skin fungal infections
TRANSCRIPT
DEFINITION:
Fungal skin infections are commonly affect the outer layer of the skin, nails and hair. Most of the fungi causing infections are usually dermatophytes (tinea), yeast (candida) and molds. The sign and symptoms depends on the type of the organisms that cause the infections. Most of the time, fungal skin infections may appear red, scaly and itchy. The rashes present have a well-defined border and sometimes it appear like a dry skin.
Type:
1. Tinea Corporis/Ringworm Fungal infections that occur at skin, buttocks, other than groin, scalp,
soles and palm area. Causative organism: dermatophytes
2. Tinea Pedis Most commonly known: athlete’s foot, kulat air Occur at the area between toes and around the foot below ankle level Causative organism: dermatophytes
3. Tinea Cruris Most commonly known: jock’s itch Occur at the area around the groin and adjacent skin to the groin Causative organism: dermatophytes
4. Tinea Versicolor In Malay: panau Skin appear to have a different colour of patches and spots, usually paler
than usual skin colour Causative organism: yeast
CAUSES
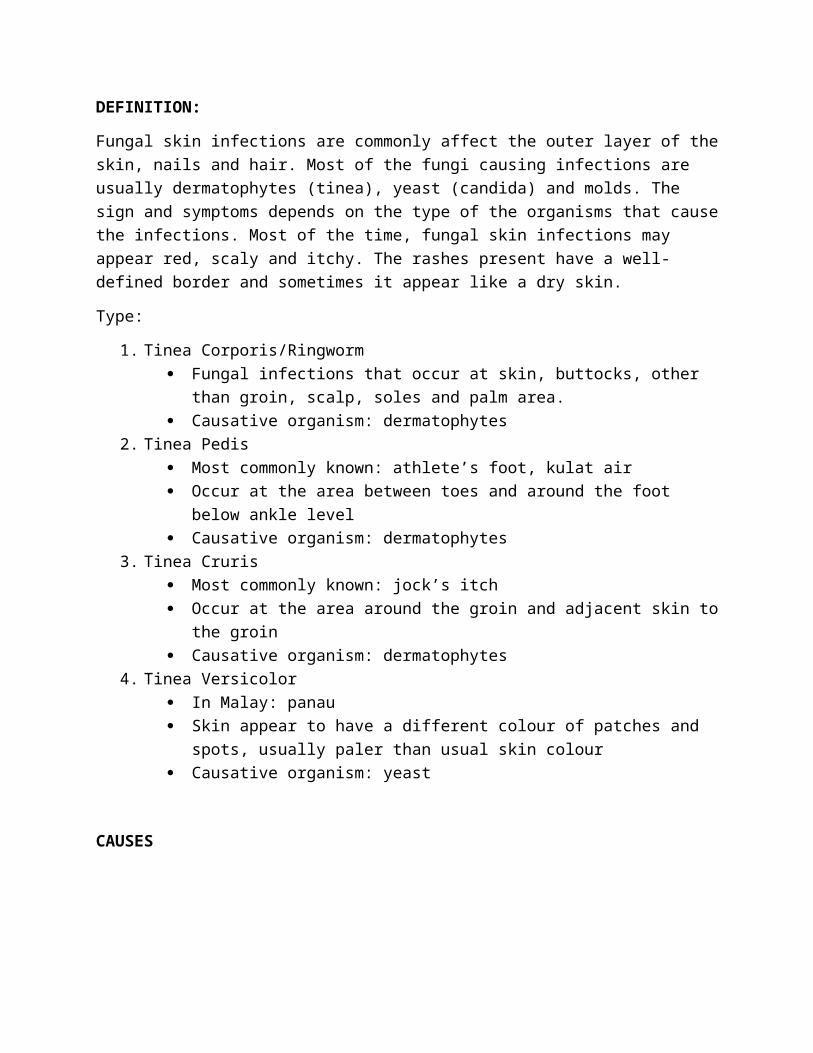
TINEA CORPORIS (ringworm)
Tinea corporis is a skin infection caused by a fungi.
Tinea corporis is caused by mold-like fungi called dermatophytes.
