health professions council standards of proficiency for
TRANSCRIPT
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Cover sheet - QAA benchmarks -
04.09.2007 Draft DD: None
Public RD: None
Health Professions Council Standards of Proficiency for Applied Psychologists Professional Liaison Group (PLG) Quality Assurance Agency Subject Benchmark Statements Executive Summary and Recommendations Introduction Subject benchmark statements are produced by the Quality Assurance Agency (QAA) and set out expectations about standards of degrees in specific subject areas. They articulate what can be expected of a graduate in terms of the abilities and skills needed to develop understanding in the specific subject. Benchmark statements are currently available in clinical psychology. The benchmarks for clinical psychology produced by the QAA and QAA Scotland are appended, together with a document which maps the benchmarks (QAA) against the generic standards. This document identifies areas where profession-specific standards might be helpful or necessary or where further discussion and consideration is required. Decision The group is invited to discuss the attached documents. Background information Subject benchmark statements are available from the Quality Assurance Agency’s website: www.qaa.ac.uk. Resource implications None Financial implications None Appendices Appendix 1: Quality Assurance Agency subject benchmark statement for Clinical Psychology (2004) Appendix 2: Quality Assurance Agency Scotland Scottish subject benchmark statement for Clinical Psychology and Applied Psychology (clinical associate) Scotland

Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Cover sheet - QAA benchmarks -
04.09.2007 Draft DD: None
Public RD: None
Appendix 3: Mapping of Mapping of Quality Assurance Agency subject benchmark statement for Clinical Psychology (appendix 1) against the generic standards of proficiency. Date of paper 21st August 2007
Benchmark statement:Health care programmes
Phase 2

ISBN 1 84482 145 5© Quality Assurance Agency for Higher Education 2004
All the Agency's publications are available on our web site www.qaa.ac.uk
Printed copies are available from:Linney DirectAdamswayMansfieldNG18 4FN
Tel 01623 450788Fax 01623 450629Email [email protected]

Clinical psychology

Subject benchmark statements: Health care programmes
Subject benchmark statements provide a means for the academic community to describe the nature andcharacteristics of programmes in a specific subject. They also represent general expectations about standardsfor the award of qualifications at a given level and articulate the attributes and capabilities that thosepossessing such qualifications should be able to demonstrate.
This subject benchmark statement refers to the degree of doctorate in clinical psychology.
Subject benchmark statements are used for a variety of purposes. Primarily, they are an important externalsource of reference for higher education institutions when new programmes are being designed anddeveloped in a subject area. They provide general guidance for articulating the learning outcomes associatedwith the programme but are not a specification of a detailed curriculum in the subject. Subject benchmarkstatements provide for variety and flexibility in the design of programmes and encourage innovation withinan agreed overall conceptual framework.
Subject benchmark statements also provide support to institutions in the pursuit of internal qualityassurance. They enable the learning outcomes specified for a particular programme to be reviewed andevaluated against agreed general expectations about standards.
Finally, subject benchmark statements may be one of a number of external reference points that are drawnupon for the purposes of external review. Reviewers do not use subject benchmark statements as a crudechecklist for these purposes however. Rather, they are used in conjunction with the relevant programmespecifications, the institution's own internal evaluation documentation, in order to enable reviewers to cometo a rounded judgement based on a broad range of evidence.
The benchmarking of academic standards for this subject area has been undertaken by a group of subjectspecialists.
In due course, the statement will be revised to reflect developments in the subject and the experiences ofinstitutions, and others who are working with it.
Contents
Foreword 1
Benchmark statement for clinical psychology 2
Introduction 2
Clinical psychologists as scientist practitioners 3
Clinical psychologists as reflective practitioners 3
Use of clinical psychology services 3
Clinical psychology programmes and maintenance of professional standards 4
Standards for awards 5
A The chartered clinical psychologist as a health care practitioner: Expectations held by the profession, employers and the public 5
B The application of clinical psychology practice in securing, maintaining or improving health and well-being 6
C Knowledge, understanding and skills that underpin the education and training of clinical psychologists 7
Teaching, learning and assessment 9
Academic and practitioner standards 11
Appendix 1 12
Clinical psychology benchmark group membership 12
Appendix 2 13
Benchmarking steering group membership 13

page 1
Foreword
This benchmark statement describes the nature and standards of programmes of study in clinical psychologythat lead to awards made by higher education institutions (HEIs) in the United Kingdom (UK) in the subject.It sets out a general framework for describing these programmes under three main categories.
A Expectations of the health professional in providing patient/client services;
B The application of practice in securing, maintaining or improving health and well-being;
C The knowledge, understanding and skills that underpin the education and training of health careprofessionals.
This represents the shared context upon which the education and training of all health care professionalsrests. It is important to emphasise that benchmark statements will continue to evolve in the light ofexperience and further developments in health care.
The main section of this statement, in addition to describing the nature and extent of programmes leading toawards in clinical psychology, describes the profession-specific expectations and requirements under the samethree categories, but emphasises that as a postgraduate qualification clinical psychology education and trainingbuilds upon the prerequisite knowledge and skills gained from the undergraduate degree in psychology.
The section on standards accords with the relevant level descriptor for awards in the qualificationsframeworks published by the Quality Assurance Agency for Higher Education.
The section on teaching, learning and assessment draws attention to the key role of practice in the design ofclient-centred learning opportunities for trainees, and to the importance of ensuring that professionalcompetence, developed through practice, is adequately assessed and rewarded. It also notes how essential itis that the integration of theory and practice is a planned process within the overall arrangements made forteaching and learning. The importance of professional accountability teamworking, interprofessionalcollaboration and communication are also emphasised.
Finally, the statement does not set a national curriculum for programmes leading to awards in clinicalpsychology. It acknowledges that the requirements of the professional and statutory regulatory bodies needto be incorporated into the design of programmes. It seeks to encourage HEIs and service providers to workcollaboratively in the design and delivery of their curricula. Its essential feature is the specification ofthreshold standards, incorporating academic and practitioner elements, against which HEIs are expected, asa minimum, to set their standards for the award.
Clinical psychology

page 2
Benchmark statement for clinical psychology
Introduction
Philosophy
The work of clinical psychologists is based on the fundamental acknowledgement that all people have thesame human value and the right to be treated as unique individuals. Clinical psychologists will treat allpeople - both clients and colleagues - with dignity and respect and will work with them collaboratively aspartners towards the achievement of mutually agreed goals. In doing this, clinical psychologists will adhereto, and be guided by, explicit and public statements of the ethical principles that underpin their work.
Purpose
Clinical psychology aims to reduce psychological distress and to enhance and promote psychological well-being by the systematic application of knowledge derived from psychological theory and research.
Aims
Clinical psychology services aim to enable service users to have the necessary skills and abilities to cope withtheir emotional needs and daily lives in order to maximise psychological and physical well-being; to developand use their capacity to make informed choices in order to enhance and maximise independence andautonomy; to have a sense of self-understanding, self-respect and self-worth; to be able to enjoy good socialand personal relationships; and to access commonly valued social and environmental facilities.
Clinical psychology services aim to enable other service providers to develop psychologically-informed waysof thinking; to use psychological knowledge to enhance and develop their professional practice to the benefitof their clients; to be able to enhance their sense of self-understanding, self-respect and self-worth; and to usepsychological data to aid decision-making at a clinical, organisational and societal level.
How these aims are achieved
The core skills of a clinical psychologist are:
assessment;
formulation;
intervention;
evaluation and research;
communication.
Assessment of psychological processes and behaviour is a competence derived from the theory and practiceof both academic and applied psychology. It is different from other activities such as diagnosis and includesboth assessing individual change and stability and comparing the individual with others. Assessmentprocedures include:
the development and use of psychometric tests;
the application of systematic observation and measurement of behaviour in both daily life contexts andother settings;
devising self-monitoring strategies for individual service users;
the use of formal and informal interviews with clients, carers and other professionals.
Results of these assessments are integrated within the context of the historical and developmental processes thatwill have shaped either an individual, family, group or organisation. Clinical psychologists have the ability toassess the suitability of different measurement procedures depending on the purpose for which the assessmentis needed, as well as being competent to devise and use one-off, individualised assessment procedures.
Formulation is the summation and integration of the knowledge that is acquired by this assessment process(which may involve a number of different procedures). This will draw on psychological theory and researchto provide a framework for describing a problem, how it developed and is being maintained. Because oftheir particular training in the linkage of theory to practice, clinical psychologists will be able to draw on a
Subject benchmark statement: Health care programmes

page 3
number of different explanatory models and so a formulation may comprise a number of provisionalhypotheses. This process provides the foundation from which actions derive. What makes this activityunique to clinical psychologists is the knowledge base and information on which they draw. The ability to access, review, critically evaluate, analyse and synthesise data and knowledge from a psychologicalperspective is one that is distinct to psychologists, both academic and applied.
Intervention, if appropriate, is based on the formulation. This may involve the utilisation of one or morepsychotherapeutic models or approaches to facilitate change. Other sorts of intervention may includetraining of others (professional staff, relatives and carers), the provision of psychological knowledge byteaching or the development of psychological skills through supervision and consultation. All theseinterventions are tests of the provisional hypotheses contained in the formulation and are subject tomodification in the light of experience and new data.
Evaluation is, therefore, a critical and integral part of the clinical psychologist's work. All activities andinterventions need to be evaluated both during their implementation and afterwards to assess the stabilityand security of change. Research includes the ongoing evaluation of assessment, formulation andintervention in relation to specific services provided. It also includes explorations of psychological processesand outcomes (basic research), the development and evaluation of specific psychological interventions(primary research) and the consolidation and evaluation of primary research (secondary research). Basic andprimary research in clinical psychology is typically uni-professional; secondary research is more usuallyconducted in collaboration with other professionals.
Communication skills are clearly integral to all aspects of a clinical psychologist's role. Effectivecommunication skills are routinely essential in relation to all aspects of work with service users and theirfamilies and with other professional staff. Communication skills include direct face to face communication,all forms of electronic and verbal communication to individual clients, their families and other key people,and the dissemination of research.
In summary, it is the mixture and synthesis of competencies, built on the body of psychological theory anddata, which are applied to helping people solve personal, family, group, work or organisational problems,that makes clinical psychology unique in health and social care.
Clinical psychologists as scientist practitioners
Clinical psychologists are more than psychological therapists. While many do practise psychotherapy at ahigh level, this is not a skill distinct to clinical psychologists, nor should it be. The background and trainingof clinical psychologists is rooted in the science of psychology, and clinical psychology is one of theapplications of psychological science to help address human problems. The ability to design and carry outinnovative applied research is a skill developed to a doctoral level in training and is important for thedevelopment and delivery of evidence-based practice. In addition, one element of research competence iscritical evaluation of research activity. While there are data that support many clinical activities, there are still major gaps in the knowledge base. One of the contributions made by clinical psychologists is thedevelopment and testing of new interventions and activities, based on psychological theory. Thus practicefeeds and draws on research and theory that in turn influences practice.
Clinical psychologists as reflective practitioners
Clinical psychologists are cognisant of the importance of self-awareness and the need to appraise and reflect ontheir own practice. They are also aware of the importance of diversity, the social and cultural context of theirwork, working within an ethical framework, and the need for continuing professional and personal development.
Use of clinical psychology services
Clinical psychologists work with individuals, couples, families, groups (therapeutic, staff, informal carers)and at the organisational and community level. They work in a variety of settings, including hospital wards,day centres, Community Mental Health Teams, NHS Trusts, primary and social care contexts and forensicsettings, and with all age groups from very young children to older people. They work with people withmild, moderate and severe mental health problems, developmental and learning disabilities, physical andsensory disability, and brain injury; people who have substance misuse problems and people with a range ofphysical health problems (eg HIV and AIDS, cancer, heart disease, pain, diabetes).
Clinical psychology

page 4
Clinical psychology programmes and maintenance of professional standards
Entry to training requires the Graduate Basis for Registration as defined by The British Psychological Society.The prerequisite undergraduate degree provides an education that develops a knowledge frameworkencompassing basic theory and scientific principles (and the limits of such theory and principles) in thedomains of human behaviour, experience and interaction.
Programmes are delivered at postgraduate level in accordance with the frameworks for higher educationqualifications produced by the Quality Assurance Agency for Higher Education. As applied to clinicalpsychology, this means that newly qualified individuals will be able to make informed judgements oncomplex clinical and research problems, often in the absence of complete information, and are able tocommunicate their ideas and conclusions clearly and effectively to specialist and non-specialist audiences.These will be based on a systematic understanding of a substantial body of knowledge that is at the forefrontof the discipline and profession of clinical psychology. Newly qualified individuals will have contributed tothe creation and development of new knowledge and be able to continue to undertake applied research anddevelopment at an advanced level. They will have the qualities and transferable skills necessary foremployment, requiring the exercise of personal responsibility and be largely autonomous in taking theinitiative in complex and unpredictable clinical situations.
Training should encompass theoretical, research and applied foundations of psychology applied to thediverse range of needs of people in the health, social care and educational settings. All programmes providea generic training, enabling graduates to work with a wide range of clients. Training takes place over threeyears of full-time study at the end of which successful candidates are awarded a doctorate of clinicalpsychology, and are eligible for registration. Chartered psychologists agree to abide by The BritishPsychological Society Code of Conduct and can be removed from the register for breaches of this Code. TheBritish Psychologist Society has a formal disciplinary process with representation of both non-psychologistsand senior and experienced psychologists.
Subject benchmark statement: Health care programmes

page 5
Standards for awards
A The chartered clinical psychologist as a health care practitioner: Expectations held by the profession, employers and public
A1 Professional autonomy and accountability of the clinical psychologist
The award holder should be able to:
maintain the standards and requirements of The British Psychological Society and the Division ofClinical Psychology (DCP);
adhere to The British Psychological Society's Code of Conduct, ethical principles and guidelines and theDCP Professional Practice Guidelines;
understand the legal and ethical responsibilities of clinical psychology practice including patient consentand confidentiality;
demonstrate awareness of the legislative and national planning context of service delivery and clinicalpsychology practice;
recognise the obligation to maintain fitness for practice and the need for continuing professionaldevelopment;
contribute to the development and dissemination of evidence-based practice within professional contexts;
recognise and cope with uncertainty, making informed judgements on complex clinical issues in theabsence of complete data;
make appropriate clinical decisions.
A2 Professional relationships
The award holder should be able to:
participate effectively in interprofessional and multi-agency approaches to health and social care;
recognise professional scope of practice and make referrals, where appropriate;
demonstrate understanding of consultancy models and the contribution of consultancy to practice;
work with others to deliver effective health care;
understand the impact of difference, diversity and social inequalities on people's lives, and itsimplications for working practices;
work effectively with users and carers to facilitate their involvement in service planning and delivery;
maintain appropriate records and make accurate reports.
A3 Personal and professional skills
The award holder should be able to:
demonstrate the ability to deliver high quality patient/client-centred care both as a solo practitioner andas a member of multidisciplinary and multi-agency teams;
practise in an anti-discriminatory, anti-oppressive manner;
draw upon clinical psychology knowledge, theory and skills in order to make professional judgements;
demonstrate high levels of research skills and scholarship;
work effectively at a high level of autonomy in complex and unpredictable situations, with awareness of thelimits of their own competence, and accepting accountability to relevant professional and service managers;
demonstrate self-awareness and ability to work as a reflective practitioner;
demonstrate a high level of communication skills in a style appropriate to specialist and non-specialistaudiences;
initiate and respond to change in a flexible manner, demonstrating transferable skills;
Clinical psychology
page 6
understand the importance and role of continuing professional development and engage in self-directedlearning that promotes professional development;
manage the emotional and physical impact of their own practice;
understand the importance and role of supervision and demonstrate its appropriate use;
demonstrate self-management skills and independence of thought and action;
demonstrate culturally competent practice.
A4 Profession and employer context
The award holder should be able to:
show an understanding of the role of the clinical psychologist within health and social care services;
adapt clinical psychology practice to a range of organisational contexts, on the basis of an understandingof pertinent organisational and cultural issues;
contribute to the development of the profession's responsibility to the NHS through teaching, researchsupervision and training of psychologists and other professionals;
take responsibility for their own professional development;
demonstrate an ability to contribute to team management and functioning;
participate in the development of new services;
recognise the value of research and other scholarly activity in relation to the development of theprofession and of patient/client care.
B The application of clinical psychology practice in securing, maintaining or improving health and well-being
Clinical psychology practice and the application of professional skills are underpinned by psychologicaltheory, evidence and understanding. The qualified clinical psychologist possesses a broad range of core skillsencompassing profession-specific and generic enabling skills.
Profession-specific skills
Sound clinical psychology practice is based on clinical and research skills that demonstrate work with clientsand systems based on a scientist practitioner and reflective practitioner model. This incorporates a cycle ofassessment, formulation, intervention and evaluation. Hence, clinical psychologists can generalise andsynthesise prior knowledge and experience in order to apply them in different settings and novel situations.They are able to think critically about, reflect upon and evaluate such knowledge and experience within aframework of evidence-based practice.
Psychological assessment
Developing and maintaining effective working alliances with clients, including individuals, families,carers and services.
Ability to choose, use and interpret a broad range of psychological assessment methods appropriate:
a to the client and service delivery system in which the assessment takes place;
b to the type of intervention which is likely to be required.
Assessment procedures in which competence is demonstrated will include:
a formal procedures (use of standardised instruments);
b systematic interviewing procedures;
c other structured methods of assessment (eg observation or gathering information from others).
Conducting appropriate risk assessment and using this to guide practice.
Subject benchmark statement: Health care programmes

