fibrate safety & metabolism - lipidcenter · fibrate/statin risk of rhabdomyolysis gemfibrozil...
TRANSCRIPT

Thomas Dayspring, MD, FACPThomas Dayspring, MD, FACPClinical Assistant Professor of MedicineClinical Assistant Professor of Medicine
University of Medicine and Dentistry of New Jersey University of Medicine and Dentistry of New Jersey New Jersey Medical SchoolNew Jersey Medical School
Attending in Medicine: St JosephAttending in Medicine: St Joseph’’s Regional Medical Center, s Regional Medical Center, Paterson and Wayne, NJPaterson and Wayne, NJ
Certified Menopause Practitioner: Certified Menopause Practitioner: North American Menopause SocietyNorth American Menopause Society
North Jersey Institute of Menopausal Lipidology North Jersey Institute of Menopausal Lipidology Wayne, New JerseyWayne, New Jersey
Fibrate Safety & Metabolism Fibrate Safety & Metabolism

FDA Indications for TriCorFDA Indications for TriCor
TriCor is indicated as adjunctive TriCor is indicated as adjunctive therapy to diet to therapy to diet to reducereduce elevated elevated
LDLLDL--CC, , Total cholesterolTotal cholesterol, , Triglycerides Triglycerides and and Apo BApo B, and to , and to increaseincrease HDLHDL--CC in adult patients in adult patients with primary hypercholesterolemia with primary hypercholesterolemia
or mixed dyslipidemiaor mixed dyslipidemia

TriCor (fenofibrate) TabletsTriCor (fenofibrate) TabletsContraindicatedContraindicated in those with a in those with a hypersensitivity to fenofibrate, hepatic or hypersensitivity to fenofibrate, hepatic or severe renal dysfunction and presevere renal dysfunction and pre--existing GB existing GB disease.disease.Is associated with rises in aminases: periodic Is associated with rises in aminases: periodic LFT monitoring is requiredLFT monitoring is requiredMay lead to cholelithiasis: if confirmed TriCor May lead to cholelithiasis: if confirmed TriCor should be discontinuedshould be discontinuedMay May increase effectsincrease effects of of coumadincoumadin

Fibrate Chemical StructuresFibrate Chemical Structures
Cl C
O
O
CH3
CH3
C COO CH
CH3
CH3
Cl O C COOC2H5
CH3
CH3
C COOH
CH3
CH3
CH2O CH2 CH2 CH2
CH3
Fenofibrate
Clofibrate
CH3Gemfibrozil

FDA Indications for TriCorFDA Indications for TriCor
Phenotype OccurrenceLipoprotein Present in
ExcessChol Trig
III Rare VLDL remnants 375-500 600600--800800IV Common VLDL 225-275 375375--500500
VLDL
I Rare Chylomicrons 250-400 >2500>2500
V Rare Chylomicrons, 350-400 17001700--25002500
TriCor is indicated in IIA, IIB, IV, VTriCor is indicated in IIA, IIB, IV, V
IIB Most common LDL,VLDL >250 150150--400400IIA Common LDL >250 <150

DrugDrug--Drug Interactions Drug Interactions Statins/FibratesStatins/Fibrates
CombinedCombined use of use of fibrates and statinsfibrates and statins has has been associated with rhabdomyolysis, been associated with rhabdomyolysis, markedly elevated creatine kinase levels, markedly elevated creatine kinase levels, and myoglobinuriaand myoglobinuria
Fenofibrate prescribing information, Abbott Laboratories, 1998.
The The combined usecombined use of fenofibrate and statins of fenofibrate and statins should be avoidedshould be avoided unlessunless the benefit the benefit of further of further alterations in lipid levels is likely to outweigh alterations in lipid levels is likely to outweigh the increased risk of this drug combinationthe increased risk of this drug combination
unlessunless

Well absorbed from GI tractWell absorbed from GI tractPeak plasma levels within 6Peak plasma levels within 6--8 hours8 hoursExcreted mainly in the urineExcreted mainly in the urineHalfHalf--life of 20 hourslife of 20 hoursIn vivoIn vivo data indicate that data indicate that neither neither fenofibrate nor fenofibric acid fenofibrate nor fenofibric acid undergoes oxidative metabolism (eg, undergoes oxidative metabolism (eg, cytochrome P450) to a significant cytochrome P450) to a significant extentextent
Fenofibrate PharmacokineticsFenofibrate Pharmacokinetics
Fenofibrate prescribing information, Abbott Laboratories, 1998.

