gluten free, positive ttg: now what? - … free, positive ttg: now what? ... objectives • describe...
TRANSCRIPT

25/04/2016
1
GLUTEN FREE, POSITIVE TTG: NOW WHAT?Jennifer Jin MD FRCPCRoyal Alexandra Hospital
GI for GPs 23 April 2016
Objectives
• Describe the role of “biopsy-free” diagnosis of celiac disease (CD)
• Describe the impact of a gluten free diet (GFD) on diagnostic tests for CD
• Discuss the role of tissue transglutaminase (tTG) monitoring in a patient with CD

25/04/2016
2
Disclosures
• None
Gluten Free Museum
25/04/2016
3
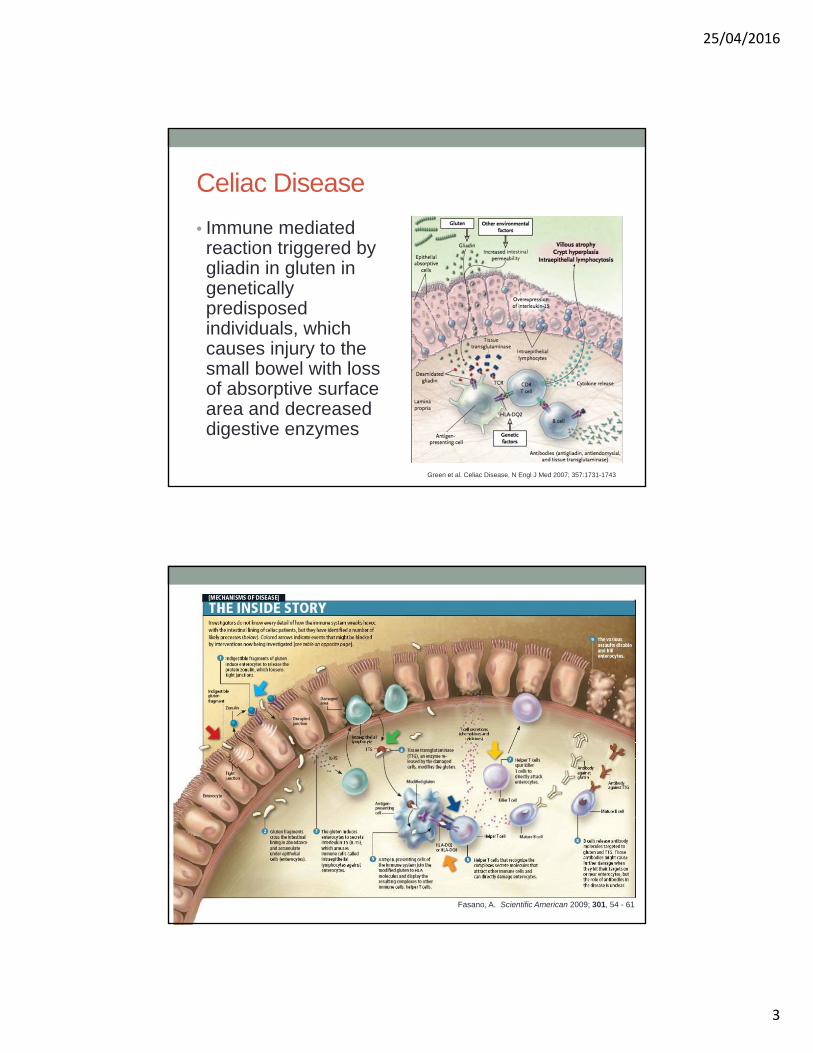
Celiac Disease
• Immune mediated reaction triggered by gliadin in gluten in genetically predisposed individuals, which causes injury to the small bowel with loss of absorptive surface area and decreased digestive enzymes
Green et al. Celiac Disease. N Engl J Med 2007; 357:1731-1743
Fasano, A. Scientific American 2009; 301, 54 - 61
25/04/2016
4
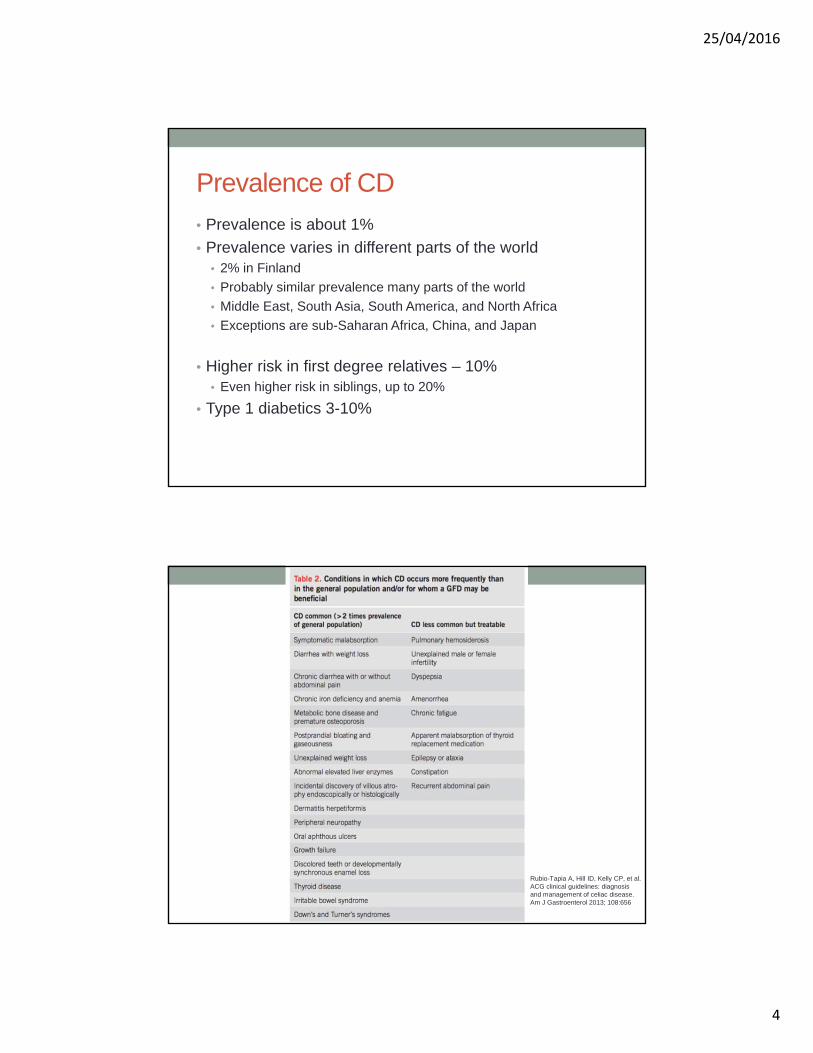
Prevalence of CD
• Prevalence is about 1%
• Prevalence varies in different parts of the world• 2% in Finland
• Probably similar prevalence many parts of the world
• Middle East, South Asia, South America, and North Africa
• Exceptions are sub-Saharan Africa, China, and Japan
• Higher risk in first degree relatives – 10%• Even higher risk in siblings, up to 20%
• Type 1 diabetics 3-10%
Rubio-Tapia A, Hill ID, Kelly CP, et al. ACG clinical guidelines: diagnosis and management of celiac disease. Am J Gastroenterol 2013; 108:656

