good bradforddistrictcaretrust community-basedcrisis services
TRANSCRIPT

Locations inspected
Name of CQC registeredlocation
Location ID Name of service (e.g. ward/unit/team)
Postcodeofservice(ward/unit/team)
BDCT Headquarters, New MIll TADHQ Intensive home treatment team BD20 6TA
BDCT Headquarters, New MIll TADHQ Intensive home treatment team BD9 6DP
BDCT Headquarters, New MIll TADHQ A&E liaison at Bradford RoyalInfirmary BD9 6RJ
BDCT Headquarters, New MIll TADHQ A&E liaison at Airedale GeneralHospital BD20 6TA
This report describes our judgement of the quality of care provided within this core service by Bradford District CareTrust. Where relevant we provide detail of each location or area of service visited.
Our judgement is based on a combination of what we found when we inspected, information from our ‘IntelligentMonitoring’ system, and information given to us from people who use services, the public and other organisations.
Bradford District Care Trust
Community-bCommunity-basedased crisiscrisisserservicvicesesQuality Report
Bradford District Care TrustNew MillVictoria RoadSaltaireShipleyWest YorkshireBD18 3LDTel: 01274 228300Website: www.bdct.nhs.uk
Date of inspection visit: 17-19 June and 1 July 2014Date of publication: 15 September 2014
Good –––
1 Community-based crisis services Quality Report 15 September 2014

Where applicable, we have reported on each core service provided by Bradford District Care Trust and these are broughttogether to inform our overall judgement of Bradford District Care Trust.
Summary of findings
2 Community-based crisis services Quality Report 15 September 2014
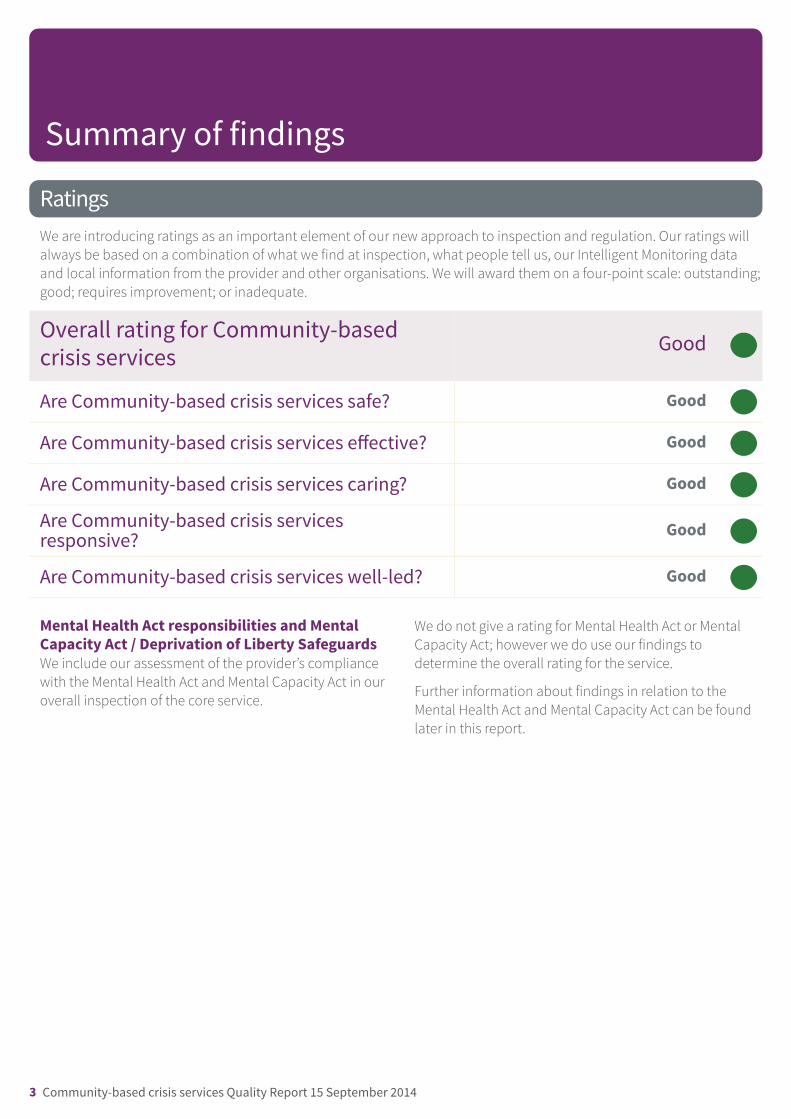
RatingsWe are introducing ratings as an important element of our new approach to inspection and regulation. Our ratings willalways be based on a combination of what we find at inspection, what people tell us, our Intelligent Monitoring dataand local information from the provider and other organisations. We will award them on a four-point scale: outstanding;good; requires improvement; or inadequate.
Overall rating for Community-basedcrisis services Good –––
Are Community-based crisis services safe? Good –––
Are Community-based crisis services effective? Good –––
Are Community-based crisis services caring? Good –––
Are Community-based crisis servicesresponsive? Good –––
Are Community-based crisis services well-led? Good –––
Mental Health Act responsibilities and MentalCapacity Act / Deprivation of Liberty SafeguardsWe include our assessment of the provider’s compliancewith the Mental Health Act and Mental Capacity Act in ouroverall inspection of the core service.
We do not give a rating for Mental Health Act or MentalCapacity Act; however we do use our findings todetermine the overall rating for the service.
Further information about findings in relation to theMental Health Act and Mental Capacity Act can be foundlater in this report.
Summary of findings
3 Community-based crisis services Quality Report 15 September 2014

Contents
PageSummary of this inspectionOverall summary 5
The five questions we ask about the service and what we found 6
Background to the service 8
Our inspection team 8
Why we carried out this inspection 8
How we carried out this inspection 8
What people who use the provider's services say 9
Good practice 9
Areas for improvement 9
Detailed findings from this inspectionLocations inspected 11
Mental Health Act responsibilities 11
Mental Capacity Act and Deprivation of Liberty Safeguards 11
Findings by our five questions 12
Summary of findings
4 Community-based crisis services Quality Report 15 September 2014