DrugDrug--Drug InteractionsDrug Interactions
Potentiation of coumarinPotentiation of coumarin--type type anticoagulants has been observed, with anticoagulants has been observed, with prolongation of the INRprolongation of the INR
•• Caution should be exercised when Caution should be exercised when coumarin anticoagulants are given in coumarin anticoagulants are given in conjunction with TriCorconjunction with TriCor
Fenofibrate should be taken at least 1 Fenofibrate should be taken at least 1 hour before, or 4hour before, or 4--6 hours after, taking a 6 hours after, taking a bile acidbile acid-- binding resin, to avoid binding resin, to avoid impeding its absorptionimpeding its absorption
Fenofibrate prescribing information, Abbott Laboratories, 1998.

In vivoIn vivo data indicate that data indicate that neither neither fenofibrate nor fenofibric acid fenofibrate nor fenofibric acid undergoes oxidative metabolism undergoes oxidative metabolism (eg, cytochrome P450) to a (eg, cytochrome P450) to a significant extent. significant extent.
Fenofibrate PharmacokineticsFenofibrate Pharmacokinetics
Fenofibrate prescribing information, Abbott Laboratories, 2003.

FDA Package Insert for FenofibrateFDA Package Insert for Fenofibrate
In a In a singlesingle--dose drug interaction studydose drug interaction study in 23 in 23 healthy adults the healthy adults the concomitant administration concomitant administration
of TriCor and pravastatinof TriCor and pravastatin resulted in resulted in no clinically no clinically important difference in the pharmacokineticsimportant difference in the pharmacokinetics of of
fenofibric acid, pravastatin or its active fenofibric acid, pravastatin or its active metabolites, 3ametabolites, 3a--hydroxy hydroxy isoiso--pravastatin when pravastatin when
compared to either drug given alonecompared to either drug given alone

Pan W-J, et al. J Clin Pharmacol . 2000;40:316-323.
Pra
vast
atin
Pla
sma
Pra
vast
atin
Pla
sma
Con
cent
ratio
n, n
g/m
LC
once
ntra
tion,
ng/
mL
Three 67-mg fenofibrate capsules + one 40-mg pravastatin tabletOne 40-mg pravastatin tablet
100
Time (hours)Time (hours)
10
1
.1
00 5 10 15
Fenofibrate Does not Increase Fenofibrate Does not Increase Pravastatin Plasma ConcentrationsPravastatin Plasma Concentrations

Simvastatin Product Information SheetSimvastatin Product Information SheetThe use of simvastatin The use of simvastatin shouldshould not exceed 10 mgnot exceed 10 mgdaily in patients receiving concomitant gemfibrozil. daily in patients receiving concomitant gemfibrozil. The combined use of simvastatin and gemfibrozil The combined use of simvastatin and gemfibrozil should be avoided unless benefits are likely to should be avoided unless benefits are likely to outweigh the risksoutweigh the risksCaution should be usedCaution should be used when prescribing when prescribing simvastatin with other lipid lowering drugs (fibrates simvastatin with other lipid lowering drugs (fibrates or > 1gm niacin)or > 1gm niacin)The benefits of further alterations in lipids with The benefits of further alterations in lipids with combined use of fibrates and niacin should be combined use of fibrates and niacin should be weighed carefully against the potential risk of these weighed carefully against the potential risk of these combinationscombinations

Effects of HighEffects of High--Dose StatinsDose StatinsAtorvastatinAtorvastatin LovastatinLovastatin SimvastatinSimvastatin
10 mg10 mg 20 mg 40 mg 80 mg20 mg 40 mg 80 mg 20 mg20 mg 40 mg 80 mg40 mg 80 mg 20 mg20 mg 40 mg 80 mg40 mg 80 mg0
-10
-20
-30
-40
-50
-602.5
2.0
1.5
1.0
0.5
0.0Elev
ated
El
evat
ed L
FTs
LFTs
(% o
f (%
of
Patie
nts)
Patie
nts)
Dec
reas
e in
LD
LD
ecre
ase
in L
DL --
CC
Davidson MH. Am J Cardiol. 2002;90(suppl):50K-60K.
Additional LDLAdditional LDL--C lowering benefit of highC lowering benefit of high--dose statins may be dose statins may be outweighed by the outweighed by the LFTsLFTs and increased risk of myositis.and increased risk of myositis.
10 mg10 mg 20 mg 40 mg 80 mg20 mg 40 mg 80 mg 20 mg20 mg 40 mg 80 mg40 mg 80 mg 20 mg20 mg 40 mg 80 mg40 mg 80 mg

Glucuronidation: Explanation of Glucuronidation: Explanation of Fibrate/Statin InteractionFibrate/Statin Interaction
““GlucuronidationGlucuronidation is a pathway for the elimination of is a pathway for the elimination of the active hydroxy acid metabolites of simvastatin, the active hydroxy acid metabolites of simvastatin, atorvastatin, and cerivastatinatorvastatin, and cerivastatin””““The most recent evidence suggests that The most recent evidence suggests that gemfibrozil inhibits simvastatin, atorvastatin, and, gemfibrozil inhibits simvastatin, atorvastatin, and, more prominently, cerivastatin glucuronidation.more prominently, cerivastatin glucuronidation.””““FenofibratesFenofibrates, however, appear to have a , however, appear to have a significantly less inhibitory effect on statin significantly less inhibitory effect on statin glucuronidationglucuronidation, and this may explain the lack of , and this may explain the lack of significant drug interaction between fenofibrate significant drug interaction between fenofibrate and statins.and statins.””
Davidson MH. Am J Cardiol. 2002;90(suppl):50K-60K.

