gaffi fungal keratitis fact sheet 2021
TRANSCRIPT
1
GAFFIFactSheet
FungalKeratitis
Keratitis is an infectionof thenormally transparent corneaof theeye,which causes
ulcerationandgradualopacification.Itmaybecausedbybacteriaorfungi(orchemical
injury)andisthemaincauseofunilateralcornealscarring1,2.Over100differentfungi
havecausedfungalkeratitisandnewpathogensareregularlydescribed3,howeverthe
common causative agents are Fusarium spp., Aspergillus flavus and fumigatus and
Candida albicans3,4. The condition is most prevalent in tropical and subtropical
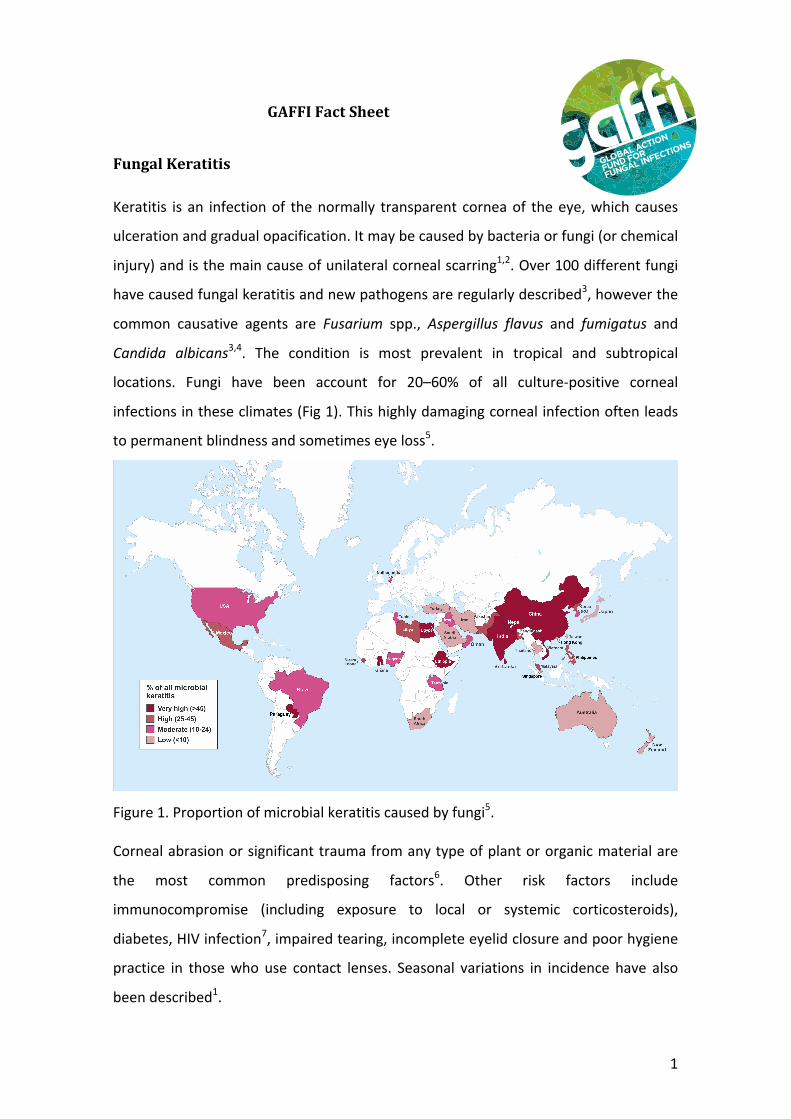
locations. Fungi have been account for 20–60% of all culture-positive corneal
infectionsintheseclimates(Fig1).Thishighlydamagingcornealinfectionoftenleads
topermanentblindnessandsometimeseyeloss5.
Figure1.Proportionofmicrobialkeratitiscausedbyfungi5.Cornealabrasionorsignificanttraumafromanytypeofplantororganicmaterialare
the most common predisposing factors6. Other risk factors include
immunocompromise (including exposure to local or systemic corticosteroids),
diabetes,HIVinfection7,impairedtearing,incompleteeyelidclosureandpoorhygiene
practice in thosewhouse contact lenses. Seasonal variations in incidence have also
beendescribed1.
