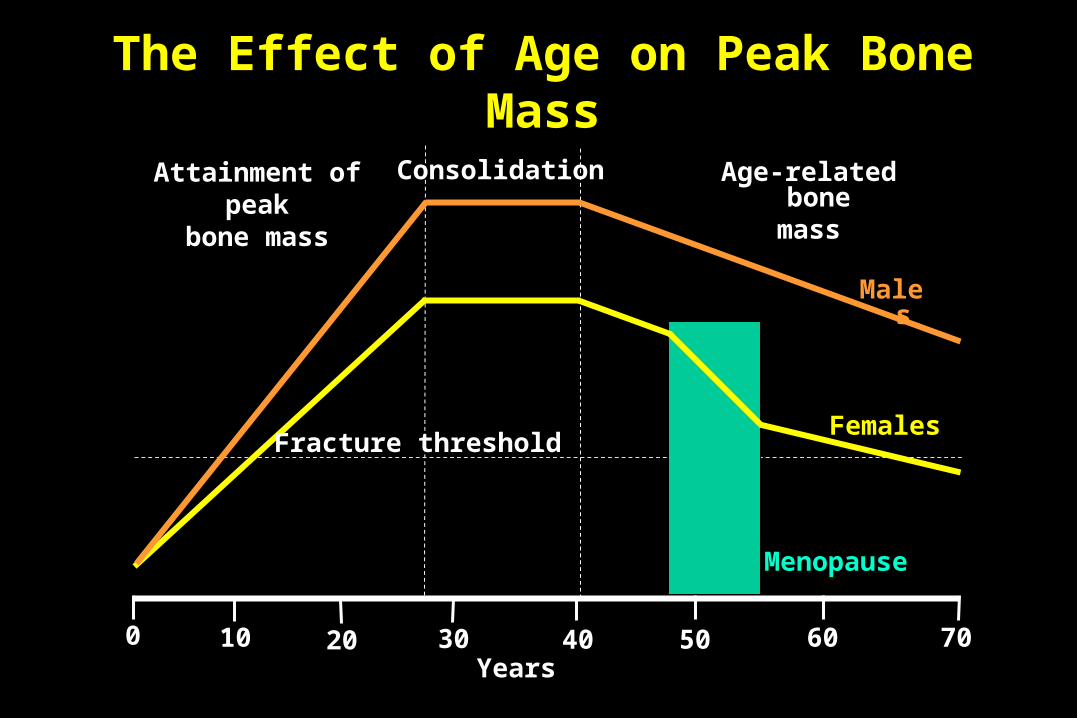
The Effect of Age on Peak Bone Mass
Attainment ofpeak
bone mass
Consolidation Age-related bone mass
Males
Females
Menopause
Fracture threshold
Years0 10 20 30 40 50 60 70

Eleanor
Has she had BMD checked??
High risk of osteoporosis from history
Would benefit form HRT even in absence of symptoms in terms of bone protection
Vicky
33 year old female, married, no children Menses stopped 18 months ago, several
pregnancy tests negative, Bloods LH 70, FSH 50, Oestradiol 42 She wants to know if she can have children She also complains of vaginal dryness and
itching even thought she has had treatment for thrush

Premature Menopause Requires estrogen replacement until age of
natural menopause Symptoms may be more severe than natural
menopause Urogenital and sexual problems also impact Cardiovascular risk increased Osteoporosis Fertility
Vicky
Consider doing autoantibody screen ?Family history prem. menopause/
behavioural problems in boys (-fragile X syndrome)
Estrogen replacement required for well being and bone protection-risk of osteoporosis
Can use high doses of HRT in this context Pregnancy possible with egg donation
Menopause Aims of Management
To maximise the quality of life of hypogonadal women by:
Reducing the impact of menopausal symptoms
Addressing the increased risk of osteoporosis

Treatment options
Lifestyle Exercise, stop smoking, limiting alcohol, caffeine &
stress, adopting a healthy diet
Natural herbs & remedies Placebo treatment reduces hot flushes by 50%
HRT Other prescription therapies
Natural herbs & remedies Phytoestrogens (Red clover)
Structural similarity to oestradiolEfficacy data insufficient
Black cohosh Buttercup family Flushes & other symptoms Data insufficient to date
Progesterone creams Acupuncture
Yvonne 62 year old housewife Severe MSK pain, hot flushes, sleep
disturbance low libido, mood swings Despirate for symptom control! BMI 40, BP 160/95 Tx for hyperlipidaemia Strong FH of IHD & 2 sisters with
breast cancer Biochemistry- post-menopausal