Glucuronidation: ? Explanation of Glucuronidation: ? Explanation of Fibrate/Statin InteractionFibrate/Statin Interaction
““Glucuronidation is a pathway for the elimination of the Glucuronidation is a pathway for the elimination of the active hydroxy acid metabolites of simvastatin, active hydroxy acid metabolites of simvastatin, atorvastatin, and cerivastatinatorvastatin, and cerivastatin””““Initially, the PK interaction between statins and gemfibrozil Initially, the PK interaction between statins and gemfibrozil was thought to be the result of an interaction with was thought to be the result of an interaction with cytochrome P450 pathways.cytochrome P450 pathways.””““The most recent evidence suggests that The most recent evidence suggests that gemfibrozil gemfibrozil inhibits simvastatin, atorvastatin, and, more prominently, inhibits simvastatin, atorvastatin, and, more prominently, cerivastatin glucuronidation.cerivastatin glucuronidation.””““FenofibratesFenofibrates, however, appear to have a significantly less , however, appear to have a significantly less inhibitory effect on statin glucuronidationinhibitory effect on statin glucuronidation, and this may , and this may explain the lack of significant drug interaction between explain the lack of significant drug interaction between fenofibrate and statins.fenofibrate and statins.””
Davidson MH. Am J Cardiol. 2002;90(suppl):50K-60K.

““Further studies conducted in human liver microsomes with Further studies conducted in human liver microsomes with atorvastatin showed that, as with simvastatin, gemfibrozil atorvastatin showed that, as with simvastatin, gemfibrozil was a less potent inhibitor of the CYP3A4was a less potent inhibitor of the CYP3A4--mediated mediated oxidation of this drug oxidation of this drug than its glucuronidationthan its glucuronidation..””““However, with cerivastatin, the glucuronidation However, with cerivastatin, the glucuronidation as well asas well asthe CYP2C8the CYP2C8-- and CYP3A4and CYP3A4--mediated oxidation pathways mediated oxidation pathways were much more susceptible to inhibition by gemfibrozil were much more susceptible to inhibition by gemfibrozil than was observed with simvastatin or atorvastatin.than was observed with simvastatin or atorvastatin.””““Collectively, the results of these studies provide metabolic Collectively, the results of these studies provide metabolic insight into the nature of druginsight into the nature of drug--drug interaction between drug interaction between gemfibrozil and statins, and a possible explanation for the gemfibrozil and statins, and a possible explanation for the enhanced susceptibility of cerivastatin to interactions with enhanced susceptibility of cerivastatin to interactions with gemfibrozilgemfibrozil..””
Prueksaritanont T, et al. JPET. 301:1042-1051, 2002.
Gemfibrozil Interacts with Statin Gemfibrozil Interacts with Statin GlucuronidationGlucuronidation

Gemfibrozil Increases Simvastatin Gemfibrozil Increases Simvastatin Plasma ConcentrationsPlasma Concentrations
Backman JT, et al. Clin Pharmacol Ther. 2000;68:122-129.
Sim
vast
atin
Aci
d, n
g/m
LS
imva
stat
in A
cid,
ng/
mL
Time, hTime, h
GemfibrozilPlacebo
8
6
0 1
4
2
02 3 4 6 8 10 12

Gemfibrozil Increases Cerivastatin Gemfibrozil Increases Cerivastatin Plasma ConcentrationsPlasma Concentrations
10
8
6
4
2
00 2 4 6 8 10 12 24
Time, hoursTime, hours
Cer
ivas
tatin
(Aci
d) n
g/m
LC
eriv
asta
tin (A
cid)
ng/
mL
+ Gemfibrozil+ Gemfibrozil
+ Placebo
Backman JT, et al. Clin Pharmacol Ther. 2002;72:685-691.

