haematological case study
TRANSCRIPT
CASE 1
HISTORY
•A 30yrs old male,presented to OPD
with malaise, tiredness and
weakness.
•He is a known alcoholic.
PHYSICAL FINDINGS
INVESTIGATIONS
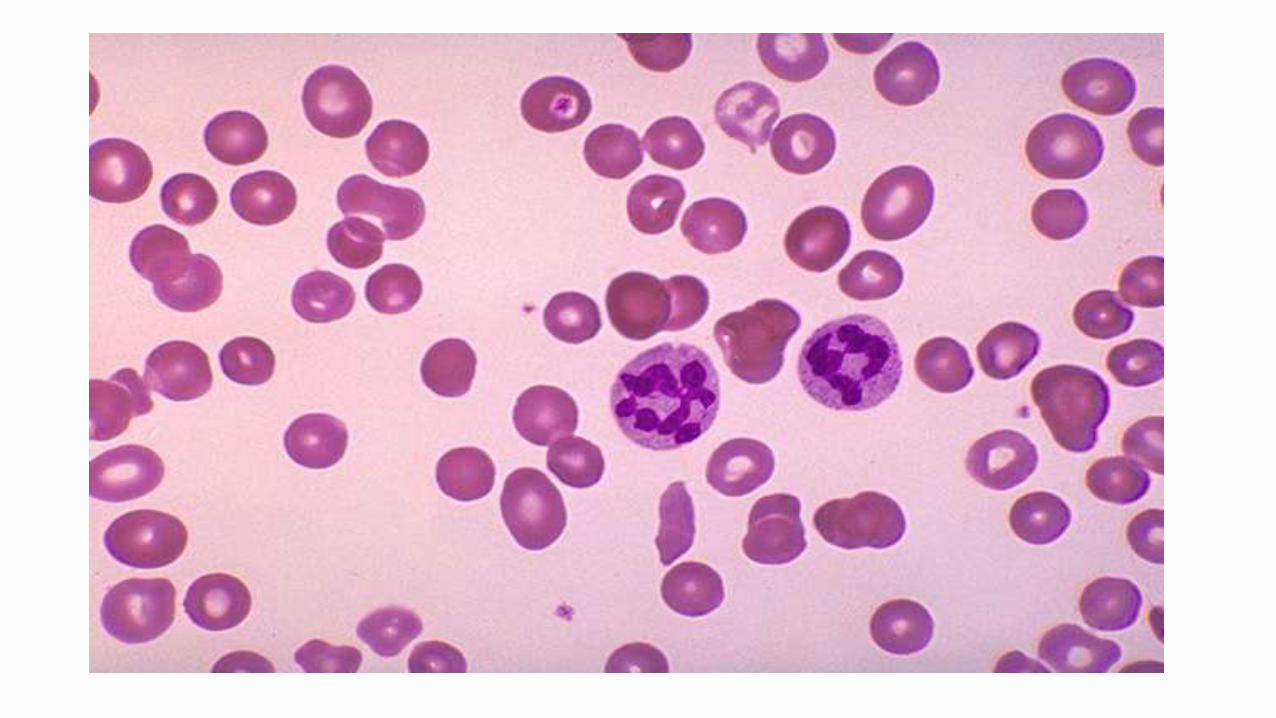
• PERIPHERAL BLOOD SMEAR- Anisopoikilocytosis
- Macro-ovalocytes
- Hypersegmented Neutrophil
• RBC INDICES- MCV- 110
- RETICULOCYTE COUNT- low
DIAGNOSIS??
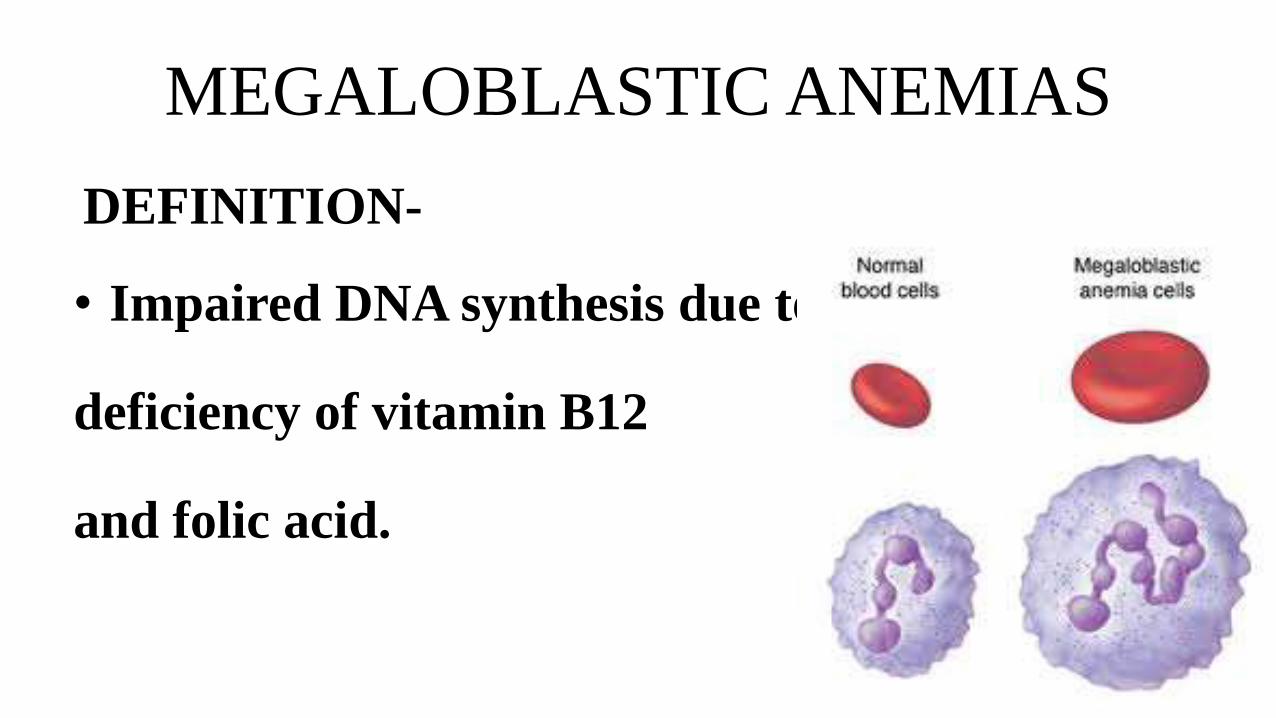
MEGALOBLASTIC ANEMIAS
DEFINITION-
• Impaired DNA synthesis due to
deficiency of vitamin B12
and folic acid.
