health and psychosocial needs of lgbt older adults study final report... · health and psychosocial...
TRANSCRIPT
FINAL REPORT
Health and Psychosocial Needs of LGBT Older Adults
Mark Brennan‐Ing, PhD1, Stephen E. Karpiak, PhD2, and Liz Seidel, MSW3
AIDS Community Research Initiative of America (ACRIA)
230 West 38th Street, 17th Floor
New York, NY 10018
Center on HIV & Aging
Prepared for:
3656 North Halsted, Chicago, IL 60613-5974
1 Mark Brennan‐Ing, PhD, Senior Research Scientist, ACRIA, 230 West 38th Street, New York, NY 10018. (212) 924‐
3934 ext. 131; (212) 924‐3936 [fax]; [email protected] . 2 Stephen E. Karpiak, PhD, Associate Director for Research, ACRIA. [email protected] . 3 Liz Seidel, MSW, Research Scientist, ACRIA, [email protected] .
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
2 | P a g e A C R I A C E N T E R O N H I V & A G I N G
Contents
EXECUTIVE SUMMARY ................................................................................................ 4
METHODOLOGY NOTES ............................................................................................ 10
INTRODUCTION ........................................................................................................... 11
DEMOGRAPHICS .......................................................................................................... 13
EDUCATION, WORK STATUS, & INCOME ............................................................. 15
RELATIONSHIPS, PARTNER STATUS & LIVING ARRANGEMENTS .............. 17
RELIGIOUS AFFILIATION, PARTICIPATION & SUPPORT ............................... 20
HEALTH STATUS & MEDICAL TREATMENT ....................................................... 20
HIV/AIDS STATUS AND SOURCE OF INFECTION ............................................... 22
VISION & HEARING FUNCTION ............................................................................... 23
MENTAL HEALTH ........................................................................................................ 24
LIFETIME & CURRENT SUBSTANCE USE.............................................................. 25
FUNCTIONAL ABILITY ............................................................................................... 26
SEXUAL ACTIVITY, HEALTH & RISK ..................................................................... 28
SOCIAL SUPPORTS FROM FAMILY, FRIENDS & NEIGHBORS ........................ 34
CAREGIVING ................................................................................................................. 41
USE OF FORMAL SERVICES ...................................................................................... 43

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
3 | P a g e A C R I A C E N T E R O N H I V & A G I N G
BENEFITS & ENTITLEMENT PROGRAM PARTICIPATION .............................. 49
BARRIERS TO SERVICES ........................................................................................... 50
NEED FOR SERVICES IN THE PREVIOUS YEAR & UNMET NEEDS ................ 52
CONCLUSIONS & IMPLICATIONS ............................................................................ 55
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
4 | P a g e A C R I A C E N T E R O N H I V & A G I N G
EXECUTIVE SUMMARY
This research study provides one of the most comprehensive descriptions of the health, well‐being and social context of Lesbian, Gay, Bisexual, and Transgender (LGBT) older adults. This effort describes the characteristics of an aging LGBT population residing in Chicago, IL. These data should be used to facilitate policy‐making and program decisions to address the current and future needs of these individuals. The study provides in‐depth data on the health status of the aging LGBT community, including sexual health and concomitant risk behaviors, as well as the challenges of living with HIV. Detailed information was collected on social networks which are critical sources of support for an aging population, regardless of sexual identity. These older LGBT adults will also need to access community‐based formal services as they age. Consequently, this study examines the service utilization patterns and the service needs of this older LGBT group, including unmet need in the past year.
The sample of just over 200 individuals had an average age of 60, 71% were men, 24% were women,
and 5% were transgender or intersex. One‐third reported being HIV‐positive and 94% of this group
were men. Those who were HIV‐positive reported an average age of 55 years, whereas those who
were HIV‐negative were older, having an average age of 62.
• Eighty‐percent of the sample identified as gay or lesbian, 14% as bisexual, and 5% as
queer/questioning.
• One‐third was Black or African American (32%), with the remaining 62% being primarily White.
• Over half of the sample had a college degree or post‐graduate education.
• In terms of work status, 29% were currently working, 13% were unemployed, and 28% were
retired. Nearly one‐third were on disability.
• A sizeable minority were experiencing income inadequacy, with 15% reporting that they did not
have enough money to cover expenses, and an additional 46% just managing to get by.
• Forty‐two percent were home owners and 46% renters, comparable to the 44% home
ownership rate in Chicago obtained from the 2010 Census.
• The majority (55%) indicated that they were not currently in a relationship and 62% reported
living alone.
• Older LGBT adults reported primarily Protestant (23%) or Catholic (19%) religious affiliations,
while 24% reported no affiliation. Nearly two‐in‐five older LGBT adults said that they turned to
their religious congregations for support.
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
5 | P a g e A C R I A C E N T E R O N H I V & A G I N G
The majority (76%) of the sample rated their health as good or excellent. The older LGBT adults with
HIV, though younger, reported significantly more health problems on average.
• Most (57 %) accessed care from a private doctor/clinic and almost 1/3 received heath services
from a public clinic or hospital.
• Almost 60% indicated having at least a little trouble with vision and 37% reported having at least
a little trouble with hearing.
• Almost half of the HIV+ group were presently smoking compared to 13% for those who were not
positive.
• Current use of alcohol (63%) and pain killers (25%) did not differ significantly by HIV status.
• Twenty‐percent of the sample reported that they were currently in recovery for a drug or
alcohol problem.
• Over 1/3 evidenced having moderate levels of depressive symptoms and 20% had severe
depressive symptomatology. Older LGBT adults with HIV were nearly twice as likely to report
severe depressive symptoms compared to the non‐infected (29% and 14%, respectively).
Among the 71 study participants who were HIV+, the average time since HIV diagnosis was 15 years.
Almost 40% had been diagnosed with HIV in the last 10 years with the majority having been infected
through unprotected anal intercourse.
• Half of this group had received an AIDS diagnosis.
• Nearly all (97%) were on antiretroviral therapy and the majority reported CD4 counts over 500
indicating their HIV infection was well controlled.
On average, older LGBT adults reported 11 people in their social networks, consisting of parents,
family members, friends and neighbors. However, as documented in previous research, older LGBT
adults tend to have friend‐centered networks consisting of “families‐of‐choice” and have less
involvement with biological family members compared to their heterosexual peers.
• Friends were the most likely to be able to provide assistance with day‐to‐day tasks as well as
provide emotional support and advice.

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
6 | P a g e A C R I A C E N T E R O N H I V & A G I N G
• Older LGBT adults were much more likely to report receiving emotional support as compared to
help with instrumental tasks (43% to 56%).
• Over one‐quarter (27%) of older LGBT adults indicated that they and their neighbors helped
each other on a regular basis.
• The older LGBT adults who were HIV+ were significantly less likely than those who were HIV‐ to
perceive that emotional support was available all or most of the time. The HIV+ group was also
significantly less likely to indicate having received all the emotional support they needed in the
past year.
• Over 80% of the study sample said they did not currently need or use caregiving assistance.
About 20% of the older adults with HIV indicated they could use caregiving support.
• Nearly one‐quarter had provided caregiving assistance to someone during the past 5 years.
This study is one of the first to examine the sexual health of older LGBT adults. Sixty‐nine percent
were sexually active during the past year. Those under age 60 were more likely to report being
sexually active compared to those who were older. Those living with HIV had significantly more sexual
relationships when compared to those who were not HIV infected.
• Older LGBT adults tended to be involved with a partner who was younger (64%).
• Older adults with HIV were significantly more likely to indicate sex was extremely important as
compared to those without HIV, but there were no differences between groups in terms of how
often they thought about sex.
• About 1/3 said that their frequency of sexual activity was what they expected and 60% reported
not having sex as often as desired.
• Forty‐one percent of older LGBT adults indicated that they had avoided sexual activity, either
because of lack of interest or physical problems (e.g., erectile dysfunction).
• In terms of safe sexual practices, approximately one‐third never used condoms during either
anal or vaginal intercourse.
• When asked why they would engage in unprotected sex, 14% of those with HIV said because
they were depressed, while only 2% of those without HIV gave that as a reason.
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
7 | P a g e A C R I A C E N T E R O N H I V & A G I N G
The study examined the utilization and satisfaction with services at the Center on Halsted as well as
those at local government offices and agencies, HIV‐related services and AIDs Service Organizations
(ASOs), health‐related services, and other older adult community‐based services.
• The most frequently used government services included the Social Security Office (43%),
Department for Family and Support Services, Senior Division/Department on Aging (27%),
Housing Authority (21%) and Medicare and Medicaid Offices (21% and 20%, respectively). Use of
government offices and agencies was greater by the HIV+ older adult.
• The HIV+ older adults as expected used more services at AIDS service organizations and HIV‐
related CBO services.
• There were only two instances where HIV status was significantly related to use of health and
long‐term care services. Older HIV+ adults were significantly more likely to have used case
management (61%) as compared to those without an HIV diagnosis (12%). Also, one‐in‐five HIV+
adults used drug and alcohol treatment/recovery in the past year as compared to 8% among
non‐HIV infected older LGBT adults.
• Senior centers were the most frequently mentioned other older adult community based service
(25%). Clergy, meal/nutrition programs, and legal services were used by about one‐in‐five older
LGBT adults during the previous year.
• Legal services were used by HIV+ people at a rate (32%) twice that of the HIV‐ group (15%).
• The most frequently utilized service provided by COH was the SAGE Congregate Meal Program
(36%) followed by SAGE social and education programs (26%). Approximately one‐in‐ten used
HIV support groups, mental health supportive services, or legal services (11%).
• The non‐HIV infected older LGBT adults were more likely to use SAGE programming at COH,
which may be related to the greater average age in this group.
• Overall, satisfaction with COH services was high with the most highly rated service being the
computer technology center, followed by SAGE social and educational programs, and SAGE
congregate meals.
• When asked what additional services they would like to see COH provide, the most frequently
mentioned were assistance with housing and employment issues, more opportunities for
socialization, and more programs aimed specifically at women.

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
8 | P a g e A C R I A C E N T E R O N H I V & A G I N G
Older LGBT adults were most likely to indicate using Medicare coverage (45%) followed by private
health insurance (43%).
• Approximately one‐quarter were enrolled in Medicaid and Food Stamps and about one‐in‐five
reported income support either through Supplemental Security Income (SSI) or Social Security
Disability (SSD).
• Only about one‐in‐ten had purchased long‐term care insurance, and fewer (3%) had private
disability coverage.
• Although 14% had served in the armed forces, only 7% received health care coverage through
the Veterans Administration (VA).
• Older adults with HIV were more likely to access Medicaid and Food Stamps (49% and 41%,
respectively) as compared to the non‐HIV positive group (16% and 18%). A similar pattern was
seen when receiving income support in the form of SSI (30% vs. 18%, respectively) or SSD (43%
vs. 10%, respectively).
Fifty‐eight percent of the sample reported at least one barrier to community‐based services. Older
LGBT adults with HIV reported significantly greater number of barriers to services, on average, as
compared with their non‐infected peers (3.9 vs. 2.2, respectively).
• Service barriers included: 1) they did not think they would be eligible to receive free services
(43%); 2) worry about the cost of services (32%); and 3) knowledge of available services and
their location (36% and 24%, respectively).
• Almost 30% thought getting services was confusing and/or difficult and a quarter thought that
they would have to wait too long.
• The most frequently mentioned organizational barrier was that staff was unhelpful or seemed
unmotivated (21%).
• Stigma and discrimination issues were mentioned by approximately one‐in‐ten, namely, feeling
that staff did not like people like themselves or that they would not receive services if they tried.
• HIV stigma also appears to be an issue, with one‐in‐five HIV+ older LGBT adults feeling “staff
didn’t like people like them” as compared with only 6% of the non‐HIV diagnosed group.
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
9 | P a g e A C R I A C E N T E R O N H I V & A G I N G
• Older HIV+ LGBT adults were also more likely to cite contextual issues, such as disclosure of their
HIV status (18%), difficulty in making or keeping appointments (13%) and childcare issues (9%)
as barriers to care.
Older LGBT adults were asked about their need for services in the past year from a list of commonly
utilized health and social services, whether their needs had been met, and if so, who provided the
help (e.g., family, community‐based organization).
• The average number of services needed in the past year was 2.5 (SD=2.2) and the average
number of unmet needs was 0.6 (SD =0.9); this did not differ significantly by HIV status.
• Half the sample identified socialization as their highest unmet need followed by about 1/4 who
noted one of the following; getting to medical appointments, post‐hospital care, counseling and
someone to call or visit regularly.

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
10 | P a g e A C R I A C E N T E R O N H I V & A G I N G
METHODOLOGY NOTES
Recruitment of this convenience sample took place in Chicago, primarily at the Center on Halsted but also at various AIDS Service Organizations, health fairs and community events throughout the city. To qualify for participation an individual had to identify as lesbian, gay, bisexual or transgender (LGBT), be 50 years of age or older and speak English as their primary language. Recruitment yielded 233 participants, resulting in 211 usable surveys. Participants provided informed consent prior to data collection. The survey instrument was self‐administered by hand using a printed copy. On average, participants took 45 to 60 minutes to complete the survey. After completing the survey they were debriefed and thanked for their participation. As an incentive participants received a $25 gift card for taking part in this research project. Research methods and materials were evaluated and approved by the Copernicus Group Independent Review Board (IRB).
The survey instrument obtained information on the following areas: (1) demographic characteristics; (2) HIV/AIDS status; (3) physical conditions; (4) informal social supports; (5) caregiving (both receiving and providing care); (6) formal service utilization; (7) mental health; (8) substance use; (9) sexual behaviors; (10) health‐related quality of life; and (11) religion/spirituality. Whenever possible standardized measures with known psychometric properties were used to insure validity and for comparison with other published data. Questions were developed based on items in Research on Older Adults with HIV (ROAH) 4 study, National Social Life, Health and Aging Project (NSHAP)5, and the Caregiving among Older Lesbian, Gay, Bisexual and Transgender New Yorkers study6. When noted in the text, ‘significant’ refers to statistically significant differences at the p <.05 level or greater.
4 Brennan, M., Karpiak, S.E., Shippy, R.A., & Cantor, M.H.(Eds.) (2009). Research on Older Adults with HIV: An in-depth examination
of an emerging population. New York: Nova Science Publishers. 5 Lindau, S. T., Schumm, L. P., Laumann, E. O., Levinson, W., O’Muircheartaigh, C. A., & Waite, L. J. (200&). A study of sexuality
and health among older adults in the United States. New England Journal of Medicine, 357, 762-74. 6 Cantor, M.H., Brennan, M., & Shippy, R.A. (2004). Caregiving among Older Lesbian, Gay, Bisexual and Transgender New Yorkers.
Washington, DC: The National Gay and Lesbian Task Force Policy Institute.
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
11 | P a g e A C R I A C E N T E R O N H I V & A G I N G
INTRODUCTION
The health, well‐being and social networks of the older Lesbian, Gay, Bisexual, and Transgender (LGBT) population are understudied. As people age they rely on the informal supports in their network for caregiving. In the United States most caregiving is provided by partners and children; LGBT older adults are more likely to live alone and less likely to have children than older heterosexuals. Although significant numbers of LGBT individuals give and receive caregiving from their family of origin some LGBT individuals have been ostracized by their family. Research suggests that LGBT persons are more likely to rely on friends, sometimes referred to as the family of choice, for caregiving and this may prove problematic as friends in the network age and also require assistance. One study of LGBT older adults found that a third of those without partners did not know who would care for them if they needed assistance.7 Without traditional caregivers, these aging adults may rely increasingly on formal support services that may not be ready to meet the needs of LGBT older adults.
Older adult sexuality is often ignored in research despite significant rates of sexual activity in this population. In 2006 the National Health Social Life, Health and Aging Project provided comprehensive information on the sexual behaviors of older adults but did not specifically address LGBT older adults; leaving a need to look specifically at the sexual behavior, satisfaction, and barriers to sexual expression among LGBT older adults. As the rate of substance abuse in the LGBT community remains high, it is also important to further examine substance use, its relationship to sexual activity including sexual risk behaviors.
HIV still disproportionately affects the LGBT community. HIV is now a chronic and manageable
disease that may be further complicated by the comorbidities associated with aging. But our research and that of others shows that today’s older HIV population finds itself again disconnected from family and again facing the challenge of stigmatization. In order to age successfully they will need long‐term caregivers. The combined management of HIV/AIDS and age‐related comorbidities will have a profound impact on an already challenged health care delivery system. The need for caregiving and its critical role in health care management is evident. This is a population at risk. As HIV/AIDS affects greater numbers of older adults, their informal support networks will be challenged to provide needed instrumental assistance and emotional support as they adapt to life with multiple chronic illnesses (e.g., arthritics, diabetes, cardiac disease) that take their place alongside the life‐threatening illness of HIV. Research data supports the conclusions that many in the growing ranks of older adults with HIV, who will be without informal caregivers, will find themselves wholly dependent on an already frayed formal care and services safety net. There is a clear need to better understand the existing social networks of these at risk older adults in order to preserve and expand that safety net to meet the needs as they age with HIV.
Lastly, given the inadequate informal social networks of many LGBT older adults and their expected reliance on the systems of formal, community‐based organizations and supports, it is
7 Met Life Mature Market Institute, Lesbian and Gay Aging Issues Network of the American Society on Aging, and Zogby International,
(2006). Out and aging: The MetLife study of lesbian and gay baby boomers. Retrieved January 1, 2007 from: http://www.metlife.com/assets/cao/mmi/publications/studies/mmi-out-aging-lesbian-gay-retirment.pdf .
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
12 | P a g e A C R I A C E N T E R O N H I V & A G I N G
imperative that we have a better understanding of service utilization in this community. What services are used? What services are needed? And what are the perceived barriers to services in the community? These data will help policy makers, program planners and service providers meet the needs of LGBT older adults and facilitate their successful aging in the community. Study Purpose
The purpose of this study is to better understand the health and psychosocial needs of the older LGBT population in Chicago as well as differences and similarities between LGBT older adults and LGBT older adults with HIV. Given what is known about the fragility of the informal networks of many of these older adults, it is imperative to gain an understanding of the integration of the systems of formal and informal social care. The goals of this cross‐sectional survey are to provide data necessary for policy makers and program planners to best meet the real needs of this population as described below:
1. To assess the health status of LGBT older adults including physical and mental health problems, health‐related quality‐of‐life, HIV status, and sexual health.
2. To assess in detail the informal social support networks and other caregiving resources that are available to the community of LGBT older adults in Chicago.
3. To determine what resources are accessed within a LGBT Community Center and which services are accessed in the larger community
4. To examine the extent of unmet need for formal services and barriers to service use among LGBT older adults.
5. To examine similarities and differences in use of services and barriers to service use of HIV‐positive LGBT older adults and HIV‐negative LGBT older adults.
6. To examine the sexual behaviors, sexual satisfaction and sexual difficulties among LGBT older adults.
AIDS Com
13 | P a g
DEMOG
The curre(n=71) repthe remaiwho repowith the Hindividualon HIV sta
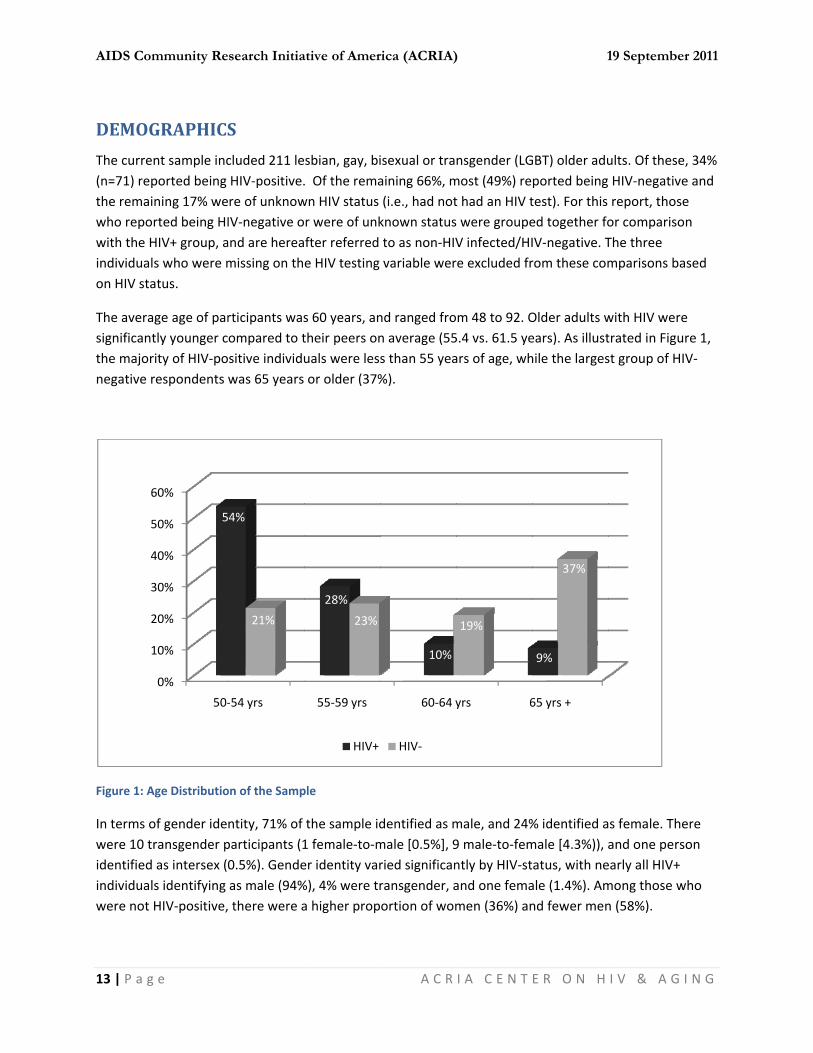
The averasignificantthe majornegative r
Figure 1: A
In terms owere 10 tidentifiedindividualwere not
1
2
3
4
5
6
mmunity Re
g e
GRAPHICS
nt sample incported being ining 17% werted being HIHIV+ group, als who were matus.
age age of partly younger crity of HIV‐porespondents
Age Distributio
of gender ideransgender p as intersex (0ls identifying HIV‐positive,
0%
10%
20%
30%
40%
50%
60%
50‐
5
search Initia
S
cluded 211 leHIV‐positive.re of unknowIV‐negative oand are hereamissing on th
rticipants wasompared to tsitive individuwas 65 years
on of the Samp
ntity, 71% of participants (10.5%). Gendeas male (94% there were a
‐54 yrs
4%
21%
ative of Amer
sbian, gay, bi. Of the remawn HIV statusr were of unkfter referred e HIV testing
s 60 years, antheir peers onuals were les or older (37%
ple
the sample id1 female‐to‐mer identity var%), 4% were tra higher prop
55‐59 yrs
28%
23%
HIV+
rica (ACRIA)
A C R
isexual or traaining 66%, m(i.e., had notknown statusto as non‐HIVvariable wer
nd ranged fron average (55s than 55 yea%).
dentified as mmale [0.5%], 9ried significanransgender, aortion of wom
60‐64 y
10%
HIV‐
)
I A C E N T
nsgender (LGmost (49%) ret had an HIV t were groupeV infected/HIre excluded fr
m 48 to 92. O5.4 vs. 61.5 years of age, wh
male, and 24%9 male‐to‐femntly by HIV‐stand one femamen (36%) an
yrs 6
19%
1
E R O N H
GBT) older aduported beingtest). For this ed together foIV‐negative. Trom these com
Older adults wears). As illusthile the larges
% identified amale [4.3%)), aatus, with neale (1.4%). Amnd fewer men
65 yrs +
9%
37%
19 Septembe
I V & A G
ults. Of these HIV‐negativereport, thoseor comparisoThe three mparisons ba
with HIV weretrated in Figust group of HI
s female. Theand one persearly all HIV+ mong those wn (58%).
r 2011
I N G
, 34% e and e n
ased
e re 1, V‐
ere on
who

