health, safety, security and environment - … safety, security and environment (hsse) management...
TRANSCRIPT

Health, Safety, Security and Environment (HSSE)
Management System Requirements
And
Incident Investigation Process
HSSE Management System
• Why have an HSSE Management System?
– To provide a systematic approach to HSSE management and serve as a foundation for continually improving HSSE performance.
– To set clear expectations for minimum HSSE requirements and provide a structure for identification and prioritization of HSSE risks.
The JIG HSSE Management System
Guideline Elements 1. Leadership, involvement and responsibility 2. Risk assessment and control 3. Asset design and construction 4. Documentation and records 5. Personnel and training 6. Occupational health and hygiene 7. Operation and maintenance 8. Management of change 9. Contractors and suppliers 10. Incident investigation and analysis 11. Emergency preparedness 12. Community 13. Management system review and improvement
HSSEMS References
• JIG Bulletin No. 32 (March 2010) – Launch of the JIG HSSE Management System
• JIG HSSEMS Guidelines – Issue 1 (March 2010) – Available in English, French and Spanish
• JIG HSSEMS Gap Analysis Tool (March 2010) – Available in English and French
• JIG Learning from Incidents Toolbox Packs – Currently 7 packs on the website

HSSE Guidelines Document
http://www.jigonline.com/publications/hsse-publication/
HSSE Root Cause Analysis & Investigation Process
Objectives • Clarify why incident investigations are needed
• To provide guidance and awareness on incident investigations to identify
root causes
• Highlight the importance of learning from incidents
• Encourage you to review and enhance your existing procedures for incident investigation
• Drive improvement in JIG HSSE performance
What is the Key Reason For Conducting Incident Investigations ?
Protect people and our
environment Manage losses
Comply with regulatory
requirements
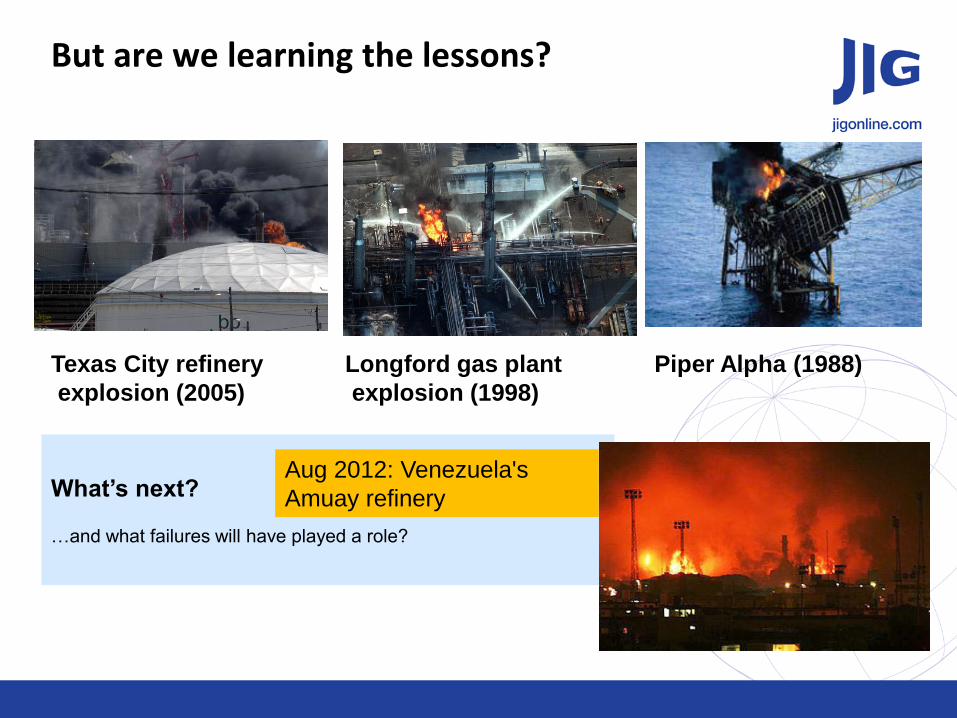
But are we learning the lessons?
What’s next?
…and what failures will have played a role?
