herpes zoster: virology, treatment, and vaccine - cecity · december 2014 outbreaks, outcomes,...
TRANSCRIPT
Outbreaks, Outcomes, Recommendations December 2014AOA Health Watch 20
Herpes zoster (HZ; shingles) occurs
following reactivation of the varicella zoster virus.
The incidence of zoster rises with increasing age
and decreasing T-cell immune function. A common complication
is postherpetic neuralgia (PHN), which causes a burning or stabbing
pain that may continue for months to years after resolution of the rash. A live varicella
zoster vaccine (Zostavax) has been approved for prevention of shingles and has been shown effective
in reducing the occurrence of zoster and incidence of PHN. This article discusses the virology, symptoms of HZ,
complications, treatment, and the available vaccine.
Herpes zoster: virology, treatment, and vaccine
Outbreaks, Outcomes, Recommendations December 2014AOA Health Watch 20
Nicole Tillman, DOLloyd J. Cleaver, DO, FAOCD
© S
HU
TTE
RS
TOC
K.C
OM

December 2014 Outbreaks, Outcomes, Recommendations AOA Health Watch 21
OverviewVaricella zoster virus (VZV) is a double-stranded DNA herpes virus responsible for causing varicella (chickenpox) and HZ.1-7 Following primary infection with chickenpox, the VZV remains latent in the dorsal root ganglion. When T-cell-mediated immunity declines, as with age, or immunosuppression, the virus can become reactivated and cause HZ.1,2,5 In the United States, there are approximately 1 million new cases per year and over half of those cases occur in people older than 60.2,4 The lifetime risk of HZ is estimated to be 10%-30%.3,6
Discussion and treatment recommendationsReactivation of VZV may be triggered by stress, fever, radiation, trauma, immunosuppression, increasing age, or may occur spontaneously. During HZ, the virus replicates in the affected dorsal root ganglion and spreads down the neural tissue, causing pain and a cutaneous eruption.1,3,5 HZ often begins with a prodrome of intense pain that occurs 4-6 days before the vesicular rash. This pain can be severe and misdiagnosed as angina, nephrolithiasis, cholecystitis, or lumbar radiculopathy.7 Following the prodrome, an erythematous, papular, or vesicular rash occurs in the dermatome corresponding to the involved dorsal root ganglion (Figure 1). The eruption most commonly occurs on the trunk and typically remains unilateral.1-3,5 Occasionally, there is not a cutaneous eruption following the prodrome of pain, which is referred to as “zoster sine herpete” (zoster without rash).1,8 In adults with an intact immune system, zoster resolves without sequelae. In immunosuppressed patients, or elderly patients, various complications may occur, including PHN, herpes ophthalmicus, facial nerve palsy, bacterial superinfection, and disseminated zoster.1,5 Ramsay Hunt syndrome occurs when the virus infects the geniculate ganglion, causing vesicles of the ear canal and/or mouth with associated tinnitus, hearing loss, nystagmus, nausea, vertigo, and facial nerve paralysis.1, 9-11 Ophthalmic zoster
occurs when the zoster virus involves the fifth cranial nerve (trigeminal nerve). Hutchinson’s sign, vesicles on the side or tip of the nose, is strongly associated with ocular involvement and warrants ophthalmic evaluation.5,10,11 Ophthalmic zoster occurs in 7% of zoster patients, with 20%-70% developing associated ocular disease, in severe cases possibly
blindness.6,11 A person with zoster can infect another with varicella (chickenpox) if the susceptible person comes in direct contact with vesicular fluid; however, a person with zoster cannot directly give another person zoster.3,11
Antiviral treatment is the optimum treatment modality and ideally should be started within the first 72 hours of symptoms.1,10 The sooner therapy is
started, the more likely it is to reduce the severity and duration of zoster. Acyclovir, famciclovir, and valacyclovir are all approved for treatment.4,5,12 Valacyclovir 1000 mg or famciclovir 500 mg can be given 3 times a day for 7 days and is generally preferred over acyclovir 800 mg, which is given 5 times a day for 7 days.10,13
Immunocompromised patients with disseminated zoster, as well as those with serious complications, may be treated with intravenous acyclovir.14 Antiviral therapy has been shown to not only reduce the duration of zoster, but also reduce the incidence of PHN.10,15
Postherpetic neuralgia (PHN) is the most common complication, occurring in 10%-30% of zoster
Source: Cleaver Dermatology.