Overall summaryBradford District Care Trust offers a range of crisis andhome treatment services including: the intensive hometreatment team (IHTT), A&E liaison service and singlepoint of access team.
Crisis and home treatment services were safe. Staffunderstood and implemented safeguarding procedureswell. The team routinely discussed caseloads and anyassociated risks, and these were also discussed moreformally during handovers. IHTT had a traffic light systemin operation, whereby staff could determine people’s risksand needs quickly and at a glance. New informationabout risks was communicated effectively. In addition,the use of the RIO electronic records system made surethat key information was shared in real time with otherteams involved in a person’s care.
People’s care and treatment was planned effectively andwas recovery-focused. Assessments were comprehensiveand took account of people’s skills, as well as their areasof need. Care and treatment was also person-centred andpeople were involved in the development of their careplans. Teams were multidisciplinary and worked welltogether, and staff received training and supervision forongoing professional development.
Staff treated people with dignity and respect. Care wasdelivered with kindness and compassion, and staff madesure that people were involved in all stages of their care,
treatment and support. Staff also listened to people’sviews and provided information clearly so that peoplecould make informed decisions. The language used bystaff was encouraging and demonstrated empathy.
Services were responsive to people’s needs and had beendeveloped in consultation with local people. People whoused the service knew who to contact for support duringthe day and at night. Staff responded quickly to changesin need and, when needed, provided more visits. IHTTteams worked closely with community mental healthteams and were involved with people before beingadmitted to hospital, during their stay in hospital andwhen planning and facilitating discharge back to thecommunity. However, there was a risk that people mightnot receive the right care at the right time because A&Eliaison was not a 24-hour service and IHTT could notprovide face-to-face assessments out-of-hours as theyonly had one member of staff on duty throughout thedistrict after 9pm seven days a week.
Crisis and home treatment services were well-led. Stafffelt well supported by their managers and were consultedabout the future direction of the trust. Staff and peoplewho used the service were encouraged to get involvedwith service development. We also saw evidence oflearning from incidents and responding to feedback. Staffunderstood the need for on going improvement of theservice and this was achieved by regular audits andmonitoring of quality.
Summary of findings
5 Community-based crisis services Quality Report 15 September 2014

The five questions we ask about the service and what we found
Are services safe?Systems for safeguarding and reporting incidents were wellestablished. Staff told us that they received feedback on reportedincidents. We also saw that lessons from team, and wider trust,incidents were included in the agenda for monthly team meetings.All teams had access to the RIO electronic records system so staffcould highlight any concerns about risk. The service used a red,amber green system to help staff identify risks to people and theyused this information to plan their visits.
The personal safety of staff was also protected. Staff working alone‘checked in’ with, or received a call from, other members of theteam.
We saw on the RIO system that risk assessments and care planswere updated and reviewed.
Good –––
Are services effective?Records for people under a Community Treatment Order (CTO) werecomprehensive. We saw evidence that people were involved in theircare and that the orders were reviewed by the multidisciplinaryteam.
We saw from records that people received a comprehensiveassessment by medical and nursing staff on initial contact. Physicalhealth monitoring was also routinely monitored as part of people’scare.
People were offered a good range of evidence-based psychologicaltherapies and were regularly asked for feedback on the services.People were complimentary about the teams and valued the servicethey received. The team manager monitored caseloads and theteam’s capacity through regular team meetings and monthlysupervision. Staff received appropriate inductions, supervision andappraisals.
Good –––
Are services caring?People told us they were treated with dignity and respect. We foundthat clinicians were skilled and knowledgeable, and that staff usedlanguage that was compassionate, clear and simple. People whoused the services had access to appropriate literature andinformation. Staff also supported people with social and domesticissues, and supported carers.
Good –––
Are services responsive to people's needs?Services had been developed in consultation with local people.People knew how to access help out-of-hours. Those in need of
Good –––
Summary of findings
6 Community-based crisis services Quality Report 15 September 2014

urgent assessment out-of-hours were told to use A&E services orcontact charitable or third sector services. If people attended A&Ethey were assessed by the psychiatric liaison team and referred toother services.
We observed teams working well together and saw many examplesof good working relationships. Teams would routinely liaise with thecrisis team about people they were particularly concerned about.They also made sure that this information was readily availableshould they receive contact from them out-of-hours.
We found evidence of trust wide learning from complaints andincidents.
Are services well-led?Staff were dedicated and felt well supported by their managers.Some staff told us that they had attended the ‘listening into actionforum’. They also had access to the minutes of managementmeetings on the intranet. We saw evidence on the intranet that staffwere consulted about the trust’s future plans.
The trust’s internet was updated as plans changed. Staff had a broadunderstanding of the changes that had been introduced in theorganisation, and people using the service were regularly asked fortheir comments and opinions about the service.
Staff were up-to-date with mandatory training, which monitoredregularly. Staff also used a variety of supervision available to themon a regular basis. Staff were knowledgeable about how to accessadvocacy services for people.
There was a trust-wide risk register in place to oversee and identifyrisks to the trust, staff and people using services. We saw that localaudits of records were completed for the care programme approach(CPA), which staff said managers were able to monitor electronically.
Good –––
Summary of findings
7 Community-based crisis services Quality Report 15 September 2014

Background to the serviceIntensive home treatment team (IHTT)
IHTTs offer a 24-hour service, seven days a week forpeople who are acutely unwell and require significantsupport. Teams consist of health and social careprofessionals who aim to provide care and support closeto where people live, and to prevent admission tohospital where possible. The teams can support peoplefollowing admission to hospital and will work withindividuals to make sure that their stay in hospital is asshort as possible. Where possible, IHTT’s will also supportpeople when they are discharged from hospital. The twoIHTTs of Bradford District Care Trust cover the city andsouth and west areas of Bradford, as well as northBradford, Airedale and Craven.
A&E liaison
The A&E liaison teams are based in the accident andemergency (A&E) departments at Airedale GeneralHospital and Bradford Royal Infirmary. People are
assessed by a psychiatric liaison nurse or other mentalhealth professional, and referred or signposted to arelevant service. Psychiatric liaison nurses are availableseven days a week between 9am and 5pm at AiredaleGeneral Hospital. A temporary initiative running from Jan2014 to March 2015 extends provision until 2am sevendays a week. Psychiatric liaison nurses are availableseven days a week between 7.00am and 3.00am atBradford Royal Infirmary. At all other times, A&E staff areable to make a referral to other services, whereappropriate.
Single point of access team
The team triages all referrals from primary care, GP’sprimarily to adult, older adult, youth services andaddictions. The team screens, records and then triagesreferrals to the appropriate team using similar criteria forsimilar services, for example adult community mentalhealth teams.
Our inspection teamOur inspection team was led by:
Chair: Angela Greatley, Chair, The Tavistock and PortmanNHS Foundation Trust
Team Leader: Jenny Wilkes, Head of Inspection –Hopsitals Directorate (Mental Health), Care QualityCommission (CQC)
The team included CQC inspectors and a variety ofspecialists: a social worker, occupational therapists, anindependent Mental Health Act advocate and a seniornurse.
Why we carried out this inspectionWe inspected this core service as part of our Wave 2 pilotmental health inspection programme.
How we carried out this inspectionTo get to the heart of people who use services’ experienceof care, we always ask the following five questions ofevery service and provider:
• Is it safe?• Is it effective?• Is it caring?
• Is it responsive to people’s needs?• Is it well-led?
We visited the crisis and home treatment services ofBradford District Care Trust on 17, 18 and 19 June 2014.Before visiting, we reviewed a range of information wehold about the core service and asked other
Summary of findings
8 Community-based crisis services Quality Report 15 September 2014