AIDS Com
14 | P a g
Figure 2: G
Sexual idelesbian, 1identified
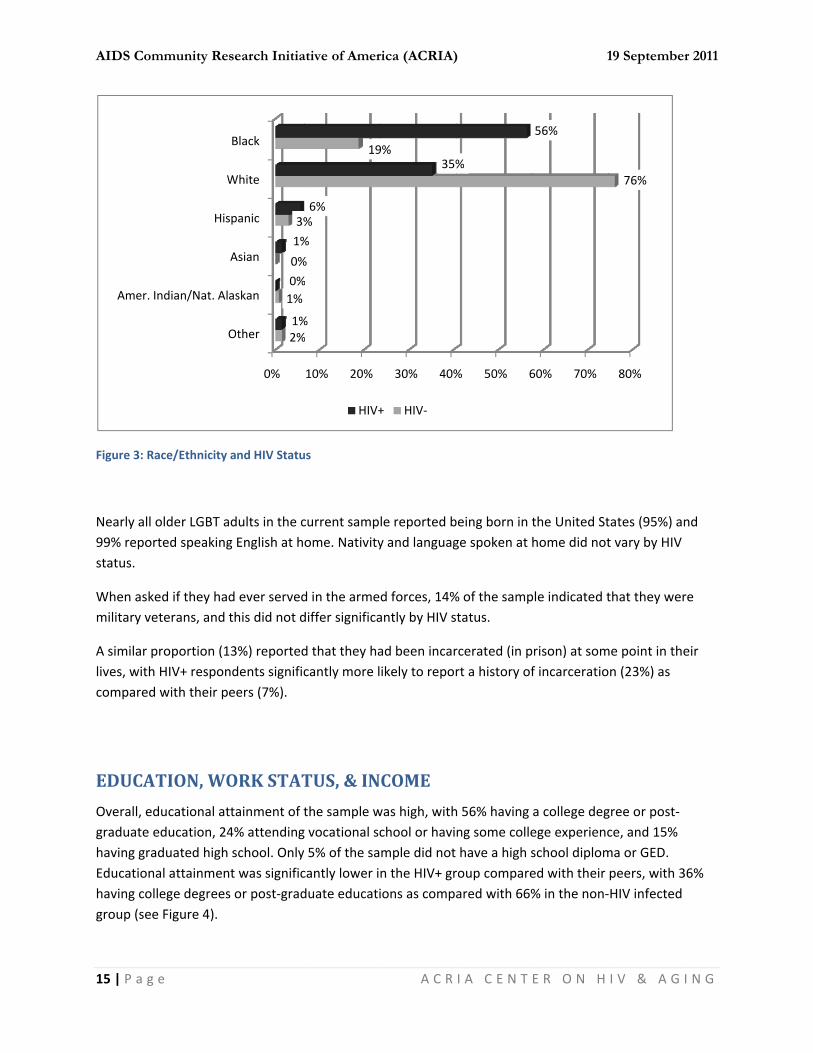
With regawere BlacHispanics Alaskans aHIV‐statuBlacks or (35%). In tAmerican
Male‐t
Femal
mmunity Re
g e
Gender Identity
entity did not4% as bisexu as heterosex
ard to race/etck or African Acomprised 4and “other” rs, reflecting tAfrican Amerthe non‐HIV is (19%).
0%
Intersex
to Female
e‐to Male
Female
Male
search Initia
y by HIV Statu
t differ significal, 3% as quexual.
thnicity, apprAmerican (32% of the samraces making the disproporricans were thinfected grou
20%
1%
4%
1%
0%
4%
0%
1%
ative of Amer
us
cantly by HIVer, and 2% as
oximately on%), with the ple, with Asiaup 1% or fewrtionate impahe majority inup, the majori
% 40
3
HIV+
rica (ACRIA)
A C R
‐status. Eights questioning
e‐third of oldremainder beans/Asian Amwer of participct of HIV in con the HIV‐posity were Whit
0% 60
36%
+ HIV‐
)
I A C E N T
ty‐percent of g. Three transg
der LGBT oldeeing primarilymericans, Amepants. Race/eommunities ositive group (5te (76%), follo
0% 8
58%
1
E R O N H
the sample idgender indivi
er adults in thy White or Caerican Indiansethnicity varieof color as sh56%), followeowed by Blac
80%
19 Septembe
I V & A G
dentified as gduals (2%)
e present samucasian (62%s and Native ed significantown in Figureed by Whites ks/African
100%
94%
r 2011
I N G
gay or
mple %).
tly by e 3.
AIDS Com
15 | P a g
Figure 3: R
Nearly all 99% repostatus.
When askmilitary ve
A similar plives, withcompared
EDUCA
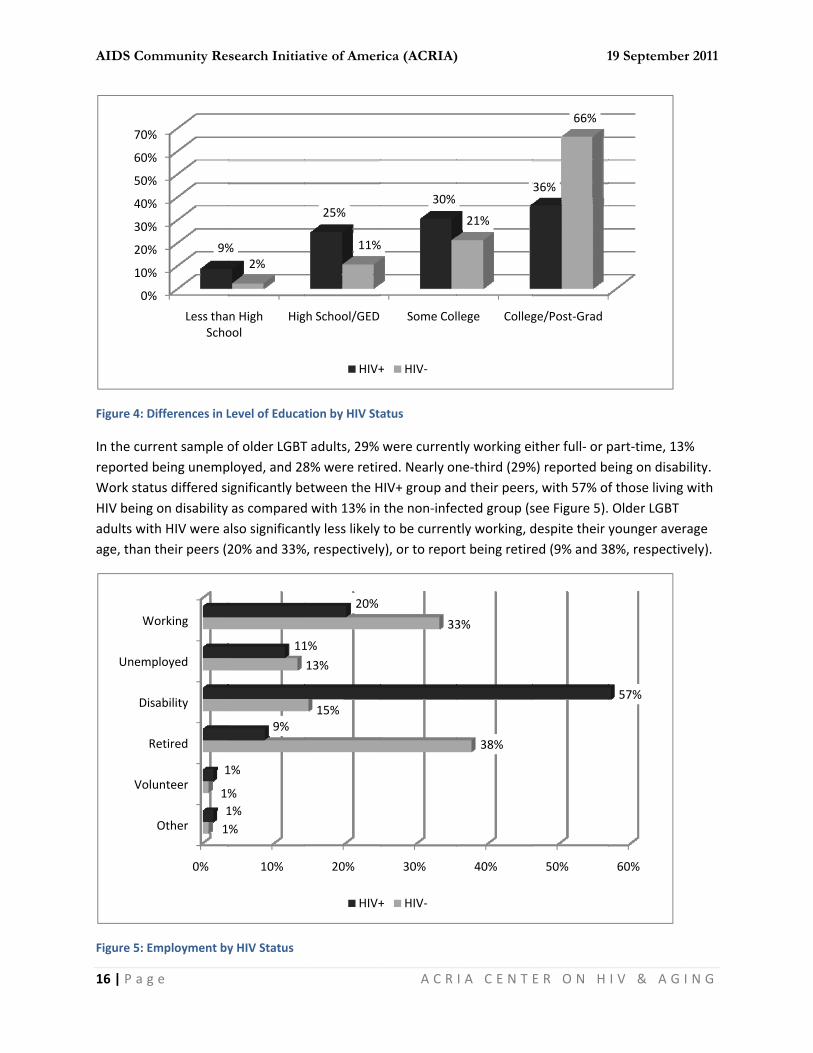
Overall, egraduate having graEducationhaving cogroup (se
Amer.
mmunity Re
g e
Race/Ethnicity
older LGBT arted speaking
ked if they haeterans, and
proportion (1h HIV+ respond with their p
ATION, WO
ducational ateducation, 24aduated highnal attainmenllege degreese Figure 4).
Indian/Nat. Al
His
W
search Initia
and HIV Statu
adults in the cg English at h
d ever servedthis did not d
13%) reportedndents significeers (7%).
ORK STAT
ttainment of t4% attending school. Onlynt was significs or post‐grad
0%
Other
askan
Asian
spanic
White
Black
2%
1%
0%
3%
1%
0%
1%
ative of Amer
us
current sampome. Nativity
d in the armediffer significa
d that they hacantly more l
TUS, & IN
the sample wg vocational sc 5% of the sacantly lower iduate educati
10% 20%
%
%
%
19
%
%
%
6%
HIV+
rica (ACRIA)
A C R
le reported by and languag
d forces, 14%antly by HIV s
ad been incarikely to repor
COME
was high, withchool or havimple did not n the HIV+ grions as compa
30% 40%
9%35%
+ HIV‐
)
I A C E N T
being born in tge spoken at h
% of the samptatus.
rcerated (in prt a history of
h 56% having ng some collehave a high sroup compareared with 66%
% 50% 6
%
1
E R O N H
the United Sthome did not
ple indicated t
rison) at somf incarceratio
a college degege experiencschool diplomed with their % in the non‐
60% 70%
56%
19 Septembe
I V & A G
tates (95%) ant vary by HIV
that they wer
me point in theon (23%) as
gree or post‐ce, and 15% ma or GED. peers, with 3‐HIV infected
80%
76%
r 2011
I N G
nd
re
eir
36%
AIDS Com
16 | P a g
Figure 4: D
In the curreported Work statHIV beingadults witage, than
Figure 5: E
0%
10%
20%
30%
40%
50%
60%
70%
Vol
R
Dis
Unem
W
mmunity Re
g e
Differences in L
rrent sample obeing unemptus differed sig on disability th HIV were atheir peers (2
Employment by
%
%
%
%
%
%
%
%
Less thaScho
9%
0%
Other
unteer
Retired
sability
ployed
Working
1
1%1
1
search Initia
Level of Educa
of older LGBTployed, and 28ignificantly beas compared
also significan20% and 33%
y HIV Status
n High ool
Hig
%2%
10%
%
%1%
1%
9%
11
ative of Amer
tion by HIV St
T adults, 29% 8% were retiretween the Hd with 13% inntly less likely %, respectively
gh School/GED
25%
11%
HIV+
20%
15%
13%
1%
20%
HIV+
rica (ACRIA)
A C R
atus
were currentred. Nearly onHIV+ group an the non‐infeto be curreny), or to repo
Some Col
30%
%
+ HIV‐
30%
33
+ HIV‐
)
I A C E N T
tly working ene‐third (29%nd their peersected group (stly working, drt being retire
llege Colleg
21%
40%
38%
3%
1
E R O N H
ither full‐ or p%) reported bes, with 57% ofsee Figure 5).despite their ed (9% and 3
ge/Post‐Grad
36%
66%
50%
19 Septembe
I V & A G
part‐time, 13eing on disabf those living Older LGBT younger aver8%, respectiv
60%
57%
r 2011
I N G
% bility. with
rage vely).

AIDS Com
17 | P a g
There wereporting managed extra, andthe HIV+ gmoney (2
Figure 6: In
RELAT
Forty‐fouwith 2% rthat they long‐termwere no swho wereon averagmore hap
Not En
Just
Enou
M
mmunity Re
g e
re high levelsthat they didto get by on d 16% reportigroup compa2%) or were j
ncome Adequa
TIONSHIPS
r percent of oeporting thatwere not cur
m relationshipsignificant diffe not HIV‐infege as compareppy on averag
nough for Expe
t Manage to Ge
gh with Little E
Money No Prob
search Initia
s of income ind not have entheir incomeng that monered to their pjust managing
acy by HIV Sta
S, PARTN
older LGBT adt they were inrrently in a rep with most references in thected reporteed with HIV+ ge in their cur
0%
enses
et By
Extra
blem
ative of Amer
nadequacy in ough money . About one‐qey was not a ppeers, with ovg to get by (5
tus
ER STATU
dults reportedn an oppositelationship. Oveporting two hese relationsd that they hadults (14.3 yrrent relations
10% 2
12%
10%
9%
HIV+
rica (ACRIA)
A C R
the current sto cover expquarter (23%problem. Incover 80% repo59%) (see Figu
US & LIVI
d that they we‐relationshipver their lifetor three suchship variablesad been in thyears and 8.9ship (5.9 and
0% 30%
20%
22%
+ HIV‐
)
I A C E N T
sample of oldenses, and 46) said they haome inadequrting either thure 6).
NG ARRA
ere currently. However, thtimes, 79% sah relationships based on HIheir current re9 years, respe5.4, respecti
% 40%
39%
30%
1
E R O N H
er LGBT adult6% indicatingad enough moacy was signihat they did n
ANGEMEN
y in a same‐sehe majority (5aid that they hps (see Figure V status, oldeelationships sectively), and vely on a sca
50%
%
19 Septembe
I V & A G
ts, with 15% that they jusoney with a lificantly worsnot have eno
TS
ex relationship55%) indicatehad been in a7). While theer LGBT adultsignificantly loreported beile of 1 to 7).
60%
59%
r 2011
I N G
st ittle se in ugh
p, ed a ere ts onger ng
AIDS Com
18 | P a g
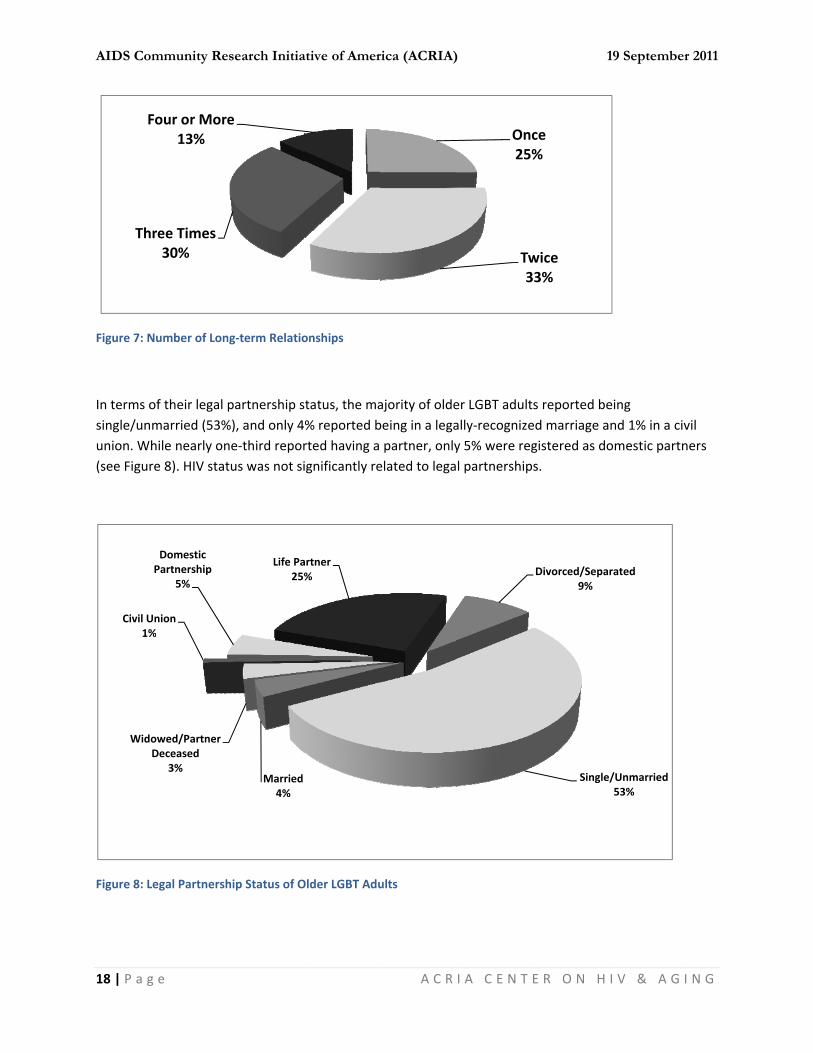
Figure 7: N
In terms osingle/ununion. Wh(see Figur
Figure 8: L
Th
F
Wido
Civil U1%
mmunity Re
g e
Number of Lon
of their legal pmarried (53%hile nearly onre 8). HIV stat
egal Partnersh
ree Times30%
Four or More13%
owed/Partner Deceased
3%
Union%
Domestic Partnership
5%
search Initia
ng‐term Relatio
partnership s%), and only 4ne‐third reportus was not si
hip Status of O
e
Married4%
Life Pa25%
ative of Amer
onships
status, the ma% reported brted having a ignificantly re
Older LGBT Adu
artner%
rica (ACRIA)
A C R
ajority of oldebeing in a legapartner, only
elated to lega
ults
)
I A C E N T
er LGBT adultally‐recognizey 5% were regl partnership
Onc25%
Tw3
1
E R O N H
s reported beed marriage agistered as dos.
ce%
wice33%
Single
Divorced/Sepa9%
19 Septembe
I V & A G
eing nd 1% in a civomestic partn
e/Unmarried53%
rated
r 2011
I N G
vil ners
AIDS Com
19 | P a g
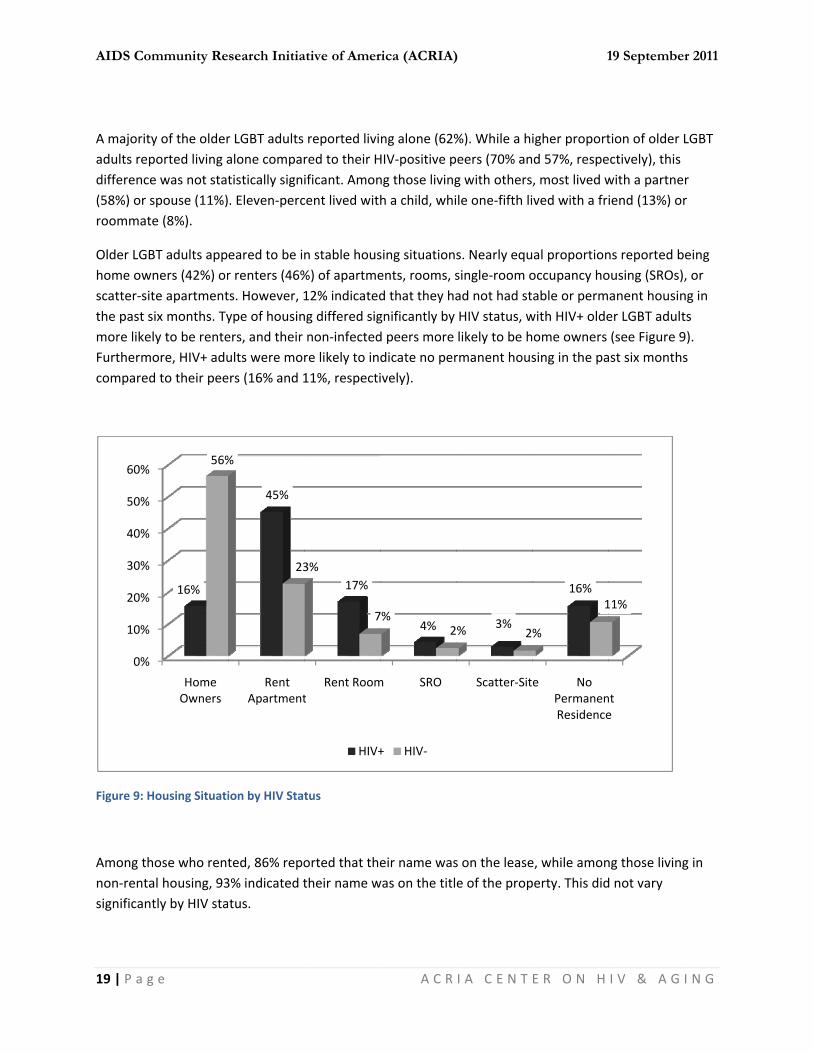
A majorityadults repdifference(58%) or sroommat
Older LGBhome owscatter‐sitthe past smore likeFurthermcompared
Figure 9: H
Among thnon‐rentasignificant
0%
10%
20%
30%
40%
50%
60%
mmunity Re
g e
y of the olderported living ae was not statspouse (11%)e (8%).
BT adults appners (42%) orte apartmentsix months. Tyly to be renteore, HIV+ adud to their pee
Housing Situati
hose who rental housing, 93tly by HIV sta
Home Owners
16%
56%
search Initia
r LGBT adults alone compartistically signi. Eleven‐perc
eared to be ir renters (46%ts. However, 1ype of housiners, and their ults were morers (16% and 1
ion by HIV Stat
ted, 86% repo3% indicated ttus.
Rent Apartment
45%
%
23
ative of Amer
reported livired to their Hificant. Amoncent lived with
n stable hous%) of apartme12% indicatedng differed signon‐infectedre likely to in11%, respecti
tus
orted that thetheir name w
tRent Room
17%3%
7
HIV+
rica (ACRIA)
A C R
ng alone (62%HIV‐positive png those livingh a child, whi
sing situationents, rooms, sd that they hagnificantly by d peers more dicate no perively).
eir name waswas on the titl
m SRO
4%7%
2
+ HIV‐
)
I A C E N T
%). While a hieers (70% ang with othersle one‐fifth li
s. Nearly equsingle‐room oad not had stHIV status, wlikely to be hrmanent hous
s on the leasee of the prop
Scatter‐Sit
3%% 2
1
E R O N H
igher proportd 57%, respe, most lived wved with a fr
al proportionoccupancy hoable or permwith HIV+ oldeome owners sing in the pa
e, while amonperty. This did
e No PermanenResidence
16%
%
1
19 Septembe
I V & A G
tion of older Lectively), this with a partneiend (13%) or
ns reported bousing (SROs),anent housiner LGBT adult(see Figure 9
ast six months
ng those livingd not vary
nt e
11%
r 2011
I N G
LGBT
r r
eing , or ng in ts 9). s
g in