Texas City refinery
explosion (2005)
Longford gas plant
explosion (1998)
Piper Alpha (1988)
Aug 2012: Venezuela's
Amuay refinery
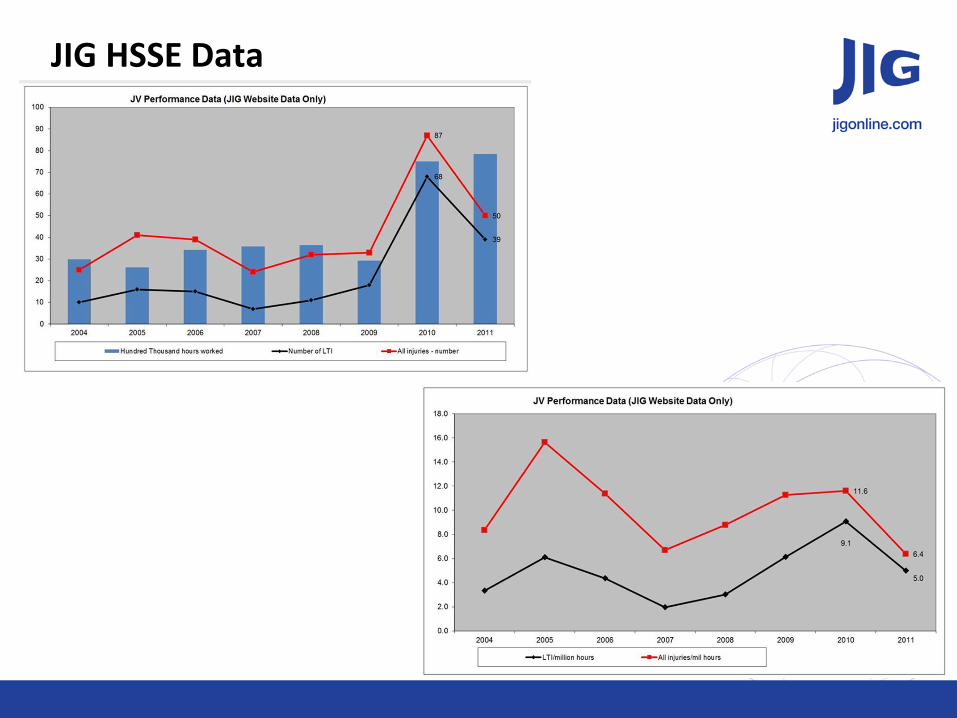
JIG HSSE Data
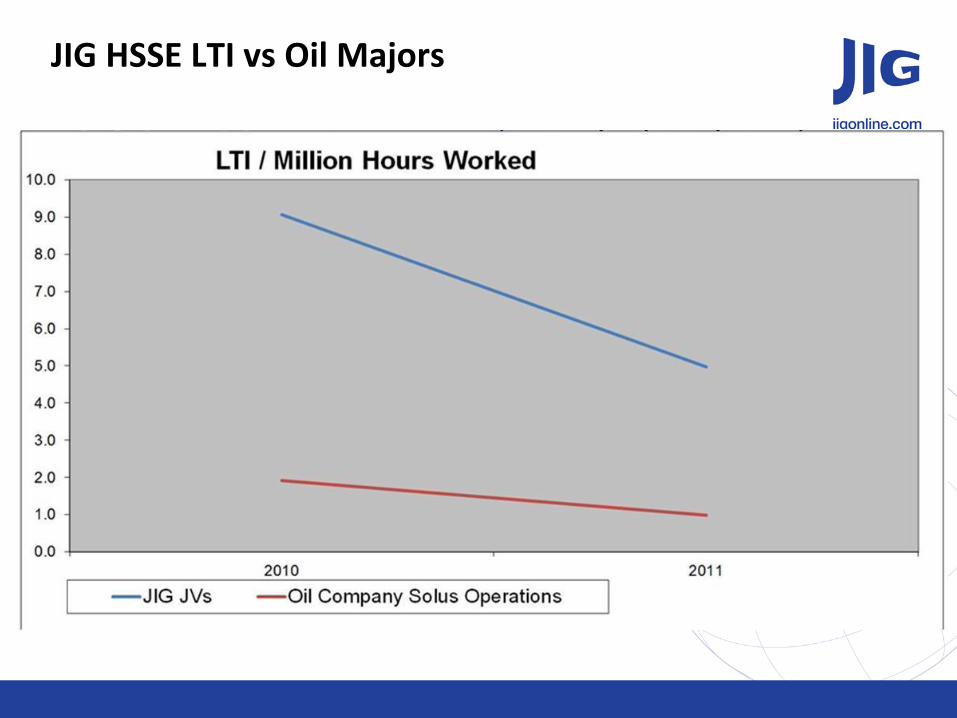
JIG HSSE LTI vs Oil Majors
Incident Investigations
An incident investigation is an after the fact reaction to an unfortunate event.
By determining the Root Cause and contributing factors, steps can be implemented through use of
policy, procedures, and training to avoid future occurrences.
The goal of the investigation is prevention and learning, not to place blame!
Causation
Remember these three basic facts:
Incidents are caused.
Incidents can be prevented if the causes are eliminated.
Unless the causes are eliminated, the same incidents will happen again.
Usually there are four or five root causes or factors that contribute to an incident. Often there are even more.
Your task, if asked to investigate an incident, is to identify as many as possible.
JIG Standards and Incident Investigation
Section 8.10.3 Section 8.10.3 Section 11.10.3 Section 2.3
See also HSSE Management System Requirements - Section 10
What is an Incident Investigation?
Perform a systematic examination
Determine (find) the facts
Identify the immediate, underlying causes (Root Causes)
Develop proposals for corrective action
Communicate & share learnings
Ensure actions are closed out
A defined process by which we:
Symptom Approach
“Errors are often the result of carelessness”.
“We need to train and motivate workers to be more careful.”
“We don’t have the time or resources to really get to the bottom of this problem.”
Root Cause Approach
Errors are the result of defects in the system. People are only part of the process.
We need to find out why this is happening and
implement corrective actions so it won’t happen again.
This is critical. We need to fix it for good or it will
come back and bite us.
Why find Underlying / Root Cause(s) ?

