fire-ems training contra costa county ems. tim w. hennessy mci plan tim w. hennessy communications...
TRANSCRIPT

FIRE-EMS TRAININGFIRE-EMS TRAINING
Contra Costa County EMSContra Costa County EMS
Tim W. HennessyMCI Plan
Tim W. Hennessy Communications Supervisor
Contra Costa County Sheriffs Communication
1975-2007
This MCI Plan is dedicated to Tim.
His expertise and commitment in
developing this plan was invaluable.

History
• 1979: First MCI Committee organized to develop plan following Yuba City bus crash in Martinez
• 1983: Board of Supervisors approved the first MCI Plan
• Several revisions to the basic plan since 1983

Current MCI Working Group
• Appointed in 2005 to conduct a ground-up rewrite of the MCI Plan
• Multidisciplinary– Fire – Emergency Ambulance Zone Provider (public
and private)– Law Enforcement– Hospitals– Public Safety Communications– EMS Agency staff

Why Rewrite the Plan?
• Improve the usefulness of the document for first responders
• Compare the Plan to the County’s current risk profile
• Compare the Plan to the County’s current public safety and EMS resources

Why Rewrite the Plan?
• Attempt to resolve weaknesses in the Plan experienced during previous incidents:– Incident command and control– Communication flow– Resource ordering and tracking
• Ensure compliance with NIMS

MCI Plan Objectives
Objective #1:
Establish a common organization, management, and communications
structure for the coordination of emergency response to a multi-
casualty incident.

MCI Plan Objectives
Objective #2:
Establish methods of triage and transportation that will provide the best
medical outcome possible for the greatest number of casualties.

MCI Plan Objectives
Objective #3:
Establish pre-defined responsibilities of all entities with key roles in achieving
successful implementation of the plan.

MCI Plan Objectives
Objective #4:
The Plan will be drilled regularly, and reviewed annually and following
significant activations of the Plan as directed by the EMS Director.
Key Concepts
• Use of Incident Command System– Expansion and contraction of
structure is dynamic and incident-driven
– Use of single point ordering for resource requests
– Emphasis on exchanging information
Key Concepts
• Importance of Unified Command• The “Rule of 2 and 4”

MCI Tiers
• Plan consolidates Expanded Medical Emergencies, Medical Advisory Alerts and MCIs into a single MCI Plan with 4 activation tiers
• Use of tiered MCI Plan reinforces the scalability of the Plan
MCI Tiers
• Use of Tiers modeled after Community Warning System Levels
• Consistent with best practices
Tier Zero
• Notification of incident with potential to escalate to a higher tier (Medical Advisory Alert)
• CWS Level II and III Incidents• Report of Active Shooter incident• Attempted emergency landing of
passenger aircraft
Tier One
• 6-10 patients with scene contained, number of patients not expected to rise
• Multi-vehicle collision• Multiple gunshot victims at
contained scene and no ongoing active shooter

Tier Two
• 10 –50 patients or less than 10 patients with substantial chance of increase in number of patients
• Transportation resource ordering switches to EMSOACC
• Petrochemical incident• Passenger train derailment• Active shooter with uncontained scene
Tier Three
• More than 50 patients or reasonable expectations of large number of casualties
• Actual or suspected WMD incident• Significant explosion in populated
area• Emergency evacuation of hospital
or SNF
Plan Components
• Responsibilities matrix/checklists• Communications flowchart• Communications overview• ICS position checklists• ICS communications forms 205 and
217A

Responsibilities Matrix
• Review pertinent matrices– Pp 7 - 16

MCI Checklists
• Common Responsibilities– Back of each checklist
• Get Assignment• Check In• Get Briefed• Get work materials• Undertake mission safely• Organize and brief subordinates• Assure comms• Use clear text• Complete forms• Demobilize as required/practical

Unit Leader Responsibilities
• Back of each checklist– Participate in planning as required– Get accurate SitStat/ReSTat of assigned units– Confirm arrival time of resources– Assign duties to subordinates as required– Develop accountability, safety and security– Supervise demobilization– Provide logistics with re-supply needs– Maintain unit log

Packaging of MCI Plan
• Standard Packaging• Hand out bundles• “You are the checklist until you
delegate it”• Morgue Manager-Law enforcement• Certs/Quals determine who does
what…not rank or position
Personnel Options
• Branch Director– Chief Officer(Fire)/Lieutenant/Captain (Law)
• EMS/Pt Transport Group Supervisors– Captain (Fire)/Sergeant (Law)/Supervisor(EMS)
• Triage/Treatment/Transport Unit Leaders– Captain(Fire)/Sergeant(Law)/Supervisor(EMS)

Transportation Group Supervisor/Unit Leader
• Only one per incident• If a Single EMS Group Supervisor
– Reports to the EMS group supervisor
• If multiple EMS Group Supervisors– Reports to the EMS Branch Director/Ops
• Single Staging area for ground transport units
• Single Helispot for air transport units