organisations to share what they knew. We held listeningevents with people that use services at the Lynfield andAiredale sites and undertook site visits to the team bases.We also carried out an unannounced inspection of theaccident and emergency (A&E) liaison service at BradfordRoyal Infirmary on 1 July 2014. During the visits we heldfocus groups with a range of staff, including nurses,doctors and therapists. We observed how people werebeing supported and reviewed the care and treatmentrecords of people who used the services. We also metand spoke with people who used the services and theyshared their views and experiences.
We reviewed and inspected the community servicesbeing provided. We visited two intensive home treatmentteams (IHTT) and the A&E psychiatric liaison team atBradford Royal Infirmary. We also visited the ‘single pointof access team’ for mental health. As this team had onlybeen in operation for three months, it was too early for usto provide a rating for this service.
In addition, we visited the IHTT at the Airedale Centre forMental Health and Lynfield Mount Hospital. Health
What people who use the provider's services sayWe held listening events before the inspection andpeople told us that the support they received from theintensive home treatment team (IHTT) was good.However, some people commented that they sometimesfelt they received limited support when they were incrisis. For example, visits from an IHTT member was onlyfor a limited time period, such as 15-minute visits.
People told us that they were involved in the planningand treatment of their care and that they could consent
to their care and treatment, as well as discuss and agreetreatment options with medical staff. The people wespoke with were very positive about the services theyreceived and described staff as ‘professional’, ‘friendly’,‘caring’ and, ‘compassionate’. We also saw examples ofhow people and their carers were consulted about theircare and treatment and how outcomes of surveys aboutthe services were used to inform staff about thestandards of service they provided.
Good practice• The trust provided on going training for staff in
psychological therapy.
• There were non-medical prescribing leads forassessment and treatment.
• Safeguarding practices were safe and staff wereknowledgeable about appropriate safeguardingreferrals.
• The lone worker policy was followed, which helped tokeep staff safe when visiting in the community.
Areas for improvementAction the provider MUST or SHOULD take toimprove
• The trust should continue to work with commissionersof services to make sure appropriate services areavailable to people 24 hours a day. The A&E psychiatricliaison teams did not operate a 24-hour service, and atBradford Royal Infirmary there were no separatefacilities to assess people in private. The out-of-hourscrisis services based at Lynfield Mount and Airedale
Centre for Mental Health only had one person on duty,so were not able to provide face-to-face assessments.This meant people were diverted to A&E departmentsor third sector providers, such as the Samaritans.
• The trust should continue to liaise with managers ofthe acute hospitals to secure an appropriateenvironment for mental health assessments in eachA&E department.
Summary of findings
9 Community-based crisis services Quality Report 15 September 2014

• The trust should continue to make sure that theimpact of major service redesign, including the
development of the single point of access andadministrative hubs, is properly monitored andmanaged to make sure that the service continues todeliver caring and responsive care.
Summary of findings
10 Community-based crisis services Quality Report 15 September 2014

Locations inspected
Name of service (e.g. ward/unit/team) Name of CQC registered location
Intensive Home Treatment Team Airedale Centre for Mental Health
Intensive Home Treatment Team Lynfield Mount Hospital
A&E Liaison at Bradford Royal Infirmary Trust Headquarters
A&E Liaison at Airedale General Hospital Trust Headquarters
Mental Health Act responsibilitiesWe do not rate responsibilities under the MentalHealth Act 1983. We use our findings as a determinerin reaching an overall judgement about the provider.
We did not monitor responsibilities under the MentalHealth Act 1983 at these locations, however we examinedthe trust’s responsibilities under the Mental Health Act atother locations and we have reported this within theoverall trust report.
Mental Capacity Act and Deprivation of Liberty SafeguardsStaff were also aware of their responsibilities under theMental Capacity Act (2005) and were able to demonstratethrough some of the treatment records reviewed. This wasevidence by how they recognised, responded and raisedissues about mental capacity.
Bradford District Care Trust
Community-bCommunity-basedased crisiscrisisserservicvicesesDetailed findings
11 Community-based crisis services Quality Report 15 September 2014

