fistula in ano new operation sloft (submucosal ligation of fistula tract)
TRANSCRIPT

SLOFT (Sub mucous Ligation Of Fistula Tract)
For Fistula in Ano
Dr D.U.PathakMS FACRSI
Jabalpur (M.P) India

Basic understanding
• The internal opening is always at the dentate line.
• High opening is usually Iatrogenic.

Role of Investigations
• Mandatory in recurrent fistulae and undetectable internal openings
• MRI is the best one.

The Aim of treatment
• Control of sepsis
• Prevention of incontinence and recurrence
• Giving him less pain, morbidity and job loss

Existing methods
• Lay open
• Seton
• Cut and repair of the sphincter after excision of the tract.
• Fistula plug
• VAAFT
• LIFT

Lay open
• Big painful wound with long term recovery
• Makes the patient incontinent at least for flatus.
• Gives a bad scar and furrow.
Seton
• Painful long term cutting of the sphincter

Excision of the tract and
Primary repair of sphincter
• Needs high expertise
• Associated with high incidence of incontinence.

Fistula plug
• Very attractive choice for affluent class
• The zero morbidity way but associated with high recurrence rate

VAAFT
• It’s a high tech costly operation

LIFT
• Sound surgical principle
• Low morbidity
• No incontinence
But
• Difficult to learn,
to do and to teach

SLOFT is nothing
but
simplified LIFT

SLOFT (Sub mucous Ligation Of Fistula Tract)
• Basic principle is of LIFT- ligation of the tract
• In SLOFT -
• It is more proximal
• It is more superficial
• Leaves behind a smaller stump of the proximal tract

Schematic representation of SLOFT
Internal opening
Tract hooked
Dentate line

Probing
• Probe is gently introduced to come out from internal opening
• Then it is bent and pulled out of the Anus.

Injection Xylocaine adrenaline
• This blanches the area and does hydro dissection around the tract
Muco-Cutaneous
Junction

Hooking the tract
• Incision is at the muco cutaneous junction
• The tract is hooked
• Here it is superficial.

Site of ligation
• It is Sub mucous and is medial to the internal sphincter

FAQ – How far from Internal opening?

Division of the Tract
Anus
Anus
Hooked tract
Tract transacted

Distal tract
• Cored out and sent for HPR .
Coring of external
tract
EAL near internal opening

Wound
• Can be Primarily closed

Fistula at 4-Oclock

Multiple tracts – method is the same
Opening at 6-O clock
Opening at 2-O clock
Opening at 2-O clock
passing gas from scrotum
All the three tracts SLOFT done separately
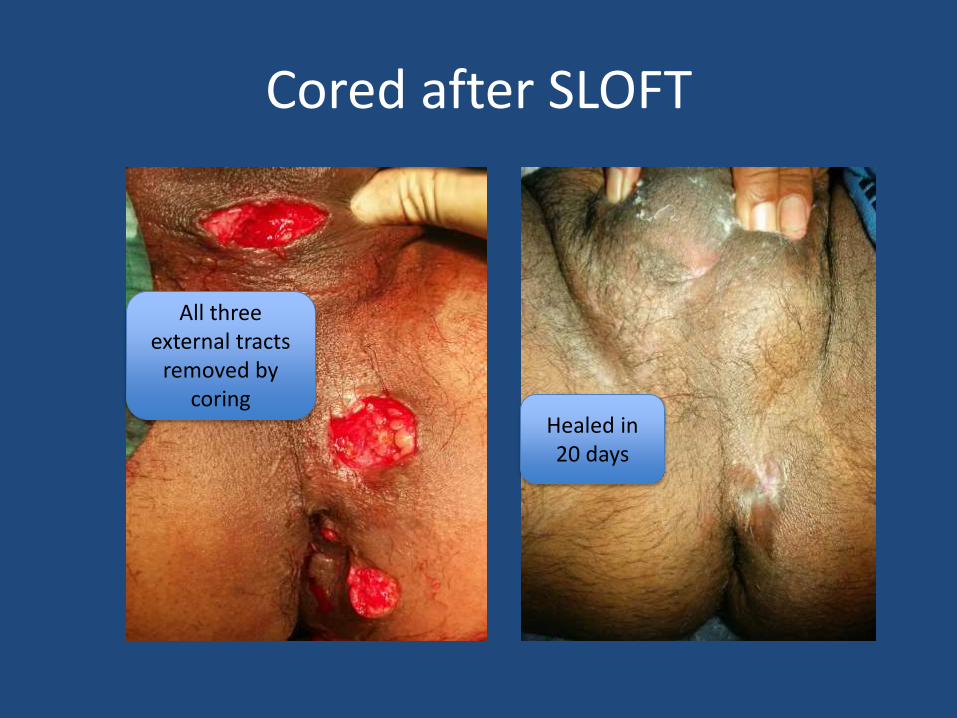
Cored after SLOFT
All three external tracts
removed by coring
Healed in 20 days

What is new in this method?
• Nothing
• In LIFT also the tract was tied and cut.
• I have just made it simple and reproducible.
Aim remains the same
disconnect the internal opening which is like a funnel pouring infection out.

Post operative period
• Discharge in a day
• No post discharge dressings

Immediate post op picture
This patient had two tracts with one para rectal blind extension.

This study
• This prospective study was carried out from January 17th 2014, till date.
• 43 patients have been operated of all types of fistulas with no exclusion criteria.
• Of them, 4 were recurrent cases
• The early results and recovery have been uneventful.

Recurrences ??
• Time only will tell the percentage but
• They are bound to occur
Recurrence bothers the patient
if
the procedure was either costly
or the recovery was painful.

Seriously looking forward for long term results
Thanks…