Incident Investigation - Process Steps
1) Preparation • Consider what might have gone wrong:
• Organisational issues • People • Technology • Environment
• Establish an investigation team with appropriate skills and training
2) Investigation Activities • Site Visit / Physical Inspection • Interviews • Document Research • Re-enactments or Modeling
3) Analysis • Determination of Causes
• Immediate • Underlying • Root
4) Reporting • Assemble Report and/or Update
Incident Record • Develop Corrective Actions • Develop & Communicate LFI
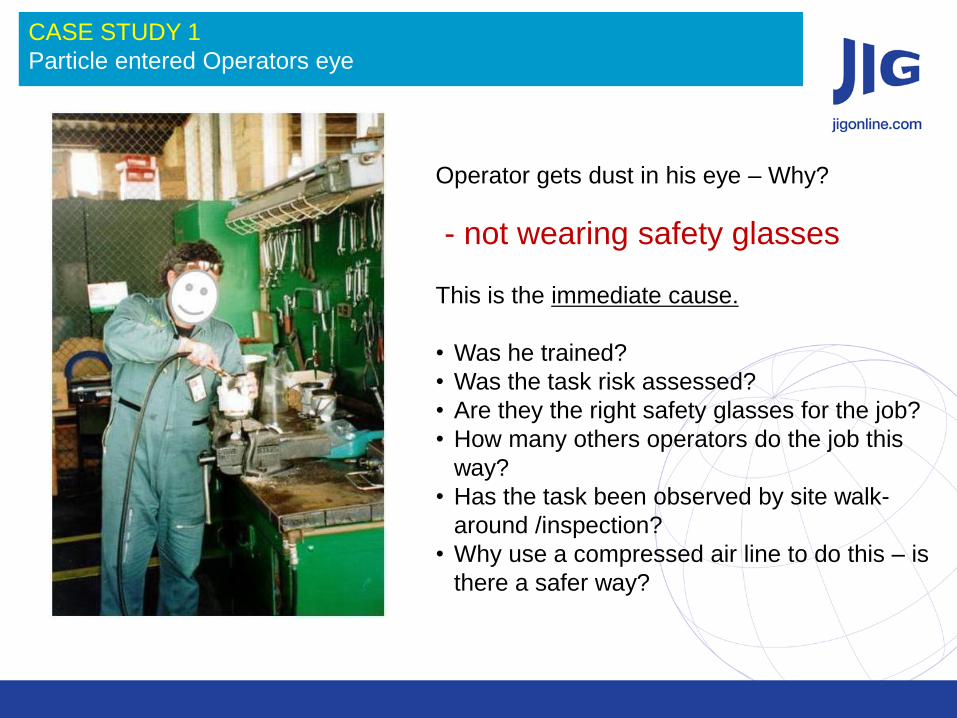
- not wearing safety glasses
This is the immediate cause.
• Was he trained?
• Was the task risk assessed?
• Are they the right safety glasses for the job?
• How many others operators do the job this
way?
• Has the task been observed by site walk-
around /inspection?
• Why use a compressed air line to do this – is
there a safer way?
CASE STUDY 1
Particle entered Operators eye
Operator gets dust in his eye – Why?

Processes to Support Incident Investigation
Fishbone Diagram
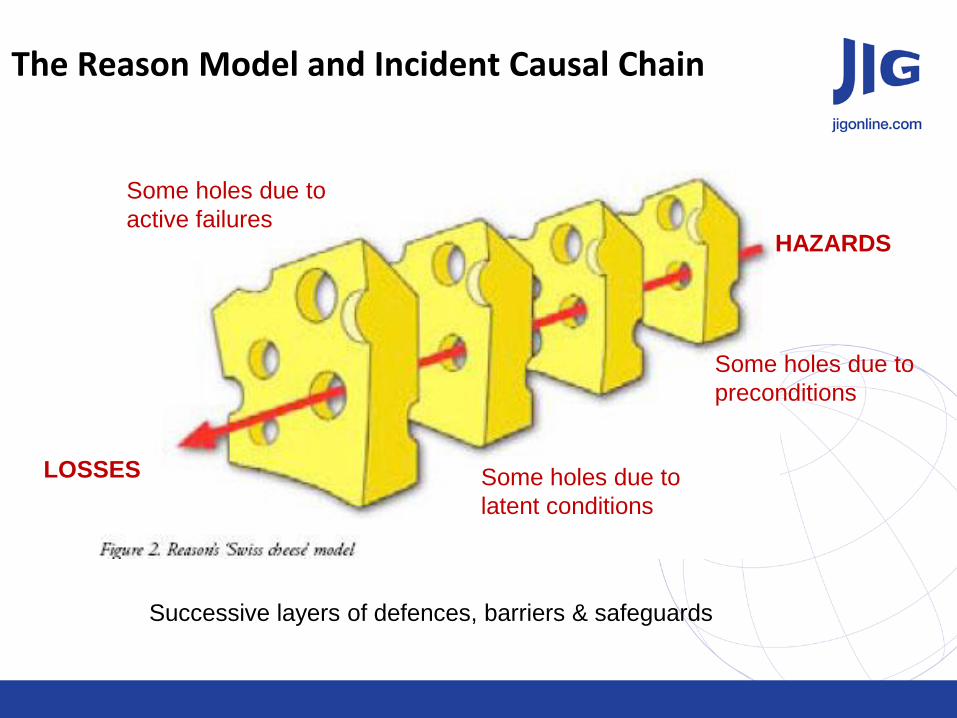
The Reason Model and Incident Causal Chain
Successive layers of defences, barriers & safeguards
HAZARDS
LOSSES
Some holes due to
active failures
Some holes due to
latent conditions
Some holes due to
preconditions
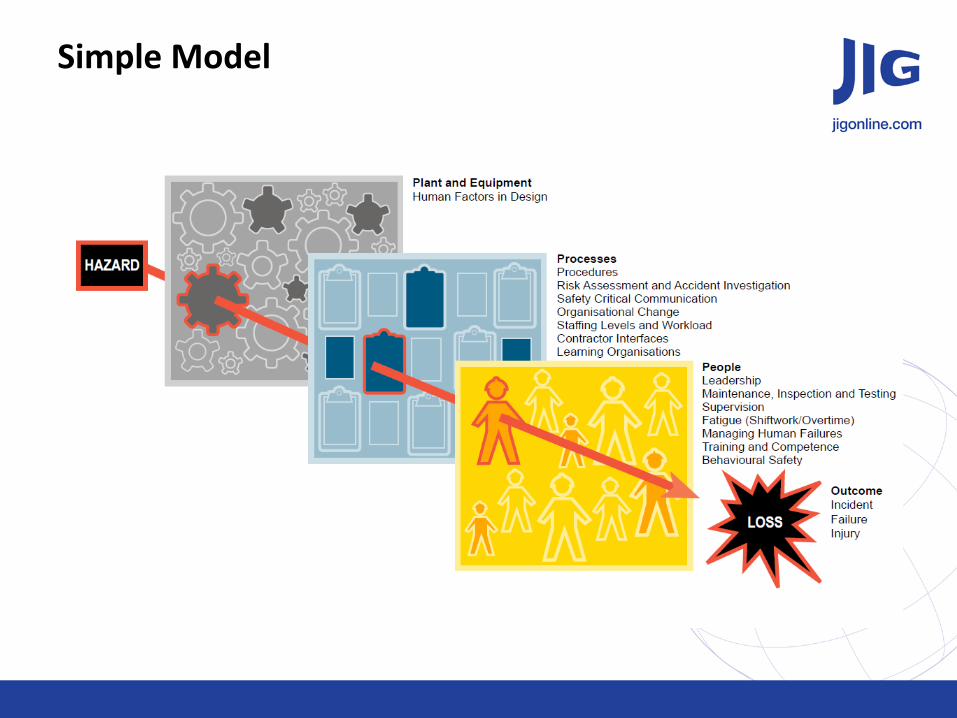
Simple Model
Investigation Traps
Put your emotions aside! - Don’t let your feelings interfere - stick to the facts!