page 7
Psychological formulation
Developing psychological formulations of presenting problems or situations which integrate informationfrom assessments within a coherent framework that draws upon psychological theory and evidence andwhich incorporates interpersonal, societal, cultural and biological factors.
Using formulations with clients to facilitate their understanding of their experience.
Using formulations to plan appropriate interventions that take the client's perspective into account.
Using formulations to assist multiprofessional understanding and communication, and theunderstanding of clients and their care.
Revising formulations in the light of ongoing intervention and when necessary re-formulating the problem.
Psychological intervention
On the basis of a formulation, implementing psychological therapy or other interventions appropriate tothe presenting problem and to the psychological, cultural and social circumstances of the client(s), and todo this in a collaborative manner with:
individuals;
couples, families or groups;
teams/services/organisations.
Implementing and recording interventions through, and with, other professions and/or with individualswho are formal (professional) carers for a client, or who care for a client by virtue of family orpartnership arrangements.
Recognising when (further) intervention is inappropriate, or unlikely to be helpful, and communicatingthis sensitively to clients and carers.
Evaluation and research
Selecting and implementing appropriate methods to evaluate the effectiveness, acceptability and broaderimpact of interventions (both individual and organisational), and using this information to inform andshape practice. Where appropriate, this will also involve devising innovative procedures.
Auditing clinical effectiveness.
Identifying gaps in the evidence base and, where such gaps exist, adapting established practice to meetthe specific needs of service users. In such cases, ongoing evaluation of adaptations is critical and formsthe basis of new developments in theory and practice.
The development of theory and practice in clinical psychology through research.
C Knowledge, understanding and skills that underpin the education and training of clinical psychologists
C1 Knowledge and understanding
The clinical psychology award holder should be able to demonstrate:
systematic acquisition and understanding of a substantial body of knowledge, including theories andevidence concerning psychological development and psychological difficulties across the lifespan andtheir assessment and remediation. This should include theory and evidence at the forefront of thediscipline relating to:
i a wide breadth of presentations - from acute to enduring and from mild to severe;
ii problems ranging from those with mainly biological causation to those emanating mainly from psychosocial factors;
iii problems of coping/adaptation to adverse circumstances that are not themselves reversible bypsychological intervention (eg physical disability, physical illness, bereavement);
iv clients from a range of backgrounds reflecting the demographic characteristics of the population;
Clinical psychology

page 8
v clients with significant levels of challenging behaviour;
vi clients across a range of levels of intellectual functioning over a range of ages;
vii clients whose disability makes it difficult for them to communicate;
viii carers and families;
ix social and contextual factors;
x teamwork, service delivery systems, and the legislative and policy frameworks;
detailed knowledge and understanding of research methods including:
i research design and methods including small N designs and those methods, both quantitative andqualitative, that are most useful in the conduct of applicable clinical research including serviceevaluation;
ii ethical issues in research;
iii statistical analysis including both exploratory and hypothesis testing methods;
iv critical appraisal of published research;
v the undertaking of supervised research work involving both a major project and also some smallerscale clinical evaluation.
The award holder will demonstrate the ability to complete an independent research project at doctoral levelsuccessfully. This will include the ability to conceptualise, design, carry out and communicate the results ofresearch that is relevant to clinical psychology theory and practice and represents a contribution to the field.
C2 Skills
The required skills are embedded in sections A and B above.
Subject benchmark statement: Health care programmes

page 9
Teaching, learning and assessment
A prerequisite for enrolment on a clinical psychology programme is the achievement of the Graduate Basisfor Registration. Thus the knowledge and skills that form the starting point for a candidate are as set out inthe subject benchmark statement for the undergraduate psychology degree (Quality Assurance Agency forHigher Education Psychology benchmark statement, 2002)
Detailed decisions about the strategies and methods for teaching, learning and assessment are for institutionsto determine, but should ensure that the learning outcomes associated with clinical psychology programmescan be achieved. Nonetheless, programmes must promote an integrative approach to the application oftheory and practice. Learning opportunities and assessment systems should facilitate the acquisition of thefull range of professional competencies. Fundamental to the basis upon which trainees are prepared for theirprofessional career, is the provision of programmes of academic study and practice-based learning which laythe foundation for career-long professional development and lifelong learning, to support best professionalpractice and the maintenance of professional standards.
Teaching and learning in clinical psychology
It is essential that programmes provide a holistic experience of training that enables trainees to develop anintegrated set of learning outcomes constituting a generic training in clinical psychology. Training should beprovided as a collaboration between HEIs and clinical services and supervisors. An appropriate structureshould be in place to facilitate this. Selection criteria should be specified and should apply equally to allcandidates. Programmes should be directed by appropriately qualified chartered clinical psychologists.
Programmes must provide a balanced and developmental set of academic, research and clinical experiencesthroughout training. The academic component needs to provide an integrated curriculum supporting theclinical and research training. The research training needs to be carefully planned and have sufficient timedevoted to it to enable trainees to conduct research at a postgraduate level and to be in a position tocontribute to the knowledge base of the profession. The clinical experience component of training needs toensure the attainment of competence across the range of required experience.
It is important to recognise that the scope of clinical psychology is substantial, so that initial trainingprovides a secure foundation encompassing the range of skills and knowledge demonstrated by theprofession. Further skills and knowledge will need to be acquired through continuing professionaldevelopment appropriate to the specific employment pathways taken by newly qualified psychologists in line with clinical governance and lifelong learning frameworks.
Clinical experience will be gained in service delivery systems that offer a coherent clinical context. This willusually be a setting oriented towards a population defined by age (eg child, adult, older people), by specialneeds (eg learning disabilities, serious mental health problems, health-related problems, substance misuse) orby a service delivery focus (eg psychological therapy). In addition, clinical experience will be gained in a rangeof service contexts (primary, secondary and tertiary care, in-patient, out-patient, community), with servicedelivery models ranging from independently organised work through to integrated interprofessional working.
Programmes will be delivered in collaboration with placement providers to reflect national and local priorities.
Trainees must undertake substantial pieces of clinical work over a substantial period of time in each of arange of settings, including:
in-patient or other residential facilities for individuals with high dependency needs, both acute and long term;
secondary health care;
community and primary care.
Trainees must gain competence in a variety of modes and types of work, including:
direct work;
indirect, through staff and/or carers;
staff training, supervision and consultancy;
work within multidisciplinary teams and specialist service systems, including some observation or otherexperience of change and planning in service systems;
working in more than one recognised model of formal psychological therapy.
Clinical psychology

page 10
It is essential that supervision in clinical placements reflects the Committee on Training in ClinicalPsychology guidelines on clinical supervision. Hence, trainees on clinical placements should receive aminimum of one hour individual supervision and three hours contact time per week. Facilities for traineeson placement must include access to office and clinical facilities. The trainee experience in clinical placementsmust be monitored regularly through appropriately timed visits by programme staff. It is essential thatclinical supervisors have access to appropriate training.
It is essential that research be integrated into practice through the inclusion of service-related researchprojects as well as a larger scale independent doctoral level study. This study should be of a standard that islikely to be publishable in a peer reviewed journal. Adequate research supervision and advice must beavailable to support trainee research, in order to promote post-qualification practice that includes researchactivity through conducting and facilitating research and applying research to inform practice.
Effective learning opportunities that underpin programme delivery require the deployment of appropriatelyqualified clinical academic staff who maintain an involvement in regular professional activity relevant to theprogramme, including clinical work and research. Programmes must be delivered in effective collaborationbetween HEIs, placement providers and clinical supervisors. Opportunities for interprofessional learningshould be maximised.
Sufficient time must be allocated to all components of learning.
Opportunities for enhancement and appraisal of personal and professional development must be provided.
Assessment
The evaluation of trainees must include assessments of academic, research and clinical competence.Programmes must ensure that the assessment system promotes the learning outcomes identified in theprogramme specification and can demonstrate that these learning outcomes have been achieved. Theassessment must give appropriate weighting to professional competence.
The HEI must take responsibility for ensuring that there are adequate procedures to ensure that trainees whoare incompetent or whose behaviour is unethical do not obtain a qualification in clinical psychology.
Subject benchmark statement: Health care programmes

page 11
Academic and practitioner standards
A doctorate in clinical psychology is a vocational qualification as well as an academic award, and as such,must prepare graduates for professional activities across widely differing fields. In particular, graduates mustpossess all the professional competencies to be able to function as a qualified clinical psychologist and thisrepresents the threshold for entry to the profession.
Newly qualified clinical psychologists should understand and embrace the core purpose and philosophy ofthe profession as described in the document prepared by the DCP of The British Psychological Society. Theyshould be committed to reducing psychological distress and enhancing and promoting psychological well-being through the systematic application of knowledge derived from psychological theory and evidence.Their work will be based on the fundamental acknowledgement that all people have the same human valueand the right to be treated as unique individuals.
Thus award holders will have:
the skills, knowledge and values to develop working alliances with clients, including individuals, carersand/or services, in order to carry out psychological assessment; develop a formulation based onpsychological theories and knowledge; carry out psychological interventions; evaluate their work; andcommunicate effectively with clients, referrers and others, orally, electronically and in writing;
the skills knowledge and values to work effectively with clients from a diverse range of backgrounds,understanding and respecting the impact of difference and diversity upon their lives;
the skills, knowledge and values to work effectively with systems relevant to clients, including, forexample, statutory and voluntary services, self-help and advocacy groups, user-led systems and otherelements of the wider community;
the skills, knowledge and values to work in a range of indirect ways to improve psychological aspects of health and healthcare;
the skills, knowledge and values to conduct research that enables the profession to develop itsknowledge base and to monitor and improve the effectiveness of its work;
high level skills in managing a personal learning agenda and self-care, and in critical reflection and self-awareness that enable transfer of knowledge and skills to new settings and problems.
The delivery and assessment of these outcomes is in accordance with the doctoral level descriptors specifiedin the Quality Assurance Agency for Higher Education frameworks for higher education qualifications. It isexpected that the minimum duration of programmes is three years, with at least 50 per cent of time allocatedto supervised clinical experience. The competencies attained are consistent with those described in theNational Occupational Standards for Applied Psychology.
Clinical psychology

page 12
Appendix 1
Clinical psychology benchmark group membership
Mr Malcolm Adams University of East Anglia
Dr Susan Llewelyn University of Oxford
Wider reference group
Course directors
Members of The British Psychological Society Committee on Training in Clinical Psychology
Members of the DCP Training Strategy Group
A Group of trainers in Clinical Psychology
Subject benchmark statement: Health care programmes
page 13
Appendix 2
Benchmark steering group membership
Professor Michael Aulton Royal Pharmaceutical Society
Dr Elizabeth Campbell The British Psychological Society
Mrs Margaret Coats General Chiropractic Council
Mr Vince Cullen General Osteopathic Council
Ms Jill Galvani The Royal Liverpool University Hospital
Ms Rosemary Grant Avon, Gloucestershire and Wiltshire Strategic Health Authority
Dr Mike Hewins Norfolk, Suffolk and Cambridgeshire Strategic Health Authority
Ms Ruth Howkins succeeded byMs Meriel Hutton Quality Assurance Team, Department of Health (England)
Ms Prue Kiddie Department of Health
Professor Jeff Lucas University of Bradford
Mrs Helen Marshall Standing Conference of Principals
Mrs Susan Montague University of Hertfordshire
Professor Audrey Paterson The Society of Radiographers(representing Allied Health Professions)
Professor Mike Pittilo (Chair) University of Hertfordshire
Ms Jenny Routledge University of East Anglia
Mr Alvan Seth-Smith General Dental Council
Mr David Skinner General Medical Council
Mr Roger Thompson Nursing and Midwifery Council
Professor Steve Trevillion General Social Care Council
Professor Diane Waller Health Professions Council
Professor Barry Winn University of Hull
Mr David Young Universities UK
Clinical psychology

Quality Assurance Agency for Higher EducationSouthgate HouseSouthgate StreetGloucesterGL1 1UB
Tel 01452 557000Fax 01452 557070Email [email protected]
QA
A 063 09/04

Scottish subject benchmark statementClinical psychology and applied psychology
(clinical associate) Scotland
A vision and framework for the provision of clinical psychology services for NHS Scotland
J U L Y 2 0 0 6

© The Quality Assurance Agency for Higher Education 2006
ISBN 1 84482 514 0
All QAA's publications are available on our website www.qaa.ac.uk
Printed copies of current publications are available from:Linney DirectAdamswayMansfieldNG18 4FN
Tel 01623 450788Fax 01623 450629Email [email protected]
Registered charity number 1062746

Subject benchmark statements: clinical psychology, and appliedpsychology (clinical associate)1
This subject benchmark statement represents the first phase in an ongoing developmentof the postgraduate training and education of Clinical Psychologists and practitioners ofApplied Psychology (Clinical Associates) for the National Health Service (NHS) Scotland.It provides both a framework and a means of detailing the nature and characteristics ofthese postgraduate programmes of professional preparation at a threshold level of entryfor clinical practice.
While this subject benchmark statement has been informed by the Recognition Schemefor subject benchmark statements (QAA, 2004) it has also taken account of the fact thatstatements that are specific to the higher education (HE) sector in Scotland are handledby QAA Scotland and are subject to a separate process and consultation (QAA, 2004).For this reason, the statement has been prepared in collaboration with key stakeholderswith a shared investment and future vision regarding both the innovative diversity andquality of programmes of preparation that meet the needs of clinical psychology servicesin NHS Scotland. More information on the devolved Scottish context, and the place ofthis benchmark statement within it, is given in the Foreword to this document.
Subject benchmark statements provide a means for the academic community to describethe nature and characteristics of programmes in a specific subject. They also representgeneral expectations about standards for the award of qualifications at a given level andarticulate the attributes and capabilities that those possessing such qualifications shouldbe able to demonstrate.
Subject benchmark statements are used for a variety of purposes. Primarily, they are animportant external source of reference for higher education institutions (HEIs) when newprogrammes are being designed and developed in a subject area. They provide generalguidance for articulating the learning outcomes associated with specific programmes butare not a specification of a detailed curriculum in the subject. Subject benchmarkstatements provide for variety and flexibility in the design of programmes and encourageinnovation within an agreed overall conceptual framework.
Subject benchmark statements also provide support to institutions in the pursuit ofenhancement-led institutional review (ELIR), (QAA, Handbook for enhancement-ledinstitutional review, 2003). They enable the learning outcomes specified for a particularprogramme to be reviewed and evaluated against agreed general expectations aboutstandards.
Finally, subject benchmark statements may be one of a number of external referencepoints that are drawn upon for the purposes of ELIR. Reviewers do not use subjectbenchmark statements as a crude checklist for these purposes however. Rather, they areused in conjunction with the relevant programme specifications, the institution's owninternal evaluation documentation, in order to enable reviewers to come to a roundedjudgement based on a broad range of evidence.
The benchmarking of threshold academic standards for this subject area has beenundertaken by a group of subject specialists in collaboration with key stakeholders in adevolved Scottish context (see Foreword). It has also been informed by the benchmarkstatement for clinical psychology undertaken within a general UK context.2
1 Working title pending the outcome of discussions about protected titles in the context of statutoryregulation of applied psychologists
2 QAA, Subject benchmark statements: Health care programmes Phase 2: Clinical psychology, Gloucester, September, 2004

The statement is subject to future revision that reflects developments in the subject, theexperience of HEIs in utilising the statement, and the evolving nature of clinicalpsychology services in NHS Scotland.
This statement is © The Quality Assurance Agency for Higher Education 2006.
It may be reproduced by educational institutions solely for educational purposes, withoutpermission. Excerpts may be reproduced for the purpose of research, private study, orreview without permission, provided full acknowledgement is given to the subjectbenchmarking group for this subject area and to the copyright of the Quality AssuranceAgency for Higher Education.

page 1
Convener's introduction
Within the UK, Scotland has devolved education and healthcare systems. This givesopportunity for HEIs and health service providers to carry forward a modernisation agendathat produces highly skilled, fit for purpose, health service personnel able to meet thehealthcare needs of the population. The ever increasing demand for psychological serviceswithin the NHS has enabled HEIs and health service providers to consider more creativeways in which this demand might be met by, for example, providing greater flexibility incareer pathways and enhancing the skill mix in the workplace.
As part of this process NHS Education for Scotland has facilitated considerabledevelopments in the education and training of postgraduate psychologists. This hasresulted in two postgraduate levels of professional preparation and competence forpractice in NHS Scotland. The two levels of award are the Doctorate in ClinicalPsychology and the Master's in Applied Psychology (Clinical Associate) respectively. The current benchmark statement aims to highlight the similarities and differencesbetween these two levels of awards in a range of domains. In so doing, this benchmarkstatement will provide postgraduate trainees, academic planners and service providers aclear guide to what competencies should be achieved following completion of each ofthe respective programmes. The benchmark statement clearly illustrates that theDoctorate in Clinical Psychology, as recognised by the British Psychological Society (BPS),is the threshold level required to work as a largely autonomous scientist practitionerwhile the Master's in Applied Psychology (Clinical Associate) is more limited with regardto the level of academic preparation and range of practice. In addition, AppliedPsychology (Clinical Associate) practitioners are required to work under the supervisionof a qualified Clinical Psychologist.
Notwithstanding the above, both levels of award require an undergraduate psychologyhonours degree that confers eligibility for BPS Graduate Basis for Registration. This,coupled with either of the postgraduate levels of award delineates the uniqueness ofClinical Psychology and Applied Psychology (Clinical Associate) practitioners. Many otherprofessions practice certain psychological techniques and specific psychologicaltherapies. However, Clinical Psychologists and Applied Psychology (Clinical Associates)must have a sound undergraduate psychology knowledge base which is furtherdeveloped during postgraduate training. This enables Clinical Psychologists in particular,and to a lesser extent Applied Psychology (Clinical Associate) practitioners to draw upona breadth and depth of psychological theory and research that enables a number ofexplanatory models to be considered when formulating hypotheses and deciding uponthe appropriateness of a range of potential interventions. Clinical Psychologists can applysuch skills across the age range of the population and in a variety of specialties whereasApplied Psychology (Clinical Associate) practitioners operate in a more circumscribedmanner within a specialty. It is the nature and extent of the knowledge base thatdifferentiates between Clinical Psychologists and Applied Psychologists (ClinicalAssociates) but is nevertheless unique to such groups thereby enabling the developmentof novel interventions derived from fundamental psychological theories and principleswhere standardised therapeutic approaches have limited applicability.