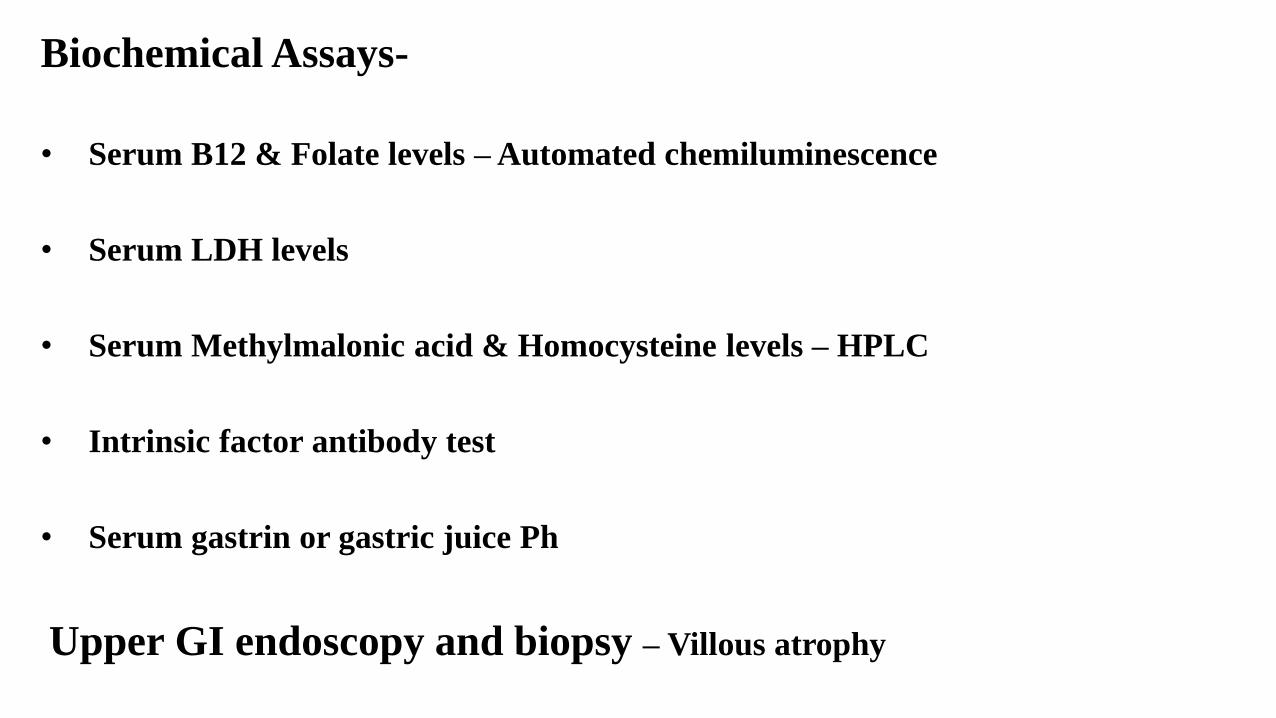
Biochemical Assays-
• Serum B12 & Folate levels – Automated chemiluminescence
• Serum LDH levels
• Serum Methylmalonic acid & Homocysteine levels – HPLC
• Intrinsic factor antibody test
• Serum gastrin or gastric juice Ph
Upper GI endoscopy and biopsy – Villous atrophy
•Increase in Homocysteine and Methy
malonic acid – Vit B 12 Deficiency
•Only increase in Homocysteine : Folate
deficiency
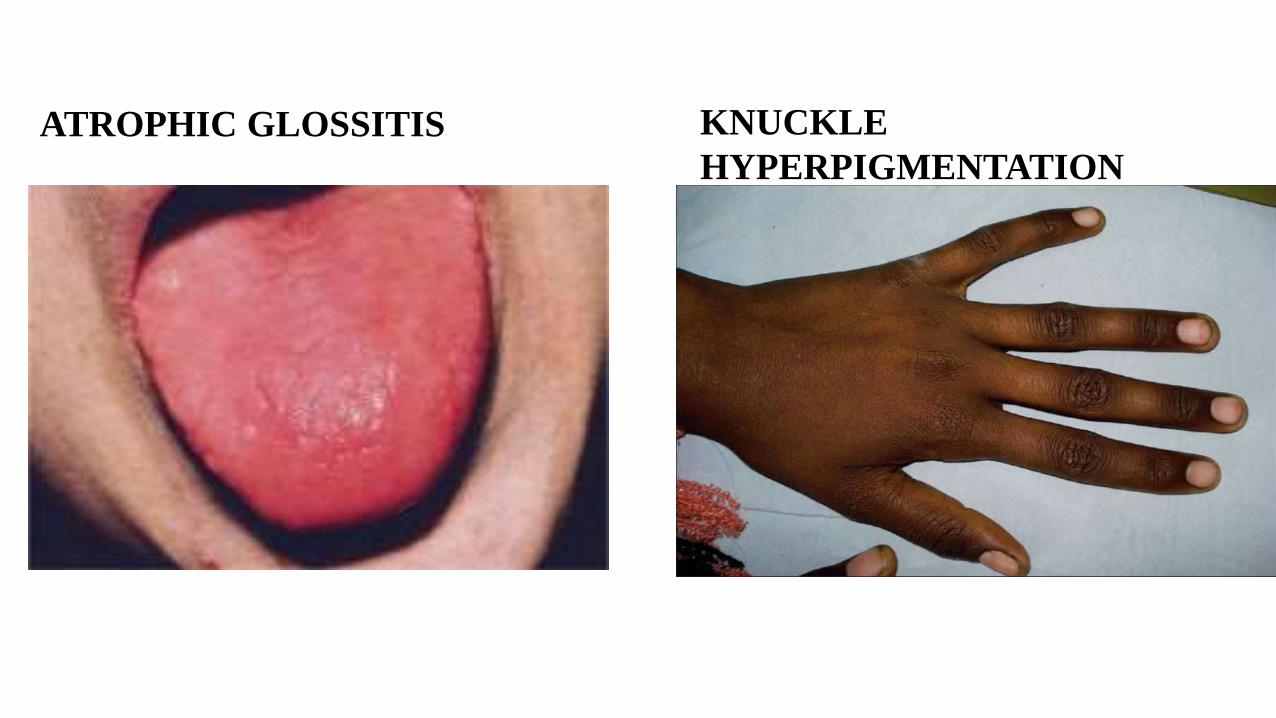
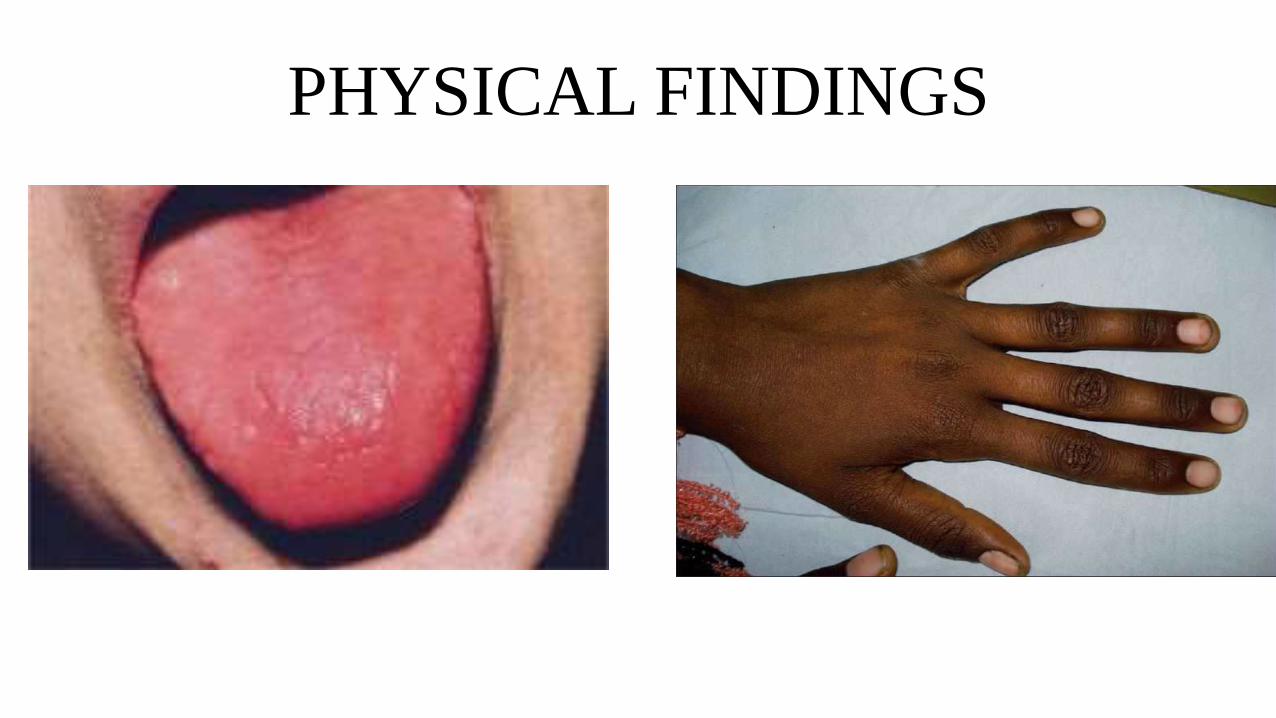
ATROPHIC GLOSSITIS KNUCKLE
HYPERPIGMENTATION

“BONE MARROW EXAMINATION IS NOT
REQUIRED FOR THE DIAGNOSIS OF
MEGALOBLASTIC ANEMIA”
CASE 2
HISTORY
• A 10yrs old girl presents with pallor and
weakness.
• Congenital anomalies seen
• Family history of cancer.
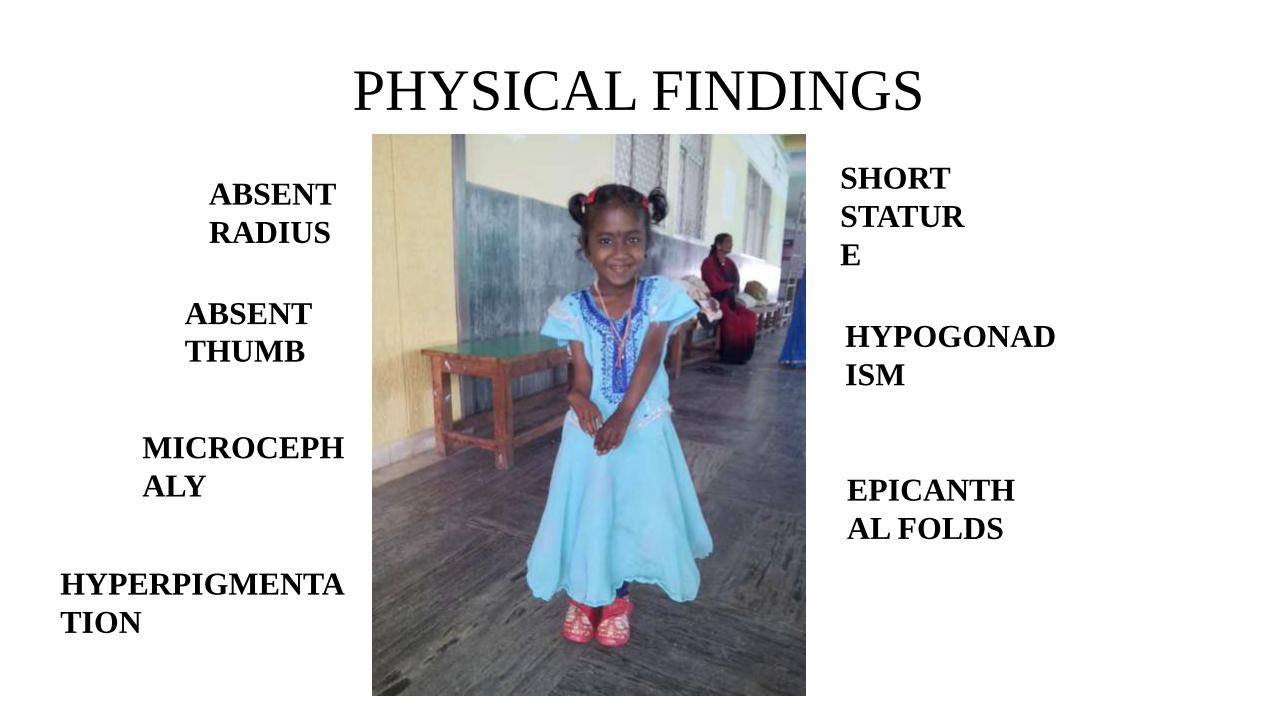
PHYSICAL FINDINGS
EPICANTH
AL FOLDS
ABSENT
THUMB
SHORT
STATUR
E
MICROCEPH
ALY
HYPERPIGMENTA
TION
HYPOGONAD
ISM
ABSENT
RADIUS
DIAGNOSIS??
