Gout in the Elderly: Updates on an Ancient Disease is a single disease process but is often classified into 4 different stages. The common denominator linking these 4 stage\ , which
59
Gout in the Elderly: Updates on an Ancient Disease Ted R. Mikuls, MD, MSPH Associate Professor June 25, 2010
Gout in the Elderly: Updates on an Ancient DiseaseTed R. Mikuls, MD, MSPHAssociate ProfessorJune 25, 2010
Objectives
• Discuss the impact of gout in the primary care of the elderly.
• Explore issues regarding the diagnostic approach and treatment of gout.
• Evaluate new gout therapies being examined in phase III trials.
Gout: Sydenham’s Description“…the victim goes to bed and sleeps in good health. About 2 o’clock in the morning he is awakened by a severe pain in the great toe…this pain is like that of a dislocation, and yet the parts feel as if cold water were poured over them…it is a violent stretching and tearing of the ligaments... the night is passed in torture…”
The Vet’s Description
“I’ve been shot, beat up, stabbed and thrown out of a helicopter, but none of that compared to the gout.”
- Birmingham, AL VAMarch, 2001
Serum Urate, Hyperuricemia, and Gout
• Serum urate (uric acid): formed in process of purine metabolism / degradation
• Hyperuricemia: serum urate values in excess of 6.8 mg/dl
• Gout: inflammatory arthritis developing as a consequence of urate deposition in the joint
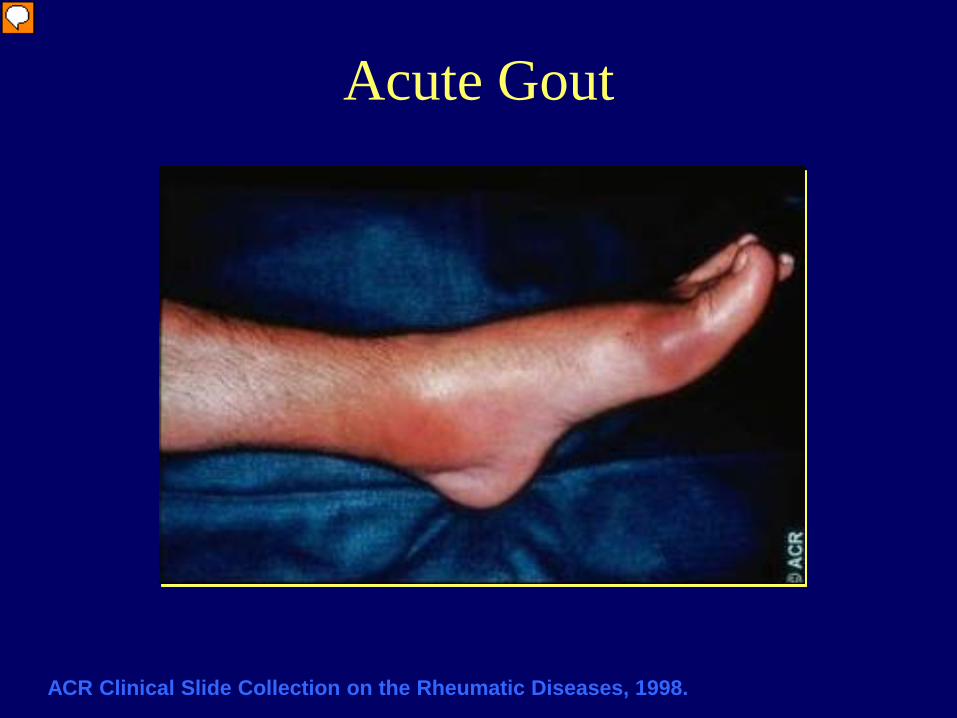
Acute Gout
ACR Clinical Slide Collection on the Rheumatic Diseases, 1998.
Presenter
Presentation Notes
This photo demonstrates a patient who is experiencing classic podagra and ankle inflammation as a result of an acute flare of gout. This patient’s condition may be mistaken for cellulitis, but gout should be considered because this marked erythema is occurring around a distal joint.
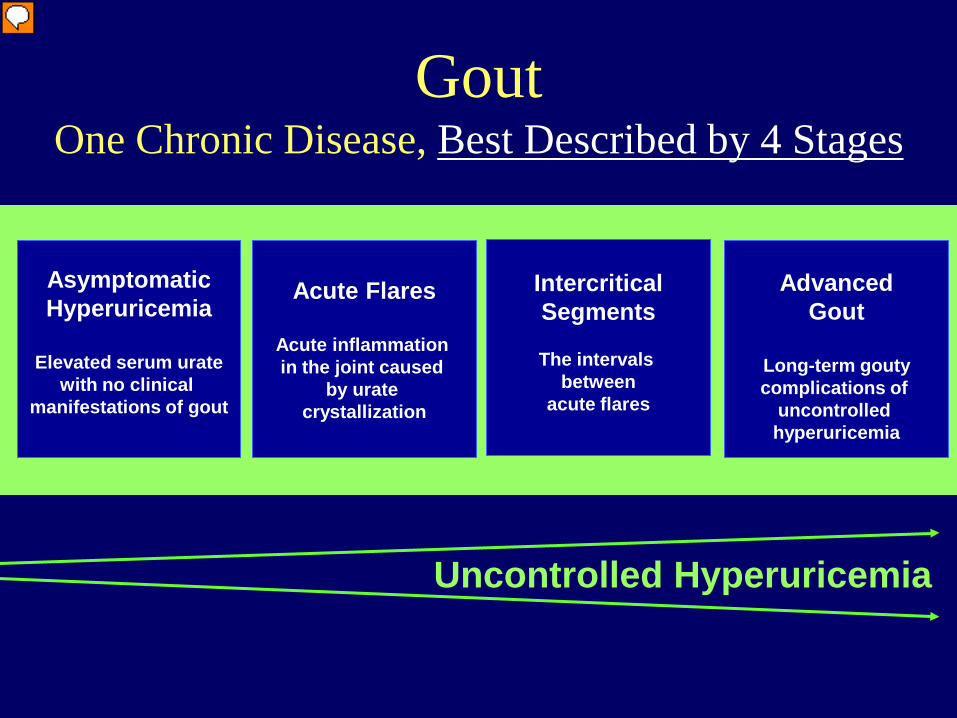
GoutOne Chronic Disease, Best Described by 4 Stages
AdvancedGout
Long-term goutycomplications of
uncontrolled hyperuricemia
IntercriticalSegments
The intervals between
acute flares
Acute Flares
Acute inflammation in the joint caused
by urate crystallization
AsymptomaticHyperuricemia
Elevated serum uratewith no clinical
manifestations of gout
Uncontrolled Hyperuricemia
Presenter
Presentation Notes
Gout is a single disease process but is often classified into 4 different stages. The common denominator linking these 4 stages, which is the underlying cause of this disease and associated chronicity, is uncontrolled hyperuricemia. The asymptomatic hyperuricemia stage is when the patient has elevated levels of uric acid, but no previous episode of an acute flare or other clinical indication of the disease. During this phase, however, monosodium urate crystals may “silently” deposit in the tissues and joints and result in “hidden damage,” which can occasionally occur over time even in the absence of clinical gout. Acute flares occur as a result of the deposition of urate crystals and activation of an inflammatory response. This causes symptoms such as inflammation and intense pain. Over time, or with the help of agents to terminate the acute flare, the flare will subside. Although the patient is not experiencing a flare during this time, the patient is still considered to have gout and is in the intercritical stage until another flare occurs. Uncontrolled hyperuricemia and resultant gout can eventually evolve into the advanced stage of the disease.
Severe Joint Involvement From Gout
Photo courtesy of N. Lawrence Edwards, MD, University of Florida.