Prescription Remedies
HRT preparations Progestogens Venlafaxine and Paroxetine Clonidine Gabapentin
Yvonne
62 year old housewife Identify ranking of symptoms Is she depressed? Would significant weight loss help well
being? If main symptom is flushing consider SSRI-
upto 70% improvement in flushes/sweating She may wish to start with a natural remedy
The Role of HRT Natural menopausal symptoms Premature menopause Surgical menopause Other causes of oestrogen deficiency
under age of 50 yrs Menopausal women at significant risk of
osteoporotic fracture Consider contraindications risks carefully
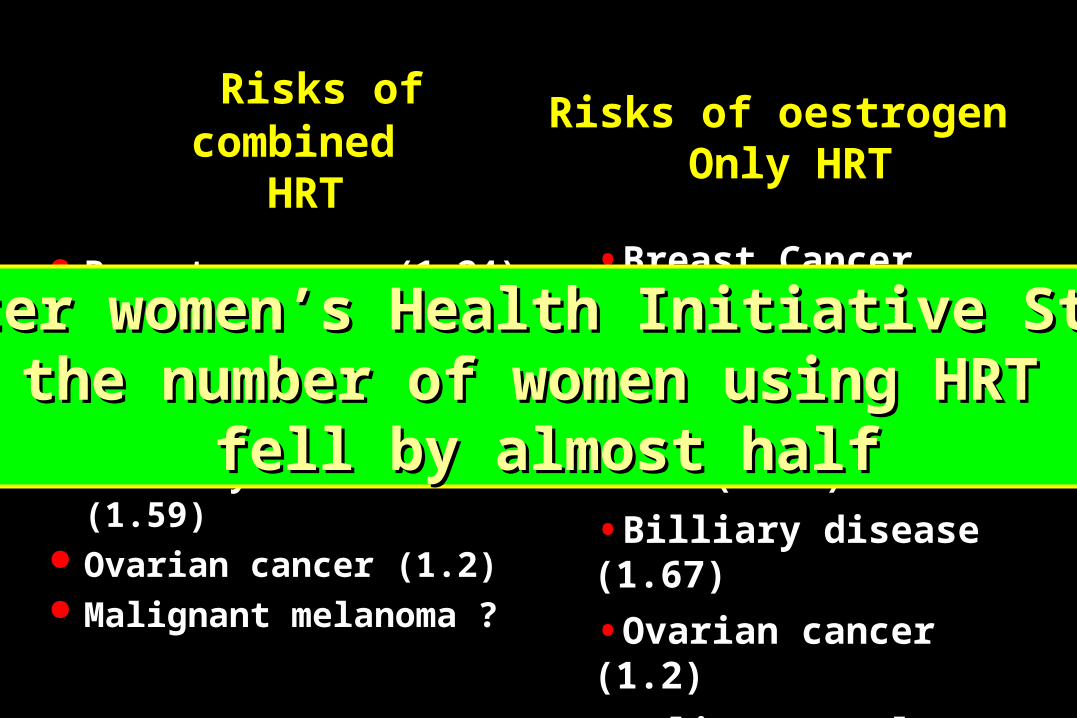
Risks of combined HRT
Breast cancer (1.24) Stroke(1.41) DVT (1.95) IHD (1.24) Billiary disease (1.59) Ovarian cancer (1.2) Malignant melanoma ?
Risks of oestrogen Only HRT
•Breast Cancer (0.77)
•Stroke (1.39)
•DVT (1.47)
•IHD (0.77)
•Billiary disease (1.67)
•Ovarian cancer (1.2)
•Malignant melanoma ?
After women’s Health Initiative StudyAfter women’s Health Initiative Studythe number of women using HRT the number of women using HRT
fell by almost halffell by almost half
Benefits of HRT
Vasomotor symptomsMood changes and insomniaOsteoporosisUrogenital symptomsSexual dysfunction

Use of HRT Start during perimenopause in natural
menopausal (earlier the better) Most women use HRT for less than 5 years Vaginal oestrogen is effective for urogenital
symptoms Merits of long term HRT should be assessed for
each individualPremature menopauseOsteoporosis
HRT preparations/combinations
Oestrogen oral/patches/gels With progestogen for women with an intact
uterus Sequential preparations (bleed) Continuous combined preparations (non-bleed)
Intrauterine progestogen
HRT; Dose and route
Use lowest dose for the shortest possible time in women with natural menopause
Women with premature menopause will need higher doses
Transdermal has less metabolic effect and probably safer

Tibolone
Synthetic steroid with oestrogenic, progestogenic and androgenic actions
Relieves symptoms Protects bones Improves sexual function Shares some of HRT risks although
possibly not all

