hanes h. brindley, sr. orthopaedic lectureship and...
TRANSCRIPT
June 13, 2014
Hanes H. Brindley, Sr. Orthopaedic Lectureship
and Orthopaedic Resident Research Forum
Hanes H. Brindley, Sr.
Orthopaedic Lectureshipand
Orthopaedic Resident Research Forum
Co-editors:Douglas Fornfeist M.D. Gina Du ParProgram Director, Medical Editor,Orthopaedic Residency Program Publications Department
3
Hanes H. Brindley, Sr. M.D.
A native of Temple, the late Hanes H. Brindley, Sr., M.D. was a graduate of the University of Texas at Austin. He earned a medical de-gree from Washington University in St. Louis, Missouri, and completed a surgical internship at Charity Hospital in New Orleans in 1943. Fol-lowing his internship, he joined the U.S. Army Medical Corps, serving in Europe during World War II. After returning to Texas, he completed a surgical residency at Scott & White and earned a master’s degree in anatomy from the University of Texas Medical Branch at Galveston. In 1950, Dr. Brindley completed a three-year orthopaedic residency at the W.C. Campbell Clinic at the University of Tennessee.
In 1951, he returned to Scott & White to practice orthopaedic surgery. He was Chief of the Division of Orthopaedic Surgery from 1974 until 1980.
As a member of the Board of Trustees of Scott & White Memorial Hospital and Scott, Sher-wood & Brindley Foundation from 1968 to 1989, Dr. Brindley served as Secretary (1969 –1972); Second Vice President (1972 – 1979); and First Vice President (1979 – 1982). He was then elected President of the Board and served in that capacity until 1984.
In addition, Dr. Brindley was a member of more than 20 local, state, regional, and national professional organizations. He was Vice President of the American Orthopaedic Association in 1979 and 1980; Past President of the Texas Orthopaedic Association in 1979 and 1980; and Vice President of the Clinical Orthopaedic Society. He also served as Chairman of the Liaison Commit-tee for the American College of Surgeons and President of the Southwestern Chapter of the Ameri-can College of Surgeons.
While at Scott & White, Dr. Brindley trained about eighty orthopaedic residents. According to his son, Dr. George W. Brindley, Dr. Brindley “instilled a desire for excellence in patient care and encouraged the natural inquisitiveness of young orthopaedic surgeons.”
Dr. Brindley’s contributions went far beyond the world of medicine and surgery. He was also a member of the first elected Temple Independent School District Board and a founding 21-year member of the Temple College Board. He received gubernatorial appointment to the Crippled Children’s Medical Advisory Commission of the State Health Department (1968 – 1984) and to the Texas Commission of Jail Standards (1975 –1987). He also served on the Temple City Commission (now called the Temple City Council) for four terms from 1978 to 1990.
After he retired from Scott & White in June 1989, he continued to practice and teach at the Olin E. Teague Veteran’s Center in Temple until his death in October 1990. He was 72 years old when he died.
Throughout Dr. Brindley’s distinguished career, he was a highly respected member of the medical community. According to Dr. Robert E. Myers, Past President and Chief Executive Officer
4
of Scott & White Memorial Hospital, “Dr. Brindley was a role model for medical professionals. He was a quiet, unassuming, gentle man who went about getting the job done.”
Dr. Kermit B. Knudsen, Past President of Scott & White Clinic, added that Dr. Brindley, who was the recipient of the Boys Scouts of America’s prestigious Silver Beaver Award for meritorious contributions, “was an individual who epitomized the lofty ideals Boy Scouts memorize and try to live by. He never stopped living by those principles: faithfulness, loyalty, dedication, kindness, and helping people. He always exhibited true humility and he was always content to do his best to help people, never expecting great praise or commendation.” Dr. Brindley is survived by his three sons, Dr. H.H. Brindley, Jr, Dr. George Brindley, and Dr. Glen Brindley; one daughter, Mrs. Don (Nan) Cuba, of San Antonio, nine grandchildren and nine great-grandchildren. He was preceded in death by his wife, Julia, son Paul, and brothers G.V. Brindley, and more recently deceased Clyde Brindley.
Dr. Brindley was part of a long-standing family tradition at Scott & White. His father, the late G.V. Brindley, Sr., M.D. was a pioneer physician and surgeon at Scott & White in the early 1900s. His brother Dr. G.V. Brindley, Jr. was a Scott & White Thoracic and Cardiovascular Surgeon. The Brindley medical legacy continues with Dr. Brindley’s three sons, Dr. H.H. Brind-ley, Jr., Orthopaedic Surgeon; Dr. George Brindley, also an Orthopaedic Surgeon; and Dr. Glen Brindley, an Ophthalmologist.
About the Lectureship . . .
In December of 1989, the Hanes H. Brindley Lectureship was established to honor Dr. Brindley’s contributions to Scott & White and the medical profession. The purpose of this lectureship is to keep physicians abreast of current knowledge, therapies, and research efforts made in Orthopaedic Surgery.
5
Scott J Mubarak, M.D.Emetitus Chief of Rady Children’s Hospital’s Pediatric
Orthopedic Division
Clinical Professor, Department of Orthopaedic Surgery University of California at San Diego
Consultant to the Naval Hospital, San Diego
Past President of the Pediatric Orthopedic Society of North America(POSNA)
Dr. Scott Mubarak is the Emeritus Chief of Rady Children’s Hospital’s Pediatric Orthopedic Division and Clinical Professor Dept. of Orthopedics at UCSD. He is a founding member of
this Pediatric Orthopedic Division and helps oversee a group of 10 pediatric orthopedic surgeons, 4 pediatric orthopedic fellows, 4 pediatric orthopedic residents and 11 nurse practitioners/physi-cian assistants.
He graduated from the University Of Wisconsin School Of Medicine, completed his Orthope-dics training at the University of California, San Diego and his Pediatric Orthopedic Fellowship at the Hospital for Sick Children in Toronto, Canada. Dr. Mubarak is board certified in orthopedics.
Dr. Mubarak is Past President of the Pediatric Orthopedic Society of North America(POSNA). He is also a member of the American Academy of Orthopaedic Surgeons, Scoliosis Research So-ciety, International Pediatric Orthopedic Think Tank, American Orthopedic Association and the European Pediatric Orthopedic Society.
Dr. Mubarak’s clinical interests are: hip dislocation, foot deformities, fractures, clubfeet, mus-cular dystrophy, cerebral palsy and compartment syndromes. He has authored 146 journal articles, 39 book chapters and a textbook entitled “Compartment Syndromes and Volkmann’s Contracture”. Some of his noteworthy publications include: (1) “Pitfalls in the Use of the Pavlik Harness for Treatment of Congenital Dysplasia, Subluxation and Dislocation of the Hip,” (2) “The San Diego Pelvic Osteotomy,” and (3) “Calcaneal, Cuboid and Cuneiform Osteomies for Valgus Foot Defor-mities.”
His honors and award include: The Alpha Omega Alpha (AOA) American Academy of Ortho-pedic Surgeons’ highest award for research on Compartment Syndromes and muscle pressure mea-surement; the Achievement Award in Anatomy, UCSD; and the Walter P. Blount Pioneer Award (POSNA) for Outstanding Clinical Scientific Paper for scientific paper on muscular torticollis.
6
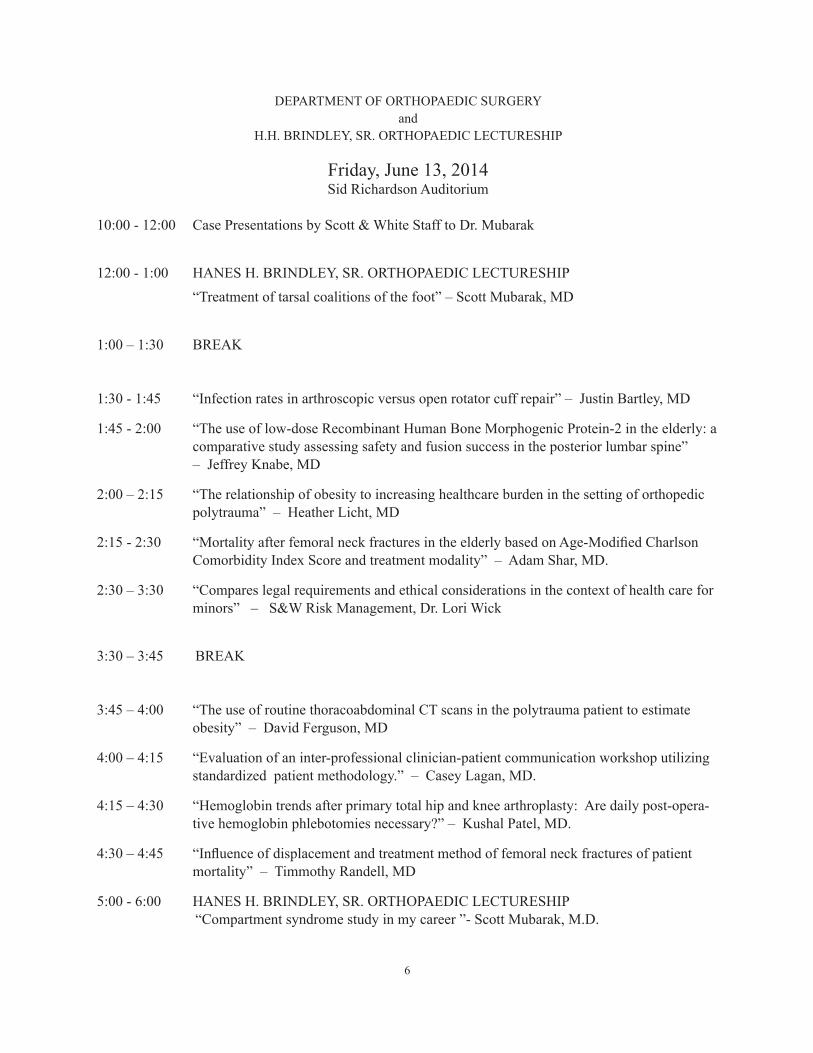
DEPARTMENT OF ORTHOPAEDIC SURGERYand
H.H. BRINDLEY, SR. ORTHOPAEDIC LECTURESHIP
Friday, June 13, 2014Sid Richardson Auditorium
10:00 - 12:00 Case Presentations by Scott & White Staff to Dr. Mubarak
12:00 - 1:00 HANES H. BRINDLEY, SR. ORTHOPAEDIC LECTURESHIP “Treatment of tarsal coalitions of the foot” – Scott Mubarak, MD 1:00 – 1:30 BREAK
1:30 - 1:45 “Infection rates in arthroscopic versus open rotator cuff repair” – Justin Bartley, MD
1:45 - 2:00 “The use of low-dose Recombinant Human Bone Morphogenic Protein-2 in the elderly: a comparative study assessing safety and fusion success in the posterior lumbar spine” – Jeffrey Knabe, MD
2:00 – 2:15 “The relationship of obesity to increasing healthcare burden in the setting of orthopedic polytrauma” – Heather Licht, MD
2:15 - 2:30 “Mortality after femoral neck fractures in the elderly based on Age-Modified Charlson Comorbidity Index Score and treatment modality” – Adam Shar, MD.
2:30 – 3:30 “Compares legal requirements and ethical considerations in the context of health care for minors” – S&W Risk Management, Dr. Lori Wick
3:30 – 3:45 BREAK
3:45 – 4:00 “The use of routine thoracoabdominal CT scans in the polytrauma patient to estimate obesity” – David Ferguson, MD
4:00 – 4:15 “Evaluation of an inter-professional clinician-patient communication workshop utilizing standardized patient methodology.” – Casey Lagan, MD.
4:15 – 4:30 “Hemoglobin trends after primary total hip and knee arthroplasty: Are daily post-opera-tive hemoglobin phlebotomies necessary?” – Kushal Patel, MD.
4:30 – 4:45 “Influence of displacement and treatment method of femoral neck fractures of patient mortality” – Timmothy Randell, MD
5:00 - 6:00 HANES H. BRINDLEY, SR. ORTHOPAEDIC LECTURESHIP “Compartment syndrome study in my career ”- Scott Mubarak, M.D.
7
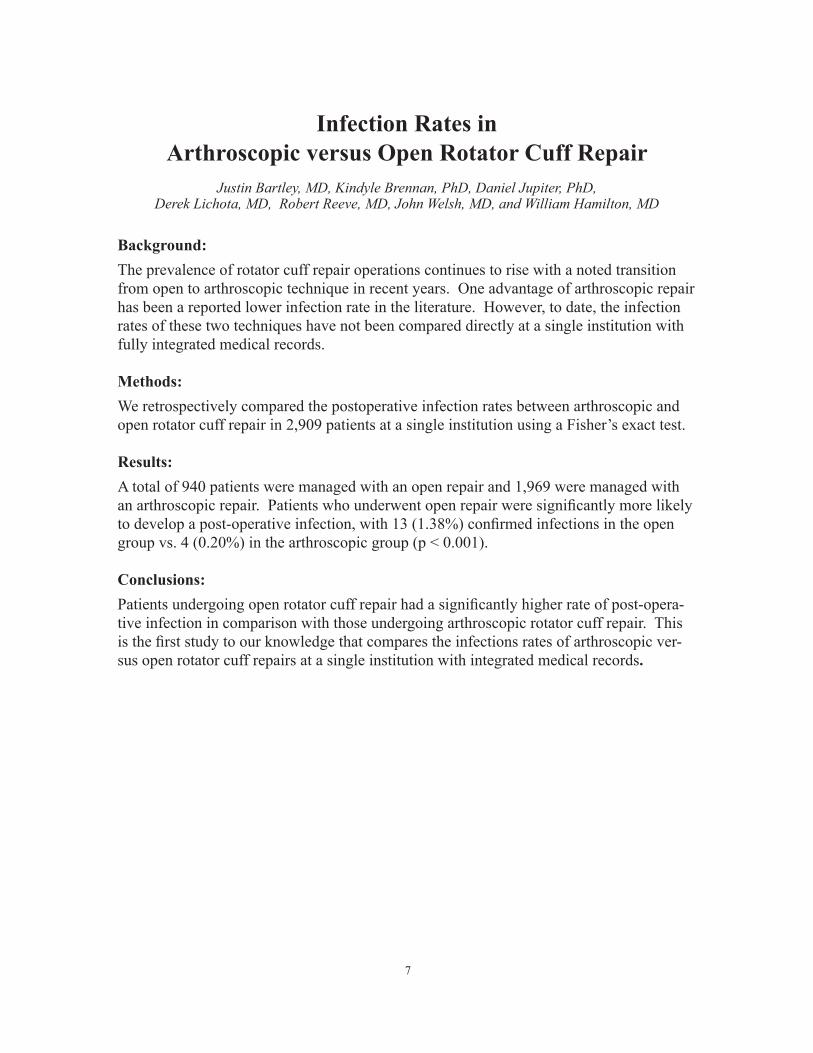
Infection Rates in Arthroscopic versus Open Rotator Cuff Repair
Justin Bartley, MD, Kindyle Brennan, PhD, Daniel Jupiter, PhD, Derek Lichota, MD, Robert Reeve, MD, John Welsh, MD, and William Hamilton, MD
Background: The prevalence of rotator cuff repair operations continues to rise with a noted transition from open to arthroscopic technique in recent years. One advantage of arthroscopic repair has been a reported lower infection rate in the literature. However, to date, the infection rates of these two techniques have not been compared directly at a single institution with fully integrated medical records.
Methods: We retrospectively compared the postoperative infection rates between arthroscopic and open rotator cuff repair in 2,909 patients at a single institution using a Fisher’s exact test.
Results: A total of 940 patients were managed with an open repair and 1,969 were managed with an arthroscopic repair. Patients who underwent open repair were significantly more likely to develop a post-operative infection, with 13 (1.38%) confirmed infections in the open group vs. 4 (0.20%) in the arthroscopic group (p < 0.001).
Conclusions: Patients undergoing open rotator cuff repair had a significantly higher rate of post-opera-tive infection in comparison with those undergoing arthroscopic rotator cuff repair. This is the first study to our knowledge that compares the infections rates of arthroscopic ver-sus open rotator cuff repairs at a single institution with integrated medical records.
8
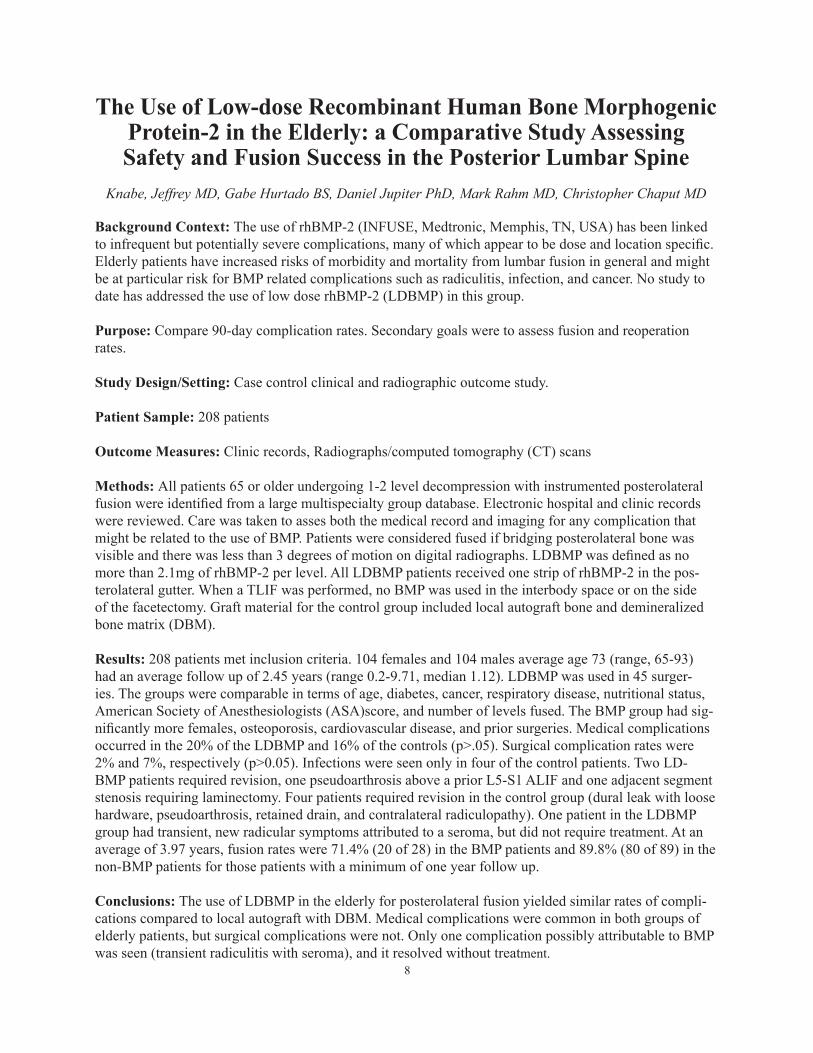
The Use of Low-dose Recombinant Human Bone Morphogenic Protein-2 in the Elderly: a Comparative Study Assessing Safety and Fusion Success in the Posterior Lumbar Spine
Knabe, Jeffrey MD, Gabe Hurtado BS, Daniel Jupiter PhD, Mark Rahm MD, Christopher Chaput MD
Background Context: The use of rhBMP-2 (INFUSE, Medtronic, Memphis, TN, USA) has been linked to infrequent but potentially severe complications, many of which appear to be dose and location specific. Elderly patients have increased risks of morbidity and mortality from lumbar fusion in general and might be at particular risk for BMP related complications such as radiculitis, infection, and cancer. No study to date has addressed the use of low dose rhBMP-2 (LDBMP) in this group.
Purpose: Compare 90-day complication rates. Secondary goals were to assess fusion and reoperation rates.
Study Design/Setting: Case control clinical and radiographic outcome study.
Patient Sample: 208 patients
Outcome Measures: Clinic records, Radiographs/computed tomography (CT) scans
Methods: All patients 65 or older undergoing 1-2 level decompression with instrumented posterolateral fusion were identified from a large multispecialty group database. Electronic hospital and clinic records were reviewed. Care was taken to asses both the medical record and imaging for any complication that might be related to the use of BMP. Patients were considered fused if bridging posterolateral bone was visible and there was less than 3 degrees of motion on digital radiographs. LDBMP was defined as no more than 2.1mg of rhBMP-2 per level. All LDBMP patients received one strip of rhBMP-2 in the pos-terolateral gutter. When a TLIF was performed, no BMP was used in the interbody space or on the side of the facetectomy. Graft material for the control group included local autograft bone and demineralized bone matrix (DBM).
Results: 208 patients met inclusion criteria. 104 females and 104 males average age 73 (range, 65-93) had an average follow up of 2.45 years (range 0.2-9.71, median 1.12). LDBMP was used in 45 surger-ies. The groups were comparable in terms of age, diabetes, cancer, respiratory disease, nutritional status, American Society of Anesthesiologists (ASA)score, and number of levels fused. The BMP group had sig-nificantly more females, osteoporosis, cardiovascular disease, and prior surgeries. Medical complications occurred in the 20% of the LDBMP and 16% of the controls (p>.05). Surgical complication rates were 2% and 7%, respectively (p>0.05). Infections were seen only in four of the control patients. Two LD-BMP patients required revision, one pseudoarthrosis above a prior L5-S1 ALIF and one adjacent segment stenosis requiring laminectomy. Four patients required revision in the control group (dural leak with loose hardware, pseudoarthrosis, retained drain, and contralateral radiculopathy). One patient in the LDBMP group had transient, new radicular symptoms attributed to a seroma, but did not require treatment. At an average of 3.97 years, fusion rates were 71.4% (20 of 28) in the BMP patients and 89.8% (80 of 89) in the non-BMP patients for those patients with a minimum of one year follow up.
Conclusions: The use of LDBMP in the elderly for posterolateral fusion yielded similar rates of compli-cations compared to local autograft with DBM. Medical complications were common in both groups of elderly patients, but surgical complications were not. Only one complication possibly attributable to BMP was seen (transient radiculitis with seroma), and it resolved without treatment.
The realtionship of obsesity 9
Background: With the rise of obesity in the American population, there has been a proportionate increase of obesity in the trauma population. While several stud-ies have suggested an increased rate of complications and costs in the general trauma situation, data specific to obese orthopedic polytrauma patients is limited. The purpose of this study was to use a CT-based mea-surement of adiposity to determine if obesity is associ-ated with an increased burden to the healthcare system in orthopedic polytrauma patients.
Methods: A prospective comprehensive trauma data-base at a Level 1 trauma center was utilized to identify 301 polytrauma patients who had orthopedic injuries and ICU admission from 2006 to 2011. Routine thora-co-abominal CT scans allowed for measurement of the Truncal Adiposity Volume (TAV). Truncal Three-Di-mensional Reconstruction Body Mass Index (TBMI) was calculated from the CT based volumes based on a previously validated algorithm. Patients with a TBMI < 30 were considered nonobese and those patients with a TBMI of 30 or greater were considered obese.
Introduction
In the last two decades, there has been a substantial increase in the prevalence of obesity in the Unit-
ed States. In 2010, more than 78 million US adults (35.7% of the adult population) were obese [1]. Obe-sity is associated with other disease processes such as metabolic syndrome (a constellation of hypertension, dyslipidemia, and diabetes in the setting of obesity), coronary artery disease, congestive heart failure, ob-structive sleep apnea, and degenerative joint disease [2,3,4]. These comorbidities can complicate medical care; and, the economic burden of treating obesity and its associated comorbidities is significant and grow-ing. From 1998 to 2008, the annual medical financial burden of obesity rose to 9.1% of all medical spend-ing, or approximately $147 billion a year [5]. It has
been estimated that medical spending is $1,429 (or 42%) higher per year for an obese patient compared to a patient of normal body mass [5].
With the increasing prevalence of obese patients, there has been a commensurate increase in the number of obese orthopedic trauma patients [6-7]. However, the impact of obesity on the treatment of the polytrau-matized patient is not fully understood. Recent studies have reported conflicting outcomes with regard to as-sociations between obesity and LOS, mortality, com-plications, discharge disposition, and other variables [6-10]. It has been suggested that these conflicting results may be due to the inherent limitations in defin-ing obesity based solely on Body Mass Index (BMI), as BMI may not be as sensitive and specific as desired [11]. BMI is a height to weight proportion calcula-
The Relationship of Obesity to Increasing Healthcare Burden in the setting of Orthopedic Polytrauma
Heather Licht, MD, Mark Murray, BS, John Vassaur, BS, Daniel Jupiter, PhD, Justin Regner, MD, Christopher Chaput, MD
The need for orthopedic surgery, in-hospital mortal-ity, length of stay (LOS), hospital costs, and discharge disposition were compared between the two groups.
Results: Of the 301 patients, 21.6% were classified as obese (TBMI ≥30). Higher TBMI was associated with longer hospital LOS (p = 0.02), more days spent in the Intensive Care Unit (p = 0.03), more frequent discharge to a long-term care facility (p < 0.0002), higher rate of orthopedic surgical intervention (p < 0.01), and increased total hospital costs (p < 0.001).
Conclusions: CT scans, which are routinely obtained at the time of admission, can be utilized to calculate truncal adiposity and investigate the impact of obesity on the polytrauma patients. Obesity is associated with higher total hospital charges, longer hospital stays, discharge to a continued care facility, and a higher rate of surgical orthopedic intervention.
Level of Evidence: Level II prognostic study; a ret-rospective review of a prospective trauma database.

