filaria and plasmodium: distribution of endemic diseases ... · filaria and plasmodium:...
TRANSCRIPT

1
XIV International Economic History Congress, Helsinki 2006
Session 46
Filaria and plasmodium: distribution of endemic diseases andwestern plain exploitation in Taiwan (draft, please do not cite without permission)
Liu Shiyung
Institute of Taiwan History
Academia Sinica
Taipei, Taiwan
Modern scientific circles believe the global warming had been speeded up andcausing various diseases. WHO’s report in 2000 points that many mosquito-bornediseases such as malaria, dengue, and yellow fever would bounce back due to the fastglobal warming. As the entomologists already knew, cold weather can limitmosquito’s activities and rest area. Therefore, the morbidity rates of thesemosquito-borne diseases reduced. Although extreme temperature can hurt mosquito,in most of the time, mosquito’s activity increases when the weather getting warmer.Environmental changes certainly cause high risk of infection of the mosquito-bornediseases. However, global warming should be the only one to blame. Before theglobal warming became a overwhelming public concern, land use or naturalexploitation had locally caused changes in mosquito living environment andfluctuation in infectious rates. The infection and geographic distribution of filariasisand malaria in Taiwan prove such phenomena happened and disclose the possiblerelation between disease and natural exploitation.
The Ecological characteristics of filariasis and malaria in Taiwan
Because of the southward migration after the seventh century in Mainland China,many Chinese doctors observed and recorded filariasis- or malaria-likesymptoms.1Early medical historian Chen Shengkun, by his training in modernmedicine, had identified some of the symptoms are actually filariasis on the latest
1 Fan Jiawei, “The migration and zhangqi illness in Lingnan region in the Six Dynasty Period”Hanxueyenjiu 16 1(1998 : 27-58

2
stage.2 Another historian Chen Bangxian even asserted a Chinese book in 800 B.C.already recorded malarial infection. 3 Despite the question remained to theirjudgment, the prevalence of filariasis and malaria in costal China including Taiwanbefore the 1950s is obvious.
According to modern parasitology, there are nine types of filaria in nature, butonly Wuchereria bancrofti and Brugia malayi mainly cause human filariasis. 4
Among them, Wuchereria bancrofti is the most common one and first to bediscovered. Demarquay in 1863 first found its microfilaria from the scrotum of aHavana patient. Bancroft later in 1876 separated imagoes in Brisbane, Australia.5
Before Bancroft’s discovery, a port-doctor Meadow already recorded many Chineseelephantiasis patients in1871 in costal China.6 Between 1872 and 1878, PatrickManson treated many elephantiasis patients in costal Fukien province. Later inAmoy, Manson proposed his discovery of the transmission and lifecycle ofmicrofilaria and mosquito, which was the inspiring mosquito-borne theory.7Bancroftand Low soon supplemented their founding to Manson’s theory8 and provided a
comprehensive picture of Wuchereria bancrofti lifecycle. (Figure 1) To Brugia
malayi, Asia is the major perch of this parasite. As early as in 1905, Ashburn andCraig found a “mutated” type of Wuchereria bancrofti in Philippine and named itFilaria philippinesis. New evidence continuously exposed, Lichtenstein and Brugdiscovered Filaria malayi in Dutch Indonesia in 1927, believed it should a new typeof filaria. However, the parasitological circles did not accept Lichtenstein and Brug’shypothesis until Rao and Maplestone’s identification of two adult worms in India inthe 1940s. Famous parasitologist Buckley finally confirmed Brug’s contribution andclassified the worm “Brugia malayi”.9
The epidemiological investigation of filariasis in China started by Chineseresearchers since 1926. Feng Lanchow identified both Wuchereria bancrofti andFilaria philippinesis (later the Brugia malayi) in Amoy in 1931. He later confirmedthe prevalence of both parasites in Chinese costal areas. Furthermore, Feng Lanchow
2 Chen Shengkun, “ A historical study of endemic diseases in southern China” Kexue yunkan 10:12(1979): 67-683 Chen Bangxian, “ Malaria history” Yishi kunglun 4:2 (1936): 1-24 Public Health Department ed., The Prevention of Filariasis (Nantou: Taiwan government, 1973), p.9.5Morishita Kaoru, New Summary ofHhuman Parasites (in Japanese), (Tokyo: Tobohdoh, 1943), pp.254-5.6 Meadows, R. “Report on the Health of Ningpo,” China Customs Report 2:1(1878).7 Manson, P., “Further Observation on Filaria Sanguinis Hominis,” China Customs Report 1:35(1871).8Public Health Department ed., The Prevention of Filariasis, pp. 20-219 Buckley J., “A new genus, Brugia, for Wuchereria spp. Of the Malayi group” paper delivered to the6th International Congress of Tropical Medicine and Malaria, Lisbon 1958, p. 35.

