h1n1 virus -update dr anna sharma mbbs msc mrcp(paeds) frcpch consultant paediatrician immunisation...
TRANSCRIPT

H1N1 virus -update
• Dr Anna Sharma• MBBS MSc MRCP(paeds)• FRCPCH• Consultant paediatrician• Immunisation clinical lead-
Hillingdon PCT

Structure of Influenza virus
• H=haemaglutinin• N=neuraminidase• Family of
orthomyxoviridae RNA viruses
• Infect humans pigs birds and horses

H1N1 virus -epidemiology

Flu pandemics
Name Year Deaths (millions) Subtype
• Russian Flu 1889-90 1 possibly H2N2
• Spanish Flu 1918-20 40 (?)H1N1
• Asian Flu 1957-58 1-1.5H2N2
• Hong Kong Flu 1968-69 0.75 H3N2
• New Jersey Flu 1976 H1N1
• Swine Flu 2009 -H1N1

What is a pandemic?
• Greek-pan=all,demos=people
• WHO definition– Emergence of a new infectious disease– Agents infect humans causing serious illness– Agents spread easily and sustainably among
humans

• Pandemic phases-WHO definitions

The 1918 pandemic
• 1918- a severe haemmorhagic disease
• Deaths by secondary infection- mainly pneumonia
• ‘Cytokine storm’ overwhelms healthy immune sytems
• Severe forms spread widely due to transport of infected soldiers in crowded trains to field hospitals

1918-19 epidemic-comparision of age profile with 1917 seasonal flu age
profile






Rate per 100,000 of new cases of pandemic influenza in England by
week and age group (17/09/09-HPA)

Antiviral prescriptions as of 17/09/09 (HPA)



Previous flu pandemics
‘Spanish flu’ 1918-19– H1N1
• Infected a third of the worlds population
• Killed 50 million in 6 months
• 200,000 died in UK• 2-3% mortality
‘Asian flu’ 1956-57– H2N2
• Mainly young children• Clinical attack rate 30%• Mortality<0.2%



UK mortality 1918figure taken from Center for Disease Control and Prevention USA

Pandemic of 1918 and now-comparision
• Started in one military installation in US
• Weakened population at end of war
• Affected mainly young adults• More serious cases often
travelled in crowded trains and in field hospitals- spreading infection
• Very rapid spread throughout the world
• Began to subside when doctors started to treat pneumonia with antibiotics
• Started in multiple generational community in Mexico
• Antivirals available before vaccine
• Heightened emergency preparedness due to alerts on anthrax/bioterrorism in 9/11
• Open and prompt monitoring of cases
• Recognised rating system to declare a pandemic
• Digital media communications• Containment of cases early on• Only milder cases tend to
travel and spread infection• Milder infection

Case Definition/Diagnostic criteria
• Fever >38 C or a history of fever
• AND• Influenza like illness-
TWO or more of– Cough– Sore throat– Rhinorrhoea– Joint /limb pains– Headache– Vomiting– Diarrhoea
• OR• Fever >38C• AND • Severe and/or life
threatening illness suggestive of an infection






Antivirals
• Tamiflu (Oseltamivir) • Relenza (nasal-more suitable for pregnant
women)• Not suitable for
– Pregnant women– Children under 1– Those in risk groups– Prophylaxis– Hot Line

Dose to prescribe antivirals in children
• Over 1 year• Oseltamivir capsules• <15 kg =30mg bd 5/7• 15-23 kg=45mg bd 5/7• 23-40 kg=60mg bd 5/7• >40 kg =75mg bd 5/7• Renal impairment• Possibly zanamivir

Under 1 year
Prescribe made up solution
• 15 mg in 1 ml • (Bitter taste)-syringe
graduated in mlCan get Tamiflu
suspension• 12 mg in 1 ml -syringe
graduated in mg• 2mg/kg bd 5/7
• Not licensed• Potential
neurotoxicity/• Encephalopathy• Could be ineffective in
<4 weeks old• RCPCH consensus
statement• So weigh up risks and
benefits
Side effects of oral antivirals
• Gastroenterological– Nausea– Abdominal pain– diarrhoea
• Neuropsychiatric– Irritability– Reduced concentration– Bad dreams– delusions