Presenter
Presentation Notes
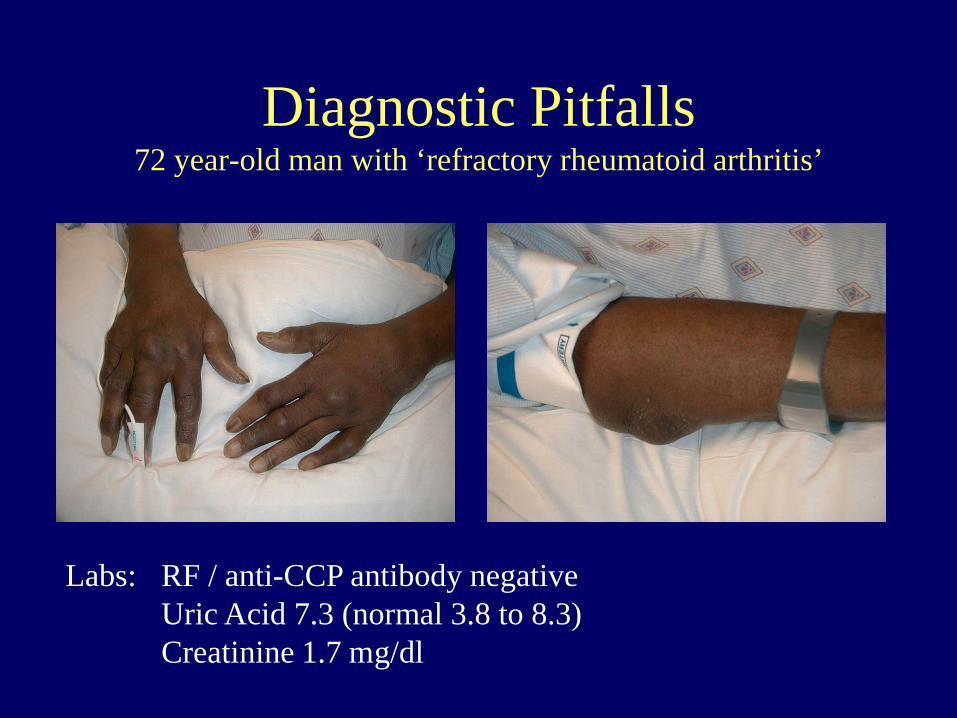
Extensive joint destruction is noted in the wrists, MCPs, PIPs, and DIPs of both hands. Classic gout erosions with "overhanging edges" are demonstrated in the left first MCP, the left third PIP, and the right third DIP (red circles). The typical soft tissue swelling and density of tophaceous deposit is noted around the fourth DIP.
Advanced Gout:Clinically Apparent Tophi
1
1. Photos courtesy of Brian Mandell, MD, PhD, Cleveland Clinic.2. Photo courtesy of N. Lawrence Edwards, MD, University of Florida.3. ACR Clinical Slide Collection on the Rheumatic Diseases, 1998.
21
3
Presenter
Presentation Notes
The advanced gout stage is often referred to as chronic tophaceous gout to indicate the presence of this clinical manifestation, which will remain unresolved in the absence of urate-lowering therapy. Tophi are characterized by solid urate deposits in connective tissues that produce irregular nodularities and joint destruction. In addition, the skin overlying the tophi may become ulcerated and exude a white, chalky material. Shown here are some common sites of tophi, including dermal tophi on the finger, periarticular tophi on the hands, and tophi on the helix of the ear. The patient who was experiencing the intradermal tophi on the knees was diagnosed and treated by multiple generalists and specialists for osteoarthritis. This photo was taken during his self-referred first visit to a rheumatologist and reinforces the point that gout is a disease that is under-recognized.1 The patient with polyarticular involvement of his hands had been misdiagnosed and treated for rheumatoid arthritis for 8 years.2 The tophi exhibited on this slide are clinically apparent, but this may not always be the case, as was seen in the previous case study examples of the tophi that formed in the bone of the knee and the palm of the hand. 1. Patient case study courtesy of Brian Mandell, MD, PhD, Cleveland Clinic. 2. Patient case study courtesy of N. Lawrence Edwards, MD, University of Florida.
Epidemiology: Incidence of Gout in U.S.• Annual Incidence
– 8 per 10,000 person-years in Framingham1
– 28 per 10,000 for male veterans2
• Cumulative Incidence – 8.6% cumulative incidence in US white male doctors3
• Increasing incidence?– Age and sex-adjusted incidence of gout in 3 decades increased 1.5-fold
using ACR gout criteria in Rochester4
– Two-fold increase in primary gout
1. Abbott RD et al. J Clin Epidemiol 1988;41:2372. Champion EW. et al. Am J Med 1987;82:421 3. Roubenoff R. et al. JAMA 1991;266:30044. Arromdee E. et al. J Rheumatol 2002;29:2403
Presenter
Presentation Notes
Framingham Study, using biennial physical examination, observed an annualized incidence rate (based on the number of new cases per person-bienniums at risk) of 0.84 per 1,000 person-years [Abbott, 1988 #11]. Among men in the Framingham Study [Abbott, 1988 #11], the overall gout incidence rate was 1.6 cases per 1,000. Roubenoff Study of gout in U.S. white men followed over 29 years. Johns Hopkins Precursors study, a prospective study of medical students enrolled from. Roubenoff and colleagues [Roubenoff, 1991 #14], using patient self-report, observed a similar incidence rate (1.7 cases per 1,000 patient-years) among male participants in the Johns Hopkins Precursors Study, a prospective cohort study involving medical students 48-64. Average incidence was 1.73 per 1000 person-years of follow-up. Incidence of gout was even higher in a study of Africian American medical students at Meharry. Docs may not be representative The Normative aging study (Champion) was a longitudinal study of aging in men that began in 1963, which examined the incidence of gout in relationship to urate levels. In contrast, gout incidence among otherwise healthy male Veterans over a 15-year follow-up period was found to be 2.8 cases per 1,000 patient-years [Campion, 1987 #25]. The higher disease incidence noted in the latter study may relate to the relatively older population that was studied or differences in the frequency of select comorbidity or medication use that may have predisposed this population to gout. Normative aging study consisted of 2000 healthy men followed for 14.9 years Incidence 4.9%/yr (not shown) In a study using the U.S. Rochester Epidemiology Project database and ACR Classification Criteria for gout diagnosis, investigators compared the age-adjusted gout incidence in 1995-96 with that of 1977-78 [Aromdee, 2002 #6]. Over this twenty-year interval, gout incidence increased from a baseline of 45.0 per 100,000 person-years (95% CI: 31.7-59.3) to 62.3 per 100,000 (95% CI: 48.4-76.2). Notably, investigators observed a two-fold increase in the incidence of primary gout (i.e. no history of diuretic exposure) (p = 0.002 for difference) over the same time period. In a study of the U.K. GPRD using physician diagnostic codes, the overall 1999 gout incidence was found to be 1.31 cases per 1,000 patient-years of follow-up (95% CI: 1.26-1.37) [Mikuls, 2004 #17].