GLOBAL ACTION
FUND FOR
FUNGAL INFECTIONS
GLOBAL ACTION
FUND FOR
FUNGAL INFECTIONS
OLD VERSION
DARKER AREAS AND TEXT FIT WITHIN CIRCLE
SMALLER VERSION (ALSO TO BE USED AS MAIN
LOGO IN THE FUTURE)
2
Incidence
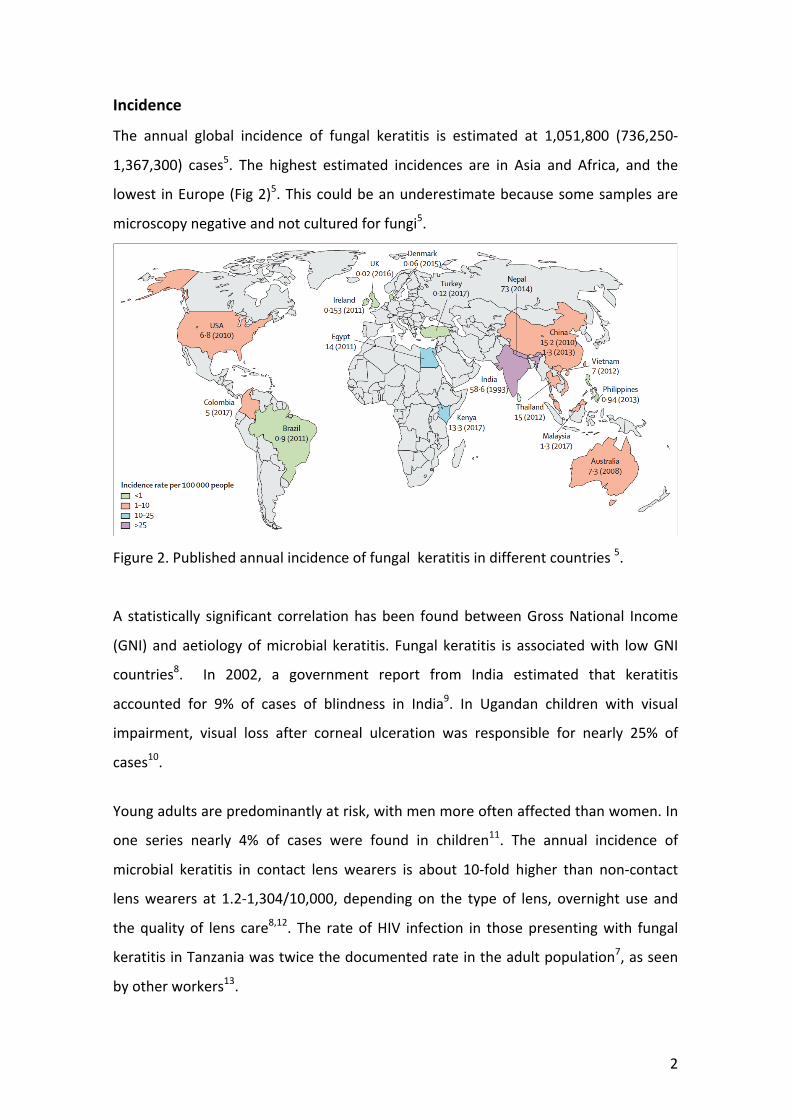
The annual global incidence of fungal keratitis is estimated at 1,051,800 (736,250-
1,367,300) cases5. The highest estimated incidences are in Asia and Africa, and the
lowest inEurope(Fig2)5.Thiscouldbeanunderestimatebecausesomesamplesare
microscopynegativeandnotculturedforfungi5.
Figure2.Publishedannualincidenceoffungalkeratitisindifferentcountries5.
A statistically significant correlationhasbeen foundbetweenGrossNational Income
(GNI) andaetiologyofmicrobial keratitis. Fungal keratitis is associatedwith lowGNI
countries8. In 2002, a government report from India estimated that keratitis
accounted for 9% of cases of blindness in India9. In Ugandan children with visual
impairment, visual loss after corneal ulceration was responsible for nearly 25% of
cases10.