* People are protected from physical, sexual, mental or psychological, financial, neglect, institutional or discriminatoryabuse
Summary of findingsSystems for safeguarding and reporting incidents werewell established. Staff told us that they receivedfeedback on reported incidents. We also saw thatlessons from team, and wider trust, incidents wereincluded in the agenda for monthly team meetings. Allteams had access to the RIO electronic records systemso staff could highlight any concerns about risk. Theservice used a red, amber green system to help staffidentify risks to people and they used this informationto plan their visits.
The personal safety of staff was also protected. Staffworking alone ‘checked in’ with, or received a call from,other members of the team.
We saw on the RIO system that risk assessments andcare plans were updated and reviewed
Our findingsTrack record on safetyStaff were trained in safeguarding vulnerable adults andchildren. Staff we spoke with were knowledgeable abouttheir responsibilities in regards to the safeguarding process.They described the process for referring any identifiedpotential or actual concerns to the relevant department.The trust policies and procedures were accessible on thetrust’s own intranet site, but the corporate policies datedfrom 2012 and had not been reviewed in 2013 as per thepolicy timescale for revision. Staff gave examples of thetype of safeguarding concerns they would report anddescribed the process for completing this. They told usconcerns were discussed with line managers whereappropriate in the first instance. Safeguarding referralswere made to Bradford City Council. Social workers formedpart of the multidisciplinary team and so were able toprovide advice and guidance on safeguarding matters.
Staff confirmed that the trust had an on-line reportingsystem to report and record incidents and near misses. Wesaw that staff had access to this system via ‘password’protected computers. The trust wide evidence provided
showed us that the trust was reporting concerns throughthe National Reporting and Learning System (NRLS). Thelevels of reporting were within expectations for a trust ofthis size.
Learning from incidents and improving safetystandardsThe trust’s serious incident data showed us that trust widelearning from serious incidents had been reviewed by thegovernance team and shared throughout the trust. Staffconfirmed this and reported that the lessons learnt fromthese incidents had been discussed within their specificteam. For example, we saw copies of the trust’s onlinesafety alerts. This provided information and guidance forstaff to follow. Most members of staff spoken with wereaware of the safety alerts and we were told they werediscussed at larger team meetings. The evidence revieweddemonstrated the trust had embedded learning fromincidents within the organisation.
Staff confirmed they had received risk assessment trainingand told us that they felt well supported by their linemanager following any safety incidents. We saw the use ofRIO was outstanding and staff used this system to updaterisk assessments and risk profiles of people on a dailybasis.
Staff told us they used the trust’s electronic incidentreporting system (EIR) for reporting any incidents, concernsor near misses. Feedback from serious untoward incidentswas fed back to the individuals involved and wider trustincidents distributed by email globally. Lessons learnt fromincidents relating to the team, and wider across the trust,were included in the agenda for monthly team meetings.Managers told us action plans were developed frominvestigations and lessons learnt. These were circulatedglobally, with feedback given to specific teams. Staff told usthey were supported and debriefed by their managerfollowing any incidents that occurred when they feltunsafe. Managers were described as supportive.
The psychiatric liaison service team were well aware of theserious incident reporting process and learning outcomesfrom this. Incidents were reported both through the
Are services safe?By safe, we mean that people are protected from abuse* and avoidable harm
Good –––
12 Community-based crisis services Quality Report 15 September 2014

Bradford District Care Trust and Bradford Royal Infirmaryincident reporting systems. Incident reporting and lessonslearnt were shared among the three trusts providing andhosting the psychiatric liaison services.
In the ‘single point of access’ service every person wasinitially triaged by the call handling staff and then passedto the individual duty workers. Duty workers could theneither divert people or tasks to the local community mentalhealth duty teams or refer to individual services. Followingthe continuous monitoring of the service, following‘teething problems’, pathways had been developed andintroduced for staff to refer people to other services withinthe trust. When the service was initially set up we saw thesystem for processing referrals had been inconsistent andled to a small number of referrals being delayed in reachingservices. This was brought to the attention of the trust andCQC during our visit. We looked into the concerns aboutthe service and spoke with the administration anddevelopment manager as well as call handling and dutystaff. We saw the administration manager had developedguidance for staff and duty officers on managing thesystems. We spoke to the development manager and sawthat measures to improve the referral system had been putin place. This included an advanced nurse practitioner tosupport duty officers as well as additional staff to supportthe primary care staff in the team. We also spoke to staffabout the model introduced for the single point of accessteam. Staff were aware that the development manager wasvisiting another trust to look at their single point of accessservice. The aim was to look at and learn from a well-established single point of access service.
Reliable systems, processes and practices to keeppeople safe and safeguarded from abuseWe saw there was information displayed in the teamfacilities onsite about the trust’s safeguarding adult’spolicy. We also saw the online safeguarding policy andprocedure and patient safeguarding information leaflets.This meant that patients and staff had been given therequired guidance in order to support them to raiseconcerns when these were identified. Agency staff told usthey had an induction and this included safeguardingadults and children training. We saw the team used theacute mental health care induction format and thisincluded training and reading the policies and proceduresfor safeguarding.
Staff were aware of the trust’s safeguarding and otherpolices. They told us that they knew how to raise anysafeguarding concerns. This was demonstrated in some ofthe individual treatment records we reviewed. Theseshowed us that risk assessments had been completed andidentified if people were at risk of exploitation or werevulnerable due to their mental health needs. Staff were alsoaware of their responsibilities under the Mental CapacityAct (2005) and were able to demonstrate, through some ofthe treatment records reviewed, how they recognised,responded and raised issues about mental capacity.
Staff were aware of the trust’s whistleblowing policy andconfirmed that they felt able to raise concerns with theirdirect line manager. We saw direct evidence of staff raisingconcerns about the referral system for the single point ofaccess team.
We saw that medication was appropriately and securelystored. Medicines management was seen to be effectivewith audits undertaken by pharmacy. We found there was asuitable medicines management system in place for thereceipt, storage, administration and recording ofmedication. However, on one occasion we saw thatmedication taken to be delivered to a person that was notat home was left in the vehicle of a staff member and notsigned back in and stored securely.
There was a lone working policy and procedure in place.We saw the paper system in place which allowed the facilityto highlight where people presented an identified risk tostaff safety. We saw ‘whereabouts’ sheets were completedwhen were out of office and the duty worker wasresponsible for ensuring those out had returned safely.
Records management was electronic and used the RIOsystem. The staff said they had good access to patientinformation and could record a detailed picture andbackground of individual risks to staff. We saw that careplans and risk assessments were generally completedwithin 48 hours of referral to the teams.
Assessing and monitoring safety and riskWe observed handovers and sat in on two team handovermeetings during our visit to the teams. These appearedwell planned and organised. Each person currentlyreceiving care was discussed, with increased time beinggiven to those who were assessed as having higher risks,including any new referrals for follow up. Appropriatesharing of information to ensure continuity and safety of
Are services safe?By safe, we mean that people are protected from abuse* and avoidable harm
Good –––
13 Community-based crisis services Quality Report 15 September 2014