Prevalence of Gout• Most common inflammatory joint disease in men
>40 years• Prevalence varies by study population
– US National Health Interview Survey of 1996 on self-reported prevalence♦ Prevalence estimated at 1.56 million men and 550,000 women1
♦ 4.6% in men, 2% in women in highest risk group2
♦ Increased from 0.5% of cases in 1969 to 1% of cases in 1996
1. Lawrence R. Arthritis Rheum. 1998;41:7782. Adams et al. http://www.cdc.gov/nchs/data/series/sr_10/sr10_200.pdf
Presenter
Presentation Notes
Estimated that 5 million adults have had gout. NHIS-- “have you or any member of your household had gout within the past year”NHIS- data shown is for those 65 to 74 yrs (average for this age range is 3.2% by self-report) Double over period from 69 to 96 but largely stable in past decade VA survey from Dr. Schumaker Lawerence estimates 8.5/1000 of ages 18 and above all sexes, races combined (from Silman Epi book) Using a large U.K. practice registry in the mid-1970’s, Currie observed an overall gout prevalence of 2.6 cases per 1,000 [Currie, 1979 #7] among the adult population. Employing a similar study methodology in 1993, Harris and colleagues found that overall gout prevalence had increased by approximately three-fold (9.5 cases per 1,000) from the time of Currie’s prior report [Harris, 1995 #8]. In a more recent study examining enrollees of the U.K. General Practice Research Database (GPRD), investigators observed the overall gout prevalence to be even higher at 13.9 cases per 1,000 [Mikuls, 2004 #17]. Similar trends in disease prevalence have been reported elsewhere. In a population-based survey from New Zealand, investigators observed the overall gout prevalence (in patients over 15 years of age) to be 4.7% [Klemp, 1997 #16], an estimate that had nearly doubled over the previous thirty years [Prior, 1966 #22]. U.S. data on gout prevalence comes from two primary sources, the National Health Interview Survey (NHIS; from 1969 to 1992) [Lawrence, 1998 #23; Lawrence, 1989 #24; Benson, 1992 #12] and the Framingham study [Hall, 1967 #10; Abbott, 1988 #11]. In the late 1960’s, investigators from the Framingham study reported a gout prevalence of 28.5 and 3.9 cases per 1,000 among adult men and women, respectively, over the age of 32 years [Hall, 1967 #10]. The NHIS, based on patient self-report, showed that the overall gout prevalence doubled during the interval from 1969 to the mid-1980’s before reaching a nadir of 8.6 cases per 1,000 in 1992 [Lawrence, 1989 #24; Lawrence, 1998 #23].
– Metabolic syndrome• Low-dose ASA• Thiazides• CSA and others
• Fructose intake• Decreased HRT (WHI
results)• Other
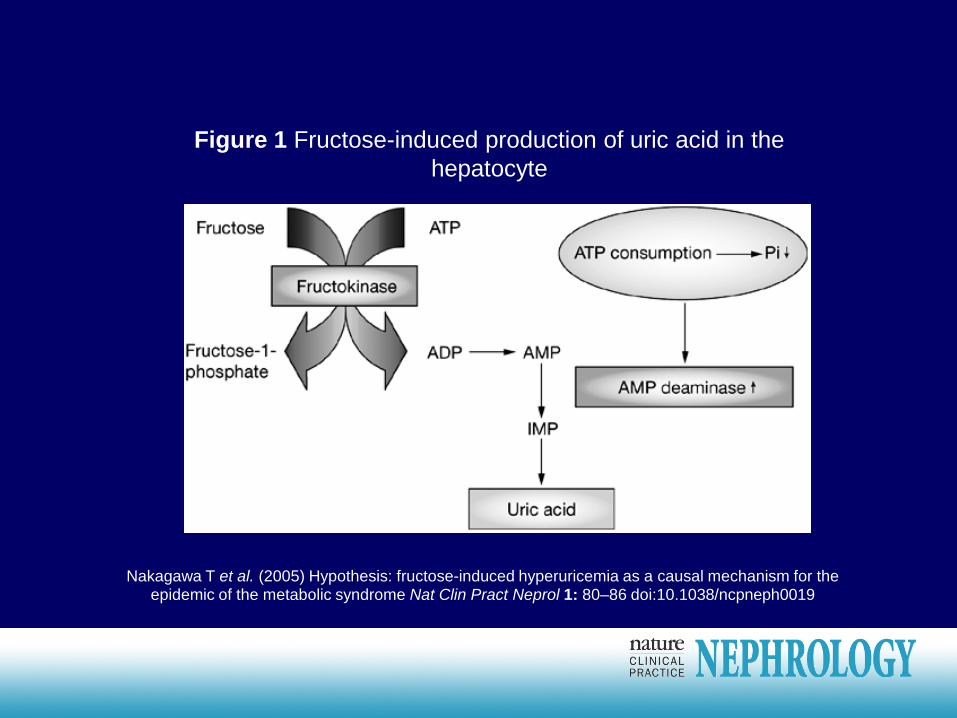
Nakagawa T et al. (2005) Hypothesis: fructose-induced hyperuricemia as a causal mechanism for theepidemic of the metabolic syndrome Nat Clin Pract Neprol 1: 80–86 doi:10.1038/ncpneph0019
Figure 1 Fructose-induced production of uric acid in the hepatocyte
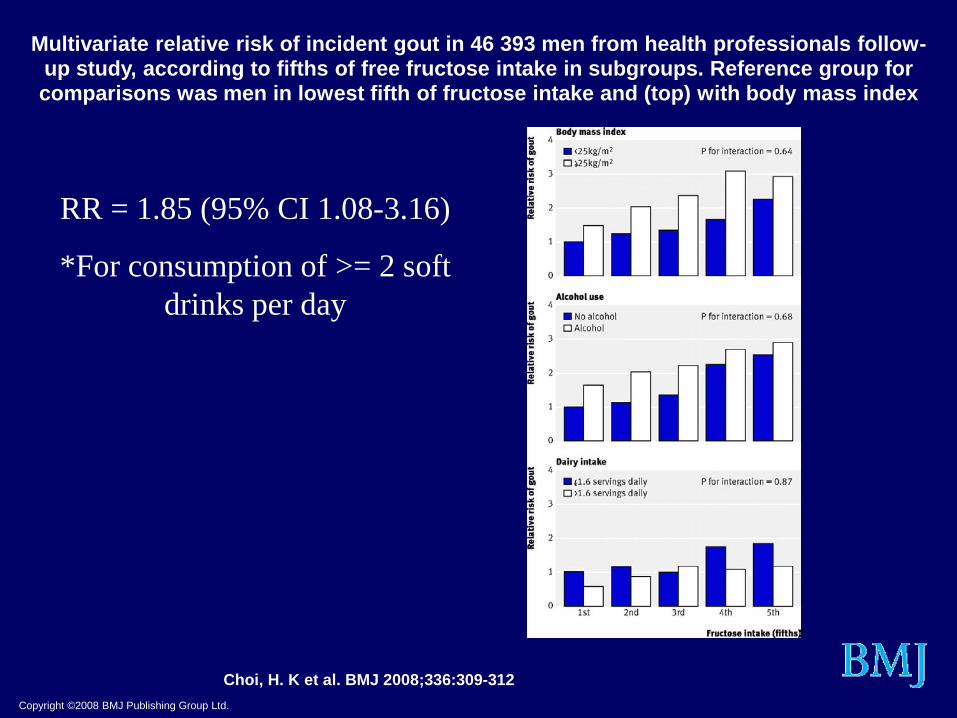
Multivariate relative risk of incident gout in 46 393 men from health professionals follow-up study, according to fifths of free fructose intake in subgroups. Reference group for comparisons was men in lowest fifth of fructose intake and (top) with body mass index
RR = 1.85 (95% CI 1.08-3.16)
*For consumption of >= 2 soft drinks per day
Gout Prevalence, GPRD 1999
0
10
20
30
40
50
60
70
80
< 55 years 55-64 years 65-74 years 75-84 years > 85 years TotalAge group
Prev
alen
ce p
er 1
,000
pat
ient
s
Men
Women
Men and Women
Mikuls T. et al Ann Rheum Dis, in press
Gout Prevalence, GPRD 1999
0
10
20
30
40
50
60
70
80
< 55 years 55-64 years 65-74 years 75-84 years > 85 years TotalAge group
Prev
alen
ce p
er 1
,000
pat
ient
s
Men
Women
Men and Women
Mikuls T. et al Ann Rheum Dis, in press
Hippocrates’ Aphorisms• Eunuchs do not take the
gout• Woman does not take
the gout unless her menses has ceased
• A young man does not become susceptible to gout until the time of indulging in copulation
460-357 B.C.
