giulio metro s.c. oncologia medica ospedale santa maria ...tecnlab/materiale...
TRANSCRIPT

mutazione di BRAF nel melanoma e
immunoterapia nel melanoma e tumore
polmonare
Giulio Metro
S.C. Oncologia Medica – Ospedale Santa Maria della
Misericordia, Azienda Ospedaliera di Perugia
“Corso di laurea in tecniche di laboratorio biomedico”
5 Aprile 2016, Perugia

Screening
SEER Stat Fact Sheets:Melanoma of the Skin
GLOBOCAN 2012
Nessun consenso esiste sulla definizione di popolazionead alto rischio o sull’appropriato intervallo di screening
La sorveglianza della popolazione ad alto rischio nonriduce la mortalità da melanoma
Evidenza insufficiente di un impatto positivo delloscreening sulla mortalità
Screening sovradiagnosi e biopsie non necessarie
POPOLAZIONE AD ALTO RISCHIO1.Storia personale2.Storia familiare3.Numerosi e atipici nevi4.Carnagione chiara in uomini e donne >65 anni

Korn E. et al. J Clin. Oncol. 2008; 26:527-34
Sopravvivenza mediana: 6.2 months
Vivi ad 1 anno: 25.5%
Sopravvivenza libera da progressione: 1.7 months
Liberi da progressione a 6 mesi: 14.5%
Meta-analisi di studi di fase II di gruppi cooperativi: cosa si puòottenere nel melanoma metastatico con la chemioterapia?

Recettori
tirosin-
chinasici
Ligando
RAS
RAF
MEK 1
GTP
GDP
MEK 2
ERK 1
ERK 2
Proliferazione &
sopravvivenza
cellulare
PI3K
AKT
mTOR
La via RAS/RAF/MEK/ERK: BRAF
BRAFi (Vemurafenib,
Dabrafenib)

BRAF
1. Flaherty KT, et al. Cancer 2010;116:4902–13.
2. Garnett MJ, et al. Cancer Cell 2004;6:313–9.
3. Karreth FA, et al. Curr Opin Genet Dev 2009;19:4–11.
• Le chinasi RAF sono componenti della via MAP chinasi1
• Le chinasi RAF mediano la via del segnale RAS-RAF, che trasmette i segnali
proliferativi dalla superficie cellulare tramite I recettori dei fattori di crescita. In
condizioni normali tali segnali mediano il controllo fisiologico della proliferazione,
differenziazione e sopravvivenza1-3
• BRAF è espresso soprattutto nei tessuti neuronali e melanociti1
• Le MAP chinasi (MEK) sono l’unico substrato conosciuto di BRAF1
• La deregolazione del segnale RAS-RAF è stata implicata nello sviluppo
tumorale3
BRAFV600
cell
proliferation and
survival
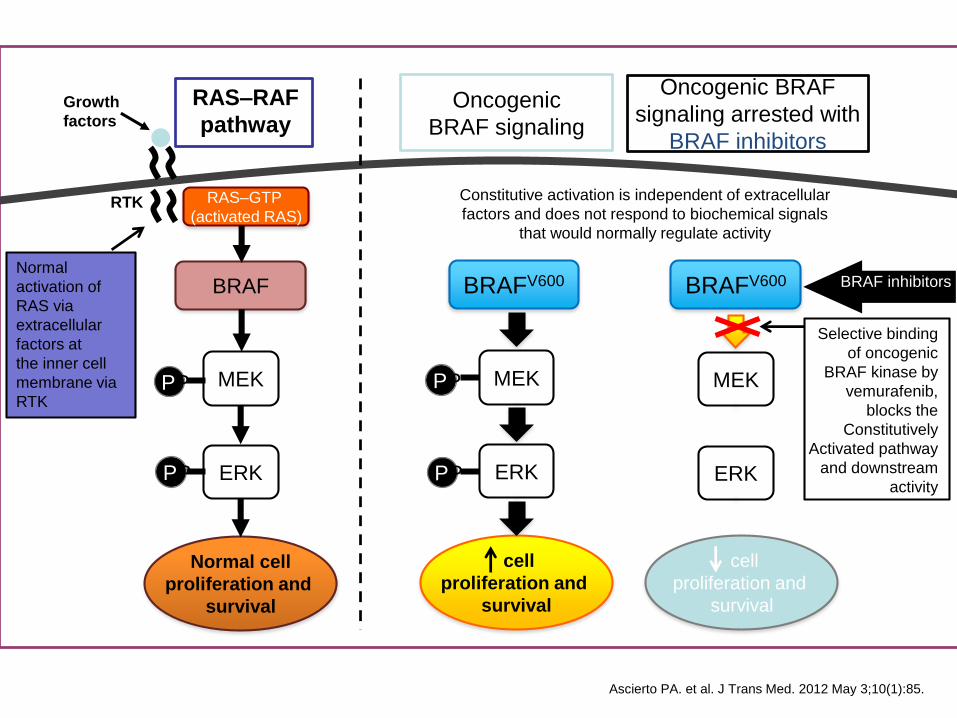
Constitutive activation is independent of extracellular
factors and does not respond to biochemical signals
that would normally regulate activity
RAS–RAF
pathway
BRAF
Normal cell
proliferation and
survival
Normal
activation of
RAS via
extracellular
factors at
the inner cell
membrane via
RTK
BRAFV600
MEK
ERK
MEK
ERK
MEK
ERK
cell
proliferation and
survival
RAS–GTP
(activated RAS)
BRAF inhibitors
Growth
factors
PP
PP
PP
PP
RTK
Oncogenic
BRAF signaling
Oncogenic BRAF
signaling arrested with
BRAF inhibitors
Selective binding
of oncogenic
BRAF kinase by
vemurafenib,
blocks the
Constitutively
Activated pathway
and downstream
activity
Ascierto PA. et al. J Trans Med. 2012 May 3;10(1):85.