The realtionship of obsesity 10
tion (kg/m2), which in general correlates with excess adiposity. Unfortunately, the BMI does not take into account body-type [11, 12]. For example, patients with high amounts of lean muscle can inaccurately be classified as obese [11, 13]. There are also difficulties with calculating an accurate BMI in the trauma set-ting. Height and weight are often difficult to accurate-ly obtain in severely injured patients, particularly at initial presentation when severe injuries can preclude mobilization. If the height and weight are obtained later, significant weight fluctuations with early fluid resuscitation can occur and can affect the accuracy of BMI calculations [14].
Given these difficulties associated with BMI, there has been recent interest in defining obesity by mea-suring adiposity instead of with traditional BMI. Ferguson et al. used CT scans to quantify obesity in polytrauma patients by assembling three-dimensional reconstructions to measure Truncal Adiposity Volume (TAV). This measurement was then used to calculate a Truncal Three-Dimensional Reconstruction BMI estimate (TBMI) [15]. Ferguson’s study showed high intra-observer and inter-observer correlations in measuring TAV: 0.99 and 0.98, respectively. In ad-dition, statistical analysis supported good correlation between TBMI and traditional BMI (correlation coef-ficient = 0.86, p<0.0001). The results from that study demonstrated the technique to be a simple, reliable, and direct way of calculating adiposity in a trauma pa-tient. The purpose of this study was to use a CT-based measurement of adiposity to determine if obesity is associated with increased total hospital charges, hos-pital LOS, need for orthopedic surgery, and worse dis-charge disposition for orthopedic polytrauma patients.
Materials and Methods
After institutional review board approval was ob-tained, a retrospective radiographic and clinical re-view was conducted. A total of 1,199 patients in a prospective comprehensive American College of Sur-geons (ACS) verified Level 1 trauma database were reviewed from January 2006 through December 2011. Inclusion criteria were 1) 911 trauma registry patients with thoracic/abdominal CT scan, 2) patients 18 years of age or older, and 3) patients with an orthopedic in-jury. Excluded from this study were patients with pen-etrating trauma, paralysis resulting from trauma, or no orthopedic injury. In addition, patients not requiring
admission to the ICU and those without adequate tho-racic/abdominal CT scans were excluded. A total of 301 patients were included in this study.
Routine thoracoabdominal CT scans that were ob-tained on all 911trauma patients upon admission were used to quantify adiposity, according to the method of Ferguson, et al. [15]. Utilizing the multidetector CT images and 3 Dimensional Reconstruction software (OsiriX, version 3.1 32-bit, OsiriX Foundation, Gene-va, Switzerland), a 3D volume rendering of adipose tis-sue from the T10 pedicle to the coccyx was created for each patient. From this 3D rendering, TAV was de-termined and measured in cubic centimeters. The TAV (in cm3) was then divided by the total image length (in mm), yielding the Body Fat Index (BFI) for each patient (Figure 1). BFI was then used to calculate a TBMI for each patient using the equations developed in Ferguson’s study. Next, patients were categorized into two groups based on their TBMI, with classes defined by the World Health Organization [12]: normal patients with TBMI less than 30, and obese patients with TBMI greater than or equal 30.
Figure 1. Truncal 3D reconstruction of adiposity in a nonobese patient obtained from the thoracoabdominal trauma CT scans and 3 Dimensional Reconstruction software which is then used to determine a Three Dimensional Reconstruction BMI estimate (TBMI).
The realtionship of obsesity 11
Age, gender, race, location of injuries, mechanism of injury, index severity score (ISS), and radiographic measurement for all patients were recorded. In addi-tion, the need for an orthopedic surgery, LOS, LOS in the ICU (ICU LOS), number of days requiring venti-lator support, hospital mortality, discharge disposition facility type, and total hospital cost were recorded for each patient.
Demographics, injuries, ISS, and mechanism of in-jury were tested for association with TBMI class us-ing the appropriate test (chi-squared/Fisher’s exact). Data are summarized utilizing simple means and SD or proportions as appropriate. Similar analyses were done with the need for orthopedic surgery, in-hospital mortality, LOS, cost and discharge disposition. Sig-nificance was set at p < 0.05.
Source of Funding
No external funding was received for this study.
Results
Study Population
The study population consisted of 301 patients, 221 (73.42%) males and 80 (26.58%) females. The aver-age age was 34.20 years (SD: 12.22), with a range from 18 to 60 years. Forty (13.29%) patients were African American, 214 (71.10%) Caucasian, 3 (1.00%) Asian, 39 (12.96%) Hispanic, and the remaining 5 (1.66%) were classified as other. Eighty-two (27.24%) pa-tients had documented traumatic brain injury (TBI). The majority of the population (172 patients; 57.14%) was involved in motor vehicle collisions (MVC). The remaining patients were victims of assaults, falls from height, motorcycle collisions (MCC), off-road vehicle accidents, pedestrian accidents, and unclassified (Ta-ble2). Mean ISS was 29.79 (SD: 12.25), with a score range of 4 to 75. Of the recorded injuries, the primary injury location was as follows: 20 (6.64%) were of ab-domen or pelvic contents, 1 (0.33%) head, 14 (4.65%) neck, 29 (9.63%) thorax, 166 (55.15%) lower extrem-ity, and 71 (23.59%) upper extremity. All 301 patients sustained an orthopedic injury, as required by the in-clusion criteria. Of those patients, 143 (47.51%) had an injury to the upper extremity, 142 (47.18%) sus-tained an injury to the lower extremity, 110 (36.54%) had a pelvic injury, and 176 (58.47%) were found to have an injury to the spine. One hundred and seventy-six (58.47%) patients required a surgery for their or-
thopedic injuries.
TBMI Classes
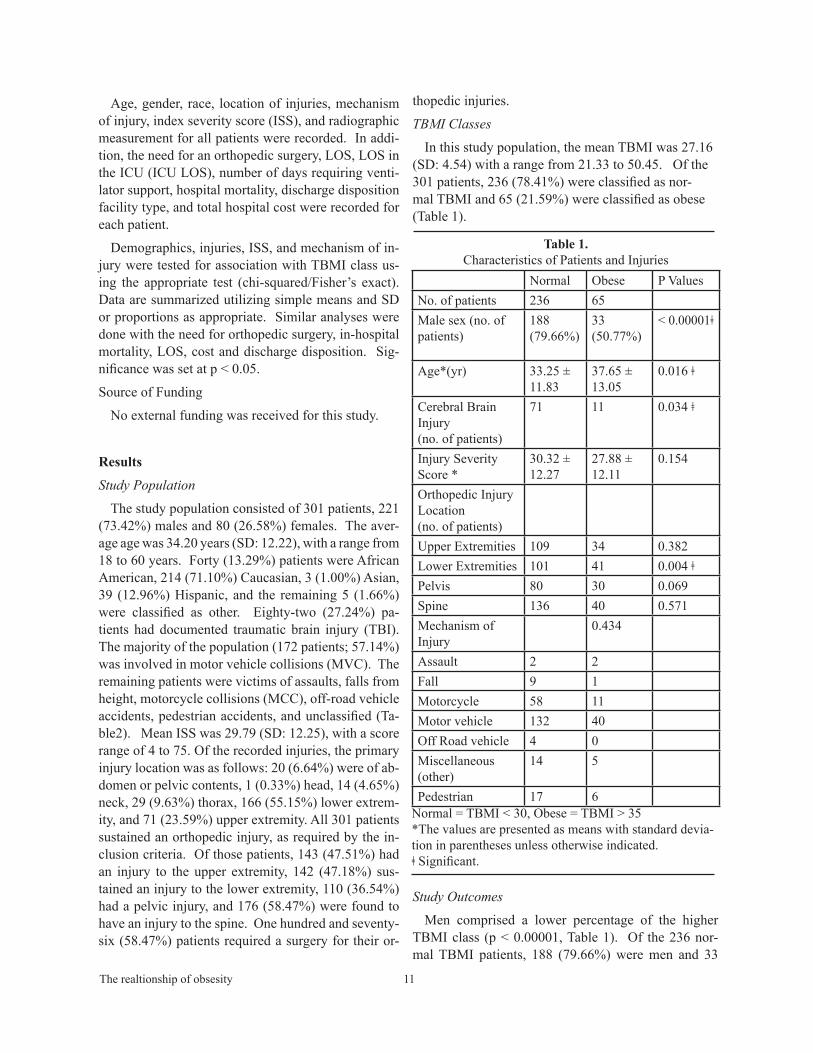
In this study population, the mean TBMI was 27.16 (SD: 4.54) with a range from 21.33 to 50.45. Of the 301 patients, 236 (78.41%) were classified as nor-mal TBMI and 65 (21.59%) were classified as obese (Table 1).
Study Outcomes
Men comprised a lower percentage of the higher TBMI class (p < 0.00001, Table 1). Of the 236 nor-mal TBMI patients, 188 (79.66%) were men and 33
Table 1. Characteristics of Patients and Injuries
Normal Obese P ValuesNo. of patients 236 65Male sex (no. of patients)
188 (79.66%)
33(50.77%)
< 0.00001ǂ
Age*(yr) 33.25 ± 11.83
37.65 ± 13.05
0.016 ǂ
Cerebral Brain Injury (no. of patients)
71 11 0.034 ǂ
Injury Severity Score *
30.32 ± 12.27
27.88 ± 12.11
0.154
Orthopedic Injury Location (no. of patients)Upper Extremities 109 34 0.382Lower Extremities 101 41 0.004 ǂPelvis 80 30 0.069Spine 136 40 0.571Mechanism of Injury
0.434
Assault 2 2Fall 9 1Motorcycle 58 11Motor vehicle 132 40Off Road vehicle 4 0Miscellaneous (other)
14 5
Pedestrian 17 6Normal = TBMI < 30, Obese = TBMI > 35*The values are presented as means with standard devia-tion in parentheses unless otherwise indicated. ǂ Significant.

The realtionship of obsesity 12
of the 65 patient in the obese class (50.77%) were men. A statistically significant association was also found between age and TBMI class (p = 0.016): nor-mal TBMI individuals had a mean age of 33.25 (SD 11.83) and obese individuals had mean age 37.65 (SD 13.05. TBMI class was also found to be statistically significantly associated with cerebral brain injury (p = 0.034) with 30% of the normal TBMI class popula-tion having a traumatic brain injury compared to 17% of the obese class. No statistically significant asso-ciations were found between TBMI class and race, mechanism of injury, or ISS. When isolating ortho-pedic injuries in our population, obesity was associ-ated with lower extremity injuries (p = 0.004) while no association was seen with upper extremity, pelvic, or spinal injuries (Table 1). Rates of orthopedic sur-gery also differed significantly between TBMI classes (p = 0.011). In this population, 129 normal patients (54.66%), and 47 (72.31%) obese patients required orthopedic surgical intervention. Dividing the obese TBMI class up further into those with TMBI between 30 and 35 (Class I) and those with TBMI ≥35 (Class II), it was demonstrated that 33 (66.66%) of the Class I obese patients and 14 (93.33%) of the Class II pa-tients required orthopedic surgery for their injuries (p = 0.006) (Figure 2).
The mean LOS was 13.25 days (SD 11.11) with a range from 1 to 83 days. Mean ICU LOS was 7.77 days (SD 7.98) with a range of 1 to 43 days. Analysis revealed an association between TBMI class and LOS (p = 0.023) and days spent in the ICU (p = 0.033). Normal TBMI patients had mean ICU LOS of 7.24 days and total LOS of 12.39 days compared to the obese patients who had a mean ICU LOS of 9.72 days
and a total LOS of 16.35 days (Table 2). A statistical association was also seen between the TMBI classes and in-hospital mortalities (p = 0.028) with an increase seen in the normal TBMI class (Table 2). Out of the 301 patients, 38 (12.62%) patients died in the hospital, 29 (9.63%) went to a continuing care hospital (CCH), 33 (10.96%) went to a skilled nursing facility (SNF), 109 (36.21%) went to a rehabilitation center, 91 (30.23%) went home, and 1 (0.33%) was transferred to a mili-tary hospital for continued care. A difference was seen between the TBMI classes and discharge disposition (chi-squared p = 0.0002), with more patient from the higher TBMI class requiring discharge to a continuing care facility such as a SNF or CCH (Table 2).
The average cost was $176,629.54 with a range from $3,799 to $819,923.02. A significant association be-tween TBMI class and accrued hospital cost was seen (p < 0.001). Normal TBMI patients had lowest mean cost of $160,606.02 (SD $119,586.18) compared to the obese patients who accrued a mean cost of $234,863.58 (SD $162.863.58).
Figure 2. Percentage of patients requiring orthopedic surgery in relation to TBMI classes.
Table 2. Comparison of outcomes by TBMI Obesity Class
Normal Obese P ValuesHospital LOS* (d) 12.39
(10.51)16.35 (12.65)
0.023 ǂ
ICU LOS* (d) 7.24 ± 7.82 9.72 ± 8.33 0.033 ǂRequired Ventila-tor* (d)
6.57 ± 8.03 8.69 ± 8.96 0.088
In-hospital mortal-ity (no. of patients)
35 3 0.028 ǂ
Orthopedic Surgery (no. of patients)
129 (54.66%)
47 (72.31%)
0.011 ǂ
Mean Cost* ($) 160,606.02 (119,586.18)
234,807.24 (162,863.58)
< 0.001 ǂ
Disposition Location
0.00016 ǂ
CCH 17 (7.2%) 12 (18.46%)SNF 18 (7.63%) 15 (23.08%)Rehab 88 (37.29%) 21 (32.31%)Home 77 (32.62%) 14 (21.54%)Expired 35 (14.83%) 3 (4.62%)Other 1 (0.42) 0 (0%)
Abbreviation: LOS, length of stay; ICU, Intensive Care Unit; CCH, Continued care hospital; SNF, skilled nursing facility; *The values are presented as means with standard deviation in parentheses unless otherwise indicated. ǂ Significant.

The realtionship of obsesity 13
Discussion
Obesity has reached epidemic proportions and is increasingly recognized as a major economic burden to the healthcare system [1,5,16,17]. BMI has tradi-tionally been used to assess obesity in studies that at-tempt to quantify the impact of excess adiposity on the healthcare system, but it can be inaccurate and difficult to obtain in orthopedic polytrauma patients [11,12,14,15]. This is the first study to use a three dimensional CT reconstruction process to explore an association between obesity and an increase in the overall burden to the trauma system. By utilizing CT based reconstructions of adipose volume to estimate obesity, this study uses data already available in most polytrauma patients to provide more direct assess-ments of obesity in this population.
The impact of obesity on injury severity in trauma patients has been examined in several recent studies. Arabi et al. hypothesized that BMI would influence injury patterns sustained in trauma, and their results indicated that overweight individuals gain a certain “cushion effect” from an increase in insulating tissue, resulting in lower ISS than normal and obese individu-als [18]. Our data supports this association between adiposity and ISS, with those patients with a normal TBMI having more severe ISS than those in the obese class. Even though our patients with higher adiposity had lower ISS, they still required significantly more orthopedic intervention and had higher in-hospital charges. One possible reason for this is that obese patients may have different rates of orthopedic inju-ries compared to patients with normal adiposity. For example, several studies have reported that the obese polytrauma patient has an increased risk of pelvic and lower extremity injuries [18-20]. A recent report re-viewing distal femur fractures showed that obese pa-tients had more severe fractures compared to nonobese patients [21]. Our results show a strong association between obesity and lower extremity injuries (Table 1). This may be the reason higher TBMI patients also required orthopedic surgical intervention more often (Table 2). However, no association was seen between TBMI class and upper extremity, pelvic, or spinal in-juries (Table 1).
Significant obesity can make the care of polytrauma patients more challenging for hospital staff and in-crease the risks of complications for trauma patients [4,22,23]. The technical difficulty in performing sur-gery can be greater due to the amount of adipose tissue
and a commensurate need for an increase in the work-ing length of surgical tools [24]. At the same time, pen-etration of fluoroscopy and image quality is decreased, which can preclude or complicate the use of newer, less invasive techniques for internal fixation [25]. Other complications that have been reported to be more com-mon in the obese surgical patient include: DVTs, nerve palsies and compartment syndromes secondary to poor positioning, and increased wound complications [24]. Obese and morbidly obese patients have as much as a 4.7-fold and 6-fold higher risk of infections, respec-tively, when compared to patients with normal BMI [4] and are 4.68 times more likely to require reopera-tion after fixation of pelvic ring injuries [21]. Since the very obese patients in our study had a significantly higher need (93% vs. 55% for nonobese) for orthopedic surgery in the first place, it is likely that the economic impact of truncal obesity on the American healthcare system is magnified in the trauma population.
Recent studies have also explored the association be-tween obesity and ICU LOS, hospital lengths of stay, and in-hospital mortality. Despite the fact that the ma-jority of these studies support an association between obesity and these outcome variables [4,16,17,20,26,27], there are some studies published showing no difference among BMI groups [28,29]. As mentioned previously, the limitations of using BMI to define obesity in the trauma population may contribute to these contradic-tory results. Traditional BMI may mistakenly classify very muscular patients as obese [15]. Despite hav-ing an obese percent body fat on DXA scans, a direct measure of adipose tissue, one study demonstrated that approximately one-half of women these were misclas-sified as non-obese [11]. The method we used to ex-trapolate BMI in this study has been shown to correlate with traditionally calculated BMI. Since it relies on a direct measurement of adiposity, it is not subject to the inaccuracy inherent in a simple height/weight propor-tion when it is applied to heavily muscled patients or patients with large amounts of interstitial fluid volumes from trauma resuscitation [14,15].
Using direct measurements of truncal adiposity nor-malized for truncal height, our study demonstrated a significant association between obesity and an increase in days spent in the ICU, total LOS, and overall hospi-tal costs. Obesity was also associated with increased hospital LOS that alone can cause an increase in hos-pital cost. The patients in the obese class stayed on average 2 days longer in the ICU and 4 days more in

The realtionship of obsesity 14
the hospital than those with a normal TBMI. Obesity is strongly associated with increase in morbidity and complications which also could explain higher accrued hospital cost during a patient’s stay [4, 26,27,29,30]. Obesity was also strongly associated with the need for orthopedic surgical intervention in our population. Over 93% of the patients in class II obesity required surgery for their orthopedic injuries, compared to only 55% of patients with normal TBMI. The additional charges from orthopedic surgical intervention increas-es the overall hospital cost in these patients, and this in combination with the longer LOS appear to be the main contributors to the significant differences in hos-pital charges seen in the obese patients.
Obesity has also been demonstrated to predict poorer discharge disposition of patients compared to those with normal weight [27,31,32]. There was an association seen between TBMI class and discharge dispositions (p = 0.0002) with a trend for patients in higher TBMI class requiring discharge to facilities specializing in continued high level of medical care such as a continuing care hospital or a skilled nursing facility. The obese patients were more likely to be discharged to skilled nursing facilities and less likely to be discharged home when compared to individu-als in the normal TBMI class. At least one study demonstrated that once at an inpatient rehabilitation center, obese patients do not have as much functional improvement as nonobese patients. Further, they have lower functional independence measurements despite having no difference in therapy participation fre-quency, therapy duration, or LOS in the rehabilitation setting [33]. While it was beyond the scope of this study to assess costs associated with obesity in the post-acute care setting, any increase in the need for further skilled care will certainly increase the costs associated with the care of the obese trauma patient.
There is strong support in the literature demonstrat-ing an association between obesity and increases in morbidity [6, 8,18,20,27,29,30,31]. Despite this, an association between obesity and higher mortality rates has not always been reported [8,27,30]. Our findings coincide with several other studies, revealing an asso-ciation between obesity and mortality (p = 0.028). It is worth noting that a higher percentage of patients in the normal TBMI class expired in the hospital. Sev-eral studies support the concept of a “cushion effect” of increased adiposity possibly leading to a protec-tive physical shield in obese patients, with evidence
of fewer head injuries and intra-abdominal injuries [18,19]. However, caution should be used when try-ing to generalize our results because of the relatively small number of obese patients in our study.
Other limitations of our study include the inability to establish causal relationships, which is inherent to any retrospective analysis. Additionally, at our institution, no standardized protocols were in place for the management for these patients; and, their treat-ment regimen was carried out per the discretion of the treating surgeon and ICU physician. The absence of underweight patients and the small number of mor-bidly obese patients may have influenced our results. This study examined the final cost of each patient’s hospital care and did not take into consideration the influences of comorbidities or complications that may affect outcomes. Although we have found associa-tions between obesity and hospital LOS, orthopedic surgery rates, hospital costs, and discharge disposi-tions, we can only hypothesize about the reason(s) for these findings. This is the first study of its kind to utilize a three-dimensional CT reconstruction process to more directly quantify adiposity in trauma patients, which may help strengthen the validity of our conclu-sions when compared to indirect methods of quantify-ing obesity.
In conclusion, the increasing prevalence in obe-sity has been shown to be a financial burden on the healthcare system in general [5,16,17]. Our study demonstrated an association between obesity and increased rates of orthopedic surgery, higher total hos-pital charges, longer ICU and total hospital stay, and decreased rate of discharge to home in the orthopedic polytrauma population. Importantly, this increase in resource utilization occurred even though our patients with higher adiposity had a trend towards lower injury severity scores. These factors should be taken into consideration when determining resource allocation and re-imbursement for care. In addition, sophisti-cated and standardized measurement techniques like direct CT based measurements of adiposity obtained at the time of admission have the potential to help more appropriately define the impact that obesity has on the orthopedic polytrauma patient.
REFERENCES:1. Ogden CL, Carroll MD, Kit BK, Flegal KM. Preva-
lence of obesity in the United States, 2009–2010. NCHS data brief, no 82. Hyattsville, MD: National

The realtionship of obsesity 15
Center for Health Statistics. 2012. Available at: http://www.cdc.gov/nchs/data/databriefs/db82.pdf Accessed September 22, 2013
. Bachman KH: Obesity, weight management, and health care costs: a primer. Dis Manag 2007;10(3):129-37.
T3. National Institutes of Health. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults—The evidence report. Obes Res 6(Suppl 2):51S–209S.
4. Serrano PE, Khuder SA, Fath JJ. Obesity as a risk factor for nosocomial infections in trauma patients. J Am Coll Surg. 2010 Jul;211(1):61-7.
5. Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Aff 2009;28(5):w822-31.
6. Nelson J, Billeter AT, Seifert B, Neuhaus V, Trentz O, Hofer CK, Turina M. Obese trauma patients are at increased risk of early hypovolemic shock: a ret-rospective cohort analysis of 1,084 severly injured patients. Crit Care. 2012 May 8;16(3):R77.
7. Alselaim N, Malaekah H, Saade M, Hussein M, Altokhais T, Albedah K, Zamakhshary M. Does obesity impact the pattern and outcome of trauma in children? J Pediatr Surg. 2012 Jul;47(7):1404-9.
8. Maheshwari R, Mack CD, Kaufman RP, Francis DO, Bulger EM, Nork SE, Henley MB. Severity of injury and outcomes among obese trauma patients with fractures of the femur and tibia: a crash injury research and engineering network study. J Orthop Trauma. 2009 Oct;23(9):634-9.
9. Shashaty MG, Meyer NJ, Localio AR, Gallop R, Bellamy SL, Holena DN, Lanken PN, Kaplan S, Yarar D, Kawut SM, Feldman HI, Christie JD. African American race, obesity, and blood product transfusion are risk factors for acute kidney injury in critically ill trauma patients. J Crit Care. 2012 Oct; 27(5):496-504.
10. Evans DC, Stawicki SP, Davido HT, Eiferman D. Obesity in trauma patients: correlations of body mass index with outcomes, injury patterns, and complications. Am Surg. 2011 Aug;77(8):1003-8.
11. Romero-Corral A, Somers VK, Sierra-Johnson J, Thomas RJ, Collazo-Clavell ML, Korinek J, Allison TG, Batsis JA, Sert-Kuniyoshi FH, Lopez-Jimenez F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int J Obes (Lond). 2008 Jun; 32(6):959-66.
12. World Health Organization. BMI Classification. Adapted from WHO, 1995, WHO, 2000, and WHO, 2004. Available at: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html. Accessed September 22, 2013
13. Shah NR, Braverman ER. Measuring adiposity in patients: the utility of body mass index (BMI), Percent Body Fat, and Leptin, PLoS One. 2012;7(4):e33308.
14. Du GB, Slater H, Goldfarb IW. Influence of dif-ferent resuscitation regimens on acute early weight gain in extensively burned patients. Burns. 1991 Apr;17(2):147-50.
15. Ferguson DF, Busenlehner BJ, Rahm MD, Mehta SM, Song J, Davis ML, Sampson WH, Chaput CD. The use of routine thoracoabdominal ct scans in the polytrauma patient to estimate obesity. Obesity (Sil-ver Spring). 2012 Jun 18. doi: 10.1038/oby.2012.163.
16. Russell GV, Pierce CW, Nunley L. Financial Im-plications of Obesity. Orthop Clin North Am. 2011 Jan;42(1):123-7.
17. Baldwin KD, Matuszewski PE, Namdari S, Esterhai JL, Mehta S. Does morbid obesity negatively affect the hospital course of patients undergoing treatment of closed, lower-extremity diaphyseal long-bone frac-tures? Orthopedics. 2011 Jan 3;34(1):18.
18. Arbabi S, Wahl WL, Hemmila MR, Kohoyda-Inglis C, Taheri PA, Wang SC. The cushion effect. J Trauma. 2003 Jun;54(6):1090-3.
19. Boulanger BR, Milzman D, Mitchell K, Rodriguez A. Body habitus as a predictor of injury pattern after blunt trauma. J Trauma. 1992 Aug;33(2):228-32.
20. Brown CV, Neville AL, Rhee P, Salim A, Velmahos GC, Demetriades D. The impact of obesity on the outcomes of 1,153 critically injured blunt trauma pa-tients. J Trauma. 2005 Nov;59(5):1048-51; discussion 1051.
21. Sems SA, Johnson M, et al. Elevated body mass index increases early complications of surgi-cal treatment of pelvic ring injuries. J Orthop Trauma. 2010 May;24(5):309-14. doi: 10.1097/BOT.0b013e3181caa21e.
22. Porter SE, Graves ML, Qin Z, Russell GV. Opera-tive experience of pelvic fractures in the obese. Obes Surg. 2008 Jun;18(6):702-8.
23. Karunakar MA, Shah SN, Jerabek S. Body mass index as a predictor of complications after operative treatment of acetabular fractures. J Bone Joint Surg Am. 2005 Jul;87(7):1498-502.
24. Jupiter JB, Ring D, Rosen H. The complications and

The realtionship of obsesity 16
difficulties of management of nonunion in the severe-ly obese. J Orthop Trauma. 1995;9(5):363-70.
25. Tucker MC, Schwappach JR, Leighton RK, Coupe K, Ricci WM. Results of femoral intramedullary nailing in patients who are obese versus those who are not obese: a prospective multicenter comparison study. J Orthop Trauma. 2007 Sep;21(8):523-9.
26. Newell MA, Bard MR, Goettler CE, Toschlog EA, Schenarts PJ, Sagraves SG, Holbert D, Pories WJ, Rotondo MF. Body mass index and outcomes in critically injured blunt trauma patients: weighing the impact. J Am Coll Surg. 2007 May;204(5):1056-61; discussion 1062-4.
27. Ciesla DJ,Moore EE, Johnson JL, Burch JM, Cothren CC, Sauaia A. . Obesity increases risk of organ failure after severe trauma. J Am Coll Surg 2006;203:539–45.
28. Batsis JA, Naessens JM, Keegan MT, Wagie AE, Huddleston PM, Huddleston JM. Impact of body mass on hospital resource use in total hip arthroplas-ty. Public Health Nutr. 2009 Aug;12(8):1122-32.
29. Neville AL, Brown CV,Weng J, Demetriades d, Velmahos GC. Obesity is an independent risk factor of mortality in severely injured blunt trauma patients. Arch Surg. 2004 Sep;139(9):983-7.
30. Winfield RD, Delano MJ, Cuenca AG, Cendan JC, Lottenberg L, Efron PA, Maier RV, Remick DG, Moldawer LL, Cuschieri J. Obese patients show a depressed cytokine profile following severe blunt injury. Shock. 2012 Mar;37(3):253-6.
31. Valiyeva E, Russell LB, Miller JE, Safford MM. Lifestyle-related risk factors and risk of future nurs-ing home admission. Arch Intern Med. 2006 May 8;166: 985-90.
32. Legner VJ, Doerner D, Reilly DF, McCormick WC. Risk factors for nursing home placement following major nonemergent surgery. Am J Med. 2004 Jul 15;117(2):82-6.
33. Vincent HK, Seay AN, Vincent KR, Atchison JW, Sadasivan K. Effects of obesity on rehabilitation outcomes after orthopedic trauma. Am J Phys Med Rehabil. 2012 Dec;91(12):1051-9.
Femoral Neck Fractures Based on Age-modified CCI 17
Mortality after Femoral Neck Fractures in the Elderly Based on Age-Modified Charlson Comorbidity Index Score
and Treatment ModalityAdam Shar, Timothy Randell, Michael L Brennan, Kindyle L. Brennan,
Daniel C Jupiter, and Zachary T Hubert.
Objectives: (1) Determine if Age-Modified Charlson Comorbidity Index (ACCI) and surgical modality impact mortality after a femoral neck fracture; and (2) determine if there is a cutoff ACCI at which the risk for mortality increases substantially.
Design: Retrospective cohort study.
Setting: Single Level 1 Trauma institution from 1998-2009.
Patients/Participants: 1,440 patients aged ≥60 with 1,525 femoral neck fractures secondary to low energy trauma. Exclusion criteria consisted of extracapsular fractures, history of surgery to proximal femur, pathologic fractures, and need for open reduction.
Intervention: Closed reduction percutaneous pinning (CRPP), hemiarthroplasty (HA), or total hip arthroplasty (THA).
Main Outcome Measurements: We divided ACCIs into severity groups (low=2-4, medium=5-6, high ≥7) and cal-culated 1-month, 6-month, 1-year, and 2-year mortality, with and without adjusting for treatment modality. Results were compared using Cox regression. We utilized Kaplan-Meier estimates to determine ACCI above which hazard ratio for death increases significantly.
Results: Increase in ACCI of 1 point increased hazard ratio for death by a factor of 1.35. There is a statistically sig-nificant increase in mortality rates between low, medium, and high ACCI groups at measured post-operative periods, even after adjusting for surgery type. High ACCI group exhibited highest mortality (60% for CRPP & 58% HA at 2 years). At ACCI ≥11, hazard ratio for death increased 5 fold, but only 6 cases (0.4%) met this criterion.
Conclusions: Increasing ACCI was associated with increased mortality, and this association remained significant even after adjusting for treatment modality. Statistically significant differences in 1-and 2-year mortality existed between ACCI groups.
Introduction
Femoral neck fractures contribute to significant morbidity and mortality in the elderly population
throughout the United States and the world, with overall estimated 1-year mortality ranging from 15-30%.1-7 Its incidence in the US is reported to be around 350,000 per year, and given the aging population, this is predicted to increase substantially.6,8 Furthermore, femoral neck frac-tures place an increasing financial burden on the health-care system. According to Braithwaite et al.,6 $20 billion dollars were spent for hip fracture care in 1997 alone, and this may increase to $62 billion by 2040. Brauer et al. also reported a significant increase in comorbidities in patients being treated for femoral neck fractures from 1986-1988 and 2003-2005.7
Most femoral neck fractures are treated operatively, with surgical options consisting of closed reduction with percutaneous pinning (CRPP), hemiarthroplasty (HA), or total hip arthroplasty (THA). When deciding upon treat-
ment modality, factors including fracture displacement, age, health and functional status, and bone quality all con-tribute to a surgeon’s decision making. Generally speak-ing, CRPP is preferred for patients with a non-displaced or valgus-impacted fracture, in less functional patients, or those with higher risk of intraoperative complications from anesthesia; whereas, HA or THA are reserved for patients who have suffered from displaced fractures and/or have higher functional or better health status.9-11 How-ever, the choice of optimal surgical treatment remains controversial.11-12
Based on previous research performed at our institu-tion using retrospective data from a large scale database, overall 1-month, 6-month, 1-year, and 2-year mortality rates after femoral neck fracture are estimated to be 6.4%, 16%, 21.5%, and 31.4%, respectively. Median survival time post-operatively was found to be 4.02 years. Among the treatment methods, patients receiving THA demon-