Youngadultsarepredominantlyatrisk,withmenmoreoftenaffectedthanwomen.In
one series nearly 4% of cases were found in children11. The annual incidence of
microbial keratitis in contact lens wearers is about 10-fold higher than non-contact
lenswearers at 1.2-1,304/10,000, depending on the typeof lens, overnight use and
thequalityof lens care8,12. The rateofHIV infection in thosepresentingwith fungal
keratitisinTanzaniawastwicethedocumentedrateintheadultpopulation7,asseen
byotherworkers13.
3
Clinicalpresentation
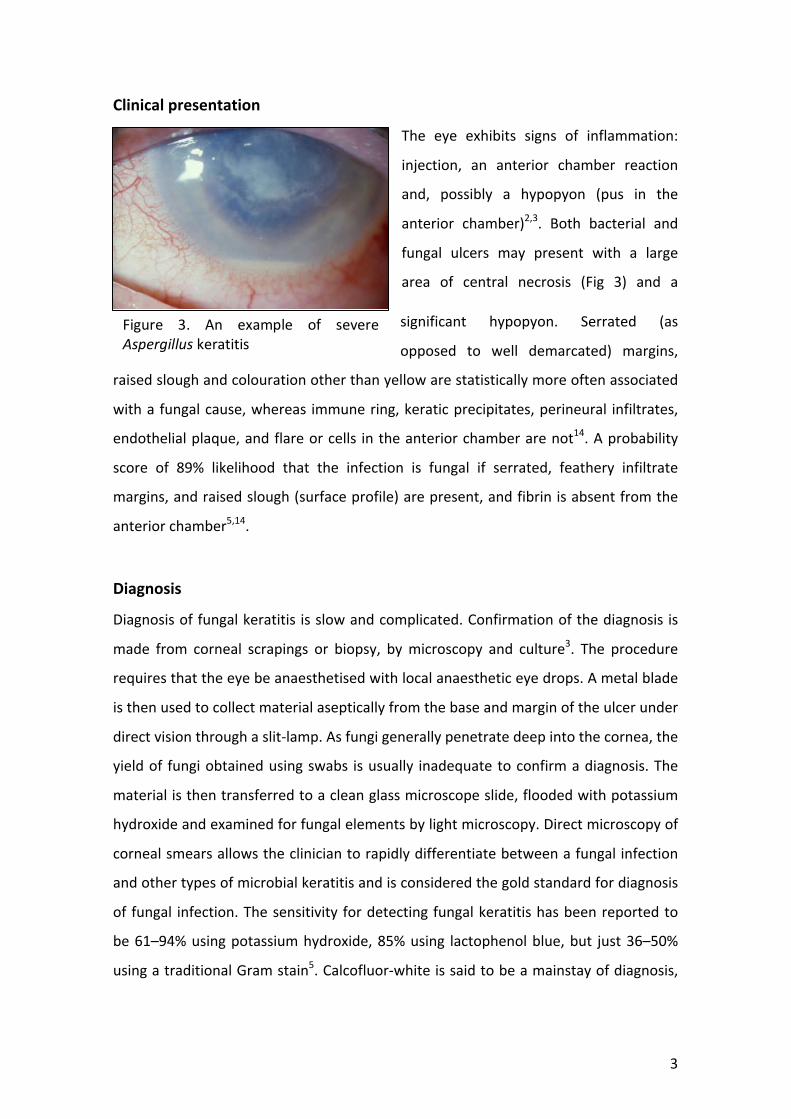
The eye exhibits signs of inflammation:
injection, an anterior chamber reaction
and, possibly a hypopyon (pus in the
anterior chamber)2,3. Both bacterial and
fungal ulcers may present with a large
area of central necrosis (Fig 3) and a
significant hypopyon. Serrated (as
opposed to well demarcated) margins,
raisedsloughandcolourationotherthanyellowarestatisticallymoreoftenassociated
withafungalcause,whereas immunering,keraticprecipitates,perineural infiltrates,
endothelialplaque,andflareorcells intheanteriorchamberarenot14.Aprobability
score of 89% likelihood that the infection is fungal if serrated, feathery infiltrate
margins,andraisedslough(surfaceprofile)arepresent,andfibrinisabsentfromthe
anteriorchamber5,14.