BRAF Mutations Affect
Kinase Activity• Ninety percent of BRAF mutations in melanoma result in substitution at
position V6002
– All tested mutations at V600 are classified as high-activity mutants
when compared with BRAFwild-type (WT)3,4
– These mutations constitutively stimulate ERK phosphorylation3
• A unifying feature of the high- and intermediate-activity BRAF mutants is
that they disrupt the hydrophobic interaction between the P loop and the
activation segment of the kinase domain4
– This results in destabilization of the inactive conformation of BRAF,
thus stimulating its kinase activity and leading to increased ERK
phosphorylation
BRAF = rapidly accelerated fibrosarcoma isoform B; ERK = extracellular signal―regulated kinase; WT = wild-type.1. Forbes SA, et al. Nucleic Acids Res 2010;38:D652–7 2. Garnett MJ, et al. Cancer Cell 2004;6:313–9.
BRAF Mutation
at Position V600
Melanomas (Total
2,651 V600X)1
Relative
Frequency (%)1
V600E 2,436 91.9
V600K 162 6.1
V600D 35 1.3
V600R 18 0.7
3. Wan PTC, et al. Cell 2004;116:855–67. 4. Pritchard C, et al. Biochem Soc Trans 2007;35:1329–33.
BRAF kinase domain structure. Position 600 is indicated in yellow. The BRAF activation segment is shown in purple; dashes indicate the region that was not resolved. The P loop is shown in green (adapted from Garnett MJ, et al).2

Types of BRAF mutation in melanoma

Clinicopathologic features
• Studies evaluating matched primary and metastatic melanomas
showed that BRAF mutations in primary tumor are maintained in
metastatic lesions1
• Patients with multiple metastasis showed, with few exceptions, the
same BRAF mutation in all tested lesions1
• BRAF mutations are early somatic events in the development of many
melanoma2
• Features of antecedent primary melanoma significantly associated with
BRAF mutation are histology (superficial and nodular), truncal
location, presence of mitoses, age at diagnosis ≤ 50 years2, 3
1. Omholt et al Clin Can res 20032. Platz A et al Mol Oncol 2008
3. Long G JCO 2011 Apr 1;29(10):1239-46
1. Long G JCO 2011 Apr 1;29(10):1239-46.2. Platz A et al Mol Oncol 2008
Prognostic and clinicopathologic associations of
oncogenic BRAF in metastatic melanoma
• The prognostic role of BRAF V600 mutation is still debated
• Some studies support a possible negative impact of BRAF mutations on
prognosis in metastatic melanoma1,2 .
• The presence of mutant BRAF had no impact on the disease-free interval from
diagnosis of first-ever melanoma to first distant metastasis; however, it may
have an impact on survival thereafter1
• BRAF mutations were significantly associated with diminished duration of
response to chemotherapy and the presence of BRAF mutations in melanoma
metastases was associated with shortened survival from the time point of
removal of the lesions or from the diagnosis of stage IV disease (Kumar 2003;
Houben 2004).

Testing Methods for BRAF Mutation Analysis
PCR Real-time Sequencing

BRAFV600E Kinase Mutation
Cellular
Proliferation
RTK
RAF
ATP
ATP
ERK
MEK
BRAFV600E
RAS
40-60% of melanomas
Chapman P. et al Abs LBA4 ASCO 2011

Vemurafenib inhibits BRAFV600E Kinase
Cellular
Proliferation
RTK
RAF
VEMURAFENIB(PLX4032, RO5185426)
ATP
ATP
ERK
MEK
BRAFV600E
RAS
40-60% of melanomas
Chapman P. et al Abs LBA4 ASCO 2011

Vemurafenib Is Selective for Oncogenic BRAF
• Vemurafenib is a small molecule inhibitor that binds potently to and selectively
inhibits the oncogenic BRAF kinase (BRAFV600)1
• Developed by a structure-guided discovery approach coupled with
optimization chemistry1,2
• Has a novel mode of action
Vemurafenib binds to the oncogenic BRAF
kinase (yellow) (adapted from Bollag G, et al)1
BRAF = rapidly accelerated fibrosarcoma isoform B.
1. Bollag G, et al. Nature 2010;467:596–9.2. Tsai J, et al. Proc Natl Acad Sci USA 2008;105:3041–6.
Vemurafenib1