Transportation Highlights
• 2/4 Concept– Continue to disperse casualties as much as
possible– Use farther hospitals first
• Especially if potential exists for “walk ins”
– Hospital polling whenever possible but certainly after 2/4 has been maximized
• Coordinate with EMSOACC as much as possible

Transportation Highlights (cont)
• Emergency Ambulance Zone Providers still responsible for normal coverage too
• If limited ambulances, minors can be transported by other means
• Tier 2 & 3 suspend ambulance to hospital comms• PCRs
– Whenever possible PCRs shall be completed– Tier 3 Branch( or designee) can suspend standard
PCR protocol and replace with triage tag info– Triage tags are minimum level of documentation

Predetermined Staging Areas
• East/Central/West• Rallying point in case of loss of
communications

Example of Tier 1 Scenario
• MVA with 7 patients in 3 vehicles– Single Medical Group– Transportation reports to Med Grp Sup– Triage patients and treat where they were
found– Do not send all patients to same hospital– Can use close hospital due to lack of
probability of self transporting patients to closest facility

Example of Tier 2 Scenario
• Shooting incidents with 21 patients– Single Medical Group– Transportation reports to Med Grp Sup– Triage patients where they are found– Litter bearers move patients to specific
treatment areas– Patients re-triaged in treatment areas and
assigned priority for transport– Avoid close proximity hospitals if possible
due to potential private transport arrivals

Example of Tier 3 Scenario
• Large structural collapse with multiple victims trapped over a widespread area– Multiple Medical Groups (probably by Division) report
to Medical Branch– Transportation reports to Medical Branch
• Still just one transportation staging area– Triage patients where they are found– Litter bearers move patients where they are found– Patient’s re-triaged in Treatment areas and assigned
priority – Maximize 2/4 concept as needed


Triage Considerations
• START Triage system– BLS personnel perfect for this– Utilize teams whenever possible– Good mission for an Engine Company– Minimal Treatment
• Do not re-triage at scene• Can re-triage in Treatment Areas

Triage Considerations (cont)
• Patients can be upgraded or downgraded– New tag if not written on– Fold old tag and give new one if started writing
patient info on it• ?Who providers litter bearers
– PT TX Unit Leader• DOA’s stay where found unless need for movement
necessitates taking them to a morgue location• Patients may not be moved to a Tx Area
– MVA’s with limited number of victims
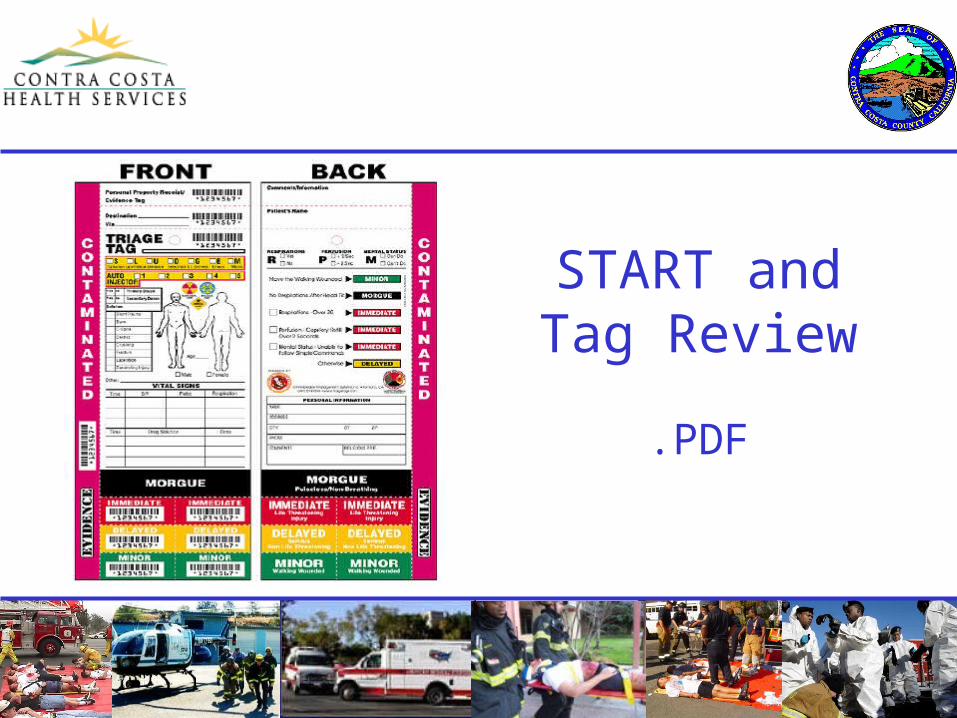
START and Tag Review