Fungi are germs that can live on the dead tissue of the hair, nails, and outer skin layers. Tinea corporis is caused by mold-like fungi called dermatophytes.
Tinea corporis is common in children, but can occur in people of all ages.
Fungi thrive in warm, moist areas. A tinea infection is more likely if you:
Have wet skin for a long time (such as from sweating)
Have minor skin and nail injuries
Do not bathe or wash your hair often
Have close contact with other people (such as in sports like wrestling)
Tinea corporis can spread easily. You can catch it if you come into direct contact with an area of ringworm on someone's body. You can also get it by touching items that have the fungi on them, such as:
Clothing
Combs
Pool surfaces
Shower floors and walls
Ringworm can also be spread by pets. (Cats are common carriers.)
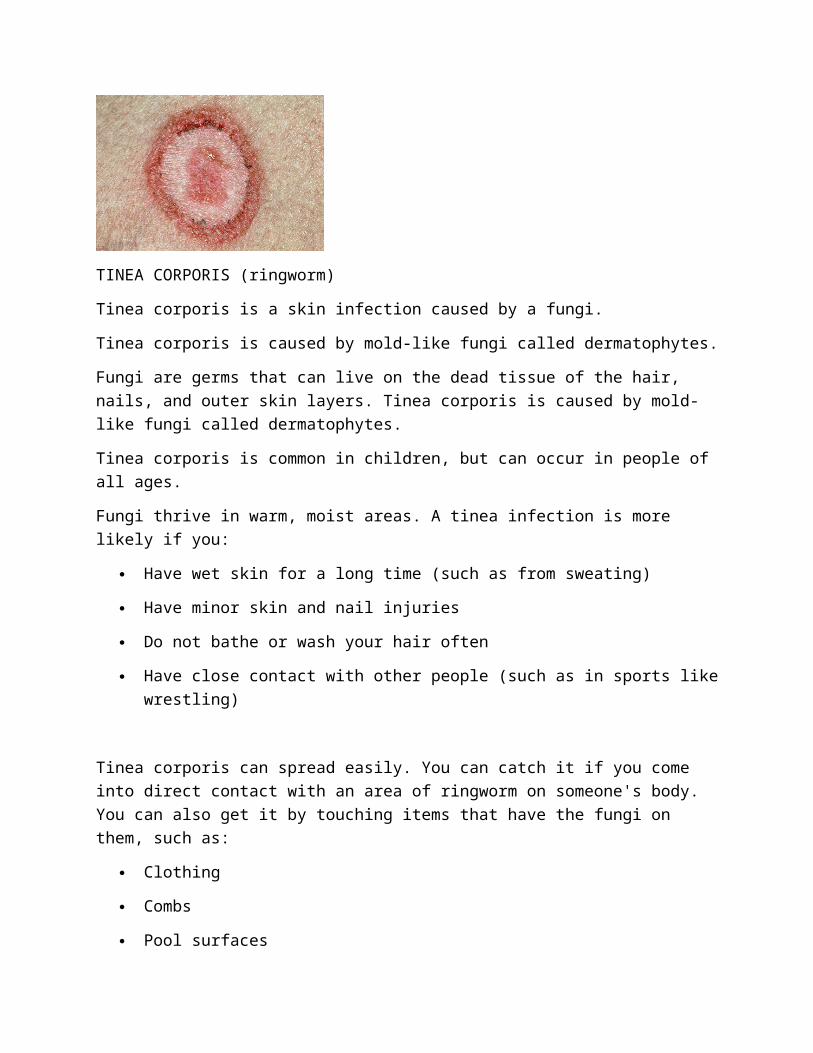
TINEA PEDIS (athlete’s foot)
Tinea pedis is a foot infection due to a dermatophyte fungus. Tinea pedis thrives in warm humid conditions and is most common in young adult men.