Vemurafenib Inhibits Tumor Growth in
Vivo1
BID = twice daily; QD = once daily; SEM = standard error of the mean.
1. Yang H, et al. Cancer Res 2010;70:5518–27.
• Vemurafenib is reported to inhibit tumor growth and prolong survival in BRAF
mutation-positive melanoma xenograft models:
Mice implanted with Colo829 xenografts started treatment 17 days after implantation. Animals were treated with vehicle or Vemurafenib at a dose of 100 mg/kg BID for 21 days or with temozolomide at a dose of 100 mg/kg once daily for 5 days
Vehicle BID x 21 days
Vemurafenib 100 mg/kg BID x 21 days
Temozolomide 100 mg/kg QD x 5 days
Days after tumor cell implant
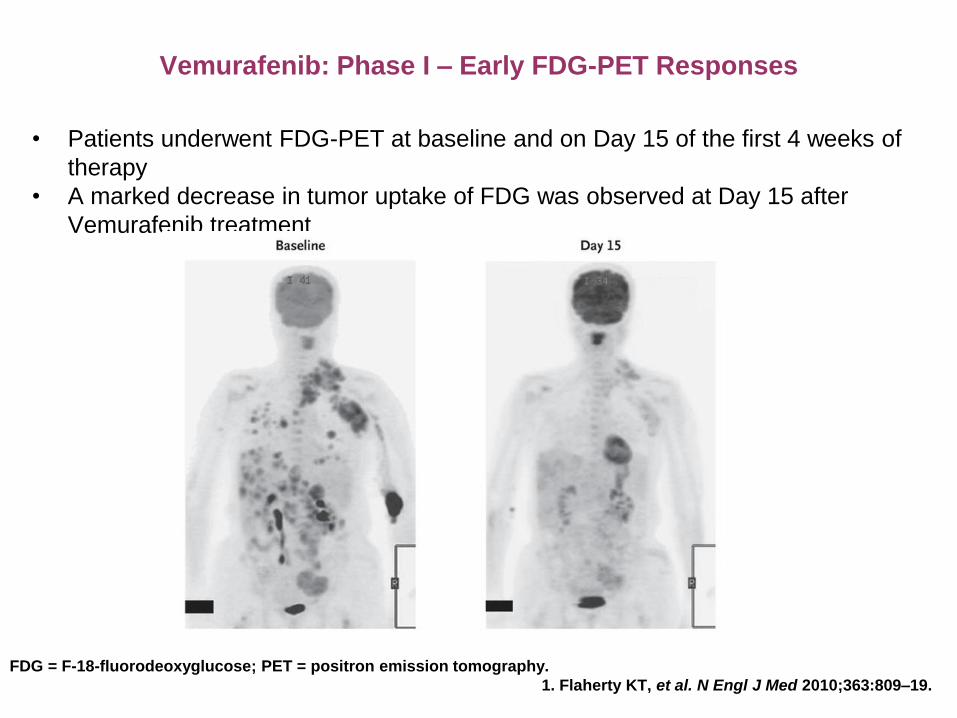
Vemurafenib: Phase I – Early FDG-PET Responses
FDG = F-18-fluorodeoxyglucose; PET = positron emission tomography.
1. Flaherty KT, et al. N Engl J Med 2010;363:809–19.
• Patients underwent FDG-PET at baseline and on Day 15 of the first 4 weeks of
therapy
• A marked decrease in tumor uptake of FDG was observed at Day 15 after
Vemurafenib treatment

BRIM-2 (NP22657): Phase II Study in Previously
Treated Patients with Metastatic Melanoma1,2
* Ascertained by the cobas® 4800 BRAF V600 Mutation Test.
AJCC = American Joint Committee on Cancer; BID = twice daily;
• Multicenter (USA and Australia), open-label, Phase II study
• Enrolment completed
• Primary endpoint:
– BORR (RECIST, version 1.1) assessed by IRC every 6 weeks
• Key secondary endpoints:
– BORR assessed by investigator
– Duration of response, PFS and OS
– Safety and tolerability
– Quality of life
– Validation of cobas® 4800 BRAF V600 Mutation Test
– PK and effect on QT interval and correlation on exposure using
electrocardiogram parameters
Vemurafenib (960 mg BID orally)
• 132 patients enrolled • Metastatic melanoma (stage IV, AJCC) • BRAFV600 positive*• Failed ≥ 1 prior therapy
1. Sosman J, et al. Oral presentation at Melanoma 2010, Sydney, Australia. 2. A Study of RO5185426 in previously treated patients with metastatic melanoma. NCT00949702. Available at www.clinicaltrials.gov (last accessed August 10, 2010).
0
10
20
30
40
50
60
70
CR+PR SD PD
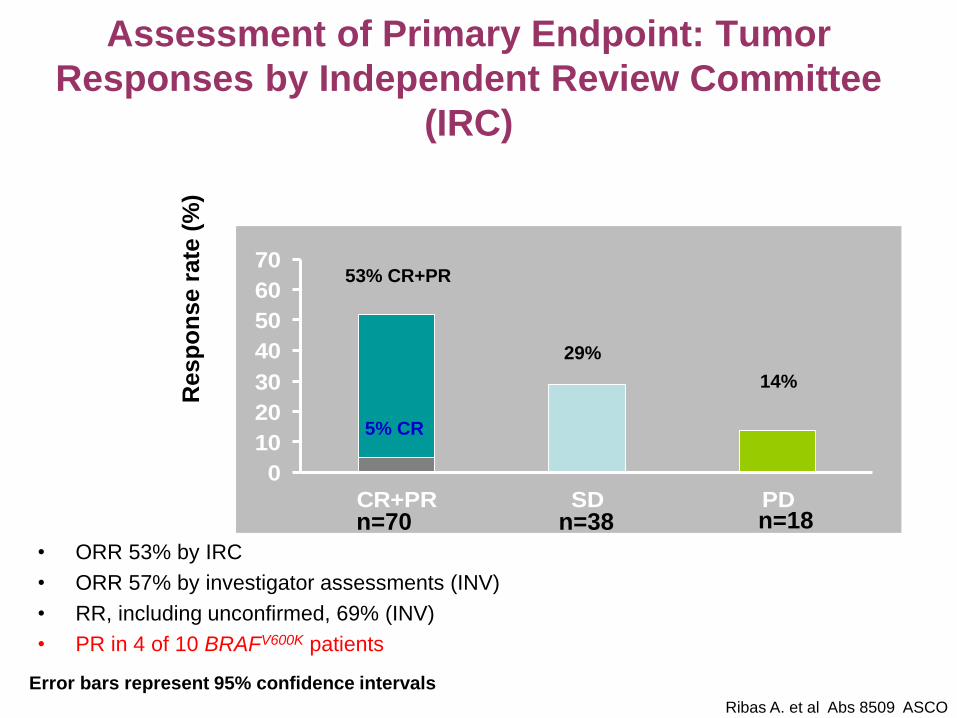
Assessment of Primary Endpoint: Tumor
Responses by Independent Review Committee
(IRC)
• ORR 53% by IRC
• ORR 57% by investigator assessments (INV)
• RR, including unconfirmed, 69% (INV)
• PR in 4 of 10 BRAFV600K patients
Resp
on
se r
ate
(%
)
n=70 n=38 n=18
53% CR+PR
5% CR
29%
14%
Error bars represent 95% confidence intervals
Ribas A. et al Abs 8509 ASCO
2011