Diagnosis
Diagnosisoffungalkeratitis isslowandcomplicated.Confirmationofthediagnosis is
made from corneal scrapings or biopsy, bymicroscopy and culture3. The procedure
requiresthattheeyebeanaesthetisedwithlocalanaestheticeyedrops.Ametalblade
isthenusedtocollectmaterialasepticallyfromthebaseandmarginoftheulcerunder
directvisionthroughaslit-lamp.Asfungigenerallypenetratedeepintothecornea,the
yieldof fungiobtainedusingswabs isusually inadequatetoconfirmadiagnosis.The
materialisthentransferredtoacleanglassmicroscopeslide,floodedwithpotassium
hydroxideandexaminedforfungalelementsbylightmicroscopy.Directmicroscopyof
cornealsmearsallowsthecliniciantorapidlydifferentiatebetweenafungalinfection
andothertypesofmicrobialkeratitisandisconsideredthegoldstandardfordiagnosis
of fungal infection.Thesensitivity fordetectingfungalkeratitishasbeenreportedto
be61–94%usingpotassiumhydroxide,85%using lactophenolblue,but just36–50%
usingatraditionalGramstain5.Calcofluor-whiteissaidtobeamainstayofdiagnosis,
Figure 3. An example of severeAspergilluskeratitis
4
andwhen combinedwithpotassiumhydroxide stains, sensitivityhasbeen shown to
riseto98·3%5.
Itisnotpossibletodifferentiatebetweengeneraandspeciesoffungionthebasisof
microscopicexaminationofthecornealsmearpreparationalone.Forthisreason,itis
advisedthatbothmicroscopyandculturearedonewheneverpossible.
Samples should be cultured on bacterial and fungalmedia3,5. Blood agar, chocolate
agar,andSabourauddextroseagarare inoculatedwithcornealscrapematerialusing
C-shaped streaks, because of the very small size of the inoculum, and only colony
growth within these parameters are regarded significant. Fungal growth is typically
slow, taking 48 hours to 10 days to become visible. Due to the diversity of fungi
cultured from cases of fungal keratitis, examination of cultures by a specialist
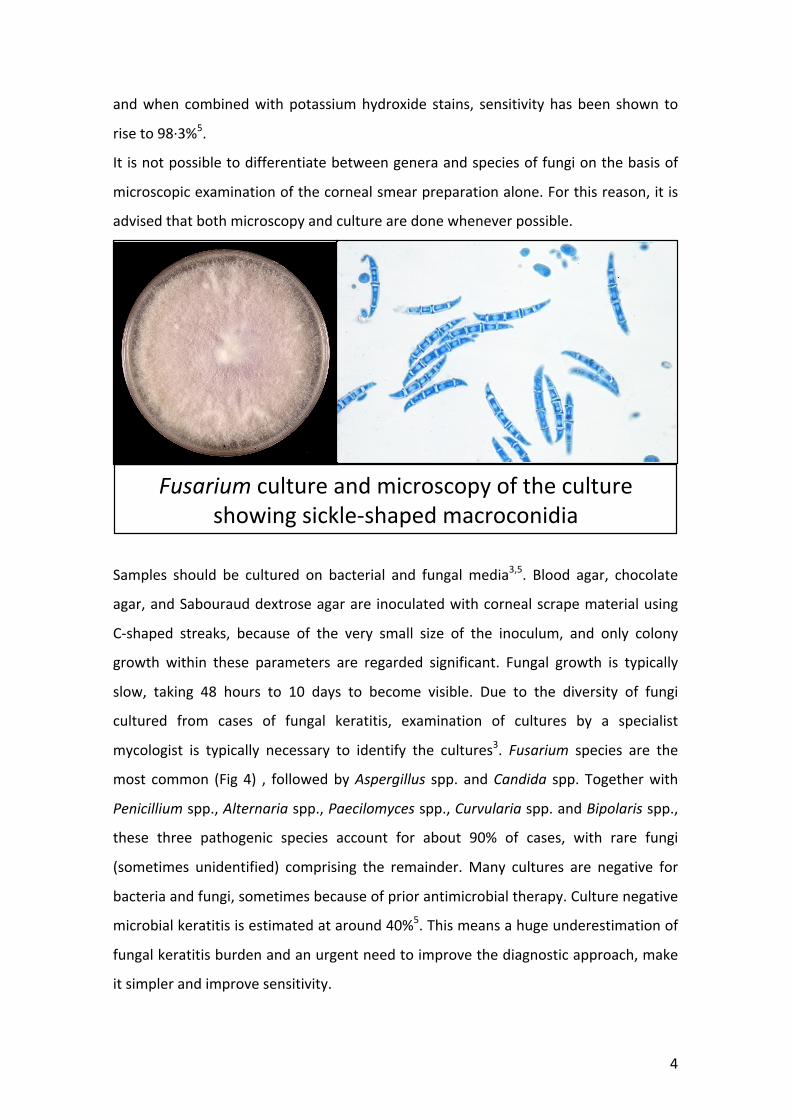
mycologist is typically necessary to identify the cultures3. Fusarium species are the