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
20 | P a g e A C R I A C E N T E R O N H I V & A G I N G
RELIGIOUS AFFILIATION, PARTICIPATION & SUPPORT
With regard to religious affiliation, the largest proportion (43%) of older LGBT respondents reported being Christian (23% Protestant and 19% Catholic). Other religious denominations were mentioned much less frequently; Jewish (8%), Buddhist (2%), and Muslim (1%). Eighteen percent indicated that their religious affiliation was “other” (e.g., New Age, agnostic). However, nearly one‐quarter reported no religious affiliation (24%) and 3% indicated being atheist. There were no significant differences in religious affiliation by HIV status.
When asked if having an LGBT identity had negatively affected participation with their religious congregations, most (77%) felt that it had not been a factor. Among those who were HIV‐positive, two‐thirds reported that living with HIV had not affected their participation, while 19% reported they were more involved with their congregations following diagnosis. However, 15% indicated they participate less often than they did before they were diagnosed.
Nearly two‐in‐five older LGBT adults (38%) said that they had turned to their religious congregations for support, and this did not differ significantly by HIV status. The types of support received from congregations varied, but the most frequently reported was spiritual and emotional support, as well as opportunities for socialization. Others reported receiving assistance through counseling, or receiving transportation help, financial assistance or nutritional support. Many noted how their congregations were “gay‐friendly” and welcoming places to go. Those not receiving support were often reluctant to disclose their LGBT identities to the congregations, and/or felt that such information would not be well‐received by the congregation due to homophobia and the anti‐gay stance of their religion.
HEALTH STATUS & MEDICAL TREATMENT
When asked to rate their physical health, a majority of older LGBT adults indicated that their health was good (48%) or excellent (28%). However, 21% reported that their health was only fair, and 3% said they were in poor health. While not statistically significant, older LGBT adults with HIV were less likely to rate their health as excellent compared to their peers (19% and 32%, respectively) and more likely to rate their health as being good (57% and 43%, respectively).
Participants were asked if they had experienced any of 26 health problems in the previous year. On average, 2.6 health conditions were reported. Older LGBT adults with HIV reported significantly more health problems on average (3.1, SD = 2.5) as compared to their non‐infected peers (2.4, SD = 2.0).
As shown in Table One below, older HIV+ LGBT adults were significantly more likely to report a number of health conditions as compared with their peers, including all types of hepatitis, sexually transmitted diseases (i.e., herpes, syphilis), neuropathy, and vision loss. Older LGBT adults who were not living with HIV were significantly more likely to report arthritis and hypertension compared to those who were HIV+, not surprising given the greater average age in the former group, and were also more likely to report “other” health problems as well (e.g., allergies, incontinence, back problems).

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
21 | P a g e A C R I A C E N T E R O N H I V & A G I N G
Table One:Proportion of Older LGBT Adults with Health Conditions by HIV Status
Health Condition Total HIV+ HIV‐ Arthritis*** 35.9 21.1 43.7 Broken Bones 4.9 4.2 5.2 Cancer 7.3 5.6 8.1 Depression 46.1 52.1 43.0 Dermatological 15.5 15.5 15.6 Diabetes 15.5 12.7 17.0 Hearing Loss 11.2 8.5 12.6 Heart Condition 13.2 12.7 13.4 Hepatitis A** 2.9 7.0 0.7 Hepatitis B*** 6.3 18.3 0.0 Hepatitis C*** 7.8 16.9 3.0 Herpes*** 7.8 18.3 2.2 Hypertension** 19.4 8.5 25.2 Impotence (males only) 13.1 14.9 11.5 Menstrual Difficulties (females only) 6.0 0.0 6.1 Migraines 4.4 5.6 3.7 Nervous System Disorder 4.4 7.0 3.0 Neuropathy*** 14.1 25.4 8.1 Pneumonia 2.4 2.0 2.2 Respiratory Condition 2.4 1.4 3.0 Sexually Transmitted Disease (other)*** 4.4 12.7 0.0 Shingles 1.9 2.8 1.5 Staph Infection 1.9 0.0 3.0 Stroke 2.4 2.8 2.3 Syphilis*** 3.4 9.9 0.0 Vision Loss*** 6.8 15.5 2.2 Other Health Problem* 12.1 5.6 15.6
* p < .05, ** p < .01, *** p < .001, Chi‐square tests of significance
When asked where they go for medical treatment, older LGBT adults were most likely to report a private doctor/clinic (57%), followed by a public clinic or hospital (29.9%). Given that few had served in the armed forces, it was not surprising that only 5% received medical treatment at a Veteran’s Administration (VA) hospital. Older LGBT adults with HIV were significantly more likely than their non‐infected peers to receive medical treatment at a public clinic/hospital (40% and 25%, respectively), and significantly less likely to use a private doctor/clinic (31% and 70%, respectively).
In terms of HIV‐related medical providers, only 3% of older LGBT HIV+ adults reported using day programs at AIDS service organizations (ASOs), but 24% had used services at a Ryan White funded clinic.
When asked about using complementary and alternative (CAM) treatments for medical issues, the most frequently reported was taking vitamins (20%), and 10% reported using either nutritional supplements,
AIDS Com
22 | P a g
herbal supservices oreported tstatus.
HIV/AI
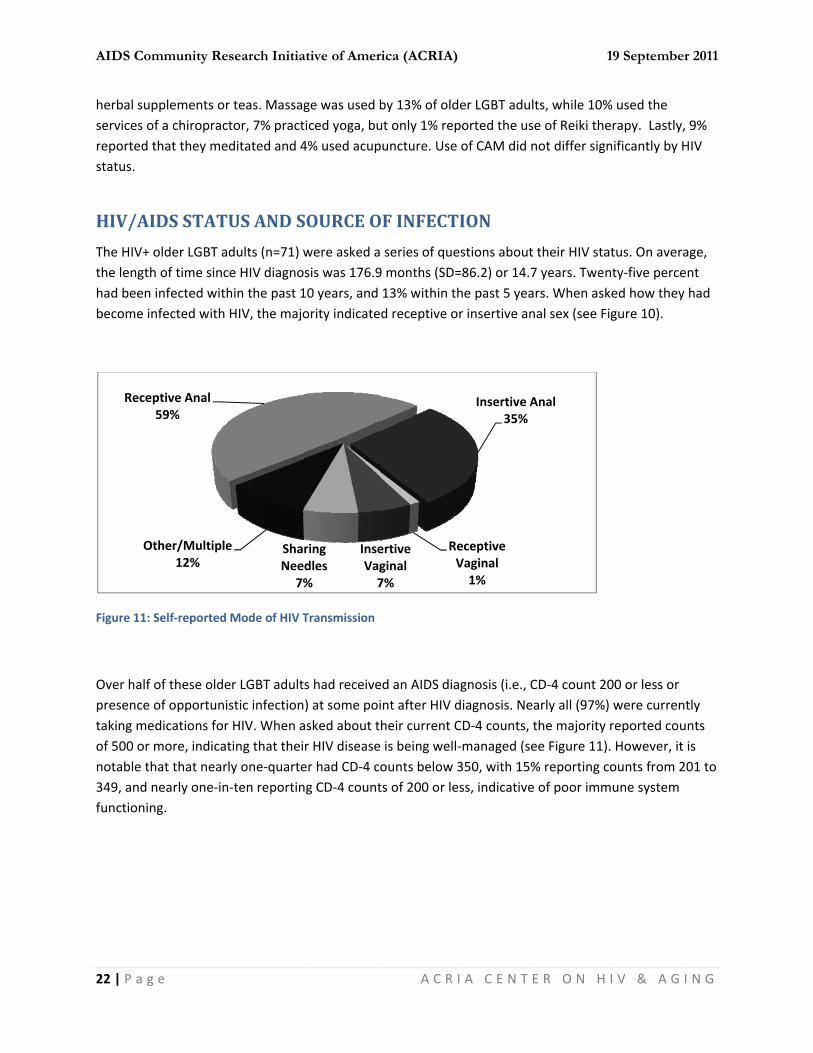
The HIV+ the lengthhad been become in
Figure 11:
Over half presence taking meof 500 or notable th349, and nfunctionin
Rece
O
mmunity Re
g e
pplements orof a chiropracthat they me
IDS STAT
older LGBT ah of time sincinfected withnfected with
Self‐reported
of these oldeof opportuniedications formore, indicathat that nearnearly one‐inng.
ptive Anal 59%
ther/Multiple12%
search Initia
r teas. Massagtor, 7% practditated and 4
US AND S
dults (n=71) wce HIV diagnohin the past 1HIV, the majo
Mode of HIV T
er LGBT adultstic infectionr HIV. When ating that theily one‐quarte‐ten reportin
ShaNee
7%
e
ative of Amer
ge was used bticed yoga, bu4% used acup
SOURCE O
were asked asis was 176.910 years, and ority indicate
Transmission
s had receive) at some poiasked about tr HIV diseaseer had CD‐4 cng CD‐4 count
InseVag7
ring dles%
rica (ACRIA)
A C R
by 13% of oldut only 1% reppuncture. Use
OF INFECT
series of que9 months (SD=13% within td receptive o
ed an AIDS diaint after HIV dheir current C is being wellounts below ts of 200 or le
RV
ertive ginal7%
)
I A C E N T
der LGBT adulported the use of CAM did n
TION
estions about=86.2) or 14.7he past 5 yeaor insertive an
agnosis (i.e., Cdiagnosis. NeCD‐4 counts, ‐managed (se350, with 15%ess, indicative
Insertive A35%
eceptive Vaginal1%
1
E R O N H
lts, while 10%se of Reiki thenot differ sign
t their HIV sta7 years. Twenars. When asknal sex (see Fi
CD‐4 count 20early all (97%)the majority ee Figure 11)% reporting ce of poor imm
Anal
19 Septembe
I V & A G
% used the erapy. Lastly,nificantly by H
atus. On averanty‐five perceked how theyigure 10).
00 or less or ) were currenreported cou. However, it counts from 2mune system
r 2011
I N G
, 9% HIV
age, ent had
tly unts is
201 to

AIDS Com
23 | P a g
Figure 11:
VISION
Participantrouble”, hearing aiwhile 60%vision. Pro62% indictrouble wwas not shearing as
Figure 12:
350 2
0%
10%
20%
30%
40%
50%
60%
70%
80%
mmunity Re
g e
Most Recent C
N & HEARI
nts were aske“a little troubids, respectiv% indicated haoblems with vcated no troubwith hearing. Gurprising thats compared w
Self‐reported
to 49925%
%
%
%
%
%
%
%
%
%
No
search Initia
CD‐4 t‐cell Cou
ING FUNC
ed to self‐repoble”, or “a lotvely). With regaving a little tvision functioble, 37% repoGiven the welt older LGBT awith the HIV+
Hearing Troub
Trouble
77%
54%
ative of Amer
unts of HIV+ LG
CTION
ort on their vt of trouble” (gard to visiontrouble with von did not difforted having all‐documenteadults who w+ group, given
ble by HIV Stat
A Little
24%
HIV+
rica (ACRIA)
A C R
GBT Older Adu
ision and heaincluding whn, 38% indicatvision, and 2%fer significanta little troubled associationwere not HIV‐in the former g
tus
201 to 315%
e Trouble
%
44%
+ HIV‐
)
I A C E N T
ults
aring and indien wearing gted they did n% indicated htly by HIV state, and 2% indns between hinfected repogroup’s great
200 o9
349
500 or Ab51%
A Lot of T
0%
1
E R O N H
cate if they elasses/contacnot have trouaving a lot oftus. With regdicated they hearing impairorted greater er average ag
or Below9%
bove%
Trouble
%2%
19 Septembe
I V & A G
experienced “ct lenses, or ble with visiof trouble withard to hearinhad a lot of rment and agproblems witge (see Figure
r 2011
I N G
“no
on, h ng,
ge, it th e 12).

AIDS Com
24 | P a g
MENTA
In additio
10‐item C
higher scosignificant(SD=5.9). non‐infecor higher,symptomdepressiv
Figure 13:
In additioPositive aaffect (e.gindicating5 to 25. Tdepressivcompared
8 Radloff, L.
Measur9 Andersen,
short fo77-84.
10 Swenson, patient
11 Watson, DPANAS
M
Not D
mmunity Re
g e
AL HEALT
n to the ques
Center for Epi
ores indicatint. The averagOlder adults ted peers (9.8, and nearly os. 10 Significane symptoms
Depression Sy
n to depressind Negative Ag., excited) rag greater posihe average sce symptoms,d with the HIV
.S. (1977). The rement, 1, 385-40E.M., Malmgrenorm of the CES-D S.L., Rose, M., Vcommunication a
D., Clark, L.A., &S scales. Journal
0%
Severe
Moderate
epressed
search Initia
TH
stion about ex
demiological
g more deprege score on thwith HIV had8 and 7.5, resone‐in‐five hantly, older LGas compared
ymptom Sever
ve symptomsAffect Schedunked on a fivtive affect (thcore in the cu non‐HIV infeV+ group (12.
CES-D Scale: A
01. n, J.A., Carter, WD (Center for Ep
Vittinghoff, E., Samong patients w
& Tellegen, A. (1l of Personality a
10%
1
ative of Amer
xperiencing d
Studies Depr
essive symptohe CES‐D in amd significantly spectively). Thd scores of 1BT HIV+ adul with their pe
rity by HIV Stat
s, older LGBT ule (PANAS). 1
ve‐point scalehe 5 negativeurrent sampleected older LG2 and 11.6, r
self-report depre
.B., & Patrick, Dpidemiologic Stud
Stewart, A., & Scwith type 2 diabete
988). Developmand Social Psycho
20% 30%
14%
17%13%
HIV+
rica (ACRIA)
A C R
depression in
ression Scale
oms. Scores omong the curhigher averahirty‐five per4 or above ints were twiceeers as seen i
tus
participants 11 The PANASe ranging from affect items e was 12.0 (SDGBT adults haespectively).
ession scale for r
D.L. (1994). Scredies Depression
chillinger, D.(200es. Medical Care
ment and validatioology, 54(6), 1063
40%
29%
HIV‐
)
I A C E N T
the past year
(CES‐D).8,9 Sc
of 10 or higherent sample oge CES‐D scocent of olderndicating a seve as likely to rn Figure 13.
were assesseS contains fivem Not at all towere not useD=4.3). Reflecad significantl
research in the ge
eening for depresScale). America
08). The influene, 46(3), 257-65. on of brief measu3-1070.
50% 60%
5
1
E R O N H
r, participants
cores range fr
er are consideof older LGBTres as compa LGBT adults vere level of dreport severe
ed for positivee items referro Extremely, wed). Possible scting differeny higher PAN
eneral population
sion in well oldean Journal of Pre
nce of depressive
ures of positive a
% 70%
69%
57%
19 Septembe
I V & A G
s completed t
rom 0 to 30 w
ered clinicallyT adults was 8ared with theihad scores ofdepressive e levels of
e affect usingring to positivwith higher scscores range ces in levels o
NAS scores as
n. Applied Psycho
er adults: evaluatieventative Medici
symptoms on cli
and negative affec
%
r 2011
I N G
the
with
y 8.3 ir f 10
g the ve cores from of
ological
ion of a ine, 10,
inician-
ct: The
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
25 | P a g e A C R I A C E N T E R O N H I V & A G I N G
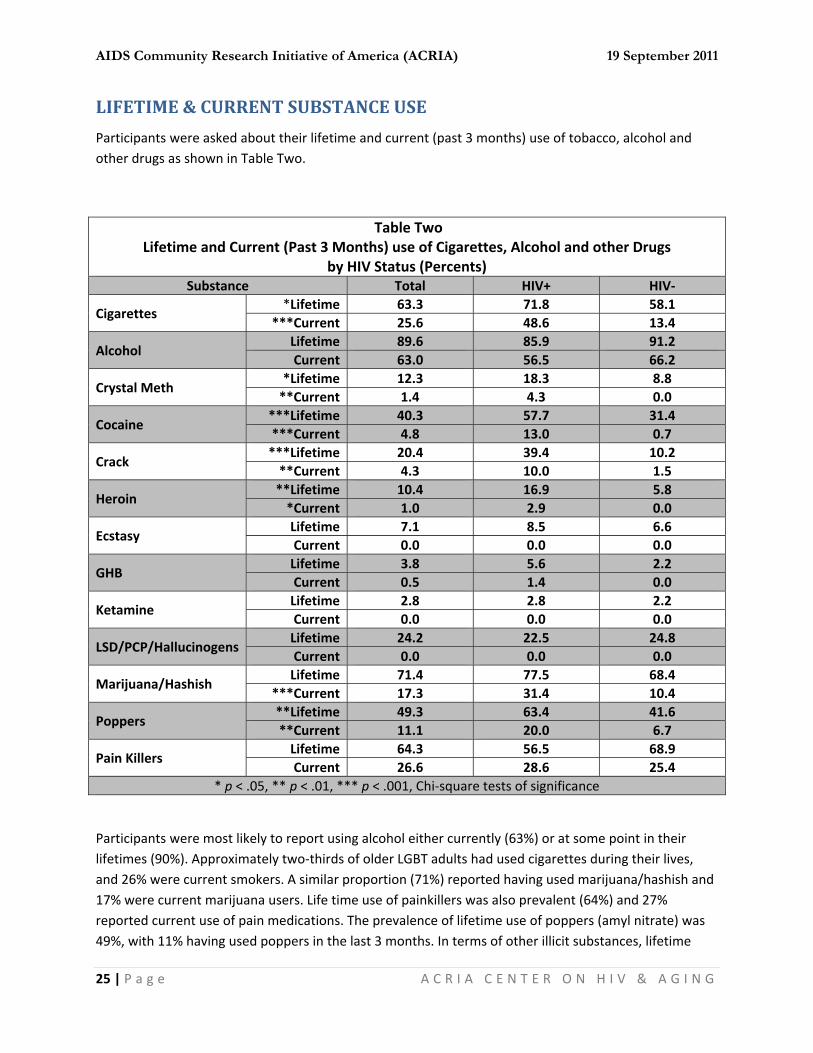
LIFETIME & CURRENT SUBSTANCE USE
Participants were asked about their lifetime and current (past 3 months) use of tobacco, alcohol and other drugs as shown in Table Two.
Table Two Lifetime and Current (Past 3 Months) use of Cigarettes, Alcohol and other Drugs
by HIV Status (Percents) Substance Total HIV+ HIV‐
Cigarettes *Lifetime 63.3 71.8 58.1
***Current 25.6 48.6 13.4
Alcohol Lifetime 89.6 85.9 91.2 Current 63.0 56.5 66.2
Crystal Meth *Lifetime 12.3 18.3 8.8 **Current 1.4 4.3 0.0
Cocaine ***Lifetime 40.3 57.7 31.4 ***Current 4.8 13.0 0.7
Crack ***Lifetime 20.4 39.4 10.2 **Current 4.3 10.0 1.5
Heroin **Lifetime 10.4 16.9 5.8 *Current 1.0 2.9 0.0
Ecstasy Lifetime 7.1 8.5 6.6 Current 0.0 0.0 0.0
GHB Lifetime 3.8 5.6 2.2 Current 0.5 1.4 0.0
Ketamine Lifetime 2.8 2.8 2.2 Current 0.0 0.0 0.0
LSD/PCP/Hallucinogens Lifetime 24.2 22.5 24.8 Current 0.0 0.0 0.0
Marijuana/Hashish Lifetime 71.4 77.5 68.4
***Current 17.3 31.4 10.4
Poppers **Lifetime 49.3 63.4 41.6 **Current 11.1 20.0 6.7
Pain Killers Lifetime 64.3 56.5 68.9 Current 26.6 28.6 25.4
* p < .05, ** p < .01, *** p < .001, Chi‐square tests of significance
Participants were most likely to report using alcohol either currently (63%) or at some point in their lifetimes (90%). Approximately two‐thirds of older LGBT adults had used cigarettes during their lives, and 26% were current smokers. A similar proportion (71%) reported having used marijuana/hashish and 17% were current marijuana users. Life time use of painkillers was also prevalent (64%) and 27% reported current use of pain medications. The prevalence of lifetime use of poppers (amyl nitrate) was 49%, with 11% having used poppers in the last 3 months. In terms of other illicit substances, lifetime
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
26 | P a g e A C R I A C E N T E R O N H I V & A G I N G
cocaine use was 40% (5% currently using), and crack‐cocaine lifetime use was 20% (4% currently using). Twelve‐percent had tried crystal meth, but only 1% reported currently using this substance. One‐in‐ten of had used heroin, but current use was low (1%). With regard to other substances, lifetime use of hallucinogens like LSD was reported by one‐quarter of older LGBT adults (24%), while lifetime use of club drugs (ecstasy, GHB, ketamine) was approximately 10% or less. No one reported the current use of hallucinogens, ecstasy or ketamine, and only one participant was currently using GHB.
Overall, older LGBT adults living with HIV were significantly more likely to report both the lifetime and current use of a number of substances, namely, cigarettes, crystal meth, cocaine, crack, heroin, and poppers. Notably, nearly half of those living with HIV were current smokers compared with only 13% of those who were not HIV‐infected. With regard to marijuana use, while lifetime prevalence did not differ based on HIV status, those who were HIV‐positive were significantly more likely to report current use than their peers (31% and 10%, respectively). However, use of alcohol and club drugs (ecstasy, GHB, and ketamine) did not differ significantly as a function of HIV status.
Twenty‐percent of the sample reported that they were currently in recovery for a drug or alcohol problem, and this did not differ significantly by HIV status.
FUNCTIONAL ABILITY
We asked respondents about any difficulty they encountered with 7 instrumental and 6 personal care activities of daily living (i.e., IADL and PADL, respectively) based on the OARS assessment.12 The task which the sample reported most frequent difficulty was found for the IADL task of housework (25%), such as sweeping or dusting, washing dishes or laundry. Difficulty getting to places out of walking distance (21%) and shopping (18%) were the next most problematic IADL tasks for the current sample of older LGBT adults, while 16% reported difficulty with meal preparation. Less than one‐in‐ten reported difficulty with using the telephone (5%), taking medications (5%) or handling money (8%). The average number of difficult IADL tasks was 1.3 (SD = 2.6), and this did not differ significantly by HIV status. Overall, 37% reported difficulty with at least one IADL task, and older LGBT adults with HIV were significantly more likely to report difficulty with at least one of these tasks as compared with their peers (47% and 31%, respectively). Figure 14 shows the proportion reporting difficulty with each IADL task by HIV status. The overall pattern was for greater proportions of those living with HIV to report difficulty with IADLs compared with their peers, however, only in the case of taking medications was this difference statistically significant.
12 Fillenbaum, G. G. (1988). Multidimensional functional assessment of older adults: The Duke Older Americans Resources and
Procedures. Hillsdale, NJ: Lawrence Erlbaum Assoc.