BRIM-3 (NO25026): Phase III Study in Previously
Untreated Patients with Metastatic Melanoma
• International, multicenter, randomized, open-label Phase III study
• This study is currently ongoing
• Co-primary endpoints:
– Overall survival
– PFS
• Key secondary endpoints:
– Efficacy: BORR, time to response, duration of response, time to
treatment failure
– Safety and tolerability
– Pharmacokinetics
– Contribute to validation of cobas® 4800 BRAF V600 Mutation Test
Vemurafenib(960 mg BID orally)
Dacarbazine(1000 mg/m2 IV q3w)
1:1
o Estimated enrollment: 680 patients o Unresectable metastatic melanoma (stage
IIIc/IV, AJCC) o BRAFV600 mutation positive, determined
by cobas® 4800 BRAF V600 Mutation Testo Chemo-naïve for advanced disease
N=680
NCT01006980. Available at www.clinicaltrials.gov (last accessed August 10, 2010).
Chapman P. et al Abs LBA4 ASCO 2011

100
90
80
70
60
50
40
30
20
10
0
Pro
gre
ssio
n-f
ree
su
rviv
al (
%)
0 6 12 18 24
338
337
63
186
22
77
3
16
0
0
100
269
37
113
14
49
0
3
No. at risk
1.6 6.9
Hazard ratio 0.38 (95% CI: 0.32–0.46)Log-rank p<0.001 (post-hoc)
Dacarbazine(n=338)
Vemurafenib (n=337)
Progression-free survival (February 01, 2012
cut-off) censored at crossover
Time (months)
Dacarbazine
Vemurafenib
Chapman P. et al. abs 8502
ASCO Ann. Meeting Chicago 2012
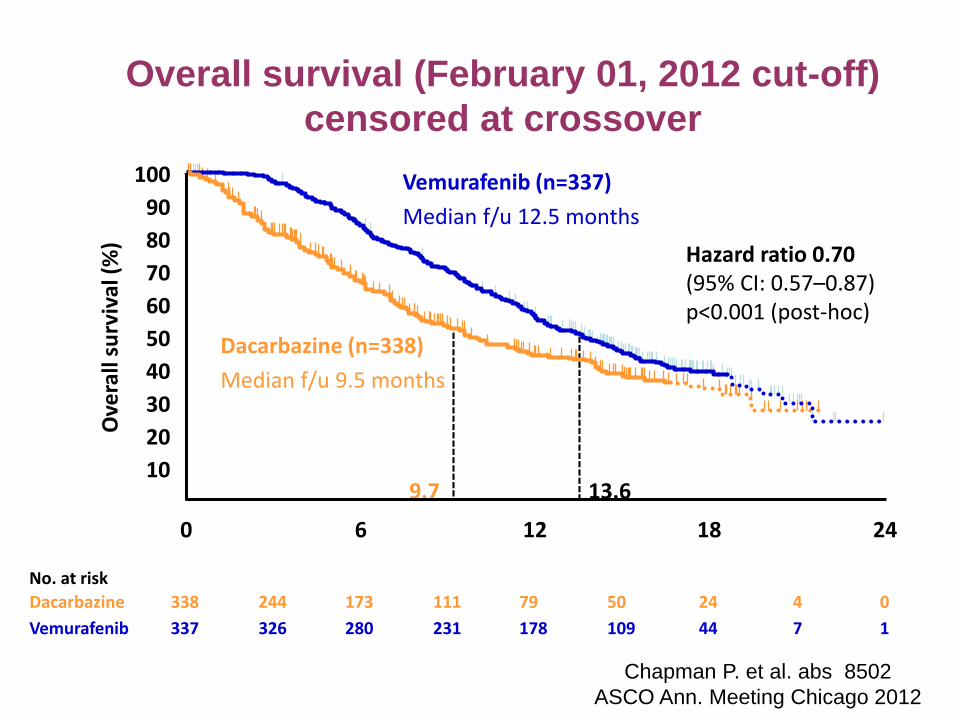
100
90
80
70
60
50
40
30
20
10
0
Ove
rall
surv
ival
(%
)
0 6 12 18 24
Vemurafenib (n=337)
Median f/u 12.5 months
Dacarbazine (n=338)
Median f/u 9.5 months
338
337
173
280
79
178
24
44
0
1
244
326
111
231
50
109
4
7
9.7 13.6
Overall survival (February 01, 2012 cut-off)
censored at crossover
Hazard ratio 0.70 (95% CI: 0.57–0.87)p<0.001 (post-hoc)
Time (months)
Dacarbazine
Vemurafenib
No. at risk
Chapman P. et al. abs 8502
ASCO Ann. Meeting Chicago 2012