“…like sugar candy on a string…”- Sir Alfred Barring Garrod
Purine Degradation to Uric Acid
• Xanthine oxidase catalyzes the final conversions to uric acid
Purine nucleosides
Xanthineoxidase
Xanthineoxidase
Purine nucleotides
Hypoxanthine
NHN
N N
OH
HO
XanthineN
N
NH
OH
N
OH
Uric acidN
N
NH
OH
HO
N
Renal Excretion
Presenter
Presentation Notes
Purine nucleotide degradation proceeds through purine nucleoside and purine base (hypoxanthine and xanthine) intermediates to uric acid. In the final steps of degradation, hypoxanthine and xanthine are irreversibly oxidized to uric acid in reactions catalyzed by the enzyme xanthine oxidase. Xanthine oxidase is an important pharmacologic target for inhibition of uric acid production in states of hyperuricemia and gout. For a schematic overview of the production and elimination of uric acid, please see slide 2 in the supplement. For a detailed description of the synthesis and degradation of purines, please see slide 3 in the supplement.
The physicochemical definition of hyperuricemia is any concentration of serum urate at or above 6.8 mg/dL. At this value, urate is no longer soluble and crystallization may occur. When examining the distribution of urate in men and women from 1965 data and using this physicochemical definition of hyperuricemia (click to display this value on the graph), it is evident that many men and a smaller percentage of women in the general population have hyperuricemia.1 Because men tend to have higher serum urate levels than women, most laboratories utilize a normative range of serum urate for men and a normative range of serum urate for women. However, regardless of the patient’s gender and the serum urate cutoffs assigned by individual laboratories, serum urate crystallizes at a concentration at or above 6.8 mg/dL in all patients, at which point they are hyperuricemic. 1. Mikkelsen et al. Am J Med. 1965;39:242-251.
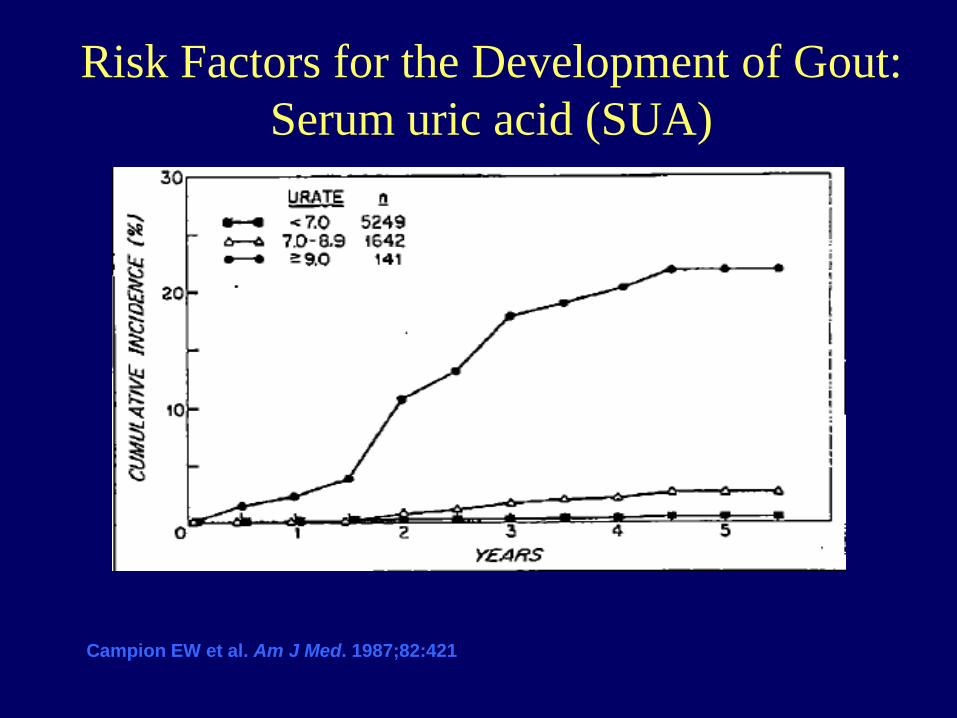
Risk Factors for the Development of Gout:Serum uric acid (SUA)
Campion EW et al. Am J Med. 1987;82:421
Risk Factors for the Development of Gout:Sex and Age
1. Abbott RD et al. J Clin Epidemiol 1988;41:2372. Arromdee E et al. J Rheumatol 2002;29:2403
• Men– Have higher serum urate levels
– In younger patients, gout overwhelmingly in men (~9:1 in subjects under 40 yrs)
• Women– Increased risk after menopause
♦ Decreased estrogen may diminish the renal excretion of uric acid
– Of gout patients older than 60, half are women
– Prevalence increasing along with increasing longevity
Presenter
Presentation Notes
Asymptomatic hyperuricemia usually develops in males during puberty and develops as gout 20 to 30 years later Tophi usually develop 11.6 years later if HUA goes untreated Rott paper is a more recent review
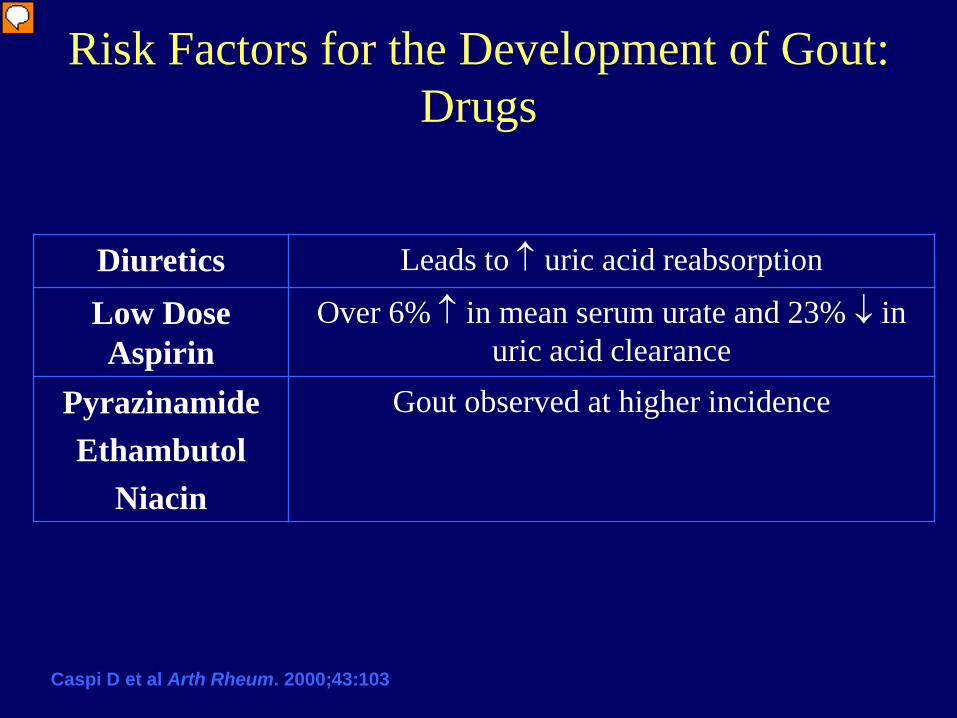
Risk Factors for the Development of Gout:Drugs
Diuretics Leads to ↑ uric acid reabsorption
Low Dose Aspirin
Over 6% ↑ in mean serum urate and 23% ↓ in uric acid clearance
PyrazinamideEthambutol
Niacin
Gout observed at higher incidence
Caspi D et al Arth Rheum. 2000;43:103
Presenter
Presentation Notes
Lasix and diazoxide initiate hyperlacticadidemia suppressing urate secretion Low dose asprin- elderly pateints on 75 mg ASA per day had changes shown PZA, ETH, and Niacin suppress uric acid secretion. Capsi paper on low dose ASA
Risk Factors for the Development of Gout:Transplant Patients
Nephrolithiasis (uric acid stones or calcium oxalate stones with a uric acid core) develops in the kidney when the urinary pH is low with or without high levels of uric acid being filtered through the kidney. A risk factor for the development of nephrolithiasis appears to be decreased ammonium excretion, which increases the acidity (decreases the pH) of the urine. Recent data has identified that this defect is also present in patients that have the metabolic syndrome, so this may be the common link between the disorders. The picture is an MRI of the kidney. The green arrow points to the presence of a uric acid stone.