FANCONI ANEMIA
• Inherited syndrome
• Autosomal recessive
• Includes- Pancytopenia
- Congenital anomalies
- Cancer susceptibility
FURTHER WORK-UP
• Demonstration of increased chromosomal
breakage in the presence of DNA cross-
linking agents such as MITOMYCIN C or
DIEPOXYBUTANE
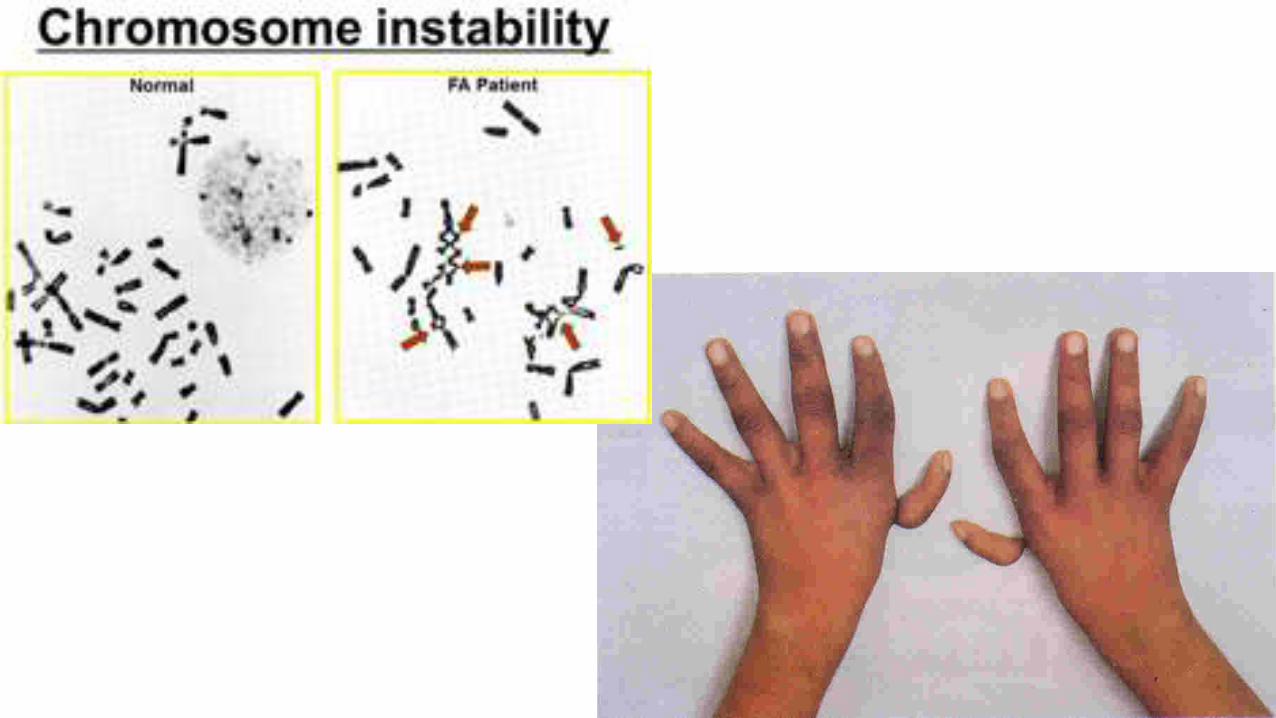
“No other constitutional
pancytopenia is associated
with an abnormal
chromosomal breakage study”
CASE 3
HISTORY
•A 55yrs old male on chemotherapy
presents with pallor and dyspnea.
•Also complains of petechiae and
frequent minor infections.
INVESTIGATIONS
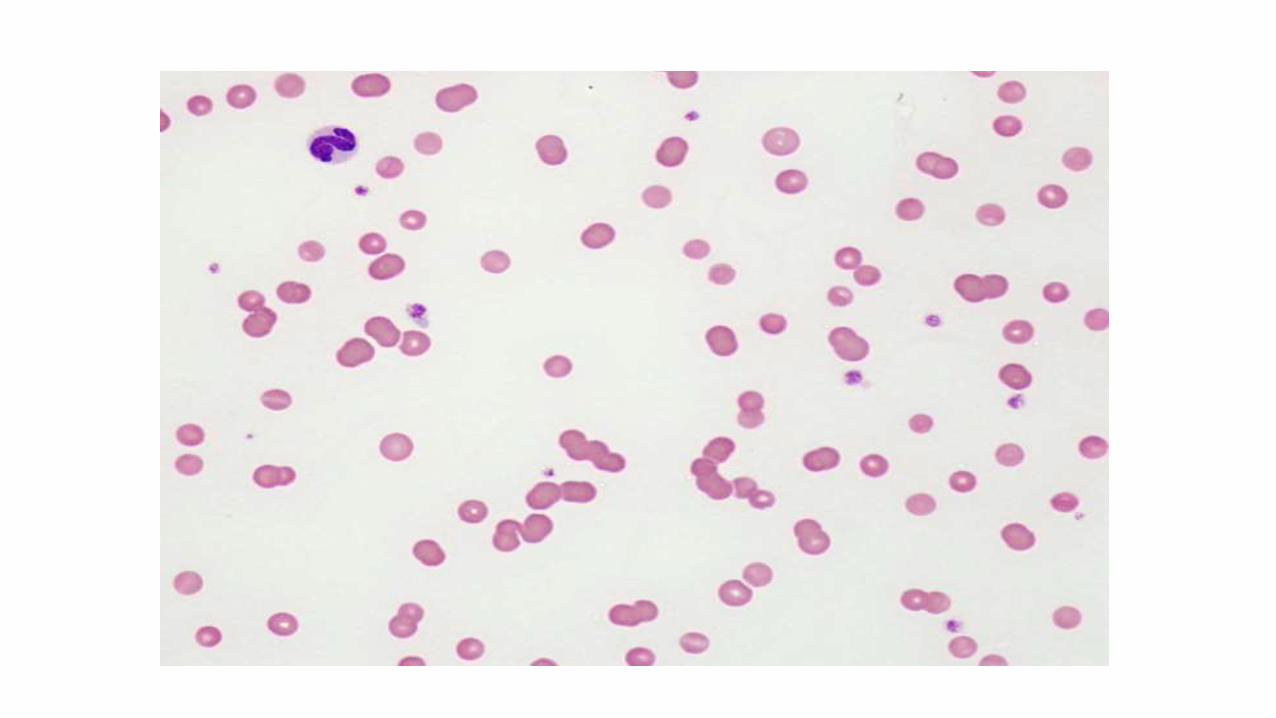
• PERIPHERAL BLOOD SMEAR-
Pancytopenia
• BONE MARROW ASPIRATION- Dry tap
DIAGNOSIS??