care was observed. On receipt of a referral people wereseen and assessed within 24 to 72 hours. Referrals wereaccepted by the recently formed single point of accessteam, community mental health teams, inpatient services,accident and emergency and GP. During our visits to threepeople using the crisis services we saw staff discussedindividual safety plans with people and how they could usethese to increase safety as well as to lessen their distress.We saw that staff offered to increase the frequency of visitsin response to risk indicators when talking to people abouttheir care. We observed an assessment by IHTT and thefamily member raised concerns about their relative beingallowed to walk out of the A&E department by A&E staffwhen their relative was a risk to themselves. The concernswere not about the psychiatric liaison team staff but theA&E staff. As a result an urgent referral had been made tothe intensive home treatment team. The relative wasadvised to complain to the relevant trust.
We reviewed six electronic records overall. Safeguardingand abuse issues were considered within the assessmentdocument. We saw that staff joint worked with otheragencies and across services to promote safety. Caseloadsand capacity were monitored by the team managerthrough daily and weekly meetings as well as monthlysupervision. These sessions included discussion aboutreferrals, discharges and levels of risk, as well asestablishing capacity for new referrals.
A&E psychiatric liaison teamThe teams based at Bradford Royal and Airedale GeneralHospitals did not provide a 24-hour service. However, theAiredale site was able to provide this service temporarilydue to winter pressure funding until the end of June 2014and has since been extended to March 2015. The staff on
duty at Bradford Royal Infirmary demonstrated that theywere able to assess the risk of patients and refer them toother services if necessary. If patients could not beassessed because they were under the influence of drugsor alcohol they had to wait until they could be assessedunless an assessment under the Mental Health Act (MHA)1983 was required. Staff were able to stay with patients ifthere was a risk identified. The staff had access to RIO andSystem 1 so could access information about, or putreferrals onto, these systems as well as update them in realtime. A system had been put in place that informed the GPby fax of people presenting at A&E. If required the policewere informed about individual concerns and carried out awelfare check on the individual.
Understanding and management of foreseeablerisksElectronic records seen showed us that people who hadrecently been assessed by the single point of access teamhad an initial risk assessment completed over thetelephone to determine which service they would bedirected to and the level of risk determined how quicklythey could access services. We saw that referrals to IHTTwere seen within 24 to 72 hours.
Assessments we reviewed included assessments of theperson’s physical health needs as well as an assessment ofand the risk to themselves or others where appropriate.Evidence was seen of the active involvement of the personin assessing risks for themselves in partnership with staff.
We saw good examples of risk assessments andsubsequent care plans linked to those CommunityTreatment Orders (CTO) reviewed during our inspection.
Are services safe?By safe, we mean that people are protected from abuse* and avoidable harm
Good –––
14 Community-based crisis services Quality Report 15 September 2014

Summary of findingsRecords for people under a Community TreatmentOrder (CTO) were comprehensive. We saw evidence thatpeople were involved in their care and that the orderswere reviewed by the multidisciplinary team.
We saw from records that people received acomprehensive assessment by medical and nursingstaff on initial contact. Physical health monitoring wasalso routinely monitored as part of people’s care.
People were offered a good range of evidence-basedpsychological therapies and were regularly asked forfeedback on the services. People were complimentaryabout the teams and valued the service they received.The team manager monitored caseloads and the team’scapacity through regular team meetings and monthlysupervision. Staff received appropriate inductions,supervision and appraisals.
Our findingsAssessment and delivery of care and treatmentWe looked at records and saw that care plans wereoutcome based and reflected progress in achieving aims ina recovery based model of care. Progress notes linked tothe care plan in place. Records we were shown wereperson-centred and demonstrated people’s involvement.People told us they were aware of their care plans and theyhad been involved in their reviews. During our visits topeople we saw that they were involved in their assessmentand care planning. We also observed staff taking calls frompeople that used the service. We observed that staff askedpeople about their care and treatment and used plainlanguage to explain medical terminology and discussedtreatment and support options with people.
We saw good evidence of comprehensive assessment bymedical and nursing staff on initial contact and theycovered all aspects of care as part of a holistic assessment.
We heard that new patients were seen within a four hourassessment target and known patients were seen within 24hours. Teams offered a good range of evidence basedpsychological therapy and we heard that psychologicalservices aimed to see patients within ten days of referral.Patients told us that they had benefitted from
psychological therapies and understood the treatmentcontract about engaging in psychological therapy. Oneperson commented that, “CBT (talking therapy) had helpedreduce the anxiety. I’m definitely seeing things are better”.
Staff were able to discuss issues around consent andcapacity and how to undertake or organise an assessmentfor people as necessary. Mental Capacity Act 2005 andDeprivation of Liberty Safeguards were part of themandatory training program.
In the single point of access service every person wasinitially triaged by the call handling staff and then passedto the individual duty workers. Duty workers could theneither divert people or tasks to the local community mentalhealth duty teams or refer to individual services.Assessment was not face-to-face by the single point ofaccess team, but referrals to crisis services were in real timeand could be responded to quickly. The duty system in thesingle point of access team is being changed to dutyworkers picking up calls from the different geographicalareas of Bradford Community trust and completing theassessment on RIO. This means the duty team will dealwith all incoming referrals and not just those linked to theirrespective geographical area. A dedicated duty team isbeing planned so there is more consistency around theassessment and referral system. RIO also links to System 1used by primary care, so information can be passedbetween the systems. Faxed referrals from GPs werescanned and uploaded into the systems so staff couldaccess the referral documents.
The A&E psychiatric liaison team was based in Airedale andBradford district hospitals. The mental health trustprovided the staff. This was not a 24-hour service. The teamconsisted of band six and seven nurses. There was also on-call medical cover with a doctor able to attend for mentalhealth assessment. Staff were able to show us the recentreferrals and assessments completed by the team. We sawthat people were assessed as quickly as possible and teamendeavoured to see people within the four hour casualtywaiting time. Assessment documents demonstrated thatstaff completed a thorough personal history. This includedrecent social, family and health information, as well ascontributing factors to the crisis. Detailed information wastaken about past contact with mental health services andthis included any previous psychiatric history. People could
Are services effective?By effective, we mean that people’s care, treatment and support achieves goodoutcomes, promotes a good quality of life and is based on the best availableevidence.
Good –––
15 Community-based crisis services Quality Report 15 September 2014

