fungal infections of the eye
DESCRIPTION
Fungal infections of the eyeTRANSCRIPT

I See Trees of Green

Red Roses Too

I See Them Bloom For Me & For You

And I Think To Myself , Such A Wonderful World

I See Skies Of Blue
And Clouds Of White

The Bright Sunny Days

The Dark Sacred Nights

And I Think To Myself
What A Wonderful World

Prevent trauma
Tears :Lysozyme, Lactoferrin, ceruloplasmin,B lysin, Complement & Ig`s
Conjunctival follicles & leukocyte defense

ANATOMY

ANATOMY
Rich vascular supply

FUNGAL INFECTIONS OF THE EYE
Presenter: Dr. Vinaykumar Hallur
Moderator: Dr. M.R. Shivaprakash

Periocular Fungal Infections
Mycoses of the Anterior Segment of the Eye
Fungal Endophthalmitis
Laboratory diagnosis
Management
Experimental models

KERATOMYCOSIS
First described by Leber (Aspergillus species) in 1879 Major cause of blindness in Asia Incidence low in Britain & North USA 6-53% of all cases of ulcerative keratitis in Asia Can occur alone or coexist with a bacterial
infection(14.1%) [Basak et al Indian J Ophthalmol. 2005 Jun;53(2):143]
Earlier phaeoid fungi (Dematiaceous) not considered to be significant but now are important cause of keratomycosis .
Rare

EPIDEMIOLOGY
PREVALENCE
North India 82.3%South India 46.1%Eastern India 32.0%Western India 38.9%
Total prevalence of fungal keratitis in India is 30.00% of total cases
Total prevalence of fungal keratitis in western 8.00% countries IJO Sep 2001
South India : 34.4% fungal keratitis, Fusarium 2007 Bharathi et al, Fusarium 43%, Aspergillus 26%, Dematitious Fungi 25% 2003 – Bharathi et al
North India : Aspergillus40% ,Fusarium 16%, Curvularia 8%, 1994- Chander et al.,Aspergillus 35 %, Fusarium 23%, Acremonium 12%, 1993-Chander et al.

AGE 21 -50 YEARS
SEX M > F (3:1)
RESIDENCE RURAL >URBAN
SOCIOECONOMIC STATUS LOW > HIGH
OCCUPATION FARMERS, LABOURER.
SEASONS AUTUMN, RAINY.
Cornea 2000; August:555-59

PREDISPOSING FACTORS• Trauma vegetable matter metallic foreign body sand/stone• Chronic topical medication• Diabetes Mellitus• Topical or systemic corticosteroids• Extended wear/bandage contact lens• Penetrating keratoplasty• Anterior uveitis • Herpes simplex keratitis

ETIOPATHOGENESIS Over 70 genera can cause mycotic keratitis Fungi of importance in microbial keratitis Moniliaceae -- Aspergillus (90%) Most common cause in World -- Fusarium(1%)Second most common cause --Paecilomyces. --Penicillium. --Pseudallescheria.
Data in brackets from Dept of ophtahlmology, PGIMER

CONTD..
• Dematiaceae. --Curvalaria. (2%) --Alternaria. --Phialophora. --Bipolaris. --Exserohilum. --Cladosporium.-- Colletotrichum • Yeast. --Candida. (2.5%) --Cryptococcus
• Dimorphic fungi. --Blastomyces. --Coccidioides. --Histoplasma. --Sporothrix.


• PATHOGENESIS
-Breach in epithelium-Compromised cornea -Immunocompromised
Contact of fungal hyphae with cornea
Filamentous Yeast

FUNGAL ADHERENCE
Filamentous Fibrinogen receptors on
mature conidia of aspergillus and fusarium
Yeast Integrin analogue, Fibronectin
receptor, Adhesive mannoprotn, Aspartyl
proteinase, Factor 6 , Endo. adhesions.