Do not pre-judge. - Find out the what really happened. - Do not let your beliefs cloud the facts.
Never assume anything. Do not make any judgments.
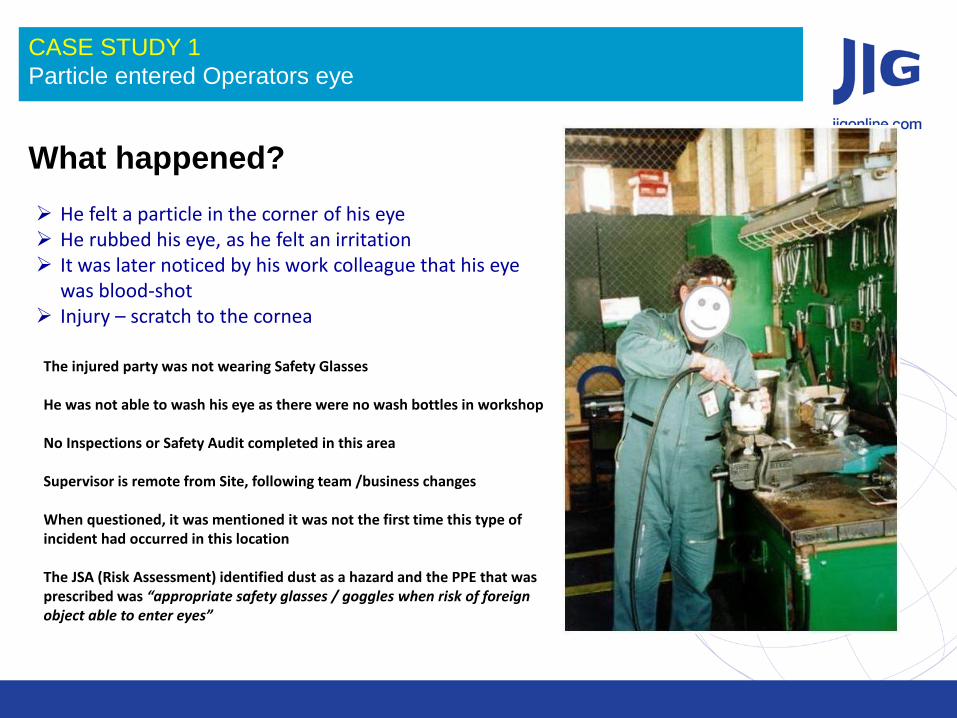
CASE STUDY 1
Particle entered Operators eye
What happened?
He felt a particle in the corner of his eye He rubbed his eye, as he felt an irritation It was later noticed by his work colleague that his eye
was blood-shot Injury – scratch to the cornea
The injured party was not wearing Safety Glasses He was not able to wash his eye as there were no wash bottles in workshop No Inspections or Safety Audit completed in this area Supervisor is remote from Site, following team /business changes When questioned, it was mentioned it was not the first time this type of incident had occurred in this location The JSA (Risk Assessment) identified dust as a hazard and the PPE that was prescribed was “appropriate safety glasses / goggles when risk of foreign object able to enter eyes”
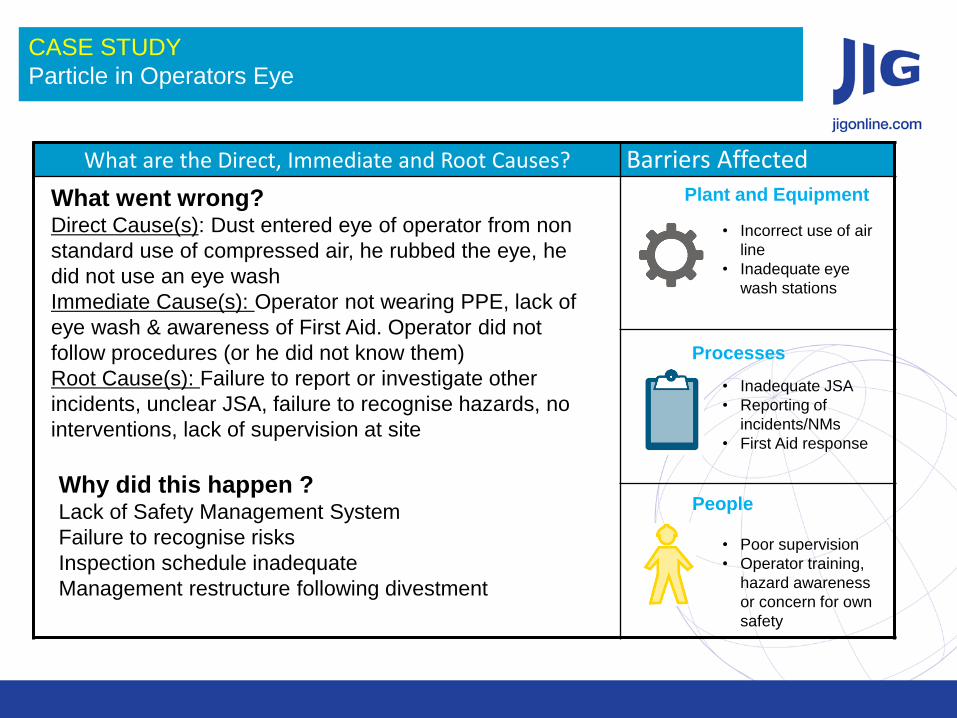
What are the Direct, Immediate and Root Causes? Barriers Affected
What went wrong? Direct Cause(s): Dust entered eye of operator from non
standard use of compressed air, he rubbed the eye, he
did not use an eye wash
Immediate Cause(s): Operator not wearing PPE, lack of
eye wash & awareness of First Aid. Operator did not
follow procedures (or he did not know them)
Root Cause(s): Failure to report or investigate other
incidents, unclear JSA, failure to recognise hazards, no
interventions, lack of supervision at site
Why did this happen ? Lack of Safety Management System
Failure to recognise risks
Inspection schedule inadequate
Management restructure following divestment
Plant and Equipment
Processes
People
CASE STUDY
Particle in Operators Eye
• Incorrect use of air
line
• Inadequate eye
wash stations
• Inadequate JSA
• Reporting of
incidents/NMs
• First Aid response
• Poor supervision
• Operator training,
hazard awareness
or concern for own
safety
Group Exercise – Let’s look at Case 2 to 7
Description of exercise: In Groups, review the incidents and the data given. Discuss in your group, and fill out the incident cause table.
Process:
1. Examine the incident given, use the data to identify the
• Direct Cause
• Immediate Cause
• Root Cause
2. Assigned the failed barriers
3. What can we learn from this incident?
Be prepared to feedback (nominate a 1 person to feedback)
Group Exercise – Let’s look at Case 2 to 7
Group Case Study
2 2
3 3