Femoral Neck Fractures Based on Age-modified CCI 18
strated the lowest mortality as compared to those treated with CRPP and HA. Patients who underwent HA had the highest mortality rate with a hazard ratio of 1.22 versus CRPP and 2.19 versus THA, on Cox regression analysis, with both differences reaching statistical significance.
Since a majority of the patients who suffer from femoral neck fractures are elderly, defined by the Unit-ed Nations as people aged 60 years and older,13 it is im-portant to consider their comorbidities when deciding upon a treatment modality. To account for this in our analyses, we used the Age-Modified Charlson Comor-bidity Index (ACCI), a scoring system that measures patient comorbidity status based on age as well as the number and severity of pre-existing diseases. The orig-inal Charlson Comorbidity Index (CCI) is the system most widely used by researchers and clinicians for as-sessing severity of patients’ comorbidities.14,15 In addi-tion to the contents of the original CCI scoring system, ACCI factors age into the scoring system by awarding one point for each decade beyond 40-49 years of age. The ACCI scoring system was validated in a study by Charlson et al.,16 where the goal was to estimate rela-tive risk of death from potentially prognostic clinical covariates. In another study, pre-operative comorbidi-ties were shown to be stronger predictors of post-op-erative complications and mortality as compared to intraoperative complications.17 According to Eiskjer et al.,1 medical conditions at the time of surgery were the most important determinants of survival in patients who underwent bipolar hemiarthroplasty for the treat-ment of a femoral neck fracture. Furthermore, studies have shown that CCI is a reliable marker for predicting mortality in elderly patients with hip fractures.18-19
Although these studies incorporate comorbidity, they do not differentiate between the types of surgical intervention. The purposes of this study were to (1) determine if ACCI and surgical modality indepen-dently impact mortality when analyzed in combina-tion using multivariate regression; and (2) determine if there a cutoff ACCI at which the risk for mortality increases substantially.
PATIENTS AND METHODSResearch Design
This study was approved by our institutional review board. The medical record database at a large level one trauma hospital was queried for diagnosis and treatment codes associated with femoral neck fracture in the years 1998-2009. The codes used were ICD-9 820, and CPT 27235, 27236, and 27132. The exclusion criteria were: age less than 60 years, fracture secondary to high energy trauma, fracture secondary to neoplasia, extracapsular
hip fracture, prior unrelated surgery to the proximal fem-oral region, need for open reduction, or treatment other than CRPP, HA, or THA.
Data collected from the chart review included medical record number (MRN), age at time of surgery/date-of-birth, gender, surgery performed (including date of sur-gery), classification of femoral neck fracture, laterality of fracture, and dates of the last contact or death note. We identified current comorbidities of each patient at the time of surgery and calculated the ACCI (Table 1). Surger-ies performed were further classified as primary/revision. Revision surgery was any reoperation following the in-dex procedure on the affected hip that met inclusion cri-teria. Only index surgeries were examined in this study. Patients’ death records were obtained from Texas Vital Statistics based on name, date of birth, and sex. All radio-graphs and reports were reviewed by the same investiga-
Table 1.Charlson Comorbidity Index Scoring System14, 16
Score Condition1 Myocardial infarction (history) Congestive heart failure Peripheral vascular disease (includes aortic aneurysm
≥6cm) Cerebrovascular disease: CVA with mild or no residua
or TIA Dementia Chronic pulmonary disease Connective tissue disease Peptic ulcer disease Mild liver disease (without portal hypertension; ex-
cludes chronic hepatitis) Diabetes without end-organ damage (excludes diet-
controlled diabetes)2 Hemiplegia Moderate or severe renal disease Diabetes with end-organ damage (retinopathy,
neuropathy, nephropathy, brittle diabetes) Tumor without metastases (exclude if >5 years from
diagnosis) Leukemia (acute or chronic) Lymphoma3 Moderate or severe liver disease6 Metastaticsolidtumor AIDS (not just HIV positive)
For each decade >40 years of age, a score of 1 is added to the above score toobtaintheAge-ModifiedCharlsonComorbidityIndexscoreTable1.Age-ModifiedCharlsonComorbidityIndexscore.14 Reprinted by J Chronic Disease. 40, Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal stud-ies: development and validation. 373-383., © (1987) with permission from Elsevier.16 Reprinted by J Clinic Epidemiol. 47(11), Charlson ME, Szatrowski TP, Person J, Gold J. Validation of a combined comorbidity index. 1245-51., © (1994) with permission from Elsevier.
Femoral Neck Fractures Based on Age-modified CCI 19
tor (TR). Picture Archiving and Communication System (PACS; Siemens AG, Erlangen, Germany), operative re-port, and radiological report were used for review of all patient films.
Surgery was performed or overseen by 1 of 20 senior staff physicians. The patients who were treated with multiple screws had reduction achieved through closed means on a fracture table, and implant placement as de-scribed by Probe et al.20 ASNIS III (Stryker, Kalamazoo, MI, USA) 6.5mm cannulated screws were used on all patients with the decision to place 3 or 4 screws based on surgeon preference. In the vast majority of hemiar-throplasty cases, a modified Hardinge lateral approach combined with a cemented modular stem was utilized. Total hip arthroplasty was also largely performed with a modified Hardinge lateral approach, with a variety of prosthetic components from different manufactures.
Statistical AnalysisDemographic and injury data as well as data describing
surgery types were summarized using means and stan-dard deviations or percentages, as appropriate. To gain an overall understanding of our population’s mortality and the impact of ACCI and surgical method, Kaplan-Meier estimates and Cox proportional hazards regression were used to examine (a) overall mortality after index surgery, (b) mortality rates as impacted by surgery type, (c) mor-tality rates as affected by ACCI, and (d) mortality as im-pacted by ACCI and surgery type independently (the last assessed in a multivariate model).
To determine if there is a cutoff ACCI at which mortal-ity increases precipitously, we dichotomized ACCI into high and low. We varied the cutoff point for dichotomi-zation between the first quartile and third quartile of ob-served scores. For each cutoff, we built a Kaplan-Meier estimator including age, gender, surgery type, displace-ment and dichotomous ACCI. The hazard ratio of mor-tality in high versus low was assessed using Cox regres-sion, and was plotted against the cutoff point, in order to visually assess appearance of any trend. To test whether these models were reliable, they were examined as fol-lows: First, a concordance index was computed for each (a Kaplan-Meier analog of the ROC). This assesses the accuracy of predictions of mortality. Second, the Akaike Information Criterion (AIC) was used to rank the models in terms of goodness of fit. Thus, we can judge whether our suggested cutoff is a reasonable model for survival.
In a post-hoc exploratory analysis, we built models where we looked within a given range of ACCI (low, medium, or high, as defined by our authors using the ra-tionale explained in the discussion portion of this manu-script), and we measured mortality at 1 month, 6 months, 1 year, and 2 years after surgery, with and without taking
surgery type into account. Tests were considered signifi-cant at α≤0.05 in all cases.
RESULTSDemographics
Using the inclusion/exclusion criteria and ICD-9 and CPT codes mentioned above, we identified 1,449 patients with 1,534 femoral neck fractures for which we had Gar-den Type classification. Of the fractures, 383 (24.97%) were in males, and 1,151 (75.03%) were in females. Of the total patients, 365 (25.19%) were male and 1,084 (74.81%) were female. Age of subjects was relatively normally dis-tributed with a mean of 80.84 (8.22) years. ACCI data was missing for 9 patients. For the rest, the mean ACCI was 5.05 (1.66). ACCI differed by gender, as males had a mean ACCI of 5.42 (1.91) and females had a mean ACCI of 4.93 (1.56), (p<0.001). After excluding patients with missing ACCI data, there were 1,440 patients with 1,525 fractures. The surgical methods employed in repair were 741, 744, and 40 for CRPP, HA, and THA groups, respectively.
Overall MortalityA Kaplan-Meier model of survival after surgery indicat-
ed that median survival time post-operatively was 1,468 days (95% CI 1,334-1,612 days). One month, 6- month, 1-year and 2-year mortality rates were estimated to be 6.2% (95% CI 5.0-7.4%), 16.0% (14.2-17.9%), 21.5% (19.4-23.6%), and 31.4% (28.9-33.8%), respectively.
Mortality Based on ACCI Cox proportional hazards model revealed that mortal-
ity did differ significantly by ACCI (p<0.001), as each in-crease of one in ACCI increased the hazard ratio for death by a factor of 1.35 (95% CI 1.30-1.40). There were also statistically significant differences (p<0.012, ANOVA) in the ACCI of patients who underwent different surgical intervention. The mean ACCI of patients who underwent CRPP was 4.98 (SD 1.75), which is slightly less than those who underwent HA (5.16, SD 1.56), but greater than those who underwent THA (4.25, SD 1.82) (see Figure 1).
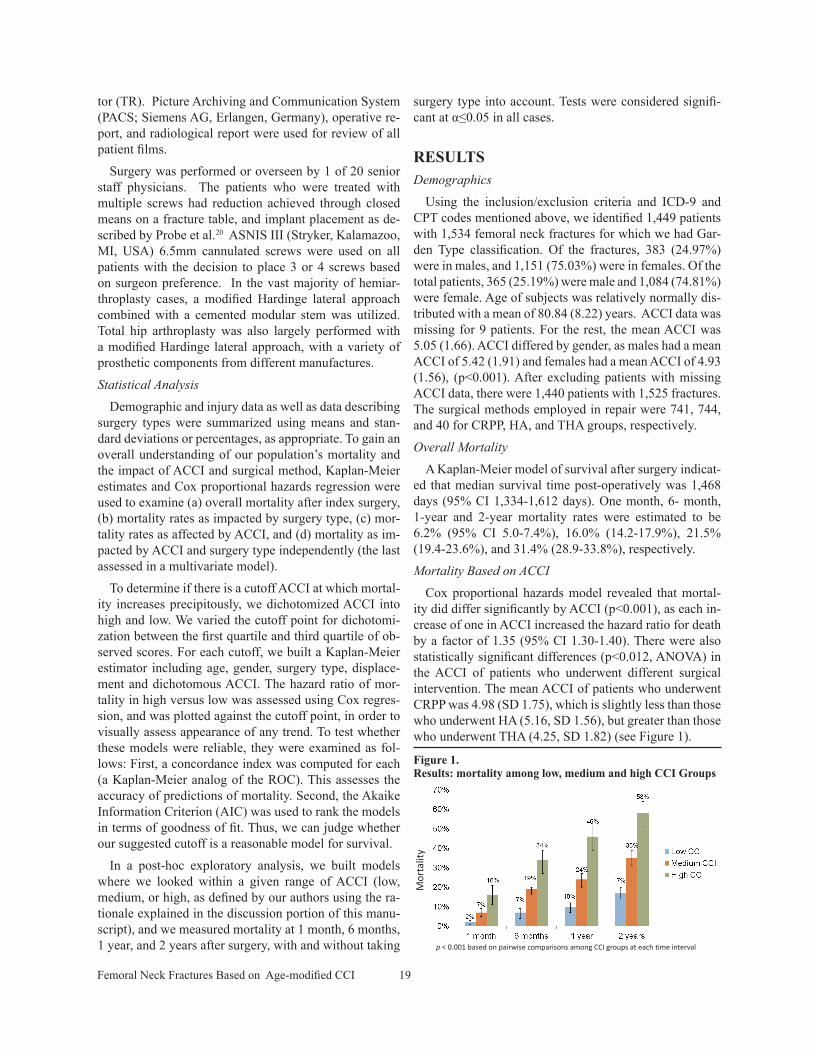
Figure 1. Results: mortality among low, medium and high CCI Groups
p < 0.001 based on pairwise comparisons among CCI groups at each time interval
Mor
talit
y
p < 0.001 based on pairwise comparisons among CCI groups at each time interval
Mor
talit
y
Femoral Neck Fractures Based on Age-modified CCI 20
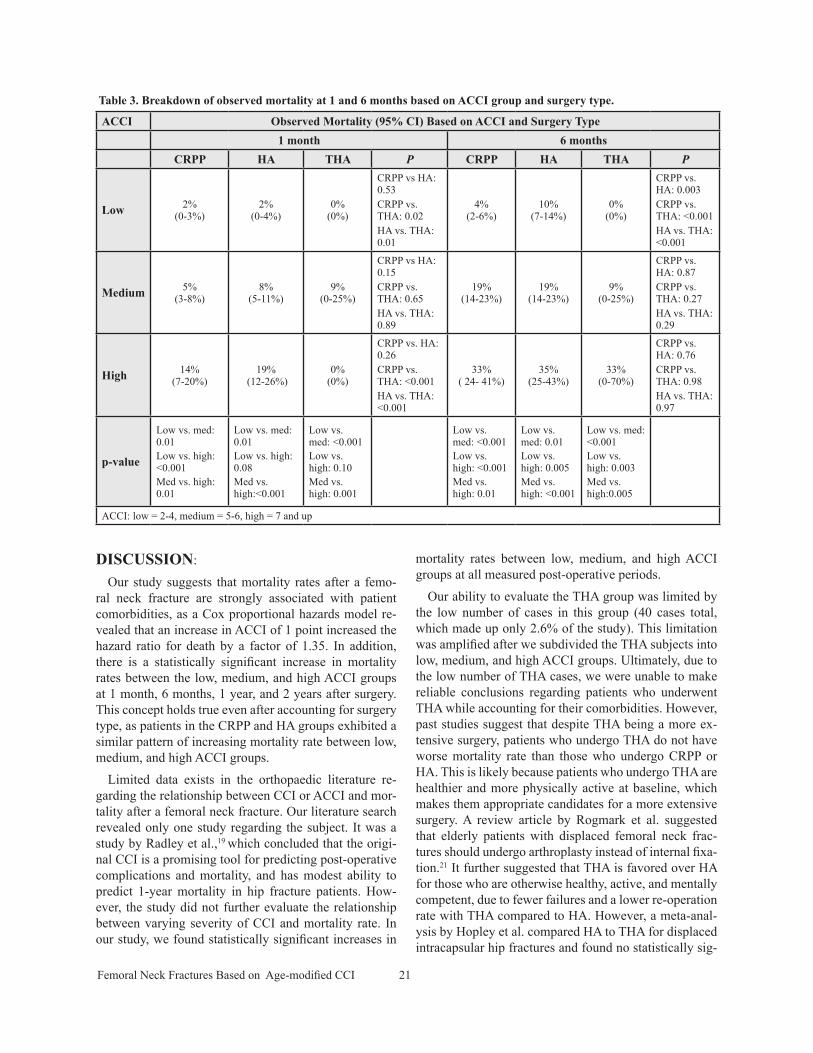
In a post-hoc exploratory analysis, we categorized the study population into 3 groups based on severity of Age-Modified CCI scores (low = 2-4, medium = 5-6, high = 7 or greater). Table 2 shows the breakdown of treatment modality based on the 3 ACCI groups.
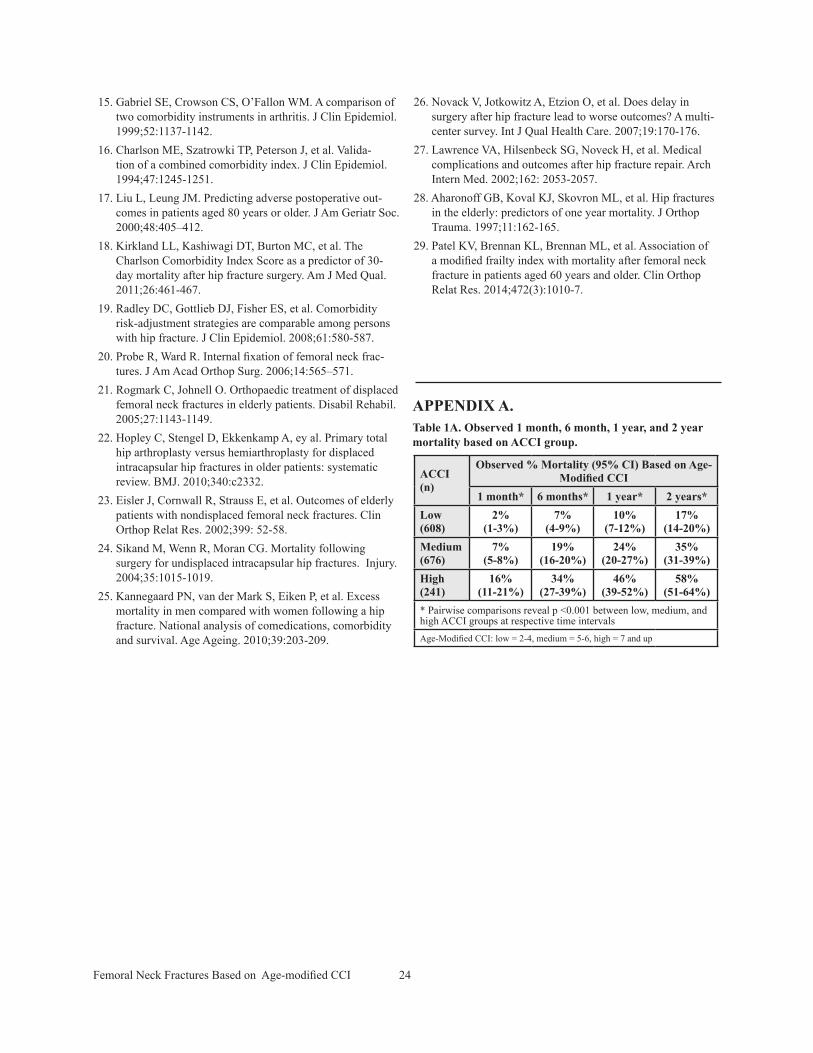
There is a statistically significant increase in observed mortality as ACCI increases from low to medium to high. This difference is observed at 1 month, 6 months, 1 year, and 2 years (Table 1A; see appendix for correspond-ing table). Using the aforementioned ACCI ranges, the 1- month mortality was 2%, 7%, and 16%, in low, me-dium and high ACCI groups, respectively (p<0.001). At 6 months, mortality was 7%, 19%, and 34%, respectively (p <0.001). At 1 year, it was 10%, 24%, and 46%, respec-tively (p <0.001). At 2 years, mortality was 17%, 35%, and 58%, respectively (p <0.001).
Mortality Based on Treatment Modality The median survival time post-operatively based on
Cox proportional hazards model was 1,537 days for CRPP (95% CI 1406-1829), 1,298 days for HA (95% CI 1110-1494), and 2,293 days for THA (95% CI 1888-NA), and the differences were statistically significant (p <0.001). Table 3 shows observed mortality at various post-operative periods based on treatment modality. Pair-wise comparisons show statistically significant differ-ences (p<0.05) in mortality between the 3 treatment mo-dalities at both 1- and 2-year post-operative periods. The HA group had the highest mortality, followed by CRPP and THA.
Mortality Based on ACCI and Treatment ModalityBased on multivariate Kaplan-Meier analysis/Cox re-
gression, the overall mortality of those who underwent THA differed from the overall mortality of those who underwent CRPP, with hazard ratio for death in THA vs.
CRPP of 0.56 (95% CI 0.33-0.96, p = 0.035). The mortal-ity of those who underwent HA differed from the mortal-ity of those who underwent CRPP (p = 0.017), and the hazard ratio for death of HA vs. CRPP was 1.18 (95% CI 1.03-1.35). The mortality of those who underwent HA differed from the mortality of those who underwent THA (p = 0.007). The hazard ratio for HA vs. THA was 2.09 (95% CI 1.23-3.56).
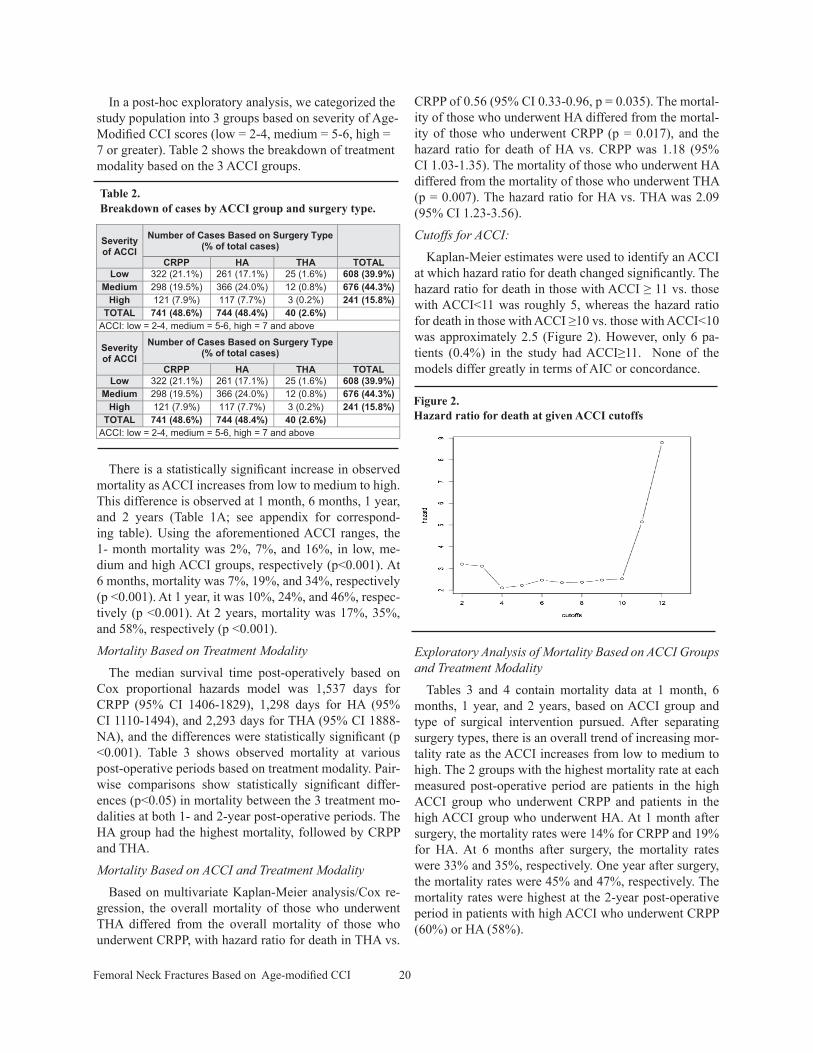
Cutoffs for ACCI:Kaplan-Meier estimates were used to identify an ACCI
at which hazard ratio for death changed significantly. The hazard ratio for death in those with ACCI ≥ 11 vs. those with ACCI<11 was roughly 5, whereas the hazard ratio for death in those with ACCI ≥10 vs. those with ACCI<10 was approximately 2.5 (Figure 2). However, only 6 pa-tients (0.4%) in the study had ACCI≥11. None of the models differ greatly in terms of AIC or concordance.
Exploratory Analysis of Mortality Based on ACCI Groups and Treatment Modality
Tables 3 and 4 contain mortality data at 1 month, 6 months, 1 year, and 2 years, based on ACCI group and type of surgical intervention pursued. After separating surgery types, there is an overall trend of increasing mor-tality rate as the ACCI increases from low to medium to high. The 2 groups with the highest mortality rate at each measured post-operative period are patients in the high ACCI group who underwent CRPP and patients in the high ACCI group who underwent HA. At 1 month after surgery, the mortality rates were 14% for CRPP and 19% for HA. At 6 months after surgery, the mortality rates were 33% and 35%, respectively. One year after surgery, the mortality rates were 45% and 47%, respectively. The mortality rates were highest at the 2-year post-operative period in patients with high ACCI who underwent CRPP (60%) or HA (58%).
Table 2. Breakdown of cases by ACCI group and surgery type.
Severityof ACCI
Number of Cases Based on Surgery Type (% of total cases)
CRPP HA THA TOTALLow 322 (21.1%) 261(17.1%) 25(1.6%) 608 (39.9%)
Medium 298 (19.5%) 366(24.0%) 12 (0.8%) 676 (44.3%)High 121 (7.9%) 117 (7.7%) 3 (0.2%) 241 (15.8%)
TOTAL 741 (48.6%) 744 (48.4%) 40 (2.6%)ACCI: low = 2-4, medium = 5-6,high=7andabove
Severityof ACCI
Number of Cases Based on Surgery Type (% of total cases)
CRPP HA THA TOTALLow 322 (21.1%) 261 (17.1%) 25(1.6%) 608 (39.9%)
Medium 298 (19.5%) 366(24.0%) 12 (0.8%) 676 (44.3%)High 121 (7.9%) 117 (7.7%) 3 (0.2%) 241 (15.8%)
TOTAL 741 (48.6%) 744 (48.4%) 40 (2.6%)ACCI: low = 2-4, medium = 5-6,high=7andabove
Table 2. Breakdown of cases by ACCI group and surgery type.
Figure 2. Hazard ratio for death at given ACCI cutoffs
Figure 2. Hazard ratio for death at given ACCI cutoffs
Femoral Neck Fractures Based on Age-modified CCI 21
ACCI Observed Mortality (95% CI) Based on ACCI and Surgery Type1 month 6 months
CRPP HA THA P CRPP HA THA P
Low 2% (0-3%)
2%(0-4%)
0% (0%)
CRPP vs HA: 0.53CRPP vs. THA: 0.02HA vs. THA: 0.01
4% (2-6%)
10% (7-14%)
0% (0%)
CRPP vs. HA: 0.003CRPP vs. THA: <0.001HA vs. THA: <0.001
Medium 5% (3-8%)
8% (5-11%)
9% (0-25%)
CRPP vs HA: 0.15CRPP vs. THA: 0.65HA vs. THA: 0.89
19% (14-23%)
19% (14-23%)
9% (0-25%)
CRPP vs. HA: 0.87CRPP vs. THA: 0.27HA vs. THA: 0.29
High 14% (7-20%)
19% (12-26%)
0% (0%)
CRPP vs. HA: 0.26CRPP vs. THA: <0.001HA vs. THA: <0.001
33% ( 24- 41%)
35% (25-43%)
33% (0-70%)
CRPP vs. HA: 0.76CRPP vs. THA: 0.98HA vs. THA: 0.97
p-value
Low vs. med: 0.01Low vs. high: <0.001Med vs. high: 0.01
Low vs. med: 0.01Low vs. high: 0.08Med vs. high:<0.001
Low vs. med: <0.001Low vs. high: 0.10 Med vs. high: 0.001
Low vs. med: <0.001Low vs. high: <0.001Med vs. high: 0.01
Low vs. med: 0.01Low vs. high: 0.005Med vs. high: <0.001
Low vs. med: <0.001Low vs. high: 0.003Med vs. high:0.005
ACCI: low = 2-4, medium = 5-6, high = 7 and up
Table 3. Breakdown of observed mortality at 1 and 6 months based on ACCI group and surgery type.
DISCUSSION:
Our study suggests that mortality rates after a femo-ral neck fracture are strongly associated with patient comorbidities, as a Cox proportional hazards model re-vealed that an increase in ACCI of 1 point increased the hazard ratio for death by a factor of 1.35. In addition, there is a statistically significant increase in mortality rates between the low, medium, and high ACCI groups at 1 month, 6 months, 1 year, and 2 years after surgery. This concept holds true even after accounting for surgery type, as patients in the CRPP and HA groups exhibited a similar pattern of increasing mortality rate between low, medium, and high ACCI groups.
Limited data exists in the orthopaedic literature re-garding the relationship between CCI or ACCI and mor-tality after a femoral neck fracture. Our literature search revealed only one study regarding the subject. It was a study by Radley et al.,19 which concluded that the origi-nal CCI is a promising tool for predicting post-operative complications and mortality, and has modest ability to predict 1-year mortality in hip fracture patients. How-ever, the study did not further evaluate the relationship between varying severity of CCI and mortality rate. In our study, we found statistically significant increases in
mortality rates between low, medium, and high ACCI groups at all measured post-operative periods.
Our ability to evaluate the THA group was limited by the low number of cases in this group (40 cases total, which made up only 2.6% of the study). This limitation was amplified after we subdivided the THA subjects into low, medium, and high ACCI groups. Ultimately, due to the low number of THA cases, we were unable to make reliable conclusions regarding patients who underwent THA while accounting for their comorbidities. However, past studies suggest that despite THA being a more ex-tensive surgery, patients who undergo THA do not have worse mortality rate than those who undergo CRPP or HA. This is likely because patients who undergo THA are healthier and more physically active at baseline, which makes them appropriate candidates for a more extensive surgery. A review article by Rogmark et al. suggested that elderly patients with displaced femoral neck frac-tures should undergo arthroplasty instead of internal fixa-tion.21 It further suggested that THA is favored over HA for those who are otherwise healthy, active, and mentally competent, due to fewer failures and a lower re-operation rate with THA compared to HA. However, a meta-anal-ysis by Hopley et al. compared HA to THA for displaced intracapsular hip fractures and found no statistically sig-