PENETRATION
Filamentous fungi: Parallel growth of hyphae to stroma, f/b release of mycotoxins, proteolytic enzymes, soluble fungal antigen
Yeast: Proliferate parallel & perpendicular to corneal stroma f/b release of protease and lipase

HOST RESPONSE FILAMENTOUS
inablity of PMN,leucocyte cell for phagocytosis
destruction of corneal stroma
penetrate descement membrane
enterAC accumulate around lens
seclusion of pupil fungal glaucoma

inability of PMN cell to ingest pseudohyphae and hyphae
furstated phagocytosis by PMN
destruction of stroma
melting of cornea
HOST RESPONSE YEAST

CLINICAL FEATURES
• Signs >> symptoms• Manifest within 24 – 48 hours• Patient present within 1st week• EARLY BI-MICROSCOPIC FINDING• Fine or coarse granular infiltrate within the
epithelium and anterior stroma • Minimal stromal infiltrate • Epithelial surface is dry rough textured, dirty gray
in color

CONT………
• Epithelium may be intact or ulcerated.• Pigmented and delicate ,feathery branching
hyphae with surrounding infiltrate• Multifocal suppurative microabsscess or satellite
lesion

CONTD….
• Advanced lesions
o Dense fibrinous material adhering to endothelium and
iris
o Total stromal infiltrate and necrosis

CONTD…………..
• Other signs• White ring (Wessely`s ring)• Conjunctival hyperemia• AC reaction• Hypopyon • endothelial plaque• Mild iritis

YEAST KERATITIS
• Risk Fatcors• Previously compromised cornea• SYSTEMIC DISEASE
Sjogren’s syndrome Erythema multiforme IgA deficiency HIV Endocrinopathy

CLINICAL FEATURE OF CANDIDA INFECTION
• Ulcer is small oval with expanding discrete
sharply demarcated ,dense yellow –white stromal
suppuration
• Feathery margins are not seen

FUNGAL ENDOPHTHALMITIS
a suppurative inflammation of inner ocular
coats and their adjacent structure
with involvement of anterior chamber and
vitreous fluid,
caused by various fungal agents

FUNGAL ENDOPHTHALMITIS
Clinically two types
Endogenous due to hematogenous
spread
Exogenous due to trauma or post
operative

EPIDEMIOLOGY
The first description of endogenous fungal endophthalmitis was by Dimmer in 1913
Candida endopthalmitis clinical entity in 1958
In U.S.A. compared to previous decades Endophthalmitis Increase from last few decades.
Incidence is increasing because of modern medical practices
USA 30 % candidemia(Last 3 decdes) develop endopthalmitis, now there is a lower incidence because of prophylacyic antifungals
CMR, October 2000, p. 662–685

PATHOGENESIS ENDOGENOUS
Multifactorial.
It is likely that sustained fungemia with even
saprophytic fungi can lead to endopthalmitis
Gupte et al -contaminant IV fluids,11 / 72 IV fluid samples
culture positive for fungi
At the time of initial infection with some
dimorphic, fungi, such as H. capsulatum & C.
immitis, unrecognized fungemia occurs and
often leads to endophthalmitis.

ENDOGENOUS ENDOPHTHALMITIS
Predisposing factors Systemic debilitating disease
Malignancy
IVDU
Chemotherapy
Systemic antibiotics
Alcoholism &
Diabetes

PATHOGENESIS ENDOGENOUS
More common in immunocompromised ie pts
on chemo or IV drug abuse
Marked trophism for eye because peculiar
blood supply of the eye.

PATHOGENESIS: EXOGENOUS
Occurs in immunocompetent people
Direct introduction of the organisms following
Surgery(Catarct removal with placement of IOL mainly
Candida spp)
Trauma(Mainly Fusarium spp. )
I/O spread from Fungal keratitis

EPIDEMIOLOGY
RACE – no racial preponderance
SEX – Male preponderance (3:1)
AGE – Young and middle age.

MORBIDITY
Prognosis depends upon virulence of organism extent of involvement timingmode of intervention
Prompt therapy following early diagnosis helps to reduce visual loss
Visual outcome of aspergillus endo. is poor d/t macular involvement.