25/04/2016
5
Dermatitis Herpetiformis
Medscape
CD associations
• Thyroiditis
• Type 1 diabetes
• Autoimmune myocarditis, Idiopathic dilated cardiomyopathy
• Sjögren's syndrome
• Systemic lupus erythematosus
• Autoimmune hepatitis, Autoimmune cholangitis, Primary biliary cirrhosis
• Inflammatory bowel disease
• Systemic and cutaneous vasculitis
• Trisomy 21, Turner’s syndrome, William’s syndrome

25/04/2016
6
Why go gluten free?
• Resolution of GI symptoms
• Decrease risk of malignancies and mortality • Small bowel adenocarcinoma
• Esophageal cancer
• B-cell and T-cell non-Hodgkin lymphomas (including intestinal T-cell lymphomas)
• Improvement of bone mineral density
• Deceases risk of infertility, spontaneous abortions, pre-term deliveries, and low birth weight infants
Testing for CD
• Autoantibodies:• IgA endomysial antibodies (anti-EMA IgA) – sensitivity 85 – 98%;
specificity 97 – 100%
• IgA tissue transglutaminase antibodies (anti-TTG IgA)–sensitivity 90 – 98%; specificity 95 – 97%
• Antibodies targeting the offending agent (gliadin):• Conventional antigliadin antibodies (AGAs – no longer done)
• Antibodies against synthetic deamidated gliadin peptides (DGPs):
• Anti-DGP IgA– sensitivity 94%; specificity 99%
• Anti-DPG IgG– sensitivity 92%; specificity 100%