H1N1 virus -vaccines

Introducing a new vaccine
• Burden of disease• Availability of timely and safe treatment for
disease• Availability and efficacy of vaccine• Safety profile of vaccine• Disease profile (age/clinical groups)• Acceptability• Cost/effectiveness









Vaccine characteristics
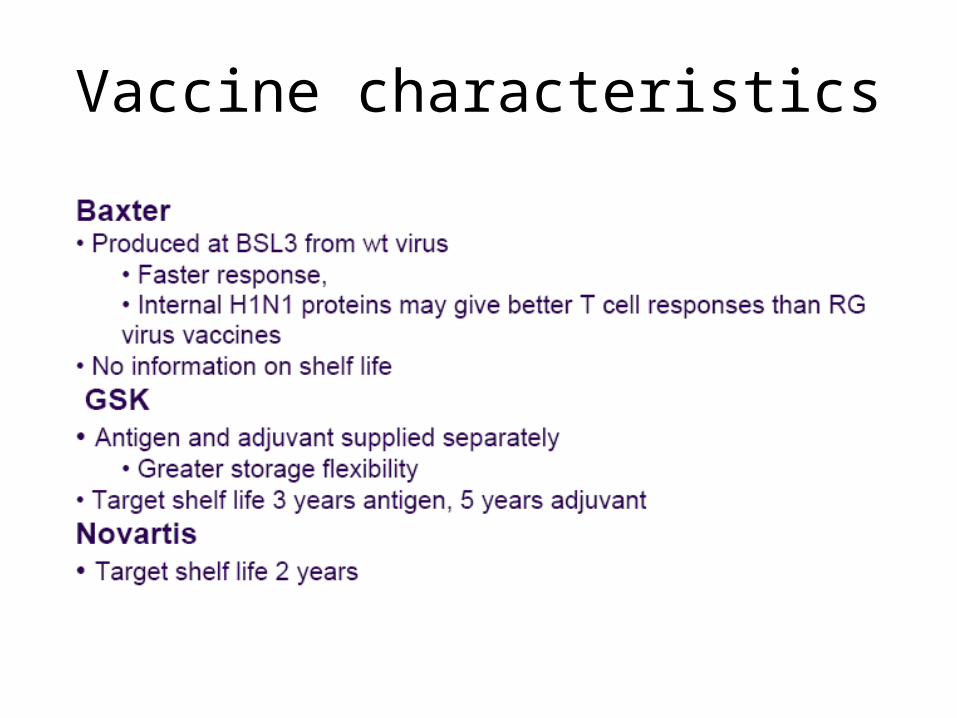
Vaccine characteristics
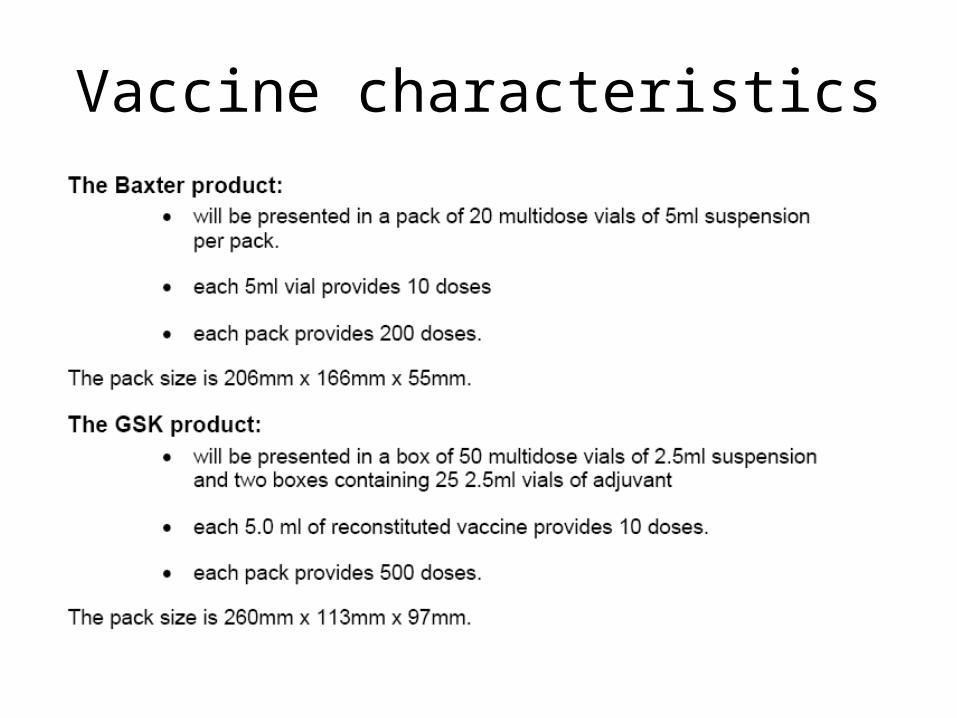
Vaccine characteristics