AIDS Com
27 | P a g
Figure 14:
Older LGBtasks withdressing/uacross a s
Figure 15:
Hand
**M
Meal P
Tran
Gettin
Wa
mmunity Re
g e
IADL Difficulty
BT adults werh the greatestundressing (9mall room (7
PADL Difficult
0%
ling Money
Medications
Housework
Preparation
Shopping
nsportation
Telephone
g In/Out of Be
lk Across Room
Feedin
Dressin
**Groomin
Bathin
search Initia
y by HIV Status
e less likely tot proportion i9%). Seven pe%), bathing (6
ty by HIV Statu
% 5%
2%
4%
0% 2
d
m
g
g
g
g
ative of Amer
s
o report difficindicating differcent or less 6%), groomin
us
10%
7%11
11
6%
HIV+
2% 4%
2%
2%
HIV+
rica (ACRIA)
A C R
culties with Pficulty was foreported diffng (5%), and f
15% 20
13%
17%
18
%
%
+ HIV‐
% 6%
4%
6%
6%
+ HIV‐
)
I A C E N T
PADL tasks as or getting in aficulty with thfeeding onese
0% 25%
21%
8%
20%
21%
8%
7%
8%
9
1
E R O N H
compared wnd out of bedhe remaining elf (3%).
30%
31%
27%
10%
10%
9%
19 Septembe
I V & A G
ith IADL tasksd (12%) and tasks; walkin
35%
%
12%
12%11%
11%
r 2011
I N G
s. The
ng
AIDS Com
28 | P a g
The averadiffer signreporting proportio15), only wHowever,all participwith more
SEXUA
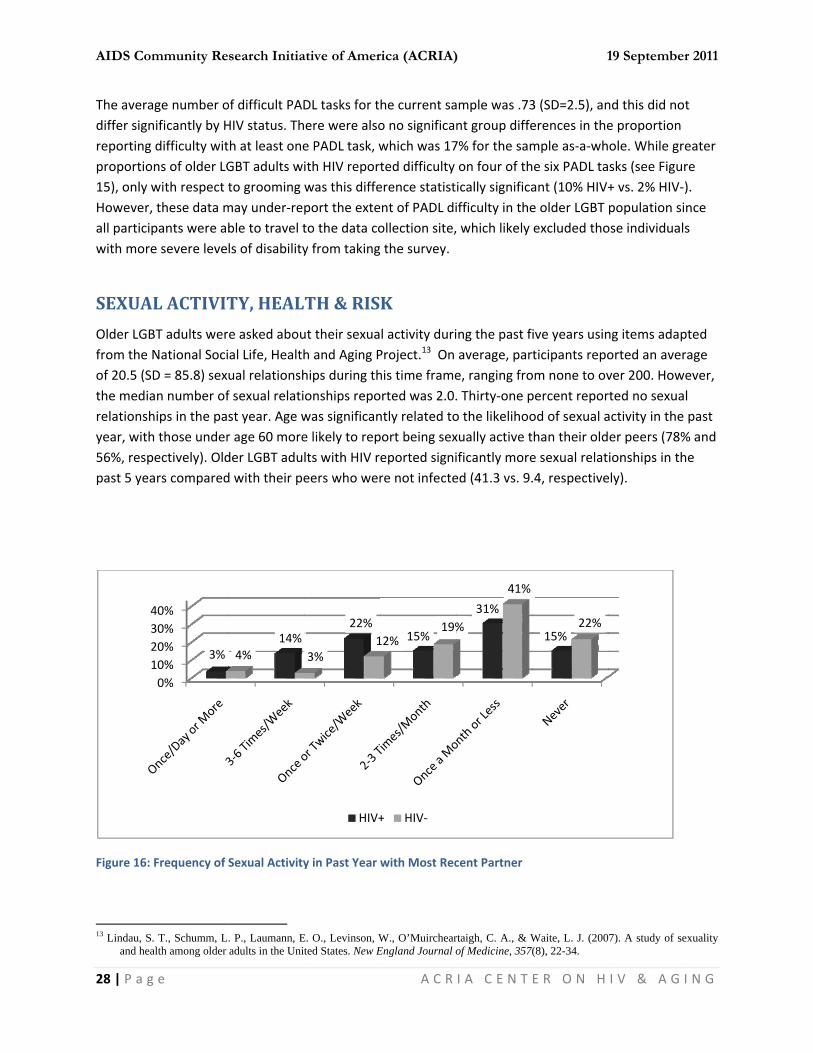
Older LGBfrom the of 20.5 (Sthe mediarelationshyear, with56%, resppast 5 yea
Figure 16:
13 Lindau, S
and hea
1234
mmunity Re
g e
age number onificantly by Hdifficulty wit
ons of older LGwith respect t these data mpants were ae severe leve
AL ACTIVIT
BT adults werNational SociD = 85.8) sexan number ofhips in the pah those underpectively). Oldars compared
Frequency of
. T., Schumm, Lalth among older
0%10%20%30%40%
3%
search Initia
of difficult PADHIV status. Thth at least oneGBT adults wito grooming may under‐reble to travel tls of disability
TY, HEAL
e asked aboual Life, Healthual relationshf sexual relatist year. Age wr age 60 moreder LGBT adud with their pe
Sexual Activity
. P., Laumann, Eadults in the Unit
14%4%
ative of Amer
DL tasks for tere were alsoe PADL task, with HIV reportwas this diffeport the exteto the data coy from taking
TH & RIS
ut their sexuah and Aging Phips during thonships repowas significane likely to replts with HIV reers who wer
y in Past Year w
E. O., Levinson, Wted States. New E
22%
3%1
HIV+
rica (ACRIA)
A C R
he current sao no significawhich was 17ted difficulty erence statistnt of PADL diollection site, the survey.
K
l activity duriProject.13 On his time frameorted was 2.0.ntly related toport being sexeported signire not infecte
with Most Rec
W., O’MuirchearEngland Journal o
15%12%19%
+ HIV‐
)
I A C E N T
ample was .73nt group diffe7% for the samon four of thically significaifficulty in the which likely
ing the past fiaverage, pare, ranging fro. Thirty‐one po the likelihooxually active tificantly moreed (41.3 vs. 9.
cent Partner
rtaigh, C. A., & Wof Medicine, 357(
31%%
41%
1
E R O N H
3 (SD=2.5), anerences in themple as‐a‐whe six PADL taant (10% HIV+e older LGBT excluded tho
ive years usinticipants repoom none to ovpercent reporod of sexual ahan their olde sexual relat.4, respective
Waite, L. J. (200(8), 22-34.
15%22%
19 Septembe
I V & A G
nd this did noe proportion ole. While grsks (see Figur+ vs. 2% HIV‐population siose individual
ng items adaported an averver 200. Howrted no sexuaactivity in the er peers (78%ionships in thely).
7). A study of se
r 2011
I N G
t
eater re ). nce s
pted rage ever, l past % and he
exuality
AIDS Com
29 | P a g
Participansignificantprepondein the HIVwhile 8% In the HIVreported (64%), 16same age recent pa
Older adupartner inSixty‐five this did no
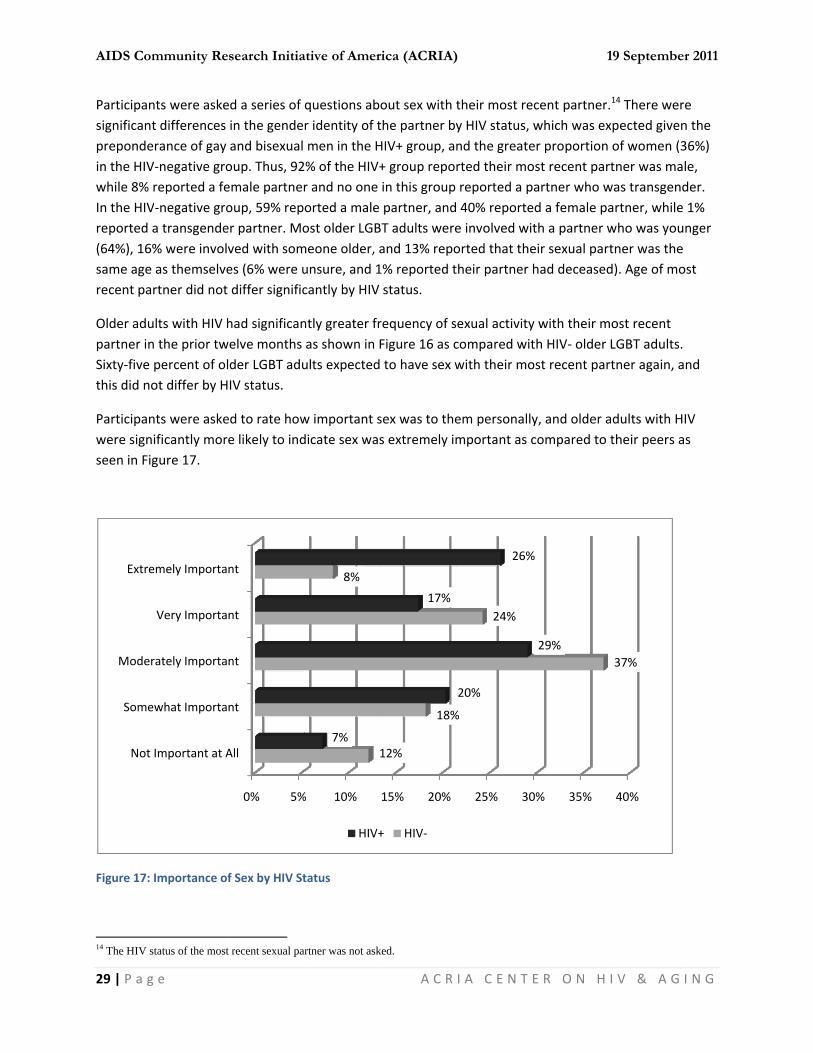
Participanwere signseen in Fig
Figure 17:
14 The HIV s
Not
Some
Moder
Extre
mmunity Re
g e
nts were asket differences erance of gay V‐negative groreported a feV‐negative groa transgende% were involvas themselvertner did not
ults with HIV hn the prior twpercent of olot differ by H
nts were askeificantly morgure 17.
Importance of
status of the most
Important at A
ewhat Importa
rately Importa
Very Importa
emely Importa
search Initia
ed a series of in the gendeand bisexual oup. Thus, 92emale partneroup, 59% reper partner. Moved with somes (6% were udiffer signific
had significanwelve months der LGBT aduIV status.
ed to rate howe likely to ind
f Sex by HIV St
t recent sexual pa
0% 5%
All
nt
nt
nt
nt
ative of Amer
questions abr identity of tmen in the H
2% of the HIV+r and no one orted a male ost older LGBmeone older, aunsure, and 1cantly by HIV
ntly greater fras shown in Fults expected
w important sdicate sex was
tatus
artner was not ask
% 10%
8%
7%
HIV+
rica (ACRIA)
A C R
out sex with tthe partner byHIV+ group, a+ group repoin this group partner, and
BT adults wereand 13% repo1% reported tstatus.
requency of sFigure 16 as c to have sex w
sex was to thes extremely im
ked.
15% 20%
12%
18%
17%
+ HIV‐
)
I A C E N T
their most rey HIV status, nd the greaterted their moreported a p 40% reportee involved wiorted that thetheir partner
exual activitycompared witwith their mo
em personallymportant as c
25% 30
%
24%
20%
26%
1
E R O N H
ecent partnerwhich was exer proportionost recent parpartner who wed a female path a partner weir sexual parhad deceased
y with their mth HIV‐ older ost recent par
y, and older acompared to
0% 35%
29%
%
19 Septembe
I V & A G
.14 There werxpected given of women (3rtner was mawas transgendartner, while who was yourtner was the d). Age of mo
most recent LGBT adults. rtner again, a
adults with Htheir peers a
40%
37%
r 2011
I N G
e n the 36%) le, der. 1% nger
ost
nd
IV s
AIDS Com
30 | P a g
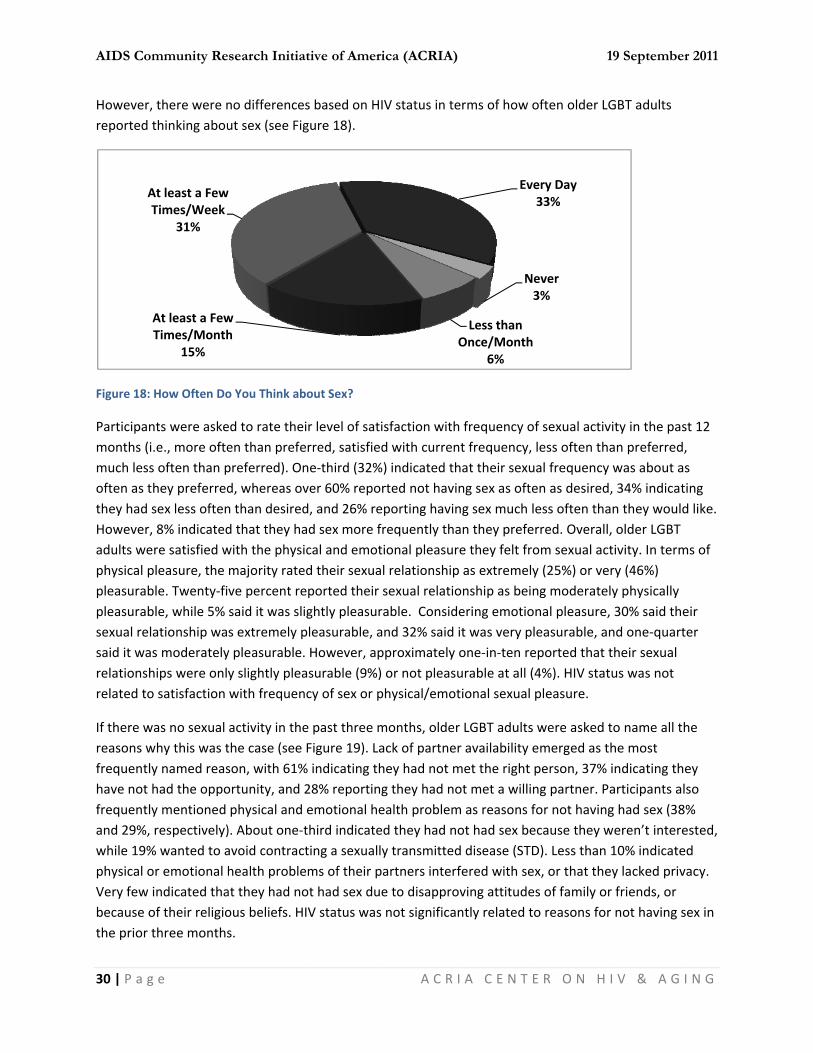
However,reported t
Figure 18:
Participanmonths (imuch lessoften as tthey had sHowever,adults wephysical ppleasurabpleasurabsexual relsaid it warelationshrelated to
If there wreasons wfrequentlyhave not frequentlyand 29%, while 19%physical oVery few because othe prior t
AT
mmunity Re
g e
there were nthinking abou
How Often Do
nts were aske.e., more oftes often than phey preferredsex less often 8% indicatedere satisfied wpleasure, the ble. Twenty‐fible, while 5% ationship was moderatelyhips were onlyo satisfaction
was no sexual why this was ty named reashad the oppoy mentioned respectively)
% wanted to aor emotional hindicated thaof their religiothree months
At least a FewTimes/Month
15%
At least a FewTimes/Week
31%
search Initia
no differenceut sex (see Fig
o You Think ab
ed to rate theen than prefepreferred). Ond, whereas ovn than desiredd that they hawith the physimajority rateve percent resaid it was slis extremely py pleasurable.y slightly pleawith frequen
activity in thethe case (see son, with 61%ortunity, and physical and ). About one‐tavoid contrachealth probleat they had noous beliefs. Hs.
w h
w
ative of Amer
s based on Hgure 18).
bout Sex?
ir level of saterred, satisfiene‐third (32%ver 60% repod, and 26% read sex more fical and emoted their sexuaeported their ightly pleasurpleasurable, a. However, apasurable (9%)ncy of sex or p
e past three mFigure 19). La
% indicating th28% reportinemotional hethird indicateting a sexuallems of their pot had sex duIV status was
rica (ACRIA)
A C R
IV status in te
isfaction withd with curren
%) indicated thorted not havieporting havinfrequently thational pleasural relationshipsexual relatiorable. Considand 32% said pproximately ) or not pleasphysical/emo
months, olderack of partnehey had not mg they had noealth problemed they had nly transmittedpartners intere to disappros not significa
)
I A C E N T
erms of how
h frequency ont frequency, hat their sexuing sex as ofteng sex much an they prefere they felt frp as extremelonship as beidering emotioit was very pone‐in‐ten reurable at all (tional sexual
r LGBT adultsr availability met the right ot met a willim as reasons fot had sex bed disease (STDrfered with seoving attitudently related t
N
Less than Once/Month
6%
Ev
1
E R O N H
often older LG
of sexual activless often th
ual frequencyen as desiredless often thaerred. Overallom sexual acy (25%) or veng moderateonal pleasure,leasurable, aeported that (4%). HIV statpleasure.
s were asked temerged as tperson, 37% ng partner. Pfor not havingecause they wD). Less than ex, or that thees of family orto reasons for
Never3%
h
very Day33%
19 Septembe
I V & A G
GBT adults
vity in the pasan preferred,y was about ad, 34% indicatan they would, older LGBT tivity. In termery (46%) ly physically , 30% said thend one‐quarttheir sexual tus was not
to name all ththe most indicating tharticipants alg had sex (38weren’t intere10% indicateey lacked privr friends, or r not having s
r 2011
I N G
st 12 , s ting d like.
ms of
eir ter
he
ey lso 8% ested, ed vacy.
sex in