25/04/2016
7
tTG IgA
• Selective IgA deficiency is more common in patients with celiac disease than in the general population
• 2 – 5% versus 0.5%
• Test for IgA levels concurrently with anti-tTG to avoid a false negative
• False positive of anti-tTG IgA is rare
Rubio-Tapia A, Hill ID, Kelly CP, et al. ACG clinical guidelines: diagnosis and management of celiac disease. Am J Gastroenterol 2013; 108:656.

25/04/2016
8
Gluten Free Museum
Role of biopsy in CD
• 2012 European Society for Pediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) guidelines:
• Histological assessment may be omitted in symptomatic patients who have high IgA anti-TG2 levels (10 times above ULN), verified by EMA positivity, and are HLADQ2 and/or HLA-DQ8 heterodimer positive
Husby S et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J. Pediatr. Gastroenterol.Nut 2012. 54(1), 136–160
25/04/2016
9
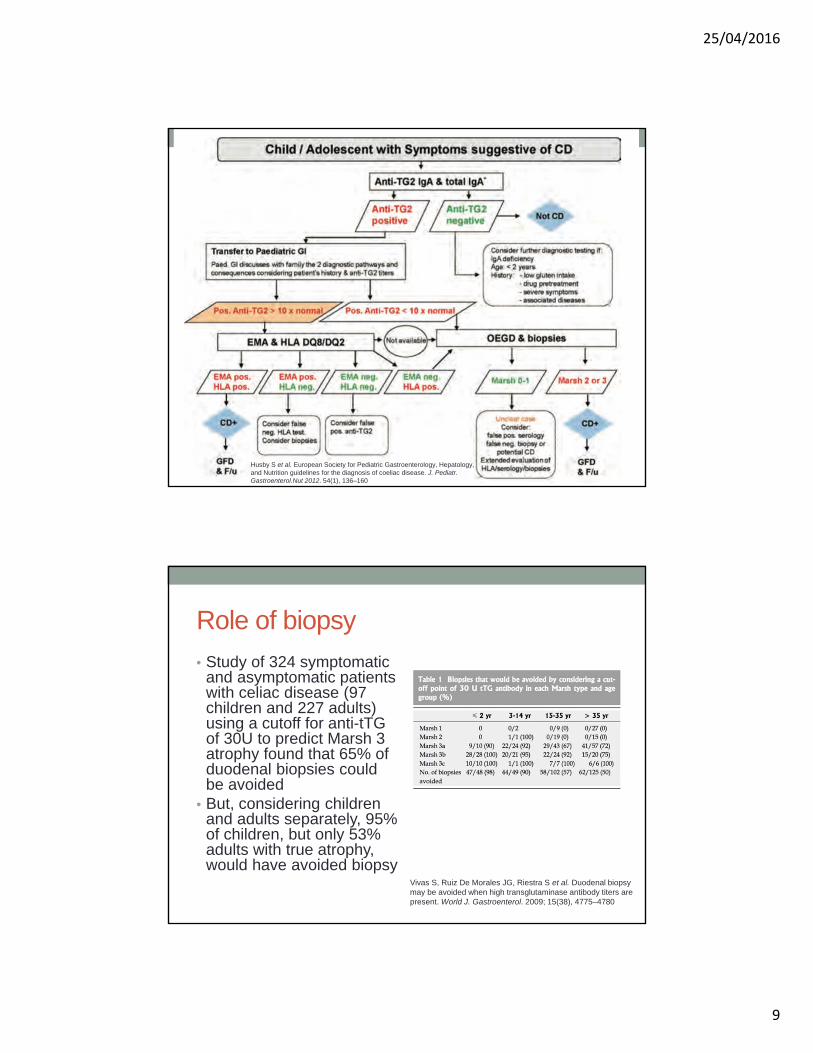
Husby S et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J. Pediatr. Gastroenterol.Nut 2012. 54(1), 136–160
Role of biopsy
• Study of 324 symptomatic and asymptomatic patients with celiac disease (97 children and 227 adults) using a cutoff for anti-tTGof 30U to predict Marsh 3 atrophy found that 65% of duodenal biopsies could be avoided
• But, considering children and adults separately, 95% of children, but only 53% adults with true atrophy, would have avoided biopsy
Vivas S, Ruiz De Morales JG, Riestra S et al. Duodenal biopsy may be avoided when high transglutaminase antibody titers are present. World J. Gastroenterol. 2009; 15(38), 4775–4780