Comorbidities Associated WithHyperuricemia That Warrant Consideration
• Obesity1,2
• Metabolic syndrome3
• Diabetes mellitus4
• Heart failure5
• Hyperlipidemia1
• Hypertension6,7
1. Nakanishi et al. Int J Epidemiol. 1999;28(5):888-893.2. Denzer et al. J Ped Endo Met. 2003;16:1225-1232. 3. Ford et al. JAMA. 2002;287:356-359.4. Boyko et al. Diabetes Care. 2000;23(9):1242-1248.5. Anker et al. Circulation. 2003;107:1991-1997.6. Gavin et al. Am J Cardiovasc Drugs. 2003;3(5):309-314.7. Feig et al. Hypertension. 2003;42:247-252.
Presenter
Presentation Notes
Multiple studies involving the listed disease states have suggested that hyperuricemia is related to each of them. These are key findings because the prevalence of the conditions has increased in the current population. Therefore, uncontrolled hyperuricemia, and the subsequent risk of gout, may be present in patients whose serum urate has never been assessed. Hyperuricemia is positively correlated with obesity.1 This was reinforced in one study of adolescents, which showed a higher BMI was associated with elevated uric acid.2 Hyperuricemia is considered to be a facet of the metabolic syndrome, along with abdominal obesity, hypertriglyceridemia, low high-density lipoprotein cholesterol, hypertension, and high fasting glucose.3 Insulin resistance is suspected to raise uric acid. An increased incidence of impaired glucose tolerance and diabetes in previously normal glucose-tolerant patients was found to be associated with hyperuricemia.4 One study demonstrated that hyperuricemia is a strong, independent marker of impaired prognosis in heart failure.5 Another study found hyperuricemia to be strongly correlated with serum triglycerides, with a weaker correlation with serum cholesterol.1 Half of untreated hypertensive patients were found to have hyperuricemia.6 Elevated uric acid has been found to precede hypertension and correlate with blood pressure in children.7 For more information on the association between hyperuricemia and hypertension, please see slides 29-30 in the supplement. 1. Nakanishi et al. Int J Epidemiol. 1999;28(5):888-893. 2. Denzer et al. J Ped Endo Met. 2003;16:1225-1232. 3. Ford et al. JAMA. 2002;287:356-359. 4. Boyko et al. Diabetes Care. 2000;23(9):1242-1248. 5. Anker et al. Circulation. 2003;107:1991-1997. 6. Gavin et al. Am J Cardiovasc Drugs. 2003;3(5):309-314. 7. Feig et al. Hypertension. 2003;42:247-252.
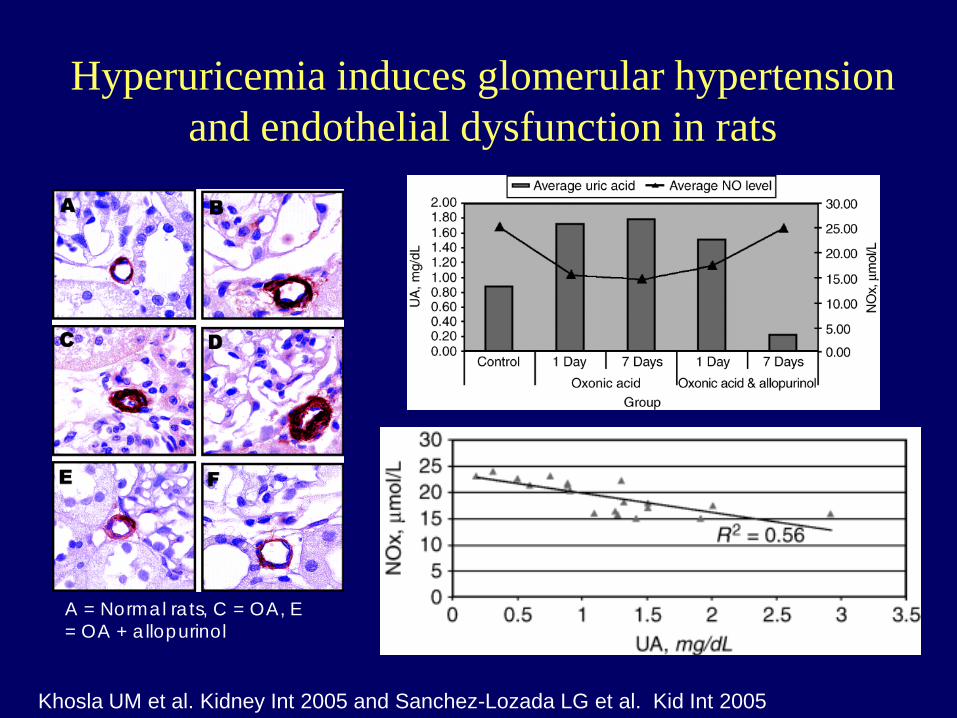
Hyperuricemia induces glomerular hypertension and endothelial dysfunction in rats
Khosla UM et al. Kidney Int 2005 and Sanchez-Lozada LG et al. Kid Int 2005
A = Normal rats, C = OA, E = OA + allopurinol
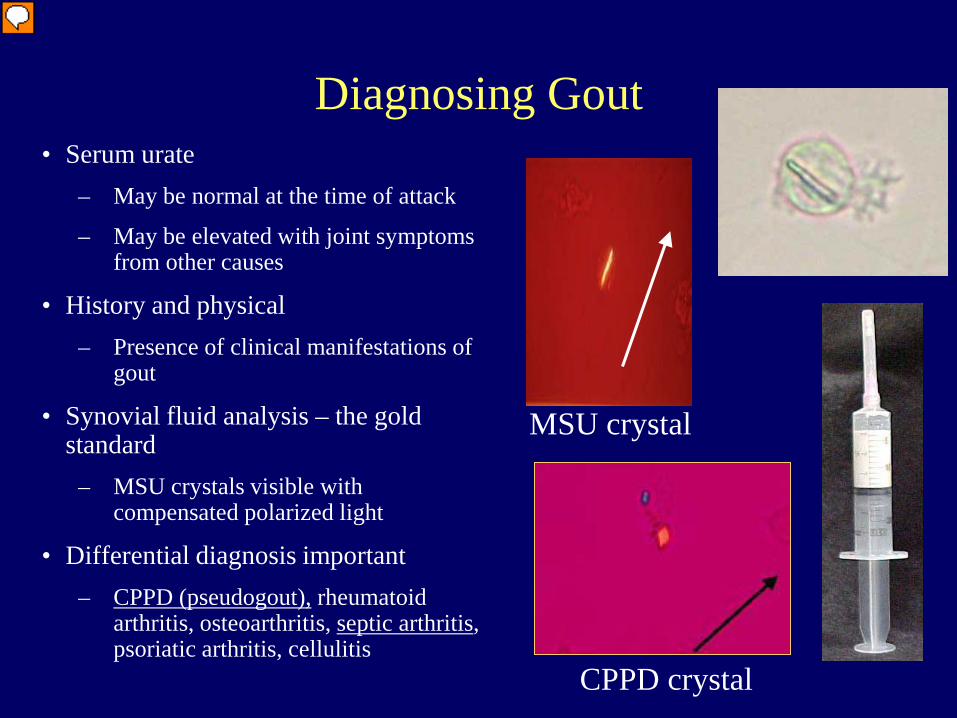
Diagnosing Gout• Serum urate
– May be normal at the time of attack
– May be elevated with joint symptoms from other causes
• History and physical– Presence of clinical manifestations of
gout
• Synovial fluid analysis – the gold standard
– MSU crystals visible with compensated polarized light
Serum urate is neither sensitive nor specific when diagnosing gout because it may be normal at the time of an attack or it may be elevated in the absence of gout. It is therefore an unreliable marker in diagnosing gout. The history and physical are important when diagnosing gout because the clinical manifestations are the first indicators of gout that the physician encounters in a gout patient. The gold standard for confirming a gout diagnosis, however, is a synovial fluid analysis for urate crystals under compensated polarized light. Gout can be mistaken for a number of rheumatic diseases, so it is also important to recognize how gout differs from these diseases in terms of clinical presentation and laboratory evaluations.