Femoral Neck Fractures Based on Age-modified CCI 22
nificant difference in mortality between the 2 groups.22 A study by Eisler et al. of patients with non-displaced fem-oral neck fractures who underwent CRPP found a 5.7% 6-month mortality rate.23 In our patient population, those with CRPP and low ACCI had a lower mortality rate than this, while those in the medium and high ACCI groups had a higher mortality rate. Those who underwent CRPP had a better survival rate than those who underwent HA. Sikand et al. found similar trends, particularly in 1-month and 1-year mortality, in patients with non-displaced sub-capital femoral neck fractures who underwent CRPP vs. HA.24
We aimed to elucidate the role of ACCI in conjunction with surgical modality impacting the risk of mortality in patients with femoral neck fractures. In our study, we used the ACCI because it also takes patient’s age into account. Since our patient population consisted of patients aged ≥60, the lowest possible Age-Modified CCI (ACCI) score for our patient population is 2 (see Figure 1), although the vast majority of patients’ ACCIs range from 3-6. Of note, ACCI does not increase on a linear scale, as most diseases weigh 1-2 points on the scoring system, but can potential-ly weigh up to 6 points (e.g., AIDS or metastatic disease). We tried to determine if there was an ACCI level above which mortality increases precipitously and found that at a cutoff ACCI ≥ 11, hazard ratio for death increased to 5
(whereas at any cutoff ACCI less than 11, the hazard ratio hovered around 2.5). However, since only 6 patients, or 0.4% of the study population, had ACCI ≥11, this finding was of limited clinical application.
In order to utilize ACCI in a more clinically applicable manner, we performed a post-hoc, exploratory analysis. We divided the study population into 3 categories of ACCI based on severity: low (2-4), medium (5-6), and high (7 and greater). We determined the low-medium cut-off under the following rationale: since ACCI increased by one with each increase in decade of age, physiologi-cally healthy older patients will have higher ACCI scores despite a low number of comorbidities. For instance, a patient in his 70s with no past medical history will have ACCI of 3 based on age alone, as will a patient in his 60s whose only comorbidity is diabetes without end organ damage. We deemed that these patients are rela-tively healthy for their age and thus should belong in the low ACCI group. We calculated 1-month, 6-month, 1-year, and 2-year mortality strictly based on ACCI, and as expected, found significant differences between the 3 groups. That difference in mortality was greater between medium and high ACCI populations (22% at 1 year, 23% at 2 years) than between low and medium ACCI popula-tions (14% at 1 year, 18% at 2 years). Remarkably, nearly half (46%) and more than half (58%) of the patients in the
ACCI Observed Mortality (95% CI) Based on ACCI and Surgery Type1 year 2 years
CRPP HA THA P CRPP HA THA P
Low8%
(5-10%)13%
(9-18%)0%
(0%)
CRPP vs HA: 0.03 CRPP vs. THA: <0.01 HA vs. THA: <0.01
14% (10-18%)
22 (17-27%)
0% (0%)
CRPP vs. HA: 0.01 CRPP vs. THA: <0.01 HA vs. THA: <0.001
Medium22%
(17-26%)26%
(21-30%)9%
(0-25%)
CRPP vs HA: 0.22 CRPP vs. THA: 0.17 HA vs. THA: 0.07
34% (28-39%)
36% (31-41%)
19% (0-40%)
CRPP vs. HA: 0.60 CRPP vs. THA: 0.24 HA vs. THA: 0.18
High47%
(37-55%) 45%
(35-54%) 33%
(0-70%)
CRPP vs. HA: 0.82 CRPP vs. THA: 0.63 HA vs. THA: 0.67
60% (50-68%)
58% (47-66%)
33% (0-70%)
CRPP vs. HA: 0.73 CRPP vs. THA: 0.34 HA vs. THA: 0.38
p-value
Low vs. med: <0.001 Low vs. high: <0.001Med vs. high: <0.001
Low vs. med: <0.001 Low vs. high: 0.01Med vs. high: <0.001
Low vs. med: <0.001Low vs. high: <0.001Med vs. high: <0.001
Low vs. med: <0.001 Low vs. high: <0.001 Med vs. high: <0.001
Low vs. med: <0.001Low vs. high: <0.001Med vs. high: <0.001
Low vs. med: <0.001 Low vs. high: <0.001 Med vs. high: <0.001
ACCI: low = 2-4, medium = 5-6, high = 7 and up
Table 4. Breakdown of observed mortality at 1and 2 years based on ACCI group and surgery type

Femoral Neck Fractures Based on Age-modified CCI 23
high ACCI group were dead at 1 and 2 years post-injury, respectively. These mortality rates are higher than report-ed in previous studies for femoral neck fractures, which did not take ACCI into account and had shorter follow-up.6, 25-28 However, there is a potential confounder in these analyses. Co-morbidities are taken into account when as-sessing surgical options, and since mortality likely var-ies among surgery types, we anticipate that surgery type is not identically distributed among the 3 ACCI groups, and this could possibly affect our mortality data. We ad-dressed this issue by analyzing mortality in the 3 ACCI groups separately, after separating patients by surgery type, and found similar effects of ACCI on survival in the CRPP and HA groups. Of note, in the low ACCI group, there was a statistical difference in both 1- and 2-year mortalities between CRPP and HA groups; this was not the case in the medium and high ACCI groups.
LimitationsDue to the retrospective nature of the study, potential
biases existed during the data collection process, as the accuracy of calculating the ACCI depended on the com-pleteness of the available medical records. There were also limitations to the ACCI scoring system itself. For example, the scores did not take into account acute ex-acerbation of a co-existing disease. Furthermore, scor-ing some of the diseases required subjective interpreta-tion of the severity of the disease. It also did not account for functional status at the time of injury, which may be linked to mortality.29
Finally, the low number of subjects in the THA group limited our ability to make statistically valid comparisons with CRPP and HA groups. This was particularly true when ACCI groups were taken into account, as in this set-ting we had more subcategories, leading to fewer patients within each category.
CONCLUSIONSThis study suggests that, in elderly patients who suf-
fered from femoral neck fractures, there is an association between an increase in ACCI and increased mortality at 1 month, 6 months, 1 year, and 2 years after surgical in-tervention. This association persists even after adjusting for surgery type. Although previous studies have evalu-ated the effect of co-morbidities on mortality, this study is unique in that (1) we represented various severities of co-morbidities using specific ACCI ranges and evaluated mortality at 4 different time points post-operatively; (2) we also accounted for type of surgical intervention in a subset analysis to eliminate the potentially confounding effect of surgery type on mortality; and (3) we have a large patient database comprising mostly of patients who underwent the most commonly utilized treatment groups
(CRPP and HA). The greatest mortality is seen in patients in the high ACCI range, surpassing 50% by 2 years (60% for CRPP and 58% for HA).
REFERENCES1. Eiskjaer S, Ostgård SE. Risk factors influencing mortality
after bipolar hemiarthroplasty in the treatment of fracture of the femoral neck. Clin Orthop Relat Res. 1991;270:295-300.
2. Craik RL. Disability following hip fracture. Phys Ther. 1994;74:387-398.
3. Sikand M, Wenn R, Moran CG. Mortality following sur-gery for undisplaced intracapsular hip fractures. Injury. 2004;35:1015-1019.
4. Stavrou ZP, Erginousakis DA, Loizides AA, et al. Mortality and rehabilitation following hip fracture. A study of 202 el-derly patients. Acta Orthop Scand Suppl. 1997;275:89-91.
5. Svensson O, Strömberg L, Ohlén G, et al. Prediction of the outcome after hip fracture in elderly patients. J Bone Joint Surg Br. 1996 Jan;78(1):115-8.
6. Braithwaite RS, Col NF, Wong JB. Estimating hip frac-ture morbidity, mortality and costs. J Am Geriatr Soc. 2003;51:364–370.
7. Brauer CA, Coca-Perraillon M, Cutler DM, et al. Incidence and mortality of hip fractures in the United States. JAMA. 2009;302:1573-1579.
8. Youm T, Koval KJ, Zuckerman JD. The economic impact of geriatric hip fractures. Am J Orthop. 1999;28:423–428.
9. Blomfeldt R, Tornkvist H, Ponzer S, et al. Comparison of internal fixation with total hip replacement for displaced femoral neck fractures. Randomized, controlled trial per-formed at four years. J Bone Joint SurgAm. 2005;87:1680-1688.
10. Rogmark C, Johnell O. Orthopaedic treatment of displaced femoral neck fractures in elderly patients. Disabil Rehabil. 2005;27:1143-1149.
11. Iorio R, Schwartz B, Macaulay W, et al. Surgical treatment of displaced femoral neck fractures in the elderly: a survey of the American Association of Hip and Knee Surgeons. J Arthroplasty. 2006;21:1124-1133.
12. Bhandari M, Devereaux P J, Tornetta P 3rd, et al. Operative management of displaced femoral neck fractures in elderly patients. An international survey. J Bone Joint Surg Am. 2005;87:2122-2130.
13. World Population Ageing 2009. Department of Economic and Social Affairs of the United Nations Population Divi-sion. Available at: http://www.un.org/en/development/desa/publications/world-population-ageing-2009.html. Accessed July 24, 2013.
14. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Disease. 1987;40:373-383.
Femoral Neck Fractures Based on Age-modified CCI 24
ACCI (n)
Observed % Mortality (95% CI) Based on Age-Modified CCI
1 month* 6 months* 1 year* 2 years*Low (608)
2% (1-3%)
7%(4-9%)
10% (7-12%)
17% (14-20%)
Medium (676)
7% (5-8%)
19%(16-20%)
24% (20-27%)
35% (31-39%)
High (241)
16% (11-21%)
34% (27-39%)
46%(39-52%)
58% (51-64%)
* Pairwise comparisons reveal p <0.001 between low, medium, and high ACCI groups at respective time intervalsAge-Modified CCI: low = 2-4, medium = 5-6, high = 7 and up
APPENDIX A.Table 1A. Observed 1 month, 6 month, 1 year, and 2 year mortality based on ACCI group.
15. Gabriel SE, Crowson CS, O’Fallon WM. A comparison of two comorbidity instruments in arthritis. J Clin Epidemiol. 1999;52:1137-1142.
16. Charlson ME, Szatrowki TP, Peterson J, et al. Valida-tion of a combined comorbidity index. J Clin Epidemiol. 1994;47:1245-1251.
17. Liu L, Leung JM. Predicting adverse postoperative out-comes in patients aged 80 years or older. J Am Geriatr Soc. 2000;48:405–412.
18. Kirkland LL, Kashiwagi DT, Burton MC, et al. The Charlson Comorbidity Index Score as a predictor of 30-day mortality after hip fracture surgery. Am J Med Qual. 2011;26:461-467.
19. Radley DC, Gottlieb DJ, Fisher ES, et al. Comorbidity risk-adjustment strategies are comparable among persons with hip fracture. J Clin Epidemiol. 2008;61:580-587.
20. Probe R, Ward R. Internal fixation of femoral neck frac-tures. J Am Acad Orthop Surg. 2006;14:565–571.
21. Rogmark C, Johnell O. Orthopaedic treatment of displaced femoral neck fractures in elderly patients. Disabil Rehabil. 2005;27:1143-1149.
22. Hopley C, Stengel D, Ekkenkamp A, ey al. Primary total hip arthroplasty versus hemiarthroplasty for displaced intracapsular hip fractures in older patients: systematic review. BMJ. 2010;340:c2332.
23. Eisler J, Cornwall R, Strauss E, et al. Outcomes of elderly patients with nondisplaced femoral neck fractures. Clin Orthop Relat Res. 2002;399: 52-58.
24. Sikand M, Wenn R, Moran CG. Mortality following surgery for undisplaced intracapsular hip fractures. Injury. 2004;35:1015-1019.
25. Kannegaard PN, van der Mark S, Eiken P, et al. Excess mortality in men compared with women following a hip fracture. National analysis of comedications, comorbidity and survival. Age Ageing. 2010;39:203-209.
26. Novack V, Jotkowitz A, Etzion O, et al. Does delay in surgery after hip fracture lead to worse outcomes? A multi-center survey. Int J Qual Health Care. 2007;19:170-176.
27. Lawrence VA, Hilsenbeck SG, Noveck H, et al. Medical complications and outcomes after hip fracture repair. Arch Intern Med. 2002;162: 2053-2057.
28. Aharonoff GB, Koval KJ, Skovron ML, et al. Hip fractures in the elderly: predictors of one year mortality. J Orthop Trauma. 1997;11:162-165.
29. Patel KV, Brennan KL, Brennan ML, et al. Association of a modified frailty index with mortality after femoral neck fracture in patients aged 60 years and older. Clin Orthop Relat Res. 2014;472(3):1010-7.

25
The Use of Routine Thoracoabdominal CTScans in the Polytrauma Patient toEstimate ObesityDavid F. Ferguson1, Bryce J. Busenlehner2, Mark D. Rahm1,2, Sachin M. Mehta2,Juhee Song3,4, Matthew L. Davis2,5, H. Wayne Sampson1,6 and Christopher D. Chaput1,2
Objective: To utilize data from routine CT scans to quantify obesity in polytrauma patients without the
need to obtain a height and weight.
Design and Methods: We utilized a comprehensive database including multidetector CT
thoracoabdominal images of all polytrauma patients admitted to a Level 1 trauma center. One thousand
one hundred seventy-four patients were reviewed from 2006 to 2008 and of these, 162 had previous
documentation of Body Mass Index (BMI) or height and weight measurements as an outpatient within 6
months of trauma activation and with a truncal girth smaller than the scanning area of the CT machine.
Truncal Adiposity Volume (TAV) was calculated from three dimensional reconstructions (3DRs) of the CT
scans of the thorax and abdomen obtained in the emergency department.
Results: Statistical analysis yielded a fairly good correlation between TAV and BMI (correlation coefficient
¼ 0.77; p-value < 0.0001). The intra-observer and inter-observer correlations in measuring TAV were
high; 0.99 and 0.98 respectively. A linear regression equation of BMI on TAV was estimated and it had a
form: 3DR BMI ¼ 20.81þ0.00064�TAV. In conclusion, TAV provides a reproducible means of evaluating
obesity in trauma patients from routinely obtained CT scans.
Conclusions: The TAV eliminates the often problematic task of obtaining a height and weight in a trauma
patient and it correlates fairly well with the most commonly used clinical method of quantifying patient
adiposity, BMI. This method may provide a more direct measurement of adiposity than does BMI, and
holds promise for improving trauma care and research in the obese patient.
Obesity (2013) 21, 997-1003. doi:10.1038/oby.2012.163
IntroductionObesity is reaching epidemic proportions in the United States, and
in 2007-2008, the age-adjusted prevalence of obesity was 33.8% (1).
This rise in obesity in the general population is reflected in increas-
ing number of polytrauma patients who are significantly overweight.
Obesity appears to affect injury patterns in multitrauma and increase
complications of treatment (2,3). Obese polytrauma patients have
been documented to stay 4.8 days longer (4) in the intensive care
unit and need 2 additional days of ventilatory support than patients
with a normal BMI (2). A higher incidence of multiple organ failure
(5) and mortality has also been reported (2,5).
BMI is an index of weight for height (kg/m2) commonly used to
classify adult weight, with >30 being defined as obese (6). How-
ever, increased adiposity without defined obesity may also be a clin-
ically relevant concern. Elevated markers of chronic inflammation
are related to increasing BMI (7), and may affect the inflammatory
response related to trauma. Edmonds et al. (8) evaluated complica-
tions and outcomes in nonobese trauma patients with attention paid
to increasing BMI. Their findings indicate a trend for worse out-
comes in patients whose BMI is elevated but still below the obesity
cutoff of 30 kg/m2, and that the risk of multiorgan failure and noso-
comial infections increase as the body adipose content increases.
BMI is generally a fairly good indicator of excess adiposity; how-
ever, since it is based on a simple height to weight proportion, the
accuracy of BMI varies according to the degree of adiposity and
lean mass (9,10). Very muscular patients can be erroneously classi-
fied as obese secondary to a high level of fat free mass. As much as
1 Department of Orthopaedic Surgery, Scott & White Hospital, Temple, Texas, USA. Correspondence: Christopher D. Chaput ([email protected])2 College of Medicine, Texas A&M Health Science Center, College Station, Texas, USA 3 Department of Biostatistics, Scott & White Hospital, Temple, Texas,USA 4 Department of Medicine, College of Medicine, Texas A&M Health Science Center, College Station, Texas, USA 5 Department of Surgery, Scott & WhiteHospital, Temple, Texas, USA 6 Department of Systems Biology and Translational Medicine, Texas A&M Health Science Center College of Medicine, Temple,Texas, USA
Disclosure: The authors declared no conflict of interest.
See the online ICMJE Conflict of Interest Forms for this article.
Received: 3 May 2012 Accepted: 30 May 2012 Published online 26 July 2012. doi:10.1038/oby.2012.163
www.obesityjournal.org Obesity | VOLUME 21 | NUMBER 5 | MAY 2013 997
Original ArticleOBESITY BIOLOGY AND INTEGRATED PHYSIOLOGY
Obesity

26
25% of men may be classified as obese by BMI standards but non-
obese based on dual-energy X-ray absorptiometry (DXA) scans. The
inverse is also true in that approximately one-half of women are
classified as nonobese by BMI, but having an obese percent body
fat by DXA (11). There are also issues specific to the polytrauma
patient that might limit the accuracy and utility of the BMI. Calcu-
lating an accurate height is difficult in the polytrauma patient, who
is generally supine, intubated, and immobilized. The weight might
be difficult to measure and document soon after arrival to the emer-
gency department when the focus is on resuscitation. Early weight
measurement is important, as significant weight fluctuations can be
seen with fluid resuscitation (12). A reproducible method to calcu-
late obesity from routine thoracoabdominal computed tomography
(CT) scans that correlates with BMI might obviate the need for
these measurements, and the study of patient obesity in the trauma
setting would be facilitated.
In addition, the calculation of adiposity by itself has potential value,
regardless of whether the degree of adiposity qualifies the patient as
obese. The adipocyte is an active cell and it is known to produce
many pro-inflammatory cytokines and chemical mediators, and
excess adiposity has potential for causing excess systemic pro-
inflammatory cytokines (13-16). Recently, interest in the potential
role of these adipokines in relationship to bone quality, heterotopic
bone, and metabolic syndrome has increased (17). A method of eas-
ily quantifying adiposity from already available studies would, thus,
facilitate further research in this area.
The purpose of this study was to use data from routine CT scans to
quantify obesity in polytrauma patients without the need to obtain a
height and weight. We hypothesized that three dimensional recon-
structions (3DRs) of standard trauma CT scans can quantify obesity in
a reproducible manner and have an acceptable correlation with BMI.
Methods and ProceduresSelection criteria and search strategyThis was a retrospective analysis with radiographic and clinical
review. A total of 1,174 patients in the comprehensive American Col-
lege of Surgeons verified level 1 database were reviewed from 2006
to 2008. Predefined inclusion criteria were (i) 911 trauma registry
patients with a CT scan and BMI available in the electronic medical
record less than 6 months prior to the trauma and (ii) patients 17 years
of age or older. Exclusion criteria for the primary group included (i)
penetrating abdominal injuries, (ii) lack of a documented BMI within
6 months of CT scan, (iii) pregnancy, (iv) obvious signs of abdominal
trauma, and (v) truncal girth larger than the scanning area of the CT
machine. There were 261 patients identified to meet inclusion criteria.
The primary group was comprised of 162 patients, and a subclass
group was also identified of 99 patients who were excluded based on
criteria (v). They fell out of the scanning range of the CT scanner due
to positioning, body habitus, or overcropping with resultant gantry
cutoff. Age, gender, height, weight, and radiographic measurements
were recorded for all patients.
Two methods were used to quantify adiposity: (i) direct measure-
ments of the subcutaneous adipose tissue were obtained from unrec-
onstructed axial CT scans and (ii) The original Dicom data was
reconstructed into coronal images, the region from T10 to the coc-
cyx selected and then a 3 dimensional volume rendering of thora-
coabdominal adipose tissue made (OsiriX, version 3.1 32-bit; OsiriX
Foundation, Geneva, Switzerland).
Multidetector CT acquisition and reconstructiontechniqueAll multidetector computerized tomographic images from 2006 to
2008 were performed on a model Siemens 64 Sensation (Siemens
Aktiengesellschaft, Munich, Germany). Patients were scanned in the
supine position in a cranial to caudal direction from the level of the
occiput to the femoral shaft with a zero point reference of the exter-
nal auditory meatus. A kVp/Ma of 120/CAREDOSE or 120/400 was
used to optimize penetration with a slice/detector rows setting of 3
mm 64 � 0.6 mm at a pitch of 0.9 and rotation time of 1 s. Meas-
urements were made on the unreconstructed CT images (Centricity
Enterprise Web, version 3.0; GE Healthcare, UK) and were com-
pared with the 3DR images for quality control.
3DRs of truncal body fat were made using the volume of interest
cutter tool within the 3DR software. This tool allows one to define a
cubic area of interest and exclude certain tissues of disinterest (in
this case, nonfat tissue). Images were cropped by focusing between
an axial view of the T10 vertebral body at the pedicles inferiorly to
the inferior-most portion of the coccyx. If transitional levels were
encountered, the films were reviewed and S1 was identified, and
eight vertebrae were counted numerically superiorly until T10 was
visualized. The total number of images and thickness were then
recorded from the cropped image and their product determined the
total image length. An image was then brought into the plane where
the superior most portion of the superior iliac crest could be seen. A
FIGURE 1 Axial view of superior iliac crest, adipose tissue highlighted 1 cm perpen-dicularly from the superior iliac crest. [Color figure can be viewed in the onlineissue, which is available at wileyonlinelibrary.com.]
Obesity The Use of Routine Thoracoabdominal CT Scans Ferguson et al.
998 Obesity | VOLUME 21 | NUMBER 5 | MAY 2013 www.obesityjournal.org
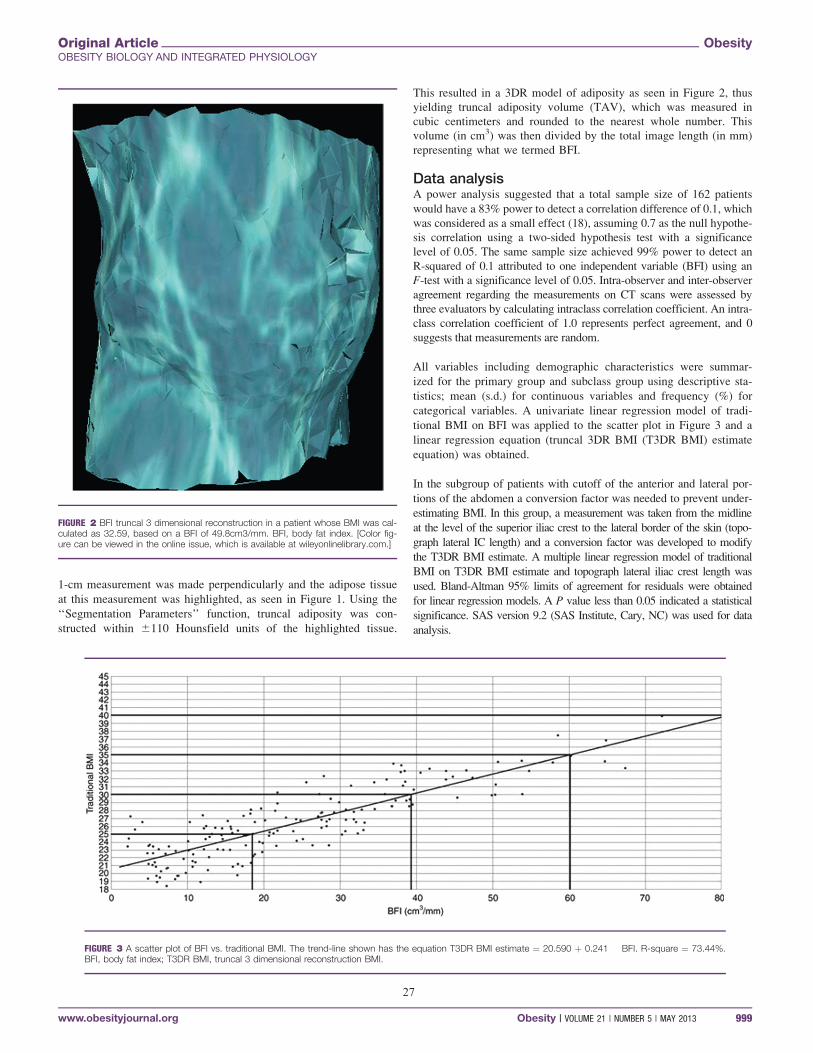
27
1-cm measurement was made perpendicularly and the adipose tissue
at this measurement was highlighted, as seen in Figure 1. Using the
‘‘Segmentation Parameters’’ function, truncal adiposity was con-
structed within 6110 Hounsfield units of the highlighted tissue.
This resulted in a 3DR model of adiposity as seen in Figure 2, thus
yielding truncal adiposity volume (TAV), which was measured in
cubic centimeters and rounded to the nearest whole number. This
volume (in cm3) was then divided by the total image length (in mm)
representing what we termed BFI.
Data analysisA power analysis suggested that a total sample size of 162 patients
would have a 83% power to detect a correlation difference of 0.1, which
was considered as a small effect (18), assuming 0.7 as the null hypothe-
sis correlation using a two-sided hypothesis test with a significance
level of 0.05. The same sample size achieved 99% power to detect an
R-squared of 0.1 attributed to one independent variable (BFI) using an
F-test with a significance level of 0.05. Intra-observer and inter-observer
agreement regarding the measurements on CT scans were assessed by
three evaluators by calculating intraclass correlation coefficient. An intra-
class correlation coefficient of 1.0 represents perfect agreement, and 0
suggests that measurements are random.
All variables including demographic characteristics were summar-
ized for the primary group and subclass group using descriptive sta-
tistics; mean (s.d.) for continuous variables and frequency (%) for
categorical variables. A univariate linear regression model of tradi-
tional BMI on BFI was applied to the scatter plot in Figure 3 and a
linear regression equation (truncal 3DR BMI (T3DR BMI) estimate
equation) was obtained.
In the subgroup of patients with cutoff of the anterior and lateral por-
tions of the abdomen a conversion factor was needed to prevent under-
estimating BMI. In this group, a measurement was taken from the midline
at the level of the superior iliac crest to the lateral border of the skin (topo-
graph lateral IC length) and a conversion factor was developed to modify
the T3DR BMI estimate. A multiple linear regression model of traditional
BMI on T3DR BMI estimate and topograph lateral iliac crest length was
used. Bland-Altman 95% limits of agreement for residuals were obtained
for linear regression models. A P value less than 0.05 indicated a statistical
significance. SAS version 9.2 (SAS Institute, Cary, NC) was used for data
analysis.
FIGURE 3 A scatter plot of BFI vs. traditional BMI. The trend-line shown has the equation T3DR BMI estimate ¼ 20.590 þ 0.241 � BFI. R-square ¼ 73.44%.BFI, body fat index; T3DR BMI, truncal 3 dimensional reconstruction BMI.
FIGURE 2 BFI truncal 3 dimensional reconstruction in a patient whose BMI was cal-culated as 32.59, based on a BFI of 49.8cm3/mm. BFI, body fat index. [Color fig-ure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Original Article ObesityOBESITY BIOLOGY AND INTEGRATED PHYSIOLOGY
www.obesityjournal.org Obesity | VOLUME 21 | NUMBER 5 | MAY 2013 999