FURTHER WORK-UP
• BONE MARROW BIOPSY-
Hypocellular marrow
• No Splenomegaly
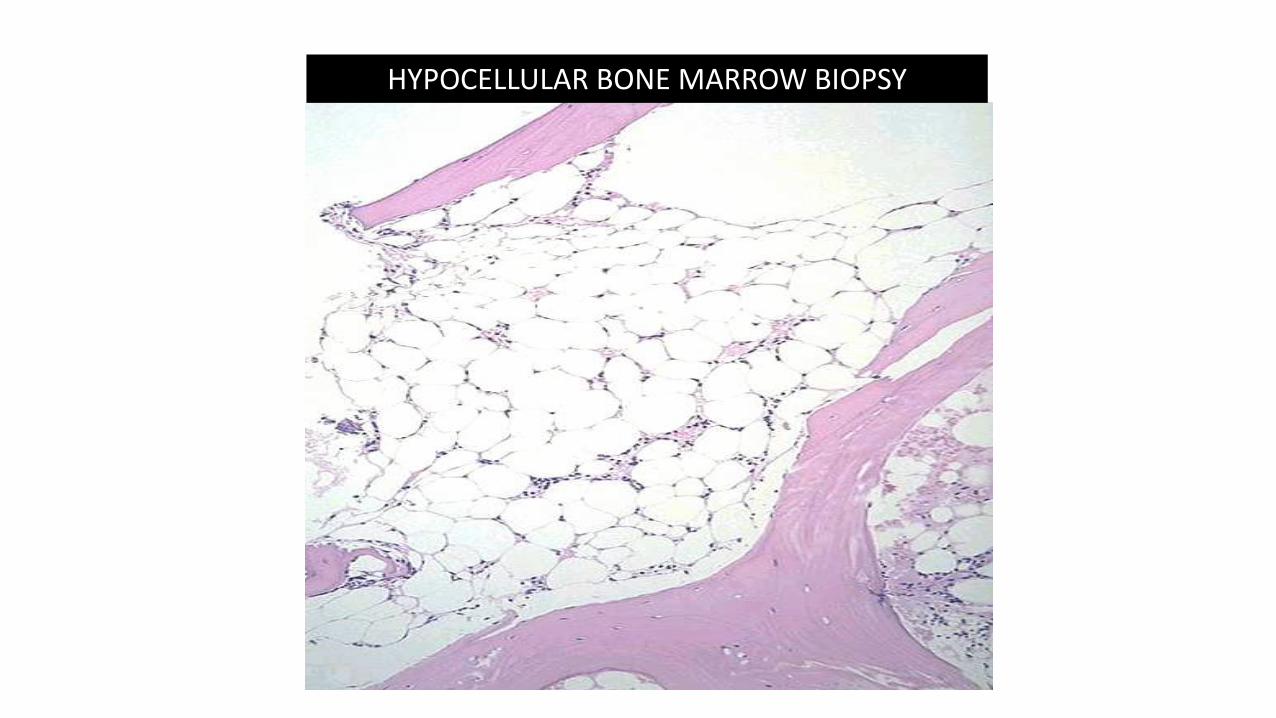
HYPOCELLULAR BONE MARROW BIOPSY
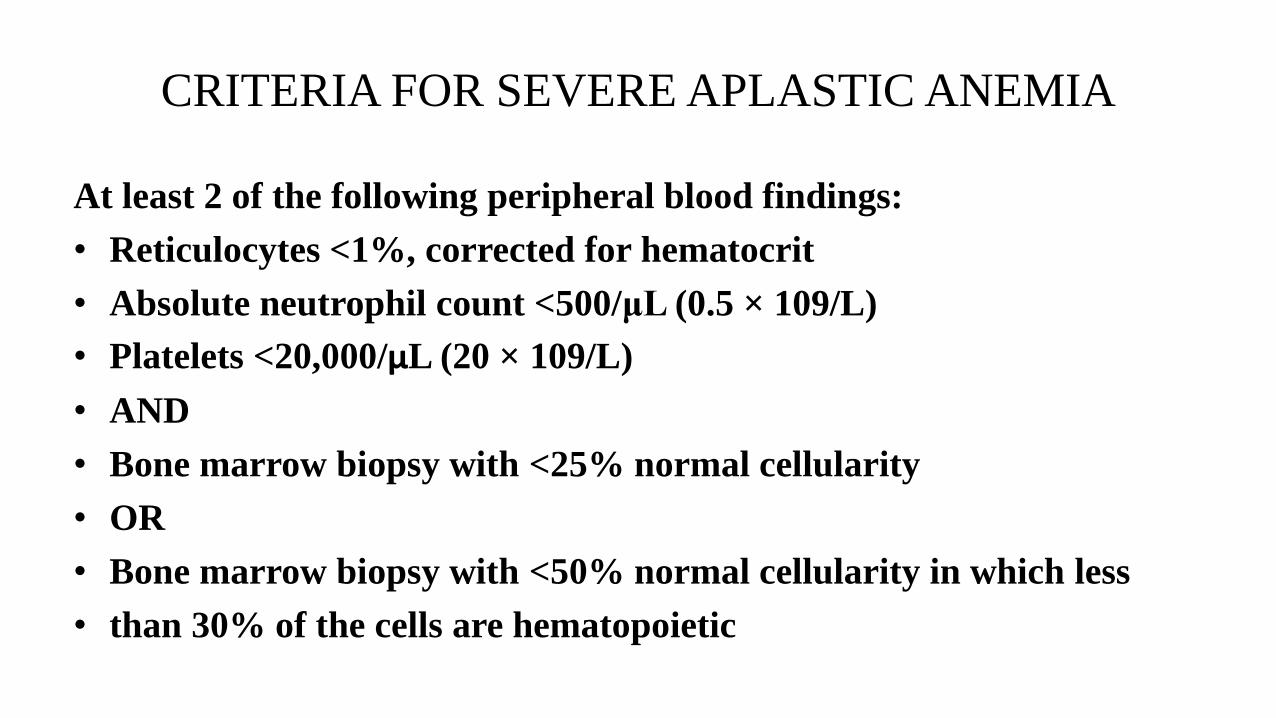
CRITERIA FOR SEVERE APLASTIC ANEMIA
At least 2 of the following peripheral blood findings:
• Reticulocytes <1%, corrected for hematocrit
• Absolute neutrophil count <500/μL (0.5 × 109/L)
• Platelets <20,000/μL (20 × 109/L)
• AND
• Bone marrow biopsy with <25% normal cellularity
• OR
• Bone marrow biopsy with <50% normal cellularity in which less
• than 30% of the cells are hematopoietic
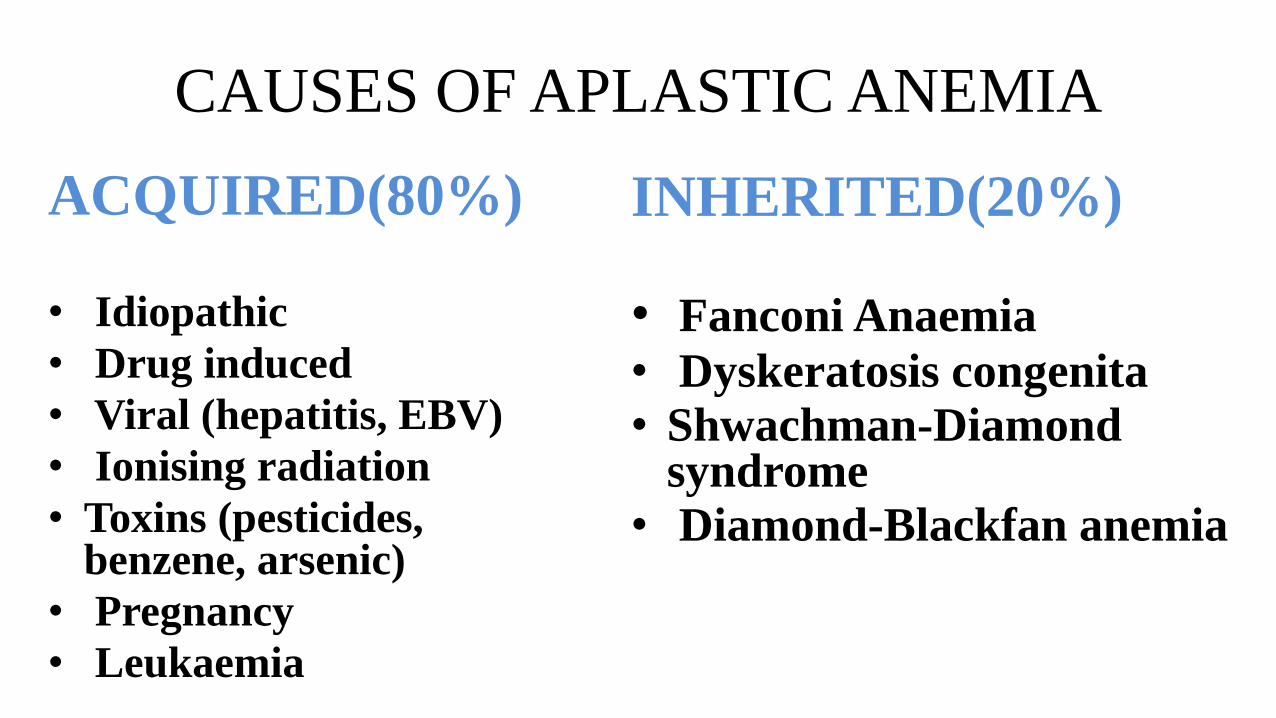
CAUSES OF APLASTIC ANEMIA
ACQUIRED(80%)
• Idiopathic
• Drug induced
• Viral (hepatitis, EBV)
• Ionising radiation
• Toxins (pesticides, benzene, arsenic)
• Pregnancy
• Leukaemia
INHERITED(20%)
• Fanconi Anaemia
• Dyskeratosis congenita
• Shwachman-Diamond syndrome
• Diamond-Blackfan anemia
DRUGS CAUSING APLASTIC ANEMIA
• Anti cancer drugs :Alkylating agents
Antimetabolities
Antimitotics
• Antibiotics : Streptomycin
Tetracycline
Methicillin
Chloramphenicol
• Anti inflammatory drugs : Indomethacin
Ibuprofen
Aspirin
• Anti thyroid : Methimazole
Methylthiouracil
Propylthiouracil
• Anti hypertensive : Methyldopa
• Anticonvulsants : Hydantoins
Carbamazepine
• Antihistaminics : Cemitidine
Chlorpheniramine
“Most common cause Of
Aplastic Anemia is
IDIOPATHIC”
CASE 4
HISTORY
• A 20yr old male presents with sudden onset
malaise and fatigue with recurrent
abdominal pain.