1976-New Jersey strain H1N1
• 40 million people vaccinated
• Vaccine withdrawn after 10 weeks
• 500 cases of Guillain Barre syndrome
• 25 deaths
• 8 fold increase in baseline incidence of Guillain Barre
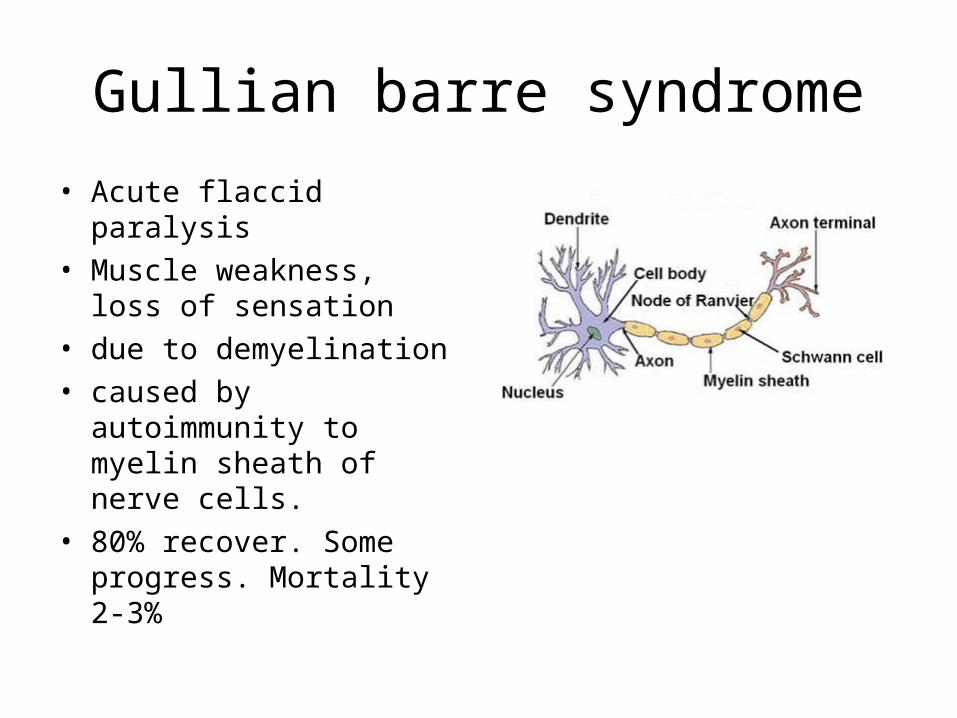
Gullian barre syndrome
• Acute flaccid paralysis • Muscle weakness, loss of
sensation• due to demyelination• caused by autoimmunity
to myelin sheath of nerve cells.
• 80% recover. Some progress. Mortality 2-3%