3
identified Anopheles sinensis is the major vector to transmit Brugia malayi whilecommon Culex spreads out Wuchereria bancrofti.10 A latest report in 2002 revealsthe geographic distribution of both parasite in China and Taiwan before the 1980s.filariasis and elephantiasis are commonly seen in middle China as well southernShandong, Henan, Anhui, Jiangsu, Zhejiang, Fukien, Jiangxi, Guangdong, Guangxi,Hainana, Hunan, Hubei, Guichow, Szechwan, and Taiwan. Most areas suffers bothparasites but Shandong, Hainana, and Taiwan have only Wuchereria bancrofti.11
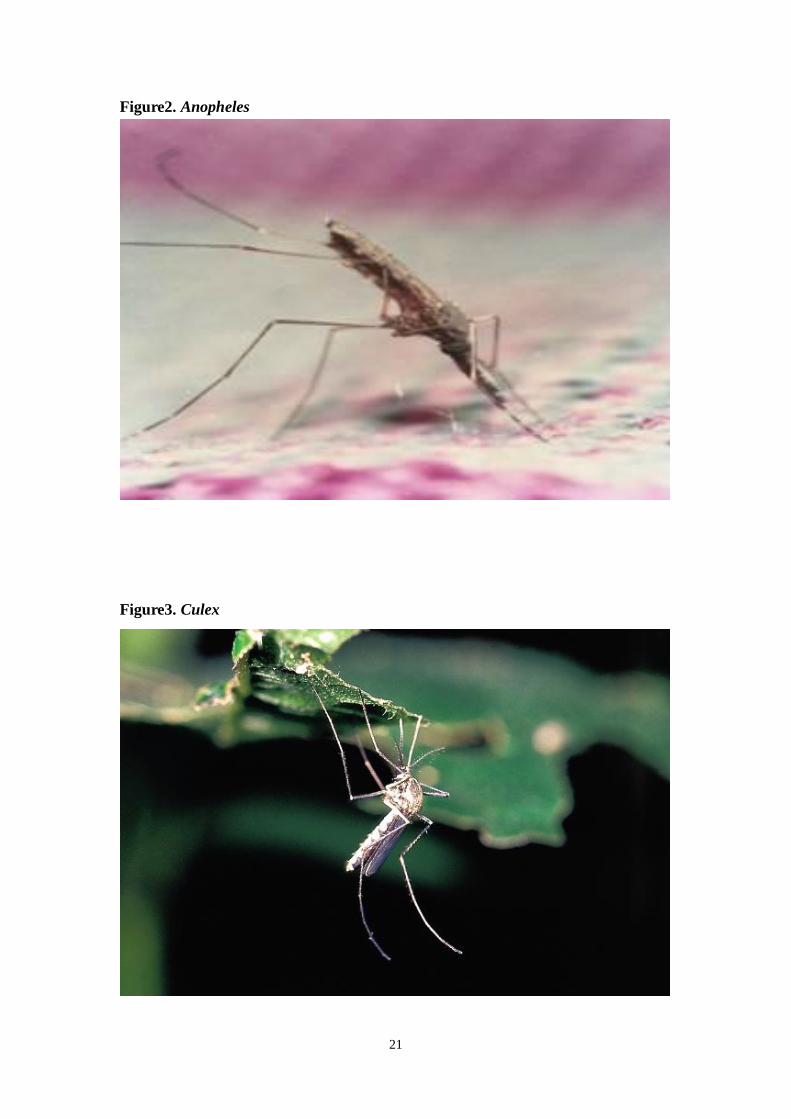
Compare to Anopheles (Photo 2) the malaria vector, Culex (Photo 3) is the majormedia of filariasis. To Brugia malayi, Anopheles sinensis, Mansonia uniformis, andAdes togoi are important media in China. They are coincidently the most commonmosquitoes in costal China. To Wuchereria bancrofti, Culex pipine pallens and Culexpipine fatigans play a main role of transmission while An. sinensis could be aninsignificant vector.12 Due to the living habits, Taiwan only has Culex pipinefatigans.13 And the lifecycle of microfilaria of Wuchereria bancrofti inside mosquitois highly determined by temperature and humidity outside. In conclusion, Wuchereriabancrofti is the only human filarial in Taiwan and usually transmits by Culex pipinefatigans. Any wet areas and container under the altitude 2,200m breed this kind ofmosquito.14Because of biological and ecological limits to filarial and mosquito, theoutbreak of filariasis in Taiwan is seasonal and regional.
Since the colonial period (1895-1945), malariologists already identified tovectors of malaria in Taiwan: Anopheles sinensis and An. minimus. Despite An.sinensis also transmits Brugia malayi in China, An. minimus shars no similarity withCulex and certainly will not transmit any filaria. In Taiwan, An. sinensis can be foundeverywhere, especially the plain has sufficient sunlight and wide range of waterreservoir. Various paddy fields and irrigation system could be the best breed ground tothem. However, An. sinensis usually bits domestic animals, seldom sucks humanblood. Although An. minimus can also be found island wide, its wiggler prefers to livein creek or small drain close to the foot of mountains. Terraced fields are their breedground. In addition, An. minimus totally relies on human blood for living.15Different
10 Feng, L.C. and Yao, K.F., “Observations on Filariasis in Huchow Chekiang, China” ChineseMedicine Journal No. 49 (1935): 796.11 Ryan ET, Wilson ME, Kain KC. “Illness after international travel,” New England Journal ofMedicine no. 347 (2002):505-16.12Public Health Department ed., The Prevention of Filariasis, p. 1113 Morishita Kaoru, New Summary ofHhuman Parasites (in Japanese), pp. 16-18 and 50-52.14 Chen Jinsheng, “Chapter 3. the ecology and prevention of tropical culex”, in Li Xuejin ed., TheEcology and Preventive Skills to Domestic Insects (Taizhong: National Zhongxin University, 2000), pp.37-39.15 Taiwan Governer-General Government, Summary of Malaria in Taiwan (Taihoku: TaiwanGoverner-General Government, 1935), pp. 1-3.