not be appropriately assessed until they had the capacityto understand the assessment process. This meant that theassessment process could be delayed due to the influenceof alcohol or drug use.
Outcomes for people using servicesWe saw monthly audit tools had been introduced tomonitor case management, health and safety and recordswhich was fed into the trust system. Feedback aboutperformance was shared with managers for their action.Staff reported that whilst this system had increased timespent on administration, it has promoted more regularreview of their caseloads and meant that people werebeing referred on to other teams or discharged whereappropriate in consultation with the consultantpsychiatrist.
Once people had been assessed in A&E they would beoffered on going support via the community mental healthteams or discharged with appropriate advice. If it had beendetermined they were not at risk they could leave A&Eproviding the relevant referral information and advice hadbeen given to them. For example, if an individual presentedunder the influence of alcohol they were advised not todrive. Information about charitable and third sectorservices was provided if people wanted to access non NHSservices. If medication was prescribed this was obtainedfrom the pharmacy prior to the person leaving. Assessmentand referral information was then faxed to the GP and theelectronic systems updated.
Staff, equipment and facilitiesStaff told us they were supported to undertake trainingoutside of mandatory training. We saw a robust supervisionprocess in place. Staff received management supervisionmonthly. Performance issues and caseload capacity wereembedded in this process. This included specialistsupervision, for Approved Mental Health Professionals(AMHP) and non-medical prescribers. Senior medical stafftold us they had regular organised peer group supervision.
Teams we visited had daily or twice daily handovermeetings, weekly clinical meeting for case discussion andalso a monthly team meeting for more team related issues,which included information sharing. Community staff hadalcohol gel available to them as part of the infection controlpolicy when visiting people in the community.
In the single point of access team we saw that the teamwere provided with cover and recruitment was on going,
with plans to expand the number of call handling staff. Theadministration manager demonstrated how they wereimproving the telephone system in use so call handlerswere able to hold taking calls until they had completed theadministration and recording process. This meant thatinformation was recorded in real time and up-to-date.
The A&E psychiatric liaison team staff told us that traininghad not been an issue for them and they had to completetheir mandatory and role specific training. We saw theelectronic recording systems in place to prompt, monitorand track staff training. Training was monitored at bothteam and service level. Staff demonstrated how theyrecorded their own learning logs on the electronic staffrecord (ESR) and how this information was collated andshared with the manager. The team manager told us theyhad arranged for clinical supervision for the team withband seven or advanced nurse practitioners. The managerconfirmed they had managerial supervision with their linemanager every six weeks and for team membersapproximately every eight weeks. Staff told us that informalpeer support was available as the manager had an opendoor policy.
Staff told us that they had received induction and trainingto prepare them for their role and were supported by theirline manager. Each member of staff spoken with told usthat they received supervision and annual appraisals fromtheir line manager as required. This meant that staffreceived the appropriate levels of support from theirimmediate manager.
Staff confirmed that systems were in place to monitor staffsickness and that they had access to occupational healthsupport. Most staff told us that they felt well supported bytheir line manager
Multi-disciplinary workingInformation on patients subject to the care programmeapproach (CPA) was shared on the electronic system whichboth health and social work staff could access. We saw thatRIO and System 1 was accessible and used to record allrelevant information. For example, if the crisis teams had aconcern about risk this was flagged electronically withother teams involved in that persons care. These systemswere well used by staff to provide information to and forother teams. We sat in on a multidisciplinary team meetingand saw the different professions worked well together andcontributed toward person centred care.
Are services effective?By effective, we mean that people’s care, treatment and support achieves goodoutcomes, promotes a good quality of life and is based on the best availableevidence.
Good –––
16 Community-based crisis services Quality Report 15 September 2014

Staff told us in all the teams we visited that capacity tomeet demand was challenging but there was good teamsupport from more senior nurses and managers. In allteams we visited staff described positive relationships withother services. This meant that a multidisciplinaryapproach to care and treatment was optimal.Multidisciplinary teams were made up of, or had inputfrom, occupational therapists, nurses, social workers andmedical staff. A good relationship was reported betweenthe crisis teams and other mental health services.
The A&E psychiatric liaison team said they worked with theintensive home treatment team who were the gatekeepersto inpatient beds. The psychiatric liaison team could referdirectly to intensive home treatment, assertive outreach,community mental health, early intervention and psychosisand inpatient beds as well as requesting MHA assessments.This meant that inpatient beds were allocated dependentupon need and the crisis services could support people asan alternative to hospitalisation if appropriate. The team atBradford Royal Infirmary said that when capacity increasedthey could get support from the intensive home treatmentteam’s staff.
In the single point of access team we saw that people couldnot access the site and there was no walk in service. Thisservice opened three months ago. The staff we spoke withwere very positive about the service but had found theinitial operational period difficult due to the evolvingsystems and processes within the service. The
development manager told us that the local clinicalcommissioning group had agreed additional funding toprovide a band 7 advanced nurse practitioner to beattached to the service as well as the development lead.This meant that the initial service development issues hadbeen recognised and improved systems put in place tocreate more fluid multidisciplinary inter-team working.
The development manager said the main concern aboutmultidisciplinary working was that duty workers were notconsistently provided so as systems changed staff did notkeep pace. Comments from duty workers were that therewas no training on the systems prior to the single point ofaccess team being introduced, but said there wereimprovements being put into place.
Mental Health Act (MHA)We did not fully monitor responsibilities under the MHA atthese locations, however we examined the trust’sresponsibilities under the MHA at other locations and wehave reported this within the overall trust report.
We saw information about the MHA was available in areasthat people accessed. We saw this was made available indifferent languages and an interpreter service was availableto people.
Records we looked at for people under a CommunityTreatment Order (CTO) were comprehensive with evidenceof people’s involvement and multi-disciplinary review
Are services effective?By effective, we mean that people’s care, treatment and support achieves goodoutcomes, promotes a good quality of life and is based on the best availableevidence.
Good –––
17 Community-based crisis services Quality Report 15 September 2014

Summary of findingsPeople told us they were treated with dignity andrespect. We found that clinicians were skilled andknowledgeable, and that staff used language that wascompassionate, clear and simple. People who used theservices had access to appropriate literature andinformation. Staff also supported people with social anddomestic issues, and supported carers.
Our findingsKindness, dignity and respectWe spoke with three people using services and two carers.They were very complimentary about the care andtreatment they received. However, one person told us, “Ittook them ages for them to get here after I telephoned; ittook them at least twenty minutes”.
We saw staff were compassionate, warm, friendly, positiveand engaging with people. People did not visit the officebase and were seen at home. We managed to speak withpeople who we visited with the intensive home treatmentteam.
We observed an assessment and reviewed notes. We foundthat cultural needs were included and staff consideredcultural or personal preferences as part of the assessment.There was a good mix of staff from different culturalbackgrounds which reflected the ethnic and culturaldiversity of the local communities.
The environment of the bay designated for mental healthassessment at Bradford Royal Infirmary offered littleprivacy and dignity as it was curtained on one side withbays either side. It was inappropriate to carry out MHAassessments which occur on a relatively regular basis.People could be cared for in that room for up to eight hours(and beyond) while waiting for a bed or MHA assessment
and it was not appropriate for the reception of people inmental distress. The trust are reliant on the acute hospitalfor the availability of premises and rooms within the A&Edepartment and we were told that there was no other areathat could be utilised on a permanent basis although aprivate room could be found on request.
People using services involvementPeople we spoke with understood about their medicationand were happy to talk to staff about side-effects as well asany benefits. People demonstrated an understandingabout their mental illness and the role of medication asone part of their holistic treatment.
Staff were clear about how to secure advocacy services forpeople. If people needed long term support from anadvocate staff told us they could refer them to theadvocacy service. People told us the social care staffworking within teams had supported them to accessservices and act as advocates when necessary. We sawevidence of appropriate literature and information beingroutinely provided to people throughout their treatmentand we saw that carers were also offered an assessmentand provided with information about services available tothem and their family members. These were available asnecessary in a variety of accessible formats. People told usthat written information was available about otherservices.
Emotional support for care and treatmentWe met and spoke with three people and two carers whoused the intensive home treatment teams. Staff we metwith told us that people’s carers were involved in theirassessment and care planning, which we saw during ourvisits to people. In all the care plans we sampled there wasevidence that carer’s were involved where possible. Thiswas balanced with a person’s right to choose who wasconsulted with about their care and treatment.
The carer of a person using the home treatment team toldus, “They have been here for me.”
Are services caring?By caring, we mean that staff involve and treat people with compassion,kindness, dignity and respect.
Good –––
18 Community-based crisis services Quality Report 15 September 2014