most common (Fig 4) , followedbyAspergillus spp. andCandida spp. Togetherwith
Penicilliumspp.,Alternariaspp.,Paecilomycesspp.,Curvulariaspp.andBipolarisspp.,
these three pathogenic species account for about 90% of cases, with rare fungi
(sometimes unidentified) comprising the remainder.Many cultures are negative for
bacteriaandfungi,sometimesbecauseofpriorantimicrobialtherapy.Culturenegative
microbialkeratitisisestimatedataround40%5.Thismeansahugeunderestimationof
fungalkeratitisburdenandanurgentneedtoimprovethediagnosticapproach,make
itsimplerandimprovesensitivity.
Fusariumcultureandmicroscopyofthecultureshowingsickle-shapedmacroconidia

5
Otherapproachesthatcanbehelpfulfor
diagnosis are molecular methods and
confocal microscopy but are technically
andcostdemanding15.Themoleculartool
of choice is PCR, which only requires a
small quantity of sample. PCR has been
shown to have high sensitivity and
specificity when compared with smear
stains and culture. PCR positively
identifies the causative fungal species in
92·6%of cases5. However, the technique
iscurrentlyoflimiteduseinlowresource
settings,wheretheburdenofdiseaseisgreatest.
Point of care testing of this disease would dramatically improve patient outcomes.
Slow diagnosis, including referral from one facility to another, worsens visual
outcome16.
Treatment
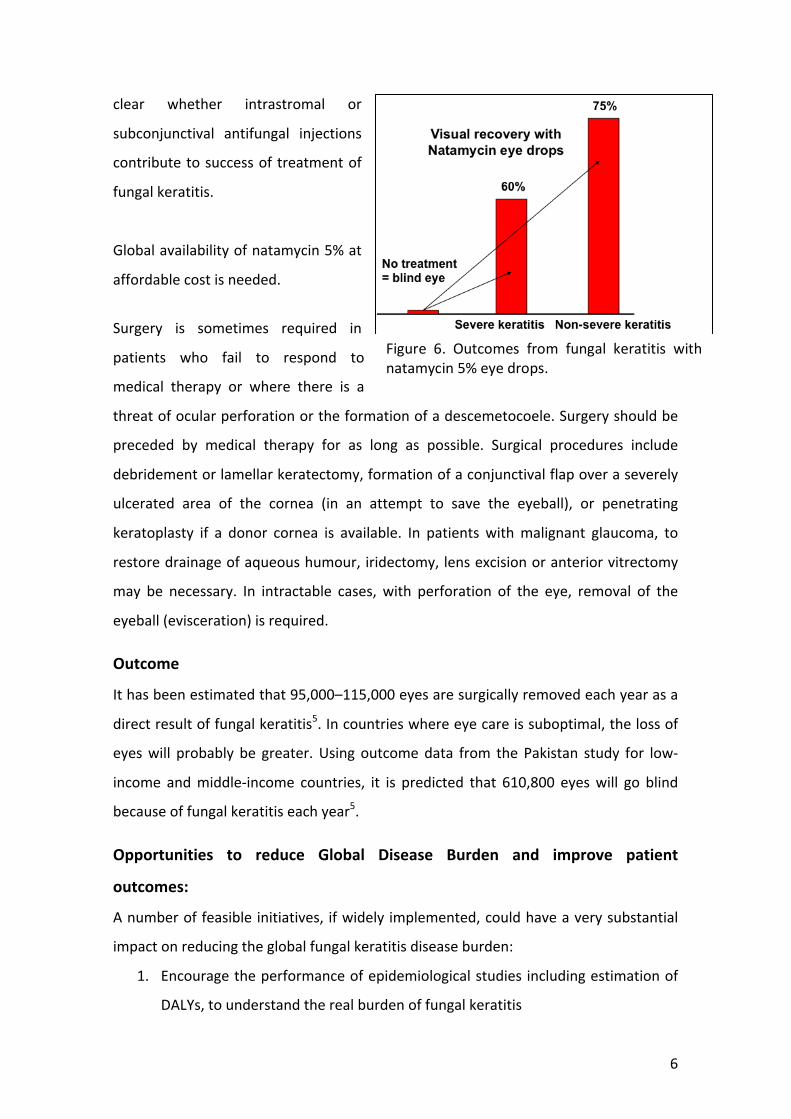
Responses to topical antifungal therapy are reasonable, with 75% of corneas not
severely affected and 60% of those severely affected being cured by topical 5%
natamycin (Primaricin)17,18.Other therapiesproduce similar response rates, although
natamycin is superior to voriconazole18. Advanced disease on presentation is
associatedwithworseoutcomes.
Natamycin 5% eye drops are not registered as treatment inmost countries, and all
suppliersareinIndia.Natamycineyedropsarenowlisted(2017)asaWHOEssential
Medicine.Thefollowingalternativeantifungaleyedropshavebeenusedwithvariable