4 4
5 5
6 6
7 7
Incident Investigation - Final Check
Investigation Report – Final Check
Fact
Are all relevant facts captured…
Causes
Underlying causes established…
Corrective Action
“SMART” Corrective Actions linked to
causes…
Final Health Check
Would the incident still happen if
corrective actions are in place?
Specific Is it clear what has to be done & by
whom?
Measurable Will we know when it has been done?
Achievable
Is it possible?
Realistic Can we afford it?
Timely Is there a completion deadline?
Learning From Incidents – JIG LFIs
Learning From Incidents – How?
• Need a way of sharing learning that drives behavioural change and
sustained learning
• Need to provide people with the time and space to think about the
causes of an incident and what they need to do prevent this
happening at their workplace
• Research shows that sharing learning via small group, face-to-face
discussions, with video footage of an incident, is more than 5 times
effective than just reading an LFI Alert (see next slide)

Learning From Incidents – Best method?
Questions Incidents / Investigations / LFI?
Back Up Slides
Case Studies for Exercises
• CASE STUDY 2 Contractor cut Wrong Pipe
• CASE STUDY 3 Hot Work Fatality
• CASE STUDY 4 Lost Workday case resulting from tripping over hose
• CASE STUDY 5 Lost Workday case resulting from pulling a hose
• CASE STUDY 6 MVI – Catering truck collided with Fueller
• CASE STUDY 7 - Finger Injury whilst lifting Hydrant Pit cover
CASE STUDY 2
Contractor cut Wrong Pipe
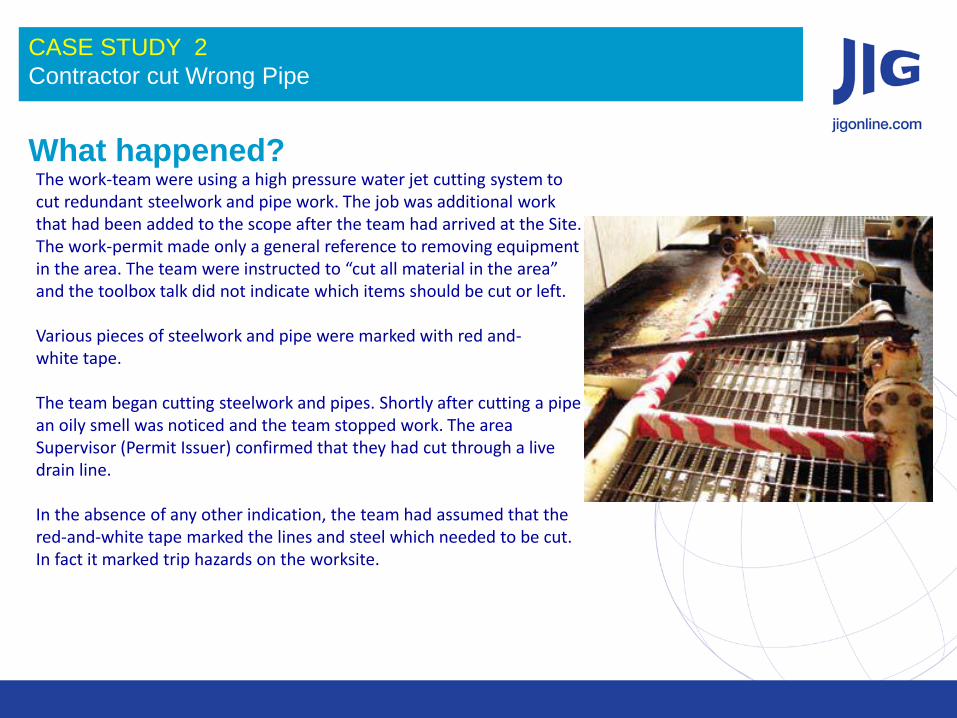
What happened? The work-team were using a high pressure water jet cutting system to cut redundant steelwork and pipe work. The job was additional work that had been added to the scope after the team had arrived at the Site. The work-permit made only a general reference to removing equipment in the area. The team were instructed to “cut all material in the area” and the toolbox talk did not indicate which items should be cut or left. Various pieces of steelwork and pipe were marked with red and- white tape. The team began cutting steelwork and pipes. Shortly after cutting a pipe an oily smell was noticed and the team stopped work. The area Supervisor (Permit Issuer) confirmed that they had cut through a live drain line. In the absence of any other indication, the team had assumed that the red-and-white tape marked the lines and steel which needed to be cut. In fact it marked trip hazards on the worksite.