28
ResultsThere were 162 patients in the primary group. The average age was
42 years (s.d.: 18), and 121 patients (74.7%) were males. The aver-
age BMI was 26 (s.d.: 4) with the minimum of 18 and the maximum
of 40. The subclass group was comprised of 99 subjects with the av-
erage age of 41 years (s.d.: 17), and 54 patients (54.5%) were males.
The average BMI was 30 (s.d.: 7) with the minimum of 19 and the
maximum of 49. There were 10 subjects (10.1%) of which BMI
exceeded the maximum BMI of the primary group.
Statistical analysis confirmed the hypothesis that T3DR of standard
trauma CT scans can estimate obesity with a high degree of reprodu-
cibility. The intra-observer and inter-observer correlations in meas-
uring BFI were higher than 0.99 and 0.98, respectively, demonstrating
excellent agreement among three raters and within each rater.
A scatter plot of traditional BMI vs. BFI demonstrated a positive
linear association between BFI and traditional BMI (correlation
coefficient ¼ 0.86; P < 0.0001; Figure 3). A linear regression equa-
tion called T3DR BMI estimate has a form: T3DR BMI estimate ¼20.590 þ 0.241 � BFI. R-square of the model was 73.44% and root
mean square error was 62.25. Figure 4 demonstrates a good agree-
ment between predicted BMI (T3DR BMI estimate) and observed
BMI (traditional BMI). Bland-Altman 95% limits of agreement for
residuals were (-4.40, 4.40), which indicated that differences
between traditional BMIs and T3DR BMI estimates were within
64.40 kg/m2 most of the time.
For the subclass of patients with gantry cutoff, T3DR BMI estimates
were calculated using the T3DR BMI estimate equation with a con-
version factor. A multiple linear regression model was applied to
estimate traditional BMI using T3DR BMI estimate and topograph
lateral IC length, and the multiple linear regression equation had a
form:
T3DR BMI estimate conversion ¼�4.860 þ 0.961 � T3DR BMI
estimate þ 0.799 � topograph lateral IC length.
R-square of the model was 88.01% and root mean square error was
62.40. This subclass of patients with gantry cutoff demonstrated a
considerably good agreement between observed BMI (traditional
BMI) and predicted BMI (T3DR BMI estimate conversion) (Figure
5). Bland-Altman 95% limits of agreement for residuals were (-4.65,
4.65), which indicated that differences between traditional BMIs and
T3DR BMI estimates with conversion were within 64.65 kg/m2
most of the time.
DiscussionOver the past 15 years, there has been a sharp increase in the use of
CT scans made possible by increasing speed of modern scanners
and advances in the quality of the images obtained (19). Previous
studies have shown that CT-based adipose tissue measurements are
reproducible and can accurately determine volumetric adiposity and
distribution (20,21,22,23). Mourtzakis et al. (23) showed that fat
mass on a single CT axial image at the level 3 had a strong cor-
relation to whole body fat mass based on whole body DXA meas-
urements (r ¼ 0.88). However, previous use of CT scans for this
purpose required multiple measurements that were time consuming
and therefore had limited adoption outside the research setting (21).
In the polytrauma patient, thoracoabdominal multidetector com-
puterized tomographics are now routinely obtained at many trauma
centers. Our 3DR method of estimating obesity allows for a repro-
ducible and easily performed method of evaluating truncal adiposity
in this patient population.
A T3DR BMI estimate equation based on a linear regression model
(Figure 3; solid line T3DR BMI estimate ¼ 20.590 þ 0.2407 �BFI) can be used to help a clinician relate a particular BFI to BMI.
FIGURE 4 Predicted BMI using BFI (truncal 3 dimensional reconstruction BMI (T3DR BMI) estimate) vs. traditional BMI. The solid line represents the line ofidentity. Equation used for T3DR BMI estimate ¼ 20.590 þ 0.2407 � BFI. R-square ¼ 73.44%. BFI, body fat index.
Obesity The Use of Routine Thoracoabdominal CT Scans Ferguson et al.
1000 Obesity | VOLUME 21 | NUMBER 5 | MAY 2013 www.obesityjournal.org
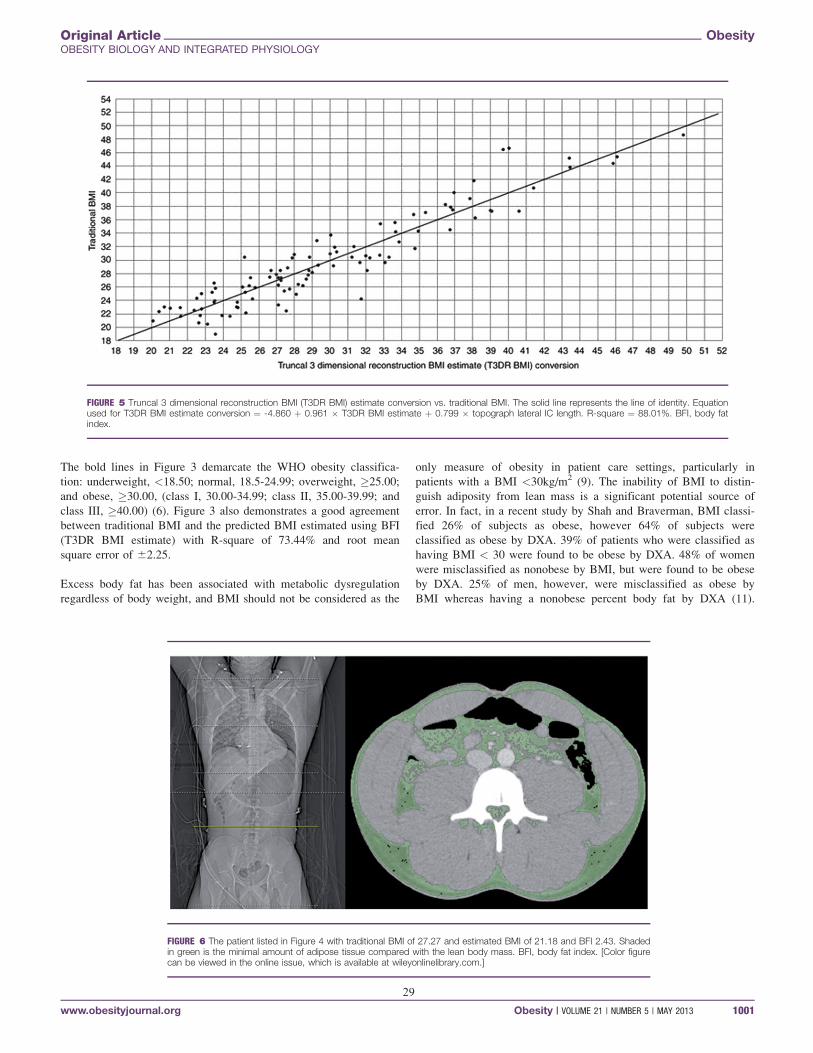
29
The bold lines in Figure 3 demarcate the WHO obesity classifica-
tion: underweight, <18.50; normal, 18.5-24.99; overweight, �25.00;
and obese, �30.00, (class I, 30.00-34.99; class II, 35.00-39.99; and
class III, �40.00) (6). Figure 3 also demonstrates a good agreement
between traditional BMI and the predicted BMI estimated using BFI
(T3DR BMI estimate) with R-square of 73.44% and root mean
square error of 62.25.
Excess body fat has been associated with metabolic dysregulation
regardless of body weight, and BMI should not be considered as the
only measure of obesity in patient care settings, particularly in
patients with a BMI <30kg/m2 (9). The inability of BMI to distin-
guish adiposity from lean mass is a significant potential source of
error. In fact, in a recent study by Shah and Braverman, BMI classi-
fied 26% of subjects as obese, however 64% of subjects were
classified as obese by DXA. 39% of patients who were classified as
having BMI < 30 were found to be obese by DXA. 48% of women
were misclassified as nonobese by BMI, but were found to be obese
by DXA. 25% of men, however, were misclassified as obese by
BMI whereas having a nonobese percent body fat by DXA (11).
FIGURE 5 Truncal 3 dimensional reconstruction BMI (T3DR BMI) estimate conversion vs. traditional BMI. The solid line represents the line of identity. Equationused for T3DR BMI estimate conversion ¼ -4.860 þ 0.961 � T3DR BMI estimate þ 0.799 � topograph lateral IC length. R-square ¼ 88.01%. BFI, body fatindex.
FIGURE 6 The patient listed in Figure 4 with traditional BMI of 27.27 and estimated BMI of 21.18 and BFI 2.43. Shadedin green is the minimal amount of adipose tissue compared with the lean body mass. BFI, body fat index. [Color figurecan be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Original Article ObesityOBESITY BIOLOGY AND INTEGRATED PHYSIOLOGY
www.obesityjournal.org Obesity | VOLUME 21 | NUMBER 5 | MAY 2013 1001

30
This discrepancy can also be seen in our data at lower BMIs (Figure
4). Figures 6 and 7 show scout views and axial views at the level of
the L4 vertebral body in a young male with substantial lean body
mass and a female with much less lean body mass. The areas high-
lighted in green illustrate the amount of fat content in two appa-
rently thin patients. Since the accuracy of traditional BMI varies
according to multiple factors, the BFI may prove to be a more accu-
rate approach to quantifying adiposity since all lean muscle and
fluid weight is easily removed and only truncal adiposity is
considered.
This study has several limitations. BMI, height and weight were not
calculated at the time of the trauma, but recorded within 6 months
of the trauma. Due to Hounsfield units corresponding to certain den-
sities, in a few patients the thin pad overlying the table of the CT
scanner highlighted when Hounsfield units were selected for TAV.
These cases could inadvertently inflate the new method of calculat-
ing obesity. In cases where this occurred, 1,000 cm3 were subtracted
from the fat volume to correct for the volume of the table pad that
was inadvertently included. In addition, when highlighting Houns-
field units, certain densities within the intestinal lumen would also
be highlighted; it is uncertain if this occurred due to artifact or to
digested lipids. This occurred rarely, and the volume of the high-
lighted region in the lumen was small and not thought to have bear-
ing upon the result.
As mentioned, a subclass of patients were also analyzed where accu-
rate T3DR BFI could not be made due to truncal girth exceeding
the scanning area of the CT (usually) or positioning/over cropping
errors by the CT technician. The T3DR BMI estimate with conver-
sion calculation using the topograph lateral IC length appears to
account for this effect allowing for BMI calculation in these individ-
uals as well.
There are several advantages in estimating obesity with BFI. Height
and weight can be difficult to obtain, and many polytrauma patients
have CT scans taken immediately on arrival before large weight
shifts due to fluid resuscitation occur. This method also allows for a
calculation of adiposity that excludes lean muscle and other nonadi-
pose tissue that, with further research, may prove to be more clini-
cally relevant than the traditional BMI. In particular, this technique
could be applied to large existing CT databases to determine associ-
ations with excess adiposity and multiple other disease states, some
of which may not have been reported previously (17).
In summary, this study supports quantifying adiposity based on
T3DRs of CT scans of the chest/abdomen/pelvis. This method is re-
producible and may more accurately reflect true adiposity. This
rapid, simple, and reproducible method can be calculated for all
patients with a CT scan using either the T3DR BMI estimate or con-
version factor equations and may more accurately reflect a patient’s
true adiposity. This method could also aid in identifying hospitalized
trauma patients with risk factors for poor outcomes that are associ-
ated with obesity, allow analysis of large trauma databases with
regard to obesity and clinical outcomes even when height and
weight measurements are not available.O
VC 2012 The Obesity Society
References1. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity
among US adults, 1999-2008. JAMA 2010;303:235-241 (doi:10.1001/jama.2009.2014).
2. Brown CV, Neville AL, Rhee P et al. The impact of obesity on the outcomes of1,153 critically injured blunt trauma patients. J Trauma 2005;59:1048-51; discussion1051.
3. Lazar MA, Plocher EK, Egol KA. Obesity and its relationship with pelvic andlower-extremity orthopedic trauma. Am J Orthop 2010;39:175-182.
4. Dossett LA, Heffernan D, Lightfoot M et al. Obesity and pulmonary complicationsin critically injured adults. Chest 2008;134:974-980.
5. Neville AL, Brown CVR, Weng J, Demetriades D, Velmahos GC. Obesity is an in-dependent risk factor of mortality in severely injured blunt trauma patients. ArchSurg 2004 139:983-987
6. World Health Organization. BMI Classification. Adapted from WHO, 1995, WHO,2000, and WHO, 2004. <http://apps.who.int/bmi/index.jsp?introPage¼intro_3.html>.
7. Festa A, D’Agostino R Jr, Williams K et al. The relation of body fat mass and dis-tribution to markers of chronic inflammation. Int J Obes Relat Metab Disord 2001;25:1407-1415.
FIGURE 7 The patient listed in Figure 4 with traditional BMI of 19.85 and estimated BMI of 24.56 and BFI 16.48.Shaded in green is the increased amount of adipose tissue compared with lean body mass. BFI, body fat index. [Colorfigure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Obesity The Use of Routine Thoracoabdominal CT Scans Ferguson et al.
1002 Obesity | VOLUME 21 | NUMBER 5 | MAY 2013 www.obesityjournal.org

31
8. Edmonds R, Billiar T, Roseng art A et al. Body Adipose Content is IndependentlyAssociated with a Higher Risk of Organ Failure and Nosocomial Infection in theNon-Obese Patient Post-Injury. 40th Annual Meeting of The Western Trauma Asso-ciation 2010.
9. Okorodudu DO, Jumean MF, Montori VM et al. Diagnostic performance of bodymass index to identify obesity as defined by body adiposity: a systematic reviewand meta-analysis. Int J Obes 2010;34:791-799.
10. Romero-Corral A, Somers VK, Sierra-Johnson J et al. Accuracy of body mass indexin diagnosing obesity in the adult general population. Int J Obes (Lond) 2008;32:959-966.
11. Shah NR, Braverman ER. Measuring adiposity in patients: the utility of body massindex (BMI), percent body fat, and leptin. PLoS ONE 2012;7:e33308.
12. Du GB, Slater H, Goldfarb IW. Influences of different resuscitation regimenson acute early weight gain in extensively burned patients. Burns 1991;17:147-150.
13. An JJ, Han DH, Kim DM et al. Expression and regulation of osteoprotegerin in adi-pose tissue. Yonsei Med J 2007;48:765-772.
14. Fried SK, Bunkin DA, Greenberg AS. Omental and subcutaneous adipose tissues ofobese subjects release interleukin-6: depot difference and regulation by glucocorti-coid. J Clin Endocrinol Metab 1998;83:847-850.
15. Gilsanz V, Chalfant J, Mo AO et al. Reciprocal relations of subcutaneous and vis-ceral fat to bone structure and strength. J Clin Endocrinol Metab 2009;94:3387-3393.
16. Gnacinska M, Malgorzewicz S, Guzek M, Lysiak-Szydlowska W, Sworczak K. Adi-pose tissue activity in relation to overweight or obesity. Endokrynol Pol 2010;61:160-168.
17. Chaput CD, Mehta SM, Busenlehner BJ et al. Obesity and hyperostosis of the spi-nal ligaments: a comprehensive CT analysis of the entire spine in a random traumapopulation. Spine J 2011;9, (Suppl):158S-159S.
18. Cohen J. Statistical Power Analysis for the Behavioral Sciences, 2nd edn. LawrenceErlbaum: New Jersey, 1988.
19. Brenner DJ, Hall EJ. Computed tomography-an increasing source of radiation expo-sure. N Engl J Med 2007;357:2277-2284.
20. Ferland M, Despr�es JP, Tremblay A et al. Assessment of adipose tissue distributionby computed axial tomography in obese women: association with body density andanthropometric measurements. Br J Nutr 1989;61:139-148.
21. Kvist H, Chowdhury B, Grangard U, Tyl�en U, Sj€ostr€om L. Total and visceral adi-pose-tissue volumes derived from measurements with computed tomography inadult men and women: predictive equations. Am J Clin Nutr 1988;48:1351-1361.
22. Seidell JC, Oosterlee A, Thijssen MA et al. Assessment of intra-abdominal and sub-cutaneous abdominal fat: relation between anthropometry and computed tomogra-phy. Am J Clin Nutr 1987;45:7-13.
23. Mourtzakis M, Prado CM, Lieffers JR et al. A practical and precise approach toquantification of body composition in cancer patients using computed tomographyimages acquired during routine care. Appl Physiol Nutr Metab 2008;33:997-1006.
Original Article ObesityOBESITY BIOLOGY AND INTEGRATED PHYSIOLOGY
www.obesityjournal.org Obesity | VOLUME 21 | NUMBER 5 | MAY 2013 1003
32
ORIGINAL REPORTS
Evaluation of an InterprofessionalClinician–Patient Communication WorkshopUtilizing Standardized Patient Methodology
Casey Lagan, MD,*† Hania Wehbe-Janek, PhD,*† Kim Waldo, RN,* Amy Fox, AA,*Chanhee Jo, PhD,*† and Mark Rahm, MD*†
*Department of Orthopaedic Surgery, Scott and White Healthcare, Temple, Texas; and †College ofMedicine, Texas A&M Health Science Center, Temple, Texas
OBJECTIVE: Communication and interpersonal skills (CIS)are one of the 6 general competencies required by the Accredi-tation Council for Graduate Medical Education (ACGME).The clinician–patient communication (CPC) workshop, devel-oped by the Institute for Healthcare Communication, providesan interactive opportunity to practice and develop CIS. Theobjectives of this study were to (1) determine the impact of aCPC workshop on orthopedic surgery residents’ CIS (2) deter-mine the impact of physician alone or incorporation of nursingparticipation in the workshop, and (3) incorporate standardizedpatients (SPs) in resident training and assessment of CIS.
METHODS: Stratified by training year, 18 residents of an Or-thopaedic Surgery Residency Program were randomized to aCPC workshop with only residents (group A, n � 9) or a CPCworkshop with nurse participants (group B, n � 9). Data in-cluded residents’ (1) CIS scores as evaluated by SPs and (2)self-reports from a 25-question survey on perception of CIS.Data were collected at baseline and 3 weeks following the work-shop.
RESULTS: Following the workshop, the combined group(group A and B) felt more strongly that the ACGME shouldrequire a communication training and evaluation curriculum(post mean � 52.7, post–pre difference � 15.94, p � 0.026).Group A residents felt more strongly that communication is alearned behavior (post mean � 82.7, post–pre difference �17.67, p � 0.028), and the addition of SPs was a valuableexperience (post mean � 59.3, post–pre difference � 16.44,p � 0.038). Group B residents reported less willingness toimprove on their communication skills (post-mean � 79.7,post–pre difference � �7.44, p � 0.049) and less improve-ment in professional satisfaction in effective communicationthan group A (post mean group A � 81.9, group B � 83.6,
post–pre difference group A � 7.11, group B � 1.89, p �0.047). Few differences between groups regarding CIS scoreswere detected.
CONCLUSIONS: While there was no demonstrable differ-ence regarding CIS, our study indicates that participants valuedthe importance of communication training and found SPs to bea valuable addition. The addition of interprofessional partici-pation appeared to detract from the experience. Further study iswarranted to elucidate the variables associated with interprofes-sional education within the context of CIS training and assess-ment using SPs in residency. (J Surg 70:95-103. © 2012Association of Program Directors in Surgery. Published byElsevier Inc. All rights reserved.)
KEY WORDS: ACGME competencies, interpersonal commu-nication, IPC course, interprofessional, residency program
COMPETENCIES: Professionalism, Interpersonal and Com-munication Skills, Systems-Based Practice
INTRODUCTION
Communication and interpersonal skills (CIS) are one of the 6general competencies the ACGME endorses to define require-ments for medical education during residency.1 CIS encom-passes multiple activities, including building quality doctor–patient relationship quality, articulate data-gathering, andpatient education.2,3 Ineffective CIS with poor physician–patientcommunication may lead to patient mistrust, dissatisfaction, andlitigation.4,5
The ACGME endorsed the 6 general competencies in 1999,and further required programs to implement both training andassessment tools addressing the competencies in 2002.6,7 Ingeneral, the core competencies lend themselves readily to tradi-tional methods of training and assessment, however, CIS alsopose interesting and unique challenges. Many alternative ap-proaches to teaching CIS are being explored in response to thedefinition of the core competencies in lieu of traditional didac-
Correspondence: Inquiries to Mark Rahm, MD, Department of Orthopaedic Surgery,MS-01-610A, Scott and White Healthcare, 2401 S 31st Street, Temple, TX 76508; e-mail:[email protected]
Journal of Surgical Education • © 2012 Association of Program Directors in Surgery 1931-7204/$30.00Published by Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jsurg.2012.06.018
95