AGENTSEndogenous Endotphthalmitis
Candia albicans
Fusarium species
Aspergillus species
Histoplasma capsulatum
Coccidioides immitis
Blastomyces dermatitidis
Cryptococcus neoformnas

C. ALBICANS
M.C.C of endogenous endopthalmitis
Infection usually starts from Choroid and then
spreads to retina
Non candida albicans fungemia & endopthalmitis is
increasing and is concern because of antimicrobial
resistance

CANDIDIAL ENDOPTHALMITIS
Current Eye Research, 1–11, Early Online, 2010

ASPERGILLUS ENDOPTHALMITIS
A. flavus second MCC
Spreads from lungs to eye
This is f/b A. fumigatus, A. niger, A. terreus,
A. glaucus , & A. nidulans .

CRYPTOCOCCAL ENDOPH.
Cryptococci spores survive in pigeons
dropping
From lung, fungus – disseminated
haematogenesouly and can affect CNS
causing fungal meningitis &
endophthalmitis in eye
Choroids is the probably first site of ocular
infections
AGENTS
Exogenous Endophthalmitis
Aspergillus spp. C. albicans,C. glabrata, C. tropicalis, C.
parapsilosis Paecilomyces spp. Fusarium spp. Acremonium spp. Curvularia spp.

PRESUMED OCULAR HISTOPLASMOSIS Occurs in immunocompetent individuals
Recognized by presence of multiple atrophic chorioretinal
scars w/o vitreous or aqueous humor inflmn.
Affect 2,000 new individuals a year in areas of endemicity
and in some cases may lead to visual loss and blindness
Arises from hematogenous spread
Not detectable in the scars of POH
Strong epidemiological evidence, principally deriving from
skin test surveys, linking the scars to histoplasmosis

CLINICAL FEATURES
Symptoms
Visual loss Pt. may be asymptomatic if the lesion is in
the peripheral retina Red eye. Photophobia. Pain. Floaters. Scotoma

Many have a classical appearance with
progressive granulomatous uveitis diffuse retinitis deep vitreous abscess.
Time to make diag. from onset of symptoms, 3 d to 4 months.

DEPARTMENTAL DATA


PERIOCULAR INFECTIONS
Palpebral involvement
As a part of generalized or local disease
First reported case 1922 case of sporotrichosis
Tinea faciale
Aspergilloma, sporotrichosis Chalazion
Blastomycosis, Coccidioidomycosis Basal cell
carcinoma
Agent No of cases in literature
Aspergillosis 2
Blastomycosis 12
C. albicans 3
Coccidioidomycosis 6
Cryptococcus spp. 3
Dermatophyte 11
Paracoccidioidomycosis 5
Rhinosporidiosis 7
Sporothrix spp. 5