Confirmed objective response rates
(RECIST 1.1) across vemurafenib clinical
trial programme
PLX 06-02
Phase I BRIM 2
BRIM-3 ORR(February 01, 2012
cut-off)
Vemurafenib
(95% CI)
56.0%
(38–74)
53.0%
(44–62)
57.0%
Dacarbazine
(95% CI)
– – 8,6%
Mc Arthur G et al ECCO/ESMO Abstract #28LBA
Chapman Annual ASCO Meeting Chicago 2012

Selected adverse events (% of patients)
Vemurafenib, n=337 Dacarbazine, n=287
Adverse events All Grade 3 Grade ≥4 All Grade 3 Grade ≥4
Arthralgia 56 6 – 4 1 –
Rash 41 9 – 2 – –
Fatigue 46 3 – 35 2 –
Photosensitivity 41 4 – 5 – –
LFTs 26 10 1 6 2 –
Cutaneous SCC 19 19 – <1 <1 –
Keratoacanthoma 11 10 – <1 <1 –
Skin papilloma 28 <1 – <1 <1 –
Nausea 38 2 – 45 2 –
Neutropenia <1 – <1 12 6 3
Discontinuations due to AE: 7% vemurafenib; 2% dacarbazine
8 patients reported new primary melanomas in the vemurafenib groupChapman P. et al. abs 8502
ASCO Ann. Meeting Chicago
2012

VEMURAFENIB
Approvazione EU, 17 February 2012
Vemurafenib è indicato come monoterapia per il
trattamento dei pazienti adulti con melanoma
avanzato e mutazione di BRAF V600.
http://ec.europa.eu/health/documents/community-register/html/h751.htm

ExperiencePatients
sample (n)
% of patients with a rapid
disease progression kinetics
BRIM-2 39 41%
BRIM-3 42 52%
Ascierto et al. 28 43%
Ackerman et al. 32 50%
Italian ipi EAP 54 41%
Fisher et al. 42 38%
Evidenza di rapida progressione di malattia all’instaurarsi della
resistenza all’inibitore di BRAF

Meccanismi di resistenza agli inibitori di
BRAF
Recettori
tirosin-
chinasici
Ligando
RAS
RAF
MEK 1
GTP
GDP
MEK 2
ERK 1
ERK 2
Proliferazione &
sopravvivenza
cellulare
PI3K
AKT
mTOR
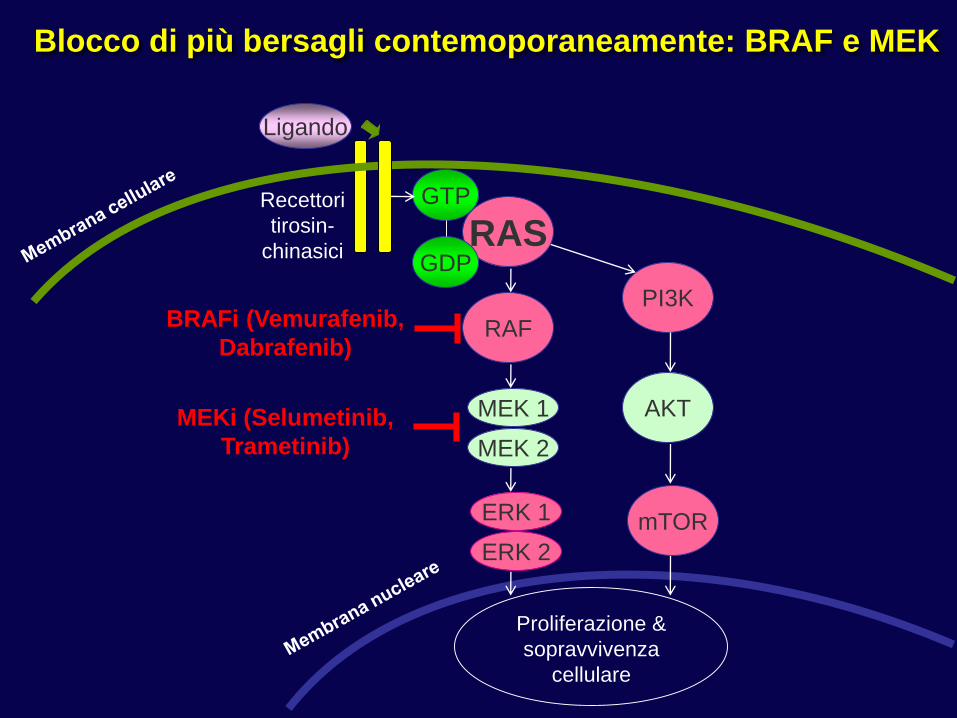
Blocco di più bersagli contemoporaneamente: BRAF e MEK
BRAFi (Vemurafenib,
Dabrafenib)
MEKi (Selumetinib,
Trametinib)