CASE STUDY 3
Hot Work Fatality
What happened?
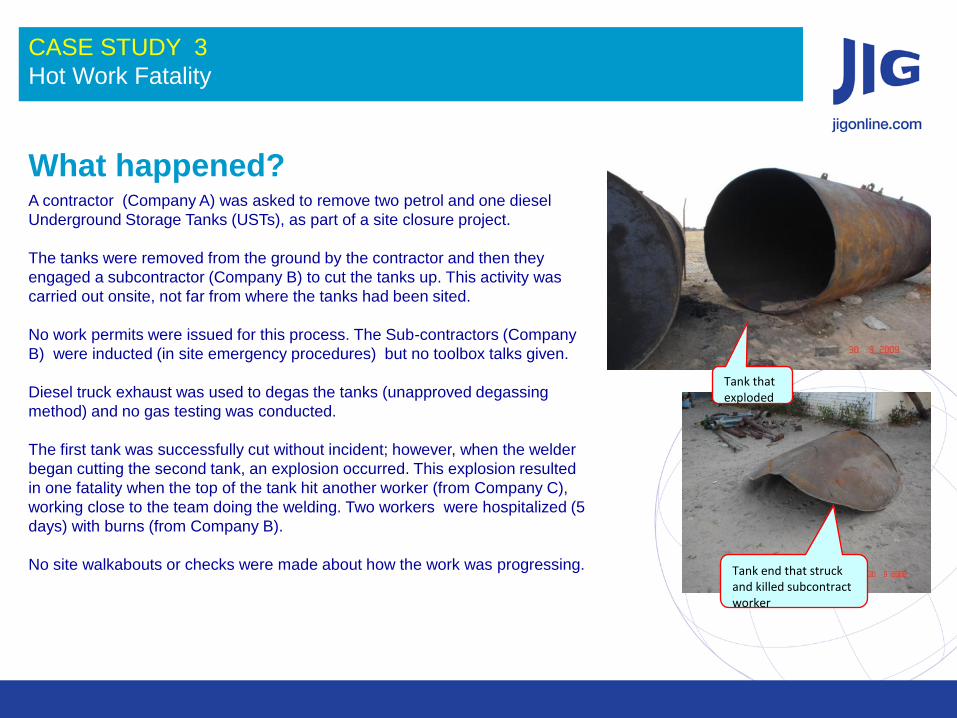
Tank that exploded
Tank end that struck and killed subcontract worker
A contractor (Company A) was asked to remove two petrol and one diesel
Underground Storage Tanks (USTs), as part of a site closure project.
The tanks were removed from the ground by the contractor and then they
engaged a subcontractor (Company B) to cut the tanks up. This activity was
carried out onsite, not far from where the tanks had been sited.
No work permits were issued for this process. The Sub-contractors (Company
B) were inducted (in site emergency procedures) but no toolbox talks given.
Diesel truck exhaust was used to degas the tanks (unapproved degassing
method) and no gas testing was conducted.
The first tank was successfully cut without incident; however, when the welder
began cutting the second tank, an explosion occurred. This explosion resulted
in one fatality when the top of the tank hit another worker (from Company C),
working close to the team doing the welding. Two workers were hospitalized (5
days) with burns (from Company B).
No site walkabouts or checks were made about how the work was progressing.
CASE STUDY 4
Lost Workday case resulting from tripping over hose
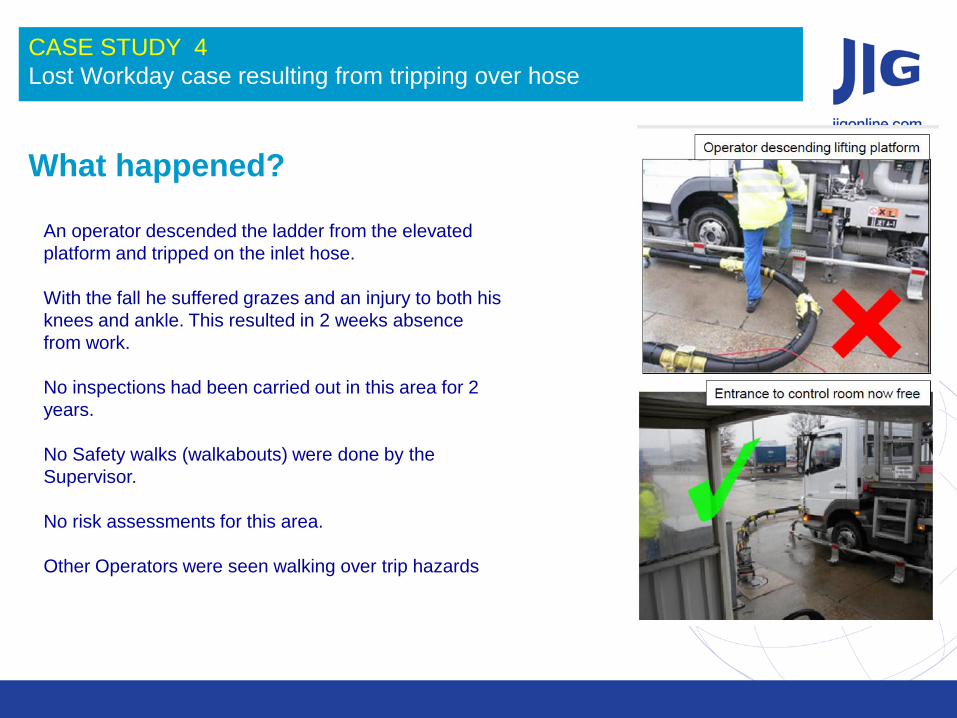
What happened? An operator descended the ladder from the elevated
platform and tripped on the inlet hose.