Figure 1. Erythematous papules and vesicles arising within a dermatome.
Almost 1 out of 3 people in the United States will develop herpes zoster during their lifetime.
Outbreaks, Outcomes, Recommendations December 2014AOA Health Watch 22
patients.3,4,9,10 This pain is described as burning, shooting, or stabbing and may last for months to years and be very debilitating.1,10,16 The risk and severity of PHN increases with increasing age—73% of zoster patients aged 70 years or older will develop some degree of it.4,14 Post herpetic neuralgia (PHN) is often resistant to treatment.1,3,4 Topical treatment modalities include topical lidocaine or capsaicin. Systemic therapy includes gabapentin, pregabalin, amitriptyline, nortriptyline, tramadol, morphine, and oxycodone.1,10,16 Zostavax is not effective in treating the pain acutely.1,16
In 2006, the US Food and Drug Administration (FDA) approved Zostavax for shingles prevention in patients aged 60 years or older.12 The Shingles Prevention Study was a randomized, double-blind, placebo-controlled study that showed that the vaccine was efficacious in reducing the burden of illness by 61.1%, incidence of HZ by 51.3%, and incidence of PHN by 66.5% in patients aged 60 years or older.2 The vaccine was most successful in patients
aged 60-69 years, with effectiveness declining as age increased. Shingles did not occur as a consequence immediately following vaccination; however, if a person developed shingles later, the course lasted 20 days, as opposed to 22 days without the vaccine. The most common adverse reactions to the vaccine
were erythema (35.6%), pain (34.3%), and swelling (26.1%) at the injection site. The study concluded that the vaccine not only reduced overall incidence of HZ, but also the incidence of PHN.2
Another randomized, double-blind, placebo-controlled study with subjects aged 50-59 years showed efficacy of
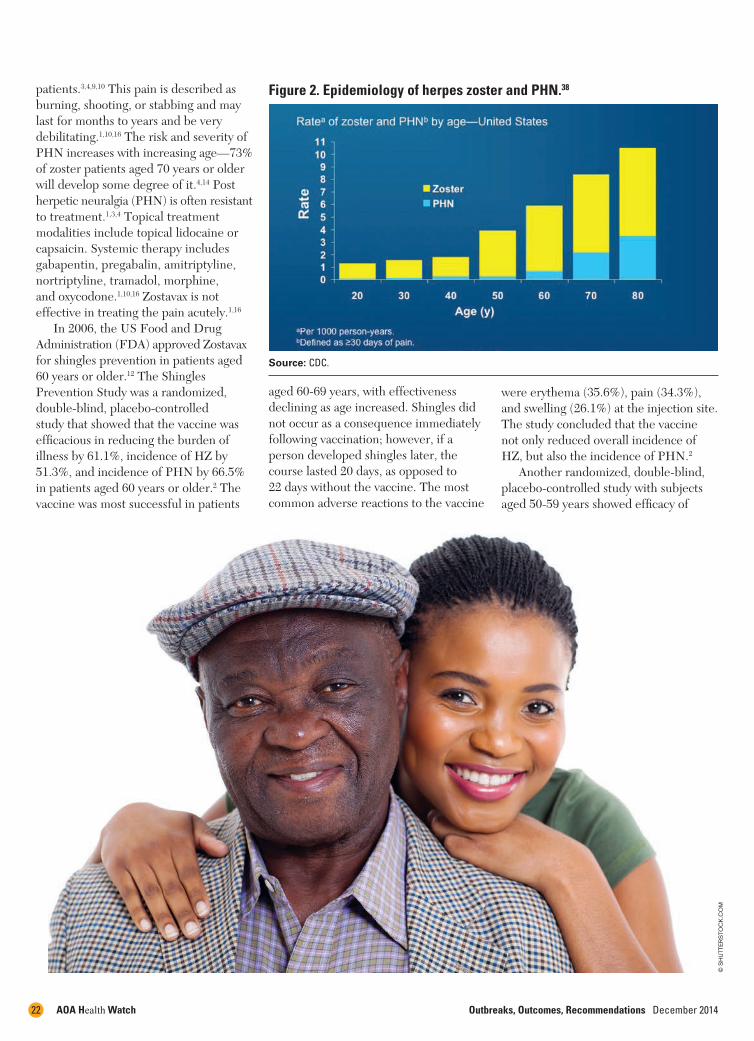
Source: CDC.