Fisher syndrome
• Variant of Guillain Barre
• Abnormal muscle co-ordination
• Paralysis of eye muscles
• Absent tendon reflexes
• Specific autoantibodies.
• Prognosis good
• Recovery within 2-4 weeks

• http://bpna.org.uk/audit/GBS/home.htm
• http://www.ich.ucl.ac.uk/clinical_information/clinical_guidelines/cmg_guideline_00007

Guillaine barre syndrome• Presenting problem(s)• History- ask about:• Onset and progression of weakness• Distribution and symmetry of weakness• Sensory symptoms (pain, parasthaesia)• Cranial nerve involvement (particularly
bulbar dysfunction, diplopia)• Gait disturbance• Sphincter disturbance• Symptoms of autonomic dysfunction
(sweating, palpitations)• Respiratory symptoms• History of recent infection/diarrhoea/fever• Medications (antibiotics, analgesics)
• Examination:• Primary assessment (ABCDE)• Conscious level (use modified Glasgow Coma
Scale)• Cranial nerve function including• Eye movements• Facial weakness• Bulbar function (speech, swallow, gag, cough,
drooling)• Peripheral neurological examination to include
evaluation of:• Motor deficit (tone, power, reflexes)• Ataxia• Sensory dysfunction (location, sensory level if
present)• Neck and spine (rigidity, tenderness, bruising)• Respiratory examination (include respiratory rate,
vital capacity, O2 sats) • Cardiovascular examination (include pulse, blood
pressure)• Abdominal examination (palpable bladder,
constipation, sensation, abdominal reflexes)

Guillain Barre-investigations• Blood tests• Full blood count• Urea& electrolytes, liver function tests• ESR• CRP• Blood culture• Swine flu antibody • Serology for mycoplasma, EBV, CMV,
Borrelia, VZV, coxsackie, campylobacter
• If indicated:– antiganglioside antibodies (anti-GQ1b
in MDS, anti-GM1 in AMAN)– Polio serology– Toxicology– Heavy metals (lead, mercury, arsenic)
• CSF (may be normal within 7 days of onset of symptoms)
• Cells• Protein• Glucose• Stool• M,C&S• Virology• Consider botulinum toxin• Urine• Consider toxicology, porphyrins• Throat swab• M,C&S• Viral culture

Guillain Barre- management
• Indications for PICU• Vital capacity <20mg/kg
or rapidly deteriorating• Rapidly progressive
tetraparesis with loss of head control
• Severe bulbar palsy• Severe autonomic
cardiovascular instability
• Indications for Immunoglobulin (see infusion schedule)
• Progressive deterioration at time of presentation
• Non-ambulent patient• Bulbar dysfunction• Respiratory compromise

Guillain Barre
• Other management considerations• Physiotherapy• Pain relief• S/C Heparin, anti-thrombotic stockings• Feeding/nutrition• Bed sore prevention, skin care• Eye care• Communication aids• Psychology