The physicochemical definition of hyperuricemia is any concentration of serum urate at or above 6.8 mg/dL. At this value, urate is no longer soluble and crystallization may occur. When examining the distribution of urate in men and women from 1965 data and using this physicochemical definition of hyperuricemia (click to display this value on the graph), it is evident that many men and a smaller percentage of women in the general population have hyperuricemia.1 Because men tend to have higher serum urate levels than women, most laboratories utilize a normative range of serum urate for men and a normative range of serum urate for women. However, regardless of the patient’s gender and the serum urate cutoffs assigned by individual laboratories, serum urate crystallizes at a concentration at or above 6.8 mg/dL in all patients, at which point they are hyperuricemic. 1. Mikkelsen et al. Am J Med. 1965;39:242-251.
Pitfalls in Gout Diagnosis• Can be polyarticular and chronic, especially in the elderly (20%
polyarticular)
• Systemic symptoms can be observed
• Urate levels can be normal, especially during the acute flare
• A ‘normal value’ may not be normal
• Other diseases may also respond to colchicine
• Women get gout
• Atypical joint involvement occurs – e.g. Heberden’s nodes
Presenter
Presentation Notes
The physician needs to be aware of several factors when assessing a patient for gout: Recognizing that gout does not always present as the typical, monoarticular acute flare is important when making the diagnosis. Although gout is caused by elevated serum urate, it is important to remember that serum urate is often normal during the flare, possibly because inflammatory mediators released may increase the excretion of uric acid.1 Colchicine is a drug that can be used to control an acute flare. However, colchicine may be effective in some other conditions, such as CPPD, so response to this agent is not an accurate way to diagnose the disease. Although gout is less common in premenopausal women, it can still occur and is worth considering in a woman presenting with gouty symptoms, especially those on thiazide diuretics. Joints other than those associated with the typical presentation of gout can experience a gout flare as well. 1. Urano et al. J Rheum. 2002;29:1950-1953.
Setons and Issues
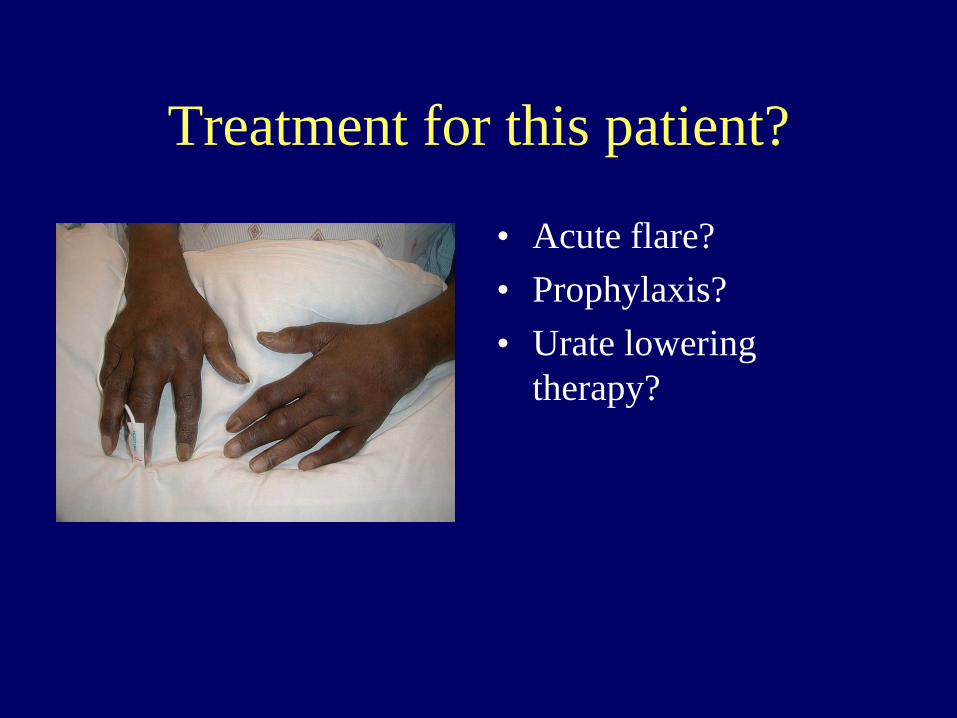
Gout Treatment
Goals of Gout Therapy
1. Terminate the acute attack
2. Prevent recurrence while lowering serum urate
3. Prevent or reverse complications from the deposition of monosodium urate or uric acid crystals (kidney disease, joint destruction)
4. Address comorbidity
5. Do NO Harm (Gout’s generally not lethal until the doctor gets involved)
I. Termination of the Acute Flare = The Gout ‘Danger Zone’ for Elderly
• Resolution of acute flare by controlling crystal-induced inflammation and pain
– Not a cure for gout♦ Only resolves the symptoms♦ After resolution, urate crystals
• The critical issues are– Rapid initiation of therapy– Appropriate duration of therapy
Presenter
Presentation Notes
Resolving the acute flare will resolve the symptoms, but it is not a cure for gout. The medications utilized do not lower serum urate, so urate crystals will remain in the joint(s) following therapy. In order to effectively achieve and maintain termination of the flare, the prescriber should be focused on selecting the appropriate agent quickly and utilizing it for the recommended duration. For more information on the medication options to terminate an acute flare, please see slides 33-35 in the supplement.