4
anopheline mosequito may live in various altitudes.16 According to Morishia’s study,altitude 900m would be the living boundary of An. sinensis and An. minimus inTaiwan. Above that height is mainly the domain of An. minimus while An. sinensisoccupies the plain areas below that altitude.17It is obvious that both anophelinemosequitoes habitual areas are much lower than Culex’s 2,200m altitude.18Generallyspeaking, the vector of filariasis, Culex pipine fatigans lives in a much wider rangethan An. sinensis and An. minimus in Taiwan. (Table 1)
Table 1, Ecological habits and distribution of Culex, An. sinensis, andAn. minimus in Taiwan
Parasites Density Rest habitsMosquitoes Wuchereria
bancroftiBrugiamalayi
MalarialPlasmodium
North Middle SouthPenghu
Islesaltitude
Anophelessinensis
x X X AA AA AAA AAPlain below1,667m.
Mansoniauniformis
X A A AAreas below500m.
Ades togoi x AA A A AAOnly incostal areas.
Culexpipinefatigans
X AAA AAA AAA AAABelow2,200m.
An. minimus X AA AA AA AMountainousareas under1,197m.
Note: x means insignificant vectors and X is major media.A represents low density, AA middle, and AAA high density.Blank in parasites item only represents non-vector of certain parasite and in
density item means no record of this type of mosquito.Resources: Morishita Kaoru, Malaria: Epidemiology and Prevention, (Tokyo:
Hankikeya, 1976), pp. 99. Public Health Department ed., The Prevention
of Filariasis, p. 57
16 Creighton Garnham, “The Incidence of Malaria at High Altitudes,” Journal of the National MalariaSociety no.7 (1948): 275-284.17 Morishita Kaoru, Malaria: Epidemiology and Prevention, (Tokyo: Hankikeya, 1976), pp. 31 and100-101.18Public Health Department ed., The Prevention of Filariasis , p.57
5
However, Table one merely reveals the possibility of the distribution of filariasisand malaria in Taiwan by the knowledge in parasitological textbooks. The realsituation of filariasis and malaria infection in colonial Taiwan did not totallymatched with the textbooks suggestion.
The discovery of filariasis in Taiwan
The earlest record of filariasis in Taiwan was from a British doctor’s note. Dr.Mayer claimed in 1886 that he observed several elephantiasis patients in Taiwan butdid mention any blood-examination.19 A Japanese doctor Ch jun Noshi in 1909indentified seven Japanese filariasis patient but could not separate the filaria from
patient’s blood. Ten years later in 1919, residential doctor of Penghu Hospital
and first found a Taiwanese chyluria patient but, still, not a clue of
filaria.20 Until 1927, a surgeon in Taihoku (Taipei in Chinese) Hospital
successfully found filaria in a tumor from a Japanese female patient. However, hehad no way to confirm the patient was infected in Taiwan.21 Next year, a army
surgeon separated filarial from the scrotum of a 14-year-old young man
who had been already spent nine years in Taiwan. strongly implied that could
a local case of filariasis.22The reports of filariasis were pretty rare before the 1920sTaiwan. The Japanese reports above were actually the only information we can find
in the professional journal-- (Formosan Journal of Medical
Association, FJMA), and had no clue to distinguish Wuchereria bancrofti and Brugiamalayi in their reports.
Lack of report in FJMA could mean no major outbreak of filariasis in Taiwan.However, a British doctor John Maxwell would not agree with Japanese observation.In his book, during the travel in southern Taiwan in 1929, Dr. Maxwell mentioned his
19 107 (1911) 78520 200 (1919)
688-68921
262 (1927) 84-8622 283 (1928) 1192

6
treatment to many local filariasis patients, concluded the filariasis in southern costalTaiwan should be prevalent and endemic.23 Maxell’s conclusion remained silent toJapanese researchers in the 1930s. Compared to the booming malarial studies,
filariasis research was definitely unimportant. Only a army surgeon submitted
his investigation of filaria to the students of normal schools between 1935 and 36.
Again, found no lead to support Maxwell’s observation.24
A. Identifying Wuchereria bancrofti in Taiwan
Without the preparation of the Pacific War, Japanese researchers might never payattention of filariasis in Taiwan. To guarantee the safe of Taiwan Strait, JapaneseNavy was expending the maintenance dock in Makung, Penghu since 1935. Healthylaborer was the major concern during the expansion. From the regular health
examination, a navy surgeon collected 229 local cases and found 99
filariasis positives with the case morbidity rate of 43.3%. Among these infected
cases, 37 patients had filarial in their blood. Under the microscope, first
proved these local positives were Wuchereria bancrofti infected and indicated the
disease was endemic in all Penghu Isle. 25 ’s report attracted a famous
parasitologist ’s attention. In 1939, led an investigation team to
Penghu to confirm ’s observation. In the conclusion, the team found a infection
rate of filarial 8.6% in Penhu Isle and all cases belonged to Wuchereria bancrofti.26
(Photo 4)
Penghu had cases did not mean Taiwan must suffer the same condition. In
order to solve the dilemma between Maxwell and , Huang Dengyun investigated
Pingdong area in southern Taiwan. Within the 5,267 examinees, no filarial career
23 Maxwell F.L., The Diseases of China (Shanghai: ABC Press, 1929), pp. 32-33.24 277 (1936) 79825 Mikrofilaria
389 (1937) 1815-182526
415 (1939) 1452-1465