AIDS Com
31 | P a g
Figure 19:
Participangratificatiof interes(43%), anthey couldwhile oneinterestedintercoursdifferencewere HIV‐compared
Forty‐onemore of t
When askwould be saying the
B
Childre
E
mmunity Re
g e
Reasons for N
nts were askeon, during tht (50%). Probd about one‐d sexually pee‐quarter hadd in sex because as a reasone based on HI‐positive beind with their p
e percent of ohe issues det
ked if they wovery likely (3ey would be u
No
Not E
Did N
Believe No Sex
Friends Wou
en/Family Wou
Emotional Prob
Emotional
Physical H
Physic
Partner N
Haven't Met W
Haven't Met
N
search Initia
No Sexual Activ
ed why they me last 12 monblems with gein‐five mentiorform, and a issues with cuse they did nn for not beinIV status on lang more likelyeers (38% an
older LGBT adailed in Figur
ould go to a c3%) or somewunlikely or ve
o Opportunity
nough Privacy
Not Want STD
Grieving
Sex Painful
w/o Marriage
uldn't Approve
uldn't Approve
blems‐Partner
Problems‐Self
Health‐Partner
cal Health‐Self
Not Interested
Willing Partner
t Right Person
Not Interested
ative of Amer
vity in the Past
may not have nths (see Figuetting and maoned lubricatsimilar propocoming to climnot find it pleng interested ack of interesy to indicate cd 20%, respe
ults indicatede 20, and this
linic to have swhat likely (1ry unlikely to
0% 10%
8%
3%
1%
3%
1%
3%
3%
8%
9%
rica (ACRIA)
A C R
t Three Month
been interesure 20). The mintaining an etion issues. Oortion reportemax too quickeasurable, andin sexual actist/problems wcoming to climectively).
d that they has did not diffe
sexual matte17%) to do so, seek such he
20% 30%
19%
%
2
)
I A C E N T
hs
sted in sex, ormost frequenerection wereOver one‐thirded difficulty inkly. Approximd very few (6%ivity. There wwith sexual grmax/orgasm t
ad avoided seer significantl
rs addressed,, with approxelp. Willingne
% 40%
37%
29%
38%
28%
32%
1
E R O N H
r had difficultntly mentionee also mentiod were anxioun coming to cmately one‐in‐%) mentionedwas only one sratification, wtoo quickly as
exual activity y by HIV statu
, about half reximately one‐ess to seek he
50% 60%
6
19 Septembe
I V & A G
y with sexualed reason wasoned frequentus about howclimax/orgasm‐five were notd pain duringsignificant with those whs an issue as
due to one ous.
eported that quarter eachelp at a clinic t
70%
61%
r 2011
I N G
s lack tly w well m, t g
ho
r
they to

AIDS Com
32 | P a g
address seindicatingpercent owere eithnot signifi
Figure 20:
Participanvaginal, oindicated reported protection
Similar ratalways usindicated intercours
In terms oprecautioprecautiowere no sHIV status
Pai
Climax/
Unab
L
mmunity Re
g e
exual mattersg they were atof participantser very (47%)icantly relate
Reasons for La
nts were asker oral sexual that they alwrarely using an.
tes of protectsed, and 7% inthat condomse. Over one‐
of taking precns and 7% sans with sex tosignificant diffs.
Problems Lubr
Erectile Dysfu
Performance A
Sex Not Pleas
in During Inter
/Orgasm Too Q
ble to Climax/O
Lacked Interest
search Initia
s differed signt least likely ts reported tha) or somewhad to seeking
ack of Sexual I
ed about the uactivity and wways used cona condom dur
ted sex were ndicating thatms were used ‐third (35%) n
cautions with ying that theoys and 5% raferences in e
0%
ricating
unction
Anxiety
surable
rcourse
Quickly
Orgasm
t in Sex
ative of Amer
nificantly by Hto seek such hat they had aat satisfied (3medical help
nterest or Gra
use of condomwhen using sendoms, whilering vaginal in
observed fort they usuallysometimes, anever used co
sex toys, a siy usually tooarely did so, wngaging in sa
10%
6%
rica (ACRIA)
A C R
HIV status, whelp as compctually sough9%) with the or satisfactio
atification in th
ms and otherex toys. With 20% said thantercourse an
r anal intercoy used a condand 4% reporondoms durin
milar patternk precautionswhile 28% nevfer vaginal or
20%
21%
19%
)
I A C E N T
ith two‐thirdsared with 43%ht medical hehelp that the
on with such h
he Past 12 Mo
r sexual precaregard to vagat they usuallynd 28% said th
urse, with 42om during anrted rarely using anal interco
n emerged wis. Eight‐percever took precr anal sex, or
30%
%
26%
1
E R O N H
s of HIV+ olde% of HIV‐ adulp for sexual ey had receivhelp.
nths
autions they tginal intercouy used condohat they neve
2% saying thatnal intercoursing a condomourse.
th 51% alwayent sometimecautions withplay with sex
40%
43%
36%
35%
19 Septembe
I V & A G
er LGBT adultults. Eighteenissues, and med. HIV statu
took during aurse, 44% oms. Howeverer used
t condoms wese. Twelve‐pem during anal
ys taking es took sex toys. Thex toys, based o
50%
%
50%
r 2011
I N G
ts ‐
most s was
nal,
r, 8%
ere ercent
ere on

AIDS Com
33 | P a g
However,likely to u
Figure 21:
Older LGmight be tdifference
I Really WI Really NeWith VeryPartner SaThink RiskFeel DeprThink PartDrunk or With a YoWith an O
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
mmunity Re
g e
with regard use condoms o
Frequency of
BT adults whotempted to hes based on H
Reasons R
Want Sex eed Affectiony Sexy/Attractays Doesn’t Wk of STDs is Loressed** tner Doesn’t High on Drugounger PersonOlder Person
* p
Always
20%
search Initia
to precautionor dental dam
Using Condom
o were sexuahave unprotecHIV status.
for Wantingeason
n tive Person Want to Use Cow**
Want to Use gs*** n
p < .05, ** p <
Usua
10%3%
ative of Amer
ns during orams as compar
ms/Dental Dam
ally active wercted sex (see
Tag to Have Un
Condom
Condom***
< .01, *** p <
ally Som
%3%
HIV+
rica (ACRIA)
A C R
l sex, older LGred to the HIV
ms during Oral
re asked abouTable Three)
able Three nprotected
Tot21.12.12.8.618.6.15.111.7.13.0
.001, Chi‐squ
metimes
8%5%
+ HIV‐
)
I A C E N T
GBT adults wiV‐negative gro
Sex
ut a variety o, and there w
Sex by HIV Sal .2 .3 .6 6 .7 1 1 .6 1 0 uare tests of s
Rarely
3%6%
1
E R O N H
ith HIV were soup as shown
f situations inwere a numbe
Status (PercHIV+ 26.2 12.3 15.4 13.8 6.2 13.8 12.3 23.1 7.7 1.5
significance
Never
55%
88%
19 Septembe
I V & A G
significantly mn in Figure 21
n which they er of significan
ents) HIV‐18.512.310.86.224.62.31.56.26.23.8
%
r 2011
I N G
more .
nt
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
34 | P a g e A C R I A C E N T E R O N H I V & A G I N G
SOCIAL SUPPORTS FROM FAMILY, FRIENDS & NEIGHBORS
As they age, people rely increasingly upon their social networks for informal support and caregiving. But as people age, their social networks often decrease in size due to events such as relocation, illness and death.15 For older LGBT adults research suggests this trend of decreasing network size is exacerbated. Many older LGBT adults rely on friends for informal support. 16 Consequently, the social networks of many of these individuals may be inadequate to provide needed levels of support as this population ages. While these friends serve as a critical source of support, they may be less likely to provide supportive care as they will likely face the challenges of aging and may need support themselves.
The current study assessed the presence of potentially supportive people in these networks of older LGBT adults. We asked about the presence and number of support element, frequency of contact, feelings of closeness, and the types of support received from family and friends. These data also allowed us to determine if those network members were “functional.” A functional member of the social network is defined as having monthly face‐to‐face contact and/or talking on the phone at least weekly, and has been used in other large‐scale studies of older adults. Functional social network members are considered to be relatively available to provide assistance in times of need, and it is their presence in a social network that provides a good indicator of social support sufficiency.
Presence of Social Network Members and Functionality. On average, older LGBT adults reported 10.6 people in their social networks (SD=7.4). Those with HIV reported significantly smaller social networks on average as compared with their non‐infected peers (8.9 and 11.5 people, respectively).
As has been documented in previous research on older LGBT adults, there was limited presence of biological family social network elements in the current sample, which was further limited when considering the functionality of these network members (see Figure 22). While 42% of participants reported having a living parent, only 26% of these parents were functional social supports. Less than one‐third reported the presence of a child (either biological or adopted/foster), and less than one‐quarter had a functional child. A similar pattern emerged with regard to grandchildren (i.e., 21% report a grandchild, but only 10% a functional grandchild). And while nearly all older LGBT adults reported a living brother or sister (84%), only 38% reported having at least one functional sibling. Furthermore, half the sample did not report the presence of other, more distant relatives in their social networks. The reasons for the discrepancy between living social network members and functional elements are varied, but include geographic relocation to the Chicago area (likely for work opportunities and the presence of a large gay and lesbian community) and unfortunately, homophobia and estrangement from biological family because of sexual identity. To compensate for the lack of informal family supports, older LGBT participants appear to rely heavily on friends, or so‐called families‐of‐choice. Friends were the most prevalent social network element mentioned (86%), and most of these friends are functional (77%) and
15 Cantor, M. H., & Brennan, M. (2000). Social care of the elderly: The effects of ethnicity, class and culture. New York: Springer. 16 Cantor, M. H., Brennan, M., & Shippy, R. A. (2004). Caregiving among Older Lesbian, Gay, Bisexual and Transgender New Yorkers.
New York: The National Gay and Lesbian Task Force Policy Institute.
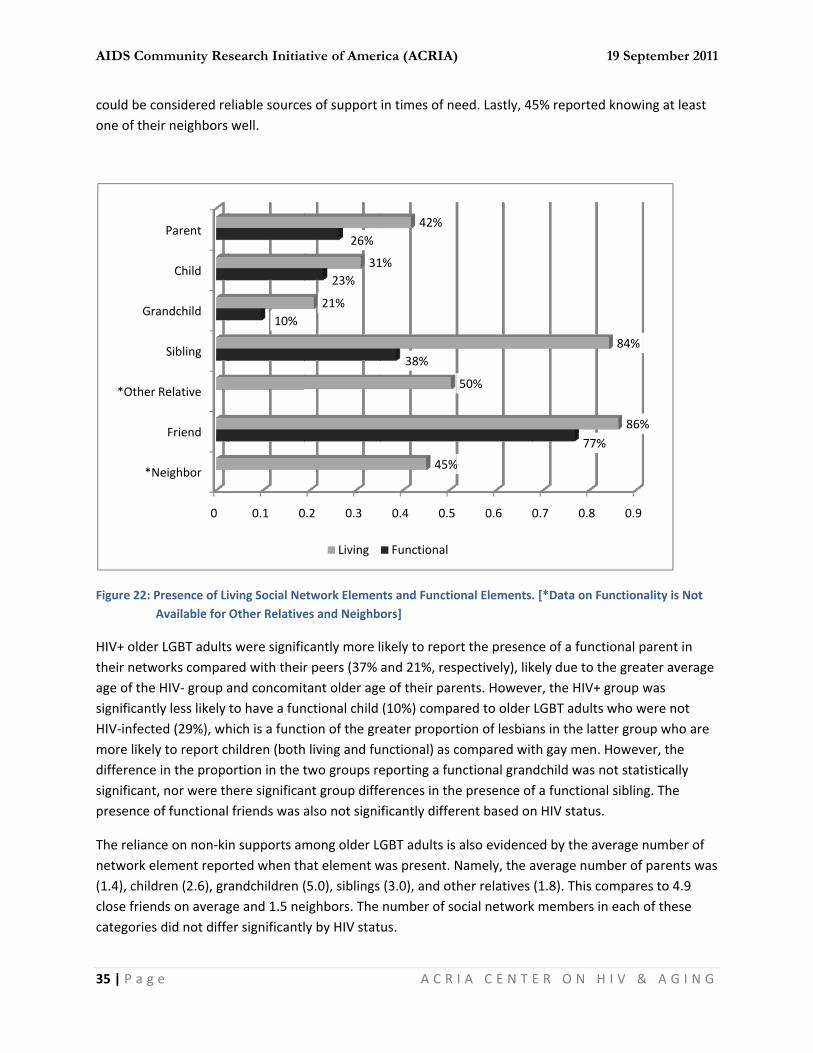
AIDS Com
35 | P a g
could be cone of the
Figure 22:
HIV+ oldetheir netwage of thesignificantHIV‐infectmore likedifferencesignificantpresence
The reliannetwork e(1.4), childclose friencategories
*
*Other
Gr
mmunity Re
g e
considered reeir neighbors
Presence of LiAvailable for
er LGBT adultsworks compare HIV‐ group atly less likely ted (29%), whly to report ce in the propot, nor were thof functional
nce on non‐kielement repodren (2.6), grnds on averags did not diffe
0
Neighbor
Friend
r Relative
Sibling
randchild
Child
Parent
search Initia
eliable sourcewell.
iving Social NeOther Relative
s were signifired with theirand concomitto have a funhich is a functhildren (bothortion in the there significa friends was a
n supports amorted when thandchildren (ge and 1.5 neer significantl
0.1 0
10%
ative of Amer
es of support
etwork Elemenes and Neighb
cantly more lr peers (37% tant older agenctional child tion of the greh living and futwo groups rent group diffealso not signi
mong older LGhat element w(5.0), siblings eighbors. The ly by HIV stat
0.2 0.3
23%
26%
21%
31
Living
rica (ACRIA)
A C R
in times of ne
nts and Functioors]
ikely to repoand 21%, rese of their par(10%) compaeater proportunctional) as ceporting a funerences in theficantly differ
GBT adults is was present. N(3.0), and otnumber of sous.
0.4 0.5
38%
45%
1%
42%
Functional
)
I A C E N T
eed. Lastly, 4
onal Elements
rt the presenpectively), likents. Howeveared to older tion of lesbiacompared witnctional grane presence ofrent based on
also evidencNamely, the aher relatives ocial network
0.6 0
%
50%
1
E R O N H
5% reported
. [*Data on Fu
ce of a functikely due to ther, the HIV+ gLGBT adults wns in the latteth gay men. Hdchild was nof a functionaln HIV status.
ed by the aveaverage numb(1.8). This cok members in
0.7 0.8
77%
19 Septembe
I V & A G
knowing at le
nctionality is N
ional parent ihe greater avegroup was who were noer group whoHowever, theot statistically sibling. The
erage numbeber of parentmpares to 4.9 each of thes
0.9
86%
84%
r 2011
I N G
east
Not
n erage
t o are y
r of ts was 9 e

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
36 | P a g e A C R I A C E N T E R O N H I V & A G I N G
Considering the importance of friends in the social networks of older LGBT adults, participants were asked how many of their friends were living with HIV, since this would likely impact the ability of this person to provide support given the greater likelihood for health comorbidities as they age. Overall, older LGBT adults reported having 1 friend on average living with HIV. Those living with HIV reported a greater number of friends living with HIV on average (1.6) as compared 0.4 among those who were not HIV‐infected. This finding suggests even greater fragility of the social networks of older LGBT HIV+ adults.
Feelings of Closeness to Social Network Members. When asked about how close they felt to various members of their social networks, older LGBT adults by and large reported having close relationships when these individuals were present. Fifty‐five percent reported feeling very close to parents (24% said they were somewhat close), while 61% indicated that they were very close to their children (29% somewhat close), and 47% reported being very close to grandchildren (33% somewhat close). With regard to siblings, however, feelings of closeness were mitigated with 36% saying they were very close and 33% indicating that they were somewhat close. But again, the importance of the family‐of‐choice for older LGBT adults was evidenced by 68% saying they were very close to their friends, and 30% reporting that they were somewhat close.
Geographic Location of Family and Friends. Suggesting that many of these older LGBT adults had migrated to Chicago from elsewhere, 65% reported that their parents lived outside of the Chicago metropolitan area, while 11% reported their parents lived in the Chicago suburbs. Nineteen‐percent reported a parent in Chicago, but out of walking distance, and only 5% had a parent living nearby (walking distance or same building). With regard to children, nearly two‐thirds lived in the Chicago metro area, but only 17% lived nearby. One‐third had children living elsewhere in Chicago and 9% had children in the Chicago suburbs. Geographic location of grandchildren and siblings was similar, with approximately 55% of participants reporting that these people lived outside of the Chicago metro area and 5% of less had these members of their networks within walking distance. As might be expected, the majority of older LGBT adults reported that their friends lived in the Chicago metro area (77%), with 22% living either in the same building or in walking distance, 39% in Chicago but not in walking distance, and 15% living in suburban areas. The geographic proximity of family and friends did not differ significantly by HIV status.
Receipt of Assistance from Family, Friends and Neighbors. Older LGBT adults were asked about help they received from family and friends, respectively. For both family and friends, participants indicated if they received help with instrumental tasks (i.e., shop/run errands, keep house/prepare meals, drive/escort to places, help with mail/correspondence, help manage money) as well as emotional support (i.e., advice on a big decision, need cheering up, talk about personal/private matters).

AIDS Com
37 | P a g
Figure 23:
As illustraless than exceptionadults repexample, errands, oadults repcompared
Older LGBwith instrcame fromstatus in texceptionmail/correparticipanfrom frien
Kee
mmunity Re
g e
Receipt of Ins
ated in Figure30% reportinn of keeping hported receivwhile nearly only 16% repoported that frd with 18% w
BT adults werumental taskm friends raththe likelihoodn. Older HIV+ espondence fnts reported rnds, and this d
Talk about
Ch
Mana
Mail/Corres
Dr
ep House/Prep
Shop/Ru
search Initia
trumental and
23, instrumeg this type ofhouse/preparing these typone‐quarter orted such heriends provideho reported f
e much moreks (range = 43her than famid of receiving LGBT adults wfrom family creceiving 1.9 did not differ
0%
t Problems
heering Up
Advice
age Money
spondence
rive/Escort
pare Meals
un Errands
ative of Amer
d Emotional Su
ental support f assistance frring meals andes of assistanof participantelp from famied them withfamily memb
e likely to rep3% to 56%), anily members. any of these were significaompared to ttypes of assisr significantly
% 10%
2%
6%
8%
7%
4%
10
Fa
rica (ACRIA)
A C R
upport from Fa
from either from either sod managing mnce from frients reported thly members. h a ride or escbers provided
ort receiving nd again, greThere were ntypes of suppantly more liktheir peers (9stance from fby HIV status
20%
23
18%
%
16%
mily Friend
)
I A C E N T
amily and Frien
family or frienource of suppmoney, greatends as opposehat friends he In a similar pcort to places such assistan
emotional suater proportino significantport from eitkely to receive9% and 2%, reamily membes. With regard
30% 40
28%
3%
ds
1
E R O N H
nds
nds tended toort. In additioer proportioned to family melped with shpattern, 28% they needednce.
upport compaons indicated differences bher family or e help with espectively). Oers and 2.2 tyd to neighbor
0% 50%
48%
48%
43%
19 Septembe
I V & A G
o be limited, won, with the ns of older LGmembers. Forhopping/runnof older LGBT to go, as
ared to assistd such supporbased on HIV friends with
On average, ypes of assistars, we asked a
60%
56%
54%
%
%
52%
r 2011
I N G
with
BT r ing T
ance rt
one
ance about