successrates:amphotericin0.15-0.3%,flucytosine1%,econazole1%,miconazole1%,
clotrimazole1%,itraconazole1%,fluconazole1%andvoriconazole1-2%,caspofungin
0.5%3. Oral itraconazole and voriconazolemay be useful in some patients. It is not
Figure 5. Venn diagram showing howthe diagnosis of fungal keratitis wasmadeinLondon15
6
clear whether intrastromal or
subconjunctival antifungal injections
contributetosuccessoftreatmentof
fungalkeratitis.
Globalavailabilityofnatamycin5%at
affordablecostisneeded.
Surgery is sometimes required in
patients who fail to respond to
medical therapy or where there is a
threatofocularperforationortheformationofadescemetocoele.Surgeryshouldbe
preceded by medical therapy for as long as possible. Surgical procedures include
debridementorlamellarkeratectomy,formationofaconjunctivalflapoveraseverely
ulcerated area of the cornea (in an attempt to save the eyeball), or penetrating
keratoplasty if a donor cornea is available. In patients withmalignant glaucoma, to
restoredrainageofaqueoushumour,iridectomy,lensexcisionoranteriorvitrectomy
may be necessary. In intractable cases, with perforation of the eye, removal of the
eyeball(evisceration)isrequired.
Outcome
Ithasbeenestimatedthat95,000–115,000eyesaresurgicallyremovedeachyearasa
directresultoffungalkeratitis5.Incountrieswhereeyecareissuboptimal,thelossof
eyeswill probably be greater.Using outcomedata from the Pakistan study for low-
income andmiddle-income countries, it is predicted that 610,800 eyeswill go blind
becauseoffungalkeratitiseachyear5.
Opportunities to reduce Global Disease Burden and improve patient
outcomes:
Anumberoffeasibleinitiatives, ifwidelyimplemented,couldhaveaverysubstantial
impactonreducingtheglobalfungalkeratitisdiseaseburden:
1. Encouragetheperformanceofepidemiologicalstudies includingestimationof
DALYs,tounderstandtherealburdenoffungalkeratitis
Figure 6. Outcomes from fungal keratitis withnatamycin5%eyedrops.