7
showed in blood-examination.27 thus based on Huang’s result, claimed
Mexwell’s observation was wrong. The places that Maxwell mentioned, could be inPenghu but no way to find in Taiwan 28 However, when Fan Pingzhen citedinvestigations between 1958 and62, he found local filariasis cases southwestern costalTaiwan. (Photo 5) His studies suggests that the southwestern costal Taiwan sufferersendemic filariasis with a single parasite Wuchereria Bancrofti. The average infectiousrate is 1.5%, much lower than in Penghu Isle.29
B. Brugia malayi showed up in post-war Taiwan
As mentioned previously, costal China has endemic Wuchereria Bancrofti andBrugia malayi but Taiwan has only Wuchereria Bancrofti. The Nationalistgovernment in China moved to Taiwan in 1949 and eventually imported some Brugiamalayi cases. Based on Fan Pingzhen’s investigation, the 27,000 cases of filariasis inthe examinee among the Chinese refugee, and the infectious rate of Brugia malayiwas nearly 50%.30 The refugee of Dachen islander in 1955 from Zhejiang cost hadeven higher infectious rate of 96%.31Strange enough, two islands, Kinmen (Quemoy)and Mazu, outside of Fukien had high filariasis rate of 45% but none of Brugia malayilocal case.32Without local and relapsing case Taiwan remains a Brugia malayi-freeisland33 while the vector Anopheles sinensis did exist and cause serious plain malariain colonial period. Since Anopheles sinensis would transmit Brugia malayi and didhappened in costal China, the same mosquito in Taiwan did not carry the sameparasite would be a myth. Several explanations such as mosquito’s habits,environmental changes, and people’s living style etc. can be added to answer the myth.Table two here would shows some results after cross-examined these factors (Table2).
27
(Acta Japonia Medicina Tropicalis) 1 2 3 ( )(1939) 411-43528 Fan Pingzhen, “ The review of filariasis study: focusing on the eradication in Quemoy”, SpecialIssue of Parasitology of National Yang-min Medical College (1982): 138.
29 Wu Y.T., Chen, C.T., “Filariasis endemic areas in the Taiwan Proper. Part 1. Incidence ofBancroftian microfilarial infection among the native people in southern Taiwan,” Formosan Journal ofMedical Association (FJMA) no. 59 (1960): 262 and 1163. Also refer to Wu Y.T., Tseng P.T. and Chen,C.T., “Recent advances in the studies of filariasis and its control in Taiwan,” in Public Health (1963):1.30 Fan P.C. and James Hsu, “Filariasis in Free China: Part 7. Incidence among the Military in Taiwan,Penghu (Pescadores) and Kinmen (Quemoy),” FJMA 5:1(1958): 29-44.31 Fan P.C. and James Hsu, “Filariasis in Free China: Part 6. Incidence of Filariasis among TachenEvacuees in Northeast Taiwan.,” FJMA no. 4(1957): 188-199.32 Fan P.C. and James Hsu, “Filariasis in Free China: Part 4. Incidence in Kinmen Chinese,” FJMAno. 2(1957): 81-95. Fan P.C. and James Hsu, “Filariasis in Free China: Part 4. Incidence in NativeChinese of Matsu Archipelago,” FJMA no. 3(1957): 137-145.33Public Health Department ed., The Prevention of Filariasis , p. 22

8
In addition, figure six also marks the ecological distribution of major mosquitovectors in Taiwan. The interaction between mosquito living environmental andenvironmental changes after human exploitation eventually altered the infection offilariasis (Wuchereria Bancrofti vs. Brugia malayi) and malaria in Taiwan.
Table 2. Filarial infection and residential living styles in Zhejiang, Fukien,Kinmen, Mazu, Taiwan, and Penghu
(Data from the investigations in the 1950s)Type of Filaria
Areas Infectious rateW.B. B.M.
Major residentialliving styles
Zhejiang 8.92% + +Fishery, rice (paddy& dry)
Dacheng 6.75% + + Fishery
13.18% + +Fishery, rice (paddy& dry)
Fukien Kinmen 19.11% + -Fishery, small-scaledry field
Mazu 11.62% + - FisheryCostal Taiwan 1.50% + - Fishery, rice (paddy)
Yunlin Less than 0.01% + - Fishery, rice (paddy)Jiayi Less than 0.01% + - Fishery, rice (paddy)Tainan 4.80% + - Fishery, rice (paddy)Gaoxiong 4.25% + - Fishery, rice (paddy)Penghu 14.85% + - fishery
Note: Shadow area means the areas were currently the control of the Nationalistgovernment.
Only local examined cases were recorded in + (positive) or – (negative).Major residential living styles only reliable to indicated examined areas.
Resources: Fan P.C. and James Hsu, “Filariasis in Free China: Part 7. Incidenceamong the Military in Taiwan, Penghu (Pescadores) and Kinmen (Quemoy),”
Chinese Medical Journal 5:1(1958): 29-31.
(Chinese Army Medical
Selected Paper) (1974) 207

9
Malaria in Taiwan
Malaria is endemic in Taiwan, which had different name over time. In the latenineteenth century Taiwan, missionary doctor George Mackay believed lethal“danshui fever” was a kind of “malaria”, caused by poisonous vapor from nearby river.
34 After the Japanese occupation, translation of western “malaria” to Japanese-tone
“mararia ( or )” implied the western influence to Japanese
malariology. Even after the anti-malaria program was enforced in the 1910, the
morbidity rate of malaria in Taiwan between 1911 and 1944 remained around 2-3%.35
In order to demonstrate the capability of managing a colony, Japanese experts had tolearn modern malariology from the west and effectively applied to Taiwan. Someanti-malaria strategies were introduced to Taiwan soon after entomologists discovered
the existence of anopheles.36 A pioneer anti-malaria program was first launch in
Beitou, a mountainous area in Taipei. Based on the experiment in Beitou, a morecomprehensive anti-malaria program began in 1913 and caused the morbidity rate ofmalaria steadily dropped to the forth of top-ten causes of death in 1923 as well the lastone in 1941. Between 1913 and 1941, environmental control of mosquito and quinineprophylaxis (Koch method) had been two major preventive policies in Japaneseanti-malaria program. Ku Ya-wen’s study indicates that core concept of anti-malariacampaign had switched from quinine prophylaxis to environmental control(anti-mosquito) after 1919. However, untrained local officials and preventive teammembers often caused misjudgment and ineffectiveness of enforcing anti-malariastrategy. Indigenous resistance and the skepticism to anti-mosquito policy in the Westinfluenced the colonial government again changed the key tone of its campaign toquinine prophylaxis in the late-1920s.37 Ku’s study points an important theme thatgaps existed between the development of local malariology and it application to thecampaign.
34 George Mackay, From Far Formosa: The Island, Its People and Missions (New York: F. H. Revellcompany, 1896), pp. 308-314.35 ( 1953) 198-20036 2 9 (1903)
31-35 (
) 2 10 (1903) 35-3937 — 11 2 (2004)
185-222