With the fall he suffered grazes and an injury to both his
knees and ankle. This resulted in 2 weeks absence
from work.
No inspections had been carried out in this area for 2
years.
No Safety walks (walkabouts) were done by the
Supervisor.
No risk assessments for this area.
Other Operators were seen walking over trip hazards
CASE STUDY 5
Lost Workday case resulting from pulling a hose
What happened?
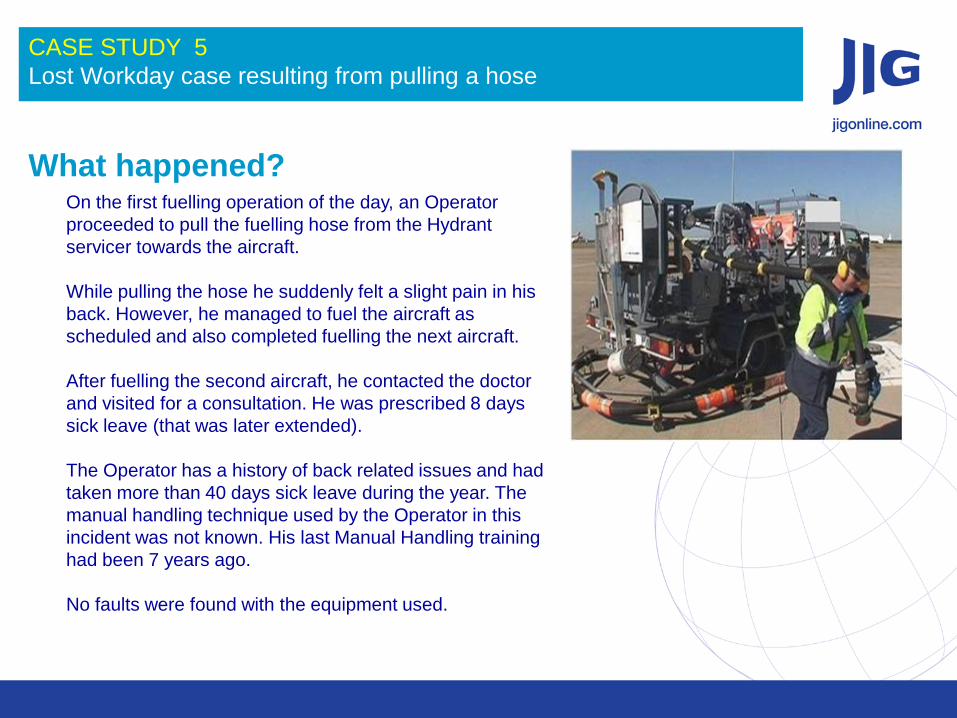
On the first fuelling operation of the day, an Operator
proceeded to pull the fuelling hose from the Hydrant
servicer towards the aircraft.
While pulling the hose he suddenly felt a slight pain in his
back. However, he managed to fuel the aircraft as
scheduled and also completed fuelling the next aircraft.
After fuelling the second aircraft, he contacted the doctor
and visited for a consultation. He was prescribed 8 days
sick leave (that was later extended).
The Operator has a history of back related issues and had
taken more than 40 days sick leave during the year. The
manual handling technique used by the Operator in this
incident was not known. His last Manual Handling training
had been 7 years ago.
No faults were found with the equipment used.
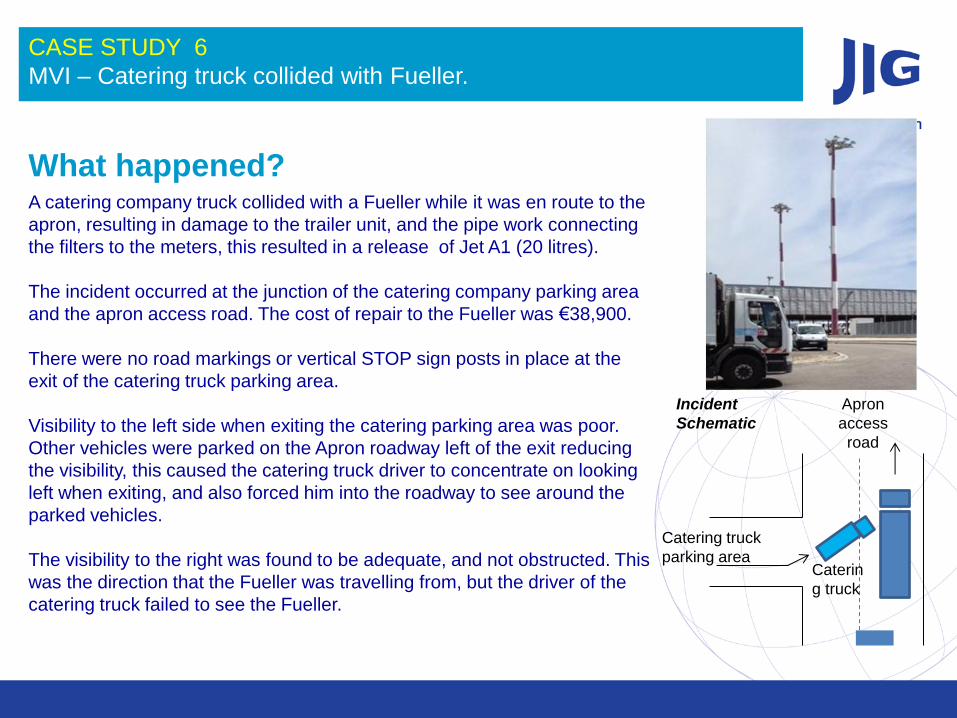
CASE STUDY 6
MVI – Catering truck collided with Fueller.