25/04/2016
10
Positive data in adults
BurginWolff A, Mauro B, Faruk H. Intestinal biopsy is not always required to diagnose celiac disease: a retrospective analysis of combined antibody tests. BMCGastroenterol. 2013; 13, 19.
Role of biopsy• In asymptomatic patients with low positive titer antibodies,
biopsy is almost always required to confirm or exclude CD, due to the risk of false positive serology
• Effect of pre-test probability• Biopsy reveals grade of mucosal abnormality which is
helpful if follow-up biopsies are needed, especially in patients with persistent or recurrent symptoms
• Important to confirm a correct diagnosis as a lifelong GFD is expensive and socially inconvenient• Definitive diagnosis may help compliance
• Important in regards to follow up for other CD related considerations, screening family members, and monitoring for complications
25/04/2016
11
Testing and GFD
• Ideally testing should be done on a gluten-containing diet
• If the duration of GFD has been brief (<1 month), serology and histology are often still abnormal
• However, some patients will also quickly revert to normal on a GFD

25/04/2016
12
Testing on a GFD
• Check serology on a GFD
• If negative can consider HLA testing or gluten challenge
HLA haplotype
• 95% of patients carry an DQ2 haplotype while the remaining 5% carry DQ8
• If negative then CD is very unlikely
• NPV>99%
• HLA testing also helpful biopsy results are equivocal

25/04/2016
13
Gluten challenge
• Formal: 3g per day of gluten (2 slices of bread) for 2 weeks and if tolerated, extend for 6 more weeks with biopsy and repeat serology at 8 weeks
When does serology normalize
• After 6 – 12 months on a GFD, 80% will be negative
• By 5 years, >90% will have negative serology
• Lower titre less sensitive for ongoing mucosal abnormality
25/04/2016
14
Symptom improvement on GFD
• Up to 70% of patients have improved symptoms after 2 weeks of a GFD
How much gluten is “safe”?
• 10mg per day probably will not cause mucosal injury in most patients

25/04/2016
15
Oats
• Commercial oats are likely contaminated with gluten
• Pure oats may be safe in limited quantities
• Limit to 50-60g per day
• Reintroduce only in mild disease or after a GFD is maintained
• Better to avoid in severe CD
Oats
• Subset of CD patients may be intolerant to pure oats avenins
• About 5%