10
Compared to the slow development of malarial treatment and environmentalengineering, Japanese malariologists paid more attention to anophelesentomology.38As early as in 1903, based on the collection of mosquitoes in northern
Taiwan by and , published a series of observation data
about (literally, biting-meat mosquitoes) on (Formosan
Journal of Medical Association). However, he did not identify the anopheles from the
category of in these reports.39 In 1904, first used Anopheles (
) to name several kinds of biting-meat mosquitoes, which he found in
Beituo area.40Obviously, without an illustrated handbook from western counterpart,Japanese malariologists did not have enough confidence to identify the anopheles
from a traditional category “ ” in this period.
Mainly because of ’s efforts and investigations in the first quarter
years of the twentieth century, the name “ ” was abandoned and totally
replaced by Anopheles ( ).41 Followed the western learning about
anopheles, Japanese malariologists first identified Anophele sinensis should be one
of the major vectors in Taiwan.42 began to suspect other anopheles in Taiwan
would also transmit malaria in 1917.43 Later in 1920, in his book
38
9 89 (1910) 239 2 8 (1903) 43
2 10 (1903) 6-11 (
) 2 11 (1903) 18-30 ( )
2 12 (1903) 12-1840 3 17 (1904) 3941 ( 1976) 8442 Takagi Tomoeda, Die hygienischen Verhältnisse der Insel FORMOSA (Dresden: Druckt von C.C.Meinhold & Söhne, Kgl. Hofbuchdruckerei, 1911), p. 141.43 16 178 (1917) 497-499

11
(The study of preventive medicine about mosquitoes in
Taiwan), announced Anophele minimus a “possible” new specie of
anopheles and one of the vectors of malaria in Taiwan. In this book,
seemed very worried the strong capability of malarial transmission by An.
minimus.44 In the following years (1917-26), found the distribution ratio
between An. sinensis and An. minimus in Taipei city was around 1:3, but changed
seasonally. In this 1926 article, with great confidence, classified An.
minimus a new specie and separate from the old category Anophele listoni.45As lateas in the 1920s, An. sinensis and An. minimus had been identified and recognizedtwo major vectors of malaria in Taiwan. Based on these entomological achievements,
in 1933 could plot a fine map about the distribution of various anopheles:
malaria cases in Taiwan had 69.2% been transmitted by An. minimus and 20.8% by
An. sinensis. Despite more mosquitoes species were discovered until 1943,46
and his colleagues already brought an important entomological foundation in the1930s for the prevention afterward.
As Ku Yawen has pointed, the main strategy of anti-malaria program in colonialTaiwan had been shaking over time. For example, between the 1910s and early 30s,Japanese malariologists intended to eradicate An. sinensis as their major target.Environmental control was their major weapon to deal with the anopheles. Expertsimported guppy fish from Hawaii and fostered in irrigation systems or creeks,47 aswell the capture capability of bats.48 Except the biological methods above, efforts had
44 ( 1920) 87-9245 nophheles Sinensis W.
25 256 (1926) 631-67246 36 393 (1937)
2800-2801 Omori, N. and Noda H., “On an anopheline mosequito, Anopheles arbumbrosus,newly found in Taiwan (in Japanese, with English summary), Studia medica Tropicalis (Formosa), no.1(1943): 83-89.47 17 188 (1918) 724-72548 Pipistrellus abramus.
29 301 (1930) 348-367
12
been inputted into the studies to alter the water temperature, light, color and PHvalues of anopheles habitat.49However due to the financial burden, environmentalcontrol was merely applied to limited areas. Because of the policy to open upTaiwanese highland, Taiwanese colonial government heavily relied on quinineprophylaxis before the 1930s.
The colonial policy to manage forests and highland in Taiwan started from theland survey between 1910 and 1914, which laid a legal foundation to introduceJapanese companies to open up Taiwanese forest.50Before the mosquito-borne theoryof modern malariology had been carefully studied in Taiwan, quinine prophylaxisalready used in 1907 at a camphor forest in Jiaxianpu, a remote mountainous area in
southern Taiwan.51The first anti-malaria program by Takagi Tomoeda ( )
after 1910, kept the core concept of quinine prophylaxis and the experience ofJiaxianpu experiment.52Following the large-scale exploitation in Taiwan’s highlandand migration weave to eastern Taiwan, blood-screen stations, an importantmechanism to identify target population, established upward to many timber landsand immigrant villages in eastern Taiwan.53While blood-screen stations intensivelybuilt in the quinine prophylaxis-applied areas, most of Japanese owned lands,environmental control was still the main anti-anopheles tool in indigenous residence.When the Great Jianan Irrigation System and Wushantou Dam were constructed onwestern plain in 1928, various tool of environmental control such as kerosene, Parisgreen, and water-level changing engineering, had been applied. Among all thetechniques of environmental control, the number of blood-screen station rapidlyincreased not only for the need of quinine prophylaxis but also set as scientificstation to collect data.54After the 1930s, blood-screen station was in charge ofidentifying target population as well collecting blood sample for malarial studies for
49
24 244 (1925) 623-649
26 263 (1927) 248-25050
11 2 (2004) 76-851 Takagi Tomoeda, Die hygienischen Verhaltnisse der Insel FORMOSA (Dersden: Druck von C.C.Meinhold & Söhne, Kgl. Hofbuchdruckerel, 1911), p. 153.52 192 (1913)53 212 (1931) 20-2854 All.
Quininization 30 316 (1931) 711-734