page 2
The challenge for the Benchmarking Group was to assimilate all of the above issues,among many others, during their deliberations. In addition, the healthcare contributionof other applied psychologists from other specialties such as forensic, counselling,occupational and health was acknowledged. However, the scope of this currentbenchmark deliberately focused upon the clinical specialty. This was because, amongapplied psychologists within NHS Scotland, this is the largest group, with the greatestservice demands, and is currently undergoing a considerable period of change andmodernisation to meet the needs of the healthcare system. The multidisciplinary groupmet on a number of occasions with subgroup meetings which focused upon specifictasks. This was then compiled into a consultation draft in a manner that ensured acoherent and consensual approach by all group members.
This document has been available for consultation to all stakeholders following whichthe Benchmarking Group considered all feedback and in so doing incorporated anumber of helpful suggestions into the final version.
Professor Kevin G PowerHead of Service, Tayside Area Clinical Psychology Department (NHS Scotland)Convener of the Benchmarking Group

page 3
Contents
Foreword 4
Benchmark statements for Clinical Psychology and Applied Psychology (Clinical Associate) 6
Introduction 6
The core skills of a Clinical Psychologist 8
The core skills of a practitioner of Applied Psychology (Clinical Associate) 9
Clinical Psychologists as scientist practitioners 10
Practitioners of Applied Psychology (Clinical Associate) as scientist practitioners 11
Use of Clinical Psychology services: Clinical Psychologists and Applied Psychology (Clinical Associates) 11
Clinical Psychology and Applied Psychology (Clinical Associate) programmes and maintenance of professional standards 11
Benchmarking of Cinical Psychology and Applied Psychology (Clinical Associate) for Scotland: Standards for awards 13
A Expectations held by the profession, employers and public 13
B Securing, maintaining and improving health and well-being 18
C Knowledge, understanding and skills 22
Teaching, learning and assessment (Clinical Psychology and Applied Psychology (Clinical Associate)) 25
Acknowledgement 31
Appendix 32
Clinical Psychology and Applied Psychology (Clinical Associate): Benchmarking Group membership (Scotland)

page 4
Foreword
This subject benchmark statement describes the nature and threshold standards ofpostgraduate programmes in clinical psychology that lead to the subject awards atdoctoral and master's level, made by HEIs in Scotland. It has been informed by the valuablework already done in which doctoral level postgraduate programmes in clinical psychologyin other parts of the UK have been benchmarked. The Scottish statement not onlyendorses this previous work but has also incorporated parts of it, and has drawn upon it invarious ways that renders the Scottish statement congruent with the wider UK context.
Within the UK context, Scotland not only has a devolved education system, it also has adevolved health care system. Postgraduate training and education for clinical psychologyin Scotland involves a close partnership between HEIs and service providers in NHSScotland. In the development of postgraduate programmes, this collaborative process iscommissioned and brokered by NHS Education for Scotland (NES) under the auspices ofthe Scottish Executive Health Department (SEHD). As with the rest of the UK, NHSScotland is currently embracing a modernisation agenda in which services are beingrestructured in a manner that meets the healthcare needs of its population by makingthe best use of high-quality resources that are both patient-centred and efficient in theirpurpose. In particular, the Kerr Report (Scottish Executive, 2005, Foreword) calls for atransformation of the NHS in Scotland 'with a series of bold initiatives which will providea framework to deliver safe, quick, and sustainable health care for the future'.3
In concert with the modernisation agenda, HEIs and service providers, in partnershipwith NES, have been sensitive to the need to meet public demand for clinical psychologyservices in NHS Scotland in a manner that not only increases the availability of theservice, but also makes best use of resources and expertise. Such proactive collaboration,while maintaining the high standard of established programmes, has seen the innovativedevelopment of flexible pathways of preparation of trainees for the practice of ClinicalPsychology at doctoral level and the introduction of Applied Psychology (ClinicalAssociate) at a different level of postgraduate award. The Benchmarking Group has takenaccount of these innovative developments. In particular the Group has recognised theuniqueness of an emerging Scottish framework in which training and subsequentsupervised clinical practice is being undertaken at master's level. Such a developmentincreases the scope of expertise that can be offered to the Scottish public while alsoserving as a platform for further training and career development at doctoral level in linewith both professional standards and the Scottish Credit and Qualifications Framework(SCQF). The Benchmarking Group has endorsed the importance of this career frameworkwhich hitherto has been lacking to the detriment of service needs and careerdevelopment (NES, 2002).4 Moreover, it is recognised that such a framework will ensurethreshold standards across Scotland while also facilitating mobility of provision to meetservice needs. In doing so, and as indicated above, this benchmark focuses upon theclinical role of applied psychologists as this is the specialty where there exists thegreatest demand, thereby encouraging HEIs to work in partnership with service providersto produce postgraduate programmes that enhance the clinical skill mix available.
This framework of progression also recognises the importance of making explicit thequality threshold standards expressed by the participating HEIs in partnership with NHSScotland, and endorsed by NES, the SEHD and QAA Scotland, while also being mindful of
3 Scottish Executive (May, 2005) A National Framework for Service Change in the NHS in Scotland: Building aHealth Service Fit for the Future, Edinburgh, Scottish Executive
4 (2002) Workforce Planning for Psychological services in NHS Scotland. NES, Edinburgh

page 5
the standards currently set by the BPS and the possibility of future regulation by the HealthProfessions Council. For this reason, the Scottish benchmark statement for ClinicalPsychology and Applied Psychology (Clinical Associate) will be presented in a frameworkthat encapsulates and supports two postgraduate levels of award. This will enable thedifferent HE providers of postgraduate Clinical Psychology and Applied Psychology (ClinicalAssociate) education and training in Scotland to meet the threshold standards in theirprogramme design while also facilitating different academic levels of provision, progressionand completion as and where appropriate. This benchmark statement sets out a flexibleand progressive framework for describing these programmes under three headings.
A Expectations of the health professional in providing patient/client services
B The application of practice in securing, maintaining or improving health and well-being
C The knowledge, understanding and skills that underpin the education and training ofhealth care professionals
It is important to note that these three headings signify a high degree of interdependence,where the academic nature of the respective programmes meet professional requirementsthat are practice-based and education-led. The main section of this statement, in additionto describing the nature and extent of programmes leading to awards in ClinicalPsychology and Applied Psychology (Clinical Associate), respectively, describes theprofession-specific expectations and requirements under the same three categories, butemphasises that postgraduate qualifications in Clinical Psychology and Applied Psychology(Clinical Associate) education and training build upon the prerequisite knowledge and skillsgained from the undergraduate honours degree in psychology.
The section on teaching, learning and assessment draws attention to the key role ofpractice in the design of client-centred learning opportunities for trainees, and to theimportance of ensuring that professional competence, developed through practice, isadequately assessed and rewarded. It also notes how essential it is that the integration oftheory and practice is a planned process within the overall arrangements made forteaching and learning. The importance of professional accountability, team working,interprofessional collaboration and communication are also emphasised.
As noted previously, the statement does not set a national curriculum for programmesleading to awards in Clinical or Applied Psychology (Clinical Associate) in Scotland. Itacknowledges that the requirements of professional and statutory regulatory bodies needto be incorporated into the design of programmes. It seeks to encourage HEIs andservice providers to work collaboratively in the design and delivery of their curricula. Itsessential feature is the specification of threshold standards, incorporating academic andpractitioner elements, against which HEIs are expected, as a minimum, to set theirstandards for the award.
Finally, the Subject benchmark statement for Clinical Psychology and Applied Psychology(Clinical Associate) in Scotland has been designed in such a way that, while mindful ofpresent service needs, also looks to the future in terms of internal quality enhancementalong with continuing professional development (CPD) via a flexible and progressive careerpathway that meets the needs of service users in accordance with the modernisationagenda. Thus the statement that follows is seen as the first phase in an ongoing evolution ofquality systems, interprofessional collaboration, and transparency of programme design in amanner that is clear to all stakeholders. In this respect it is presented as a sound frameworkfor the future of clinical psychology services in Scotland.

page 6
Benchmark statements for Clinical Psychology and AppliedPsychology (Clinical Associate)
Introduction
Two postgraduate levels of award
This benchmark statement incorporates a vision and framework that acknowledges anddescribes two postgraduate and interrelated academic levels of professional preparationfor clinical psychology services for NHS Scotland. These are the Doctorate in ClinicalPsychology, and the Master's in Applied Psychology (Clinical Associate), respectively. The Doctorate in Clinical Psychology is recognised as the threshold level of preparationnecessary to work as a largely autonomous scientist practitioner and subsequentindependent investigator in the field of clinical psychology as recognised by the BPS.Further detail on this level of preparation is given below.
The Master's in Applied Psychology (Clinical Associate) is more circumscribed, not only interms of the academic level of preparation, but also in terms of subsequent practice.Unlike the Doctorate in Clinical Psychology, the purpose of the master's-level programmein Applied Psychology (Clinical Associate) is not to prepare a largely autonomouspractitioner, nor a subsequent independent investigator trained to operate at theforefront of psychological theory and its potential applications. Rather such master'sprogrammes prepare graduates in psychology to work with specific or particular clientgroups and not across a range of client groups. Such work is also limited to a predefinedrange and severity of problems experienced by a particular client group, and will becarried out with the support and under the supervision of a chartered ClinicalPsychologist. This development is seen as both timely and productive for two principalreasons. First, and as noted in the Foreword, it is congruent with the modernisationagenda of NHS Scotland in seeking innovative and effective ways of providing qualityservice provision to meet the health care needs of the Scottish public by increasing thenumber of practitioners with expertise in particular types of problems. Second, and asalso noted in the Foreword, it serves as a framework for further training and careerdevelopment at doctoral level in line with both professional standards and the SCQF.
This benchmark statement incorporates two postgraduate levels of award in which therewill be some common elements relating to standards of professional practice. However,there will also be distinctive differences, both quantitative and qualitative, which theBenchmarking Group has taken into account. For this reason, the pages dealing withstandards for the awards, organised under the three main headings given above, arepresented in a manner that incorporates both levels of award while also highlighting thesubstantive differences between them. In this way, future programme planners may takeaccount of these differences by focusing upon the appropriate level for the programmethey are designing. Finally, and importantly, such a mode of presentation seeks toreinforce the fact that the master's level of preparation, while increasing service provisionfor NHS Scotland, is also part of an educational framework in which the master's level ofpreparation in Applied Psychology (Clinical Associate) may be seen as a platform fromwhich to progress towards undertaking the Doctorate in Clinical Psychology. Concordantwith such a vision and framework of progression, it is envisaged that HEIs offering theDoctorate in Clinical Psychology may take the previous education, training and

page 7
professional experience of these Applied Psychology (Clinical Associate) practitioners intoaccount in their respective programme designs.
Philosophy
The work of Clinical Psychologists and practitioners of Applied Psychology (ClinicalAssociates) is based on the fundamental acknowledgement that all people have the samehuman value and the right to be treated as unique individuals. Thus they will treat allpeople - both clients and colleagues - with dignity and respect and will work with themcollaboratively as partners towards the achievement of mutually agreed goals. In doingthis, they will adhere to, and be guided by, explicit and public statements of the ethicalprinciples that underpin their respective work.
Purpose
Clinical Psychology and Applied Psychology (Clinical Associate), respectively, aim toreduce psychological distress and to enhance and promote psychological well-being bythe systematic application of knowledge derived from psychological theory and research.Clinical Psychologists in particular do not simply apply such knowledge. They alsocontribute to its generation and development through primary research, and knowledgeof the breadth and depth of the science of psychology in all of its foci andmanifestations. This includes adaptive integration from various theories and research-based psychological approaches tailored to particular client or organisational strategies.Thus Clinical Psychologists are a resource for other health care professionals.
Aims
Clinical psychology services aim to enable service users to have the necessary skills andabilities to cope with their emotional needs and daily lives in order to maximisepsychological and physical well-being; to develop and use their capacity to makeinformed choices in order to enhance and maximise independence and autonomy; tohave a sense of self-understanding, self-respect and self-worth; to be able to enjoy goodsocial and personal relationships; and to access commonly valued social andenvironmental facilities. Applied Psychology (Clinical Associate) practitioners workingwithin clinical psychology services have the same aim but with particular client groupsrather than across a range of client groups.
Clinical psychology services aim to enable other service providers to developpsychologically-informed ways of thinking; to use psychological knowledge to enhanceand develop their professional practice to the benefit of their clients; to be able toenhance their sense of self-understanding, self-respect and self-worth; and to usepsychological data to aid decision-making at a clinical, organisational and societal level.Applied Psychology (Clinical Associate) practitioners working within clinical psychologyservices are not expected to deliver this range of activity, but to focus on particular clientgroups within agreed intervention strategies in a manner that meets public need.

page 8
The core skills of a Clinical Psychologist
Assessment
Formulation
Intervention
Evaluation and research
Communication and consultancy
Self management
Assessment of psychological processes and behaviour is a competence derived from thetheory and practice of both academic and applied psychology. It is different from otheractivities such as diagnosis and includes both assessing individual change and stabilityand comparing the individual with others. Assessment procedures include:
the development and use of psychometric tests
the application of systematic observation and measurement of behaviour in bothdaily life contexts and other settings
devising self-monitoring strategies for individual service users
the use of formal and informal interviews with clients, carers and other professionals.
Results of these assessments are integrated within the context of the historical anddevelopmental processes that will have shaped an individual, family, group ororganisation. Clinical Psychologists have the ability to assess the suitability of differentmeasurement procedures depending on the purpose for which the assessment isneeded, as well as being competent to devise and use one-off, individualised assessmentprocedures.
Formulation is the summation and integration of the knowledge that is acquired by thisassessment process (which may involve a number of different procedures). This will drawon psychological theory and research to provide a framework for describing a problem,how it developed and is being maintained. Because of their particular training in thelinkage of theory to practice, Clinical Psychologists will be able to draw on a number ofdifferent explanatory models and so a formulation may comprise a number ofprovisional hypotheses. This process provides the foundation from which actions derive.What makes this activity unique to Clinical Psychologists is the knowledge base andinformation on which they draw. The ability to access, review, evaluate, analyse andsynthesise data and knowledge from a psychological perspective is one that is a primaryfeature of psychology, both academic and applied.
Intervention, if appropriate, is based on formulation. This may involve the utilisation ofone or more psychotherapeutic models or approaches to facilitate change. Other sorts ofintervention may include training of others (professional staff, relatives and carers), theprovision of psychological knowledge by teaching, or the development of psychologicalskills through supervision and consultation. All these interventions are tests of theprovisional hypotheses contained in the formulation and are subject to modification inthe light of experience and new data, including flexible and adaptive integration from arange of theories and research-based knowledge from the science of psychology.
Evaluation is, therefore, a critical and integral part of the Clinical Psychologist's work. Allactivities and interventions need to be evaluated both during their implementation and
page 9
afterwards to assess the stability and security of change. Research includes the ongoingevaluation of assessment, formulation and intervention in relation to specific servicesprovided. It also includes explorations of psychological processes and outcomes (basicresearch), the development and evaluation of specific psychological interventions (primaryresearch) and the consolidation and evaluation of primary research (secondary research).Basic and primary research in clinical psychology is typically uni-professional; secondaryresearch is more usually conducted in collaboration with other professionals. Psychologistsmay input into a variety of audit activities because good audit is also good research.
Communication and consultancy skills are clearly integral to all aspects of a ClinicalPsychologist's role. Effective communication skills and consultancy are routinely essentialin relation to all aspects of work with service users and their families and with otherprofessional staff. Communication skills include direct face to face communication, allforms of electronic and verbal communication to individual clients, their families andother key people, and the dissemination of research. Psychologists need also to playincreasing roles in health promotion, public health, and the provision of policy advice.
Self-management skills include those that are both personal and professionally related.Psychologists need to be aware of personal needs and take action as appropriate. Theyshould ensure awareness of fitness-to-practice issues, boundaries of practice, and theneed for CPD. Clinical Psychologists are cognisant of the importance of self-awarenessand the need to appraise and reflect on their own practice. As reflective practitioners,psychologists are also aware of the importance of diversity, the social and culturalcontext of their work, working within an ethical framework, and the need for continuingprofessional and personal development.
In summary, it is the mixture and synthesis of competencies, built on the body ofpsychological theory and data, which are applied to helping people solve personal,family, group, work or organisational problems, that makes clinical psychology unique inhealth and social care.
The core skills of a practitioner of Applied Psychology (Clinical Associate)
Assessment
Formulation
Intervention
Evaluation and research
Communication
Self management
Assessment of psychological processes and behaviour is a competence derived from thetheory and practice of both academic and applied psychology. It is different from otheractivities such as diagnosis and includes both assessing individual change and stabilityand comparing the individual with others. Assessment procedures include:
the use of established psychometric tests in the area of specialism
the application of systematic observation and measurement of behaviour in bothdaily life contexts and other settings
page 10
the use of self-monitoring strategies for individual service users
the use of formal and informal interviews with clients and carers.
These assessment strategies and measures will be conducted within pre-establishedstrategies and procedures pertinent to specific client group.
Formulation is the summation and integration of the knowledge that is acquired by thisassessment process (which may involve a number of different procedures). This will drawon psychological theory and research to provide a framework for describing a problem,how it developed and is being maintained, according to a pre-established body ofknowledge. In the case of Applied Psychology (Clinical Associate), formulation consists ina critical understanding of the relationship between information gathered fromassessment and the rationale for subsequent therapeutic approaches to intervention asand where appropriate.
Intervention, if appropriate, is based on formulation. This may involve the utilisation ofone or more psychotherapeutic models or approaches to facilitate change. In the case ofApplied Psychology (Clinical Associate), this will be contingent upon the client groupand will involve agreed strategies of intervention in the delivery of Level B services.5
Evaluation is a critical and integral part of the work involved in Applied Psychology(Clinical Associate). All activities and interventions need to be evaluated both duringtheir implementation and afterwards to assess the stability and security of change.Practitioners of Applied Psychology (Clinical Associate) will evaluate their own work withspecific client groups in conjunction with the clinical supervision of a ClinicalPsychologist. Such practitioners may also undertake small-scale research, audit ordevelopment projects, or be part of a research team led by Clinical Psychologists.
Communication skills are clearly integral to all aspects of the role of practitioners ofapplied psychology (healthcare). Effective communication skills are routinely essential inrelation to all aspects of work with service users and their families and with otherprofessional staff. Communication skills include direct face to face communication, allforms of electronic and verbal communication to individual clients, their families andother key people, and the writing of case reports.
Self-management skills include those that are both personal and professionally related.Such practitioners need to be aware of personal needs and take action as appropriate.They should ensure awareness of fitness-to-practice issues, and boundaries of practice.Practitioners of Applied Psychology (Clinical Associate) will become increasinglycognisant of the importance of self-awareness and the need to appraise and reflect ontheir own practice. As reflective practitioners, they will also become aware of theimportance of diversity, the social and cultural context of their work, working within anethical framework, and the need for continuing professional and personal development.
Clinical Psychologists as scientist practitioners
Clinical Psychologists are more than psychological therapists. While many do practisepsychotherapy at a high level, this is not a skill distinct to Clinical Psychologists, norshould it be. The background and training of Clinical Psychologists is rooted in the
5 Level B refers to circumscribed psychological care that is appropriately delivered by specialist accreditedtherapists from a variety of disciplines and that can be described by procedure and protocol (NES, 2002).