INFECTIONS OF THE LACRIMAL GLAND
Fungi found to account for only 5% of infections .
14% of cases of congenital dacryocystitis
Principally Aspergillus spp. and C. albicans
implicated
Epiphora is only clinical finding
Lid edema, conjunctival injection, and swelling in the
medial canthus; pressure over the area usually
results in a purulent discharge through the lower
punctumThomas, CMR, Oct 2003,
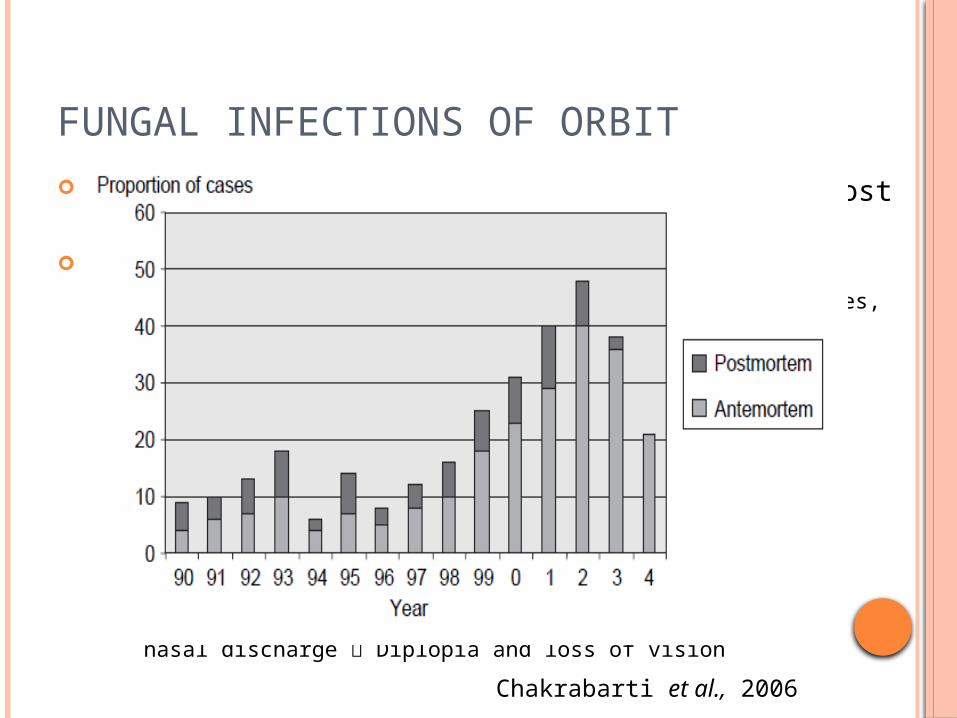
FUNGAL INFECTIONS OF ORBIT
Proximity of sinuses to orbit, susceptible host & pathogen
Zygomycosis Rhinoorbitocerebral : one-third to one-half of all cases,
Incidence increasing Major risk factor : uncontrolled diabetes mellitus(70% DKA) Other predisposing factors
Chronic alcoholism Renal transplantation Hematological malignancies Steroid therapy Breach of skin
Starts with symptoms consistent with sinusitis Bloody nasal discharge Diplopia and loss of vision
Chakrabarti et al., 2006

INFECTIONS OF ORBIT Invasive aspergillosis
Increased frequency infection :widespread prophylaxis with fluconazole
[VanBurikJH et al. The effect of prophylactic fluconazole on the clinical Spectrum of fungal diseases in bone marrow transplant recipients with special attention to hepatic
candidiasis.Medicine(Baltimore) 1998;77:246−54.]
Exact prevalence of invasive aspergillosis in India is not known [Chakrabarti et al , Japanese Journal of Medical Microbiology vol 49, 165-72, 2008]

INVASIVE ASPERGILLOSIS
Other fungi mimicking aspergillosis Bipolaris spp. Alternaria spp. Curvularia spp. C. immitis B. dermatitidis Histoplasma spp. Penicillium spp.
C/F orbital inflammation & a red proptotic eye with or
without associated pain ophthalmoplegia may develop Embolization of vessels of the optic nerve, or
direct involvement of the nerve may occur

FUNGAL CONJUNCTIVITIS Can occur indepently or with keratomycosis Clinically rare entity Fungi may be present without causing inflammation
in~ 25% pts Topical application tetracycline X 4 wks increased
prevalence 28.7%[Nema, H.V., O.P. Ahuja, A. Bal and L.N. Mohapatra, Effects of topical corticosteroids
and antibiotics on mycotic flora of conjunctiva. Am. J. Ophthal., 1968. 65: p. 747–750].
Topical applications of corticosteroids X 3 wks increase prevalence of fungi 18.8-67%
[Mitsui, Y. and J. Hanabusa, Corneal infections after cortisone therapy. Br. J.Ophthal., 1955. 39: p. 244–250.]
C. albicans follows steroid LA Pseudomembrane Other organisms Aspergillus, Blastomycosis,
Sporothrix, Coccidiodomycosis