Figure 2. Epidemiology of herpes zoster and PHN.38
© S
HU
TTE
RS
TOC
K.C
OM

December 2014 Outbreaks, Outcomes, Recommendations AOA Health Watch 23
Zostavax for this age group. There were 30 cases of zoster in the vaccinated group, compared with 99 in the placebo group. Vaccine efficacy for preventing zoster was 69.8% in this population.17 In 2011, the vaccine was approved by the FDA for patients aged 50 years or older; however, the Centers for Disease Control and Prevention (CDC) only recommends the vaccine for patients aged 60 years or older.3,11,12
Zostavax is a live attenuated vaccine given subcutaneously in the upper arm and is the only vaccine available for preventing zoster. It may be coadministered with the pneumococcal vaccine and the injectable influenza vaccine, but should not be
coadministered with another live vaccine.3 It is not indicated for the treatment of shingles, PHN, or to prevent chickenpox.3,7 The CDC recommends giving the vaccine whether or not the person remembers having had chickenpox. Studies have shown that giving 2 doses of the vaccine did not boost the immunity beyond the levels achieved following 1 dose; therefore, no booster dose is recommended.12,18 Recurrences of HZ are rare (1%-5%) because an episode of zoster boosts the immunity, effectively “immunizing” against subsequent episodes; however, the CDC still recommends giving the vaccine after a zoster episode.3,4,10,13
The vaccine is contraindicated in anyone with a history of anaphylaxis to gelatin or neomycin, with acquired or primary immunodeficiency syndromes (such as AIDS), with lymphoma or leukemia, or those receiving chemotherapy or radiation.11,12 If it has been more than 3 months since chemotherapy or radiation, the vaccine is safe. The vaccine should be given at least 2 weeks before treatment with corticosteroids. In patients receiving recombinant human immune mediators or modulators, the vaccine should be given 1 month before or after therapy. Low doses of 6-mercaptopurine (≤1.5 mg/kg/day), azathiaprine (≤ 3.0 mg/kg/day), or
© S
HU
TTE
RS
TOC
K.C
OM
Outbreaks, Outcomes, Recommendations December 2014AOA Health Watch 24
methotrexate (≤ 0.4 mg/kg/week), are not contraindications. Humoral immunodeficiency, such as hypogammaglobulinemia, is not a contraindication.11,12 Because the vaccine is a live vaccine, it is contraindicated in pregnant women. Zostavax should not be given to children and should not be used as a substitution for the
varicella (chickenpox) vaccine.11,12 An acute episode of zoster treated in an outpatient clinic costs $112-$287. If hospitalized the cost drastically increases to $3321-$7206.19 The vaccine costs roughly $150. Medicare part D covers the shingles vaccine; however, patients might be required to pay a copay or a portion of the cost. Medicare part B does not cover the vaccine.
The CDC recommends zoster vaccine for individuals aged 60 years and older.
December 2014 Outbreaks, Outcomes, Recommendations AOA Health Watch 25
Nicole Tillman, DO, is a first-year dermatology resident at Northeast Regional Medical Center/ATSU, in Kirksville, Missouri. She graduated from Kirksville College of Osteopathic Medicine in Kirksville, Missouri. Dr Tillman can be reached at [email protected].
Lloyd J. Cleaver, DO, FAOCD, is program director for dermatology at Northeast Regional Medical Center/ATSU, in Kirksville, Missouri. Dr Cleaver graduated from Kirksville College of Osteopathic Medicine in Kirksville, Missouri and completed his internship and residency at the Navy Regional Medical Center in San Diego, California. He is board certified in dermatology and Mohs surgery. Dr Cleaver can be reached at [email protected].
Medicaid may possibly cover the vaccine. Most private health insurance plans cover the vaccine for people aged 60 years or older, and some plans cover for people aged 50-59.11 Over 300,000 outpatient visits, 375,000 prescriptions, 9700 emergency room visits, and 10,000 hospitalizations were projected to be eliminated with the vaccine, saving an estimated $82-$103 million dollars.20
Final notesAs the population of the United States ages, the incidence of HZ is expected to increase. Zoster is associated with various complications, commonly PHN, and the elderly are most at risk. The safety and efficacy of Zostavax has been demonstrated with multiple trials; still, only 14.4% of adults aged 60 years or older were vaccinated in 2010.14 Encouraged vaccination against HZ will positively impact the health and quality of life for the steadily growing elderly population.