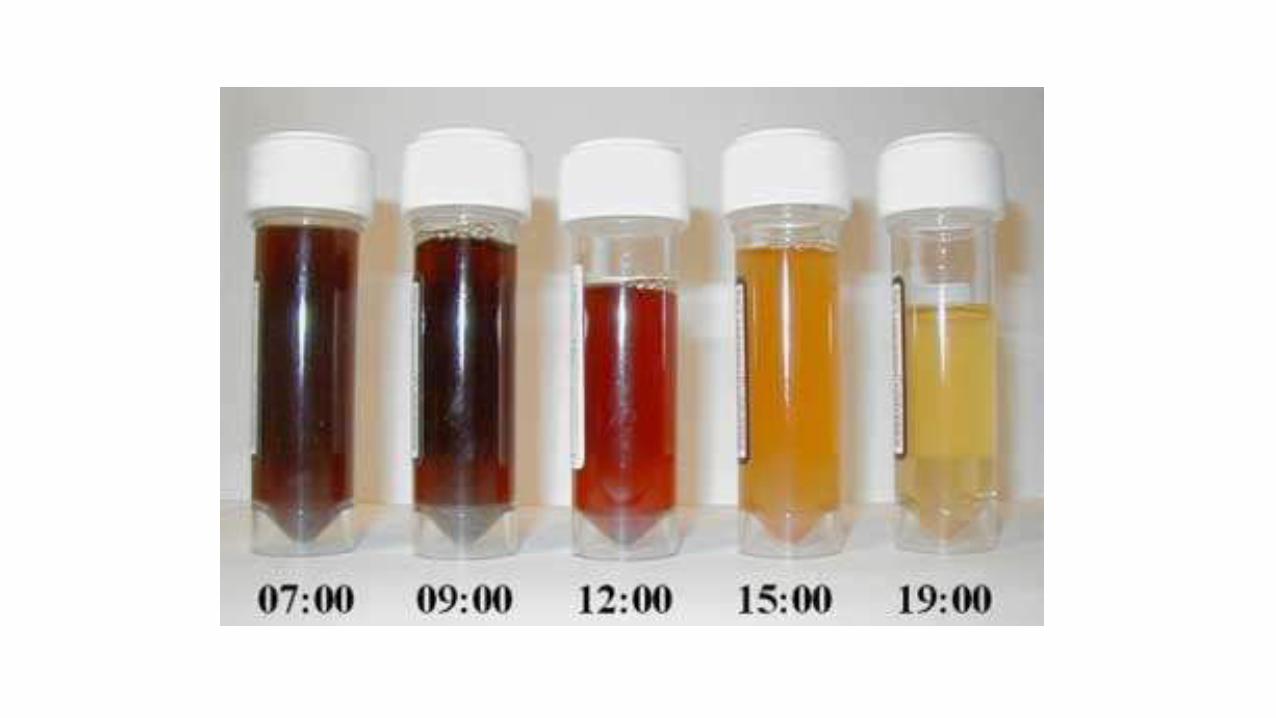
• He also complains of dark color urine on
waking up.

INVESTIGATIONS
• PERIPHERAL BLOOD EXAMINATION-
Hemolytic picture seen
• BONE MARROW EXAMINATION-
Hypoplastic
DIAGNOSIS??
FURTHER WORK UP
• HAM’S TEST
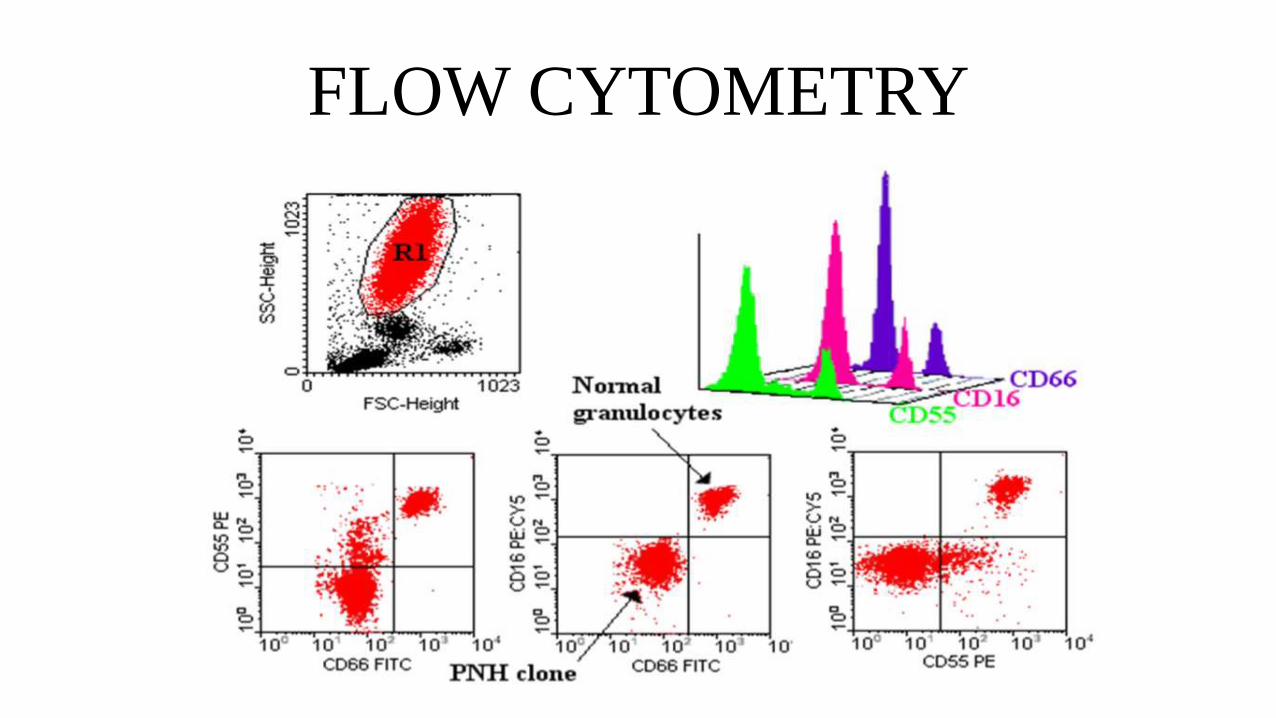
FLOW CYTOMETRY
PAROXYSMAL NOCTURNAL
HAEMOGLUBINURIA
• PNH arises as a result of nonmalignant clonal
expansion of one or more hematopoietic stem
cells that have acquired somatic mutation of the
X-chromosome gene PIGA
(phosphatidylinositol glycan class A)
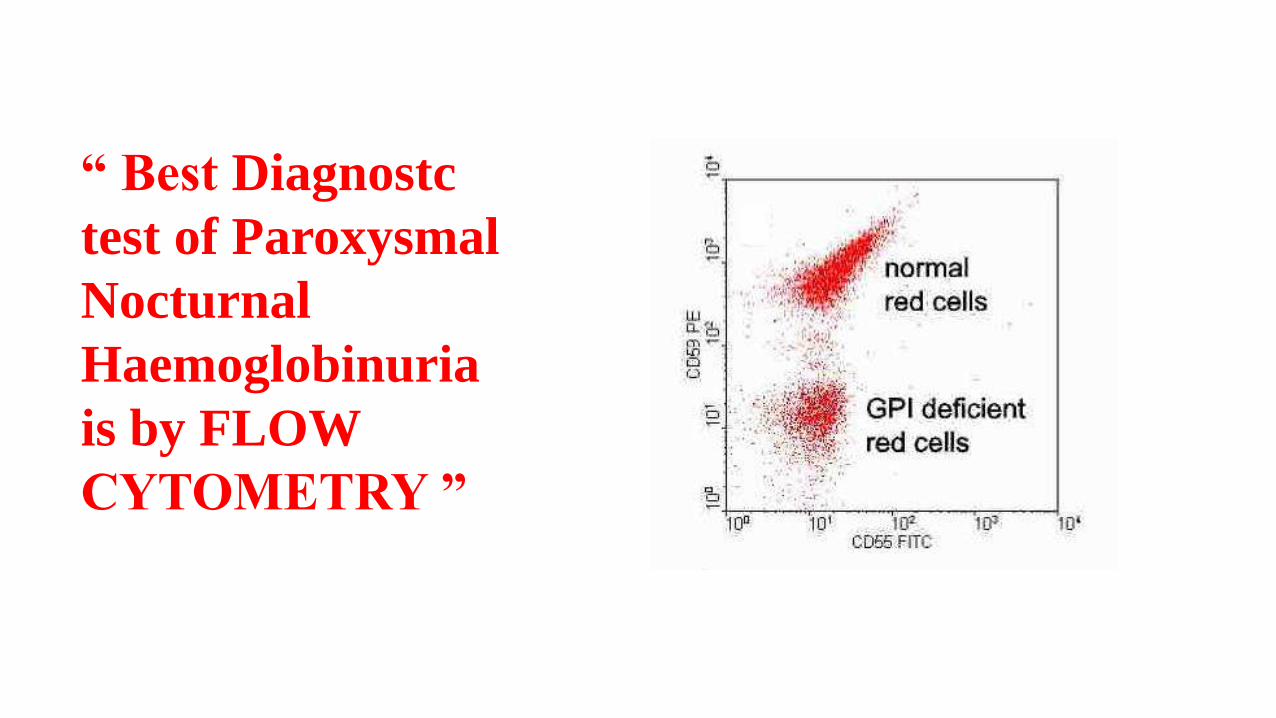
“ Best Diagnostc
test of Paroxysmal
Nocturnal
Haemoglobinuria
is by FLOW
CYTOMETRY ”
CASE 5
HISTORY
• A 8yr old child comes with sudden onset fever
and fatigue.