EXPERIMENTAL MODELS FK
Albino, wild rabbit , Dutch belted rabbit
Previously immunocompromised corticosteroids locally or systemically
Fractionated cobalt whole-body radiation
administration of antilymphocyte serum
alloxan-induced diabetes
Intra lamellar injection or Superficial
inoculation of spore suspension

CONTD..
IL inoculation : C. albicans, C. krusei, C. tropicalis, C. pseudotropicalis,
Aspergillus spp., Cephalosporium spp., F. solani, Lasiodiplodia
sp.
Superficial inoculation: C. albicans, C. tropicalis, C. pseudotropicalis, Aspergillus spp.,
Allescheria boydii, Cephalosporium spp., Geotrichum sp.
Antibacterial prophylaxis & use of characterized
strain ensures reproducibilty.
IO penetration of ketokonazole in rabbit has been
tried as a therapeutic modaliities

OTHERS
Mice BALB/c mice ip cyclophosphamide 180 mg/kg 1,3, & 5d Scarified corneas /keratoplasty rat cornea in b/w space topically inoculated Easy handling
Rat Wistar rats or Lewis rats Suitable size & immune response Size of eyes better surgical manipulation
Pigs Large size, ease of fitting contact lens
Owl monkeys Not better than Rabbit keratomycosis model
ENDOPHTHALMITIS MODELS
Rabbits Both immunocompetent and immunocompromised rabbits
are used Used mainly for endogenous endophthalmitis 0.5 ml of 2 X 107 org/ ml into auricular vein intravitreal inoculation of 1,000 CFU of susceptible C.
albicans
Junko et al Jpn. J. infect. Dis., 60, 33-39, 2007 Mice
Fusarium solani in immunocompetent mice Inocula of 5 x 10(6) conidia injected into the lateral tail veinMayayo et al Med Mycol. 1998 Oct;36(5):249-53


DIAGNOSIS
History
Physical examination
Detailed examination of the affected
High risk of suspicion

LABORATORY DIAGNOSIS
Sample collection and transport Biopsy Corneal scraping, corneal button AC tap Vitreous tap Fluids Lens
Swabs not encouraged
Sterile leak proof container ASAP
Delay 4°C with exception of blood and vitreous (30-
37°C ) & swab (15%)

SAMPLES Detailed examination of affected eye using
slit lamp
Tissues diagnostic material harvested by experienced ophthalmologist after LA or SA
Biopsy Scraping :15 Bard – parker surgical blade from the
base & margin(thoroughly) of ulcer aseptically or Kimura’s platinum spatula
Impression smear(Jain et al 2006 – PGIMER, Chandigarh – equally sensitive and specific as Scrappings)
Vitreous tap 300 microL using 23 G needle Aqeous tap 200 microL using 23 G needle

CONVENTIONAL TECHNIQUES
Direct microscopy Rapid and cost effective 10% KOH preparation Gram & Geimsa stain Calcoflour Stain – Easy and fast H&E, GMS, PAS, cytologic preparation
Culture SDA, Blood agar, CHROM agar
Susceptibility testing According to CLSI guidelines

CONVENTIONAL
Nonspecific fluorescent stain – {calcoflour white, blankophor, uvitex 2B} – used in tissue sections and cytopathologic preparation of rapid diagnosis of mycotic
infections. Chander et al. Sensitivity of Calcofluor white – 95.2% compared
to 71.4 % for KOH and culture. fluorescent microscope wavelength of 365 nm.
Acridine orange staining – useful in early diagnosis of keratomycosis
PAS (Periodic acid schiff) stain can also use.

CULTURE
Corneal scraping inoculated on agar plate as a ‘C’ or ‘S’ shaped streak incubated at 25 & 37°C X 4wks
Fungal growth in the form of the streak ensure that the growth is from the inoculum / specimen rather than a laboratory contaminant.
Two sets of SDA with antibiotic, inoculated and incubated at 250 C & 370C separately x 4 wks.
Keeping a possibility of dimorphic fungi

CULTURE
Vitreous fluid inoculated on routine fungal
culture media .
Vitreous sample should be concentrate either
by
centrifugation
Millipore filtration

CULTURE
All the culture checked everyday during first week and twice a week during next 3 week weeks.
Positive culture are more convincing when growth is obtained on more than one
occasion.