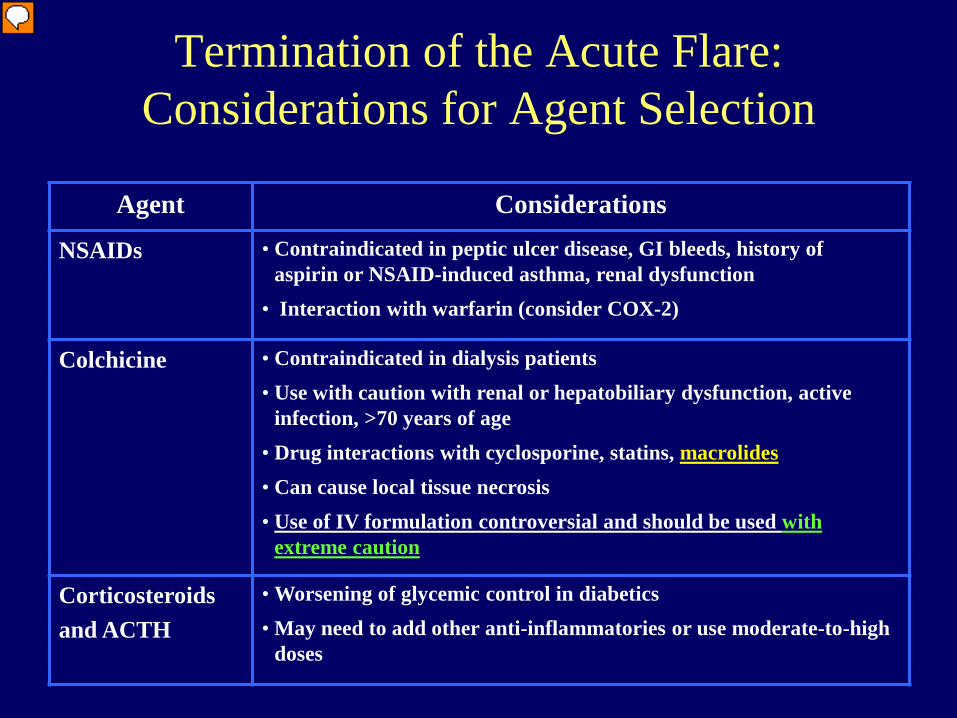
Termination of the Acute Flare:Considerations for Agent Selection
Agent Considerations
NSAIDs • Contraindicated in peptic ulcer disease, GI bleeds, history of aspirin or NSAID-induced asthma, renal dysfunction
• Interaction with warfarin (consider COX-2)
Colchicine • Contraindicated in dialysis patients • Use with caution with renal or hepatobiliary dysfunction, active
infection, >70 years of age• Drug interactions with cyclosporine, statins, macrolides• Can cause local tissue necrosis• Use of IV formulation controversial and should be used with
extreme caution
Corticosteroidsand ACTH
• Worsening of glycemic control in diabetics• May need to add other anti-inflammatories or use moderate-to-high
doses
Presenter
Presentation Notes
Contraindications and other caveats associated with the recommended agents need to be compared to patient comorbidities, polypharmaceutical regimens, and other relevant candidate characteristics before an agent is selected. Parenteral colchicine should be used carefully and with appropriate dosing because improper dosing may result in renal failure, bone marrow suppression, paralysis, and death. This is why a number of rheumatologists avoid giving colchicine via the intravenous route. For more information on the considerations for agents used to terminate an acute flare, please see slide 36 in the supplement.
Prophylaxis Against Flares
• Purpose– To maintain the intercritical segments of gout– Agents useful for decreasing the frequency and severity
of acute flares will not stop the destructive aspects of gout
• Prophylactic options– Low-dose, oral colchicine (0.6 mg daily to b.i.d.)– NSAIDs (i.e. naprosyn in low dose, 375mg b.i.d)
• Initiate agents prior to starting urate-lowering therapy
– Duration? Likely 6 months or longer!!
Presenter
Presentation Notes
To prevent patients from experiencing an acute flare once they have entered the intercritical phase, chronic colchicine or NSAIDs are used. The long-term use of these agents will prevent the inflammation and pain associated with an acute flare, but will not lower serum urate. This means that as uncontrolled hyperuricemia continues to occur and expand the total body urate pool, the result will be “silent” tissue deposition. In other words, crystals will continue to form, deposit, and be destructive to the tissue or joint. However, the use of these agents will prevent the next step in this process, the expected clinical manifestations of a gout flare which include inflammation and pain. The initiation of urate-lowering agents will cause a decline in serum urate, which is known to precipitate a flare. Therefore, when initiating a patient on urate-lowering therapy, the concomitant use of these prophylactic agents is recommended to prevent this common occurrence and foster compliance with hypouricemic agents.
Treating Hyperuricemia and Preventing Disease Progression
• Goals– Lower urate <6 mg/dL to allow depletion of serum urate pool and
deposited crystals (often lower than upper normal lab values)
– Achieve appropriate urate levels without drug toxicity
• Therapy should be lifelong– Intermittent therapy or withdrawal of agents leads to recurrence of
acute attacks, tophi, etc
• Approved urate-lowering agents for gout include– Uricosuric agents
– Xanthine oxidase inhibitor (Allopurinol)
Presenter
Presentation Notes
Treating the hyperuricemia and preventing the formation and deposition of monosodium urate crystals in turn prevents the disease from progressing and, hopefully, eliminates the disease process. Monosodium urate crystals form when the serum urate level meets or exceeds the point of saturation (6.8 mg/dL). Therefore, utilizing hypouricemic therapy to lower the serum urate to below 6 mg/dL prevents the formation of crystals and also allows the present crystals to dissolve. This prevents the progressive joint and tissue destruction as well as eliminates the clinical manifestations of gout. Multiple studies examining intermittent therapy or withdrawal of urate-lowering therapy have found that the clinical manifestations of gout return. This is probably because the chronic, underlying problem causing hyperuricemia, urate overproduction or uric acid underexcretion, is still present. Therefore, lifelong therapy is recommended. For evidence supporting the use of urate-lowering therapy, please see slides 37-40 in the supplement.
Uricosuric Agents
• Uricosuric agents– Probenecid
– Sulfinpyrazone (ex-US)
– Benzbromarone (ex-US)
– Losartan (mild uricosuric)
– Fenofibrate (mild uricosuric)
• Advantage– Uricosurics reverse the most common physiologic
abnormality in gout
Presenter
Presentation Notes
Uricosuric agents act by enhancing the renal excretion of uric acid. Mechanistically, these agents can correct the underlying cause of hyperuricemia in most patients, as 80%-90% of them are hyperuricemic due to impaired uric acid excretion. For information on the mechanism of action of uricosurics, please see slide 41 in the supplement.
Uricosuric Agents• Limitations
– Efficacy dependent on renal function♦ Ineffective if CrCL <50 mL/min
– BID to TID dosing
– Risk of uric acid crystallization in the urine and formation of stones
1. Koopman, ed. Arthritis and Allied Conditions. 14th ed. Lippincott, Williams and Wilkins; 2001:2321.
1
Presenter
Presentation Notes
The use of uricosurics is minimal because of the associated limitations. Because these agents exert their effects by enhancing uric acid clearance through the kidney, they will have little to no effect in patients with compromised kidney function. The risk of kidney stones is present with uricosurics if patients do not maintain adequate fluid intake. Uricosurics push excessive amounts of uric acid through the kidney and may crystallize and deposit there if adequate fluid is not present to flush it through. Any rapid decline in serum urate will precipitate a flare, so prophylactic agents should be considered, as well as a low initial dose of the uricosuric, with escalations to target level. Another limitation to these agents is that they interact with many other drugs. The drugs listed above are some examples of agents that have altered metabolism or elimination when administered concomitantly with probenecid.
Allopurinol
HO
XanthineN
N
NH
OH
N
OH
Uric acidN
N
NH
OH
HO
N
Hypoxanthine
NHN
N N
OHXanthineoxidase
Xanthineoxidase
Allopurinol
N
N
NH
N
OH
OxypurinolN
N
NH
N
OH
OH
Xanthineoxidase
Allopurinol and oxypurinol block the conversion of hypoxanthine to xanthine to uric acid
Allopurinol and metabolite oxypurinol are purine analogs and both substrates and inhibitors of xanthine oxidase
Presenter
Presentation Notes
Serum urate also can be lowered by inhibiting production. This is done by blocking the actions of the enzyme xanthine oxidase, responsible for the final steps in the conversions of purines to serum urate. Allopurinol is currently the only approved xanthine oxidase inhibitor. Allopurinol and its active metabolite oxypurinol are both purine analogs, which is evident by the close resemblance in structure to the purine bases hypoxanthine and xanthine. By blocking the production of serum urate, allopurinol and oxypurinol cause the accumulation of the precursors hypoxanthine and xanthine. These precursors are much more soluble than serum urate, so the chances of crystallization and precipitation of these bases are much lower. This significantly decreases the likelihood of the clinical manifestations of gout.