AIDS Com
38 | P a g
the level otheir neigemergenchelp to ea
Figure 24:
Nand somefamily andreport nereluctant There weeither fam
Sofriends, thdegree ofeach relatwas equathere wasrelationshconsistenonly statisillustrate social net
0%
5%
10%
15%
20%
25%
30%
35%
mmunity Re
g e
of mutual helghbors helpedcies. Howeverach other. The
Negative Supp
Negative Sociae may be negad friend in thegative suppoto talk (24% vre no significamily or friends
ocial Supporthey may also f reciprocity intionship type l, or if they res a trend for ohips, than to pt with a greatstically signifia pattern of iworks.
%
%
%
%
%
%
%
%
ReluctaNeed
search Initia
lp provided. Od each other ar, about one‐ese helping re
port Received
al Support. Native in natureir social netwrt from familyvs. 17%) and ant differences.
t Reciprocity.be sources on their suppowhether theeceived moreolder LGBT adprovide moreter level of necant with regnter‐depende
nt when You ded to Talk
24%
17%
ative of Amer
Over one‐quaa lot, while 37third (36%) inelationships w
from Family a
ot all interactre. Therefore,works as showy as compareupsetting thees by HIV stat
While olderf assistance tort exchangesy provided me support thandults who wee help than theed among Hgard to parenence betwee
Upset YouFee
3
Family
rica (ACRIA)
A C R
arter (27%) of7% said that sndicated thatwith neighbo
and Friends
tions with me, we asked pawn in Figure 2ed to friends, e participant tus in the like
LGBT adults to members o with the me
more support tn they providre HIV+ to rechey received aIV+ older LGBts and siblingn older LGBT
u/Hurt Your elings
35%
22%
y Friends
)
I A C E N T
f older LGBT asuch assistanct they and thers did not diff
embers of thearticipants ab24. Older LGBparticularly wor hurting theelihood of rep
may receive of their social mbers of thethan they reced in return. ceive more has compared BT adults. Howgs. But regardadults and m
Refused t
11
1
E R O N H
adults indicatce was provideir neighbors fer significant
e social netwoout negative BT adults werwith regard toeir feelings (3porting negat
support fromnetworks. Wir social netwceived, if the As illustratedelp, or be in rwith their pewever, these dless of HIV stmembers of th
to Help
1%9%
19 Septembe
I V & A G
ed that they ded only in did not provitly by HIV sta
ork are positiexperiences re more likelyo them being 35% vs. 22%).ive support fr
m family and We assessed thworks by askinsupport exchd in Figure 25reciprocal eers. This woudifferences wtatus, these dheir informal
r 2011
I N G
and
ide tus.
ive, with y to
. rom
he ng for hange ,
uld be were data
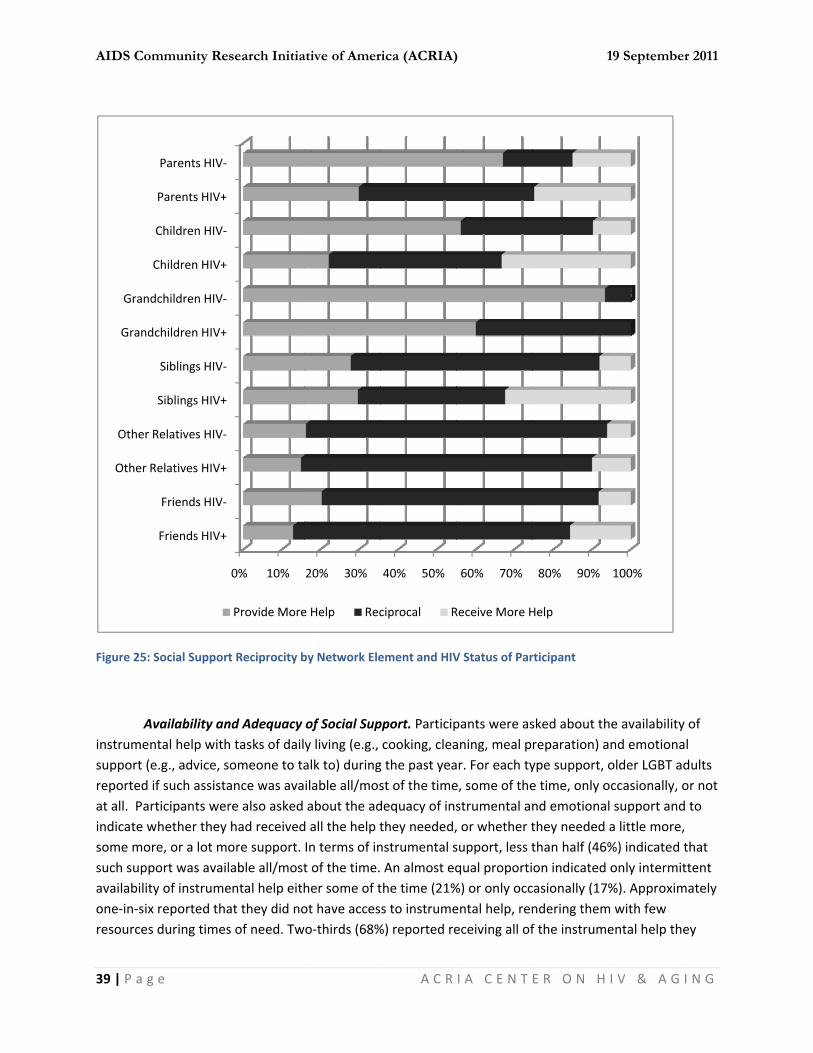
AIDS Com
39 | P a g
Figure 25:
Ainstrumensupport (ereported at all. Parindicate wsome morsuch suppavailabilitone‐in‐sixresources
Other R
Other
Grand
Grand
mmunity Re
g e
Social Support
vailability anntal help withe.g., advice, sif such assistarticipants werwhether they re, or a lot mport was availty of instrumex reported thas during times
Friends HIV+
Friends HIV‐
Relatives HIV+
Relatives HIV‐
Siblings HIV+
Siblings HIV‐
dchildren HIV+
dchildren HIV‐
Children HIV+
Children HIV‐
Parents HIV+
Parents HIV‐
search Initia
t Reciprocity b
nd Adequacy h tasks of dailsomeone to taance was avare also asked had receivedore support. lable all/mostental help eithat they did nos of need. Tw
0% 10%
Provide More
ative of Amer
by Network Ele
of Social Supy living (e.g., alk to) duringilable all/mosabout the ad
d all the help tIn terms of int of the time.her some of tot have acceswo‐thirds (68%
20% 30%
e Help Rec
rica (ACRIA)
A C R
ement and HIV
pport. Participcooking, cleag the past yeast of the timedequacy of insthey needed,nstrumental s An almost eqthe time (21%s to instrume%) reported re
40% 50%
ciprocal R
)
I A C E N T
V Status of Par
pants were asaning, meal par. For each tye, some of thestrumental an, or whether tsupport, less tqual proporti%) or only occental help, reneceiving all of
60% 70%
Receive More H
1
E R O N H
rticipant
sked about threparation) aype support, oe time, only ond emotionalthey needed than half (46%on indicated casionally (17%ndering themf the instrume
80% 90%
Help
19 Septembe
I V & A G
he availabilityand emotionaolder LGBT adoccasionally, ol support anda little more,%) indicated tonly intermit%). Approxim
m with few ental help the
100%
r 2011
I N G
y of al dults or not d to that ttent mately
ey

AIDS Com
40 | P a g
needed d(19% needthe availa
In terms o(60%) as cwas availaemotionaemotionathey needneeded a and 14% sdifference
Figure 26:
As illustrato indicatwere morsignificant(39% and particularpositive g
0%
10%
20%
30%
40%
50%
60%
70%
mmunity Re
g e
uring the preded a little mability nor the
of emotional compared witable some of l support hadl support, fewded in this reglittle more susaid they neee in the perce
Emotional Sup
ated in Figuree emotional sre likely to indtly less likely 54%, respecrly of note witgroup as comp
All/Most o
42%
search Initia
evious year. Bmore help, 7% e adequacy of
support, a grth instrumentthe time (17%d not been avwer older LGBgard (49%) asupport duringeded a lot moeptions of em
pport Availabi
26, older LGsupport was adicate the unato indicate hactively), and wth regard to npared with 8%
of Time Som
68%
ative of Amer
But for the reneeded somf instrumenta
eater proporttal help. Near%) or only occvailable duringBT adults repos was the caseg the previoure emotional
motional suppo
lity by HIV Sta
BT adults whoavailable all oavailability ofaving receivewere more likneeding a lot % of the non‐
me of the Time
27%
13%
HIV+
rica (ACRIA)
A C R
maining thirde more help, al support diff
tion indicatedrly equal propcasionally (16g the previouorted that thee for instrumes year, while support duriort availabilit
atus
o were HIV+ wor most of thef support. As ed all the emoely to indicatmore emotio‐infected grou
Only Occas
20%
+ HIV‐
)
I A C E N T
d, instrumentand 5% needfered significa
d that it was aportions indic6%). Howeveus year. Despiey had receivental help. Tw14% indicateing this periodty and adequa
were significae time (42% aseen in Figurotional suppote needing adonal support, up.
ionally N
13%
1
E R O N H
al support waded a lot morantly by HIV s
available all/mcated that emer, for almost ite the greateved all/most owenty‐three ped needing sod. There wereacy based on
antly less likeand 68%, respe 27, the HIVrt they neededditional suppendorsed by
Not at All
11%6%
19 Septembe
I V & A G
as not adequae help). Neithstatus.
most of the timotional suppone‐in‐ten (8er availability of the supporpercent said tme more supe significant HIV status.
ly than their pectively), anV+ group was ed in the pastport. This was24% of the H
r 2011
I N G
ate her
ime port 8%), of rt they pport,
peers nd
t year s HIV‐
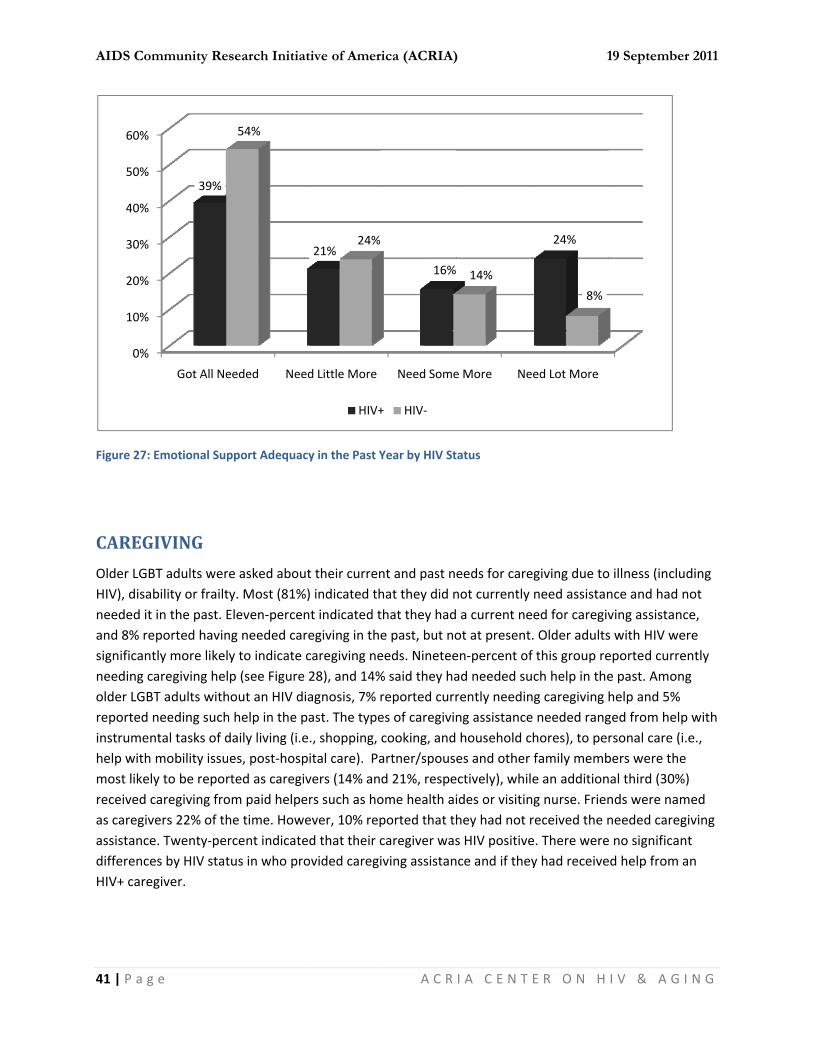
AIDS Com
41 | P a g
Figure 27:
CAREG
Older LGBHIV), disaneeded itand 8% resignificantneeding colder LGBreported instrumenhelp with most likelreceived cas caregivassistancedifferenceHIV+ care
0%
10%
20%
30%
40%
50%
60%
mmunity Re
g e
Emotional Sup
GIVING
BT adults werbility or frailt in the past. Eeported havintly more likelcaregiving helBT adults withneeding suchntal tasks of dmobility issuy to be reporcaregiving frovers 22% of the. Twenty‐peres by HIV stategiver.
Got All Ne
39%
search Initia
pport Adequac
e asked abouty. Most (81%Eleven‐percenng needed cary to indicate p (see Figurehout an HIV dh help in the pdaily living (i.ees, post‐hosprted as caregiom paid helpehe time. Howrcent indicatetus in who pro
eeded Nee
54%
ative of Amer
cy in the Past Y
ut their curren%) indicated thnt indicated tregiving in thcaregiving ne
e 28), and 14%iagnosis, 7% past. The typee., shopping, pital care). Pavers (14% aners such as hoever, 10% reped that their covided caregi
ed Little More
21%24%
HIV+
rica (ACRIA)
A C R
Year by HIV St
nt and past nhat they did nthat they hade past, but noeeds. Ninetee% said they hareported curres of caregivincooking, andartner/spousd 21%, respeome health aiported that thcaregiver wasiving assistan
Need Some
16%
+ HIV‐
)
I A C E N T
tatus
eeds for carenot currently a current neot at present.en‐percent ofad needed surently needinng assistance household ces and other ectively), whilides or visitinhey had not rs HIV positivence and if they
e More Ne
14%
1
E R O N H
egiving due toneed assistaned for caregiv. Older adultsf this group rech help in theng caregiving e needed ranghores), to pefamily membe an additiong nurse. Frienreceived the ne. There werey had receive
ed Lot More
24%
8%
19 Septembe
I V & A G
o illness (inclunce and had nving assistancs with HIV weeported curree past. Amonhelp and 5% ged from helprsonal care (ibers were thenal third (30%nds were namneeded carege no significaned help from a
r 2011
I N G
uding not ce, ere ently g
p with .e., e %) med giving nt an

AIDS Com
42 | P a g
Figure 28:
Older LGBprovide exasked parNearly onthat they past two yproviding Participanpartner (2adults wit17%, resprespectivewho was this experconsideracaregiversthemselve
0
10
20
30
40
50
60
70
80
90
mmunity Re
g e
Current and R
BT adults are xtensive carerticipants whene‐quarter (24were currentyears, and 52care and thents were mos20%). Only 5%th HIV were mpectively), andely). Twenty‐tHIV‐positive, rience (46%) aable levels of s indicated thes, but this di
Have NoCareg
67.
search Initia
Recent Caregiv
not only recipegiving assistaether they ha4%) reported tly caring for 2% had provide time since tht likely to rep% reported camore likely tod less likely totwo percent oand those was compared mutual careghat their caregid not differ b
ot Needed giving
1
88.1
ative of Amer
ing Needs by H
pients of careance to both tad provided cathat they hadsomeone, 22ded care betwhe caregivingport caring foraring for a chi report caringo have cared of older LGBTho were HIV+to their peer
giving supportgiving responby HIV status.
CurrentCareg
18
HIV+
rica (ACRIA)
A C R
HIV Status
egiving, but ptheir familiesaregiving assid provided su% said they hween three an episode did r a family meld or neighbog for a friend for a partner/T caregivers re+ themselves rs without an t among the Hnsibilities had .
ly Need giving
8.6
6.7
+ HIV‐
)
I A C E N T
revious resea of origin andistance to othuch assistancehad provided nd five years not differ signmber (44%), or, and 2% foras compared/significant oeported that were significHIV diagnosiHIV communiinterfered w
Needed CarPas
14
1
E R O N H
arch has found their familiehers within the. Of this groucare to someago. The likenificantly by Hfollowed by ar a grandchildd with their peother (15% anthey had carantly more liks (14%), suggity. Twenty‐p
with their abili
regiving in st
.35.2
19 Septembe
I V & A G
d that they es of choice. Whe past five yeup, 26% repoeone within thelihood of HIV status. a friend (24%d. Older LGBTeers (62% andd 25%, ed for someokely to indicagesting percent of ty to care for
r 2011
I N G
We ears. orted he
) or a T d
one te
r

AIDS Com
43 | P a g
USE OF
Older LGBagencies, communitsatisfactio
GSocial SecDivision/DMedicaid Resourceswere the agencies dutilizationHIV+ used(2.6 and 1
Figure 29:
Veter
***Dep
mmunity Re
g e
F FORMAL
BT adults werHIV‐related sty‐based servon with servic
Government Ocurity Office (Department oOffices (21%s Administratleast frequendiffered signin than their pd significantly1.2, respective
Use of Governtests of signif
**
**
rans Adminstra
**Chicago H
pt. of Human R
***Soci
search Initia
L SERVICE
e asked abouservices and Avices. Participces provided
Offices and Ag43%), followeon Aging (27% and 20%, restion in the prently reported ficantly by HIeers. On avery more serviceely).
nment Offices ficance]
*Medicaid Off
*Medicare Off
ation/VA Hosp
Pol
Housing Author
Resources Adm
**Dept. on Ag
ial Security Off
ative of Amer
ES
ut their use ofAIDs Service Opants were alsby the Cente
gencies. The ed by the Dep%). Next werespectively). Twevious year. Uservices. As sV status, withrage, older LGes of this type
and Agencies
0% 10%
fice
fice
ital
lice
rity
min.
ing
fice
6%
HIV+
rica (ACRIA)
A C R
f services obtOrganizationsso asked specr on Halsted.
most frequenpartment for e the Chicago wenty‐percenUse of the Veshown in Figuh HIV+ older GBT adults use on average
by HIV Status
% 20% 3
12%
13%
9%
12%
14%
10%
20%
%
13%
+ HIV‐
)
I A C E N T
tained from gs (ASOs), heacific question
ntly utilized sFamily and SHousing Authnt had also usterans Adminure 29, use of LGBT adults med 1.7 servicethan did thei
[* p < .05, ** p
0% 40%
31%
37%
34%
31%
39%
39%
1
E R O N H
overnment olth‐related ses about their
ervice in this upport Servichority (21%) ased the Depanistration (8%f government more likely toes (SD=1.9). Tir non‐infecte
p < .01, *** p <
50% 60%
%
%
19 Septembe
I V & A G
offices and ervices, and outilization of
group was thces, Senior and Medicarertment of Hu
%) and Police offices and o report such Those who weed counterpar
< .001, Chi‐squ
70%
65%
r 2011
I N G
other f and
he
e and uman (12%)
ere rts
uare