• Also gives history of recurrent pneumonia.
• On examination- generalised lymphadenopathy
present.
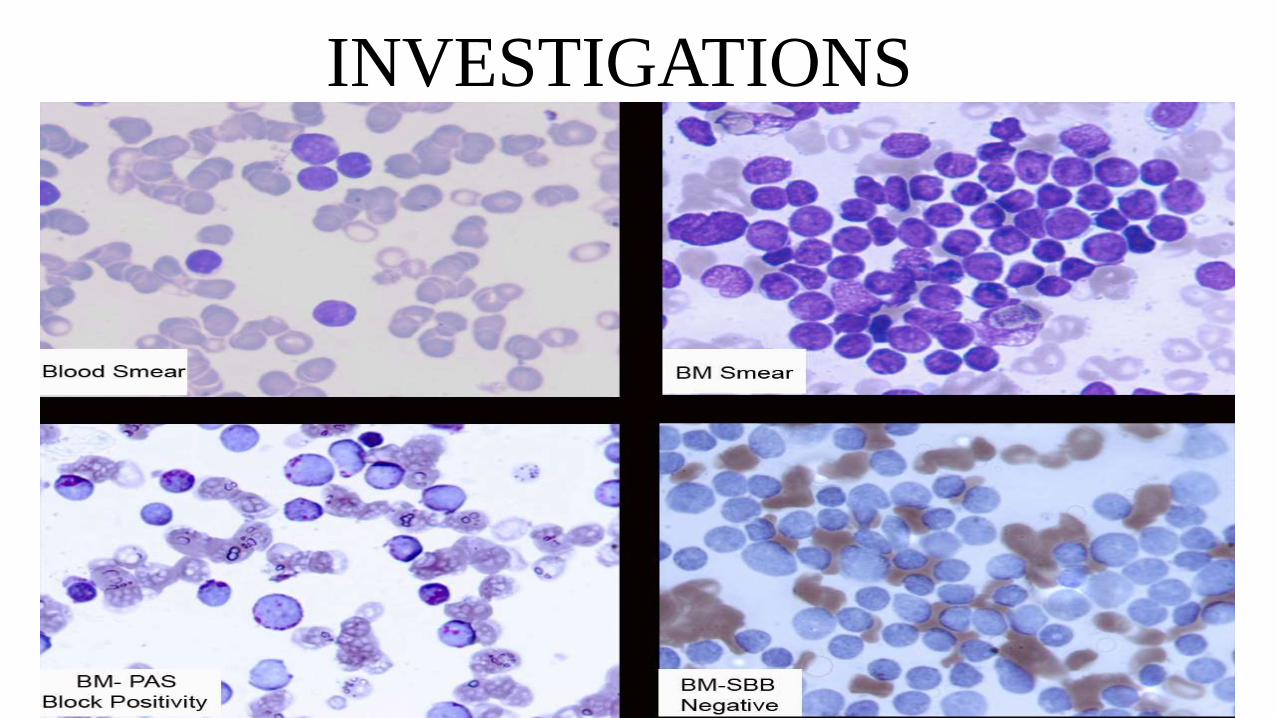
INVESTIGATIONS
DIAGNOSIS??
FURTHER WORK-UP
• CYTOGENETIC STUDY- t(12;21) present.
ACUTE LYMPHOBLASTIC
LEUKEMIA
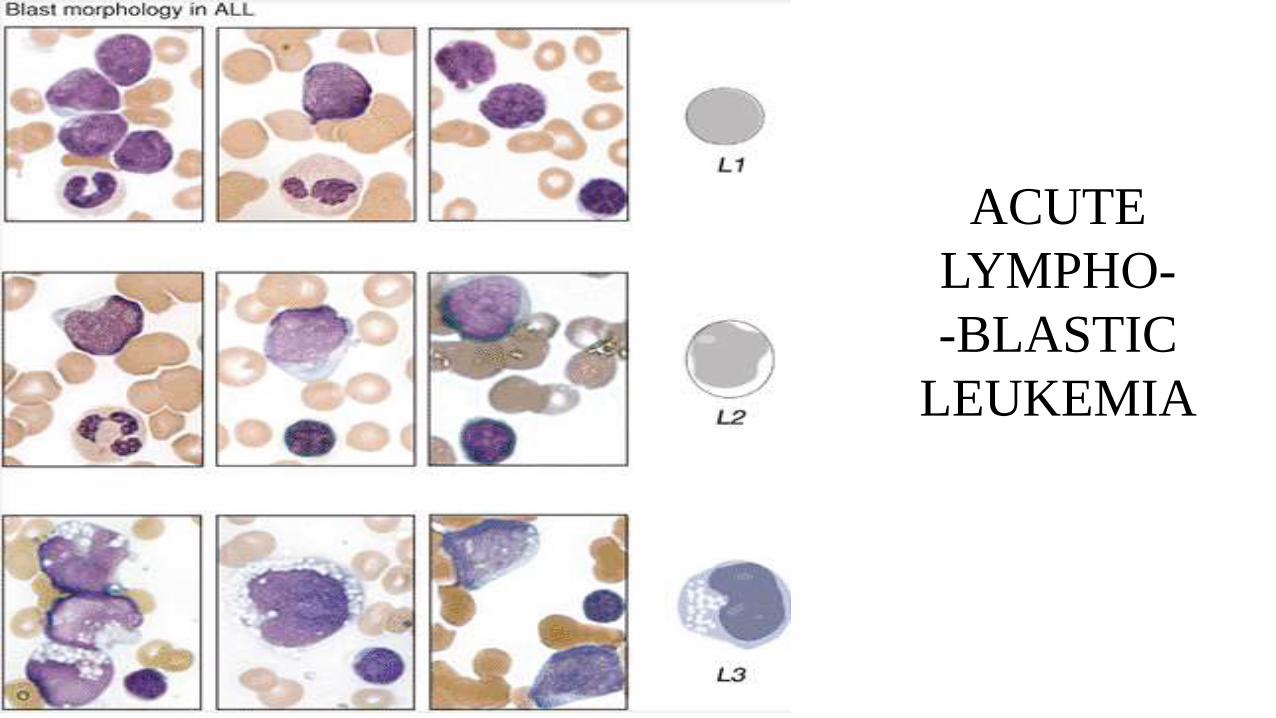
ACUTE
LYMPHO-
-BLASTIC
LEUKEMIA
CASE 6
HISTORY
• A 40 yrs old male complains of fever and
malaise.
• On examination had gum hypertrophy and
splenomegaly.
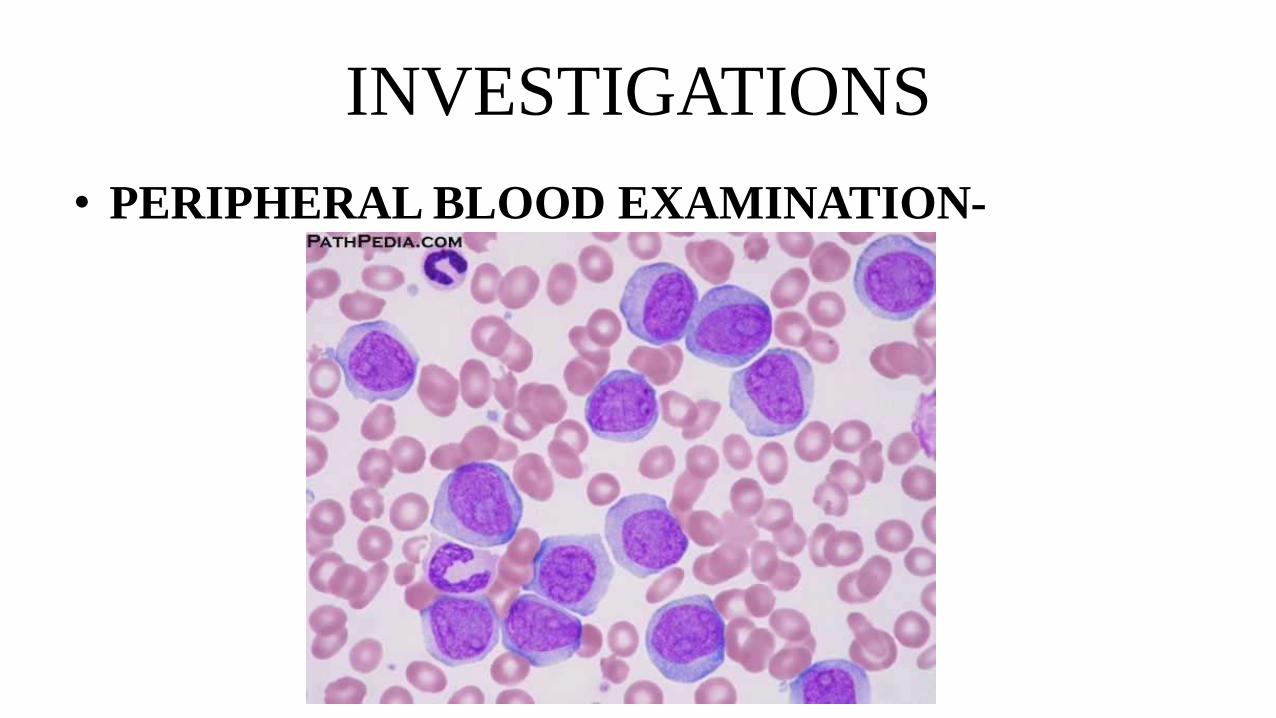
INVESTIGATIONS
• PERIPHERAL BLOOD EXAMINATION-
DIAGNOSIS
??
