gfr and its clinical importance - renal function
TRANSCRIPT

Urinary system: Renal function
Clinical Importance of GFR
Dr Manish Chandra PrabhakarMGIMS Sewagram

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Renal functions
1- Regulation of plasma ionic composition 2- Regulation of plasma volume 3- Regulation of plasma osmolarity 4- Regulation of plasma hydrogen ion
concentration (pH) 5- Removal of metabolic wastes and
foreign substances 6- Secondary endocrine organ

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Figure 18.1

Kidney anatomy

Nephron

Figure 18.5
The juxta-glomerular apparatus

Figure 18.6
Blood supply to the kidney

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Renal exchange processes
1- Glomerular filtration – in renal capsule 2- Reabsorption – in renal tubules 3- Secretion – in renal tubules

Glomerular filtration
Plasma is filtered through fenestrated epithelium
About 180 liters of plasma are filtered per day filtrate
Filtrate = plasma - proteins
About 2 liters of urine produced per day

Overall fluid movement in the kidneys

Forces acting on filtration
Glomerular capillary hydrostatic pressure due to blood hydrostatic pressure against capillary wall (BHP)
Glomerular osmotic pressure due to the presence of solutes (proteins) in the blood (BOP)
Bowman’s capsule hydrostatic pressure pressure of filtrate against Bowman’s capsule wall (CHP)
Bowman’s capsule osmotic pressure due to the pressure of solutes in the filtrate (COP)
Net filtration rate fluid moves from the glomerulus into the capsule

Glomerular filtration
The glomerular filtration rate (GFR) = volume of plasma filtered per unit of time = 125 ml/min 180 liters per day
Filtration fraction = GFR/renal plasma
flow = 20%

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Reabsorption: Proximal convoluted tubule (PCT)
Glucose, amino-acid, sodium will be pumped out of the tubules, by active transport (ATP needed)
Chloride will follow sodium into the peritubular space (accumulation of positive charges draws chloride out)
Water will move into the peritubular space because of osmosis
Some compounds present in high concentration in the filtrate but low in the blood can move through diffusion
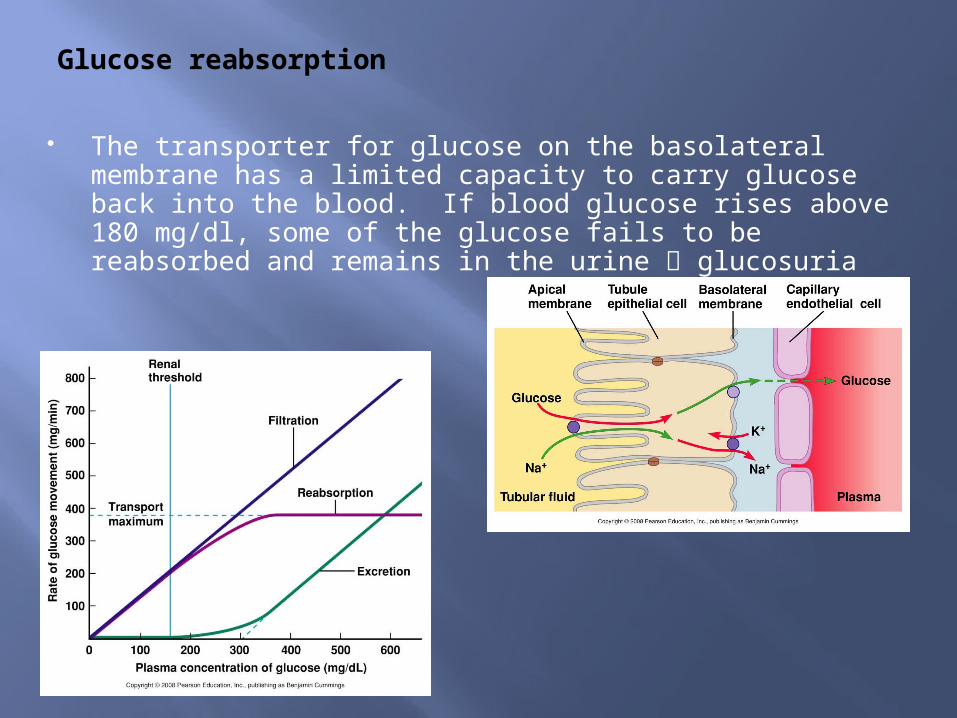
Glucose reabsorption
The transporter for glucose on the basolateral membrane has a limited capacity to carry glucose back into the blood. If blood glucose rises above 180 mg/dl, some of the glucose fails to be reabsorbed and remains in the urine glucosuria

Reabsorption: Proximal convoluted tubule (PCT)
70% of sodium and water are reabsorbed in PCT
Reabsorption is not regulated
Amino-acids, glucose should be 100% reabsorbed at the end of the PCT
The filtrate, at the end of the PCT should be iso-osmolar to the filtrate at the beginning