13
laboratorists The number of the station and blood samples increased dramaticallyafter the 1930s (table 3), providing pathological information about plasmodium.55
Table 3. Increase of blood-screen station and samples between 1910 and 1941
Year Blood-screen station Examined case(A) Positive (B) Ratio (B/A)(%)
1910 no record 6,946 95 1.371911 12 101,064 4,311 4.271912 no record 218,868 2,786 2.641913 no record 269,999 6,366 2.361914 no record 286,334 6,553 2.291915 no record 218,361 8,389 3.841916 no record 354,299 11,888 3.361917 44 690,369 20,821 3.021918 58 942,605 20,073 2.131919 75 1,120,535 27,404 2.451920 68 1,032,336 20,270 1.961921 75 1,103,563 21,460 1.941922 78 1,210,432 30,278 2.001923 89 1,293,176 32,368 2.501924 117 1,636,439 47,232 2.891925 no record 1,732,182 42,528 2.461926 111 1,749,202 37,256 2.121927 117 1,927,826 36,523 1.891928 127 2,024,786 37,217 1.831929 132 2,188,089 38,504 1.761930 146 2,300,900 33,644 1.461931 155 2,370,553 44,329 1.881932 no record 2,430,740 67,265 2.771933 no record 2,470,950 72,092 2.921934 164 2,618,670 72,272 2.621935 no record 2,578,930 78,698 3.051936 186 2,771,631 83,989 3.031937 no record 2,811,822 85,575 3.041938 no record 3,214,736 106,167 3.30
55 Liu Shiyung, “Grafting Modern Public Health Measures in Colonial Taiwan: A Case Study of anAnti-Malaria Program,” paper delivered to
2004/11 7-10

14
1939 no record 3,459,364 116,822 3.381940 no record 3,595,122 98,047 2.731941 180 3,659,154 105,430 2.88
( 1935)
8-9
( 1972) 299b
The boom of blood-screen station was the result of the construction in timberland, immigrant villages in eastern Taiwan, and exploitation on western plain.Information accumulated from blood-screen stations indicates the malaria casesdropped after the exploitation on western plain in the 1930s while the casescomparatively increased in timber land and eastern immigrant villages (maps 7 and8). 56 Compared to filarial study in colonial Taiwan, malaria-related researchobviously attracted more attention and reached better results. Differed from theacademic declaration by the Japanese, indigenous people had equally kept theirexperience of infection by malaria and filaria, which roughly matched the distributionof each mosquito vector and reflected the lifestyle in colonial period.
Filaria and malaria in indigenous memory, lifestyle, and exploitation
Researchers of diseases history usually ask questions like: why, where, or whatdiseases occurred.57However, a more useful attitude to explore filaria and malaria inTaiwan would be the study of their absence and eradication. Culex is prevalent inTaiwan while anopheles would exist only in some geographic condition. Obviouslythe existence of vector could not be the answer for the differential morbidity ratesbetween filariasis and malaria in Taiwan. Meanwhile, An. sinensis transmits malariaon plain but seems has no similar capacity to spread Brugia malayi. Even the samevector of both parasites would only carry plasmodium rather than filarial in Taiwan?A very common explanation for these questions was the long distance betweenTaiwan and Mainland China. The average width of Taiwan Strait is about 200kilometer, blocked the migration of people and diseases in Taiwan from China.However, the outbreak of plague and cholera before the 1910s and minus cases of
56 Liu Shiyung, “GIS, Malaria and Highland Environment in Colonial Taiwan,” paper delivered to TheSecond International Workshop of Colonial Medicine 2000/10
57 Gosgen, R.G., Dunbar, R.I.M. et al., “Evolutionary interpretation of the diversity of reproductivehealth and disease,” in Stephen Stearns ed., Evolution in Health and Disease. (Oxford University Press,Oxford, 1999), pp. 108-109.

15
typhoid in 1930s indicated that Taiwan was continuously under the thread ofinfectious diseases from costal China.58 Another case would retort the commonhypothesis above. In the 1950s, the Nationalist government retreated to Taiwan.Chinese refugee in two islands outside of Fukein, Quemoy and Matsu had highinfectious rate of Wuchereria bancrofti but no sign of Brugia malayi.59 Meanwhile,Dachen refugees from Zhejiangthe cost carried Brugia malayi but had no localtransmission or relapsing local cases when they moved to Taiwan in the early 1960s.60
Cases above imply the geographic block could not be the only factor to explain whyTaiwan has rare cases of Wuchereria bancrofti and no infection of Brugia malayi.
For Table 1, An. sinensis would be the vector of both Brugia malayi andplasmodium. However this anopheles did not transmit Brugia malayi before and after1945 while it really carried malaria on Taiwan’s plain before the 1960s. No wonder,the Public Health Department of Taiwan Provincial Government reported “Brugiamalayi rarely relapse in a new place (Taiwan).”61 The reduction of An. sinensispopulation in western plain since the colonial period would be essential to explainwhy Taiwan has no local case of Brugia malayi. This hypothesis would also good toexplain the situation of Quemoy and Matsu. According to Hsu Yubo’s investigation,Quemoy suffered high morbidity rate of filariasis of Wuchereria bancrofti and had themosquito population of 56-88% Culex as well only 6% An. sinensis.62The morbidityrate of filariasis in Matsu and Penghu islands were even lower as the proportion of An.sinensis dropped to 0.8% and less.63 Without case of Brugia malayi on the islandsurrounding Taiwan and much lower An. sinensis population after the 1950s, westernTaiwan should free from the tread of filarisis by Brugia malayi.
Taiwan had no local case of Brugia malayi but Wuchereria bancrofti, because ofPenghu had high morbidity rate of this filariasis. Parasitologist Fan Bingzhendiscovered some isolated fishing villages in the southwestern cost in Taiwan had localfilariasis of Wuchereria bancrofti. The villagers were actually moved from PenghuIsles and kept close relation in fishing and social connection like marriage64 with
58 Takagi Tomoeda, Die hygienischen Verhaltnisse der Insel FORMOSA (Dersden: Druck von C.C.Meinhold & Söhne, Kgl. Hofbuchdruckerel, 1911), p. 101-102, 130-132.59 Fan, P.C., “Filariasis eradication on Kinmen Proper, Kinmen (Quemoy) Island, ROC,” Acta Tropicano. 47(1990): 161-169. Fan P.C. and James Hsu, “Filariasis in Free China: Part 4. Incidence inNative Chinese of Matsu Archipelago,” Chinese Medical Journal no. 3(1957): 137-145.60 Fan P.C. and James Hsu, “Filariasis in Free China: Part 6. Incidence of Filariasis among TachenEvacuees in Northeast Taiwan.,” Chinese Medical Journal no. 4(1957): 196-199.61Public Health Department ed., The Prevention of Filariasis , p. 1162Public Health Department ed., The Prevention of Filariasis , p. 1363 Chen, H.H., “Filarial infection among the mosquitoes collected in Pescadors, TAMRI (monthlyreport), no. 31(1955): 8-964 Fan P.C. and James Hsu, “Filariasis in Free China: Part 2. Incidence in Taiwanese Chinese,” Chinese