ACUTE MYELOID LEUKEMIA- M5
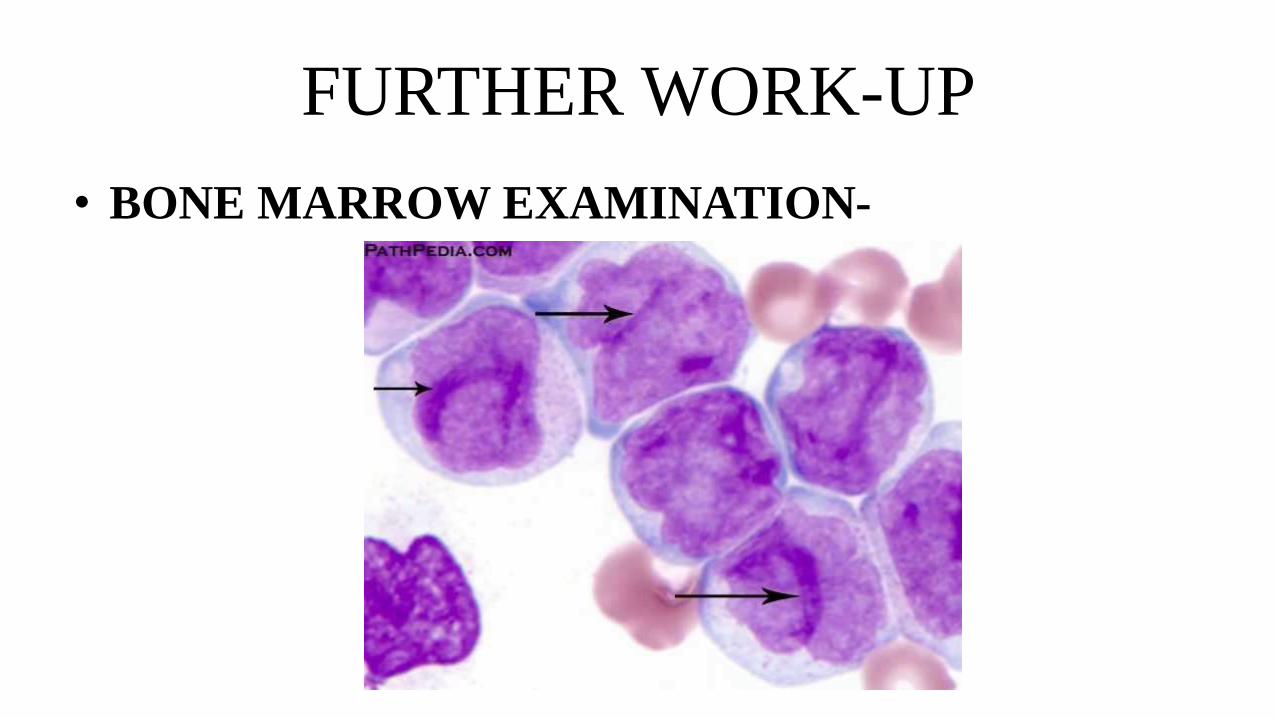
FURTHER WORK-UP
• BONE MARROW EXAMINATION-
CASE 7
HISTORY
• A 70 yrs old male patient complains of
fever and weakness.
• He has history of recurrent infections.
• History of unprovoked bleeding from skin
and gums.
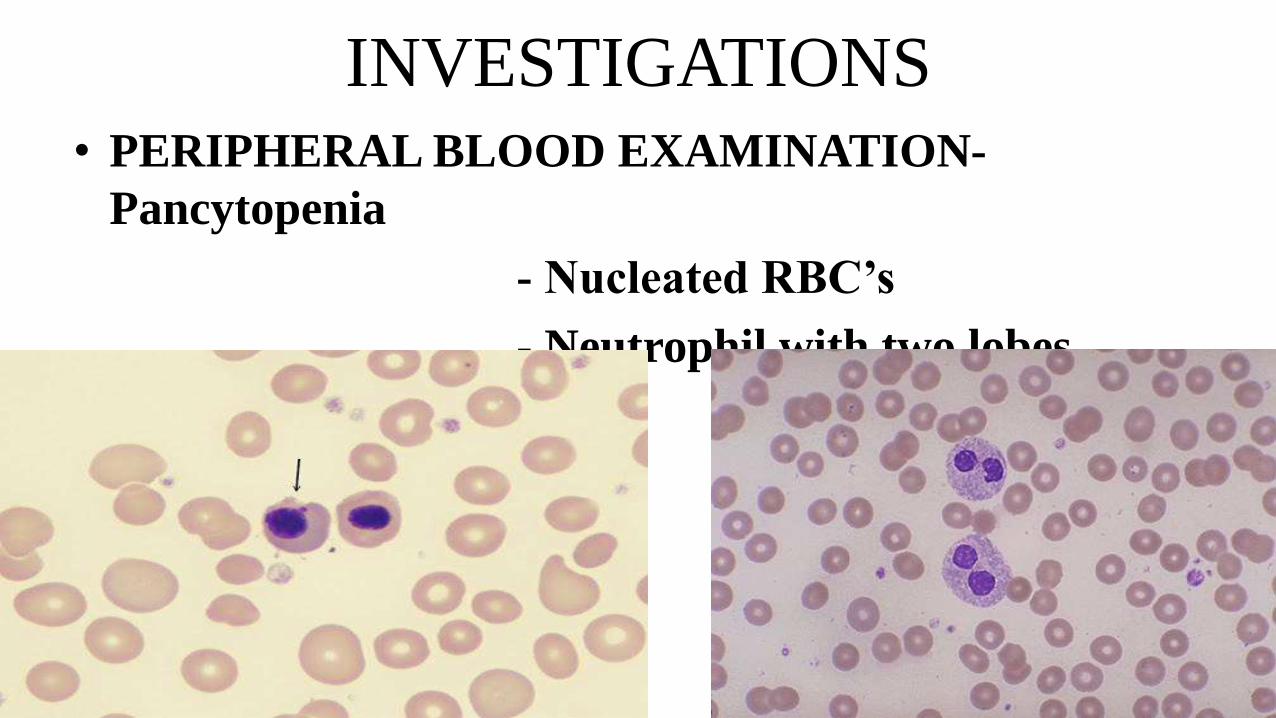
INVESTIGATIONS• PERIPHERAL BLOOD EXAMINATION-
Pancytopenia
- Nucleated RBC’s
- Neutrophil with two lobes
DIAGNOSIS??

FURTHER WORK-UP
• BONE MARROW EXAMINATION- Ring sideroblasts seen
- Megakaryocytes with multiple nuclei.
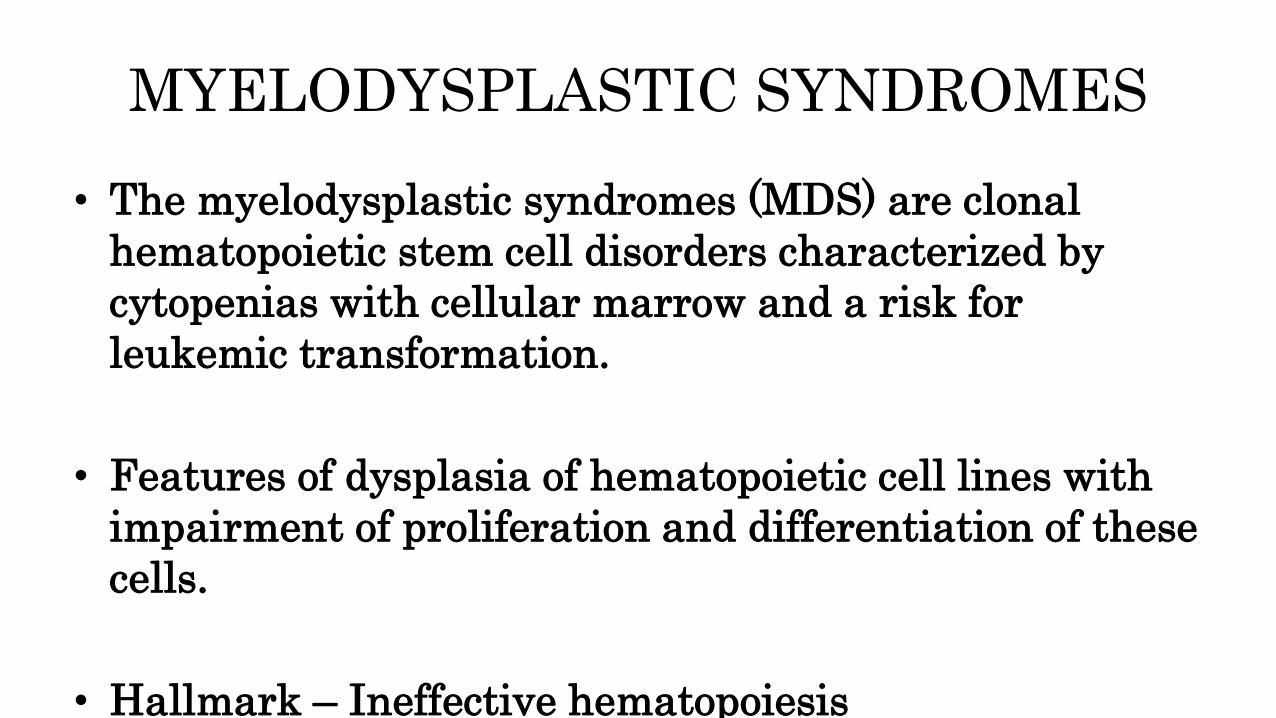
MYELODYSPLASTIC SYNDROMES
• The myelodysplastic syndromes (MDS) are clonal
hematopoietic stem cell disorders characterized by
cytopenias with cellular marrow and a risk for
leukemic transformation.