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Reabsorption: Loop of Henle
Characteristics of Loop of Henle:
-- Descending tubule: permeable to water has no sodium pumps
-- Ascending loop: thick epithelium is impermeable to water but has many sodium pumps
-- Na+, Cl- and K+ are pumped out into the interstitial fluid Cl- follows (electrochemical gradient) water follows by osmosis = counter-current multiplier
-- formation of an osmotic gradient in the renal medulla which is important for water reabsorption in the CT

Figure 19.7 (1 of 6)

Figure 18.4
Reabsorption: Loop of Henle
Additional filtrate is reabsorbed
The filtrate is concentrated as it travels through the loop but returns to a concentration similar to the other end.
Reabsorption in this segment is also (like PCT) not regulated

So, why is the loop of Henle useful?
The longer the loop, the more concentrated the filtrate and the medullary IF become
Importance: the collecting tubule runs through the hyperosmotic medulla more ability to reabsorb H2O
Desert animals have long nephron Loop More H2O is reabsorbed

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Reabsorption: DCT and CT
DCT and CT tubular walls are different from the PCT and Loop of Henle wall:
-- DCT and CT walls have tight junctions and the membrane is impermeable to water
-- the cell membrane has receptors able to bind and respond to various hormones: ADH, ANP and aldosterone
-- The binding of hormones will modify the membrane permeability to water and ions

Reabsorption: DCT and CT
ADH is low no binding to receptors H2O is not reabsorbed back into the bloodH2O remains in the renal tubule high urine volume
ADH is released by post. Pituitary Binds to receptors in CT channels open H2O moves into the IF and blood low urine volume

Regulation of ADH secretion
The neurosecretory neurons for ADH (in the hypothalamus) are located near the center monitoring blood osmotic pressure
if BOP ↑ ADH secretion and release ↑ water reabsorption ↑ blood is diluted BOP↓ (typical homeostatic regulation)
If BOP ↓ ADH secretion and release ↓ H2O reabsorption ↓ BOP ↑ urine volume ↑
Lack of ADH? Symptoms?
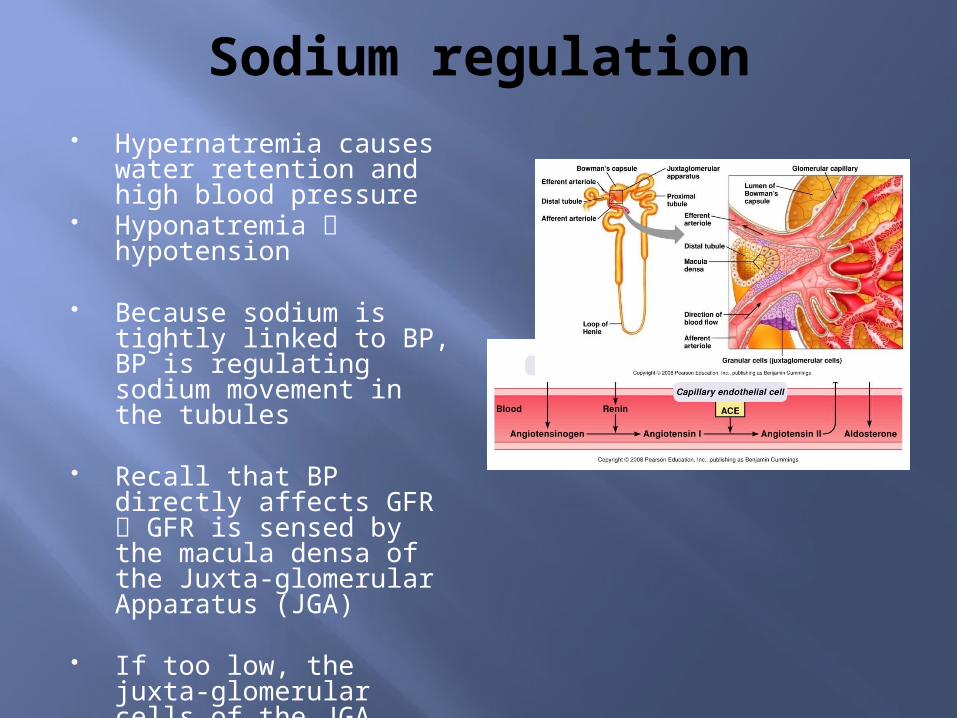
Sodium regulation Hypernatremia causes
water retention and high blood pressure
Hyponatremia hypotension
Because sodium is tightly linked to BP, BP is regulating sodium movement in the tubules
Recall that BP directly affects GFR GFR is sensed by the macula densa of the Juxta-glomerular Apparatus (JGA)
If too low, the juxta-glomerular cells of the JGA secrete renin into the blood

Sodium regulation
As a result, aldosterone will be secreted by the adrenal cortex promotes sodium reabsorption in the DCT and CT.
Another hormone, Atrial Natriuretic Peptide or ANP promotes sodium dumping by the DCT and CT.