Dabrafenib+trametinib vs Vemurafenib Vemurafenib+cobimetinib vs
vemurafenib+placebo
Sopravvivenza libera da progressione con inibitore di BRAF
+ inibitore di MEK
Dabrafenib/trametenib PFS = 11.4 months
vs HR = 0.56
Vemurafenib PFS = 7.3 months
ORR= 64% vs 51%
Vemurafenib/cobimetinib PFS = 9.9 months
vs HR = 0.51
vemurafenib/placebo PFS = 6.2 months
ORR= 68% vs 45%
Larkin J. et al N Engl J Med. 2014Robert C. et al N Engl J Med. 2015

HR= 0.69
(95% CI 0.53-0.89)
P=0.002
HR = 0.65
(95% CI 0.42-1.00)
P=0.046
Larkin J, et al N Engl J Med. 2014Robert C, et al N Engl J Med. 2015
Sopravvivenza globale con inibitore di BRAF
+ inibitore di MEK
Dabrafenib+trametinib vs Vemurafenib Vemurafenib+cobimetinib vs
vemurafenib+placebo
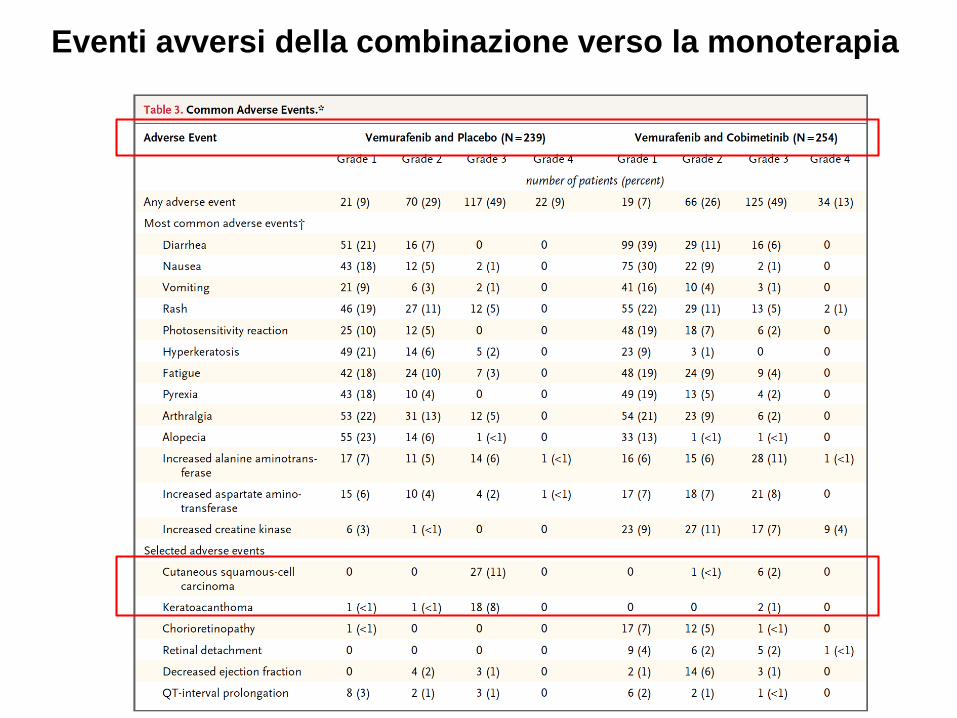
Eventi avversi della combinazione verso la monoterapia

Science, 2013Science 2013


I “checkpoint” immunitari
CTLA-4 = cytotoxic T-lymphocyte-associated antigen 4 ; MHC = major histocompatibility complex; PD-1 = programmed death-1;
PD-L1 = programmed death ligand 1; TCR = T-cell receptor.
Blocco CTLA-4 (ad esempio
ipilimumab)
Blocco PD-1 (ad es. nivolumab,
pembrolizumab)
Fase di iniziazione Fase di effettrice

D E C E M B E R 2 0 1 1 | VO L 4 8 0 | N AT U R E | 4 8 1
Recettori delle cellule T co-stimolatori

From Michot et al. Eur J Cancer 2016
Mel = melanoma; RCC = renal cell carcinoma; NSCLC = non-small cell lung cancer; HNSCC = head &
neck squamous cell cancer; B Cell NHL = B cell non-Hodgkin lymphoma; MSI High CRC = microsatellite
instability high colorectal carcinoma; TNBC; triple negative breast cancer; Mesoth = mesothelioma;
HCC = hepatocellular carcinoma; Oesophag = oesophageal; SCLC = small cell lung cancer
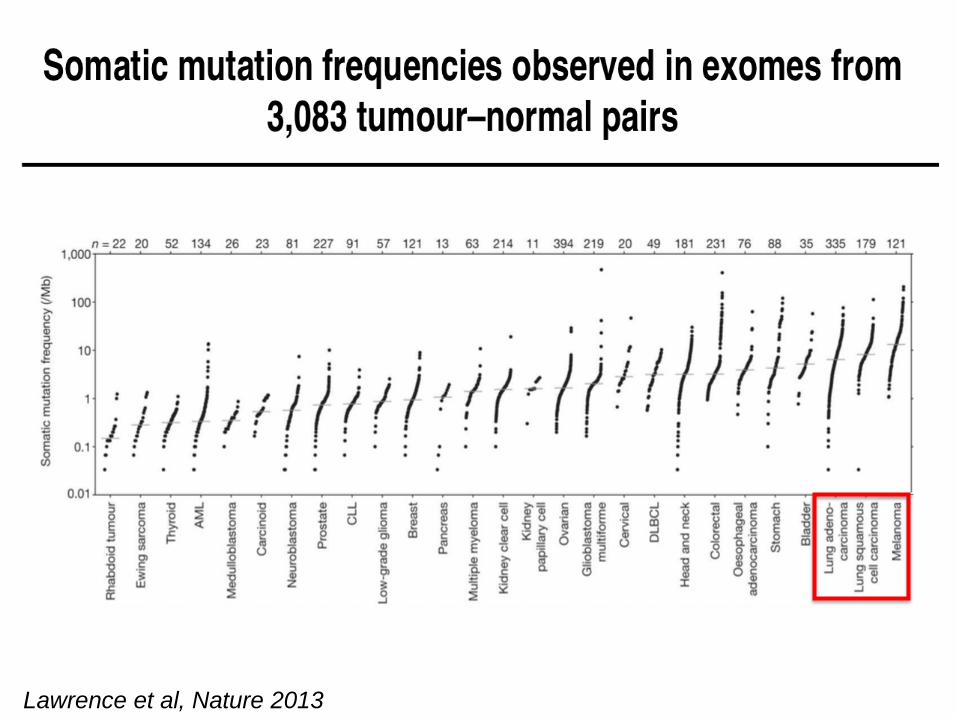
Lawrence et al, Nature 2013Lawrence et al, Nature 2013