• Features of dysplasia of hematopoietic cell lines with
impairment of proliferation and differentiation of these
cells.
• Hallmark – Ineffective hematopoiesis
CASE 8
HISTORY
• A 40 yr old male presents with fever and cough.
• He also complains of fatigue and weakness.
• On examination shows enlarged cervical lymph
nodes.
INVESTIGATIONS
• CHEST X-RAY- Shows pleural effusion.
• PERIPHERAL BLOOD SMEAR-
Pancytopenia.

DIAGNOSIS??
FURTHER WORKUP
• BONE MARROW EXAMINATION-
Granuloma
• ZN STAIN- Shows acid fast bacilli.
• HIV POSITIVE
DISSEMINATED TUBERCULOSIS

Granuloma in a trephine biopsy section of
bone marrow from a
patient with AIDS and disseminated
atypical mycobacterial infection. H&E
Bone marrow granuloma from a patient with
AIDS and disseminated Mycobacterium avium
intracellulare infection. The macrophages
contain many acid-fast bacillli. Ziehl–Neelsen
stain
CASE 9

HISTORY
• Mr. A 55yrs old male patient, a railway
worker, consulted his doctor for tiredness,
malaise and anorexia.
• He was found to be mildly jaundiced with
an enlarged irregular hepatomegaly and
considerable ascites.
INVESTIGATIONS
• PERIPHERAL BLOOD SMEAR- Anisopoikilocytosis
- Macrocytosis
- Target cells
- Stomatocytes
DIAGNOSIS??
FURTHER WORKUP
• SONOGRAPHY- Enlarged spleen
• BONE MARROW EXAMINATION-
Normocellular marrow with hematopoeisis
• HEPATITIS VIRUS STUDIES- Negative for A,
B and C.
HYPERSPLENISM• Splenic hyperactivity with increased blood cell destruction.
Diagnostic criteria
1. Splenomegaly
2. Pancytopenia
3. Normal or hypercellular bone marrow
4. Reversibility by splenectomy
HAEMOPHAGOCYTIC SYNDROME
• Also called Hemophagocytic lymphohistiocytosis
Clinical features
• Fever
• Hepatosplenomegaly
• Jaundice
• Lymphadenopathy
• Rash
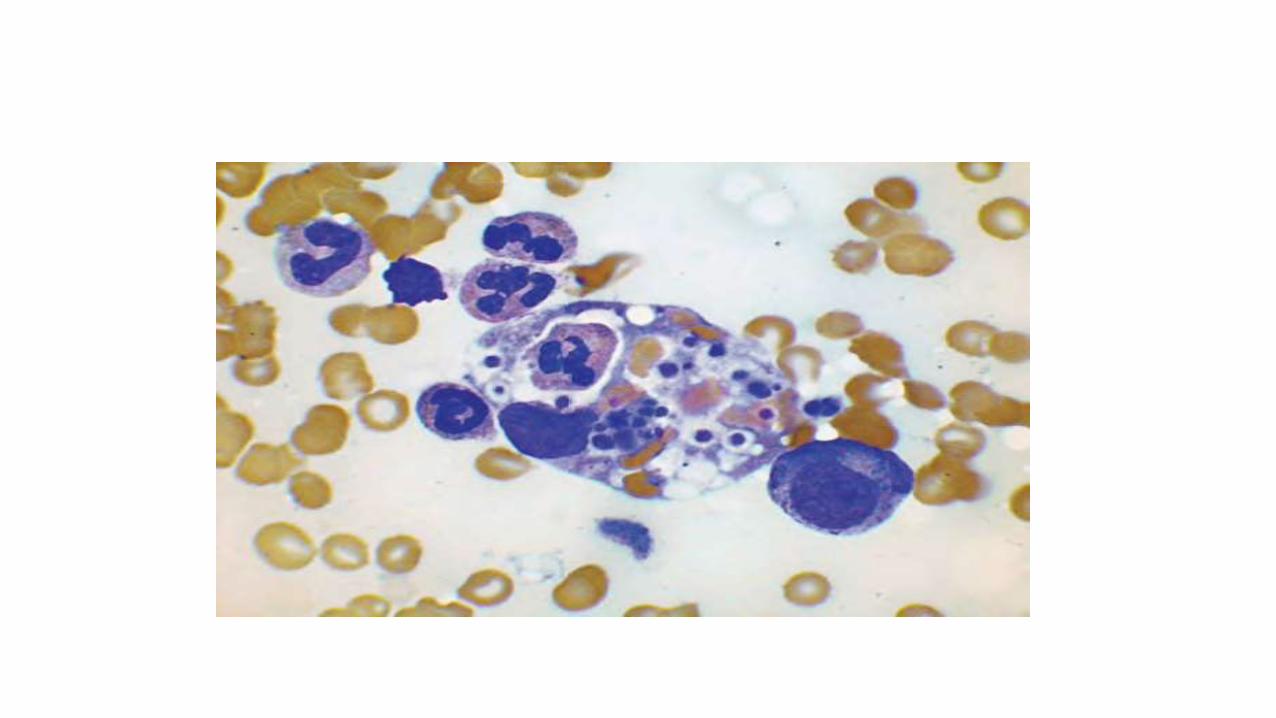
LABORATORY FINDINGS
• Histiocytosis
• Hemophagocytosis
• Pancytopenia
• Eleveted serum ferritin
• Elevated liver enzymes
DYSKERATOSIS CONGENITA
• RARE inherited disorder.
• X-linked Recessive, autosomal dominant,
autosomal recessive.
• Pancytopenia + dematological
manifestation.
• Nail dystrophy and leukoplakia.
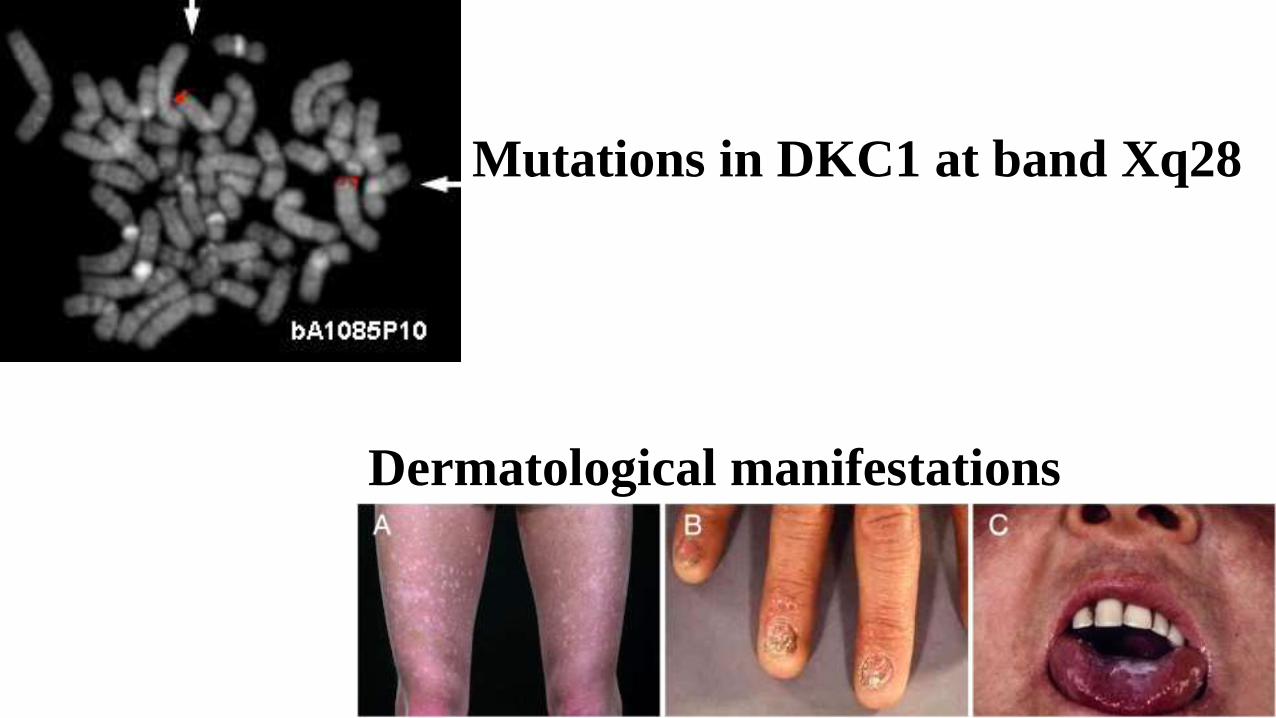
Mutations in DKC1 at band Xq28
Dermatological manifestations
INFECTIONS
• HIV
• Infectious mononucleosis
• Hepatitis B
• Hepatitis C
• Measles
• Hepatitis A
• Parainfluenza
• Influenza