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Secretion and excretion
Secretion: Selective transport of molecules from the peritubular fluid to the lumen of the renal tubules
Excretion: Molecules are dumped outside the tubules
Example of excreted waste products: urea, excess K+, H+, Ca++

Clinical applications
Carbonic anhydrase inhibitors:
Osmotic diuretics:
Thiazide diuretics
Loop diuretics:
K+ sparring diuretics:

Diuretics DiureticSite of Action Mechanisms of Action Predictable Side Effects
Osmotic diuretic(e.g., mannitol)
Proximal tubuleThin descending limbDistal tubuleCollecting ducts
- impedes water reabsorption and indirectly impedes Na+ reabsorption by blocking the convective movement of Na+
- volume contraction often with increased serum osmolality
Carbonic anhydrase inhibitors
Proximal tubule - impedes HCO3-, H+, Na+
reabsorption- HCO3
- loss, .: acidosis
Loop diuretics (eg. furosemide)
TAL - blocks Cl-, Na+ and K+ reabsorption (via Na+/K+/2Cl- pump)
- increased K+ losses, because of increased Na+ delivery with increased aldosterone
Thiazides Early distal tubule - blocks Cl- reabsorption, creating intraluminal negative
charge which impedes Na+ reabsorption
- increased K+ losses, because of increased Na+ delivery with increased aldosterone
Aldosterone bockers
Late distal tubuleEarly collecting ducts
- blocks Na+/K+ antiports, impeding Na+ reabsorption and K+ secretion (K+ sparing effect)
- increased plasma [K+]

Clinical application: the Glomerular Filtration Rate
GFR: important value for estimating the kidney function.
Calculated by using molecules which are filtered but not secreted nor reabsorbed.
P X GFR = U X V P = plasma concentration of A, in
mg/mL GFR = glomerular filtration rate of
plasma, in mL/min U = urine concentration of A, in
mg/mL V = rate of urine production in, in
mL/min Solving the equation for GFR will
give: GFR = (U X V)/P
GFR = (U X V)/P

Clinical application: the Glomerular Filtration Rate
Best molecule to use: inulin but not occurring naturally in the body
Second best: creatinine
Urea: cannot be used since it is both secreted and reabsorbed (why is it so?)

Outline
Functions Anatomy Urine formation:
- Filtration- Reabsorption
- Proximal Convoluted Tubule (PCT)- Loop of Henle- Distal Convoluted Tubule (DCT)
- Secretion Regulation of GFR Micturition

Regulation of glomerular filtration rate
GFR needs to be constant (p. 519, Fig. 18.10)
Changes in BHP will affect GFR strongly BHP is a function of SBP
GFR regulation:- to increase GFR:
**vasoconstrict efferent vessel
** vasodilate afferent vessel

Regulation of glomerular filtration rate
Vasoconstriction of the efferent vessel is under the control of:--Epinephrine/Norepinephrine from the ANS-- Angiotensin II from the renin-angiotensin system
Vasodilation of the afferent vessel is under the control of: - paracrines secreted by the
macula densa stimulate vasodilation of neighboring vessel
- myogenic reflex (automatic constriction of smooth muscles lining the wall when the artery is stretched by increased pressure

Outline
Functions Anatomy Renal exchange processes Regional specialization of renal tubules Excretion Regulation of GFR Micturition

Micturition
Controlled by the sacral parasympathetic NS
Stretch sensors in the bladder wall send impulses to the sacral spine
reflex opening of the urethral smooth muscle
Impulses also sent to the cortex to notify the brain of the need to urinate
if the moment is OK, the person will go to the bathroom (hopefully!), and will open the skeletal (voluntary) muscle of the urethral sphincter the person will be able to urinate

Figure 18.21
Micturition: Clinical cases What will happen to
a person who has suffered a spinal cord injury to T10? Which kind of problem(s) will (s)he have?
Why can’t baby control urination? What type of “problem” do they have?
What about older people who dribble urine? What causes that?

Applications: Sea-water raft
Billy is stuck on a raft in the middle of the ocean, without food or water.
In order to get a few extra hours of life and a chance to be found ( a boat), should Billy drink some sea-water or his own urine?
Justify your answer.

Clinical applications: Water intake:
- drink- food- catabolism
Overall, intake should equal output
Urine output should be less than water intake (drinks)
Urine is constantly formed at a minimum rate of about 20-30 ml/h
Water output
- urine- feces- anabolism- respiration

Clinical cases 1- Martha is a patient in a
nursing home. She is 84 year-old, senile and weak. She is bed bound and does not feed herself anymore. She has a urinary catheter and you noticed, at the beginning of your shift that the bag had a small amount of dark yellow urine.
I&O (intake and output): intake 650 cc and output 250 cc.
What do you think?- are the numbers balanced?- if not, what could be wrong?
2- Henrietta is Martha's roommate, also in not very good shape. She has been on IV fluid receiving 100ml/h.
I&O 900ml. Her urine output is 250 ml (she has a catheter).
What do you think? - are the numbers
balanced?- if not, what could be wrong?