H1N1 virus –2009/10 vaccine programme



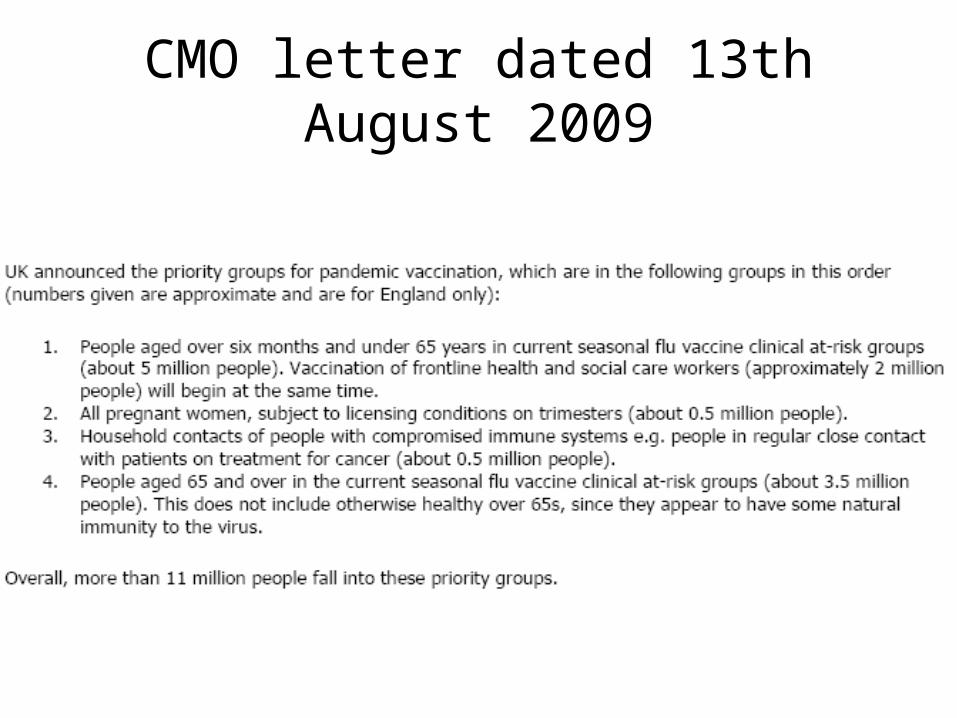
CMO letter dated 13th August 2009

Influenza vaccination plan in Hillingdon
• August/September 09– Vaccine programme planning– Health professionals’ training
• October 09– Delivery of vaccine, syringes and needles to
• Hillingdon Hospital• Mount Vernon Hospital• 2 other community sites
– Vaccination of health and social care workers, priority groups
• Seasonal flu vaccine to be offered with second dose of H1N1 flu vaccine

Vaccine uptake
• Uptake in 2008/9– 74.1% in over 65’s– 47.1% in clinical risk groups under 65– 16.5% in Staff nationally
– WHO target is 75%

Vaccination of health and social care professionals
• Occupational Health Services Programme via Hillingdon Hospital and Hillingdon Council.– GP’s, Practice Nurses– Hospital Staff (including cleaners)– PCT staff– Volunteer workers– Dentists, Community Pharmacists– Social care staff– Students, trainees in direct contact with patients– Staff in nursing care homes

Vaccination of priority groups
• People age 6 months to 65 years in clinical high risk groups to be offered seasonal flu vaccine and swine flu vaccine.– Identification and call/recall in primary care– ‘Primary care clusters’ to operate in the event
of staff shortage due to sickness/surge– Trained PCT nursing staff to be deployed to
assist vaccination sessions.– Records to be entered onto EMIS


Definition of ‘High risk’ groups
• Immunosuppressed
• Long term respiratory illness
• Long term renal illness

Clinical risk groups-contd

Clinical risk groups-contd

Vaccination of Priority groups
• ‘All pregnant women subject to licensing conditions’ Pregnant women in their 2nd and 3rd trimester– Identification and call/recall in primary care
assisted by midwives (community/hospital)– Information given by midwives– Vaccination in primary care– Data entry onto EMIS checked by midwives.

Priority groups
• Household contacts of the immunosupressed

Priority groups contd
• Over 65’s in clinical risk groups

Data recording/consent
• PGD to cover vaccine
• Staff trained to national minimum standards for immunisation
• Consent informed via leaflet/discussion
• Immunisation data recorded on patient record (pchr/card)
• And on EMIS/Occupational health data base

Monitoring side effects
• Record in notes
• MHRA ‘yellow card’ system
• BPSU ‘orange card’ surveillance system
• BNSU



Notification of new cases-europe-WHO update

Notification of new cases- world-WHO update