page 11
science of psychology, and clinical psychology is one of the applications of psychologicalscience to help address human problems. The ability to design and carry out innovativeapplied research is a skill developed to a doctoral level in training and is important forthe development and delivery of evidence-based practice. In addition, one element ofresearch competence is evaluation of research activity. While there are data that supportmany clinical activities, there are still major gaps in the knowledge base. One of thecontributions made by Clinical Psychologists is the development and testing of newinterventions and activities, based on psychological theory; thus, practice both draws onand influences research and theory.
Practitioners of Applied Psychology (Clinical Associate) as scientistpractitioners
While the main activity of practitioners of Applied Psychology (Clinical Associate) will bethat of psychological therapy and a limited range of other agreed activities pertinent tospecific client groups, it is important to recognise that such master's programmes ofpreparation will still introduce students into the conceptual framework of the scientistpractitioner. Thus although their range of expertise and activities will be within agreedboundaries, their practice will still be informed by the science of psychology. In thevision and framework set out in this document, it is also recognised that such initialpreparation may serve as the first postgraduate step towards subsequent doctoral leveltraining. This makes it all the more important that the preparation of such practitionersbe conceptualised and organised around the scientist practitioner model.
Use of Clinical Psychology services: Clinical Psychologists and AppliedPsychology (Clinical Associates)
Clinical Psychologists work with individuals, couples, families, groups (therapeutic, staff,informal carers) and at the organisational and community level. They work in a variety of health and social care settings in primary, secondary and tertiary care with clientsfrom across the lifespan. They work with people with mild, moderate and severe mentalhealth problems, developmental and learning disabilities, physical and sensory disability,and brain injury; people who have substance misuse problems and people with a rangeof physical health problems (eg HIV and AIDS, cancer, heart disease, pain, diabetes).
While Clinical Psychologists work with a range of client groups as stated above, thoseengaging in Applied Psychology (Clinical Associate) work with particular or single clientgroups. For example, such particular groups may be adults with mild to moderateanxiety and depression; alternatively it may involve aspects of clinical work with children,or the elderly. In each case, such practitioners of Applied Psychology (Clinical Associate)work with the support, and under the supervision of, chartered Clinical Psychologists inthe delivery of Level B services.
Clinical Psychology and Applied Psychology (Clinical Associate)programmes and maintenance of professional standards
Entry to training, at both doctoral and master's level, requires the Graduate Basis forRegistration as defined by the BPS. The prerequisite undergraduate honours degreeprovides an education that develops a knowledge framework encompassing basic theory

page 12
and scientific principles (and the limits of such theory and principles) in the domains ofhuman behaviour, experience and interaction.
Programmes are delivered at postgraduate level in accordance with the SCQF. As appliedto clinical psychology, this means that newly qualified individuals will be able to makeinformed judgements on complex clinical and research problems, often in the absenceof complete information, and are able to communicate their ideas and conclusionsclearly and effectively to specialist and non-specialist audiences. These will be based on asystematic understanding of a substantial body of knowledge that is at the forefront ofthe discipline and profession of clinical psychology. Newly qualified individuals will havecontributed to the creation and development of new knowledge and be able to continueto undertake applied research and development at an advanced level. They will have thequalities and transferable skills necessary for employment, requiring the exercise ofpersonal responsibility and be largely autonomous in taking the initiative in complex andunpredictable clinical situations.
Master's graduates in Applied Psychology (Clinical Associate) will, through respectiveprogrammes of preparation, have the expertise to work with specific client groups withspecific problems. They will be aware of ongoing research concerning these clientgroups. They will understand that psychology in healthcare is an applied science and beaware of gaps in knowledge, both their own and in the field in general. They willcommunicate effectively with both their colleagues and clients. They will understand thecircumscribed nature of their expertise and will know when to consult with seniorcolleagues under whose support and supervision they practise.
Training at doctoral level should encompass theoretical, research and appliedfoundations of psychology applied to the diverse range of needs of people in the health,social care and educational settings. All doctoral programmes provide a generic training,enabling graduates to work with a wide range of clients. Training takes place over threeyears of full-time study or equivalent part-time study at the end of which successfulcandidates are awarded a doctorate of clinical psychology, and are eligible forregistration. Chartered psychologists agree to abide by the BPS Code of Ethics andConduct and can be removed from the register for breaches of this Code. The BPS has aformal disciplinary process with representation of both non-psychologists and senior andexperienced psychologists.
Training at master's level should encompass theoretical, research and appliedfoundations of psychology applied to the needs of specific client groups as noted above.Training takes place over one year of full-time study or part-time equivalent at the end ofwhich successful candidates are awarded a master's degree in Applied Psychology(Clinical Associate) in which the specific client group may be named in the title of theaward. Such practitioners of Applied Psychology (Clinical Associate) are not yet eligiblefor registration by the BPS. However, they are expected to abide by the BPS Code underthe auspices of their chartered clinical psychology supervisors, and their terms andconditions of employment.

page 13
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Mai
ntai
n th
e st
anda
rds
and
req
uire
men
ts o
fth
e BP
S an
d th
e D
ivis
ion
of C
linic
alPs
ycho
logy
(D
CP)
.
Adh
ere
to t
he B
PS's
Cod
e of
Con
duct
, et
hica
lp
rinci
ple
s an
d gu
idel
ines
, an
d th
e D
CP
Prof
essi
onal
Pra
ctic
e G
uide
lines
199
5.
Und
erst
and
the
lega
l and
eth
ical
resp
onsi
bilit
ies
of c
linic
al p
sych
olog
y p
ract
ice
incl
udin
g p
atie
nt c
onse
nt a
nd c
onfid
entia
lity.
Dem
onst
rate
aw
aren
ess
of t
he le
gisl
ativ
e an
dna
tiona
l pla
nnin
g co
ntex
t of
ser
vice
del
iver
yan
d cl
inic
al p
sych
olog
y p
ract
ice.
Reco
gnis
e th
e ob
ligat
ion
to m
aint
ain
fitne
ssfo
r p
ract
ice
and
the
need
for
CPD
.
Con
trib
ute
to t
he d
evel
opm
ent
and
diss
emin
atio
n of
evi
denc
e-ba
sed
pra
ctic
ew
ithin
pro
fess
iona
l con
text
s.
Mak
e ap
pro
pria
te c
linic
al d
ecis
ions
.
A1
Pro
fess
ion
alau
ton
om
y an
dac
coun
tab
ility
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Mai
ntai
n th
e st
anda
rds
and
req
uire
men
tsof
the
BPS
.
Adh
ere
to t
he B
PS's
Cod
e of
Con
duct
,et
hica
l prin
cip
les
and
guid
elin
es.
Und
erst
and
the
lega
l and
eth
ical
resp
onsi
bilit
ies
of w
orki
ng in
hea
lthca
rese
ttin
gs a
s a
clin
ical
ly s
uper
vise
dp
ract
ition
er,
incl
udin
g p
atie
nt c
onse
nt a
ndco
nfid
entia
lity.
Dem
onst
rate
aw
aren
ess
of t
he le
gal a
ndna
tiona
l im
por
tanc
e of
del
iver
ing
psyc
holo
gica
l ser
vice
s in
hea
lthca
re s
ettin
gs.
Reco
gnis
e th
e ob
ligat
ion
to m
aint
ain
fitne
ss f
or p
ract
ice
and
the
need
for
CPD
.
Enga
ge w
ith r
elev
ant
asp
ects
of
the
know
ledg
e ba
se o
f cl
inic
al p
sych
olog
y an
dco
ntrib
ute
to e
vide
nce-
base
d pr
actic
ew
ithin
circ
umsc
ribed
pro
fess
iona
l con
text
s.
Mak
e ap
pro
pria
te c
linic
al d
ecis
ions
with
inth
e ra
nge
of o
ne's
exp
ertis
e, s
eeki
nggu
idan
ce w
here
ap
pro
pria
te.
Ben
chm
arkin
g o
f C
lin
ical
Psy
cho
log
y an
d A
pp
lied
Psy
cho
log
y (C
lin
ical
Ass
oci
ate)
fo
rSc
otl
and
: St
and
ard
s fo
r aw
ard
s
AEx
pec
tati
on
s h
eld
by
the
pro
fess
ion
, em
plo
yers
an
d p
ub
lic

page 14
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Part
icip
ate
effe
ctiv
ely
in in
terp
rofe
ssio
nal
and
mul
ti-ag
ency
ap
pro
ache
s to
hea
lth a
ndso
cial
car
e.
Reco
gnis
e p
rofe
ssio
nal s
cop
e of
pra
ctic
e an
dm
ake
refe
rral
s, w
here
ap
pro
pria
te.
Dem
onst
rate
und
erst
andi
ng o
f co
nsul
tanc
ym
odel
s an
d th
e co
ntrib
utio
n of
con
sulta
ncy
to p
ract
ice.
Wor
k w
ith o
ther
s to
del
iver
effe
ctiv
ehe
alth
care
.
Und
erst
and
the
imp
act
of d
iffer
ence
, di
vers
ityan
d so
cial
ineq
ualit
ies
on p
eop
le's
lives
, an
dth
eir
imp
licat
ions
for
wor
king
pra
ctic
es.
Wor
k ef
fect
ivel
y w
ith u
sers
and
car
ers
tofa
cilit
ate
thei
r in
volv
emen
t in
ser
vice
pla
nnin
gan
d de
liver
y.
Mai
ntai
n ap
pro
pria
te r
ecor
ds a
nd m
ake
accu
rate
rep
orts
.
A2
Pro
fess
ion
alre
lati
on
ship
s
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Part
icip
ate
effe
ctiv
ely
in in
terp
rofe
ssio
nal
and
mul
ti-ag
ency
ap
pro
ache
s to
hea
lthan
d so
cial
car
e.
Reco
gnis
e p
rofe
ssio
nal s
cop
e of
pra
ctic
e,an
d w
here
lim
its o
f ex
per
tise
are
reco
gnis
ed t
o m
ake
app
rop
riate
ref
erra
l to
a ch
arte
red
Clin
ical
Psy
chol
ogis
t.
Dem
onst
rate
the
abi
lity
to o
ffer
psy
chol
ogic
ally
bas
ed a
dvic
e to
hea
lthp
rofe
ssio
nal c
olle
ague
s w
ithin
one
'sci
rcum
scrib
ed a
rea
of p
ract
ice.
Wor
k w
ith o
ther
s to
del
iver
effe
ctiv
ep
sych
olog
ical
tre
atm
ents
.
Und
erst
and
the
imp
act
of d
iffer
ence
,di
vers
ity a
nd s
ocia
l ine
qua
litie
s on
peo
ple
'sliv
es,
and
thei
r im
plic
atio
ns f
or w
orki
ngp
ract
ices
.
Wor
k ef
fect
ivel
y w
ith u
sers
and
car
ers
tofa
cilit
ate
thei
r in
volv
emen
t in
ser
vice
deliv
ery.
Mai
ntai
n ap
pro
pria
te r
ecor
ds a
nd m
ake
accu
rate
rep
orts
.

page 15
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Dem
onst
rate
the
abi
lity
to d
eliv
er h
igh
qua
lity
pat
ient
/clie
nt-c
entr
ed c
are
both
as
a so
lo p
ract
ition
er a
nd a
s a
mem
ber
ofm
ultid
isci
plin
ary
and
mul
ti-ag
ency
tea
ms.
Prac
tise
in a
non
-dis
crim
inat
ory,
no
n-op
pre
ssiv
e m
anne
r.
Dra
w u
pon
clin
ical
psy
chol
ogy
know
ledg
e,th
eory
and
ski
lls in
ord
er t
o m
ake
pro
fess
iona
lju
dgem
ents
.
Dem
onst
rate
hig
h le
vels
of
rese
arch
ski
lls a
ndsc
hola
rshi
p.
Wor
k ef
fect
ivel
y at
a h
igh
leve
l of
auto
nom
yin
com
ple
x an
d un
pre
dict
able
situ
atio
ns,
with
awar
enes
s of
the
lim
its o
f th
eir
own
com
pet
ence
, an
d ac
cep
ting
acco
unta
bilit
y to
rele
vant
pro
fess
iona
l and
ser
vice
man
ager
s.
A3
Pers
on
al a
nd
pro
fess
ion
al s
kills
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Dem
onst
rate
the
abi
lity
to d
eliv
er h
igh
qua
lity
care
to
indi
vidu
al c
lient
s, a
nd b
ean
effe
ctiv
e m
embe
r of
mul
tipro
fess
iona
lan
d m
ulti-
agen
cy t
eam
s.
Prac
tise
in a
non
-dis
crim
inat
ory,
no
n-op
pre
ssiv
e m
anne
r.
Dra
w u
pon
psy
chol
ogy
know
ledg
e, t
heor
yan
d sk
ills
in o
rder
to
mak
e ap
pro
pria
teju
dgem
ents
reg
ardi
ng p
atie
nt c
are.
Dem
onst
rate
ap
pro
pria
te le
vels
of
rese
arch
skill
s an
d cr
itica
l thi
nkin
g.
Wor
k ef
fect
ivel
y, w
ith a
war
enes
s of
the
limits
of
thei
r ow
n co
mp
eten
ce,
and
acce
ptin
g ac
coun
tabi
lity
to r
elev
ant
pro
fess
iona
l and
ser
vice
man
ager
s.

page 16
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Dem
onst
rate
sel
f-aw
aren
ess
and
abili
ty t
ow
ork
as a
ref
lect
ive
pra
ctiti
oner
.
Dem
onst
rate
effe
ctiv
e an
d ap
pro
pria
teco
mm
unic
atio
n sk
ills.
Initi
ate
and
resp
ond
to c
hang
e in
an
effe
ctiv
em
anne
r, de
mon
stra
ting
tran
sfer
able
ski
lls.
Man
age
the
emot
iona
l and
phy
sica
l im
pac
tof
the
ir ow
n p
ract
ice.
Und
erst
and
the
role
and
impo
rtan
ce o
fsu
perv
ision
and
dem
onst
rate
its
appr
opria
te u
se.
Dem
onst
rate
sel
f-m
anag
emen
t sk
ills
and
inde
pen
denc
e of
tho
ught
and
act
ion.
Dem
onst
rate
cul
tura
lly c
omp
eten
t p
ract
ice.
A3
Pers
on
al a
nd
pro
fess
ion
al s
kills
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Dem
onst
rate
sel
f-aw
aren
ess
and
abili
ty t
ow
ork
as a
ref
lect
ive
pra
ctiti
oner
.
Dem
onst
rate
effe
ctiv
e an
d ap
pro
pria
teco
mm
unic
atio
n sk
ills.
Initi
ate
and
resp
ond
to c
hang
e in
an
effe
ctiv
em
anne
r, de
mon
stra
ting
tran
sfer
able
ski
lls.
Reco
gnis
e th
e em
otio
nal a
nd p
hysi
cal
imp
act
of t
heir
own
pra
ctic
e an
d se
ek h
elp
whe
re a
pp
rop
riate
.
Dev
elop
und
er t
he s
uper
visi
on a
ndm
ento
rshi
p o
f a
char
tere
d C
linic
alPs
ycho
logi
st.
Dev
elop
sel
f-m
anag
emen
t sk
ills
unde
r th
esu
per
visi
on o
f a
char
tere
d C
linic
alPs
ycho
logi
st.
Dem
onst
rate
cul
tura
lly c
ompe
tent
pra
ctic
e.