33
tic methods. These include simulated situations, ObjectiveStructured Clinical Exams (OSCE), role play, the use of stan-dardized patients (SPs), creation of portfolios, direct observa-tion, journaling, and a host of other methods.8-13 Simulationmethodologies using SPs may be effective tools for teaching andassessing CIS. SPs are individuals trained to accurately andconsistently simulate a patient case and to assess the physicianbehavior based on fixed criteria. This educational tool has be-come more accepted, and assessment strategies using SPs havebeen shown to reliably measure physician–patient CI.8,14-19
SPs have been utilized by medical schools in OSCEs to objec-tively measure numerous areas of clinical competence and theUnited States Medical Licensure Examination requires passinga similar Clinical Skills examination before licensure.20-22 TheACGME also endorses the use of SPs in training and as anoutcome assessment tool to measure residents’ competency invarious areas, including CIS.23 The CPC workshop was devel-oped by the Institute for Healthcare Communication to pro-vide participants with an interactive opportunity to practiceand develop CIS,24 and has been endorsed by the AmericanAcademy of Orthopaedic Surgeons as a means to improve CIS.Participants work individually and in teams to analyze video-taped reenactments of actual cases, reach agreement on effectivecommunication, and create effective responses where appropri-ate. Participants also role play in simulated cases during theworkshop to practice CIS. While interprofessional communica-tion is considered an important facet of effective healthcare com-munication and patient care, it is uncertain if educational activitieswould be more beneficial with multidisciplinary participants (i.e.,including nurses, rather than physicians alone).25,26 Scott andWhite Memorial Hospital (SWMH), a level 1 academic traumacenter, is affiliated with the Texas A&M Health Science Center(HSC), College of Medicine in Temple, Texas. Simulation includ-ing SPs has been a fundamental educational tool for teaching andassessing CIS for various components in our HSC. Since 2009,the CPC workshop has been delivered as a Continuing MedicalEducation activity to multiple departments. The followingstudy was designed to incorporate the CPC workshop, SPs, andinterprofessional education into an orthopedic residency pro-gram for CIS teaching and assessment. We sought to (1) deter-mine the impact of an interprofessional CPC workshop onorthopedic surgery residents’ CIS, (2) determine the impact ofphysician alone or incorporation of nursing participation in theworkshop, and (3) incorporate SPs in resident training andassessment of CIS.
METHODS
Study Design
This study was a pre–post two-group randomized study evalu-ating the impact of a CPC workshop on orthopedic surgeryresidents’ CIS.
Human Subjects
The study was granted an exempt status by the Scott and WhiteInstitutional Review Board. Before the workshop, study partic-ipants received information describing the study details andvoluntary involvement. Participant information was de-identi-fied, and results were saved in a secure locked environment,only accessible to the research team.
Participants
Eighteen residents of the Orthopaedic Surgery Residency Pro-gram were stratified based on training year to one of two CPCworkshop groups. Group A (n � 9) attended a CPC workshopwith only fellow residents, while group B (n � 9) attended a CPCworkshop with nurses included as participants. Nine nurses wererecruited from SWMH electronic news distribution. Registerednurses who had not previously participated in a healthcare com-munication workshop were eligible to participate.
Clinician–Patient Communication Workshop
The CPC workshop was 4 hours in duration and includeddidactic discussion, small group and simulated scenarios withSPs. Due to time constraints, both workshops were conductedin 1 day with group A as a morning session and group B anafternoon session. The workshops were led by trained CPCfaculty (A.F. and K.W.) who conduct the workshop on a regu-lar basis. The activities took place at a simulation center, mod-eled as a state-of-the-art “mini hospital,” including a Standard-ized Patient Clinic.
Standardized Patient Scenarios
Six orthopedic-focus simulation scenarios were developed forresident assessment. The scenarios were developed by an ortho-pedic surgeon (M.R.) and a medical educator experienced in SPmethodology (H.W.J.) using an SP case scenario template pro-vided by the Scott and White Standardized Patient Program.Case content included case objectives, summary, setting, SPrecruitment specifications, SP presentation during the encoun-ter, chief complaint/opening statement, current and past med-ical history, family history, social-personal profile, and state-ments/questions/responses to be stated verbatim. The scenarioswere 10 minutes in duration. The 3 scenarios used at baselinewere pelvic metastases, knee pain, and intoeing. The 3 scenariosused at follow-up were end of life, back pain, and ulna fracture.The cases were similar in difficulty and type. The cases wererandomized for utilization during pre- and post-assessment.Additionally, the order of the SP encounters was randomizedand the residents participated in the encounters in the standard-ized order. CPC workshop scenarios with SPs were utilized forthe workshop simulations. The scenarios were prepiloted withthe research team and with SPs before utilization in the study.SPs were trained to accurately and reliably portray the cases byan SP educator of the Scott and White Standardized Patient
96 Journal of Surgical Education • Volume 70/Number 1 • January/February 2013
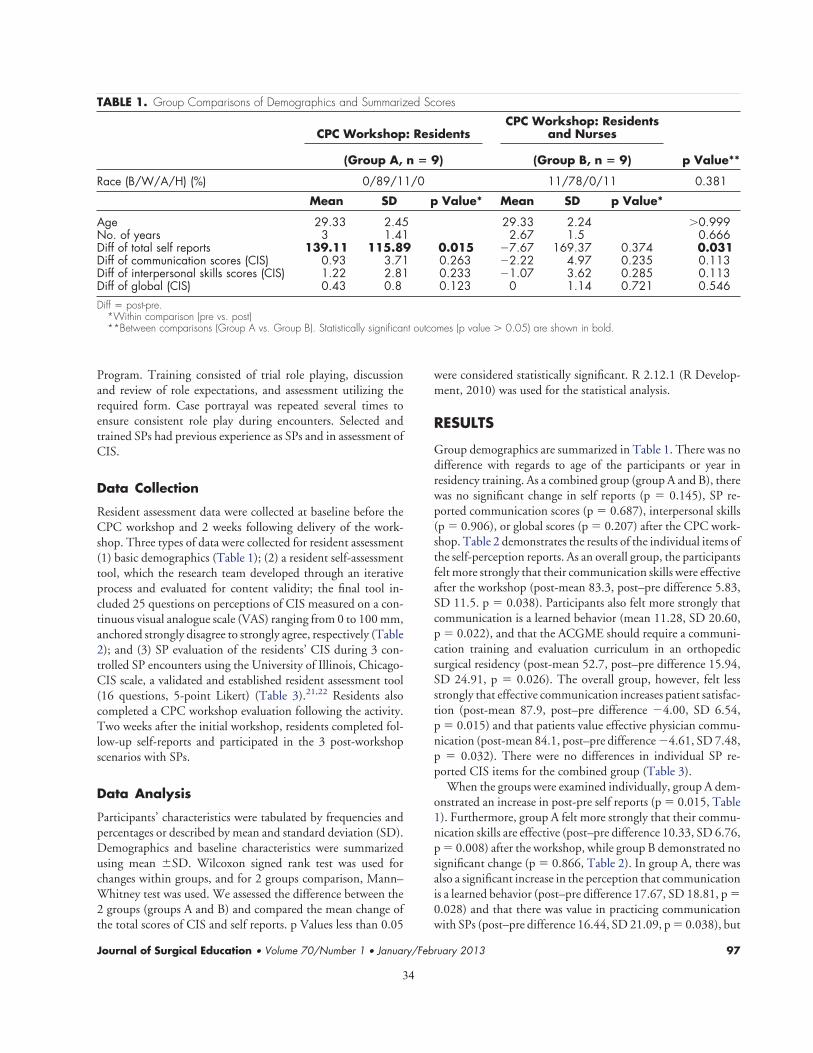
34
Program. Training consisted of trial role playing, discussionand review of role expectations, and assessment utilizing therequired form. Case portrayal was repeated several times toensure consistent role play during encounters. Selected andtrained SPs had previous experience as SPs and in assessment ofCIS.
Data Collection
Resident assessment data were collected at baseline before theCPC workshop and 2 weeks following delivery of the work-shop. Three types of data were collected for resident assessment(1) basic demographics (Table 1); (2) a resident self-assessmenttool, which the research team developed through an iterativeprocess and evaluated for content validity; the final tool in-cluded 25 questions on perceptions of CIS measured on a con-tinuous visual analogue scale (VAS) ranging from 0 to 100 mm,anchored strongly disagree to strongly agree, respectively (Table2); and (3) SP evaluation of the residents’ CIS during 3 con-trolled SP encounters using the University of Illinois, Chicago-CIS scale, a validated and established resident assessment tool(16 questions, 5-point Likert) (Table 3).21,22 Residents alsocompleted a CPC workshop evaluation following the activity.Two weeks after the initial workshop, residents completed fol-low-up self-reports and participated in the 3 post-workshopscenarios with SPs.
Data Analysis
Participants’ characteristics were tabulated by frequencies andpercentages or described by mean and standard deviation (SD).Demographics and baseline characteristics were summarizedusing mean �SD. Wilcoxon signed rank test was used forchanges within groups, and for 2 groups comparison, Mann–Whitney test was used. We assessed the difference between the2 groups (groups A and B) and compared the mean change ofthe total scores of CIS and self reports. p Values less than 0.05
were considered statistically significant. R 2.12.1 (R Develop-ment, 2010) was used for the statistical analysis.
RESULTS
Group demographics are summarized in Table 1. There was nodifference with regards to age of the participants or year inresidency training. As a combined group (group A and B), therewas no significant change in self reports (p � 0.145), SP re-ported communication scores (p � 0.687), interpersonal skills(p � 0.906), or global scores (p � 0.207) after the CPC work-shop. Table 2 demonstrates the results of the individual items ofthe self-perception reports. As an overall group, the participantsfelt more strongly that their communication skills were effectiveafter the workshop (post-mean 83.3, post–pre difference 5.83,SD 11.5. p � 0.038). Participants also felt more strongly thatcommunication is a learned behavior (mean 11.28, SD 20.60,p � 0.022), and that the ACGME should require a communi-cation training and evaluation curriculum in an orthopedicsurgical residency (post-mean 52.7, post–pre difference 15.94,SD 24.91, p � 0.026). The overall group, however, felt lessstrongly that effective communication increases patient satisfac-tion (post-mean 87.9, post–pre difference �4.00, SD 6.54,p � 0.015) and that patients value effective physician commu-nication (post-mean 84.1, post–pre difference �4.61, SD 7.48,p � 0.032). There were no differences in individual SP re-ported CIS items for the combined group (Table 3).
When the groups were examined individually, group A dem-onstrated an increase in post-pre self reports (p � 0.015, Table1). Furthermore, group A felt more strongly that their commu-nication skills are effective (post–pre difference 10.33, SD 6.76,p � 0.008) after the workshop, while group B demonstrated nosignificant change (p � 0.866, Table 2). In group A, there wasalso a significant increase in the perception that communicationis a learned behavior (post–pre difference 17.67, SD 18.81, p �0.028) and that there was value in practicing communicationwith SPs (post–pre difference 16.44, SD 21.09, p � 0.038), but
TABLE 1. Group Comparisons of Demographics and Summarized Scores
CPC Workshop: ResidentsCPC Workshop: Residents
and Nurses
p Value**(Group A, n � 9) (Group B, n � 9)
Race (B/W/A/H) (%) 0/89/11/0 11/78/0/11 0.381
Mean SD p Value* Mean SD p Value*
Age 29.33 2.45 29.33 2.24 �0.999No. of years 3 1.41 2.67 1.5 0.666Diff of total self reports 139.11 115.89 0.015 �7.67 169.37 0.374 0.031Diff of communication scores (CIS) 0.93 3.71 0.263 �2.22 4.97 0.235 0.113Diff of interpersonal skills scores (CIS) 1.22 2.81 0.233 �1.07 3.62 0.285 0.113Diff of global (CIS) 0.43 0.8 0.123 0 1.14 0.721 0.546Diff � post-pre.
*Within comparison (pre vs. post)**Between comparisons (Group A vs. Group B). Statistically significant outcomes (p value � 0.05) are shown in bold.
Journal of Surgical Education • Volume 70/Number 1 • January/February 2013 97

35
TABLE 2. Group Comparisons on Difference of Individual Scales of Self-Perception Reports
Overall Group A Group B
PreMean
PostMean Diff
pValue*
Premean
Postmean Diff
pValue*
Premean
Postmean Diff
pValue*
pValue**
I have a strong awareness of theimportance of effectiveclinician–patientcommunication.
83.6 85.1 1.5 �0.999 82.7 87.6 4.89 0.635 84.4 82.6 �1.89 0.634 0.452
I have experienced high-stresssituations requiring effectivecommunication skills.
84.3 84.2 �0.11 0.827 80.8 86.9 6.11 0.138 87.8 81.4 �6.33 0.038 0.034
Effective communication topatients is vital to being agood surgeon.
88 86.4 �1.61 0.121 88.1 88.4 0.33 0.593 87.9 84.3 �3.56 0.109 0.825
My communication skills withpatients are effective.
77.4 83.3 5.83 0.038 72.4 82.8 10.33 0.008 82.4 83.8 1.33 0.866 0.07
Effective communication skillspositively impact patient safety.
84.4 84.3 �0.17 0.965 83.8 85.2 1.44 0.515 85.1 83.3 �1.78 0.44 0.269
There is value in practicingcommunications skills withstandardized patients.
43.7 51.3 7.61 0.117 42.9 59.3 16.44 0.038 44.6 43.3 �1.22 0.953 0.133
I am confident applying effectivecommunication skills withpatients’ family members.
77.5 83.7 6.17 0.114 74.3 84.3 10 0.068 80.7 83 2.33 0.726 0.25
Effective communication withpatients is more difficult inhigh-stress situations.
77.8 83.7 5.94 0.151 83.4 88.9 5.44 0.635 72.1 78.6 6.44 0.26 0.724
Communication skills are alearned behavior.
61.8 73.1 11.28 0.022 65 82.7 17.67 0.028 58.6 63.4 4.89 0.343 0.232
I am willing to communicateeffectively with patients.
88.4 88.3 �0.17 0.924 87.7 89.3 1.67 0.373 89.2 87.2 �2 0.4 0.269
There is value in practicingcommunications skills withnurses.
70.3 70.9 0.56 0.879 80.7 83.3 2.67 0.514 60 58.4 �1.56 0.677 0.535
Effective communication skillsincrease patient satisfaction.
91.9 87.9 �4 0.015 90.2 88.4 �1.78 0.292 93.6 87.3 �6.22 0.02 0.425
I am confident applying effectivecommunication skills withpatients.
81.9 81.7 �0.22 0.711 80.1 86.4 6.33 0.123 83.7 76.9 �6.78 0.314 0.093
I enjoy communicating withpatients.
76.9 81.6 4.67 0.736 76.8 80.7 3.89 0.445 77 82.4 5.44 0.511 0.307
The ACGME should require acommunication training andevaluation curriculum inorthopedics surgical residency.
36.7 52.7 15.94 0.026 43.1 56.4 13.33 0.213 30.3 48.9 18.56 0.058 0.596
98
Journ
alo
fSu
rgica
lEduca
tion
•Volum
e70/N
umber
1•
January/February2013
TABLE 2. Continued.
Overall Group A Group B
PreMean
PostMean Diff
pValue*
Premean
Postmean Diff
pValue*
Premean
Postmean Diff
pValue*
pValue**
Effective communication skillsreduce the likelihood ofexposure to malpracticelitigation.
89.8 87.3 �2.5 0.176 89.1 88 �1.11 0.593 90.4 86.6 �3.89 0.172 0.593
My nurse-physiciancommunication during high-stress situations is effective.
78.3 82.1 3.72 0.66 79 80.6 1.56 0.888 77.7 83.6 5.89 0.483 0.86
I find professional satisfaction incommunicating effectively withpatients.
78.2 82.7 4.5 0.636 74.8 81.9 7.11 0.141 81.7 83.6 1.89 0.514 0.047
Clinician–patient communicationworkshops are an effectivemethod for communicationskills training.
48.9 59.7 10.72 0.053 54.3 69.4 15.11 0.051 43.6 49.9 6.33 0.514 0.31
Effective communication skillspositively impact patient care.
84.3 82.6 �1.72 0.948 80.8 84.9 4.11 0.155 87.8 80.2 �7.56 0.154 0.084
Patients’ family members valueeffective physiciancommunication.
85.2 85.8 0.56 0.501 83.7 88.2 4.56 0.155 86.8 83.3 �3.44 0.553 0.144
I am willing to enhance mycommunication skills withpatients.
86.4 83.7 �2.67 0.325 85.7 87.8 2.11 0.396 87.1 79.7 �7.44 0.049 0.057
Effective communication skillsincrease clinician satisfaction.
82.4 84 1.61 �0.999 80.9 86.1 5.22 0.44 83.9 81.9 �2 0.362 0.216
My communication skills withpatients’ family members areeffective.
80.7 83.6 2.89 0.448 79.2 85 5.78 0.327 82.1 82.1 0 0.953 0.479
Patients value effective physiciancommunication.
88.7 84.1 -4.61 0.032 89.1 85 �4.11 0.086 88.3 83.2 �5.11 0.175 0.894
Statistically significant outcomes (p-value � 0.05) are shown in bold.*Post-pre difference within comparison.**Between comparisons (group A vs. group B).
Journ
alo
fSu
rgica
lEduca
tion
•Volum
e70/N
umber
1•
January/February2013
99

36
TABLE 3. Group Comparisons on Difference of Individual Items of Standardized Patients’ Evaluations
Overall Group A Group B
PreMean
PostMean
Post–PreDiff
pValue*
PreMean
PostMean
Post–PreDiff
pValue*
PreMean
PostMean
Post–PreDiff
pValue*
pValue**
I felt you were telling meeverything; being truthful, upfront, and frank; not keepingthings from me.
4.6 4.5 �0.06 0.614 4.7 4.6 �0.04 0.705 4.5 4.4 �0.07 0.763 0.963
I felt like you discussed withme my options.
4.3 4.1 �0.19 0.289 4.4 4.4 0.07 0.719 4.3 3.8 �0.44 0.15 0.104
I felt you made sure that Iunderstood those options.
4.3 4 �0.3 0.085 4.4 4.3 �0.11 0.518 4.1 3.7 �0.48 0.119 0.303
I felt you asked my opinion,allowing me to make myown decision.
4 4 0.04 0.943 3.9 4.3 0.41 0.159 4 3.7 �0.33 0.311 0.1
I felt you encouraged me toask questions.
4.2 4.3 0.06 �0.999 4.4 4.5 0.11 0.461 4.1 4.1 0 0.73 0.682
I felt you answered myquestions, never avoidingthem.
4.5 4.4 �0.11 0.375 4.6 4.6 0.04 0.705 4.4 4.2 �0.26 0.202 0.161
I felt you clearly explainedwhat I needed to knowabout my problem; how andwhy it occurred.
4.2 4.1 �0.13 0.497 4.3 4.4 0.15 0.606 4.1 3.7 �0.41 0.234 0.128
I felt you clearly explainedwhat I should expect next.
4.3 4.3 0.04 0.726 4.3 4.6 0.3 0.194 4.2 4 �0.22 0.478 0.192
I felt you greeted me warmlyupon entering the room.
4.7 4.6 �0.06 0.426 4.7 4.7 0 �0.999 4.7 4.6 �0.11 0.332 0.154
I felt you were friendlythroughout the encounter.You were never crabby orrude to me.
4.7 4.6 �0.11 0.259 4.6 4.7 0.11 0.461 4.7 4.4 �0.33 0.058 0.105
I felt that you treated me likewe were on the same level.You never “talked down” tome or treated me like achild.
4.5 4.5 �0.02 0.793 4.4 4.6 0.15 0.472 4.6 4.4 �0.19 0.436 0.277
I felt you let me tell my storyand were careful not tointerrupt me while I wasspeaking.
4.6 4.6 0.09 0.305 4.5 4.7 0.19 0.157 4.6 4.6 0 �0.999 0.243
I felt you showed interest in meas a “person.” You neveracted bored or ignored whatI had to say.
4.5 4.5 0 0.949 4.6 4.7 0.07 0.666 4.5 4.4 �0.07 0.864 0.418
100
Journ
alo
fSu
rgica
lEduca
tion
•Volum
e70/N
umber
1•
January/February2013
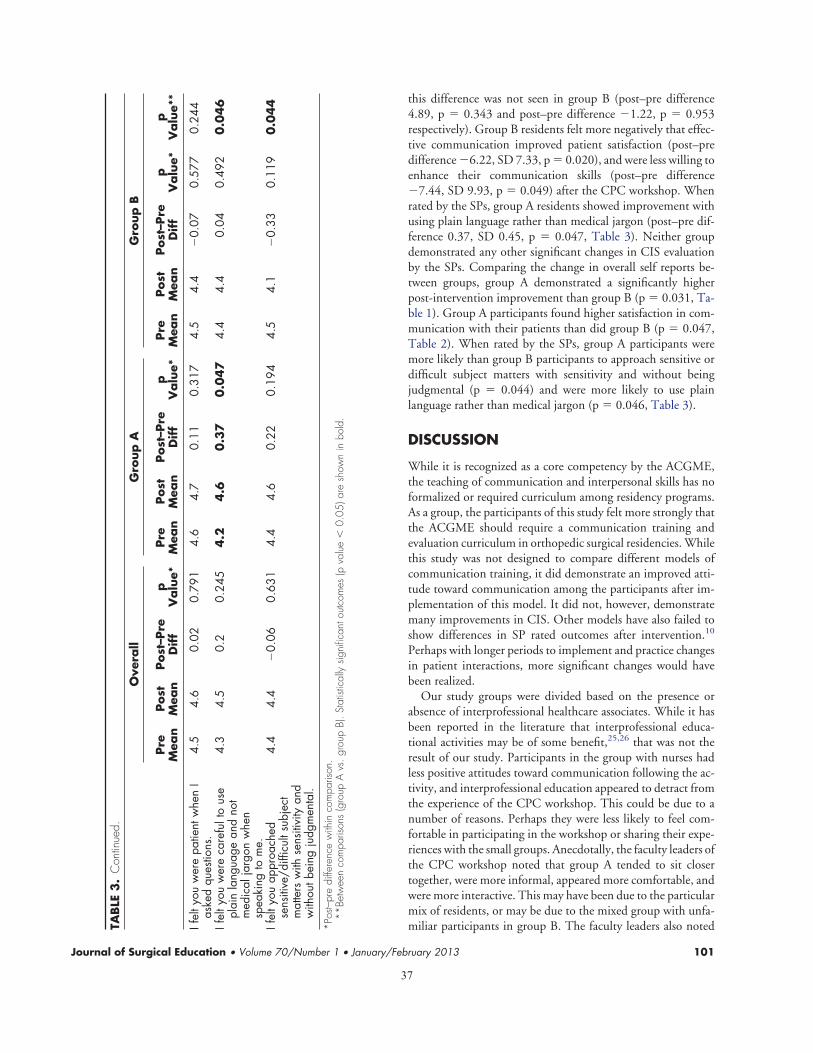
37
this difference was not seen in group B (post–pre difference4.89, p � 0.343 and post–pre difference �1.22, p � 0.953respectively). Group B residents felt more negatively that effec-tive communication improved patient satisfaction (post–predifference �6.22, SD 7.33, p � 0.020), and were less willing toenhance their communication skills (post–pre difference�7.44, SD 9.93, p � 0.049) after the CPC workshop. Whenrated by the SPs, group A residents showed improvement withusing plain language rather than medical jargon (post–pre dif-ference 0.37, SD 0.45, p � 0.047, Table 3). Neither groupdemonstrated any other significant changes in CIS evaluationby the SPs. Comparing the change in overall self reports be-tween groups, group A demonstrated a significantly higherpost-intervention improvement than group B (p � 0.031, Ta-ble 1). Group A participants found higher satisfaction in com-munication with their patients than did group B (p � 0.047,Table 2). When rated by the SPs, group A participants weremore likely than group B participants to approach sensitive ordifficult subject matters with sensitivity and without beingjudgmental (p � 0.044) and were more likely to use plainlanguage rather than medical jargon (p � 0.046, Table 3).
DISCUSSION
While it is recognized as a core competency by the ACGME,the teaching of communication and interpersonal skills has noformalized or required curriculum among residency programs.As a group, the participants of this study felt more strongly thatthe ACGME should require a communication training andevaluation curriculum in orthopedic surgical residencies. Whilethis study was not designed to compare different models ofcommunication training, it did demonstrate an improved atti-tude toward communication among the participants after im-plementation of this model. It did not, however, demonstratemany improvements in CIS. Other models have also failed toshow differences in SP rated outcomes after intervention.10
Perhaps with longer periods to implement and practice changesin patient interactions, more significant changes would havebeen realized.
Our study groups were divided based on the presence orabsence of interprofessional healthcare associates. While it hasbeen reported in the literature that interprofessional educa-tional activities may be of some benefit,25,26 that was not theresult of our study. Participants in the group with nurses hadless positive attitudes toward communication following the ac-tivity, and interprofessional education appeared to detract fromthe experience of the CPC workshop. This could be due to anumber of reasons. Perhaps they were less likely to feel com-fortable in participating in the workshop or sharing their expe-riences with the small groups. Anecdotally, the faculty leaders ofthe CPC workshop noted that group A tended to sit closertogether, were more informal, appeared more comfortable, andwere more interactive. This may have been due to the particularmix of residents, or may be due to the mixed group with unfa-miliar participants in group B. The faculty leaders also notedTA
BLE
3.
Con
tinue
d.
Ove
rall
Gro
up
AG
roup
B
Pre
Mea
nPost
Mea
nPost
–Pre
Dif
fp
Valu
e*Pre
Mea
nPost
Mea
nPost
–Pre
Dif
fp
Valu
e*Pre
Mea
nPost
Mea
nPost
–Pre
Dif
fp
Valu
e*p
Valu
e**
Ifel
tyou
wer
epa
tient
whe
nI
aske
dqu
estio
ns.
4.5
4.6
0.02
0.79
14.
64.
70.
110.
317
4.5
4.4
�0.
070.
577
0.24
4
Ifel
tyou
wer
eca
refu
lto
use
plai
nla
ngua
gean
dno
tm
edic
alja
rgon
whe
nsp
eaki
ngto
me.
4.3
4.5
0.2
0.24
54
.24
.60
.37
0.0
47
4.4
4.4
0.04
0.49
20
.04
6
Ifel
tyou
appr
oach
edse
nsiti
ve/d
ifficu
ltsu
bjec
tm
atte
rsw
ithse
nsiti
vity
and
with
outb
eing
judg
men
tal.
4.4
4.4
�0.
060.
631
4.4
4.6
0.22
0.19
44.
54.
1�
0.33
0.11
90
.04
4
*Pos
t–pr
edi
ffere
nce
with
inco
mpa
rison
.**
Betw
een
com
paris
ons
(gro
upA
vs.
grou
pB)
.St
atist
ical
lysig
nific
anto
utco
mes
(pva
lue
�0.
05)a
resh
own
inbo
ld.
Journal of Surgical Education • Volume 70/Number 1 • January/February 2013 101