AIDS Com
44 | P a g
Hsignificantdiagnosis followed and Howareported which is lireported
Figure 30:
***Ch
***T
***H
***Chi
mmunity Re
g e
HIV‐related Setly more likel(see Figure 3by Test Positiard Brown Heusing serviceikely due to tusing 2.9 HIV
Use of HIV‐relsignificance]
*
hicago Women
**
*South Sid
Test Positive A
Howard Brown
cago House &
*Cen
***AIDS Found
search Initia
ervices and ASy to report th30). The AIDS ive Aware Neealth Center (s at either thesting and coV‐related/ASO
lated Services
***Other ASOs
n's AIDS Project
**CORE Center
de Help Center
Aware Network
n Health Center
Social Services
nter on Halsted
***BeHIV
dation Chicago
ative of Amer
SOs. As expehe use of ASOFoundation o
etwork (41%),38%). Howeve Center on Hounseling progO services, sig
and ASOs [* p
0% 10%
s
t
r
r
k
r
s
d
V
o
0%
0%
0%
3%
2%
2%
0%
2%
HIV+
rica (ACRIA)
A C R
cted, older LGOs and HIV‐reof Chicago wa the HIV/AIDSver, approximHalsted or Hograms at thesnificantly gre
p < .05, ** p < .
% 20%
17%
2
16%
13%
12%
+ HIV‐
)
I A C E N T
GBT adults whlated servicesas the most frS services fro
mately 20% of oward Brown se agencies. eater than the
.01, *** p < .00
30% 40%
23%
31%
3
26%
3
26%
1
E R O N H
ho were HIV‐s than those wrequently meom the Centernon‐HIV infe(23% and 17%On average, oe 0.3 reported
01, Chi‐square
% 50%
41%
38%
38%
19 Septembe
I V & A G
positive werewithout an Hentioned (57%r on Halsted (ected LGBT ad%, respectiveolder LGBT add by their pee
e tests of
60%
57%
r 2011
I N G
e IV %), (38%) dults ely), dults ers.
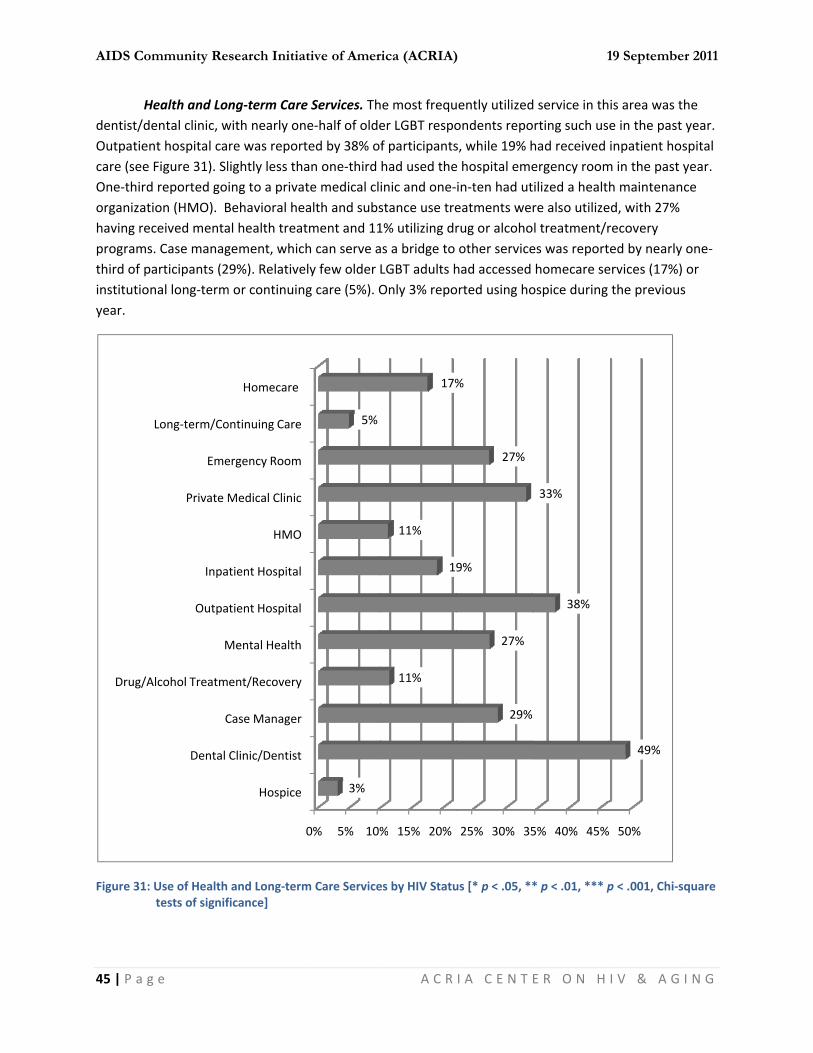
AIDS Com
45 | P a g
Hdentist/deOutpatiencare (see One‐thirdorganizathaving recprogramsthird of painstitutionyear.
Figure 31:
Drug/A
mmunity Re
g e
Health and Loental clinic, wnt hospital caFigure 31). Sld reported goion (HMO). Bceived mentas. Case managarticipants (2nal long‐term
Use of Health tests of signif
Dental
C
Alcohol Treatm
M
Outpa
Inpa
Private M
Eme
Long‐term/Co
search Initia
ng‐term Carewith nearly onre was reportlightly less thaing to a privaBehavioral heal health treatgement, whic9%). Relative
m or continuin
and Long‐termficance]
Hospice
Clinic/Dentist
Case Manager
ent/Recovery
Mental Health
tient Hospital
tient Hospital
HMO
Medical Clinic
ergency Room
ontinuing Care
Homecare
ative of Amer
e Services. Thne‐half of oldeted by 38% oan one‐third te medical clealth and substment and 11h can serve aely few older ng care (5%). O
m Care Service
0% 5% 10%
3%
5%
rica (ACRIA)
A C R
he most frequer LGBT respof participantshad used theinic and one‐stance use tre1% utilizing dras a bridge to LGBT adults hOnly 3% repo
es by HIV Statu
% 15% 20%
11%
19
11%
17%
)
I A C E N T
uently utilizedondents repos, while 19% he hospital emein‐ten had uteatments werug or alcohoother servicehad accessed orted using ho
us [* p < .05, **
25% 30% 35
29%
27%
9%
27%
%
1
E R O N H
d service in thorting such ushad received ergency roomtilized a healtre also utilizeol treatment/res was reporthomecare seospice during
* p < .01, *** p
5% 40% 45%
38%
33%
19 Septembe
I V & A G
is area was the in the past inpatient hos
m in the past yh maintenanced, with 27% recovery ted by nearly ervices (17%) the previous
p < .001, Chi‐sq
% 50%
49%
r 2011
I N G
he year. spital year. ce
one‐or s
quare
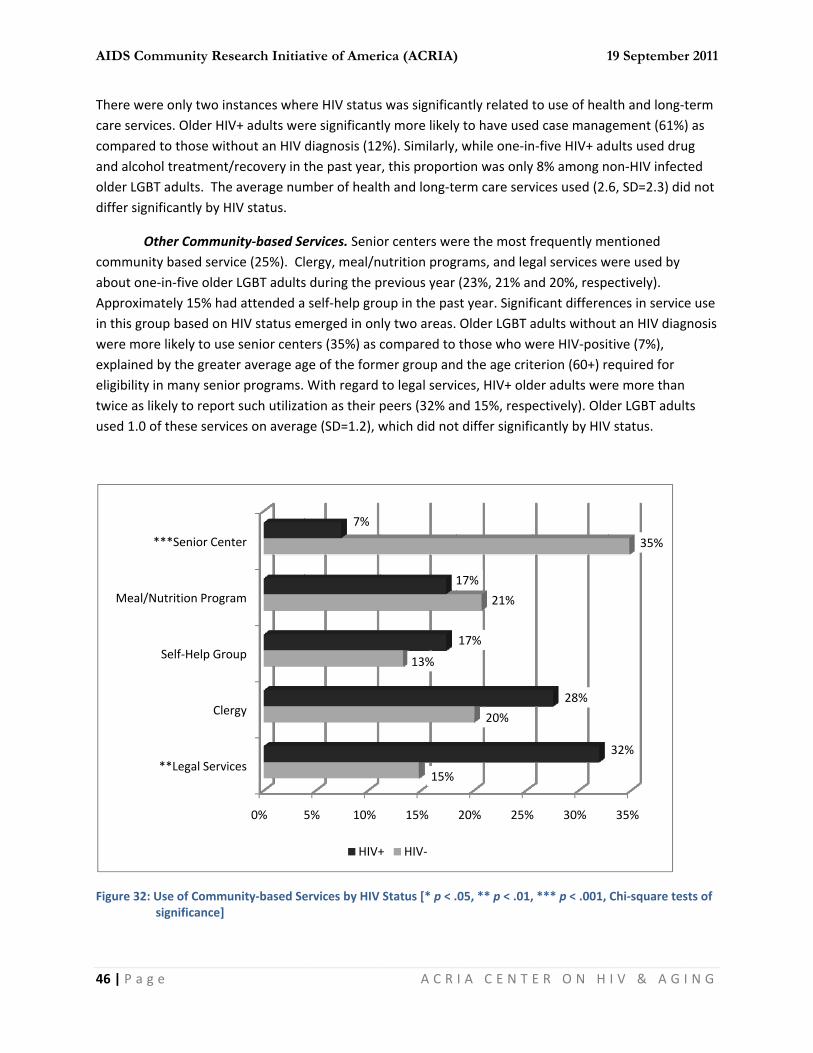
AIDS Com
46 | P a g
There wecare servicomparedand alcoholder LGBdiffer sign
Ocommunitabout oneApproximin this growere morexplainedeligibility twice as liused 1.0 o
Figure 32:
Meal/N
mmunity Re
g e
re only two inces. Older HId to those withol treatmentBT adults. Thenificantly by H
Other Commuty based serve‐in‐five oldemately 15% haoup based on re likely to usd by the greatin many senioikely to reporof these servi
Use of Commusignificance]
**Legal Servi
Cle
Self‐Help Gro
Nutrition Progr
***Senior Cen
search Initia
nstances wheV+ adults wethout an HIV /recovery in te average numHIV status.
nity‐based Sevice (25%). Clr LGBT adultsad attended aHIV status eme senior centter average agor programs. rt such utilizaces on averag
unity‐based Se
0%
ices
ergy
oup
ram
nter
ative of Amer
ere HIV statusre significantdiagnosis (12the past yearmber of healt
ervices. Seniolergy, meal/ns during the p self‐help gromerged in oners (35%) as cge of the formWith regard tion as their pge (SD=1.2), w
ervices by HIV
5% 10%
7%
HIV+
rica (ACRIA)
A C R
s was significaly more likely2%). Similarly,r, this proportth and long‐te
or centers weutrition progprevious year oup in the pasly two areas.compared to mer group anto legal servipeers (32% anwhich did not
Status [* p < .
15%
15%
13%
+ HIV‐
)
I A C E N T
antly related ty to have used, while one‐intion was onlyerm care serv
ere the most frams, and leg(23%, 21% anst year. Signif Older LGBT athose who wd the age critces, HIV+ oldnd 15%, respt differ signifi
.05, ** p < .01,
20% 25%
20%
21%
17%
17%
1
E R O N H
to use of head case managn‐five HIV+ ady 8% among nvices used (2.
frequently megal services wnd 20%, respeficant differenadults withouwere HIV‐positterion (60+) reder adults werectively). Oldcantly by HIV
, *** p < .001,
% 30%
28%
19 Septembe
I V & A G
lth and long‐gement (61%dults used drunon‐HIV infect6, SD=2.3) did
entioned were used by ectively). nces in servicut an HIV diagtive (7%), equired for re more thander LGBT adulV status.
Chi‐square tes
35%
35%
32%
r 2011
I N G
term ) as ug ted d not
e use gnosis
ts
sts of
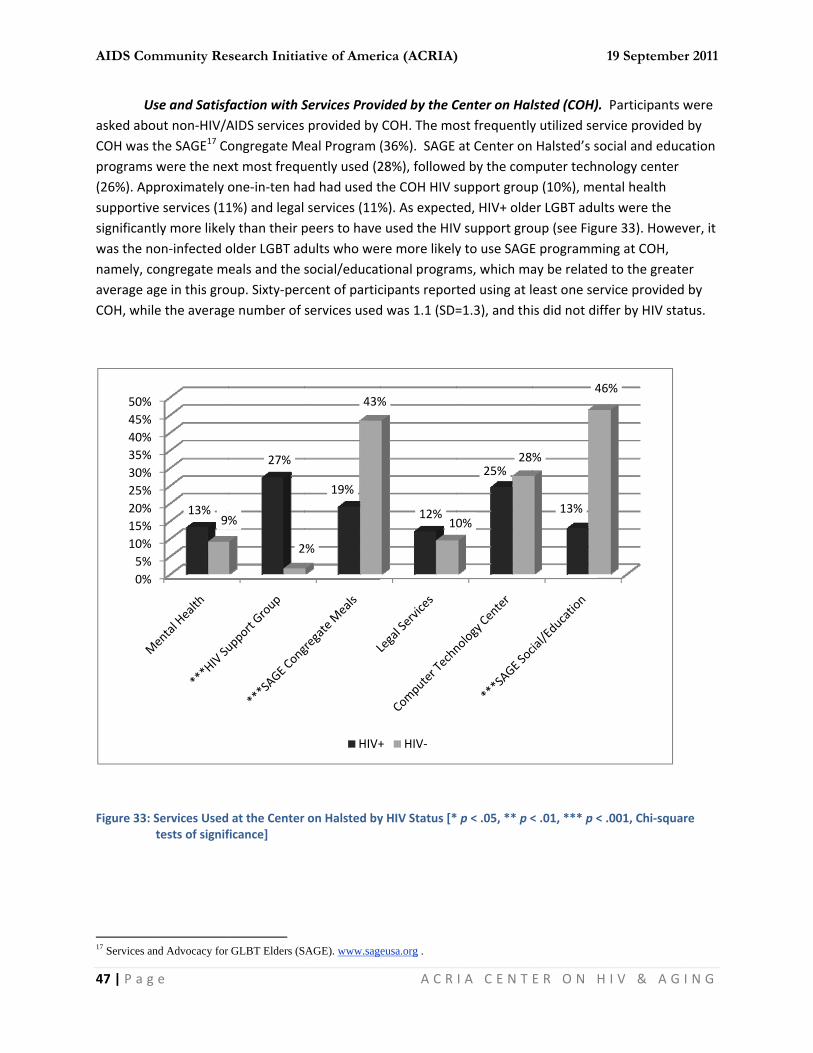
AIDS Com
47 | P a g
Uasked aboCOH was programs(26%). Apsupportivsignificantwas the nnamely, caverage aCOH, whil
Figure 33:
17 Services a
0%5%
10%15%20%25%30%35%40%45%50%
mmunity Re
g e
Use and Satisfout non‐HIV/Athe SAGE17 Cos were the nexpproximately oe services (11tly more likelon‐infected ocongregate mage in this grole the averag
Services Usedtests of signif
and Advocacy for
13%9
search Initia
faction with SAIDS servicesongregate Mxt most frequone‐in‐ten ha1%) and legaly than their polder LGBT adeals and the oup. Sixty‐pere number of
at the Centerficance]
r GLBT Elders (S
27%
%
2
ative of Amer
Services Prov provided by eal Program (uently used (2ad had used t services (11%peers to havedults who wesocial/educatrcent of particservices used
r on Halsted by
SAGE). www.sag
19%
2%
43%
HIV+
rica (ACRIA)
A C R
vided by the CCOH. The mo(36%). SAGE28%), followethe COH HIV s%). As expecte used the HIVre more likelytional progracipants repord was 1.1 (SD=
y HIV Status [*
eusa.org .
12%
%
10
+ HIV‐
)
I A C E N T
Center on Halost frequentlyat Center on
ed by the comsupport grouped, HIV+ oldeV support groy to use SAGEms, which mated using at l=1.3), and thi
* p < .05, ** p <
25%
0%
28
1
E R O N H
lsted (COH). y utilized serv Halsted’s soc
mputer technop (10%), mener LGBT adultoup (see FigurE programminay be related east one servis did not diff
< .01, *** p < .
13%
%
46
19 Septembe
I V & A G
Participants wvice provided cial and educology center ntal health ts were the re 33). Howevng at COH, to the greatevice providedfer by HIV stat
001, Chi‐squar
%
r 2011
I N G
were by ation
ver, it
er by tus.
re
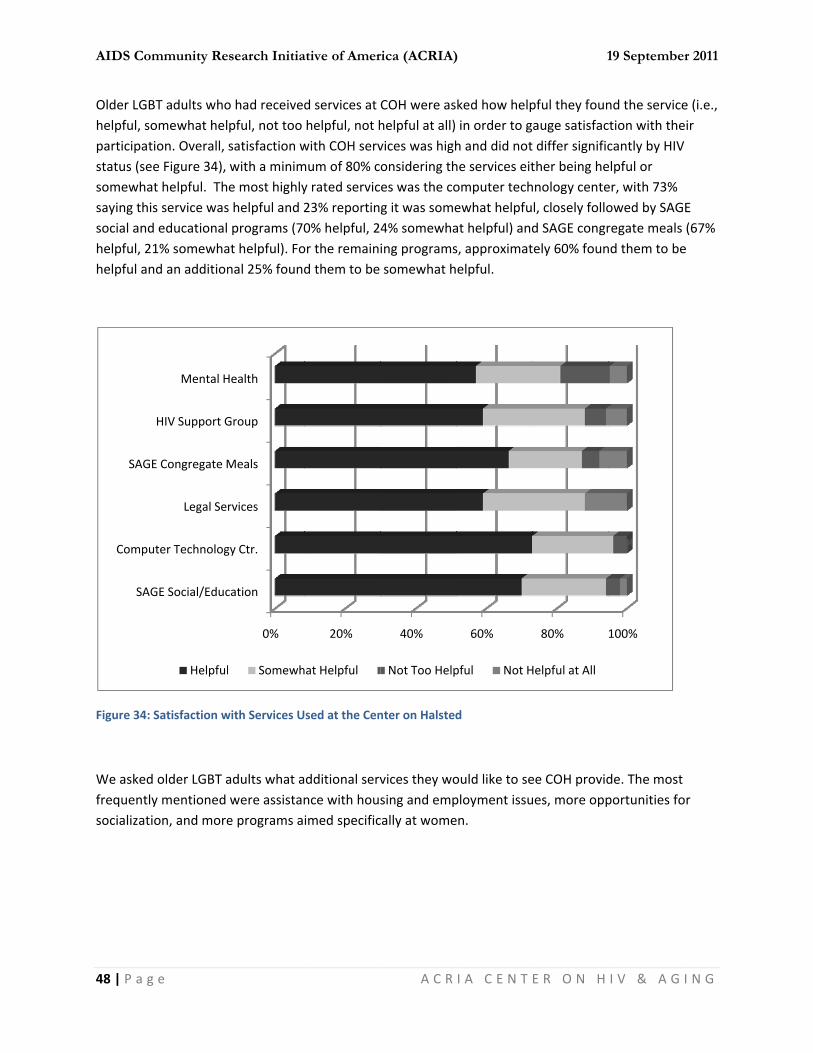
AIDS Com
48 | P a g
Older LGBhelpful, soparticipatstatus (sesomewhasaying thisocial andhelpful, 2helpful an
Figure 34:
We askedfrequentlysocializati
SAG
Compu
SAGE
mmunity Re
g e
BT adults whoomewhat heltion. Overall, e Figure 34), at helpful. Ths service wasd educational 1% somewhand an addition
Satisfaction w
d older LGBT ay mentioned ion, and more
GE Social/Educ
uter Technolog
Legal Ser
E Congregate M
HIV Support G
Mental H
Helpful
search Initia
o had receivedpful, not too satisfaction wwith a minime most highlys helpful and 2programs (70
at helpful). Fonal 25% found
with Services U
adults what awere assistane programs a
0%
cation
gy Ctr.
rvices
Meals
Group
Health
Somewh
ative of Amer
d services at helpful, not hwith COH servmum of 80% cy rated servic23% reportin0% helpful, 2or the remaind them to be
Used at the Cen
dditional servnce with houimed specific
20%
hat Helpful
rica (ACRIA)
A C R
COH were ashelpful at all) vices was highonsidering thes was the cog it was some4% somewhaing programssomewhat h
nter on Halsted
vices they wosing and empcally at wome
40%
Not Too Help
)
I A C E N T
ked how helpin order to gh and did nothe services eitomputer techewhat helpfuat helpful) ands, approximatelpful.
d
ould like to seployment issuen.
60%
pful Not H
1
E R O N H
pful they founauge satisfact differ significther being hehnology centel, closely follod SAGE congrtely 60% foun
ee COH providues, more opp
80%
Helpful at All
19 Septembe
I V & A G
nd the servicection with thecantly by HIVelpful or er, with 73% owed by SAGregate meals nd them to be
de. The most portunities fo
100%
r 2011
I N G
e (i.e., eir
E (67% e
or
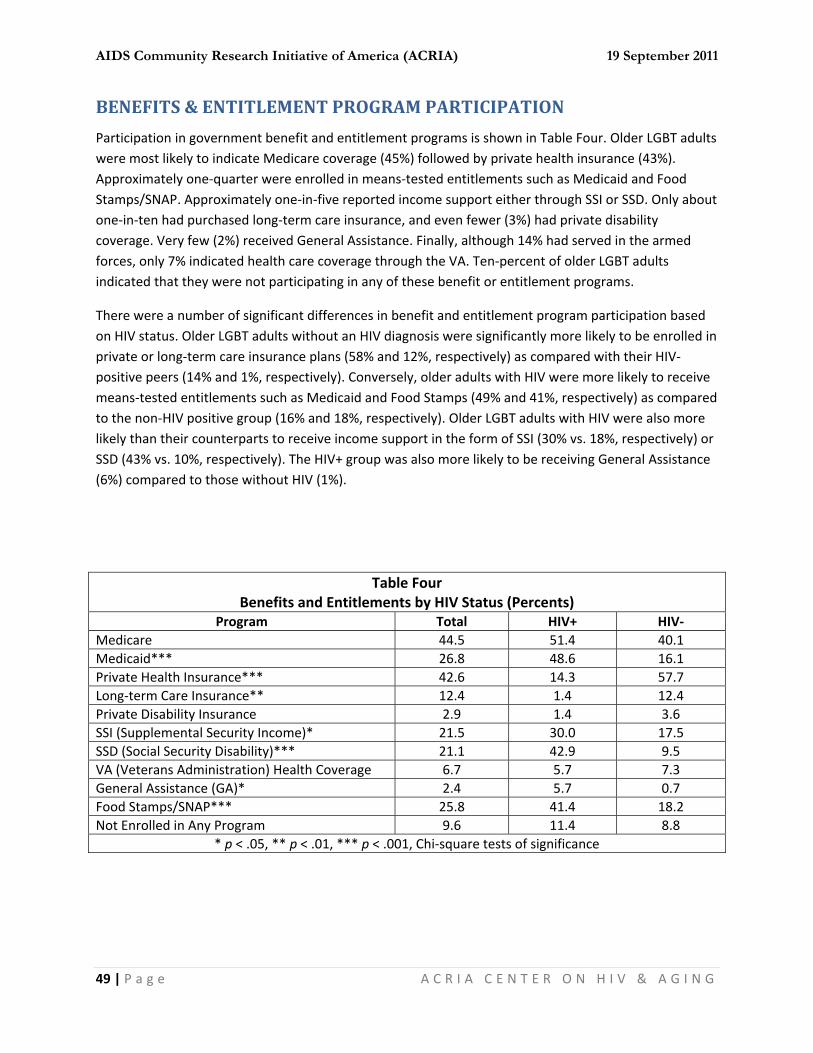
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
49 | P a g e A C R I A C E N T E R O N H I V & A G I N G
BENEFITS & ENTITLEMENT PROGRAM PARTICIPATION
Participation in government benefit and entitlement programs is shown in Table Four. Older LGBT adults were most likely to indicate Medicare coverage (45%) followed by private health insurance (43%). Approximately one‐quarter were enrolled in means‐tested entitlements such as Medicaid and Food Stamps/SNAP. Approximately one‐in‐five reported income support either through SSI or SSD. Only about one‐in‐ten had purchased long‐term care insurance, and even fewer (3%) had private disability coverage. Very few (2%) received General Assistance. Finally, although 14% had served in the armed forces, only 7% indicated health care coverage through the VA. Ten‐percent of older LGBT adults indicated that they were not participating in any of these benefit or entitlement programs.
There were a number of significant differences in benefit and entitlement program participation based on HIV status. Older LGBT adults without an HIV diagnosis were significantly more likely to be enrolled in private or long‐term care insurance plans (58% and 12%, respectively) as compared with their HIV‐positive peers (14% and 1%, respectively). Conversely, older adults with HIV were more likely to receive means‐tested entitlements such as Medicaid and Food Stamps (49% and 41%, respectively) as compared to the non‐HIV positive group (16% and 18%, respectively). Older LGBT adults with HIV were also more likely than their counterparts to receive income support in the form of SSI (30% vs. 18%, respectively) or SSD (43% vs. 10%, respectively). The HIV+ group was also more likely to be receiving General Assistance (6%) compared to those without HIV (1%).
Table Four Benefits and Entitlements by HIV Status (Percents)
Program Total HIV+ HIV‐ Medicare 44.5 51.4 40.1 Medicaid*** 26.8 48.6 16.1 Private Health Insurance*** 42.6 14.3 57.7 Long‐term Care Insurance** 12.4 1.4 12.4 Private Disability Insurance 2.9 1.4 3.6 SSI (Supplemental Security Income)* 21.5 30.0 17.5 SSD (Social Security Disability)*** 21.1 42.9 9.5 VA (Veterans Administration) Health Coverage 6.7 5.7 7.3 General Assistance (GA)* 2.4 5.7 0.7 Food Stamps/SNAP*** 25.8 41.4 18.2 Not Enrolled in Any Program 9.6 11.4 8.8
* p < .05, ** p < .01, *** p < .001, Chi‐square tests of significance