page 17
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Show
an
unde
rsta
ndin
g of
the
rol
e of
the
Clin
ical
Psy
chol
ogis
t w
ithin
hea
lth a
nd s
ocia
lca
re s
ervi
ces.
Ada
pt
Clin
ical
Psy
chol
ogy
pra
ctic
e to
a r
ange
of o
rgan
isat
iona
l con
text
s on
the
bas
is o
f an
unde
rsta
ndin
g of
per
tinen
t or
gani
satio
nal
and
cultu
ral i
ssue
s.
Con
trib
ute
to t
he d
evel
opm
ent
of t
hep
rofe
ssio
n's
resp
onsi
bilit
y to
NH
S Sc
otla
ndth
roug
h te
achi
ng,
rese
arch
sup
ervi
sion
, an
dtr
aini
ng o
f p
sych
olog
ists
and
oth
erp
rofe
ssio
nals
.
Take
res
pon
sibi
lity
for
thei
r ow
n p
rofe
ssio
nal
deve
lop
men
t.
Dem
onst
rate
an
abili
ty t
o co
ntrib
ute
to t
eam
man
agem
ent
and
func
tioni
ng.
Part
icip
ate
in t
he d
evel
opm
ent
of n
ew s
ervi
ces.
A4
Pro
fess
ion
an
dem
plo
yer
con
text
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Show
an
unde
rsta
ndin
g of
the
rol
es o
fp
ract
ition
ers
of A
pp
lied
Psyc
holo
gy(C
linic
al A
ssoc
iate
) w
ithin
hea
lth a
ndso
cial
car
e se
rvic
es.
Adap
t Ap
plie
d Ps
ycho
logy
(C
linic
alAs
soci
ate)
pra
ctic
e to
a r
ange
of r
elev
ant
cont
exts
on
the
basis
of a
n un
ders
tand
ing
ofpe
rtin
ent
orga
nisa
tiona
l and
cul
tura
l iss
ues.
Enga
ge in
tea
chin
g w
ithin
the
ran
ge o
fth
eir
exp
ertis
e.
Take
res
pon
sibi
lity
for
thei
r ow
np
rofe
ssio
nal d
evel
opm
ent.
Dem
onst
rate
an
abili
ty t
o co
ntrib
ute
tote
am f
unct
ioni
ng.
Part
icip
ate
in t
he d
evel
opm
ent
of s
ervi
ces.

page 18
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Clin
ical
Psy
chol
ogy
pra
ctic
e an
d th
eap
plic
atio
n of
pro
fess
iona
l ski
lls a
reun
derp
inne
d by
psy
chol
ogic
al t
heor
y,ev
iden
ce a
nd u
nder
stan
ding
. Th
e q
ualif
ied
Clin
ical
Psy
chol
ogis
t p
osse
sses
a b
road
ran
geof
cor
e sk
ills
enco
mp
assi
ng p
rofe
ssio
n-sp
ecifi
can
d ge
neric
ena
blin
g sk
ills.
Dev
elop
and
mai
ntai
n ef
fect
ive
wor
king
allia
nces
with
clie
nts,
incl
udin
g in
divi
dual
s,fa
mili
es,
care
rs a
nd s
ervi
ces.
Dem
onst
rate
the
abi
lity
to c
hoos
e, u
se a
ndin
terp
ret
a br
oad
rang
e of
psy
chol
ogic
alas
sess
men
t m
etho
ds a
pp
rop
riate
to t
he c
lient
and
ser
vice
del
iver
y sy
stem
inw
hich
the
ass
essm
ent
take
s p
lace
to t
he t
ype
of in
terv
entio
n w
hich
is li
kely
to b
e re
qui
red.
Dem
onst
rate
com
pet
ence
in t
he f
ollo
win
gas
sess
men
t p
roce
dure
sfo
rmal
pro
cedu
res
(use
of
stan
dard
ised
inst
rum
ents
)sy
stem
atic
inte
rvie
win
g p
roce
dure
sot
her
stru
ctur
ed m
etho
ds o
f as
sess
men
t(e
g ob
serv
atio
n m
etho
ds,
gath
erin
gin
form
atio
n fr
om p
roxi
es,
etc)
Con
duct
ap
pro
pria
te r
isk
asse
ssm
ent
and
use
this
to
guid
e p
ract
ice.
B1
Pro
fess
ion
-sp
ecif
icsk
ills
Pro
fess
ion
-sp
ecif
ic s
kills
B1a
Psy
cho
log
ical
asse
ssm
ent
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Ap
plie
d Ps
ycho
logy
pra
ctic
e an
d th
eap
plic
atio
n of
pro
fess
iona
l ski
lls a
reun
derp
inne
d by
psy
chol
ogic
al t
heor
y,ev
iden
ce a
nd u
nder
stan
ding
acc
ordi
ng t
oag
reed
inte
rven
tion
stra
tegi
es w
ith a
sing
le c
lient
gro
up a
nd u
nder
the
sup
ervi
sion
of
a ch
arte
red
Clin
ical
Psyc
holo
gist
. Th
is a
pp
lies
to B
1 a,
b,
c an
dd
belo
w.
Dev
elop
and
mai
ntai
n ef
fect
ive
wor
king
allia
nces
with
clie
nts
and,
whe
reap
pro
pria
te,
sign
ifica
nt o
ther
s.
Dev
elop
the
abi
lity
to c
hoos
e, u
se a
ndun
ders
tand
a r
ange
of
psy
chol
ogic
alas
sess
men
t m
etho
ds a
pp
rop
riate
to
to t
he c
lient
and
ser
vice
del
iver
y sy
stem
in w
hich
the
ass
essm
ent
take
s pl
ace
to t
he t
ype
of in
terv
entio
n w
hich
islik
ely
to b
e re
qui
red.
Dem
onst
rate
com
pet
ence
in t
he f
ollo
win
gas
sess
men
t p
roce
dure
sfo
rmal
pro
cedu
res
(use
of
stan
dard
ised
inst
rum
ents
)sy
stem
atic
inte
rvie
win
g p
roce
dure
sot
her
stru
ctur
ed m
etho
ds o
fas
sess
men
t.U
nder
sup
ervi
sion
, co
nduc
t ris
kas
sess
men
t an
d us
e th
is t
o gu
ide
pra
ctic
e.
B
Secu
rin
g,
mai
nta
inin
g a
nd
im
pro
vin
g h
ealt
h a
nd
wel
l-b
ein
g
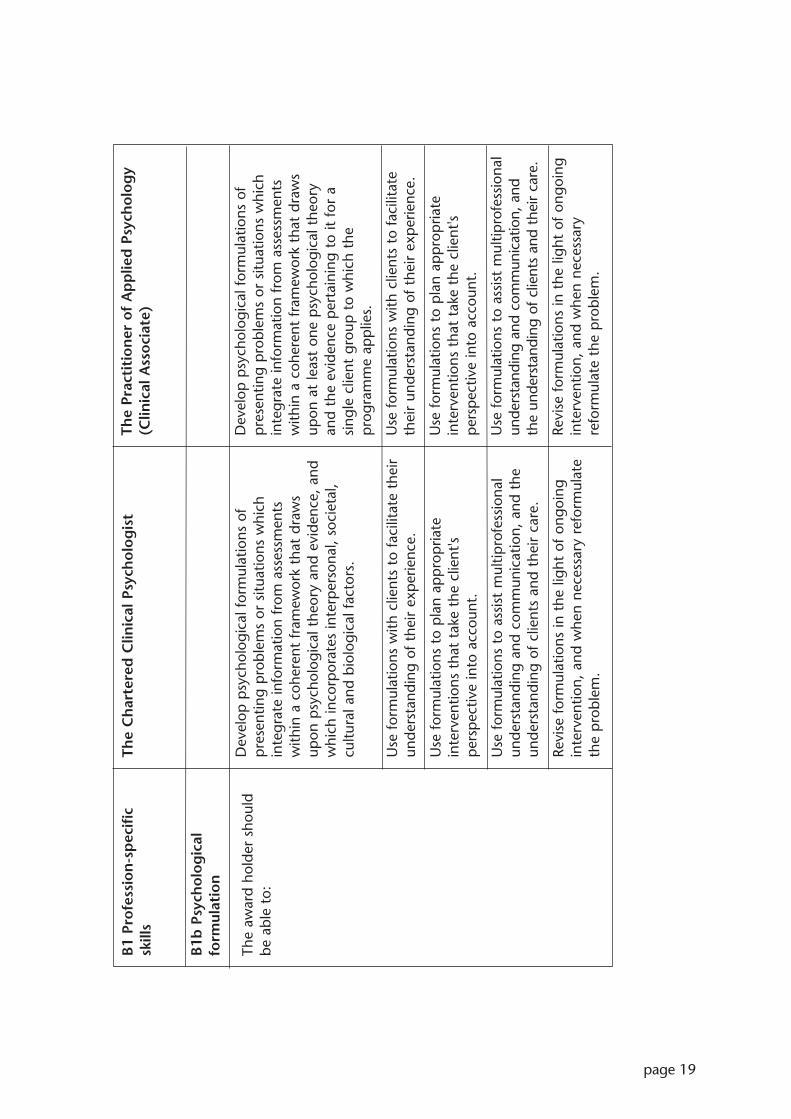
page 19
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Dev
elop
psy
chol
ogic
al f
orm
ulat
ions
of
pre
sent
ing
pro
blem
s or
situ
atio
ns w
hich
inte
grat
e in
form
atio
n fr
om a
sses
smen
tsw
ithin
a c
oher
ent
fram
ewor
k th
at d
raw
sup
on p
sych
olog
ical
the
ory
and
evid
ence
, an
dw
hich
inco
rpor
ates
inte
rper
sona
l, so
ciet
al,
cultu
ral a
nd b
iolo
gica
l fac
tors
.
Use
for
mul
atio
ns w
ith c
lient
s to
fac
ilita
te t
heir
unde
rsta
ndin
g of
the
ir ex
per
ienc
e.
Use
for
mul
atio
ns t
o p
lan
app
rop
riate
inte
rven
tions
tha
t ta
ke t
he c
lient
's p
ersp
ectiv
e in
to a
ccou
nt.
Use
for
mul
atio
ns t
o as
sist
mul
tipro
fess
iona
lun
ders
tand
ing
and
com
mun
icat
ion,
and
the
unde
rsta
ndin
g of
clie
nts
and
thei
r ca
re.
Revi
se f
orm
ulat
ions
in t
he li
ght
of o
ngoi
ngin
terv
entio
n, a
nd w
hen
nece
ssar
y re
form
ulat
eth
e p
robl
em.
B1
Pro
fess
ion
-sp
ecif
icsk
ills
B1b
Psy
cho
log
ical
form
ulat
ion
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Dev
elop
psy
chol
ogic
al f
orm
ulat
ions
of
pre
sent
ing
pro
blem
s or
situ
atio
ns w
hich
inte
grat
e in
form
atio
n fr
om a
sses
smen
tsw
ithin
a c
oher
ent
fram
ewor
k th
at d
raw
sup
on a
t le
ast
one
psy
chol
ogic
al t
heor
yan
d th
e ev
iden
ce p
erta
inin
g to
it f
or a
sing
le c
lient
gro
up t
o w
hich
the
pro
gram
me
app
lies.
Use
for
mul
atio
ns w
ith c
lient
s to
fac
ilita
teth
eir
unde
rsta
ndin
g of
the
ir ex
per
ienc
e.
Use
for
mul
atio
ns t
o p
lan
app
rop
riate
inte
rven
tions
tha
t ta
ke t
he c
lient
'sp
ersp
ectiv
e in
to a
ccou
nt.
Use
for
mul
atio
ns t
o as
sist
mul
tipro
fess
iona
lun
ders
tand
ing
and
com
mun
icat
ion,
and
the
unde
rsta
ndin
g of
clie
nts
and
thei
r ca
re.
Revi
se f
orm
ulat
ions
in t
he li
ght
of o
ngoi
ngin
terv
entio
n, a
nd w
hen
nece
ssar
yre
form
ulat
e th
e p
robl
em.
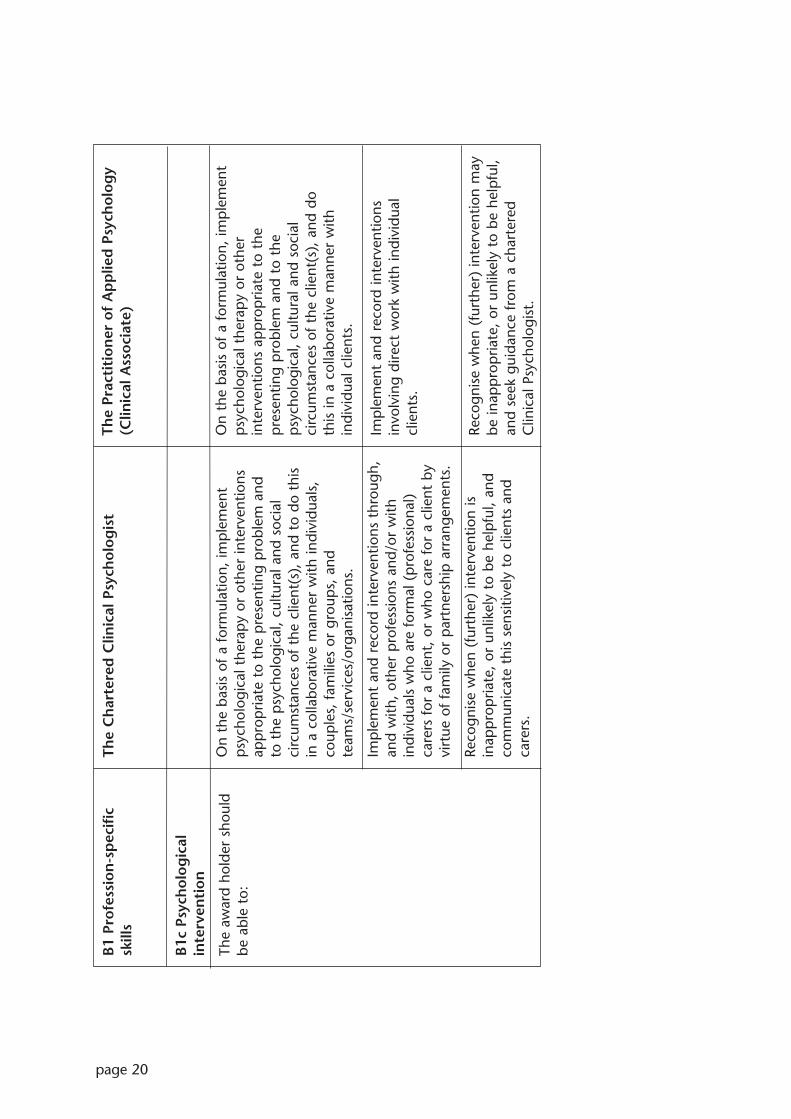
page 20
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
On
the
basi
s of
a f
orm
ulat
ion,
imp
lem
ent
psy
chol
ogic
al t
hera
py
or o
ther
inte
rven
tions
app
rop
riate
to
the
pre
sent
ing
pro
blem
and
to
the
psy
chol
ogic
al,
cultu
ral a
nd s
ocia
lci
rcum
stan
ces
of t
he c
lient
(s),
and
to
do t
his
in a
col
labo
rativ
e m
anne
r w
ith in
divi
dual
s,co
uple
s, f
amili
es o
r gr
oup
s, a
ndte
ams/
serv
ices
/org
anis
atio
ns.
Imp
lem
ent
and
reco
rd in
terv
entio
ns t
hrou
gh,
and
with
, ot
her
pro
fess
ions
and
/or
with
indi
vidu
als
who
are
for
mal
(p
rofe
ssio
nal)
care
rs f
or a
clie
nt,
or w
ho c
are
for
a cl
ient
by
virt
ue o
f fa
mily
or
par
tner
ship
arr
ange
men
ts.
Reco
gnis
e w
hen
(fur
ther
) in
terv
entio
n is
inap
pro
pria
te,
or u
nlik
ely
to b
e he
lpfu
l, an
dco
mm
unic
ate
this
sen
sitiv
ely
to c
lient
s an
dca
rers
.
B1
Pro
fess
ion
-sp
ecif
icsk
ills
B1c
Psy
cho
log
ical
inte
rven
tio
n
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
On
the
basi
s of
a f
orm
ulat
ion,
imp
lem
ent
psy
chol
ogic
al t
hera
py
or o
ther
inte
rven
tions
ap
pro
pria
te t
o th
ep
rese
ntin
g p
robl
em a
nd t
o th
ep
sych
olog
ical
, cu
ltura
l and
soc
ial
circ
umst
ance
s of
the
clie
nt(s
), a
nd d
o th
is in
a c
olla
bora
tive
man
ner
with
indi
vidu
al c
lient
s.
Imp
lem
ent
and
reco
rd in
terv
entio
nsin
volv
ing
dire
ct w
ork
with
indi
vidu
alcl
ient
s.
Reco
gnis
e w
hen
(fur
ther
) in
terv
entio
n m
aybe
inap
pro
pria
te,
or u
nlik
ely
to b
e he
lpfu
l,an
d se
ek g
uida
nce
from
a c
hart
ered
Clin
ical
Psy
chol
ogis
t.

page 21
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Sele
ct a
nd im
ple
men
t ap
pro
pria
te m
etho
dsto
eva
luat
e th
e ef
fect
iven
ess,
acc
epta
bilit
yan
d br
oade
r im
pac
t of
inte
rven
tions
(bo
thin
divi
dual
and
org
anis
atio
nal),
and
use
thi
sin
form
atio
n to
info
rm a
nd s
hap
e p
ract
ice.
Whe
re a
pp
rop
riate
, al
so d
evis
e in
nova
tive
pro
cedu
res.
Aud
it cl
inic
al e
ffect
iven
ess.
Iden
tify
gap
s in
the
evi
denc
e ba
se a
nd,
whe
resu
ch g
aps
exis
t, a
dap
t es
tabl
ishe
d p
ract
ice
tom
eet
the
spec
ific
need
s of
ser
vice
use
rs.
Reco
gnis
e th
at,
in s
uch
case
s, o
ngoi
ngev
alua
tion
of a
dap
tatio
ns is
crit
ical
and
for
ms
the
basi
s of
new
dev
elop
men
ts in
the
ory
and
pra
ctic
e.
Dev
elop
the
ory
and
pra
ctic
e in
clin
ical
psy
chol
ogy
thro
ugh
rese
arch
.
B1
Pro
fess
ion
-sp
ecif
icsk
ills
B1d
Eva
luat
ion
an
dre
sear
ch
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Sele
ct a
nd im
ple
men
t ap
pro
pria
tem
etho
ds t
o ev
alua
te t
he e
ffect
iven
ess
ofin
terv
entio
ns w
ith in
divi
dual
clie
nts,
and
use
this
info
rmat
ion
to in
form
and
sha
pe
pra
ctic
e.
Aud
it cl
inic
al s
ervi
ces.
Iden
tify
gap
s in
the
rel
evan
t kn
owle
dge
base
.
Con
duct
ap
pro
pria
te s
ervi
ce-r
elat
edre
sear
ch u
sing
a r
ange
of
stan
dard
and
spec
ialis
ed r
esea
rch
or e
qui
vale
ntin
stru
men
ts a
nd t
echn
ique
s of
enq
uiry
,ei
ther
indi
vidu
ally
und
er s
uper
visi
on,
or
as p
art
of a
res
earc
h te
am.