Jenny
50 yr old police officer Menopausal symptoms++ Had TAH for endometriosis 4 years before Now feels so bad that she can’t work, thinks
she will lose her job soon. Can’t afford to be un-employed
Has maternal aunt who died of breast cancer age 45
Relative contraindications
Breast cancer Thromboembolic disease Coronary heart disease Stroke Gall bladder disease Dementia Migraine
Jenny
Difficult problem Quality of life vs. uncertain cancer risk Could have trial of low dose oestrogen only
transermal HRT with close monitoring & referral to breast cancer family history clinic
Spell out risks versus benefits
Joan
52 year old cleaner Menses stopped 1 year ago Reduced libido, low mood no flushes Worried her partner is going to leave
her Tried HRT no benefit
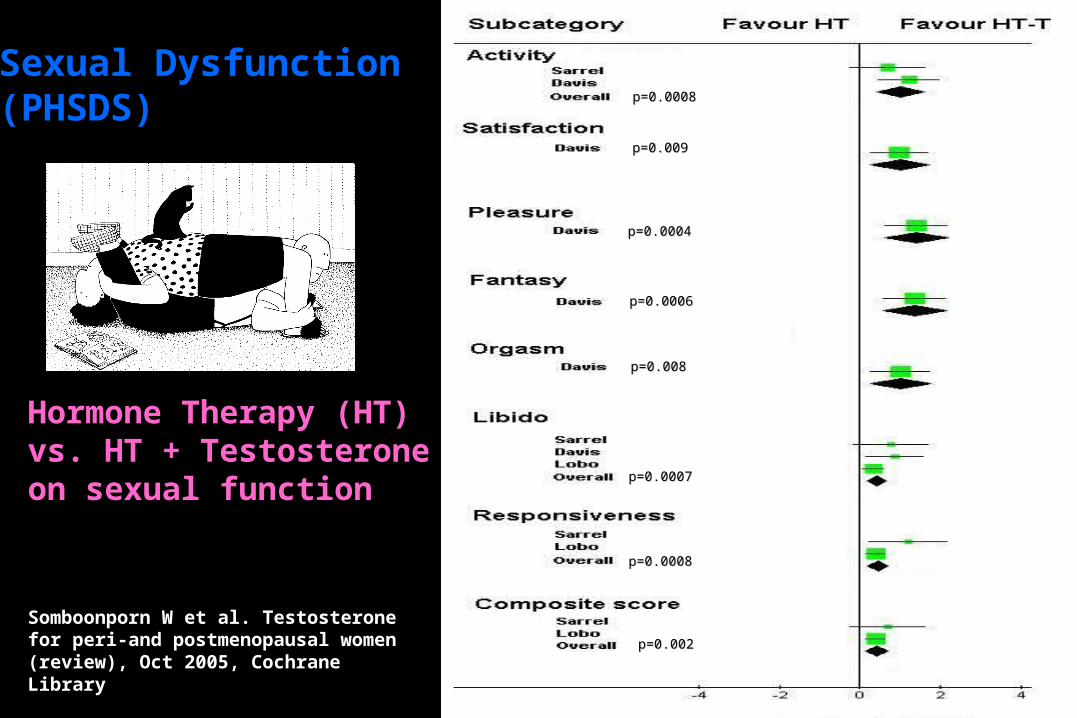
Somboonporn W et al. Testosterone for peri-and postmenopausal women (review), Oct 2005, Cochrane Library
Hormone Therapy (HT) vs. HT + Testosteroneon sexual function
p=0.002p=0.002
p=0.0008p=0.0008
p=0.0007p=0.0007
p=0.008p=0.008
p=0.0006p=0.0006
p=0.0004p=0.0004
p=0.009p=0.009
p=0.0008p=0.0008
Sexual Dysfunction(PHSDS)
Indications for Androgen Therapy
Progressive loss of libido and sexual enjoyment associated with non specific tiredness, loss of drive, motivation and sense of well being
Exclude clinical depression or other explanation
Joan
52 rear old cleaner management? Is she depressed? Is the reduced libido lack of interest or physical
(vaginal discomfort/pain) or both If complex psychosexual issues consider referral
to specialist clinic Consider topical oestrogen Consider testosterone/HRT combination
Oral restandol/intrinsa patches
Urogenital Atrophy
10 - 40% of hypogonadal women are symptomatic
Oestrogens effective in the management Most convincing evidence being in support
of local treatment Doses lower than conventionally used

Conclusions
HRT has well recognised benefits and well publicised risks
Consider the indications and risk carefully and discuss them with the patient
Tailor the treatment offered to the needs of the individual patient

Thank-You!