Istituto Toscano Tumori – Livorno, Italy
Altered protein contain new epitopes for immune recognition, providing a common denominator for immunotherapy
High mutational rates may contribute to increased immunogenicity

ORR significantly higher with nivolumab vs dacarbazine
(40.0% vs 13.9%, respectively; P < .001)
Biological: Nivolumab
Biological: Placebo matching Nivolumab
Drug: Dacarbazine
Drug: Placebo matching Dacarbazine
R
418 pts
Primary End-Point Overall Survival

Survival End Points
HR for death: 0.42 (99.79% CI: 0.25-0.73; P < .001)
HR for death or disease progression: 0.43 (95% CI: 0.34-0.56; P < .001)
Robert C, et al. N Engl J Med. 2014
The future approach will be greatly informed by results of trials comparing BRAF/MEK inhibition followed by anti–PD-1/PD-L1 plus ipilimumab, vs the opposite strategy, and those evaluating the combination of anti–PD-1/PD-L1 plus ipilimumab.
Treatment paradigm in advanced melanoma poised for change… again
Symptom load may still matter
Toxicity may be an issue
Combination yields promising outcomes

Squamous cell lung cancer: Overall Survival
Symbols represent censored observations
Nivolumab
Docetaxel
135 113 86 69 52 31 15 7 0
137 103 68 45 30 14 7 2 0
Number of Patients at Risk
Time (months)
Nivolumab
Docetaxel
1-yr OS rate = 42%
1-yr OS rate = 24%
OS
(%
)Nivolumab
n = 135
Docetaxel
n = 137
mOS mo,
(95% CI)
9.2
(7.3, 13.3)
6.0
(5.1, 7.3)
# events 86 113
HR = 0.59 (95% CI: 0.44, 0.79), P = 0.00025
24211815129630
100
90
80
70
60
50
40
30
10
0
20

OS by PD-L1 Expression
mOS (mo)
Nivolumab Docetaxel
PD-L1 ≥1% 9.3 7.2
PD-L1 <1% 8.7 5.9
mOS (mo)
Nivolumab Docetaxel
PD-L1 ≥5% 10 6.4
PD-L1 <5% 8.5 6.1
mOS (mo)
Nivolumab Docetaxel
PD-L1 ≥10% 11 7.1
PD-L1 <10% 8.2 6.1
1% PD-L1 Expression level 5% PD-L1 Expression level 10% PD-L1 Expression level
Nivolumab PD-L1+
Nivolumab PD-L1–
Time (months)
24211815129630
Time (months)
24211815129630
Time (months)
24211815129630
100
90
80
70
60
50
40
30
10
0
20
OS
(%
)
24211815129630
100
90
80
70
60
50
40
30
10
0
20
Docetaxel PD-L1+
Docetaxel PD-L1–

Non-squamous cell lung cancer:
Overall Survival
Symbols represent censored observations.
Nivolum
ab
(n =
292)
Doceta
xel
(n =
290)
mOS, mo 12.2 9.4
HR = 0.73 (96% CI: 0.59, 0.89);
P = 0.0015
Nivolumab
Docetaxel
1-yr OS rate = 51%
1-yr OS rate = 39%
292 232 194 169 146 123 62 32 09
290 244 194 150 111 88 34 10 05
Nivolumab
Docetaxel
Number of Patients at Risk
OS
(%
)
Time (months)
100
90
80
70
60
50
40
30
10
0
20
27211815129630 24

Nivo
Doc
Nivo
Doc
100
90
80
70
60
50
40
30
10
0
20
Time (months)
100
90
80
70
60
50
40
30
10
0
20
24211815129630 27
Time (months)
24211815129630 27
Symbols represent censored observations.
OS by PD-L1 Expression
mOS (mo)
Nivo 10.4
Doc 10.1
mOS (mo)
Nivo
17.2
Doc
9.0
mOS (mo)
Nivo
9.9
Doc 10.3
mOS (mo)
Nivo
19.4
Doc
8.0
Time (months)
≥5% PD-L1 expression level
<5% PD-L1 expression level
mOS (mo)
Nivo
18.2
Doc
8.1
mOS (mo)
Nivo
9.7
Doc
10.1
≥1% PD-L1 expression level
HR (95% CI) = 0.59 (0.43, 0.82)
Time (months)
<1% PD-L1 expression level
OS
(%
)
HR (95% CI) = 0.90 (0.66, 1.24)
HR (95% CI) = 0.43 (0.30, 0.63)
HR (95% CI) = 1.01 (0.77, 1.34)
OS
(%
)
Time (months)
Time (months)
≥10% PD-L1 expression level
<10% PD-L1 expression level
HR (95% CI) = 0.40 (0.26, 0.59)
HR (95% CI) = 1.00 (0.76, 1.31)
24211815129630 27
100
90
80
70
60
50
40
30
10
0
20
100
90
80
70
60
50
40
30
10
0
20
24211815129630 27
24211815129630 27
100
90
80
70
60
50
40
30
10
0
20
24211815129630 27
100
90
80
70
60
50
40
30
10
0
20