25/04/2016
16
Untreated CD – micronutrient deficiencies
• Iron
• Folic Acid
• Vitamin B12 and B6
• Vitamin D
• Copper, zinc, carnitine
Monitoring of CD
• TTG IgA
• BMD
• Pneumococcal vaccination • Hyposplenism
25/04/2016
17
Gluten Free Museum
Non-responsive or refractory CD• Persistent symptoms, signs or lab abnormalities typical of
CD despite 6 – 12 months of GFD• 7 – 30% of patients
• Most common cause is inadvertent gluten ingestion (35-50%)
• Other causes:• Irritable bowel syndrome (normal mucosa)• Other dietary intolerances such as lactose intolerance (normal
mucosa)• Pancreatic inefficiency (normal mucosa)• Microscopic colitis • Small bowel bacterial overgrowth (may have villous atrophy)• True refractory CD, ulcerative jejunitis, lymphoma
25/04/2016
18
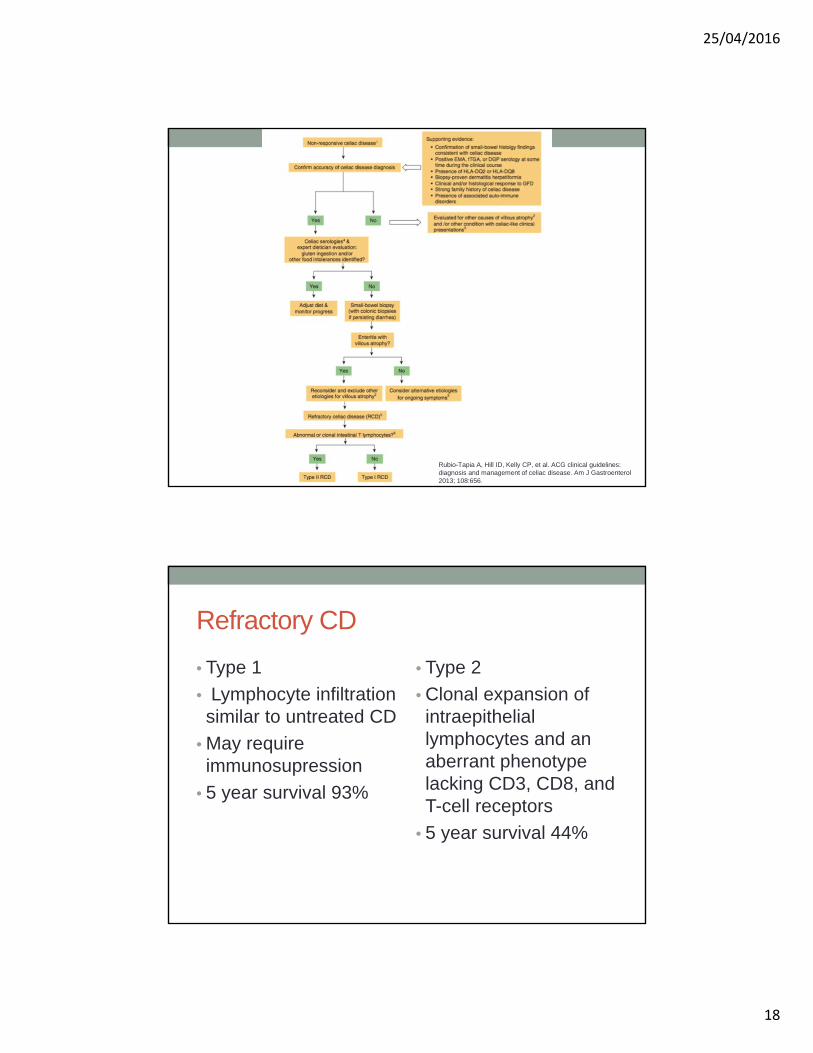
Rubio-Tapia A, Hill ID, Kelly CP, et al. ACG clinical guidelines: diagnosis and management of celiac disease. Am J Gastroenterol2013; 108:656.
Refractory CD
• Type 1
• Lymphocyte infiltration similar to untreated CD
• May require immunosupression
• 5 year survival 93%
• Type 2
• Clonal expansion of intraepithelial lymphocytes and an aberrant phenotype lacking CD3, CD8, and T-cell receptors
• 5 year survival 44%
25/04/2016
19
TTG levels
• Italian study of 2245 patients over 5 years with annual anti-tTG
• Proportion of patients with negative tTG progressively increased from 83% to 93% during the 5-year follow-up
• Affected by• Poor adherence to gluten-free diet (HR 4.764)
• Long duration of gluten-free diet (HR 0.929)
• Female gender (HR 1.472) were independently associated with serological outcome
• In individual patients, 69% were “persistently negative”, 1% “persistently positive” and 30% “intermittently negative or positive”
• In a US study, the median time from onset of GFD to achieve mucosal healing was 3 years
• Could consider a follow-up biopsy in adults after 2 years of starting a GFD to assess for mucosal healing