Tinea pedis is most frequently due to:
Trichophyton (T.) rubrum
T. interdigitale, previously called T. mentagrophytes var. interdigitale
Epidermophyton floccosum
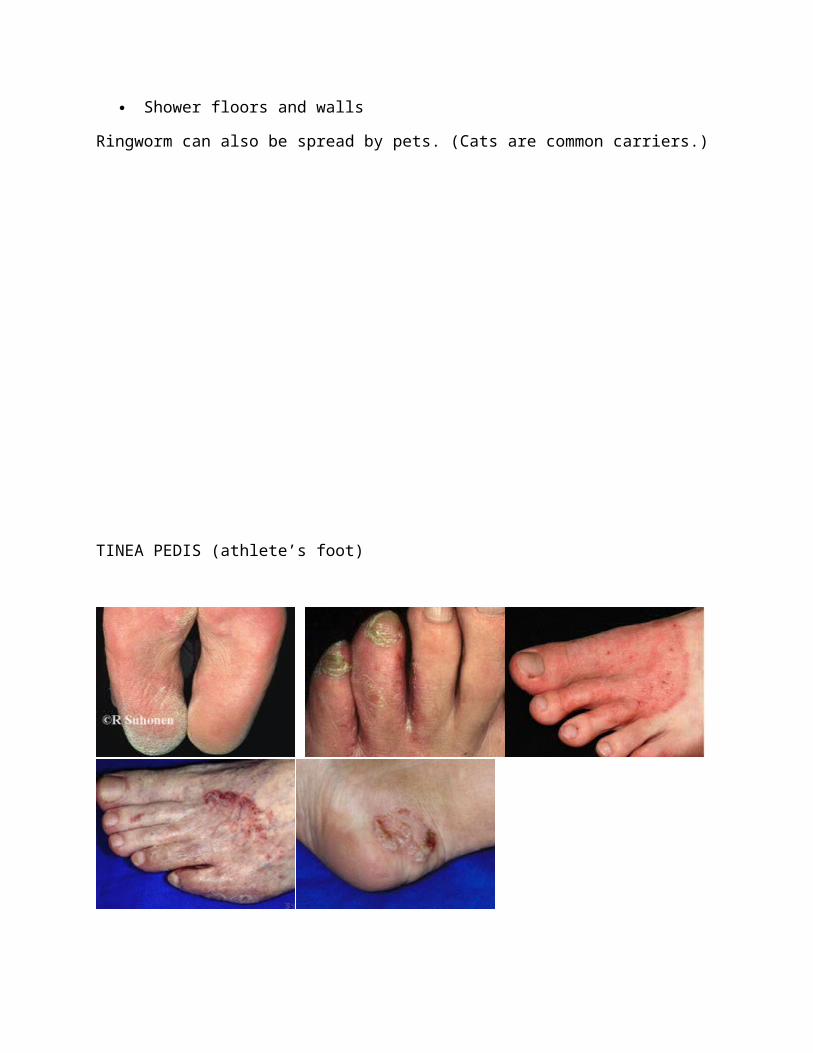
TINEA VERSICOLOUR(pityriasis versicolor)
The fungus Pityrosporum ovale is a type of yeast that’s found on the surface of the skin. It normally doesn’t cause any health problems. However, sometimes this yeast begins to grow out of control, affecting the natural color, or pigmentation, of your skin.
Tinea versicolor occurs when Pityrosporum ovale grows rapidly on the surface of the skin.
Hot, humid weather
Oily skin
Hormonal changes
Weakened immune system
TINEA CRURIS (jock itch)
Jock itch is most commonly contracted by coming into contact with clothing or towels contaminated with the fungus. It can also spread from an athete's foot outbreak.
Jock itch may also be caused by the spread of athlete's foot fungus to the groin.
The groin provides a warm and humid environment, which encourages fungus growth
Excessive perspiration can also encourage fungus growth
EPIDEMIOLOGY:
A total of 18 prevalence studies of the general population in developing countries (10 in sub-Saharan Africa) can be considered representative of large geographical areas; of these, 13 provided data specific to children, 17 to rural areas, and 4 to urban areas. All reported high prevalence figures for skin diseases (21-87%), the following disorders being the commonest in children: pyoderma (prevalence range 0.2-35%, 6.9-35% in sub-Saharan Africa), tinea capitis (1-19.7%), scabies (0.2-24%, 1.3-17% in sub-Saharan Africa), viral skin disorders (0.4-9%, mainly molluscum contagiosum),

pediculosis capitis (0-57%), dermatitis (0-5%), and reactions due to insect bites (0-7.2%).