Summary of findingsServices had been developed in consultation with localpeople. People knew how to access help out-of-hours.Those in need of urgent assessment out-of-hours weretold to use A&E services or contact charitable or thirdsector services. If people attended A&E they wereassessed by the psychiatric liaison team and referred toother services.
We observed teams working well together and sawmany examples of good working relationships. Teamswould routinely liaise with the crisis team about peoplethey were particularly concerned about. They also madesure that this information was readily available shouldthey receive contact from them out-of-hours.
We found evidence of trust wide learning fromcomplaints and incidents.
Our findingsPlanning and delivering servicesThe intensive home treatment team was accessed byreferral from general practice via the community mentalhealth team (CMHT) duty system during normal workinghours or single point of access. Otherwise, through out-of-hours services, other primary care health professionals,secondary care inpatient, police stations and A&Edepartments.
The home treatment teams were able to provide telephonesupport and in a crisis assess people and requestassessment under the MHA. Community mental healthteams could alert the intensive home treatment and bedmanagement teams of any pending crisis when peopleaccessed a range of services. This meant that appropriatesystems to share information with other services wereestablished.
Staff informed us that people needing an inpatient bed hadto access this through the intensive home treatmentteams.
Right care at the right timeWe saw that following referral people were seen by theintensive home treatment team within 4 hours for newpatients or 24 hours for known patients. We saw that
people were offered access to psychological therapieswithin 10 working days and that people were referred toother teams when the ‘crisis’ phase had passed or asappropriate for further support. People were not kept onthe team’s caseloads and staff worked within NICE(National Institute for Health and Care Excellence)guidance.
The single point of access team was based at the Airedaleand Lynfield Mount hospital sites and offered a telephonereferral service for the whole trust to which GPs referred to.There were no medical staff in the team. Call handlers tookthe initial contact and passed the referral to the dutyofficers. Duty officers also took referrals from primary care.Duty officers completed the referral process and passedless priority work to the duty teams based in thecommunity mental health teams. The team operatedMonday to Friday 8am to 5pm.
A non-medical prescriber assessment was being furtherdeveloped as part of the service. Crisis teams had non-medical prescriber nurses based with them. We spoke withnon-medical prescribing staff and reviewed a treatmentplan. Staff told us this role was functioning well.
During the unannounced visit we case tracked some of therecent breaches of the four-hour waiting rule in A&E. Wesaw that there were at times delays in referring to A&Eliaison but this was usually accounted for or reported asthe person receiving urgent medical attention, recoveringfrom physical health issues or as intoxicated. The A&Eliaison service was as responsive as they could be whennormally only one person was on duty. We saw that A&Eliaison saw people within short periods of time once theywere referred during the core hours of when a service wasprovided.
However, there were spikes in demand. For example on amorning before the inspection, there were seven peoplereferred to A&E liaison. Some of these referrals related topeople who had not been able to access a service due tothe gap in provision throughout the night – although someof these referrals were from the wards rather than theA&E. These referrals were prioritised but it still meant thatthere was a delay in seeing everybody who was referred.
Care PathwayStaff told us that all members of the team were valued andrespected regardless of discipline or level of seniority. Wesaw how team members worked collaboratively and well
Are services responsive topeople’s needs?By responsive, we mean that services are organised so that they meet people’sneeds.
Good –––
19 Community-based crisis services Quality Report 15 September 2014