38
that there were some interprofessional differences in opinionand philosophy that created some tension in group B, whichthey felt impacted the quality of the workshop. Faculty ob-served that group B residents were much less interactive andappeared uncomfortable. Results in the literature to this pointhave been somewhat mixed on the effectiveness of interprofes-sional education,25,26 and this study points out that furtherresearch into this subject is warranted to elucidate some of thevariables associated with interprofessional education. One ob-jective of this study was to incorporate SPs into the training andassessment of CIS. Group A residents found the addition of SPsvaluable, and the SPs were able to provide some valuable feed-back on participant performance. It is unclear as to why groupB residents found less value in the addition of SPs, although thismay also be related to interprofessional aspect of their CPC.While there was no detectable documented change in overallperformance, the SPs were able to document some specific im-provements in the interpersonal skills area. The SPs also simu-lated high stress and sensitive situations that are sometimesencountered, which allowed for teaching and evaluation inthese settings without involving a vulnerable patient or familymember. The addition of SPs to a communication workshopwas seen as a beneficial and valuable addition to the CPCworkshop, which traditionally involves workshop partici-pants role-playing.
There are several limitations to this study, one being smallsample size. Small group dynamics could certainly play a role inthe overall attitude towards the workshop. Another potentialconfounder is the timing of the CPC workshop. Group A wasperformed in the morning, while group B attended the work-shop in the afternoon. The workshop faculty noted that groupB was more frequently interrupted by pagers and other clinicalresponsibilities. Fatigue and general attitudes toward the work-shop may have been influenced by the time of day as well.Additionally, ceiling effects may have contributed to the lack ofpost–pre changes noted by the positive baseline responses mea-sured by both assessment tools. CIS is considered an importantfacet of resident education, and there have been considerablymore resources and thought given to teaching and evaluation inthis arena. Although interprofessional communication is an im-portant area of clinical communication, we found that inter-professional involvement in this CPC workshop detracted fromthe overall attitude toward communication and the willingnessto continue to improve in CIS. This type of educational expe-rience, which is heavily founded on interaction and designed toimprove awareness and communication skills essential for clin-ical practice,24 may be best accomplished with participants whoare already comfortable with one another and are comfortablesharing their thoughts and experiences. Other models may lendthemselves better to interprofessional involvement. The addi-tion of SPs to this curriculum is seen as beneficial for a numberof reasons, as discussed above. The obvious deterrence to im-plementing a communication workshop complete with SPs in-cludes cost, time, and planning that must be invested in such aprogram. With effective communication being linked to im-
proved patient satisfaction and decreased litigation, the ques-tion remains to be answered if the investment in a formal com-munication curriculum would lead to improved outcomes inthese areas.
ACKNOWLEDGMENTS
This work was generously supported by an OMeGA MedicalGrants Association Core Competency Innovation grant no.716. The authors thank the Scott and White Standardized Pa-tient Program for training the SPs, and the Temple CollegeClinical Simulation Center for providing the facilities. Theyalso thank Mr. Glen Cyer for publication editorial assistance.
REFERENCES
1. Accreditation Council for Graduate Medical Education.ACGME Outcome Project; 2007. Available at: http://www.acgme.org/outcome/comp/compFull.asp. Accessed2011.
2. Schirmer JM, Mauksch L, Lang F, et al. Assessing com-munication competence: A review of current tools. FamMed. 2005;37:184-192.
3. Teutsch C. Patient-doctor communication. Med ClinNorth Am. 2003;87:1115-1145.
4. Chan DK, Gallagher TH, Reznick R, Levinson W. Howsurgeons disclose medical errors to patients: a study usingstandardized patients. Surgery. 2005;138:851-858.
5. Lefevre FV, Waters TM, Budetti PP. A survey of physi-cian training programs in risk management and commu-nication skills for malpractice prevention. J Law Med Eth-ics. 2000;28:258-266.
6. General Competencies A and Outcomes assessment fordesignated institutional officials. Available at: http://www.acgme.org/acWebsite/irc/irc_competencies.asp. Accessed 2011.
7. ACGME. General competency requirements effectiveJuly 1, 2002. Memorandum from Cynthia Taradejna todesignated institutional officals, institutional administra-tors, and members of institutional GMECs. Feb. 2002;6
8. Hassett JM, Zinnerstrom K, Nawotniak RH, Schimpf-hauser F, Dayton MT. Utilization of standardized pa-tients to evaluate clinical and interpersonal skills of surgi-cal residents. Surgery. 2006;140:633-639.
9. Frey K, Edwards F, Altman K, Spahr N, Gorman RS. The“collaborative Care” curriculum: an educational modeladdressing key ACGME core competencies in primarycare residency training. Med Educ. 2003;37:786-789.
10. Hulsman RL, Ros WJ, Winnubst JA, Bensing JM. Teach-ing clinically experienced physicians communication
102 Journal of Surgical Education • Volume 70/Number 1 • January/February 2013
39
skills. A review of evaluation studies. Med Educ. 1999;33:655-668.
11. Lurie SJ, Mooney CJ, Lyness JM. Measurement of thegeneral competencies of the accreditation council forgraduate medical education: a systematic review. AcadMed. 2009;84:301-309.
12. Hobgood CD, Riviello RJ, Jouriles N, Hamilton G. As-sessment of communication and interpersonal skills com-petencies. Acad Emerg Med. 2002;9:1257-1269.
13. Shayne P, Gallahue F, Rinnert S, et al. Reliability of a corecompetency checklist assessment in the emergency depart-ment: the standardized direct observation assessment tool.Acad Emerg Med. 2006;13:727-732.
14. McLaughlin K, Gregor L, Jones A, Coderre S. Can Stan-dardized patients replace physicians as OSCE examiners?BMC Med Educ. 2006;6:12.
15. Donnelly MB, Sloan D, Plymale M, et al. Assessment ofresidents’ interpersonal skills by faculty proctors and stan-dardized patients: a psychometric analysis. Acad Med.2000;75:S93-S95.
16. Moulton CA, Tabak D, Kneebone R, et al. Teachingcommunication skills using the integrated procedural per-formance instrument (IPPI): a randomized controlledtrial. Am J Surg. 2009;197:113-118.
17. Rinker B, Donnelly M, Vasconez HC. Teaching patientselection in aesthetic surgery: use of the standardized pa-tient. Ann Plast Surg. 2008;61:127-131.
18. Yudkowsky R, Alseidi A, Cintron J. Beyond fulfilling thecore competencies: an objective structured clinical exam-ination to assess communication and interpersonal skillsin a surgical residency. Curr Surg. 2004;61:499-503.
19. Yudkowsky R, Downing SM, Sandlow LJ. Developing aninstitution-based assessment of resident communicationand interpersonal skills. Acad Med. 2006;81:1115-1122.
20. Sloan DA, Donnelly MB, Schwartz RW, Strodel WE.The objective structured clinical Examination. The newgold standard for evaluating postgraduate clinical perfor-mance. Ann Surg. 1995;222:735-742.
21. Epstein RM, Hundert EM. Defining and assessing profes-sional competence. JAMA. 2002;287:226-235.
22. Colliver JA, Swartz MH. Assessing clinical performancewith standardized patients. JAMA. 1997;278:790-791.
23. Accreditation Council for Graduate Medical Education.ACGME Outcome Project; 2007. Available at: http://www.acgme.org/Outcome/assess/ToolTable.pdf. Access-ed 2011.
24. Institute of Healthcare Communication Patient-CenteredCommunication Series: clinician–patient communica-tion to enhance health outcomes workshop. Available at:http://healthcarecomm.org/wp-content/uploads/2011/05/CPC-workshop-overview1.pdf. Accessed December 14,2011.
25. Zwarenstein M, Bryant W. Interventions to promote col-laboration between nurses and doctors. Cochrane Data-base Syst Rev. 2000; issue 2;Art No. CD000072. Availableat: http://DOI:10.1002/14651858.CD000072. Accessed2011.
26. Reeves S, Zwarenstein M, Goldman J, et al. Interpro-fessional education: effects on professional practice andhealth care outcomes. Cochrane Database Syst Rev.2008;issue 1;Art No.CD002213. Available at: http://DOI:10.1002/14651858.CD002213.pub2. Accessed 2011.
Journal of Surgical Education • Volume 70/Number 1 • January/February 2013 103
40
Hemoglobin Trends after Primary Total Hip and Knee Arthroplasty: Are Daily Post-Operative Hemoglobin
Phlebotomies Necessary?Kushal Patel, M.D.
INTRODUCTION:Common practice is daily post-operative hemoglobin level evaluation in patients undergoing primary total arthroplasty of the hip (THA) and knee (TKA). Frequently, no specific action is taken secondary to these lab results. Our study examined post-operative hemoglobin trends in primary joint arthroplasty pa-tients. We hypothesize that post-operative hemoglobin values do not drop significantly enough to warrant daily phlebotomy in many patients and thereby, improve patient satisfaction and reduce costs.
METHODS:Retrospective review of patients who underwent primary THA and TKA from 2009 to 2011. Data col-lected included laterality, age, gender, intra-operative estimated blood loss, body mass index, pre-opera-tive hemoglobin level, and post-operative hemoglobin level 0-8, 8-24, 24-48, and 48–72 hours post-oper-ative. Patients who underwent conversion to total joint arthroplasty were excluded.
RESULTS:A total of 1929 [One thousand nine hundred and twenty-nine] patients (497 (25.7%) THA and 1433 (74.3%) TKA) were included. Bilateral TKA accounted for 227 of 1433 TKA patients. Mean abso-lute drop in hemoglobin from pre-operative levels at 0-8, 8-24, 24-48 and 48-72 hours post-operative were, for unilateral TKA patients, -1.8±0.9, -2.4±1.0, -3.2±1.1, and -3.5±1.2; for bilateral TKA patients, -2.4±0.8, -2.8±1.2, -3.9±1.2, and -4.4±1.5; and for THA patients, -2.4±1.0, -2.81±1.0, -3.5±1.1, and -4.1±1.8. In THA patients at 24 hours post-operative 173 (34.8%), 72 (14.5%), and 29 (5.8%) patients had hemoglobin values below 10.0, 9.0, and 8.0, respectively. Corresponding numbers in TKA patients were 320 (22.3%), 92 (6.4%), and 17(1.2%) patients.
DISCUSSION AND CONCLUSION:With projected rises in elective primary THA and TKA and greater focus on cost and patient satisfaction, daily phlebotomy for hemoglobin values is a potential area of improvement. Our study provides trends in hemoglobin after THA and TKA and questions whether examination of daily hemoglobin values is neces-sary. In the appropriately selected patient, phlebotomy draws to examine hemoglobin can be forgone especially in the early post-operative period.
Influence of Displacement and Treatment Methods on Patient Mortality after Femoral Neck Fracture 41
Influence of Displacement and Treatment Methods on Patient Mortality after Femoral Neck Fracture
Donavan K. Murphy, Timmothy Randell, Kindyle L. Brennan, Juhee Song, John M. Hamilton, Michael L. Brennan, and Robert A. Probe.
OBJECTIVES: To determine if femoral neck fractures (FNF) displacement and treatment selection influence pa-tient mortality.
DESIGN/SETTING: Retrospective review at Level I trauma center
PARTICIPANTS: 1788 individuals with FNFs treated at a single institution over 11 years
MEASUREMENTS: A review of patient records with low-energy fractures treated with Closed Reduction Mul-tiple Cannulated Screws (CRMCS), Hemiarthroplasty (HA), or Total Hip Arthroplasty (THA) were included. FNFs were classified as nondisplaced or displaced. Associations with treatment method, revision, age, comorbidities, and gender were examined.
RESULTS: There were 1474 patients, 371 (25.17%) male and 1103 (74.83%) female. Ages ranged from 60-106 (80.82) years. CRMCS, HA, and THA were performed on 766, 758, and 41 fractures, respectively. There were 1139 displaced fractures treated by CRMCS (363), HA (745), and THA (41) and 396 nondisplaced fractures treated by CRMCS (383), HA (13), and THA (0). Comparing displaced and nondisplaced fractures, no significant dif-ference in survival rate was found in any time interval except at 1 month; nondisplaced fractures demonstrated a statistically significant lower mortality rate (4.1%) comparing to displaced fractures (6.9%). When comparing mor-tality between treatment groups, mortality of those undergoing HA was higher than those undergoing CRMCS at all intervals; THA survival was longest. The hazard ratio for HA vs. CRMCS was 1.24, for age >80 versus 2.16 for ages 60-70, men compared with women was 1.55.
CONCLUSION: HA was associated with a higher mortality rate when compared to CRMCS and THA. Treatment selection and comorbid factors must be accounted for when contemplating treatment for FNFs. There is a need to further stratify this patient population and expand on the significance of all comorbid conditions.
INTRODUCTION
Femoral neck fracture is a devastating injury to the elderly, with overall mortality reported between 15-
30% within the first year after fracture.1-14 This health-care burden is carried not only by the patients and their families, but by our healthcare system as well. Ray et al. reported that in 1995 the United States devoted $13.8 billion in health care spending to treatment of osteopo-rotic fractures, with $8.7 billion going toward the treat-ment of hip fractures alone.15 While geriatric hip fracture incidence is decreasing,16 world-wide annual prevalence of femoral neck fractures is expected to increase from 1.26 million cases per year in 1990 to 4.5 million cases per year by 2050.17 Understanding factors associated with poor outcomes following surgical management of these fractures is increasingly important, given the expected rise in prevalence.
The majority of femoral neck fractures are treated sur-gically with internal fixation (IF), hemiarthroplasty (HA), or total hip arthroplasty (THA). The choice of optimal surgical treatment is currently controversial, with several investigators reporting superior clinical outcomes and
fewer complications following HA and THA, as com-pared to IF.18-24 Others, however, have suggested higher rates of mortality following arthroplasty as compared to internal fixation.7, 25
Although several prior studies have evaluated the im-pact of the mode of surgical treatment on outcomes and mortality rates, few have considered the impact of frac-ture displacement.24 The purpose of this study was to ret-rospectively compare overall mortality of displaced and nondisplaced femoral neck fractures after the primary surgical intervention among the three surgical treatments. Secondarily, we analyzed a) overall mortality after reop-eration surgery for each index procedure, b) mortality rates by age (decade) at time of surgery, c) mortality rates by gender, and d) we described the death associated co-morbidities.
METHODSThis study was approved by our institutional review
board. The medical record database at a level one trauma hospital was queried for diagnosis and treatment codes

Influence of Displacement and Treatment Methods on Patient Mortality after Femoral Neck Fracture 42
associated with femoral neck fracture between the years 1998 and 2009. The codes used were ICD9 - 820, CPT 27235, 27236, and 27132. The exclusion criteria were age less than 60 years, fracture secondary to high energy trauma, fracture secondary to neoplasia, extracapsular hip fracture, prior unrelated surgery to proximal femoral region, need for open reduction, or treatment other than closed reduction with IF, HA, or THA. The record search revealed 1788 patients meeting our criteria for chart re-view.
Data collected from the chart review included medi-cal record number (MRN), age/DOB, sex, surgery(s) performed with date of surgery, classification of femoral neck fracture as displaced or nondisplaced, and dates of the last contact or death note. Surgeries performed were further classified as right/left and primary/reoperation. Reoperation surgery was any surgery following the index procedure on the affected hip that met inclusion criteria. Patients’ death records were obtained from Texas Vital Statistics based on name, date of birth, and sex.
All radiographs and reports were reviewed by the same investigator (TR). Radiographs from 1998 to August 2002 were not stored digitally or readily available for review, thus the classification of these femoral neck frac-tures was established by review of fracture description by the operating orthopedic surgeon or radiological record. Picture archiving and communication system (PACS) was used for review of all patient films from August 2002 to 2011. Femoral neck fractures were classified as non-displaced or displaced. Fractures were considered non-displaced if they were identified as OTA 31B1.1-3. Frac-tures were considered displaced if they were 31B3.1-3 or 31B2.3. Based on the Garden classification, fractures were nondisplaced (types I-II) and displaced (types III-IV). The intergrader agreement for Garden Stages 1, 2, 3, and 4 fractures is reportedly low (kappa, 0.03-0.56) but high (kappa, 0.67-0.77) for nondisplaced (Garden Stages 1 and 2) and displaced (Garden Stages 3 and 4) fractures.26 A subset of radiographs was used to assess and ensure interobserver reliability with two board-certi-fied trauma surgeons and four chief residents. Consistent with previous reports, intergrader reliability was greater than 90% for nondisplaced and displaced fracture groups.
Those patients treated with multiple screws had reduc-tion achieved through closed means on a fracture table and implant placement as described by Probe et al.27 AS-NIS III (Stryker) 6.5mm cannulated screws were used on all patients with the decision to place three or four screws based on posterior comminution. In the vast majority of hemiarthroplasty cases, a modified Hardinge lateral ap-proach combined with a cemented modular stem was utilized. Total hip arthroplasty was also performed with a modified Hardinge lateral approach using a variety of
prosthetic components from different manufactures.
STATISTICAL ANALYSISDemographic data, injury and surgery types, and occur-
rence of reoperation were summarized using means and percentages, as appropriate.
Chi-squared tests/Fisher’s exact tests were used to com-pare surgery types between displaced and nondisplaced fractures. The ages at surgery were compared between fracture and surgery types using t-tests and ANOVA.
Kaplan-Meier estimates and Cox proportional hazards regression was used to examine a) mortality rates by frac-ture type (displaced vs. nondisplaced), b) mortality rates by surgery type, c) overall mortality after index procedure and reoperation surgery, d) mortality rates by age (de-cade) at time of surgery, e) mortality rates by operative year, and f) mortality rates by gender. In all cases where fracture type is a covariate, patients missing fracture class data were excluded from the analysis. In certain models we compared rates at 1 and 6 months and 1 and 2 years post operatively. We view this as exploratory analysis and do not apply a multiple test correction. We also carried out pairwise comparisons between groups in some cases where there are more than two strata (e.g., operative year). Tests were run at 5% significance (p≤0.05) in all cases. Additionally, we examined co-morbidity by recording the ICD-9 codes of those who died and calculating the num-ber of patients per code.
RESULTSICD-9 and CPT code searches resulted in 1788 identi-
fied patients. Following chart review and application of exclusions, there were a total of 1474 patients, with 1565 fractures: 371 (25.17%) were male and 1103 (74.83%) female (Figure 1). Ages ranged from 60-106 years; they were roughly normally distributed with a mean of 80.82
Figure 1. Chart review and application of exclusion
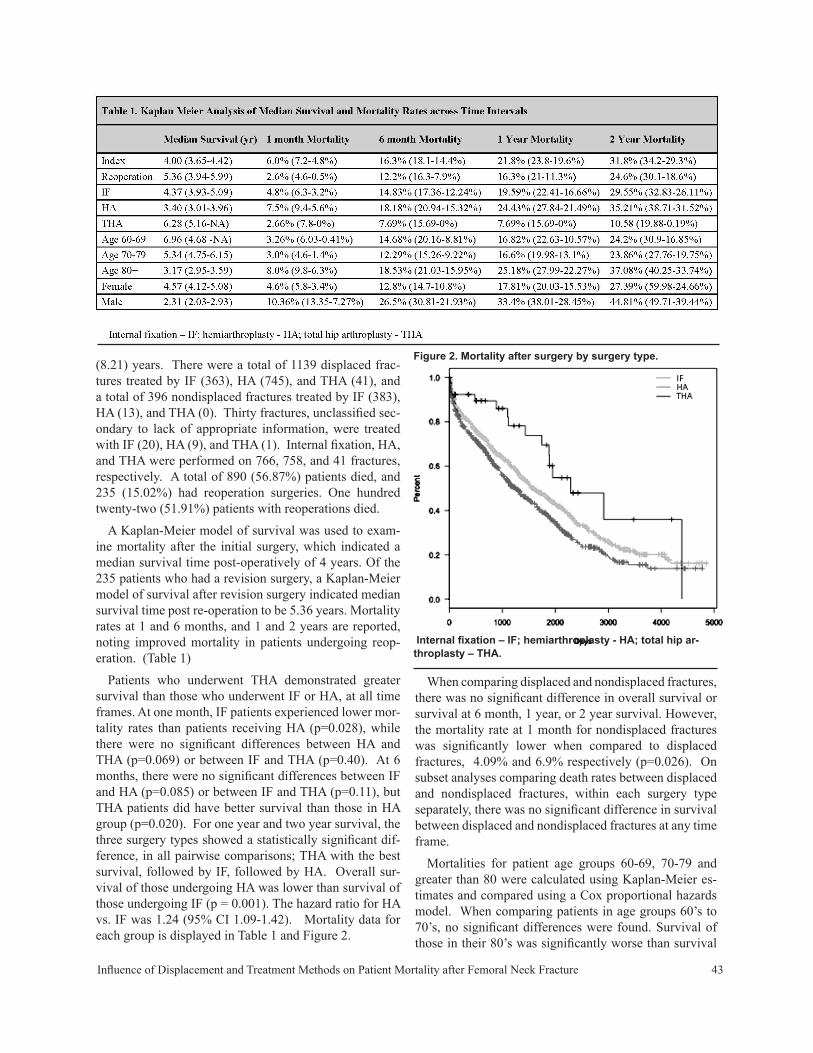
Influence of Displacement and Treatment Methods on Patient Mortality after Femoral Neck Fracture 43
(8.21) years. There were a total of 1139 displaced frac-tures treated by IF (363), HA (745), and THA (41), and a total of 396 nondisplaced fractures treated by IF (383), HA (13), and THA (0). Thirty fractures, unclassified sec-ondary to lack of appropriate information, were treated with IF (20), HA (9), and THA (1). Internal fixation, HA, and THA were performed on 766, 758, and 41 fractures, respectively. A total of 890 (56.87%) patients died, and 235 (15.02%) had reoperation surgeries. One hundred twenty-two (51.91%) patients with reoperations died.
A Kaplan-Meier model of survival was used to exam-ine mortality after the initial surgery, which indicated a median survival time post-operatively of 4 years. Of the 235 patients who had a revision surgery, a Kaplan-Meier model of survival after revision surgery indicated median survival time post re-operation to be 5.36 years. Mortality rates at 1 and 6 months, and 1 and 2 years are reported, noting improved mortality in patients undergoing reop-eration. (Table 1)
Patients who underwent THA demonstrated greater survival than those who underwent IF or HA, at all time frames. At one month, IF patients experienced lower mor-tality rates than patients receiving HA (p=0.028), while there were no significant differences between HA and THA (p=0.069) or between IF and THA (p=0.40). At 6 months, there were no significant differences between IF and HA (p=0.085) or between IF and THA (p=0.11), but THA patients did have better survival than those in HA group (p=0.020). For one year and two year survival, the three surgery types showed a statistically significant dif-ference, in all pairwise comparisons; THA with the best survival, followed by IF, followed by HA. Overall sur-vival of those undergoing HA was lower than survival of those undergoing IF (p = 0.001). The hazard ratio for HA vs. IF was 1.24 (95% CI 1.09-1.42). Mortality data for each group is displayed in Table 1 and Figure 2.
When comparing displaced and nondisplaced fractures, there was no significant difference in overall survival or survival at 6 month, 1 year, or 2 year survival. However, the mortality rate at 1 month for nondisplaced fractures was significantly lower when compared to displaced fractures, 4.09% and 6.9% respectively (p=0.026). On subset analyses comparing death rates between displaced and nondisplaced fractures, within each surgery type separately, there was no significant difference in survival between displaced and nondisplaced fractures at any time frame.
Mortalities for patient age groups 60-69, 70-79 and greater than 80 were calculated using Kaplan-Meier es-timates and compared using a Cox proportional hazards model. When comparing patients in age groups 60’s to 70’s, no significant differences were found. Survival of those in their 80’s was significantly worse than survival
Figure 2. Mortality after surgery by surgery type.
Internal fixation – IF; hemiarthroplasty - HA; total hip ar-throplasty – THA.
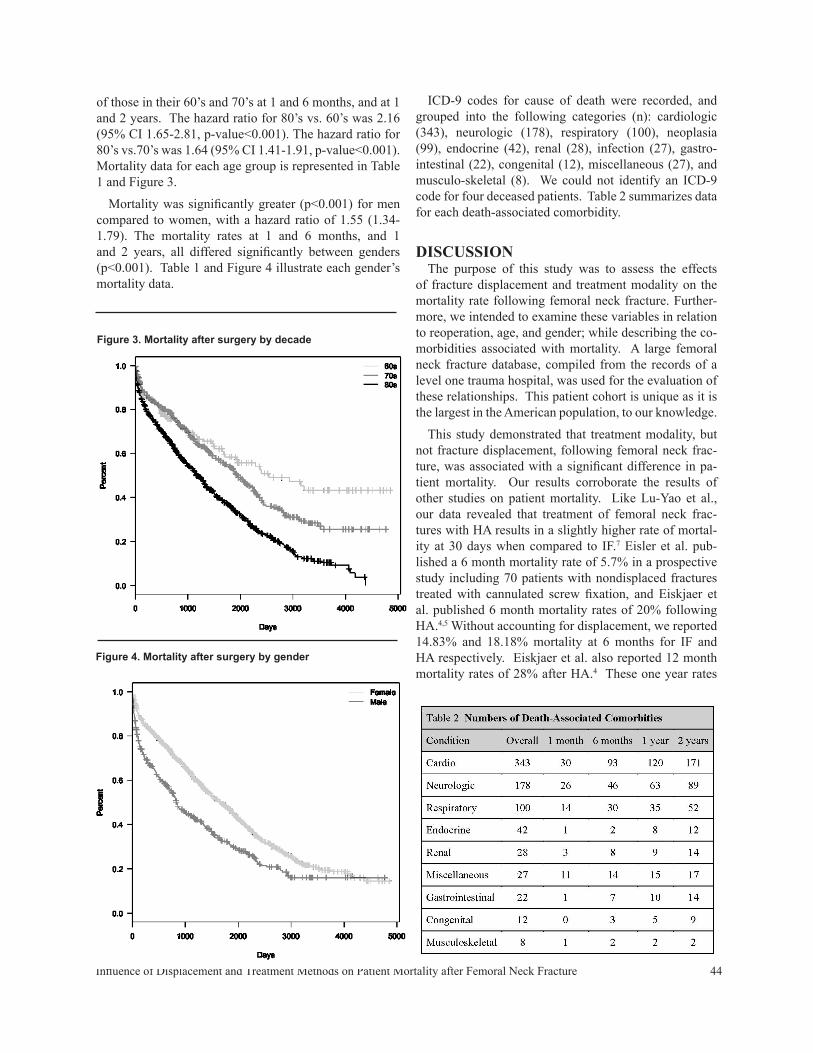
Influence of Displacement and Treatment Methods on Patient Mortality after Femoral Neck Fracture 44
of those in their 60’s and 70’s at 1 and 6 months, and at 1 and 2 years. The hazard ratio for 80’s vs. 60’s was 2.16 (95% CI 1.65-2.81, p-value<0.001). The hazard ratio for 80’s vs.70’s was 1.64 (95% CI 1.41-1.91, p-value<0.001). Mortality data for each age group is represented in Table 1 and Figure 3.
Mortality was significantly greater (p<0.001) for men compared to women, with a hazard ratio of 1.55 (1.34-1.79). The mortality rates at 1 and 6 months, and 1 and 2 years, all differed significantly between genders (p<0.001). Table 1 and Figure 4 illustrate each gender’s mortality data.
Figure 3. Mortality after surgery by decade
Figure 4. Mortality after surgery by gender
ICD-9 codes for cause of death were recorded, and grouped into the following categories (n): cardiologic (343), neurologic (178), respiratory (100), neoplasia (99), endocrine (42), renal (28), infection (27), gastro-intestinal (22), congenital (12), miscellaneous (27), and musculo-skeletal (8). We could not identify an ICD-9 code for four deceased patients. Table 2 summarizes data for each death-associated comorbidity.
DISCUSSIONThe purpose of this study was to assess the effects
of fracture displacement and treatment modality on the mortality rate following femoral neck fracture. Further-more, we intended to examine these variables in relation to reoperation, age, and gender; while describing the co-morbidities associated with mortality. A large femoral neck fracture database, compiled from the records of a level one trauma hospital, was used for the evaluation of these relationships. This patient cohort is unique as it is the largest in the American population, to our knowledge.
This study demonstrated that treatment modality, but not fracture displacement, following femoral neck frac-ture, was associated with a significant difference in pa-tient mortality. Our results corroborate the results of other studies on patient mortality. Like Lu-Yao et al., our data revealed that treatment of femoral neck frac-tures with HA results in a slightly higher rate of mortal-ity at 30 days when compared to IF.7 Eisler et al. pub-lished a 6 month mortality rate of 5.7% in a prospective study including 70 patients with nondisplaced fractures treated with cannulated screw fixation, and Eiskjaer et al. published 6 month mortality rates of 20% following HA.4,5 Without accounting for displacement, we reported 14.83% and 18.18% mortality at 6 months for IF and HA respectively. Eiskjaer et al. also reported 12 month mortality rates of 28% after HA.4 These one year rates

Influence of Displacement and Treatment Methods on Patient Mortality after Femoral Neck Fracture 45
are higher than those in other studies28-32, but consis-tent with our results (24.43% mortality at one year after HA). In our study, at each time interval of interest, HA showed a significantly increased mortality as compared to IF and THA. Mortality rate of THA was significantly better than other treatment options, possibly secondary to selection bias. A commonly recognized practice pattern is for the more active and healthier patients to more likely be considered for the more invasive THA. Other factors which could explain why HA patients have an increased mortality include: increased blood loss, anesthesia time, rehabilitation, and functional deficits. These factors were not examined in this study; leaving a number of question for future investigations.
Overall mortality following reoperation was slightly better than that following the index procedure. This too may be explained by a selection bias: healthier patients are likelier to be considered by surgeons to be capable of performing well following reoperation. Additionally, it is the healthier patients who are likely to survive to a point where reoperation is needed. When examining patients based on age by decade (60-69, 70-79, and greater that 80), we found that our patient population has an increased mortality rate as compared to data form the US Census, and that older patients have a statistically significantly in-creased mortality compared to younger patients. Using 2009 US Census data, mortality rates of people in their 60s, 70s, and 80s were 1.2%, 3.0%, and 9.5%, respec-tively.35 Using a Kaplan Meier estimate, death rates of our patient population were estimated at 16.1% for patients in their 60s, 15.9% for patients in their 70s, and 23.8% for patients in their 80s. While comparing the older patients in our study to younger patients, we found that there is an almost 10% difference at 1 year and 13% difference at 2 years between those greater than 80 and those younger. It appears that age greater than 80 provides some prog-nostic value when considering mortality. Our data also reiterates that men have increased mortality when com-pared to women; this has been previously shown in the literature.4,33,34
Aside from surgical intervention, other variables have been indicated for their role in mortality of patients with femoral neck fractures. Conditions such as renal disease, heart failure, cardiac ischemia, and neurologic impair-ment have been shown to increase mortality.4, 34, 36 The data reported here based on ICD-9 codes associated with patients’ death continues to reaffirm that mortality is de-pendent on patient comorbidity at the time of the injury and surgery. This data could only be used in a descriptive nature secondary to the method of collection, so rigorous statistical comparisons could not be performed. Future studies designed to analyze the role of comorbidities in the mortality rate of these cohorts are warranted.
This study does present limitations. The retrospective nature of this study, without randomization and blinding, does impart a possibility for a selection bias. The pa-tients’ treatments were selected based on the evaluation of the x-rays by each primary surgeon. Although indica-tions for surgery were largely the same for each surgeon, variability is unavoidable. Despite their choice of treat-ment, each fracture after 2002 was reviewed by a single grader and analyzed in its treatment group. Radiographs prior to 2002 were not available for review, so radio-logical reports and orthopedic surgeon descriptions were used to classify fractures. Although inter-grader reliabil-ity is reported high, this does break uniformity among data collected.
CONCLUSIONOur data illustrate the importance of treatment selec-
tion on patient mortality and also shed light on the fact that many of these patients have confounding conditions that may be increasing their mortality risk. Many factors must be accounted for when contemplating treatment for femoral neck fractures. Although noting a higher mortal-ity rate at each time interval with hemiarthroplasty, other studies on this patient population show the risk of com-plication and reoperation is greater with IF. All of this information should be taken into account. More research has to be done to further risk stratify this patient popula-tion and detail the significance of all comorbid conditions of a patient.
REFERENCES1. Aharonoff GB, Koval KJ, Skovron ML, Zuckerman JD. Hip
fractures in the elderly: predictors of one year mortality. J Orthop Trauma 1997;11: 162-5.
2. Craik RL. Disability following hip fracture. Phys Ther 1994;74: 387-98.
3. Dretakis E, Kritsikis N, Economou K, Christodoulou N. Bilat-eral non-contemporary fractures of the proximal femur. Acta Orthop Scand 1981;52: 227-9.
4. Eiskjaer S, Ostgård SE. Risk factors influencing mortality after bipolar hemiarthroplasty in the treatment of fracture of the femoral neck. Clin Orthop Relat Res 1991;(270): 295-300.
5. Eisler J, Cornwall R, Strauss E, Koval K, Sui A, Gilbert M. Outcomes of elderly patients with nondisplaced femoral neck fractures. Clin Orthop Relat Res 2002;(399): 52-8.
6. Koval KJ, Skovron ML, Aharonoff GB, Zuckerman JD. Predic-tors of functional recovery after hip fracture in the elderly. Clin Orthop Relat Res 1998;(348): 22-8.
7. Lu-Yao GL, Keller RB, Littenberg B, Wennberg JE. Outcomes after displaced fractures of the femoral neck. A meta-analysis of one hundred and six published reports. J Bone Joint Surg Am 1994;76: 15-25.
8. Magaziner J, Simonsick EM, Kashner TM, Hebel JR, Kensora JE. Survival experience of aged hip fracture patients. Am J Public Health 1989;79: 274-8.