Children present a higher prevalence rate than adults for pyoderma (especially those under 5 years), certain mycoses (tinea capitis), and, to a lesser extent, scabies. In addition, there have been reports of a particularly high prevalence of pyoderma and/or scabies in more limited settings, or in particular communities (e.g., Aboriginal communities from Pacific).
Incidence data in the general population are scarce, those that are available varying considerably from one place to another for pyoderma (e.g. 10.7% by year to 1.57 per 100 person-weeks in children), and for scabies. Data from five areas suggest that skin disorders commonly represent one of the main organ-specific reasons for visiting a primary healthcare centre, the ratio of visits due to skin problems being in the range 6-23.7% (the highest rates in children); in such centres, the main disorders appear to be pyoderma and scabies, while diseases lacking a specific diagnosis are also common.
The cost of skin diseases has been estimated on few occasions only, but was found significant in the two areas where evaluated. Community-based data from three areas indicated that certain disorders (mainly scabies and pyoderma) were more likely to result in a request for treatment than other skin diseases (tinea capitis, viral disorders, pediculosis capitis).
Data from 18 available bacteriological studies suggest that group A streptococci remain the main etiological agent of pyoderma (either primary or secondary to scabies) in many tropical developing countries, followed by Staphylococcus aureus. The prognosis of pyoderma appears overall to be good, with a global risk for poststreptococcal glomerulonephritis estimated to be largely under 1% in many areas. Lethality related to pyoderma appears very low, except possibly in children aged less than 3 months in whom it has been reported on occasions. to be a significant source of severe bacteraemic sepsis.
The severity of scabies appears to be related to superinfection, which occurs in 16-67% of cases and bears the same risks as primary pyoderma, and to epidemics whose frequency over the world appears largely underestimated. Overall, tinea capitis appears to be a benign disorder, rarely presenting with superinfection, and with spontaneous healing around puberty. The other very common skin disorders (molluscum contagiosum, pediculosis capitis) are also almost constantly benign. Where HIV infection is common, its contribution to the epidemiology of common skin diseases is unknown.
Despite the relative paucity of objective data and some methodological restrictions, it can be assumed that the main etiological factors whose role is probably significant in developing countries are a hot and humid climate (pyoderma), low hygiene and poor access to water (pyoderma), high interpersonal contact and household overcrowding

(scabies and pyoderma), and certain other skin conditions like reactions to insects bites and scabies (pyoderma).
There have also been several reports on the frequency of skin diseases (mainly pyoderma and/or ectoparasitoses/ scabies) in specific population groups: street-children in Kenya (prevalence of skin diseases, 50.9%) [33], child workers in Nigeria (skin infection, 12%) [34], refugee camp in Sierra Leone (scabies, 77-86% in children) [35], remote Amerindian villages in Amazonia (pyoderma, 11%) [36], jungle villages in Panama (pyoderma, 11-20% according to age) [37], an orphanage community in India (pyoderma, 10%) [38], slums in Brazil (scabies 8.8%, p. capitis 43%) [39], and remote aboriginal communities in Oceania, mainly Australia [40-43], and Malaysia [44]. Aboriginal communities from Australia and the Pacific islands exhibited particularly high prevalence figures in children, and often adults, for scabies, beta-haemolytic group A streptococcal pyoderma, and dermatophytoses (scabies: 25% (adults) to 50% (children); pyoderma: 10-70%).
Reference: http://apps.who.int/iris/bitstream/10665/69229/1/WHO_FCH_CAH_05.12_eng.pdf
The increasing population of immunocompromised individuals is a major factor in the emergence of opportunistic fungal infections. The human immunodeficiency virus (HIV) disease epidemic has been shown to be responsible for dramatic increases in cryptococcosis, penicilliosis and histoplasmosis. As HIV patients are at increased risks for fungal infections, the concentration of this group of patients in a single centre may result in a different fungal epidemiological profile as compared with a general hospital, non-infectious disease reference centre.