16
their home island.65The fisherman would be infected in Penghu and brought theparasite back to Taiwan. The success of environmental control66 and anti-malariacampaign since the 1920s67reduced the mosquito population including Culex inTaiwan. In addition, the remote and isolated location of these infected villagesreduced the possibility of the transmission from villages to outsiders. 68 Bothsituation kept the local filariasis within a very limited areas and had been neglectedfrom years. Map 5 shows the location of filariasis cases in Taiwan, revealing thedifficulty to discover their existence without strong motive.
To the motive, unlike malaria, filariasis was not so important for Japaneseexperts to attract international attention.69 In addition, no motive for the colonialgovernment to conduct a overwhelming filariasis survey in these poor fishing
locations. ’s investigation in Penghu in the1930s actually revealed the
military needs in colonial government. Isolated fishing villages in costal Taiwan hadno luck to attract governmental attention to organize such survey. Therefore, surveysin Taiwan were done in limited base and without sufficient cases. With no solid
study result in hands, no wonder rejected Mexwell’s report and claimed no
local cases of filariasis in Taiwan but only imported cases form Japan. 70 Toacademic circles in colonial Taiwan, filariasis did not exist. However, to the people
suffered, they kept the vivid memory in various stories. A Chinese novel
(Husband has no testicles) describes elephantiasis patients and their conflict withdoctor from the cities. The suffering villagers took the cases in colonial periods,argued with doctors from Taipei city to keep their testicles, a traditional simple ofbeing a man.71 Before the preventive medicine of filariasis (Diethylcarbamazine)
Medical Journal 2:3&4 (1955): 161.65Fan Pingzhen, “ The review of filariasis study: focusing on the eradication in Quemoy”, Special Issueof Parasitology of National Yang-min Medical College (1982): 17666Public Health Department ed., The Prevention of Filariasis , p. 4967 ( 1935) 49-5568 1910
12 (1910 6 ) 73-7469 12 8(1962) 3670Fan Pingzhen, “ The review of filariasis study: focusing on the eradication in Quemoy”, Special Issueof Parasitology of National Yang-min Medical College (1982): 13771 Wang Xiangqi, Husband has no testicles (Taiepi: Lianjin, 1990).

17
was introduced, similar rumors were circulated. Without idea of modern filariasis,fishermen believed diseases like elephantiasis and rheumarthritis, caused by
“continuously exposed to humid and salty sea wind.”72Under the same working
condition, salt workers shared the same concept with the fisherman, declared they
“cannot avoid the tread of elephantiasis and rheumatism due to the working
condition under the strong sea wind.”73 The sea wind”etiology of elephantiasis not
only reflects the ignorance of the sufferers, but also implies the filarisis should causeproblem for years. To malaria, indigenous Taiwanese seemed clearly knew theanopheles theory and plasmodium pathogen since the 1920s.
No matter western miasma theory or Chinese zhangqi etiology, both wererapidly replaced by modern malriology after the 1910s due to the Japaneseanti-malaria program. Malariology in colonial Taiwan was not only an advanceknowledge to support Japanese efforts to eradicate malaria, but also a platform forJapanese malariologists to gain international recognition as well the confidence ofcolonized society.74 Despite the controversies of Japanese anti-malaria strategies,after the extension of anti-malaria program in the 1920s and 30s, the Taiwaneseseemed to trust in malariology and willingly followed preventive rules. As A-nan(male, 72 years old) described, “In school,…we had routine blood test and physicalexamination every semester,… at home, the sanitary policeman was rigid inenvironmental cleanness and clearing…. From newspaper, I learned a lot ofknowledge about malaria and…, when I was infected, I believed the doctor wouldgive me proper medicine.”75 The academic malariology after the application in the1920s eventually had its institutional and media channels to education the colonizedsociety. The popularized facets of malarialolgy at least rooted in a generation ofTaiwanese like A-nan, who was a school boy in the mid-1930s.
Concluding remarks
The interaction among human being, mosquitoes, and parasites in naturalenvironment is highly complex. This article revealed the tangle and limit of
72 Chen, male, born in 1938, a former salt worker at Tainan Salt Factory. Interviewd in March, 25,2005.73 Li, female, borin around 1942, a wife of the owner of a drugstore in Tainan. Interviewed in March,25, 2005.74 ( 1976) 875 Interview with A-nan (fake name) in Baiho, Tainan county on the 27th of July, 2002. A-nan was born
in 1929 and became a member of local DDT spraying team in the 1956.