Influence of Displacement and Treatment Methods on Patient Mortality after Femoral Neck Fracture 46
9. Michel JP, Hoffmeyer P, Klopfenstein C, Bruchez M, Grab B, d’Epinay CL. Prognosis of functional recovery 1 year after hip fracture: typical patient profiles through cluster analysis. J Gerontol A Biol Sci Med Sci 2000;55: M508-15.
10. Sikand M, Wenn R, Moran CG. Mortality following surgery for undisplaced intracapsular hip fractures. Injury 2004;35: 1015-9.
11. Stavrou ZP, Erginousakis DA, Loizides AA, Tzevelekos SA, Papagiannakos KJ. Mortality and rehabilitation following hip fracture. A study of 202 elderly patients. Acta Orthop Scand Suppl 1997;275: 89-91.
12. Svensson O, Strömberg L, Ohlén G, Lindgren U. Prediction of the outcome after hip fracture in elderly patients. J Bone Joint Surg Br 1996;78: 115-8.
13. Petersen MB, Jørgensen HL, Hansen K, Duus BR. Factors affecting postoperative mortality of patients with displaced femoral neck fracture. Injury 2006;37: 705-11.
14. Rodriguez J, Herrara A, Canales V, Serrano S. Epidemiologic factors, morbidity and mortality after femoral neck fractures in the elderly. A comparative study: internal fixation vs. hemiar-throplasty. Acta Orthop Belg 1987;53: 472-9.
15. Ray NF, Chan JK, Thamer M, Melton LJ 3rd. Medical expen-ditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Founda-tion. J Bone Miner Res 1997;12: 24-35.
16. Stevens JA, Rudd RA. Declining hip fracture rates in the United States. Age Ageing 2010;39; 500-3.
17. Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int 1997;7: 407-13.
18. Heetveld MJ, Rogmark C, Frihagen F, Keating J. Internal fixa-tion versus arthroplasty for displaced femoral neck fractures: what is the evidence? J Orthop Trauma 2009;23: 395-402.
19. Aleem IS, Karanicolas PJ, Bhandari M. Arthroplasty versus internal fixation of femoral neck fractures: a clinical decision analysis. Ortop Traumatol Rehabil 2009;11: 233-41.
20. Frihagen F, Nordsletten L, Madsen JE. Hemiarthroplasty or internal fixation for intracapsular displaced femoral neck frac-tures: randomised controlled trial. BMJ 2007;335: 1251-4.
21. Blomfeldt R, Törnkvist H, Ponzer S, Söderqvist A, Tidermark J. Displaced femoral neck fracture: comparison of primary total hip replacement with secondary replacement after failed internal fixation: a 2-year follow-up of 84 patients. Acta Orthop 2006;77: 638-43.
22. Bjørgul K, Reikerås O. Hemiarthroplasty in worst cases is bet-ter than internal fixation in best cases of displaced femoral neck fractures: a prospective study of 683 patients treated with hemi-arthroplasty or internal fixation. Acta Orthop 2006;77: 368-74.
23. Blomfeldt R, Törnkvist H, Ponzer S, Söderqvist A, Tidermark J. Comparison of internal fixation with total hip replacement for displaced femoral neck fractures. Randomized, controlled trial performed at four years. J Bone Joint Surg Am 2005;87: 1680-8.
24. Murphy DK, Randell T, Brennan KL, Probe RA, Brennan ML. Treatment and displacement affect the reoperation rate for femoral neck fracture. Clin Orthop Relat Res 2013;471: 2691-702.
25. Parker MJ, White A, Boyle A. Fixation versus hemiarthroplas-ty for undisplaced intracapsular hip fractures. Injury 2008;39: 791-5.
26. Frandsen PA, Anderson E, Madsen F, Skjodt T. Garden’s classification of femoral neck fractures: an assessment of inter-observer variation. J Bone Joint Surg Br 1988;70: 588-90.
27. Probe R, Ward R. Internal fixation of femoral neck fractures. J Am Acad Orthop Surg 2006;14: 565-71.
28. Parker MJ, Pryor G, Gurusamy K. Hemiarthroplasty versus in-ternal fixation for displaced intracapsular hip fractures: A long-term follow up of a randomised trial. Injury 2010;41: 370-3.
29. Blomfeldt R, Tornkvist H, Eriksson K, Söderqvist A, Ponzer S, Tidermark J. A randomised controlled trial comparing bipolar hemiarthroplasty with total hip replacement for displaced intracapsular fractures of the femoral neck in elderly patients. J Bone Joint Surg Br 2007;89: 160-5.
30. Ravikumar KJ, Marsh G. Internal fixation versus hemiarthro-plasty versus total hip arthroplasty for displaced subcapital fractures of femur – 13 year results of a prospective randomized study. Injury 2000;31: 793-7.
31. Rogmark C. Carlsson A. Johnell O. Sernbo I. A prospective randomised trial of internal fixation versus arthroplasty for dis-placed fractures of the neck of the femur. Functional outcome for 450 patients at two years. J Bone Joint Surg Br. 2002;84: 183-8.
32. Gjertsen JE, Vinje T, Engesaeter, Lie SA, Havelin LI, Furnes O, et al. Internal screw fixation compared with bipolar hemiar-throplasty for treatment of displaced femoral neck fractures in elderly patients. J Bone Joint Surg Am 2010;92: 619-28.
33. Dzupa V, Bartonícek J, Skála-Rosenbaum J, Príkazský V. Mortality in patients with proximal femoral fractures during the first year after the injury. Acta Chir Orthop Traumatol Cech 2002;69: 39-44.
34. Karagiannis A, Papakitsou E, Dretakis K, Galanos A, Megas P, Lambiris E, et al. Mortality rates of patients with a hip fracture in a southwestern district of Greece: ten-year follow-up with reference to the type of fracture. Calcif Tissue Int 2006;78: 72-7.
35. Kochanek KD, Xu J, Murphy SL, Mininõ AM, Kung H. Deaths: Final Data for 2009. National Vital Statistics Reports 2011;60(3) Available at http://www.cdc.gov/nchs/data/nvsr/nvsr60/nvsr60_03.pdf Accessed June 6 2013.
36. Tierney GS, Goulet JA, Greenfield ML, Port FK. Mortality after fracture of the hip in patients who have end-stage renal disease. J Bone Joint Surg Am 1994;76: 709-12.

47
DAVID FERGUSONDavid Ferguson, Bryce J Busenlehner; Mark D Rahm, Sachin M Mehta, Juhee Song, Matthew L Davis, H. Wayne Sampson, and Christopher Chaput. The use of routine thoracoabdominal CT Scans in the polytrauma patient to estimate obesity.
2012 Jun 18 [Epub ahead of print] PMID: 22705837 doi: 10.1038/oby.2012.163Podium presentation, Orthopaedic Research and Education Foundation (OREF/ORS) Central Texas Resident Research Symposium, UT Health Science Center, San Antonio, TX, December 10, 2010. Poster presentation, 27th Annual Meeting of the Orthopaedic Trauma Association, San Antonio, Texas. October 12 - 15, 2011
__________________________________________
CASEY LAGANCasey Lagan, Mark Rahm, et al. Evaluation of the clinician-patient communication workshop.
Poster presentation, The Association for Surgi-cal Education Annual Meeting, San Diego, CA, March 22, 2012.
Casey Lagan, Hania Wehbe-Janek, Kim Waldo, Amy Fox, Chanhee Jo, Mark Rahm. Evaluation of an interprofessional clinician-patient communication workshop utilizing standardized patient methodol-ogy.
J Surg Educ. 2013 Jan-Feb;70(1):95-103. doi: 10.1016/j.jsurg.2012.06.018
__________________________________________
KUSHAL PATELHank C Wallace, Robert A. Probe, Christopher D Chaput, Kushal V Patel. Operative treatment of hip fractures in patients on Clopidogrel: a case-control study.
Iowa Orthop J. 2012;32:95-9. PMID: 23576928Podium Presentation, American Academy of Orthopaedic Surgeons 75th Annual Meeting San Francisco, CA, March 2008
Wallace HC, Probe RA, Chaput CD, Patel KV. Operative Treatment of Hip Fractures in Patients on
Clopidogrel: A Case Control Study. The Iowa Orthopedic Journal. 2012: 95 – 99.
Christopher D Chaput, Kushal V Patel, George W Brindley, et al. Influence of a Platelet Concentrate on Prosthetic Bone Ingrowth in a Rabbit Model.
Journal of Surgical Orthopaedic Advances. 2007; 16(4): 159 – 163.Podium Presentation, American Academy of Orthopaedic Surgeons 74th Annual Meeting. San Diego, CA, February 2007.
Kushal V Patel, Dan C Jupiter, Bryce C Allen. Hemoglobin trends after primary total hip and knee arthroplasty: are daily post-operative hemoglobin phlebotomies necessary?
Podium Presentation, SOA Resident Travel Grand Award Winner 2013, Southern Orthopaedic As-sociation Annual Meeting, Palm Beach, FL, July 2013
Kushal V Patel, Adam Shar, Zachary T Hubert, Timmothy R Randell, Daniel C Jupiter, Kindyle L Brennan, Michael L Brennan, Robert A Probe, Mat-thew L Davis. A modified frailty index: correlation to one and two-year mortality in geriatric femoral neck fractures.
Paper Presentation, American Academy of Ortho-paedic Surgeons Annual Meeting 2013. Chicago, IL. March 18-23, 2013Podium Presentation, Southern Orthopaedic As-sociation Annual Meeting. White Sulfur Springs, WV, July 2012.Clinical Orthopaedics and Related Research. 2014 Mar; 472(3):1030-5.
Kushal V Patel, Kwon Park, Daniel C Jupiter, Kin-dyle L Brennan, Michael L Brennan. Mortality and morbidity of femur fractures in high energy elderly trauma patients.
Paper Presentation, American Academy of Orthopaedic Surgeons Annual Meeting 2013. Chicago, IL. March 19-23, 2013
Kushal V Patel, Kindyle L Brennan, Matthew L Davis, Daniel C Jupiter, and Michael L Brennan.
CURRENT RESIDENT PUBLICATIONS / PRESENTATIONS

48
High-energy femur fractures increase morbidity but not mortality in elderly patients.
Clinical Orthopaedics and Related Research. 2014 Mar;472(3):1030-5. doi: 10.1007/s11999-013-3349-0. Epub 2013 Oct 29
Kushal V Patel, Daniel C Jupiter, Kindyle L Bren-nan, Matthew L Davis, and Michael L Brennan. Mortality and morbidity of femur fractures in high energy elderly trauma patients.
Clinical Orthopaedics and Related Research. 2014 Mar; 472(3):1010-7. doi: 10.1007/s11999-013-3334-7.
Kusha V Patel, Kwon Park, Daniel C Jupiter, Kindlye L. Brennan, Matthew L Davis, Michael L Brennan. Mortality and morbidity in high energy trauma patients, aged 60 and greater, with femoral shaft fractures.
Poster Presentation, Southern Orthopaedic As-sociation Annual Meeting. White Sulfur Springs, WV, July 18th -21st 2012.
Kushal V Patel, Kindyle L Brennan, Michael L Brennan, Daniel C Jupiter, Adam Shar, Matthew L Davis, Association of a modified frailty index with mortality after femoral neck fracture in patients aged 60 years and older.
Clinical Orthopaedics and Related Research. 2014 Mar;472(3):1010-7. doi: 10.1007/s11999-013-3334-7
Kushal V Patel, Judith Linton, E. Sullivan, Douglas A Barnes. Pre-Adolescent Single Event Multilevel Surgery Outcomes in Adolescents with Spastic Diplegic Cerebral Palsy.
Poster Presentation, American Academy of Or-thopaedic Surgeons Annual Meeting 2014. New Orleans, LA
_________________________________________
TIMMOTHY RANDELLDonavan K Murphy, Timmothy Randell, Kindyle L Brennan, Juhee Song, John M. Hamilton, Michael L Brennan, Robert A Probe. Influence of displacement and treatment method on survivorship of the index
procedure for femoral neck fracture. Paper Presentation #76 - Orthopaedic Trauma Association 2011 Annual Meeting. San Antonio, Texas; October 2011.
Timmothy Randell, Daniel Jupiter, Kindyle L. Brennan, John Hamilton, Michael Brennan. Influ-ence of displacement and treatment method of femoral neck fractures on patient mortality.
Presented - Southern Orthopaedic Association Annual Meeting. White Sulfur Springs, WV, July 18th -21st 2012.
Donavan K. Murphy, Timmothy Randell, Kindyle L. Brennan, Robert A. Probe, and Michael L. Bren-nan. Treatment and displacement affect the reop-eration rate for femoral neck fracture.
Clinical Orthopaedics and Related Research. 2013 Aug; 471(8):2691-702. doi: 10.1007/s11999-013-3020-9
J Lemmon, Timmothy Randell, and P Benhaim. “Carpal Bone Fractures” (Chapter 62).
In Jeffrey E. Janis (Ed.), Essentials of Plastic Surgery, 2nd Edition, 2014, pp741-749, St. Louis, MO: QMP
Adam Shar, Timothy Randell, Michael L Brennan, Kindyle L Brennan, Daniel C Jupiter, and Zachary T Hubert. Mortality of femoral neck fractures in the elderly based on age-modified charlson comor-bidity index score.
Podium presentation, 29th Annual Southern Orthopaedic Association on July 19, 2012, in Sulphur Springs, WV
_________________________________________
MATTHEW ELLINGTONMatthew Ellington, Brett N Robin, Daniel C Jupiter and Bryce Allen. Plateau-Patella angle in evalua-tion of patellar heights in osteoarthritis.
Knee. 2014 Mar 20. pii: S0968-0160(14)00058-1. doi: 10.1016/j.knee.2014.02.026. [Epub ahead of print]Poster Presentation, Western Orthopaedic As-sociation’s Annual Meeting, Portland, OR, June
CURRENT RESIDENT PUBLICATIONS / PRESENTATIONS

49
2012.Southern Orthopaedic Association Annual Meet-ing, West Virginia, July 2012.
Brett N Robin, Matthew Ellington, Chanhee Jo, Michael L. Brennan. Bone mineral density of the lumbar spine and femoral neck do not correlate with loss of reduction in elderly distal radius.
Podium presentation, Hanes H. Brindley, Sr. Or-thopaedic Lectureship and Orthopaedic Resident Research Forum, Temple, TX, June 10, 2011.Podium presentation, Western Orthopaedic As-sociation Annual Meeting 2012, Portland OR, Poster presentation, Southern Orthopaedic As-sociation Meeting 2012
Brett N. Robin, Matthew Ellington, Chanhee Jo, Bryce C Allen. Patella-Plateau angle in evaluation of patellar height after total knee arthroplasty.
Journal of Arthroplasty. 2014 Jan 28. pii: S0883-5403(14)00068-0. doi: 10.1016/j.arth.2014.01.026. [Epub ahead of print]Poster presentation, American Academy of Ortho-paedic Surgeons Annual Meeting, Feb 2012, San Francisco, CA., Alternate podium presentation
Brett N Robin, Matthew D Ellington, Daniel C Ju-piter, and Michael L Brennan. Relationship of bone mineral density of spine and femoral neck to distal radius fracture stability in patients over 65.
Journal of Hand Surgery (American). 2014 May;39(5):861-866.e3, doi: 10.1016/j.jhsa.2014.01.043. [Epub ahead of print]
Matthew Ellington, Judith Linton, A Scott, and Douglas Barnes. Rectus femoris transfer versus rectus intramuscular lengthening for the treatment of stiff knee gait in children with cerebral palsy.
Accepted for podium presentation. Pediatric Orthopaedic Society of North American Annual Meeting, Hollywood, CA, 2014
__________________________________________
JOSHUA GRIFFINJoshua Griffin, Bryce C. Allen, Kindyle L Brennan, Daniel C Jupiter. Hemoglobin A1c as a predictor of
complications after total knee arthroplasty. Annual Meeting of the Western Orthopaedic As-sociation, Portland, OR, June 13-16, 2012.
Joshua Grffin, Donavan K. Murphy, Kindyle L. Brennan, Michael L Brennan, Daniel C Jupiter. The impact of age on reoperation rates for femoral neck fractures treated with percutaneious pinning and hemiarthroplasty?
Harley & Betty Baxter Resident Award Winner, 2013, Southern Orthopeadic Association Annual Meeting, Palm Beach Fl, July 2013.Resident/Fellow Award 2013, Western Orthopae-dic Association Young Investigator Awards. 2013.
__________________________________________
MATTHEW JORDONMatthew Jordan, J Reilly, Daniel Jupiter, Kindyle L Brennan, K Hitt, Christopher Chaput. Body mass in-dex in relation to total hip arthroplasty complication.
Journal of Arthroplasty (currently under revision). Abstract accepted for poster presentation at 2013 Western Orthopedic Association Annual Meeting.
Matthew Jordan, Travis Wilson, Daniel Jupiter, Bryce Allen, Christopher Chaput. Local soft-tissue thickness as a significant risk factor for complica-tions after total hip arthroplasty.
Podium presentation at 2014 Southern Orthope-dic Association Annual Meeting. Winner of the Resident Research Award.
Matthew Jordan, Kip Murphy, Judith Linton, Alli-son Scott - Shriners Hospital for Children, Hous-ton, TXRevision Hamstring Lengthening in Children with Cerebral Palsy. Currently preparing manuscript __________________________________________
DONAVAN K. MURPHYDonavan K. Murphy, Timmothy Randell, Kindyle L. Brennan, Juhee Song, John M. Hamilton, Michael L. Brennan, Robert A. Probe. Influence of displacement and treatment method on survivorship of the index procedure for femoral neck fracture.
Paper Presentation #76. Orthopaedic Trauma
CURRENT RESIDENT PUBLICATIONS / PRESENTATIONS

50
Association 2011 Annual Meeting. San Antonio, Texas; October 2011.
Donavan K. Murphy, Timmothy Randell, Kindyle L. Brennan, Robert A. Probe, Michael L. Brennan.Treatment and displacement affect the reoperation rate for femoral neck fracture.
Clin Orthop Relat Res. 2013 Aug;471(8):2691-702. doi: 10.1007/s11999-013-3020-9
Joshua Grffin, Donavan K. Murphy, Kindyle L. Brennan, Michael L Brennan, Daniel C Jupiter. The impact of age on reoperation rates for femoral neck fractures treated with percutaneious pinning and hemiarthroplasty?
Harley & Betty Baxter Resident Award Winner, 2013, Southern Orthopeadic Association Annual Meeting, Palm Beach Fl, July 2013.Resident/Fellow Award 2013, Western Orthopae-dic Association Young Investigator Awards.
__________________________________________
JUSTIN BARTLEYJustin Bartley, Kindyle Brennan, Christopher Chaput, William Hamilton, Daniel Jupiter, Derek Lichota, Robert Reeve, and John Welsh. Infec-tion rates in arthroscopic versus open rotator cuff repair
Justin Bartley, Scott M. Munroe, and Russell A. Ward. Fibrous dysplasia in the calcaneus
Scott and White Research Days Poster Presenta-tion: May 2013
__________________________________________
JEFFREY KNABE
Jeffrey Knabe. The use of low-dose recombi-nant Human Bone Morphogenic Protein-2 in the elderly: a comparative study assessing safety and fusion success in the posterior lumbar spine.__________________________________________
HEATHER LICHTHeather Licht, John Vassaur, Mark Murray, Daniel Jupiter, Justin Regner, and Christopher Chaput.
The relationship of obesity to increasing healthcare burden in the setting of orthopedic polytrauma.
Podium presentation, American Academy of Or-thopaedic Surgeons Annual Meeting 2014. New Orleans, LA Podium presentation, Baylor Scott & White Research Days May 2014. Temple, TX
__________________________________________
ADAM SHARAdam Shar, Timothy Randell, Michael L Brennan, Kindyle L. Brennan, Daniel C Jupiter, and Zachary T Hubert. Mortality of femoral neck fractures in the elderly based on Age-Modified Charlson Comor-bidity Index Score.
Podium presentation - 29th Annual Southern Orthopaedic Association on July 19, 2012, in Sulphur Springs, WV
Lawson A B Copley, Major Alison Kinsler, Tay-lor Gheen, Adam Shar, David Sun, and Richard Brown. The impact of evidence-based clinical practice guidelines applied by a multidisciplinary team for the care of children with osteomyelitis.
Journal of Bone and Joint Surgery (American). 2013; 95: 686-93. PMID:23595066
Kushal V Patel, Kindyle L Brennan, Michael L Brennan, Daniel C Jupiter, Adam Shar, and Matthew L Davis, Association of a modified frailty index with mortality after femoral neck fracture in patients aged 60 years and older.
Clinical Orthopaedics and Related Research. 2014 Mar;472(3):1010-7. doi: 10.1007/s11999-013-3334-7
__________________________________________
NATHAN B. HAILE Nathan B Haile, Christopher Chaput, Aditya Mohan Muzumdar, David M. Gloystein, Vasilios A. Zerris, Paul Justin Tortolani, Mark Rahm, Mark Moldavsky, Suresh Chinthakunta, Saif Khalil.Anterior fixation of floating facet fractures in the cervical spine. a prospective case series and bio-mechanical analysis.
CURRENT RESIDENT PUBLICATIONS / PRESENTATIONS
51
1948Ed Thomas 1950Larry Thompson
1951C.L. Hay
1952J. Fernandez
1954J.F. Tracey
1958R.A. Barrow, Jr.
1960W.A. Ross
1961J.D. McGovern, Jr.
1963D.T. Lazarz
1964 R. H. Bushey
1965R. L. Pentecost
1966Jaime Contreras
1968J.L. ZumBrunnenP.H. RymesPedro Quiroga
1969R.C. CarnahamF.J. Sawchuck
1970C.R. RousseauRufino H. Gonzalez
1971J.E. SwinkJames T. (Tom) Hodges
1972John HardimanDavid Steiner
1973George BruceRichard GuistraMarques E. Rhoades
1974 William E. Swan
1975William E. SheffieldFrank R. Vincenti
1976Ricardo N. AdobbatiEric J. Wilson
1977 Gary D. SnookDavid M. AllenSteven J. Mackey
1978John W. DitzlerAllan Hibbard
1979John C. CarterCharles F. Kallina
1980Howard L. CrockettJoe M. Todd
1981Thomas M. KleuserRobert D. Harper
1982Steven A. CordSteven E. Nolan
1983Wilson H. LandersDavid O. GilloryGary R. Williams
1984David W. DuffnerDaniel MacRandallStephen D. Ruyle
1985Carl L. CannonTed D. SpearsSteve C. Wilson
1986William P. HamiltonScott OrthRobert Shackelford
1987Craig R. DuhonR. Chris EstesDavid A. Roberts
1988James R. BischoffDaniel RipaRoger C. Sessions
1989Kevin C. McLeodJeffrey C. NielsonRobert A. Probe
Orthopaedic Resident Alumni
52
1990Thomas M. CarrellScott D. CochranRichard D. Nixon
1991Kirby D. HittDavid HowieRobert E. Reeve
1992Sherwood DuhonDerek K. LichotaMark D. Rahm
1993David A. BenavidesC. Kent BoeseMark D. Young
1994Steven T. CarawanStephen P. CourtneyAndrew A. Stoebner
1995Marshall G. BacaEugene E. CurrySteve A. Shapiro
1996Robert K. LieuranceTodd M. RaabeRichard B. Schultz
1997Thoma J. EllisKalin D. KelsoEdwin M. Roeder
1998Douglas S. FornfeistDarey A. PhilbrickJeffrey N. Spaw
1999 Michael L. RamseyJordan G. StanleyHarold G. Weems, Jr.
2000 Jonathan W. Fontenot J. Kevin RudderSteven H. Weeden
2001 James W. Burnett Michael D. DersamPlinio Antonio Caldera
2002Christopher D. ChaputMatthew P. CubbageScott M. Munroe
2003Reagan L. CrossnoeKyle C. GirodBradley D. Harman
2004Brett E. CaseyTimothy B. DixonMichael J. Leahy
2005Craig C. GreeneCharles F. Kallina, IVMarcus Roux
2006Eric HooleyRobert ReddixJ. Kevin Smith
2007Michael L. BrennanRussell J. ClarkDonald S. Stewart
2008Derek T. PadonRussell A. Ward
2009Clint D. BarnettJason D. CarterRyan M. Tibbetts
2010John P. AkinsRichard B. BarberNicholas P. SouderHenry (Hank) Wallace
2011Jason L. BrannenDavid E. DominguezDaniel L. Stahl
2012Garrison Benton Cyrus Caroom Christopher SouderCoy Wright
2013Jared Allred Matthew DriscollDavid KummerfeldBrett Robin
Orthopaedic Resident Alumni Continued
53
2012 Orthopaedic Residents
PGY-5
PGY-4
David Ferguson Casey Lagan Kushal Patel Timmothy Randell
Matthew Ellington Joshua Griffin Matthew Jordan Donavan Murphy

54
Travis Anthony Guadalupe de la Fuente Nathan Haile Clayton Vaughan
PGY-2
PGY-3
PGY-1
Justin Bartley Jeffrey Knabe Heather Licht Adam Shar
Tyler Cooper Gerardo Myrin John Welsh Travis Wilson

55
Conflict of InterestPresenters will disclose whether one or more of the following potential conflicts of interest exist with the program’s commercial support; honorarium/expenses; grants; a consultant role; speaker’s bureau member; stock ownership; or other special relationships.
AccreditationScott & White is accredited by the Accreditation Council of Continuing Medical Education to sponsor medical education to physicians.
Continuing Education CreditScott & White designates this live activity for a maximum of 7 AMA PRA Category 1 Credits™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
Faculty DisclosuresDr. Mubarak has disclosed he has a financial relationship with Smith & Nephew in the form of consultant fees; Smith & Nephew, Lippincott Williams and Wilkins in the form of royalties.
Educational grant by
56