page 22
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Dem
onst
rate
acq
uisi
tion
and
unde
rsta
ndin
gof
a s
ubst
antia
l bod
y of
kno
wle
dge,
incl
udin
gth
eorie
s an
d ev
iden
ce c
once
rnin
gp
sych
olog
ical
dev
elop
men
t an
d p
sych
olog
ical
diffi
culti
es a
cros
s th
e lif
esp
an a
nd t
heir
asse
ssm
ent
and
rem
edia
tion.
Thi
s sh
ould
incl
ude
theo
ry a
nd e
vide
nce
at t
he f
oref
ront
of t
he d
isci
plin
e re
latin
g to
a w
ide
brea
dth
of p
rese
ntat
ions
, fr
omac
ute
to e
ndur
ing
and
from
mild
to
seve
rep
robl
ems
rang
ing
from
tho
se w
ith m
ainl
ybi
olog
ical
cau
satio
n to
tho
se e
man
atin
gm
ainl
y fr
om p
sych
osoc
ial f
acto
rsp
robl
ems
of c
opin
g/ad
apta
tion
to a
dver
seci
rcum
stan
ces
that
are
not
the
mse
lves
reve
rsib
le b
y p
sych
olog
ical
inte
rven
tion
(eg
phy
sica
l dis
abili
ty,
phy
sica
l illn
ess,
bere
avem
ent)
clie
nts
from
a r
ange
of
back
grou
nds
refle
ctin
g th
e de
mog
rap
hic
char
acte
ristic
sof
the
pop
ulat
ion
clie
nts
with
sig
nific
ant
leve
ls o
fch
alle
ngin
g be
havi
our
clie
nts
acro
ss a
ran
ge o
f le
vels
of
inte
llect
ual f
unct
ioni
ng o
ver
a ra
nge
of a
ges
clie
nts
who
se d
isab
ility
mak
es it
diff
icul
tfo
r th
em t
o co
mm
unic
ate
care
rs a
nd f
amili
esso
cial
and
con
text
ual f
acto
rs,
team
wor
k,se
rvic
e de
liver
y sy
stem
s, a
nd le
gisl
ativ
ean
d p
olic
y fr
amew
orks
.
C K
no
wle
dg
e,un
der
stan
din
g a
nd
ski
lls
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Syst
emat
ic a
cqui
sitio
n an
d w
orki
ngkn
owle
dge
of a
t le
ast
one
psy
chol
ogic
alth
eory
rel
evan
t to
the
ir cl
inic
al p
ract
ice
ina
spec
ific
area
with
par
ticul
ar c
lient
grou
ps.
Thi
s m
ay in
clud
e th
eory
and
evid
ence
-bas
ed p
ract
ice
rela
ting
top
sych
olog
ical
pro
blem
s fr
om a
def
ined
rang
e of
sev
erity
clie
nts
from
a d
efin
ed c
lient
gro
upp
ertin
ent
to t
he p
rogr
amm
eca
rers
and
fam
ilies
soci
al a
nd c
onte
xtua
l fac
tors
team
wor
k, s
ervi
ce d
eliv
ery
syst
ems
and
legi
slat
ive
and
pol
icy
fram
ewor
ks.
C K
no
wle
dg
e, u
nd
erst
and
ing
an
d s
kil
ls
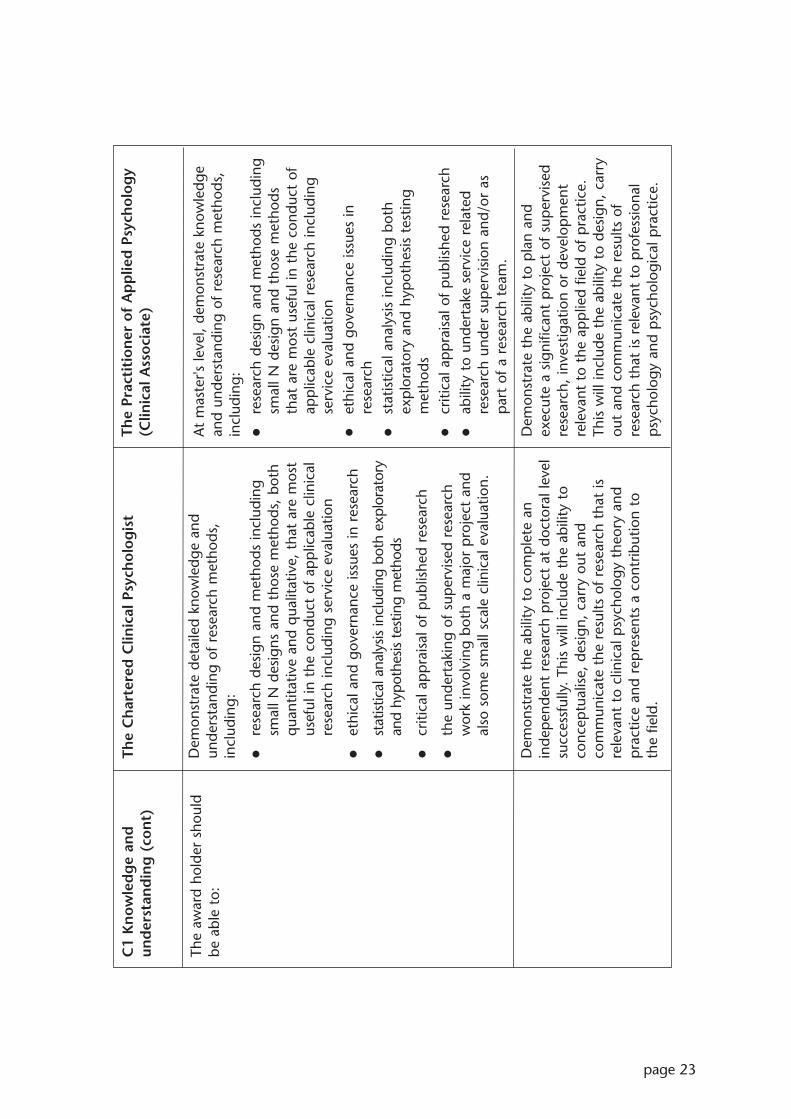
page 23
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Dem
onst
rate
det
aile
d kn
owle
dge
and
unde
rsta
ndin
g of
res
earc
h m
etho
ds,
incl
udin
g:
rese
arch
des
ign
and
met
hods
incl
udin
gsm
all N
des
igns
and
tho
se m
etho
ds,
both
qua
ntita
tive
and
qua
litat
ive,
tha
t ar
e m
ost
usef
ul in
the
con
duct
of
app
licab
le c
linic
alre
sear
ch in
clud
ing
serv
ice
eval
uatio
n
ethi
cal a
nd g
over
nanc
e is
sues
in r
esea
rch
stat
istic
al a
naly
sis in
clud
ing
both
exp
lora
tory
and
hypo
thes
is te
stin
g m
etho
ds
criti
cal a
pp
rais
al o
f p
ublis
hed
rese
arch
the
unde
rtak
ing
of s
uper
vise
d re
sear
chw
ork
invo
lvin
g bo
th a
maj
or p
roje
ct a
ndal
so s
ome
smal
l sca
le c
linic
al e
valu
atio
n.
Dem
onst
rate
the
abi
lity
to c
omp
lete
an
inde
pen
dent
res
earc
h p
roje
ct a
t do
ctor
al le
vel
succ
essf
ully
. Th
is w
ill in
clud
e th
e ab
ility
to
conc
eptu
alis
e, d
esig
n, c
arry
out
and
com
mun
icat
e th
e re
sults
of
rese
arch
tha
t is
rele
vant
to
clin
ical
psy
chol
ogy
theo
ry a
ndp
ract
ice
and
rep
rese
nts
a co
ntrib
utio
n to
th
e fie
ld.
C1
Kn
ow
led
ge
and
und
erst
and
ing
(co
nt)
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
At
mas
ter's
leve
l, de
mon
stra
te k
now
ledg
ean
d un
ders
tand
ing
of r
esea
rch
met
hods
,in
clud
ing:
rese
arch
des
ign
and
met
hods
incl
udin
gsm
all N
des
ign
and
thos
e m
etho
dsth
at a
re m
ost
usef
ul in
the
con
duct
of
app
licab
le c
linic
al r
esea
rch
incl
udin
gse
rvic
e ev
alua
tion
ethi
cal a
nd g
over
nanc
e is
sues
inre
sear
chst
atis
tical
ana
lysi
s in
clud
ing
both
exp
lora
tory
and
hyp
othe
sis
test
ing
met
hods
criti
cal a
pp
rais
al o
f p
ublis
hed
rese
arch
abili
ty t
o un
dert
ake
serv
ice
rela
ted
rese
arch
und
er s
uper
visi
on a
nd/o
r as
par
t of
a r
esea
rch
team
.
Dem
onst
rate
the
abi
lity
to p
lan
and
exec
ute
a si
gnifi
cant
pro
ject
of
sup
ervi
sed
rese
arch
, in
vest
igat
ion
or d
evel
opm
ent
rele
vant
to
the
app
lied
field
of
pra
ctic
e.Th
is w
ill in
clud
e th
e ab
ility
to
desi
gn,
carr
you
t an
d co
mm
unic
ate
the
resu
lts o
fre
sear
ch t
hat
is r
elev
ant
to p
rofe
ssio
nal
psy
chol
ogy
and
psy
chol
ogic
al p
ract
ice.

page 24
The
Ch
arte
red
Clin
ical
Psy
cho
log
ist
Dem
onst
rate
a c
ritic
al u
nder
stan
ding
of
the
fact
tha
t so
und
app
lied
psy
chol
ogy
pra
ctic
e is
base
d on
clin
ical
and
res
earc
h sk
ills
that
enga
ge a
nd e
mer
ge f
rom
wor
k w
ith c
lient
san
d sy
stem
s ba
sed
on a
sci
entis
t-p
ract
ition
eran
d re
flect
ive
pra
ctiti
oner
mod
el.
This
inco
rpor
ates
a c
ycle
of
asse
ssm
ent,
form
ulat
ion,
inte
rven
tion
and
eval
uatio
n, a
sou
tline
d ea
rlier
. H
ence
Clin
ical
Psy
chol
ogis
tsca
n ge
nera
lise
and
synt
hesi
se p
rior
know
ledg
e an
d ex
per
ienc
e in
ord
er t
o ap
ply
them
in d
iffer
ent
sett
ings
and
nov
elsi
tuat
ions
. Th
ey a
re a
ble
to t
hink
crit
ical
lyab
out,
ref
lect
up
on,
and
eval
uate
suc
hkn
owle
dge
and
exp
erie
nce
with
in a
fram
ewor
k of
evi
denc
e-ba
sed
pra
ctic
e.
C2
Skill
s
The
awar
d ho
lder
sho
uld
be a
ble
to:
The
Prac
titi
on
er o
f A
pp
lied
Psy
cho
log
y(C
linic
al A
sso
ciat
e)
Dem
onst
rate
an
unde
rsta
ndin
g of
the
fac
tth
at s
ound
ap
plie
d p
sych
olog
y p
ract
ice
isba
sed
on c
linic
al a
nd r
esea
rch
skill
s th
aten
gage
and
em
erge
fro
m w
ork
with
clie
nts
and
syst
ems
base
d on
a s
cien
tist-
pra
ctiti
oner
and
ref
lect
ive
pra
ctiti
oner
mod
el.
This
inco
rpor
ates
a c
ycle
of
asse
ssm
ent,
for
mul
atio
n, in
terv
entio
n an
dev
alua
tion,
as
outli
ned
earli
er.
The
pra
ctiti
oner
of
Ap
plie
d Ps
ycho
logy
(Clin
ical
Ass
ocia
te)
is a
beg
inni
ng s
cien
tist
pra
ctiti
oner
who
wor
ks u
nder
the
sup
ervi
sion
of
a ch
arte
red
Clin
ical
Psyc
holo
gist
, w
ith a
sin
gle
clie
nt g
roup
with
a c
ircum
scrib
ed r
ange
of
pro
blem
s,in
clud
ing
typ
e an
d se
verit
y. S
uch
pra
ctiti
oner
s w
ork
larg
ely
with
in a
gree
din
terv
entio
n st
rate
gies
as
they
beg
in t
oen
gage
with
kno
wle
dge
at t
he f
oref
ront
of
thei
r ra
nge
of e
xper
tise.
With
in s
uch
aco
ntex
t, t
hey
deve
lop
the
abi
lity
to t
hink
criti
cally
abo
ut,
refle
ct u
pon
, an
d ev
alua
tesu
ch k
now
ledg
e an
d ex
per
ienc
e w
ithin
afr
amew
ork
of e
vide
nce-
base
d p
ract
ice.

page 25
Teaching, learning and assessment (Clinical Psychology and AppliedPsychology (Clinical Associate))
A prerequisite for enrolment on either a Clinical Psychology programme or an AppliedPsychology (Clinical Associate) programme is the achievement of the Graduate Basis forRegistration. Thus the knowledge and skills that form the starting point for a candidateare as set out in the Subject benchmark statement for psychology or its equivalent.
Detailed decisions about the strategies and methods for teaching, learning andassessment are for institutions to determine, but should ensure that the learningoutcomes associated with Clinical Psychology and Applied Psychology (Clinical Associate)programmes, respectively, can be achieved. Nonetheless, programmes must promote anintegrative approach to the application of theory and practice. Learning opportunitiesand assessment systems should facilitate the acquisition of the full range of professionalcompetencies appropriate to the respective programme. Fundamental to the basis uponwhich trainees are prepared for their professional career, is the provision of programmesof academic study and practice-based learning which lay the foundation for career-longprofessional development and lifelong learning, to support best professional practice andthe maintenance of professional standards.
Teaching and learning in Clinical Psychology
It is essential that programmes provide a holistic experience of training that enablestrainees to develop an integrated set of learning outcomes constituting a generic trainingin clinical psychology. Training should be provided as a collaboration between HEIs andclinical services and supervisors. An appropriate structure should be in place to facilitatethis. Selection criteria should be specified and should apply equally to all candidates.Programmes should be directed by appropriately qualified chartered Clinical Psychologists.
Programmes must provide a balanced and developmental set of academic, research andclinical experiences throughout training. The academic component needs to provide anintegrated curriculum supporting the clinical and research training. The research trainingneeds to be carefully planned and have sufficient time devoted to it to enable trainees toconduct research at a postgraduate level and to be in a position to contribute to theknowledge base of the profession. The clinical experience component of training needsto ensure the attainment of competence across the range of required experience.
It is important to recognise that the scope of Clinical Psychology is substantial, so thatinitial training provides a secure foundation encompassing the range of skills andknowledge demonstrated by the profession. Further skills and knowledge will need to beacquired through CPD appropriate to the specific employment pathways taken by newlyqualified psychologists in line with clinical governance and lifelong learning frameworks.
Clinical experience will be gained in service delivery systems that offer a coherent clinicalcontext. This will usually be a setting oriented towards a population defined by age (eg child, adult, older people), by special needs (eg learning disabilities, serious mentalhealth problems, health-related problems, substance misuse) or by a service deliveryfocus (eg psychological therapy). In addition, clinical experience will be gained in arange of service contexts (primary, secondary and tertiary care, in-patient, out-patient,community), with service delivery models ranging from independently organised workthrough to integrated interprofessional working.