18
environmentalist, parasitological, and entomological explanations to the spread offilariasis and malaria in Taiwanese history. No single factor (mosquito, environment,and parasites) would determine the risk of outbreak. To the distribution of vectors,culex should bring more filariasis cases than anopheles to malaria in Taiwan. Thereality was totally opposite. Despite of much bigger population of culex in Taiwan,the mosquito did not have chance to carry the parasite from isolated fishing villages.In addition, only An. sinensis would mainly transmit Brugia malayi and plasmodiumon western plain in Taiwan. However, the morbidity rate of malaria on Taiwan’s plaindeclined after the 1920s and reducing An. sinensis population seemed never carriedthe filaria of Brugia malayi. The construction of Jianan Irrigation System and thefollowing extension of anti-malaria program could alter the ecological environment ofAn. sinensis’s survival.
Preliminarily reviewed the disease history of filariasis and malaria, the authorwould briefly conclude following points. First, the discovery or existence of certaindisease to academic circles would be determined by various non-medical motives. Incolonial Taiwan, military needs and economic exploitation could be two importantmotives. Secondly, to the economic condition, filariasis in colonial Taiwan waslooked like an infectious disease of fishing villages while malaria was islandwide.Moreover, compare to the moving situation of malaria cases after the 1930s, plainmalaria by An. sinensis rapidly reduced as the mountainous malaria by An. minimusdecreased comparatively slower. Finally, inner migration within Taiwan could be notsignificant during the colonial period. Slow movement of indigenous population couldbe the reason why the filariasis cases were limited in costal fishing villages and can beexplained by villager’s social or economic behavior pattern. With the similarconsideration, the moving of timber workers created clear routes of malaria infectionfrom plain to forests after the late-1920s. When weaves of urban refugees ran tomountainous areas to avoid the booming after 1943, they might be infected by bitingof An. minimus and brought the “old” malaria back to the cities on western plain afterthe 1945.
19
Appendix
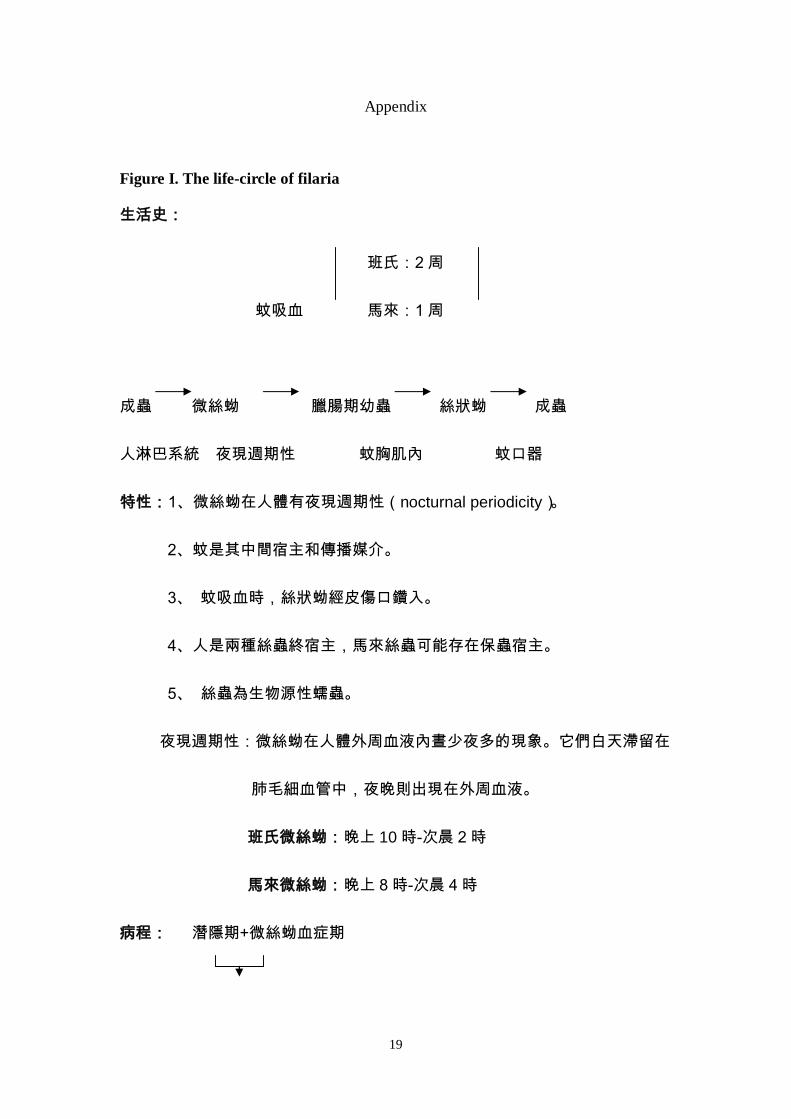
Figure I. The life-circle of filaria
nocturnal periodicity
10

20
1
2
Panicker, K.N. and Dhanda, V., “Community participation in the control of
filariasis,” World Health Forum 3:2&3 (1992):179-80.
21
Figure2. Anopheles
Figure3. Culex

22
Map 4. The investigation areas of Yokogawa team in 1939
415 (1939) 1461

23
Map5. Distribution of filariasis on the southwestern cost in the 1960s Taiwan
Fan Pingzhen, “ The review of filariasis study: focusing on the eradication
in Quemoy”, Special Issue of Parasitology of National Yang-min MedicalCollege (1982): 135. Wu Y.T.,, Tseng P.T. and Chen, C.T., “Recent advances in
the studies of filariasis and its control in Taiwan,” (1963) 1

24
Map 6. Distribution of filariasis in China and Taiwan
Fan P.C. and James Hsu, “Filariasis in Free China: Part 7. Incidence
among the Military in Taiwan, Penghu (Pescadores) and Kinmen (Quemoy),”
Chinese Medical Journal 5:1(1958): 29-31.
(Chinese Army Medical
Selected Paper) (1974) 207 Fan Pingzhen, “The review of
filariasis study: focusing on the eradication in Quemoy”, Special Issue ofParasitology of National Yang-min Medical College (1982): 135.

25
Map 7. Distribution of malaria in China and Taiwan
http://whqlibdoc.who.int/publications/2005/9241580364_chap7.pdf

26
Map 8. Distribution of malarial cases in 1918 Taiwan

27
( 1927)
Map 9. Distribution of malarial cases in1924 Taiwan
1920

28
(900-1,200 )
( 1927)