together. Transfer of care between teams was said to befaster as community mental health and assertive outreachstaff were located in the same offices in some areas andthis helped speed up transfers to these teams. Staff told usthat since the case management system was introducedconsultant caseloads had been reviewed and reduced. Thishad created a more fluid system and capacity in thecommunity mental health teams had increased, withwaiting times to access these services reduced. Casemanagement monitoring had been introduced into teamsso managers could monitor that people were accessing therelevant care pathway and being referred to other servicesor discharged within appropriate timescales.
Staff were clear about the lines of accountability and whoto escalate any concerns to. Staff were able to describe theother services involved in people’s care pathways and howthe intensive home treatment and A&E services workedwith other services.
The intensive home treatment teams were involved withpeople prior to their discharge from inpatient wards andwith people requiring intensive home treatment follow up.Staff from the respective teams linked into inpatient multi-disciplinary and discharge planning meetings. This meantpeople’s transition back into the community was wellcoordinated and not unnecessarily delayed.
Within teams initial triage was undertaken with peoplebeing referred either by phone or face-to-face to agreeupon the immediate plan of care and level of contact. Thishad a degree of flexibility and was subject to change inconsultation with people. This meant teams we visitedoperated with a degree of flexibility to meet patient needs.
The single point of access and A&E psychiatric liaison staffsaid they worked toward ensuring the patients care
pathway to other services was smooth. However, theseservices were not available 24 hours. A&E psychiatricliaison service at Bradford Royal Infirmary and at AiredaleGeneral Hospital did not operate 24 hours a day. At AiredaleDistrict General Hospital commissioners had extended theopening hours of the service, but this was due to end inMarch 2015. We spoke with the modern matron and servicemanager for Airedale and Bradford hospitals. They told usthat the psychiatric liaison team was responsive to patientsneeds and saw patients as soon as was possible. They saidthe staff from the respective teams would assess patientson inpatient acute medical wards as well as A&E. They saidthey valued the staff and teams responsiveness and hopedthat the teams could increase and offer longer hours sothey could respond over a 24-hour period on a permanentbasis.
Learning from concerns and complaintsStaff were aware of the trust’s complaints policy.Complaints were received directly and passed to the teammanager or from the patient advice and liaison service(PALS). Staff told us that complaints were referred to thePALS service and they did not get involved in individualcomplaints. Advocacy services could also be accessed ifpatient’s required support with making or during acomplaint.
Evidence of trust-wide learning from complaints andincidents was demonstrated through the team managersharing with staff and globally through updates via thetrust email and intranet system. This information wasincluded and discussed in monthly team meetings. Stafftold us they were not always informed of the outcome ofthe complaints made at team level.
Are services responsive topeople’s needs?By responsive, we mean that services are organised so that they meet people’sneeds.
Good –––
20 Community-based crisis services Quality Report 15 September 2014
Summary of findingsStaff were dedicated and felt well supported by theirmanagers. Some staff told us that they had attended the‘listening into action forum’. They also had access to theminutes of management meetings on the intranet. Wesaw evidence on the intranet that staff were consultedabout the trust’s future plans.
The trust’s internet was updated as plans changed. Staffhad a broad understanding of the changes that hadbeen introduced in the organisation, and people usingthe service were regularly asked for their comments andopinions about the service.
Staff were up-to-date with mandatory training, whichmonitored regularly. Staff also used a variety ofsupervision available to them on a regular basis. Staffwere knowledgeable about how to access advocacyservices for people.
There was a trust-wide risk register in place to overseeand identify risks to the trust, staff and people usingservices. We saw that local audits of records werecompleted for the care programme approach (CPA),which staff said managers were able to monitorelectronically.
Our findingsVision and strategyMost of the staff we spoke with told us they felt wellsupported by their managers. They all spoke positivelyabout their role and demonstrated their dedication toproviding quality patient care. They told us that teammanagers and the board engaged with them, providedinformation and consulted with them in a variety offormats. Key messages about the trust werecommunicated to team managers by senior managementand this was then shared with the team.
We ran a number of focus groups as part of the inspectionand spoke to a wide number of staff groups. Staff reportedthat management at team level was good and they feltsupported. However, a number of staff complained thatwhilst they were aware of the trust’s vision and values, theyfelt disconnected from the process of change and that
issues fed back through the consultation process were notlistened to. Team managers commented that they weresupported by their managers but they may not appreciatethe impact that changes had on staff.
Responsible governanceStaff told us that they felt well supported by their linemanager. Staff told us that they received clinical,managerial and group supervision as required. Staffattended monthly team meetings. The trust vision wascascaded through the intranet ‘Connect’ and updateemails. Staff were aware of the ‘culture’ conversations butnot many had participated in them as they said they didnot always have the time to do so.
Staff told us team meetings were good for feedback inregard to audits undertaken. The team meeting weobserved shared relevant information about people theteam were supporting as well as trust business.
We saw evidence of how the trust monitored seriousuntoward incidents within specific services. For examplewe saw a report on figures for the last six months onserious untoward incidents and deaths. There was someevidence that the trust was using the incidents as alearning experience. For example, when they had not beengiven sufficient evidence about people risks or criminal orforensic histories.
In relation to the A&E liaison services, there were limitedjoint arrangements with the acute trust to consider thequality of clinical care, monitoring of quality andgovernance arrangements of the A&E liaison services otherthan the A&E breaches and local quantitative data that theA&E liaison sent to their managers. There were manager tomanager meetings taking place. The acute trust monitoredinformation and data on A&E breaches including where thebreach was attributable to Bradford District Care Trustincluding performance within and outside the four-hourbreach and performance against any locally agreedtargets. This showed that there had been 48 breaches inthe last six months attributable to mental health delayswhich for overall breaches within A&E related to a smallproportion.
From April 2014, where the breach was over eight hoursthere was a root cause analysis undertaken. We were toldthat there has only been one such incident since Aprilwhere mental health was concerned. This related to delaysin waiting for an out-of-hours mental health assessment.
Are services well-led?By well-led, we mean that the leadership, management and governance of theorganisation assure the delivery of high-quality person-centred care, supportslearning and innovation, and promotes an open and fair culture.
Good –––
21 Community-based crisis services Quality Report 15 September 2014

The two trusts contributed to the root cause analysis whichprovided a full description of why the breach had occurredbut limited detail about what could be done to prevent areoccurrence.
Monthly monitoring of records were submitted to thegovernance team by managers. They received reports tomonitor their performance. Audits of records we saw werein-depth in regard to outcomes for people contained incare plans and progress notes. Staff attendance on trainingwas monitored by managers and we saw evidence of highattendance rates for staff training. Training data was seenand this was updated and shared with staff. Staff reportedthat their individual electronic staff records for trainingwere inaccurate at times. We were told by managers thatwhen the system was introduced there was an IT error andthat this had now been fixed. At the time of the errorinformation uploaded by staff was not always recorded.Staff reported that sickness and absence was monitoredand we saw information from the trust that long termsickness absence was higher for a period of time but wasimproving.
Leadership and cultureWe saw a supportive culture within teams. Staff had abroad understanding of the current and future need of the
organisation. We saw that staff were passionate about theirwork and showed a genuine compassion for people. Stafftold us that the chief executive had visited their teams andengaged with staff.
EngagementPeople were asked about their views of the service, forexample in the use of satisfaction surveys which relatedspecifically to the team that cared for them. These askedthem to rate the quality of the staff that supported them.Teams also provided people with surveys about the servicethey had received and we saw evidence of the results ofsurveys in staff offices. There was a high satisfaction ratefrom people using the service. This meant the trust activelysought people’s opinion and participation in improvingservice delivery. Staff were knowledgeable about how toaccess advocacy services for people.
Performance improvementStaff understood their aims and objectives in regard toperformance and learning. Staff told us they valued thesupervision they received and that it was “supportive”. Wesaw that service developments were being monitored forrisks, efficacy and with consideration of local needs. Wesaw that monthly team meetings focussed on teamobjectives and direction particularly through theimplementation of new ways of working as part of thequality audit feedback.
Are services well-led?By well-led, we mean that the leadership, management and governance of theorganisation assure the delivery of high-quality person-centred care, supportslearning and innovation, and promotes an open and fair culture.
Good –––
22 Community-based crisis services Quality Report 15 September 2014