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
50 | P a g e A C R I A C E N T E R O N H I V & A G I N G
BARRIERS TO SERVICES
We asked older LGBT adults about perceived barriers they faced when accessing community‐based services (see Table Five). These barriers can be grouped into access barriers, staff and organizational barriers, and contextual issues. Fifty‐eight percent of participants reported at least one barrier to service, and the average number of barriers reported was 2.8 (SD=3.5). Older adults with HIV reported a significantly higher number of barriers, on average, in comparison to the non‐HIV infected group (3.9 and 2.2 barriers, respectively).
As a group, access barriers were the most frequently mentioned, ranging between 23% and 43%. Financial considerations were prominent, with 43% saying they didn’t think they would be eligible to receive free services, while 32% worried about the cost of such services. Knowledge of available services (24%) and where one could obtain such services (35%) were also frequently mentioned. Twenty‐eight percent felt that the process of getting services was confusing and/or difficult, while 23% thought that they would have to wait too long.
Table Five Perceived Barriers to Community‐based Services
Service Access Barriers Valid Percents Don’t think services exist around here 23.5 Don’t know where to go for services 34.5 Would have to wait too long for services 23.4 Services cost too much to afford 31.7 Don’t think eligible for free services 43.1 Process of getting services too confusing/difficult 28.1
Staff/Organizational Barriers Valid Percents People at the agency not helpful/Don’t seem motivated to help 21.2 People who run services don’t like people like you 10.8 Afraid you won’t be treated if you go for services 9.9 People at the agency don’t speak the same language as you 5.5 Have trouble telling people at the agency what you need 8.4
Contextual Barriers Valid Percents Its’ hard to get there (transportation) 17.2 Don’t know what to do with kids when getting services 4.0 Someone might find out HIV status 6.9 Hard to make or keep appointments 7.4 You have to take care of other people 6.5 Worry that family/friends would be against the service 5.0
With regard to staff and organizational barriers, the most frequently mentioned was that staff was unhelpful or seemed unmotivated which was endorsed by over one‐fifth of older LGBT adults. Stigma and discrimination issues were mentioned by approximately one‐in‐ten, namely, feeling that staff did not like people like themselves or that they would not receive services if they tried. Less than 10%
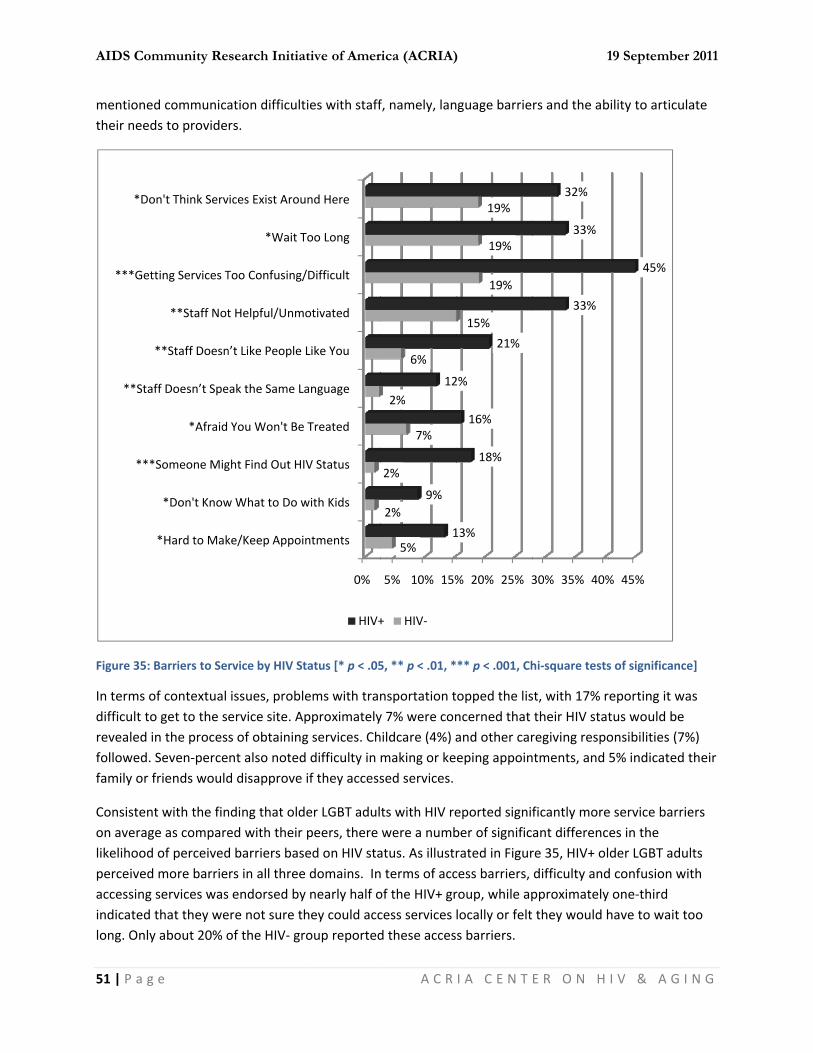
AIDS Com
51 | P a g
mentionetheir need
Figure 35:
In terms odifficult torevealed ifollowed. family or f
Consistenon averaglikelihoodperceivedaccessing indicated long. Only
***
**Sta
***Get
*Do
mmunity Re
g e
ed communicads to provide
Barriers to Se
of contextual o get to the sin the procesSeven‐percefriends would
nt with the finge as compared of perceivedd more barrieservices wasthat they wey about 20% o
*Hard to Mak
*Don't Know
*Someone Mig
*Afraid
aff Doesn’t Spe
**Staff Doesn
**Staff Not
tting Services T
on't Think Serv
search Initia
ation difficultrs.
rvice by HIV St
issues, problervice site. As of obtainingnt also notedd disapprove
nding that olded with their d barriers basrs in all threes endorsed byere not sure thof the HIV‐ gr
ke/Keep Appoi
w What to Do w
ght Find Out HI
You Won't Be
eak the Same L
n’t Like People
t Helpful/Unm
Too Confusing/
*Wait T
vices Exist Arou
ative of Amer
ties with staff
tatus [* p < .05
ems with tranpproximatelyg services. Chd difficulty in if they access
der LGBT adulpeers, there ed on HIV stae domains. Iny nearly half ohey could accroup reported
0%
ntments
with Kids
IV Status
Treated
anguage
Like You
otivated
/Difficult
Too Long
und Here
HIV+
rica (ACRIA)
A C R
f, namely, lan
5, ** p < .01, *
nsportation ty 7% were conhildcare (4%) amaking or kesed services.
ts with HIV rewere a numbatus. As illustrn terms of accof the HIV+ grcess services d these acces
5% 10% 15%
5%
2%
2%
7%
2%
6%
1
9%
12
+ HIV‐
)
I A C E N T
nguage barrie
** p < .001, Ch
opped the lisncerned that and other careping appoin
eported signifber of significrated in Figurcess barriers, roup, while aplocally or felts barriers.
% 20% 25% 3
15%
19%
19%
19%
13%
18%
16%
2%
21%
1
E R O N H
rs and the ab
hi‐square tests
st, with 17% rtheir HIV statregiving respontments, and
ficantly moreant differencre 35, HIV+ oldifficulty andpproximately they would h
30% 35% 40%
33%
33%
32%
19 Septembe
I V & A G
bility to articu
s of significanc
reporting it wtus would beonsibilities (75% indicated
e service barres in the der LGBT adud confusion wy one‐third have to wait t
% 45%
45%
r 2011
I N G
late
ce]
as %) their
iers
ults with
too

AIDS Com
52 | P a g
With regapeers to fappears tcomparedlanguage
Older HIVstatus (185% or few
NEED F
Older LGButilized he(e.g., famparticipanyear was significant
Figure 36:
Vistin
Assista
mmunity Re
g e
ard to staff anfeel that staff o be an issued with only 6%barriers or no
V+ LGBT adult8%), difficultywer of the HIV
FOR SERV
BT adults werealth and socily, communints in the curr2.5 (SD=2.2) atly by HIV sta
Need for Serv
Help with
ng Nurse/Hom
Someon
nce Getting to
Post‐
Personal/Fam
H
Meals Bro
search Initia
nd organizatiowas unmotiv, with one‐in‐% of the non‐ot receiving t
s were also m in making orV‐ group repo
VICES IN T
e asked aboucial services, wty‐based orgarent study anand the averatus.
vices in the Pre
Socialization
h Entitlements
me Health Aide
ne to Call/Visit
o Doctor/Clinic
‐Hospital Care
ily Counseling
Finding a Job
Home Repairs
Houeskeeping
ught to Home
ative of Amer
onal barriers, vated or unhe‐five HIV+ ad‐HIV diagnosereatment.
more likely to r keeping apprted these co
THE PREV
ut their need fwhether theiranization). Figd unmet neeage number o
evious Year
0% 10%
4%
rica (ACRIA)
A C R
HIV+ LGBT oelpful (33% anults feeling “sed group. Sim
cite contextupointments (1ontextual serv
VIOUS YEA
for services inr needs had bgure 36 showd. The averagof unmet nee
20%
23
12%
18%
23
18%
)
I A C E N T
lder adults wnd 15%, respestaff didn’t lik
milar patterns
ual issues, suc3%) and childvice barriers.
AR & UNM
n the past yeabeen met, andws the extent ge number ofeds was 0.6 (S
30% 40%
3%
25%
32%
28%
29%
3%
1
E R O N H
were twice as ectively). HIVke people likewere observe
ch as disclosudcare issues (
MET NEED
ar from a list d if so, who pof need for sef services neeSD =0.9); this
% 50%
51
19 Septembe
I V & A G
likely as theirV stigma also e them” as ed regarding
ure of their HI9%). In contr
DS
of commonlyrovided the hervices amoneded in the padid not differ
60%
1%
r 2011
I N G
r
IV ast,
y help ng ast r

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
53 | P a g e A C R I A C E N T E R O N H I V & A G I N G
Meals Brought to the Home. Four‐percent of older LGBT adults reported that they needed meals brought to them at home during the previous year (n=8). Of those, two‐thirds indicated that they had not gotten all the help they needed. Sources of help for this need included family and friends (44%), while 56% received help from community‐based organizations (i.e., Vital Bridges, Meals‐on‐Wheels). HIV status was not significantly related to the need for meals at home, whether this need was met, or who provided the help.
Housekeeping and Home Care. Nearly one‐in‐five older LGBT adults reported that they had needed help with housekeeping or personal care in the home over the previous year (18%). Eighteen‐percent of those needing such help indicated that they did not receive all the help they needed with housekeeping and care in the home. In most cases, family, friends and neighbors supplied the needed assistance (45%), although the Division of Rehabilitation Services (DRS) provided assistance to 18% of those with this need. An additional 38% received help from other sources, usually other social service agencies (e.g., Catholic Charities), the VA, or paid helpers. The need for housekeeping/home care, the extent to which this need was met, and source of assistance did not differ significantly by HIV status.
Home Repairs. Help with home repairs was needed by 23% of older LGBT adults, and of those who needed this help, 26% did not receive all the help they needed. Friends and neighbors were the most likely to have provided this help (48%), while family members helped 17% of the time. Only 6% had turned to the Illinois Housing Development Authority Home Modification Program. Approximately one‐third had hired a contractor/paid helper or asked for assistance from the building superintendent or management. The need for home repairs, as well as unmet need and source of support did not vary by HIV status.
Help Finding a Job. Eighteen‐percent of older LGBT adults reported that they had needed help finding a job in the past year. Of those, slightly less than two‐thirds (64%) did not receive all the help that they needed in this area. Nearly two‐thirds (64%) turned to family and friends for help in finding a job, while 18% had received help from Chicago House. The remainder had mostly received help from the other agencies, such as the Illinois Department of Employment Services or Jewish Vocational Services. The need for help in finding a job, unmet need, and sources of assistance were not related to HIV status.
Personal or Family Counseling. Counseling assistance, either personal or family, was the third highest in terms of need in the previous year (29%), and over one‐quarter (27%) who needed this assistance reported that they did not receive all the help they needed. Relative to other service needs, family and friends were not relied upon extensively (26%). Nearly one‐in‐five (19%) had turned to COH for such assistance. The remaining two‐thirds received help with counseling from private therapists, hospitals (including the VA), and other community‐based organizations. The need for personal and family counseling, unmet need, and source of help did not vary significantly by HIV status.
Post‐Hospital Care. Approximately one‐in‐five (21%) older LGBT adults reported needing help following a stay in the hospital in the previous year and most (86%) received all the help they needed in this regard. Sources of assistance for help after a hospital stay was largely provided by friends and neighbors (54%) followed by family members (30%). Fourteen‐percent had received assistance from a
AIDS Community Research Initiative of America (ACRIA) 19 September 2011
54 | P a g e A C R I A C E N T E R O N H I V & A G I N G
case manager. Twenty‐four percent received help from other community‐based organizations. HIV status was not significantly related to need for post‐hospital help, unmet need, or source of support.
Someone to Take to Doctor/Clinic. The second most frequently mentioned need by older LGBT adults in the past year was assistance in getting to the doctor’s office or a medical clinic (32%). Only 10% reported not receiving all the help they needed in this regard. Family (41%) and friends/neighbors (54%) were the most frequently named sources of assistance, although 10% had relied on a case manager and 15% had used some other source of help (the PACE program was most often mentioned). The need for an escort to the doctor/clinic, unmet need and source of assistance did not vary significantly by HIV status.
Someone to Call or Visit Regularly. The need for a regular contact, either by a visit in‐person or by phone, was indicated by one‐quarter of older LGBT adults. Seventeen‐percent reported that they did not have their needs in this area met. Support in this area was equally likely to come from family (41%) as compared with friends (44%). Six‐percent had utilized the SAGE friendly visiting program, and 9% had used the services of another source, with medical personnel being the most frequently mentioned. HIV status was not significantly related to need, unmet need, or source of assistance in this area.
Visiting Nurse, Home Health Aide, or Home Attendant. Need for this type of homecare service was reported by 12% of older LGBT adults and nearly one‐third who needed such help indicated they did not receive all the assistance they needed in the past year. Thirteen‐percent relied on family members and the same proportion relied on friends. Seventeen‐percent had turned to a case manager for help with homecare services, but most (58%) had turned to some type of home health care agency for assistance. The need for this type of assistance, unmet need and source of support were again unrelated to HIV status.
Help with Government Entitlements. Help navigating the entitlement system was an expressed need for 23% of older LGBT adults in the past year. Approximately one‐third had turned to family (15%) or friends (15%) for assistance in this area. Twenty‐one percent had used Ryan White Case Management, and all of these individuals were HIV positive. About half (49%) had turned to some other social service organization for help with entitlements. The need for help with entitlement in the past year differed significantly by HIV status, with 40% of older LGBT HIV+ adults indicating this need as compared with 14% of non‐HIV diagnosed individuals. However, the proportion whose needs were not met and the source of assistance did not differ significantly by HIV status.
Someplace to Socialize or Meet People. Need for socialization opportunities was the most frequently mentioned expressed need among older LGBT participants in the current study. Over half (51%) expressed the need for more socialization and 14% reported that they did not receive all the help they needed in this regard. COH was the most frequently cited source of providing a place for socialization (39%), while 19% had turned to some other community‐based organization such as a church, ASO or Howard Brown. One‐quarter (24%) had received help in this regard from friends and neighbors, and 19% reported family members as their source of assistance. The need for socialization and unmet need in this area did not differ as a function of HIV status. However, older LGBT adults who

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
55 | P a g e A C R I A C E N T E R O N H I V & A G I N G
were not diagnosed with HIV were more likely to name COH as a source of socialization help (75%) as compared with the HIV+ group (33%).
CONCLUSIONS & IMPLICATIONS
This research study data conducted for COH provides a comprehensive assessment of the present and emerging needs of their aging LGBT community. There are several subgroups within this study which include those defined by gender and those defined by HIV serostatus. Many significant differences were seen when HIV status is a factor. Some of these differences are most evident in health measurements. But it is noteworthy that the HIV+ group, who are overwhelmingly men, have an average age of 55, while those without an HIV diagnosis were 62 years‐of‐age on average. This age difference is one contributing factor to observed group differences base on HIV serostatus.
This sample of older LGBT adults reflects the immediate environs of Chicago. Nearly half own their residence, with most others having secure housing. However, an almost equal percentage stated they were unemployed and were barely able to meet expenses. This population has social networks that are largely reliant on friends rather than families of origin. The majority lives alone and do not have a long‐term partner/relationship. Without the typical supports intrinsic to close family connections and those derived from long‐term relationships, this group of older adults will confront increasing financial challenges as well as increased isolation. Sustaining the costs of a residence by a single aging person, with a fixed income, reduced work options and decreased opportunities for socialization, creates high risk for successful aging. This is especially true of the HIV+ group within this study. Additionally the burden of chronic disease can make normal routines difficult and strain financial resources.
The vast majority of the sample report being in good health, and many receive coverage for healthcare via private insurance. But rates of smoking, substance and alcohol use, and depression may represent a risk to their current favorable health status. Over half of the HIV+ group currently smokes cigarettes on a regular basis. This behavior places them at very high risk for multiple illnesses and must be addressed. One‐in‐five of older LGBT adults were in a substance abuse recovery program, and others may also be at risk for substance use problems. Outreach to encourage enrollment in these programs is needed.
Depression is the single most consistent predictor of poor health outcomes. The high rates of depressive symptoms in this population reflect a major need for targeted mental health services for older adults in general, that appear to be exacerbated among the older LGBT population. To address this problem, encouraging those with depression to seek care from their health providers is needed, as well as public education campaigns that describe the symptoms and management options of depression. Depression in the LGBT population in part reflects the internalization of social stigmas that contribute to social isolation and destructive self‐medication behaviors.
The sexual health of these aging LGBT people provides data that is new and emerging. The study shows clearly that regardless of HIV status large proportions of older LGBT adults engage in sexual behaviors that place them and partners at risk for STI infection including HIV, regardless of HIV status. These data support the need for STI and HIV prevention programs that target the LGBT older adult as well as

AIDS Community Research Initiative of America (ACRIA) 19 September 2011
56 | P a g e A C R I A C E N T E R O N H I V & A G I N G
education and social media campaigns that are inclusive of people who are every age and sexual identity. Sexual desire and behavior is not the domain exclusively of young people. That misperception must be changed.
Barriers were encountered by this population as they sought aging support services outside of the COH programs. Those perceived barriers can only be ameliorated and removed by communication and interaction between the LGBT communities, especially COH. In order to achieve successful aging the older LGBT adult must be able to access all community based services. This will require outreach and education to mainstream senior service providers to ensure that they are culturally competent when engaging older LGBT and/or HIV‐positive adults, and understand the special needs and characteristics of these populations.
The service need that was identified as having the highest priority and highest level of unmet need was opportunities for socialization. Socialization has long been recognized as a critical determinant of successful or healthy aging. As one ages social networks reduce in size as friends die or can no longer travel due to disease burden. A spouse who survives the death of a partner is often left with surviving children and other relatives who share this loss and provide support. This is not typical of the aging LGBT adult. Research shows that those older adults with strong social networks often have a higher quality of life, longer life spans and better health status. Many studies show that strong social support may be a protection against cognitive decline. Socialization allows a person to feel connected and to create meaningful relationships. Catalysts for this include social gatherings, as well as home visits and even the telephone call or connections that occur on line. Providing opportunities for socialization that are welcoming and accessible for large numbers of aging LGBT people with diverse interest and personalities is a massive challenge. Addressing that challenge will define the near future of LGBT centers and result in better health and well‐being for those whom they serve.