The distribution of races was significantly associated with HIV status. Among the HIVnegative individuals, the Malays comprised more than half (55.6%) of patients, followed by Chinese and Indians. However, among HIV-positive individuals, only one-third were Malays. Chinese, Myanmar, Indonesian and other races formed the other two-thirds of patients (Figure 1). Other races included Vietnamese, Bangladeshi, Pakistani, Caucasians and other East Asians. The most common groups of fungi isolated were yeasts (80.5%), followed by thermally dimorphic fungi (16.9%) and moulds (2.6%). Among isolates, Candida albicans was the most commonly isolated.
All age groups were affected. The most commonly affected age groups in this study were adults aged 18 years and above. A high male-to-female ratio (2.9:1) was noted in our patient population. Almost half of male patients were infected with HIV (43.9%) compared to (20.0%) in female patients. The distributions of mycoses among all patients were highest in Malays, followed by Chinese and Indians; however, this may reflect normal ethnic distribution in Malaysia. The distribution of race between HIV-positive group and HIV-negative group differed significantly (p<0.001). Malay predominance in HIV-negative group was significantly diminished by increases in Chinese, Myanmar and Indonesian proportions.
Almost two-thirds (62.6%) of positive fungal cultures came from the infectious disease (ID) and general medical wards. This finding may be attributed to the patient population in those wards with serious underlying medical conditions, including HIV as compared with other wards.
Reference : http://iiumedic.net/imjm/v1/download/Volume%2012%20No%201/Vol12No1%20p39-42.pdf
RISK FACTOR:
General:
Warm, moist environment such as shoes, socks,swimming pools, locker rooms, and the floors of public showers. Spread from person to person through direct contact or indirectly from objects carrying the fungus. Direct contact with infected people or animals. It also may be spread on clothing or furniture. Heat and humidity may help to spread the infection.
Specific:
1. Weak immune systems:
a. organ transplant patients
b. people living with hiv/aids
c. cancer patients
d. hospitalized patients
e. stem cell tranplants patients
f. people taking medications that weaken the immune systems
2. How did I get a fungal infection?You can get a fungal infection by touching a person who has one. Some kinds of fungi live on damp surfaces, like the floors in public showers or locker rooms. You can easily pick up a fungus there. You can even catch a fungal infection from your pets. Dogs, cats and farm animals can be infected with a fungus. Often this infection looks like a patch of skin where fur is missing.
3. Antibiotic Use & Fungal Infections:Antibiotics are medicines designed to kill harmful bacteria that are causing infection or illness. Sometimes these drugs can also reduce the helpful bacteria that live in the body. When these populations are reduced, fungi may take the opportunity to colonize.
4. Corticosteroid Use & Fungal Infections:Corticosteroids are a group of drugs that reduce inflammation. They effectively treat many skin disorders. Unfortunately, these drugs also can reduce our immune response and improve conditions for fungus growth.
5. Medical Conditions & Fungal Infections:Individuals with diabetes and some cancers, such as leukemia, are more susceptible to fungal infections than the general population.
6. Compromised Immune System & Fungal Infections:The immune system is a set of chemical and cellular responses that attack disease-causing organisms and help prevent their growth. A number of factors can depress this system. These include chemotherapy (cancer-killing drugs) and acquired immune deficiency syndrome (AIDS).A depressed immune system less effectively fights off all types of infection. Thus a fungus that normally would be controlled by the immune system may begin to grow.
7. Environmental Factors & Fungal Infections:Fungi require moisture to grow and reproduce. Fungal infections are more prevalent in warm, moist areas of the body, such as the mouth and vagina. Also, sweaty clothes and shoes can enhance fungus growth on the skin. Exposure to fungi is more frequent in communal areas with moisture, such as locker rooms and showers.
8. Hereditary Factors & Fungal Infections:Some people seem to have a genetic predisposition toward fungal infections. They may contract infections more easily than others exposed to the same conditions. Whether this is due to differences in immune response, skin chemistry, or other factors is not known.
9. Transmission of Fungal Infections:Fungal infections can be passed from person to person or from objects and surfaces to a person. Also, an individual can transfer infection to other parts of the body by touching.