page 26
Programmes will be delivered in collaboration with placement providers to reflectnational and local priorities. Trainees must undertake substantial pieces of clinical workover a substantial period of time in each of a range of settings, including primary,secondary and tertiary care environments, and with a range of client groups, both acuteand long term, and those with high dependency needs.
Trainees must gain competence in a variety of modes and types of work, including:
direct work
indirect, through staff and/or carers
staff training, supervision and consultancy
work within multidisciplinary teams and specialist service systems, including someobservation or other experience of change and planning in service systems
working in more than one recognised model of formal psychological therapy.
It is essential that supervision in clinical placements reflects the Committee on Training in Clinical Psychology guidelines on clinical supervision. Hence, trainees on clinicalplacements should receive a minimum of one hour individual supervision and threehours contact time per week. Facilities for trainees on placement must includeappropriate resources. The trainee experience in clinical placements must be monitoredregularly through appropriately timed visits by programme staff, under the direction of a Clinical Psychologist. It is essential that clinical supervisors have access to appropriatetraining in order to develop supervisory and appropriate related skills.
It is essential that research be integrated into practice through the inclusion of service-related research projects as well as a larger scale independent doctoral-level study. Thisstudy should be of a standard that is likely to be publishable in a peer reviewed journal.Adequate research supervision and advice must be available to support trainee research,in order to promote post-qualification practice that includes research activity throughconducting and facilitating research and applying research to inform practice.
Effective learning opportunities that underpin programme delivery require thedeployment of appropriately qualified clinical academic staff who maintain aninvolvement in regular professional activity relevant to the programme, including clinicalwork and research. Programmes must be delivered in effective collaboration betweenHEIs, placement providers and clinical supervisors. Opportunities for interprofessionallearning should be optimised.
Sufficient time must be allocated to all components of learning.
Opportunities for enhancement and appraisal of personal and CPD must be provided ina manner that positively encultures the student into the importance of CPD as a centralpart of professional practice.
Teaching and learning in Applied Psychology (Clinical Associate)
It is essential that programmes provide a holistic experience of training that enables traineesto develop an integrated set of learning outcomes specific to providing service needs for aspecific client group. Training should be provided as a collaboration between HEIs and
page 27
clinical services and supervisors. An appropriate structure should be in place to facilitate this.Selection criteria should be specified and should apply equally to all candidates.Programmes should be directed by appropriately qualified chartered Clinical Psychologists.
Programmes must provide a balanced and developmental set of academic, research andclinical experiences throughout training. The academic component needs to provide anintegrated curriculum supporting the clinical and research training. The research trainingneeds to be carefully planned and have sufficient time devoted to it to enable trainees toconduct research at postgraduate master's level and to be in a position to engage withrelevant aspects of the knowledge base of the profession. The clinical experiencecomponent of training needs to ensure the attainment of competence specific to therequired experience necessary for subsequent practice.
It is important to recognise that although the scope of Applied Psychology (ClinicalAssociate) is circumscribed to preparation for working with specific client groups withinpre-established protocols, the initial one year training, or part-time equivalent, mustnevertheless provide a secure foundation encompassing the identified range of skills andknowledge necessary to carry out these activities. Further skills and knowledge will needto be acquired through continuing professional development appropriate to the specificemployment pathways taken by the newly qualified in line with clinical governance andlifelong learning frameworks. This latter recognises that a number of these master'sgraduates may proceed to doctoral level training as their career progresses.
Supervised clinical experience will be gained in service delivery systems that offer acoherent clinical context pertinent to a particular client group and range of problems.This will usually be a setting oriented towards a single population defined by age (eg child, or adult, or older people) dependent upon the particular programme beingundertaken. Programmes will contain a strong psychological therapy component, againrelevant to a specific range of problems within a single client group under thesupervision of a Clinical Psychologist. Experience may be gained in a range of servicecontexts relevant to the needs of such single client groups.
Programmes will be delivered in collaboration with placement providers to reflectnational and local priorities for NHS Scotland. Trainees must gain appropriate experiencein clinical work in settings appropriate to the particular client group. This may include:
in-patient or other residential facilities
secondary health care
community and primary care.
Trainees must gain competence in a variety of modes and types of work, including:
direct supervised work
work within multidisciplinary teams and specialist service systems
working in at least one mode of formal psychological therapy.
It is important that the practice-experience of trainees is adequately and effectivelysupervised in every module to which practice pertains. The amount and type ofsupervision should be clearly stated in programme documents and be judged as
page 28
appropriate by approvals panels comprised of experts in the field. Facilities for traineeson placement must include access to sufficient resources. The trainee experience inclinical placements must be monitored regularly through appropriately timed visits byprogramme staff. It is essential that clinical supervisors have access to appropriatetraining in order to develop supervisory and appropriate related skills.
Following the model of the scientist practitioner, it is important that master's leveltrainees are introduced into this model by the inclusion a significant research element inprogramme design. It is essential that the research component is integrated into theprogramme in such a way that research and evaluation are seen as an integral part ofprofessional practice.
Effective learning opportunities that underpin programme delivery require thedeployment of appropriately qualified clinical academic staff who maintain aninvolvement in regular professional activity relevant to the programme, including clinicalwork and research. Programmes must be delivered in effective collaboration betweenHEIs, placement providers and clinical supervisors. Opportunities for interprofessionallearning should be entertained where appropriate.
Sufficient time must be allocated to all components of learning.
Opportunities for enhancement and appraisal of personal and professional developmentmust be provided.
Assessment (Clinical Psychology and Applied Psychology (Clinical Associate))
The evaluation of trainees must include assessments of academic, research and clinicalcompetence appropriate to doctoral level and master's level, respectively. The respectiveprogrammes must ensure that the assessment system promotes the learning outcomesidentified in each of the programme specifications, and can demonstrate that theselearning outcomes have been achieved. The assessment must give appropriate weightingto clinical and professional competence in the workplace.
The HEI must take responsibility for ensuring that there are adequate procedures toensure that trainees who are incompetent or whose behaviour is unethical do not obtaina qualification in Clinical Psychology or Applied Psychology (Clinical Associate),respectively.
Academic and practitioner standards (Clinical Psychology)
A Doctorate in Clinical Psychology is a vocational qualification as well as an academicaward, and as such, must prepare graduates for professional activities across widelydiffering fields. In particular, graduates must possess all the professional competencies tobe able to function as a qualified Clinical Psychologist and this represents the thresholdfor entry to the profession.
Newly qualified Clinical Psychologists should understand and embrace the core purposeand philosophy of the profession as described in the document prepared by the Divisionof Clinical Psychology of the BPS. They should be committed to reducing psychologicaldistress and enhancing and promoting psychological well-being through the systematic

page 29
application of knowledge derived from psychological theory and evidence. Their workwill be based on the fundamental acknowledgement that all people have the samehuman value and the right to be treated as unique individuals.
Thus award holders will have:
the skills, knowledge and values to develop working alliances with clients, includingindividuals, carers and/or services, in order to carry out psychological assessment;develop a formulation based on psychological theories and knowledge; carry outpsychological interventions; evaluate their work; and communicate effectively withclients, referrers and others, orally, electronically and in writing
the skills knowledge and values to work effectively with clients from a diverse rangeof backgrounds, understanding and respecting the impact of difference and diversityupon their lives
the skills, knowledge and values to work effectively with systems relevant to clients,including, for example, statutory and voluntary services, self-help and advocacygroups, user-led systems and other elements of the wider community
the skills, knowledge and values to work in a range of indirect ways to improvepsychological aspects of health and healthcare
the skills, knowledge and values to conduct research that enables the profession todevelop its knowledge base and to monitor and improve the effectiveness of its work
high-level skills in managing a personal learning agenda and self-care, and in criticalreflection and self-awareness that enable transfer of knowledge and skills to newsettings and problems.
The delivery and assessment of these outcomes is in accordance with the doctoral leveldescriptors specified in the frameworks for higher education qualifications. It is expectedthat the minimum duration of programmes will be three years full-time or part-timeequivalent, with at least 50 per cent of time allocated to supervised clinical practice. Thecompetencies attained are consistent with those described in the National OccupationalStandards for Applied Psychology.
Academic and practitioner standards (Applied Psychology (Clinical Associate))
A master's degree in Applied Psychology (Clinical Associate) is a vocational qualificationas well as an academic award, and as such, must prepare graduates for professionalactivity in the appropriate field and form of practice to which the programme pertains.Such graduates must possess the professional competencies to be able to function as amember of a team delivering psychological services as advised or referred by a charteredClinical Psychologist under whose clinical supervision they work.
Practitioners of Applied Psychology (Clinical Associate) should be committed to reducingpsychological distress and enhancing and promoting psychological well-being throughthe systematic application of knowledge derived from psychological theory and evidencepertaining to their particular field of practice. Their work will be based on thefundamental acknowledgement that all people have the same human value and theright to be treated as unique individuals.

page 30
Thus award holders will have:
the skills, knowledge and values to develop working alliances with clients, includingindividuals and carers, in order to carry out psychological assessment; develop aformulation based on psychological theories and knowledge; carry out psychologicalinterventions; evaluate their work; and communicate effectively with clients, referrersand others, orally, electronically and in writing
the skills knowledge and values to work effectively with a single client group from adiverse range of backgrounds, understanding and respecting the impact of differenceand diversity upon their lives
the skills, knowledge and values to work effectively with systems relevant to clients,including, for example, statutory and voluntary services, self-help and advocacygroups, user-led systems and other elements of the wider community
the skills, knowledge and values to conduct research that engages with and isinformed by the profession's knowledge base, to enable and improve theeffectiveness of their work and service delivery
developed skills in managing a personal learning agenda and self-care, and in criticalreflection and self-awareness that enable transfer of knowledge and skills to newsettings and problems.
The delivery and assessment of these outcomes is in accordance with master's leveldescriptors specified in the frameworks for higher education qualifications. It is expectedthat the minimum duration of programmes will be one full-time year or part-timeequivalent, with at least 50 per cent of such time allocated to supervised clinicalpractice. The competencies attained will be consistent with those in the subset describedby the Committee for the Training of Clinical Psychologists Accreditation Criteria forparticular client groups with a specific range of problems.

page 31
Acknowledgement
The Benchmarking Group wish to acknowledge the valuable work done by the UK clinicalpsychology benchmarking group as presented in Subject benchmark statements: Health careprogrammes Phase 2: Clinical psychology, produced by QAA. The Scottish BenchmarkingGroup for Clinical Psychology and Applied Psychology (Clinical Associate) have drawn onthe above work to remain congruent with a UK context, while also focusing upon a visionand framework that pertains to the needs of NHS Scotland.

page 32
Appendix
Clinical Psychology and Applied Psychology (Clinical Associate):Benchmarking Group membership (Scotland)
Pauline Adair, University of DundeeMalcolm Adams, BPS (UK), Membership and Professional Training BoardGeraldine Bienkowski, NES, Psychology Advisory GroupElizabeth Campbell, University of GlasgowGeorge Deans, BPS, DCP (Scotland)Terry Griffiths, NHS LothianBridget Hanna, NESCathy Kyle, NHS Ayrshire & ArranJohn Murphy, SEHD, Human Resources DirectorateMick Power, University of EdinburghIan Pullen, SEHDAnn Smyth, NESJudy Thomson, NHS YorkhillHugh Toner, NHS FifeDiane Waller, Health Professions Council (UK)
ChairKevin Power, NHS Tayside and University of Stirling
Supported byRob Coward, NESJohn Drummond, University of Dundee
QAA Scotland officersDavid BottomleyHeather Gibson

QA
A 109 05/06
QAA Scotland183 St Vincent Street GlasgowG2 5QD
Tel 0141 572 3420Fax 0141 572 3421Email [email protected] www.qaa.ac.uk

Mapping of Quality Assurance Agency Subject Benchmark Statement for Clinical Psychology against the generic standards of proficiency
QAA subject benchmark statement Standards of proficiency A1 Professional autonomy and accountability of the clinical psychologist
Maintain the standards and requirements of the BPS and DCP 1a.1 (with reference to HPC) Adhere to the BPS’s code of conduct, ethical principles and guidelines and the DCP professional practice guidelines
1a.1 (with reference to HPC)
Understand the legal and ethical responsibilities of clinical psychology practice including consent and confidentiality
1a.1, 1a.4
Demonstrate awareness of the legislative and national planning context of service delivery and clinical psychology practice
1a.1 (legal and ethical boundaries) The ‘national planning context’ is not included in the generic standards
Recognise the obligation to main fitness to practise and the need for continuing professional development
1a.8
Contribute to the development and dissemination of evidence based practice within professional contexts
2b.1 (evidence based practice, evaluation of practice, evaluation of research)
Recognise and cope with uncertainty, making informed judgements on complex clinical issues in the absence of complete data
2b.1, 2b.2 Uncertainty is not explicitly covered in the generic standards
Make appropriate clinical decisions 2b.2
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
1

QAA subject benchmark statement Generic Standards of proficiency
A2 Professional relationships Participate effectively in inter-professional and multi-agency approaches to health and social care
1b.2
Recognise professional scope of practice and make referrals, where appropriate
1a.6, 1a.8 (scope of practice) and 1b.1 (referrals)
Demonstrate understanding of consultancy models and the contribution of consultancy to practice
This is not included in the generic standards
Work with others to deliver effective healthcare 1b.1 and 1b.2 Understand the impact of difference, diversity and social inequalities and its implications for working practices
1a.1, 1a.2 This may not be sufficiently covered in generic standards
Work effectively with users and carers to facilitate their involvement in service planning and delivery
1b.1
Maintain appropriate records and make accurate reports 2b.5
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
2

QAA subject benchmark statement Standards of proficiency
A2 Personal and professional skills Demonstrate the ability to deliver high quality patient / client-centred care both as a solo practitioner and as a member of multidisciplinary and multi-agency teams
1b.2
Practise in an anti-discriminatory and anti-oppressive manner 1a.2 Draw upon clinical psychology, knowledge, theory and skills in order to make professional judgements
2b.2
Demonstrate high levels of research skills and scholarship 2b.1 The level of research skills and scholarship specific to the profession may not be covered in the generic standards
Work effectively at a high level of autonomy in complex and unpredictable situations, with awareness of the limits of their own competence, and accepting accountability to relevant professional and service managers
1a.6
Demonstrate self awareness and ability to work as a reflective practitioner
2c.2
Demonstrate a high level of communication skills in a style appropriate to specialist and non-specialist audiences
1b.3 (effective and appropriate communication skills) The generic standards do not specifically refer to specialist audiences
Initiate and respond to change in a flexible manner, demonstrating transferable skills
2b.2
Understand the importance and role of continuing professional development and engage in self directed learning that promotes professional development
1a.8
Manage the emotional and physical impact of their own practice This is not specifically covered in the generic standards, although
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
3

standard 1a.8 covers ‘fitness to practise’ in the round Understand the importance and role of supervision and demonstrate its appropriate use
This is not covered in the generic standards
Demonstrate self management skills and independence of thought and action
1a.6, 1a.7
Demonstrate culturally competent practice 1a.2, 1b.3
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
4
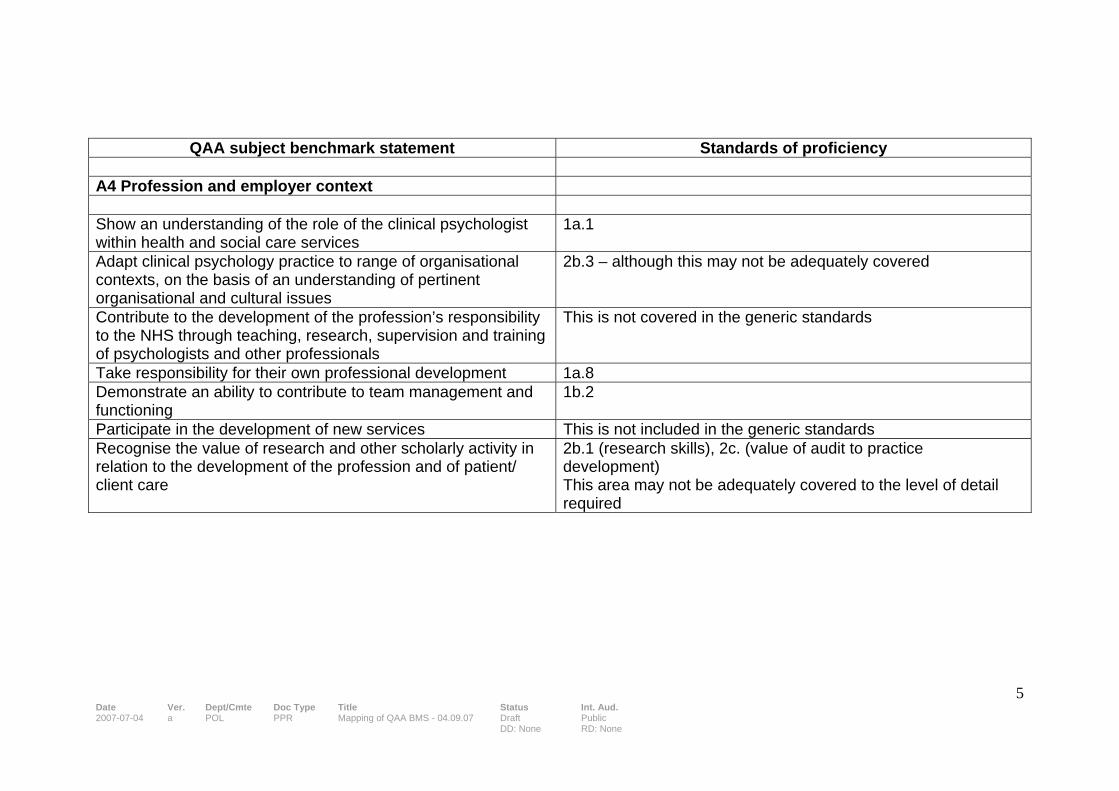
QAA subject benchmark statement Standards of proficiency
A4 Profession and employer context Show an understanding of the role of the clinical psychologist within health and social care services
1a.1
Adapt clinical psychology practice to range of organisational contexts, on the basis of an understanding of pertinent organisational and cultural issues
2b.3 – although this may not be adequately covered
Contribute to the development of the profession’s responsibility to the NHS through teaching, research, supervision and training of psychologists and other professionals
This is not covered in the generic standards
Take responsibility for their own professional development 1a.8 Demonstrate an ability to contribute to team management and functioning
1b.2
Participate in the development of new services This is not included in the generic standards Recognise the value of research and other scholarly activity in relation to the development of the profession and of patient/ client care
2b.1 (research skills), 2c. (value of audit to practice development) This area may not be adequately covered to the level of detail required
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
5
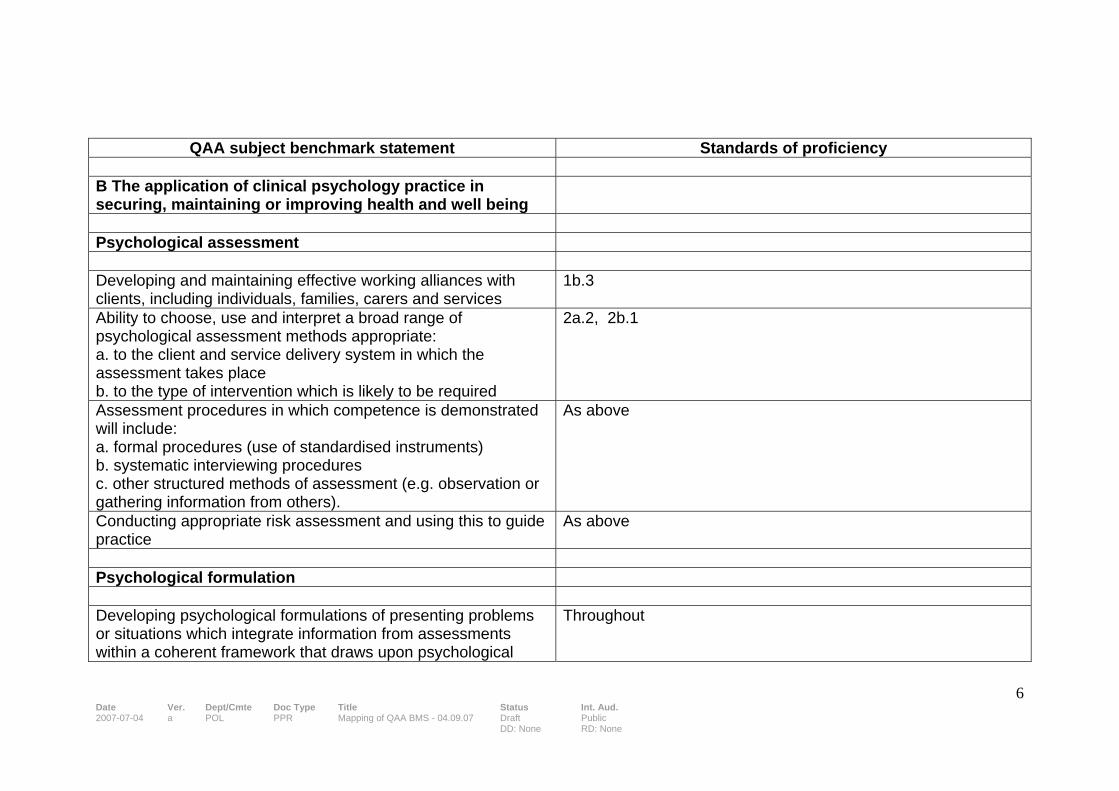
QAA subject benchmark statement Standards of proficiency
B The application of clinical psychology practice in securing, maintaining or improving health and well being
Psychological assessment Developing and maintaining effective working alliances with clients, including individuals, families, carers and services
1b.3
Ability to choose, use and interpret a broad range of psychological assessment methods appropriate: a. to the client and service delivery system in which the assessment takes place b. to the type of intervention which is likely to be required
2a.2, 2b.1
Assessment procedures in which competence is demonstrated will include: a. formal procedures (use of standardised instruments) b. systematic interviewing procedures c. other structured methods of assessment (e.g. observation or gathering information from others).
As above
Conducting appropriate risk assessment and using this to guide practice
As above
Psychological formulation Developing psychological formulations of presenting problems or situations which integrate information from assessments within a coherent framework that draws upon psychological
Throughout
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
6