What happened?
Hose & Coupling
Catering truck
parking area Caterin
g truck
Apron
access
road
Incident
Schematic
A catering company truck collided with a Fueller while it was en route to the
apron, resulting in damage to the trailer unit, and the pipe work connecting
the filters to the meters, this resulted in a release of Jet A1 (20 litres).
The incident occurred at the junction of the catering company parking area
and the apron access road. The cost of repair to the Fueller was €38,900.
There were no road markings or vertical STOP sign posts in place at the
exit of the catering truck parking area.
Visibility to the left side when exiting the catering parking area was poor.
Other vehicles were parked on the Apron roadway left of the exit reducing
the visibility, this caused the catering truck driver to concentrate on looking
left when exiting, and also forced him into the roadway to see around the
parked vehicles.
The visibility to the right was found to be adequate, and not obstructed. This
was the direction that the Fueller was travelling from, but the driver of the
catering truck failed to see the Fueller.
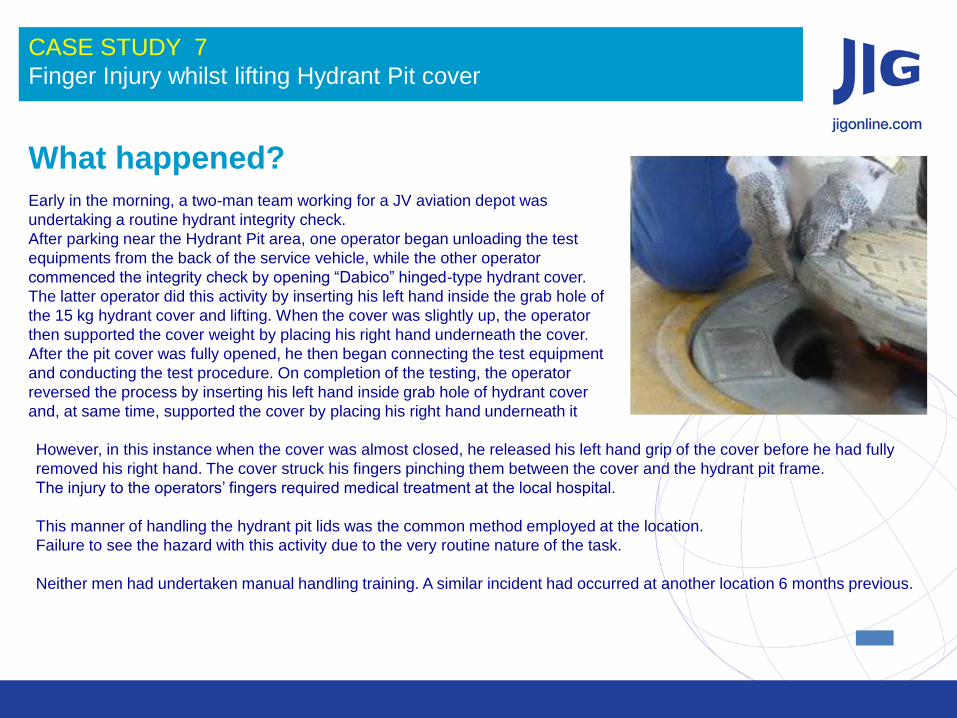
CASE STUDY 7
Finger Injury whilst lifting Hydrant Pit cover
What happened?
Early in the morning, a two-man team working for a JV aviation depot was
undertaking a routine hydrant integrity check.
After parking near the Hydrant Pit area, one operator began unloading the test
equipments from the back of the service vehicle, while the other operator
commenced the integrity check by opening “Dabico” hinged-type hydrant cover.
The latter operator did this activity by inserting his left hand inside the grab hole of
the 15 kg hydrant cover and lifting. When the cover was slightly up, the operator
then supported the cover weight by placing his right hand underneath the cover.
After the pit cover was fully opened, he then began connecting the test equipment
and conducting the test procedure. On completion of the testing, the operator
reversed the process by inserting his left hand inside grab hole of hydrant cover
and, at same time, supported the cover by placing his right hand underneath it
However, in this instance when the cover was almost closed, he released his left hand grip of the cover before he had fully
removed his right hand. The cover struck his fingers pinching them between the cover and the hydrant pit frame.
The injury to the operators’ fingers required medical treatment at the local hospital.
This manner of handling the hydrant pit lids was the common method employed at the location.
Failure to see the hazard with this activity due to the very routine nature of the task.
Neither men had undertaken manual handling training. A similar incident had occurred at another location 6 months previous.
What are the direct, immediate and underlying causes? Barriers (controls) affected
What went wrong?
Why did this happen ?
Plant and Equipment
Processes
People
CASE STUDY #
Incident _________________________
What can we learn from this incident?
CASE STUDY #
Incident _________________________