Advantages of Allopurinol
• Effective for both overproducers and underexcretors
• Convenience of single daily dose– vs. Probenecid (b.i.d. to t.i.d. dosing)
• Can be efficacious in patients with renal insufficiency
Presenter
Presentation Notes
Allopurinol is used much more frequently than the uricosurics because it expands the treatable patient populations and is more practical in terms of dosing. Xanthine oxidase inhibition is effective for both etiologies of hyperuricemia: the overproduction of urate and the underexcretion of uric acid. Allopurinol also is efficacious in patients with renal dysfunction, although some precautions have to be taken in these patients to minimize adverse effects. In terms of dosing, allopurinol is more practical than uricosurics because it can be given once daily.
Limitations of Allopurinol
• “Standard” doses may not achieve target serum urate– In one study, only 53% of allopurinol
• Need for dose adjustment according to renal function– Metabolites excreted by kidney
• Precipitation of an acute attack– Lowering serum urate mobilizes
deposited crystals
1. Perez-Ruiz. Ann Rheum Dis. 1998;57:545-549.
< 6 mg/dl>= 6mg/dl
Serum urate level in gout patients taking
allopurinol 300mg/day
53%47%
Presenter
Presentation Notes
Xanthine oxidase inhibition is currently the gold standard in urate-lowering therapy, and the choice of an agent is limited to allopurinol. This can be problematic because there are significant limitations to its use. The standard, recommended dose of allopurinol is 300 mg/day, but this dose may not achieve target serum urate levels <6 mg/dL, as one study demonstrated in more than half of the patients on allopurinol. This indicates that poor control of hyperuricemia with this dose is common. Higher doses of 450 to 600 mg/day did achieve this target.1 Although this agent is effective in patients with renal insufficiency, allopurinol and oxypurinol are excreted by the kidney and can therefore accumulate in this state. It is recommended that doses lower than the standard 300 mg daily be utilized with compromised renal function, but this may not effectively lower serum urate, as other studies have proven. As with uricosurics or drugs or conditions that may cause a rapid decline in serum urate, flares can occur. This limitation can be avoided by administering prophylactic agents when initiating allopurinol, as well as beginning with a low dose of allopurinol and escalating to target level. 1. Perez-Ruiz. Ann Rheum Dis. 1998;57:545-549.
*Requires careful dose reduction (combination can be hazardous)
1. Koopman, ed. Arthritis and Allied Conditions. 14th ed. Lippincott, Williams and Wilkins; 2001:2321.2. Emmerson. N Engl J Med. 1996;334:445-451.
1
– Thiazide diuretics interfere with the excretion of allopurinol and may enhance toxicity2
Presenter
Presentation Notes
Drug interactions are a concern with allopurinol, especially with the oncology agents azathioprine and 6-mercaptopurine. These drugs are metabolized and inactivated by xanthine oxidase, so when this enzyme is inhibited by the concomitant administration of allopurinol, the amount of active drug increases. Dose reduction of azathioprine and 6-mercaptopurine is necessary to avoid life-threatening toxicities. Cyclophosphamide toxicity and bone marrow suppression are enhanced with allopurinol. Increased levels of warfarin may occur when it is administered concomitantly with allopurinol due to altered hepatic metabolism. A 20% incidence of skin rash has been reported in patients with the co-administration of allopurinol and ampicillin or amoxicillin. The action of thiazide diuretics on the kidney may inhibit the excretion of allopurinol and oxypurinol, resulting in accumulation and toxicity. This is important to note because diuretics can be the secondary cause of gout in many patients, so the combination of these agents may be a common occurrence.
Limitations of Allopurinol
• Adverse effects– Rash
– GI intolerance (diarrhea, nausea)
– Increase in transaminases
– Bone marrow suppression (uncommon)
– Severe hypersensitivity syndrome♦ Occurs early in treatment
♦ Infrequent, but life threatening (20% mortality)
♦ Immediate drug withdrawal and supportive therapy
Presenter
Presentation Notes
Adverse effects of allopurinol can range from benign symptoms to severe and potentially life-threatening conditions. Severe hypersensitivity syndrome occurs early in the treatment course of allopurinol. Although it is infrequent, the serious complications that develop with standard doses (200 to 400 mg/day) can lead to mortality. It is speculated that the development of this syndrome is associated with accumulation in renal insufficiency. The recommended treatment for this condition is the institution of supportive therapy and the immediate withdrawal of the agent. Hande et al. Am J Med. 1984;76:47-56.
Addressing Comorbidity
• Treat HTN (role of ARB?), hyperlipidemia• Weight reduction• Decrease alcohol consumption (wine??)• Vitamin C (uricosuric effect)• Avoid excessive intake of purine-rich foods?
– Anchovies, herring, sardines, mussels, clams, organ meats, beer
– Will only reduce urate levels by 1 mg/dL
Presenter
Presentation Notes
Based on the risk factors for gout that were previously discussed, such as increased BMI and high alcohol intake, patients should be instructed to modify their lifestyles accordingly to help control their gout. These modifications are useful recommendations, but should not be relied upon as primary control of gout. For example, avoiding purine-rich foods such as those listed above may slightly decrease serum urate, but may not provide enough of a decrease to prevent the supersaturation of serum urate, resultant crystal formation, joint deposition, and subsequent flares.
New Gout Therapies in the Last 40 years
Presenter
Presentation Notes
Adverse effects of allopurinol can range from benign symptoms to severe and potentially life-threatening conditions. Severe hypersensitivity syndrome occurs early in the treatment course of allopurinol. Although it is infrequent, the serious complications that develop with standard doses (200 to 400 mg/day) can lead to mortality. It is speculated that the development of this syndrome is associated with accumulation in renal insufficiency. The recommended treatment for this condition is the institution of supportive therapy and the immediate withdrawal of the agent. Hande et al. Am J Med. 1984;76:47-56.
New Gout Therapies in the Last 40 years
• Febuxostat (Uloric)
• A non-purine, xanthine oxidase inhibitor
• Current data support– Potent inhibition with significant urate reduction
– Ability to administer in renal insufficiency with no dosage adjustments1
♦ Mainly metabolized by oxidation and glucuronidation in the liver2
– Appears to be safe and tolerable agent
N
N
NH
N
OH
AllopurinolFebuxostat
O
CN
SCO2
H
NCH3
Presenter
Presentation Notes
Adverse effects of allopurinol can range from benign symptoms to severe and potentially life-threatening conditions. Severe hypersensitivity syndrome occurs early in the treatment course of allopurinol. Although it is infrequent, the serious complications that develop with standard doses (200 to 400 mg/day) can lead to mortality. It is speculated that the development of this syndrome is associated with accumulation in renal insufficiency. The recommended treatment for this condition is the institution of supportive therapy and the immediate withdrawal of the agent. Hande et al. Am J Med. 1984;76:47-56.
Fubuxostat (Uloric) in Gout• Adverse Effects
– Gout flares– LFTs– CVD events
• Primary outcome = SUA < 6.0, last 3 mos.• Dose = 40mg to 80mg once daily
Future Treatment of Hyperuricemia: Uricase Enzymes
• Uricase enzymes further catabolize uric acid to a more soluble, readily excretable form
Pay et al. Curr Rheumatol Rep. 2003;5(3):213-214. http://www.phoenixpharm.org/products/uricasepeg20.htm.
Sundy J et al A&R, 2007
Presenter
Presentation Notes
The metabolism of purines and the excretion in the form of uric acid is a property unique to humans and a few primate species because the enzyme necessary for further degradation is missing. This enzyme, uricase, metabolizes uric acid to allantoin. Allantoin is more soluble, and therefore less likely to crystallize, and readily excretable. By administering the pharmacologic version of this enzyme, uric acid is further catabolized and excreted as allantoin. There are a few uricase enzymes that are currently available, as well as some that are in development.
Diagnostic Pitfalls72 year-old man with ‘refractory rheumatoid arthritis’