SIGNS & SYMPTOMS
a) Ringworm (tinea corporis)
Known as “kurap”
Red, itchy flat scaly area on arms, legs, or body
Patch’s border expand, forms almost a circular ring
Irregular, wavy outlined ring
b) Athlete’s foot (tinea pedis)
Known as “kaki makan air”
Ulceration between toes
Soft, pale, and white skin when it’s wet
Itching
Stinging and burning
c) Jock’s itch (tinea cruris)
Reddish patches spread out from the fold near the groin towards the upper thighs (for poster, hajar x reti nk shorten ayat ni..nk buat “reddish patches at groin area”, takut trlalu sama dgn snior’s)
Itching
Burning
d) Tinea versicolor
Known as “panau”
Discoloured patches on torso and shoulders
Scaling
May accompanied by itching
REFERENCES
http://www.mayoclinic.org
Rutter, P. (2009) Community Pharmacy: Symptoms, Diagnosis and Treatment, 2nd Edition. Elsevier Limited.
COMPLICATION FOR FUNGAL INFECTION
- Spread to another part of body such as to, legs and toenails, hands fingernails and any essentially body area.
- Such as fungal nail infection(onychomycosis) for tinea pedis.- With a patient with lack of immune response like diabetic patient cause ulceration
neuropathy (loss of pain) and gangrene.- Prone to bacterial infection causes inflammation on the skin (cellulitis) if left
untreated.- Tinea versicolor reinfection in high rate thus must wait for a few months for
disappearance of white spots after skin regenerate.
DIAGNOSED AND TEST
1. Tinea corporis (ringworm)
2. Tinea pedis ( athlete’s foot)
3. Tinea versicolor
4. Jocks itch (tinea cruris)
By performing a physical examination :-
Vital sign
Inspection on infected skin
By taking history before get the infection :-
Sexual history
HIV status
Gym or sports activity
Use of communal pool or whirlpool
Pets
Travel history
Skin scrappings :-
Infected skin will be tested with potassium hydroxide.
Small area of infected skin will be scrapes off.
Then, it will be placed in potassium hydroxide.
The potassium hydroxide will kills all normal cells.
So the fungal cells will be easily seen under microscope.
Fungal cultures.
ANTIFUNGAL TREATMENT
1. Topicals
Clotrimazole
Econazole
Ketoconazole sometimes combined with mild steroid
Miconazole (hydrocortisone) to reduce inflammation
Tioconazole
Terbinafine
How to use cream? Apply cream to the affected area two times a day for 2 weeks and continue for 5 to 7days until it heals.
2. Shampoo which contain ketoconazole help to treat scalp fungal infections and certain skin conditions.
3. Pessaries are tablets which are designed to be put into the vagina.
4. Intravenous (severe) –injected into the bloodstream
5. Oral- swallowed in capsule, pill or liquid form
PREVENTION/ALTERNATIVES/SUPPLEMENT
Types of infection Prevention Alternatives/supplement

Tinea corporis/Ringworm on body
Ringworm is contagious. It spreads when you have skin-to-skin contact with a person or animal that has it.
To prevent the infection from spreading:a. Avoid infected animalsb. Don't share personal itemsc. Keep clean
Topical application of :a. Tea tree oil- may kill
fungus, and reduce allergic skin reactions.
b. Garlic oil- can inhibit unwanted fungi
Each of these is effective at reducing the symptoms of itching and burning.Tinea pedis/
athlete's footPrevent athlete's foot by keeping your feet clean and dry.Example:- Take time to dry your feet, including each toe, thoroughly-Wear cotton socks to absorb sweat- Wear sandals to prevent bare feet from touching floors contaminated with fungi.
Tinea Cruris/Jock itch (Groin)
Reduce your risk of jock itch by:- Keep your groin area dry.- Wear clean underwear.- Don't share personal items- Avoid tightfitting clothes/underwear
Tinea versicolor Tinea Versicolor can be caused by malnutrition and vitamin deficiencies. To prevent or improve the condition is eat a healthy balanced diet or take vitamin supplements
Vitamins that can help regulate melanin production so that the hypo-pigmented spots typical of Tinea Versicolor disappear faster.
a. Vitamin B12 regulates melanin production
b. Vitamin C is important for collagen production
c. Vitamin A can treat skin that is blotchy in colour; it can even out your skin tone
d. Vitamin E is an anti-oxidant that protects and repairs skin