25/04/2016
20
Resources
• Referral to dietitian
• Canadian Celiac Association • www.celiac.ca
• Food choices, labeling, cross contamination, recipe adaptation, advice on social situations
• Links to local chapters
Take home points
• Keep a high index of suspicion as symptoms are variable, and can affect patients of all ages and ethnicities
• Remember to order an IgA in case there is a deficiency
• Optimal to obtain biopsies on a gluten containing diet
• HLA DQ2 and DQ8 have a very high NPV (>99%)
• By 6 – 12 months 80% of patients will be negative
• If recurrent symptoms, review diet, check serology, consider refractory CD
25/04/2016
21
References • Rubio-Tapia A, Hill ID, Kelly CP, et al. ACG clinical guidelines: diagnosis and management of celiac disease. Am J Gastroenterol 2013; 108:656• Rostom A, Murray JA, Kagnoff MF. American Gastroenterological Association (AGA) Institute technical review on the diagnosis and management of celiac
disease. Gastroenterology. 2006 Dec;131(6):1981-2002.• Bai JC, Fried M, Corazza GR, et al. World Gastroenterology Organisation global guidelines on celiac disease. J Clin Gastroenterol 2013; 47:121• Wu J, Xia B, von Blomberg BME, et al. Coeliac disease: emerging in China? Gut 2010; 59: 418– 9• Van de Wal Y, Kooy Y, van Veelen P, Peña S, Mearin L, Papadopoulos G, Koning F Selective deamidation by tissue transglutaminase strongly enhances
gliadin-specific T cell reactivity. J Immunol. 1998;161(4):1585• (Lewis NR, Scott BB. Meta-analysis: deamidated gliadin peptide antibody and tissue transglutaminase antibody compared as screening tests for coeliac
disease. Aliment Pharmacol er 2010 ;31:73–81)• van der Windt DA, Jellema P, Mulder CJ et al. Diagnostic testing for celiac disease among patients with abdominal symptoms: a systematic review. JAMA
2010; 303:1738–46 • Swallow K, Wild G, Sargur R et al. Quality not quantity for transglutaminase antibody 2: the performance of an endomysial and tissue transglutaminase test
in screening coeliac disease remains stable over time. Clin. Exp. Immunol 2012; 171(1), 100–106 • Husby S, Koletzko S, Korponay-Szabo IR et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of
coeliac disease. J. Pediatr. Gastroenterol.Nut 2012. 54(1), 136–160 • Vivas S, Ruiz De Morales JG, Riestra S et al. Duodenal biopsy may be avoided when high transglutaminase antibody titers are present. World J.
Gastroenterol. 2009; 15(38), 4775–4780• Rashtak S, Ettore MW, Homburger HA et al. Comparative usefulness of deamidated gliadin antibodies in the diagnosis of celiac disease. Clin Gastroenterol
Hepatol 2008;6(4):426-32 • BurginWolff A, Mauro B, Faruk H. Intestinal biopsy is not always required to diagnose celiac disease: a retrospective analysis of combined antibody tests.
BMCGastroenterol. 2013; 13, 19• Vermeersch P, Geboes K, Marien G, Hoffman I, Hiele M, Bossuyt X. Defining thresholds of antibody levels improves diagnosis of celiac disease.
Clin.Gastroenterol. Hepatol. 2013; 11(4), 398–403 • Katz KD, Rashtak S, Lahr BD et al. Screening for celiac disease in a North American population: sequential serology and gastrointestinal symptoms. Am.
J.Gastroenterol. 2011; 106(7), 1333–1339 • Zanini B, Lanzarotto F, Mora A et al. Five year time course of celiac disease serology during gluten free diet: results of a community based “CD-Watch”
program. Dig Liver Dis 2010;42:865–70• Abdulkarim AS, Burgart LJ, See J et al. Etiology of nonresponsive celiac disease: results of a systematic approach. Am J Gastroenterol 2002;97:2016–21• Nachman F, del Campo MP, González A, et al. Long-term deterioration of quality of life in adult patients with celiac disease is associated with treatment
noncompliance. Dig Liver Dis 2010; 42: 685–91. • Akobeng AK, omas AG. Systematic review: tolerable amount of gluten for people with coeliac disease. Aliment Pharmacol er 2008;27:1044–52).• Rashid M, Butzner D, Burrows V et al. Consumption of pure oats by individuals with celiac disease: a position statement by the Canadian Celiac
Association. Can J Gastroenterol 2007;21:649–51) • Zanini B, Lanzarotto F, Mora A et al. Five year time course of celiac disease serology during gluten free diet: results of a community based “CD-Watch”
program. Dig Liver Dis 2010;42:865–70.