theory and evidence which incorporates interpersonal, societal, cultural and biological factors. Using formulations with clients to facilitate their understanding of their experience
2b.1, 2b.2
Using formulations to plan appropriate interventions that take the client’s perspective into account
2b.3
Using formulations to assist multiprofessional understanding and communication, and the understanding of clients and their care
2a.3, 1b.2
Revising formulations in light of ongoing intervention and when necessary re-formulating the problem
2b.1
Psychological intervention On the basis of a formulation, implementing psychological therapy or other interventions appropriate to the presenting problem and to the psychological, cultural and social circumstances of the client, and to do this in a collaborative manner with:
• individuals; • couples, families, or groups; • teams/ services/ organisations
2b.4, 1b.
Implementing and recording interventions through, and with, other professions and/or with individuals who are formal (professional) carers for a client, or who care for a client by virtue of family or partnership arrangements
2b, 2b.5
Recognising when (further) intervention is unlikely to be helpful, and communicating this sensitively to clients and carers
2b.3, 1b.3
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
7

Evaluation and research Selecting and implementing appropriate methods to evaluate the effectiveness, acceptability and broader impact of interventions (both individual and organisational) and using this information to inform and shape practice. Where appropriate, this will also involve devising innovative procedures.
2b.1
Auditing clinical effectiveness 2c.1 Identifying gaps in the evidence base and, where such gaps exist, adapting established practice to meet the specific needs of service users. In such cases, ongoing evaluation of adaptations is critical and form the basis of new developments in theory and practice
2b.1 (research) This is not covered in the existing generic standards
The development of theory and practice in clinical psychology through research
Although 2b. covers research, this may not be adequately covered in the standards
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
8

QAA subject benchmark statement Standards of proficiency
C Knowledge, understand and skills that underpin the education and training of clinical psychologists
C1 Knowledge and understanding Systematic acquisition and understanding of a substantial body of knowledge, including theories and evidence concerning psychological development and psychological difficulties across the lifespan and their assessment and remediation. This should include theory and evidence at the forefront of the discipline relating to:
• wide breadth of presentations – from acute to enduring and from mild to severe;
• problems ranging from those with many biological causation to those emanating mainly from psychosocial factors;
• problems of coping/adaptation to adverse circumstances that are not themselves reversible by psychological intervention (e.g physical disability, physical illness, bereavement);
• clients from a range of backgrounds reflecting the demographic characteristics of the population;
• clients with significant levels of challenging behaviour; • clients across a range of levels of intellectual functioning
over a range of ages; • clients whose disability makes it difficult for them to
3a.1, 3a.2 The generic standards do not cover these areas to this level of detail
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
9

communicate; • carers and families; • social and contextual factors; • teamwork, service delivery systems, and the legislative
and policy frameworks. Detailed knowledge and understanding of research methods including:
• Research design and methods including small N designs and those methods, both quantitative and qualitative, that are most useful in the conduct of applicable clinical research including service evaluation
• Ethical issues in research • Statistical analysis including both exploratory and
hypothesis testing methods • Critical appraisal of published research • The undertaking of supervised research work involving
both a major project and also some smaller scale clinical evaluation
Research and audit are covered in 2b and 2c
The award holder will demonstrate the ability to complete an independent research project at doctoral level successfully. This will include the ability to conceptualise, design, carry out and communicate the results of research that is relevant to clinical psychological theory and practice and represents a contribution to the field
This is not covered in the existing generic standards
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
10

Analysis of mapping The initial mapping has identified the following areas where elements of the benchmark statements may not be adequately included in the existing generic standards. QAA Subject benchmark statement Notes Recognise and cope with uncertainty, making informed judgements on complex clinical issues in the absence of complete data
This area does not seem to be covered in the generic standards and it may be appropriate to add a profession-specific standard
Demonstrate understanding of consultancy models and the contribution of consultancy to practice
This is not covered in the generic standards. Is this area appropriate as a threshold ability or understanding rather than a particular occupational area or role?
Understand the impact of difference, diversity and social inequalities and its implications for working practices
1a.1 is about respecting the rights of patients and their role in the diagnostic and therapeutic process, whilst 1a.2 is about acting in a non-discriminatory manner. It may be that these standards are sufficient to cover this area
Work effectively with users and carers to facilitate their involvement in service planning and delivery
This is covered by 1b.1 ‘be able to work, where appropriate, in partnership with other professionals, support staff, service users and their relatives and carers’. However, depending on the focus in the profession, it could be helpful to highlight key elements of this approach. For example, in 2b.3 of the standards for physiotherapists we say ‘understand the need to agree the goals, priorities and methods of physiotherapy intervention in partnership with the service user’
Demonstrate high levels of research skills and scholarship Whilst research skills are covered in generic standard 2b.1, it might be helpful and necessary to drill down further. In the clinical scientists standards, the advanced nature of the research skills required are articulated in the profession-specific
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
11
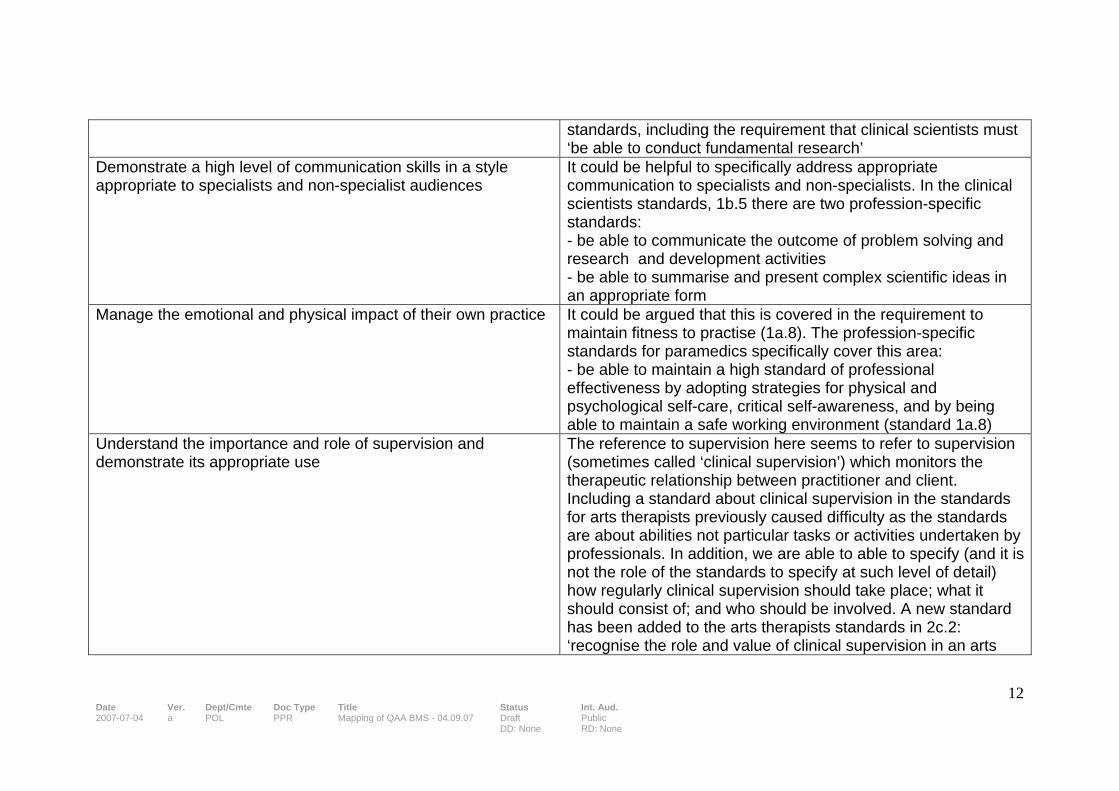
standards, including the requirement that clinical scientists must ‘be able to conduct fundamental research’
Demonstrate a high level of communication skills in a style appropriate to specialists and non-specialist audiences
It could be helpful to specifically address appropriate communication to specialists and non-specialists. In the clinical scientists standards, 1b.5 there are two profession-specific standards: - be able to communicate the outcome of problem solving and research and development activities - be able to summarise and present complex scientific ideas in an appropriate form
Manage the emotional and physical impact of their own practice It could be argued that this is covered in the requirement to maintain fitness to practise (1a.8). The profession-specific standards for paramedics specifically cover this area: - be able to maintain a high standard of professional effectiveness by adopting strategies for physical and psychological self-care, critical self-awareness, and by being able to maintain a safe working environment (standard 1a.8)
Understand the importance and role of supervision and demonstrate its appropriate use
The reference to supervision here seems to refer to supervision (sometimes called ‘clinical supervision’) which monitors the therapeutic relationship between practitioner and client. Including a standard about clinical supervision in the standards for arts therapists previously caused difficulty as the standards are about abilities not particular tasks or activities undertaken by professionals. In addition, we are able to able to specify (and it is not the role of the standards to specify at such level of detail) how regularly clinical supervision should take place; what it should consist of; and who should be involved. A new standard has been added to the arts therapists standards in 2c.2: ‘recognise the role and value of clinical supervision in an arts
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
12
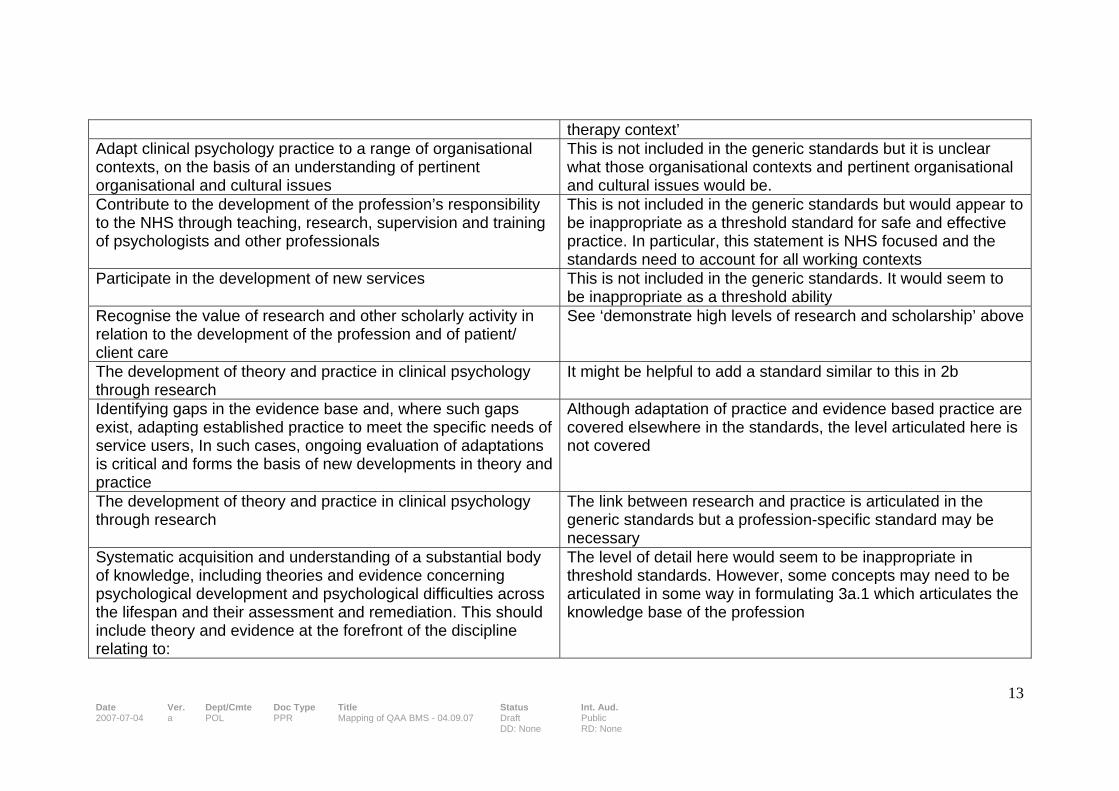
therapy context’ Adapt clinical psychology practice to a range of organisational contexts, on the basis of an understanding of pertinent organisational and cultural issues
This is not included in the generic standards but it is unclear what those organisational contexts and pertinent organisational and cultural issues would be.
Contribute to the development of the profession’s responsibility to the NHS through teaching, research, supervision and training of psychologists and other professionals
This is not included in the generic standards but would appear to be inappropriate as a threshold standard for safe and effective practice. In particular, this statement is NHS focused and the standards need to account for all working contexts
Participate in the development of new services This is not included in the generic standards. It would seem to be inappropriate as a threshold ability
Recognise the value of research and other scholarly activity in relation to the development of the profession and of patient/ client care
See ‘demonstrate high levels of research and scholarship’ above
The development of theory and practice in clinical psychology through research
It might be helpful to add a standard similar to this in 2b
Identifying gaps in the evidence base and, where such gaps exist, adapting established practice to meet the specific needs of service users, In such cases, ongoing evaluation of adaptations is critical and forms the basis of new developments in theory and practice
Although adaptation of practice and evidence based practice are covered elsewhere in the standards, the level articulated here is not covered
The development of theory and practice in clinical psychology through research
The link between research and practice is articulated in the generic standards but a profession-specific standard may be necessary
Systematic acquisition and understanding of a substantial body of knowledge, including theories and evidence concerning psychological development and psychological difficulties across the lifespan and their assessment and remediation. This should include theory and evidence at the forefront of the discipline relating to:
The level of detail here would seem to be inappropriate in threshold standards. However, some concepts may need to be articulated in some way in formulating 3a.1 which articulates the knowledge base of the profession
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
13
• wide breadth of presentations – from acute to enduring and from mild to severe;
• problems ranging from those with many biological causation to those emanating mainly from psychosocial factors;
• problems of coping/adaptation to adverse circumstances that are not themselves reversible by psychological intervention (e.g physical disability, physical illness, bereavement);
• clients from a range of backgrounds reflecting the demographic characteristics of the population;
• clients with significant levels of challenging behaviour; • clients across a range of levels of intellectual functioning
over a range of ages; • clients whose disability make sit difficult for them to
communicate; • carers and families; • social and contextual factors; • teamwork, service delivery systems, and the legislative
and policy frameworks Detailed knowledge and understanding of research methods including:
• Research design and methods including small N designs and those methods, both quantitative and qualitative, that a most useful in the conduct of applicable clinical research including service evaluation
• Ethical issues in research
Please see previous notes regarding research It might be necessary to add a standard around ethical issues in research – although it should be noted that more general principles about ethical behaviour, in research and in all other areas of professional life, are articulated in the standards of conduct, performance and ethics
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
14

• Statistical analysis including both exploratory and hypothesis testing methods
• Critical appraisal of published research • The undertaking of supervised research work involving
both a major project and also some smaller scale clinical evaluation
The award holder will demonstrate the ability to complete an independent research project at doctoral level successfully. This will include the ability to conceptualise, design, carry out and communicate the results of research that is relevant to clinical psychological theory and practice and represents a contribution to the field
The standards necessary for safe and effective practice and the level of an academic award are two separate matters (please see paper “Background and context” – PLG 4th September 2007)
Date Ver. Dept/Cmte Doc Type Title Status Int. Aud. 2007-07-04 a POL PPR Mapping of QAA BMS - 04.09.07 Draft
DD: None Public RD: None
15