CONVENTIONAL TECHNIQUES
Serological techniques
Diagnosis of Histoplasmosis, Blastomycosis
MOLECULAR TECHNIQUES
PCR based detection methods
PCR
Rapid molecular identification of fungal pathogens in corneal samples from
suspected keratomycosis cases. J Med Microbiol. 2006 Nov;55(Pt 11):1505-9.
PCR - SSCP
Sensitive and rapid polymerase chain reaction based diagnosis of mycotic
keratitis through single stranded conformation polymorphism. Am J
Ophthalmol. 2005 Nov;140(5):851-857.
Nested PCR
Comparative study of Gram stain, potassium hydroxide smear, culture and nested PCR in
the diagnosis of fungal keratitis. Ophthalmic Res. 2010;44(4):251-6.

MOLECULAR TECHNIQUES
PCR-RFLP
Diagnosis of Aspergillus fumigatus endophthalmitis from
formalin fixed paraffin-embedded tissue by polymerase chain
reaction-based restriction fragment length polymorphism Indian
J Ophthalmol. 2008 Jan-Feb;56(1):65-6.
Real time quantitative PCR
Detection and quantification of pathogenic bacteria and
fungi using real-time polymerase chain reaction by cycling
probe in patients with corneal ulcer. Arch
Ophthalmol. 2010 May;128(5):535-40.

PRINCIPLES OF TREATMENT
As with any other fungal infection , look & treat
for any predisposing illness
Confirm lab diagnosis
Look for and treat any superadded infection
Remember Poor penetration of antifungal drugs
Corticosteroids are contraindicated
Use both surgical and medical approach whenever needed
Close follow up is required

FUNGAL KERATITIS
Superficial (early keratitis): Topical natamycin (5%) (hyphae) Topical 0.15% amphotericin B or topical fluconazole (yeasts) Debridment of the epithelium
Deeper and larger lesions: Subconjunctival or intravenous miconazole Ketoconazole, itraconazole, fluconazole or voriconazole (p.o.) Intracameral amphotericin B
Surgical treatment: Cyanoacrylate tissue adhesive Amniotic membrane transplantation Penetrating keratoplasty
ENDOGENOUS ENDOPHTHALMITIS
Systemic antifungal agents: Fluconazole,
voriconazole (azole compounds)
Systemic antifungal agents: Amphotericin B:
Parenteral ± intravitreal
Pars plana vitrectomy
EXOGENOUS ENDOPHTHALMITIS
Intraocular (intracameral ± intravitreal) amphotericin
B
Intravitreal voriconazole or miconazole
Subconjunctival antifungal agents: when associated
with keratitis
Systemic antifungal agents: fluconazole,
ketoconazole, voriconazole, itraconazole, miconazole,
and amphotericin B: important in
immunocompromised patients
Pars plana vitrectomy

MUCORMYCOSIS
Radical surgery+ antifungal therapy +
correcting underlying conditions
Amphotericin B Ist DOC(Amphotericin B given
IV at a daily dose of 1.0-1.5 mg/kg infused
during 2-4 hr for a total of 1-4 g)
Lipid formulations of amphotericin B
alternativeFerri: Practical Guide to the Care of the Medical Patient, 8th ed

INVASIVE ASPERGILLOSIS
Voriconazole 6 mg/kg IV q12h for 2 doses,
then 4 mg/kg q12h PO Rx for adults is
200 mg bid or 4 mg/kg bid.
Caspofungin in pts who fail to respond to or
are unable to tolerate other antifungal drugs.
The recommended dosage is 70 mg on the
first day and 50 mg qd thereafter given as a
single dose IV over 1 hr.Ferri: Practical Guide to the Care of the Medical Patient, 8th ed

Even though we cannot live forever, let our eyes live and give sight for the needy! I have pledged my eyes, you can do that too..