Representative PD-L1 expression in NSCLC samples stained using Dako assay
PD-L1 expression measured:– using a sensitive and specific rabbit anti-human PD-L1 antibody (clone 28-8)– as a percentage of tumoural plasma membrane staining of any intensity (information on
immune cell expression recorded qualitatively)
NegativeControl
Antibody
Positive
% Staining 1% 5% 20% 65%
Antonia et al., WCLC, 2013

Nivolumab more effective in smokers
VariableORR, % (n/N) [95%
CI]P-value
Smoking exposure 0.018
≤5 pack-yrs 0 (0/14) [0, 23]
>5 pack-yrs 30 (20/66) [20, 43]
Time since quitting 0.22
Current smoker 27 (6/22) [11, 50]
1–5 yrs prior 46 (6/13) [19, 75]
6–15 yrs prior 17 (2/12) [2, 48]
>15 yrs prior 18 (6/33) [7, 36]
0
20
80
60
40
Months Since Treatment Initiation
100
PFS
(%
)
PFS by smoking exposure
Never/minimal smokers (mPFS 1.7 months)Former/current smokers (mPFS 2.2 months)HR (95% CI) = 0.41 (0.22, 0.74), P = 0.003
mPFS = median Progression-free survival
Hellmann et al et al. ASCO 2014

Kroemer et al. Oncoimmunology. 2012;1(5): 579–580. .
Matsushita et al. Nature.2012 Feb 8;482(7385):400-4.
Synder et al. NEJM. 2014; 371. Rizvi et al. Science. 2015; 348.
• These mutations lead to
tumor specific
neoepitopes which
serve as neoantigens.
• Those tumors with the
most highly antigenic
proteins are more likely
to lead to a T cell
response.
• Each patients tumor
mutanome is unique
and there appears to be
certain candidate
neoantigens or
neoantigen signatures
that lead to more
durable immune
responses.

Potenziale tossicità auto-immune: nessun organo è risparmiato
From Michot et al. Eur J Cancer 2016
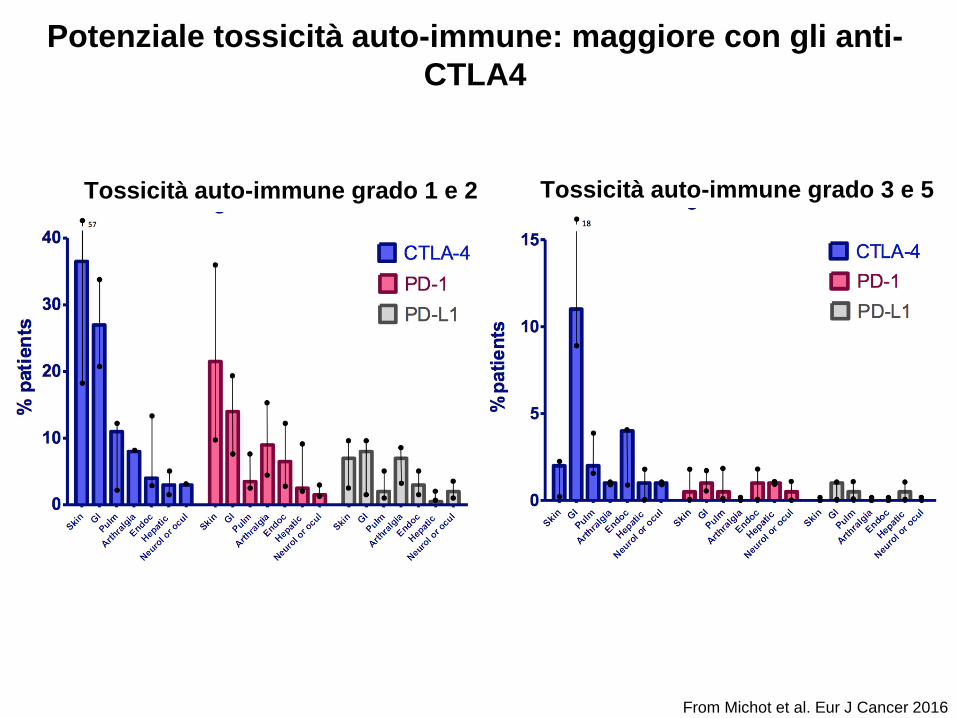
Potenziale tossicità auto-immune: maggiore con gli anti-
CTLA4
Tossicità auto-immune grado 1 e 2 Tossicità auto-immune grado 3 e 5
From Michot et al. Eur J Cancer 2016

Conclusioni
• Vemurafenib ha cambiato la storia naturale dei pazienti con
melanoma avanzato e mutazione di BRAF
• L’immunooncologia rappresenta il presente e il futuro della
terapia oncologica e rappresenta una modalità trasversale
di terapia oncologica