7
2. Provide training and availability in classical diagnostic procedures including
sampling,culturetechniquesandfungalspeciesidentification
3. Optimize use of antifungal therapy in resource limited settings through
promotingaglobalapproachtotheprevention,diagnosisandmanagementof
microbialkeratitis
4. Develop a point of care antigen test able to differentiates bacterial infection
fromfungalinfection,
5. Investigatethevalueofintroducingcombinationtreatmentwithantibioticand
antifungaleyedropsversusearlydiagnosisofthecauseandtargetedtherapy,
6. Ensurethatantifungaltreatments,especiallynatamycineyedrops,arereadily
accessibleeverywhere
7. Developprophylacticorpre-emptivetreatmentguidelinesforocularinjuries
8. Delivertraininginappropriatedeliveryoftheeyedrops,dosingandtiming
9. Encourage theperformanceof clinical trials todetermine thebest treatment
forfungalkeratitis.
JuanLuisRodriguezTudela
GAFFI,Geneva
February2021
References
1.Guidelinesforthemanagementofcornealulceratprimary,secondaryandtertiarycarehealthfacilitiesintheSouth-EastAsiaRegion.WHORegionalOfficeforSouth-EastAsia.Ophthal/126.
2.BadieeP.Mycotickeratitis,aStateoftheArtReview.JundishapurJMicrobiol2013;6:e8561.
3. Thomas PA, Kaliamurthy J. Mycotic keratitis: epidemiology, diagnosis andmanagement.ClinMicrobiolInfect.2013;19:210-20.
4. Leck AK, Thomas PA, Hagan M, et al. Aetiology of suppurative corneal ulcers inGhanaand south India, andepidemiologyof fungal keratitis.Br JOphthalmol. 2002;86:1211-5.
5. Brown L, LeckAK,GichangiG, BurtonMJ,DenningDW. The global incidence anddiagnosis of fungal keratitis. Lancet Infect Dis 2020. https://doi.org/10.1016/S1473-3099(20)30448-5
8
6.TilakR,SinghA,MauryaOP,etal.MycotickeratitisinIndia:afive-yearretrospectivestudy.JInfectDevCtries.2010;4:171-4.
7.BurtonMJ,PithuwaJ,OkelloE,etal.MicrobialkeratitisinEastAfrica:whyaretheoutcomessopoor?OphthalmicEpidemiol2011;18:158-63.
8. Stapleton F, Keay L, Edwards K, Naduvilath T, Dart JK, Brian G, Holden BA. Theincidence of contact lens-relatedmicrobial keratitis in Australia. Ophthalmol 2008;115:1655-62.
9.GovernmentofIndia.Nationalsurveyonblindness.1991-2001.Report2002.
10.WaddellK.ChildhoodblindnessandlowvisioninUganda.Eye1998;12:184–192.
11.DeorukhkarS,KatiyarR,SainiS.Epidemiologicalfeaturesandlaboratoryresultsofbacterial and fungal keratitis: a five-year study at a rural tertiary-care hospital inwesternMaharashtra,India.SingaporeMedJ2012;53:264-7.
12.JengBH,GritzDC,KumarAB,etal.EpidemiologyofulcerativekeratitisinNorthernCalifornia.ArchOphthalmol2010;128:1022-8.
13.Mselle J. Fungal keratitis as an indicator of HIV infection in Africa. Trop Doctor1999;29:133–35.
14. Thomas PA, Leck AK,MyattM. Characteristic clinical features as an aid to thediagnosisofsuppurativekeratitiscausedbyfilamentousfungi.BrJOphthalmol2005;89:1554-8.
15.OngHS,FungSS,MacleodD,DartJK,TuftSJ,BurtonMJ.Alteredpatternsoffungalkeratitis at a London ophthalmic referral hospital: an eight-year retrospectiveobservationalstudy.AmJOphthalmol2016;168:227–36.
16. Arunga S, Kintoki GM, Gichuhi S, et al. Delay along the care seeking journey ofpatientswithmicrobialkeratitisinUganda.OphthalmicEpidemiol2019;26:311–20.
17.KalavathyCM,ParmarP,Kaliamurthy J,etal.Comparisonof topical itraconazole1%withtopicalnatamycin5%forthetreatmentoffilamentousfungalkeratitis.Cornea2005;24:449-52.
18.PrajnaNV,KrishnanT,MascarenhasJ,etal.TheMycoticUlcerTreatmentTrial:Arandomized trial comparing natamycin vs voriconazole. Arch Ophthalmol 2012 Dec10:1-8.