References1. Mueller NH, Gilden DH, Cohrs RJ,
Mahalingam R, Nagel MA. Varicella zoster virus infection: clinical features, molecular pathogenesis of disease, and latency. Neurol Clin. 2008;26(3):675-678.
2. Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352(22):2271-2284.
3. Centers for Disease Control and Prevention. Shingles (herpes zoster). http://www.cdc.gov/shingles/index.html. Accessed September 20, 2014.
4. Weaver, BA. The burden of herpes zoster and postherpetic neuralgia in the United States. J Am Osteopath Assoc. 2007;107(3 suppl 1):S2-S7.
5. Gnann JW, Jr., Whitley RJ. Clinical practice. Herpes zoster. N Engl J Med. 2002;347(5):340-346.
6. Ragozzino MW, Melton LJ, III, Kurland LT, Chu CP, Perry HO. Population-based study of herpes zoster and its sequelae. Medicine (Baltimore). 1982;61(5):310-316.
7. Drolet M, Oxman MN, Levin MJ, et al. Vaccination against herpes zoster in developed countries: state of the evidence. Hum Vaccin Immunother. 2013;9(5):1177-1184.
8. Gilden DH, Wright RR, Schneck SA, Gwaltney JM, Jr., Mahalingam R. Zoster sine herpete, a clinical variant. Ann Neurol. 1994;35(5):530-533.
9. Sweeney CJ, Gilden DH. Ramsay Hunt syndrome. J Neurol Nuerosurg Pyschiatry. 2001;71(2):149-154.
10. Dworkin RH, Johnson RW, Breuer J, et al. Recommendations for the management of herpes zoster. Clin Infect Dis. 2007;44(suppl 1):S1-S26.
11. Harpaz R, Ortega-Sanchez IR, Seward JF; Advisory Committee on Immunization Practices (ACIP) Centers for Disease Control and Prevention (CDC). Prevention of herpes zoster. MMWR Recomm Rep. 2008;57(RR-5):1-30.
12. FDA. Zostavax vaccine. http://www.fda.gov/downloads/BiologicsBloodVaccines/Vaccines/ApprovedProducts/UCM132831.pdf. Accessed September 21, 2014.
13. Tyring SK, Beutner KR, Tucker BA, Anderson WC, Crooks RJ. Antiviral therapy for herpes zoster; randomized, controlled clinical trial of valacyclovir and famciclovir therapy in immunocompetent patients 50 years and older. Arch Fam Med. 2000;9(9):863-869.
14. Nagel MA, Gilden D. The challenging patient with varicella-zoster virus disease. Neurol Clin Pract. 2013;3(2):109-117.
15. Jackson JL, Gibbons R, Meyer G, Inouye L. The effect of treating herpes zoster with oral acyclovir in preventing postherpetic neuralgia. A meta analysis. Arch Intern Med. 1997;157(8):909-912.
16. Gan EY, Tian EA, Tey HL. Management of herpes zoster and post-herpetic neuralgia. Am J Clin Dermatol. 2013;14(2):77-85.
17. Schmader KE, Levin MJ, Gnann JW, et al. Efficacy, safety, and tolerability of herpes zoster vaccine in persons aged 50-59 years. Clin Infect Dis. 2012;54(7):922-928.
18. Vermeulen JN, Lange JM, Tyring SK, et al. Safety, tolerability, and immunogenicity after 1 and 2 doses of zoster vaccine in healthy adults ≥ 60 years of age. Vaccine. 2012;30(5)904-910.
19. Holcomb K, Weinberg JM. A novel vaccine (Zostavax) to prevent herpes zoster and postherpetic neuralgia. J Drugs Dermatol. 2006;5(9):863-866.
20. Pellissier JM, Brisson M, Levin MJ. Evaluation of the cost-effectiveness in the United States of a vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. Vaccine. 2007;25(49):8326-8337.
© S
HU
TTE
RS
TOC
K.C
OM