Kyrklund C, et al. Clin Pharmacol Ther. 2001;69:340-345.
Lova
stat
in A
cid,
ng/
mL
Lova
stat
in A
cid,
ng/
mL
Time, hTime, h
GemfibrozilPlaceboBezafibrate
8
6
4
2
00 2 4 6 8 10 12
Gemfibrozil, but not Bezafibrate, Increases Gemfibrozil, but not Bezafibrate, Increases Lovastatin Plasma ConcentrationsLovastatin Plasma Concentrations

Glucuronidation of Fibrates Glucuronidation of Fibrates Gemfibrozil and FenofibrateGemfibrozil and Fenofibrate
Glu
curo
nide
For
mat
ion,
G
lucu
roni
de F
orm
atio
n,
pmo/
min
/mg
pmo/
min
/mg
30002500200015001000500
50
0
HLM 1A1 1A3 1A10 1A9 2B7 2B15
GemfibrozilGemfibrozilFenofibrateFenofibrate
Prueksaritanont T, et al. Drug Metab Dispos. 2002;30:1280-128
Statins utilize UGT 1A1 and 1A3 for metabolismStatins utilize UGT 1A1 and 1A3 for metabolism
Gemfibrozil competitively Gemfibrozil competitively competes with statins for competes with statins for UGT 1A1 and 1A3 UGT 1A1 and 1A3
Fenofibrate primarily Fenofibrate primarily utilizes UGT 1A9 and utilizes UGT 1A9 and 2B7 for metabolism2B7 for metabolism
UGT = UDP Glucuronyl transferaseUGT = UDP Glucuronyl transferase

Effect on Glucuronidation of Statin Hydroxy Effect on Glucuronidation of Statin Hydroxy Acids Acids -- Gemfibrozil Versus FenofibrateGemfibrozil Versus Fenofibrate
InhibitorInhibitor
SubstrateSubstrate Gemfibrozil ICGemfibrozil IC5050* (* (μμM)M) Fenofibrate ICFenofibrate IC5050* (* (μμM)M)
Simvastatin Hydroxy Simvastatin Hydroxy 354354 682682AcidAcid
AtorvastatinAtorvastatin 316316 Not DoneNot Done
CerivastatinCerivastatin 8282 433433
Gemfibrozil CGemfibrozil Cmaxmax†† ((μμM)M) Fenofibrate CFenofibrate Cmax max †† ((μμM)M)
100100--300300 1515--5555§§
Prueksaritanont T, et al. Poster presented at 2002 AHA.
*Obtained following coincubation of fibrates and simvastatin hydroxy acid in human liver microsomes.†Reported values following 600 mg BID gemfibrozil or 200 mg QD fenofibrate in humans.§Measured as fenofibric acid.

Effect on Glucuronidation of Statin Hydroxy Effect on Glucuronidation of Statin Hydroxy Acids Acids -- Gemfibrozil Versus FenofibrateGemfibrozil Versus Fenofibrate
Prueksaritanont T, et al. Poster presented at 2002 AHA.
Although glucuronidation of all statins is inhibited by gemfibrozil: simvastatin, atorvastatin, and rosuvastatin appear to be less susceptible than cerivastatinInitial studies indicate the fenofibrate is much lessinhibitory than gemfibrozil on statin glucuronidationFor rosuvastatin, the significant effect of gemfibrozil on both glucuronidation and oxidation is similar to cerivastatin, suggestion the potential for a pharmacokinetic interaction between this new statin and gemfibrozil

Lipophilicity Lipophilicity -- HydrophilicityHydrophilicity
SimvastatinSimvastatin
LovastatinLovastatin
FluvastatinFluvastatin
AtorvastatinAtorvastatin
RosuvastatinRosuvastatin
PravastatinPravastatin
Most LipophilicMost Lipophilic
Most HydrophilicMost Hydrophilic
Hydrophilic (low lipophilicity) statins may have greater
accumulation in the liver via selective membrane carriers and decreased accumulation in peripheral tissues through passive diffusion and thus
inhibit greater selective inhibition of liver HMG-CoA
reductase.
J Pharm Sci 1991;80:830-834Trends Pharmacol Sci 1998;19:26-37
Am J Cardiol 2001;97(suppl):28B-32B

Effect of Gemfibrozil and Fenofibrate on Effect of Gemfibrozil and Fenofibrate on Rosuvastatin Plasma ConcentrationsRosuvastatin Plasma Concentrations
00.20.40.60.8
11.21.41.61.8
2
GemfibrozilFenofibrate
GemfibrozilGemfibrozil FenofibrateFenofibrate
1.07
1.90
AU
C ra
tioA
UC
ratio
Ratio of rosuvastatin AUC in fibrateRatio of rosuvastatin AUC in fibrate--treated treated patients to AUC in placebopatients to AUC in placebo-- treated patientstreated patients

0.10.1
11
1010
0 55 1010 1515 2020 2525 3030 3535
Plas
ma
Con
cent
ratio
n (n
g/m
L)Pl
asm
a C
once
ntra
tion
(ng/
mL)
Time (h)Geometric mean (SD) plasma concentrations of rosuvastatin over time on day 7 after dosing of rosuvastatin alone and rosuvastatin in combination with fenofibrate
Rosuvastatin (10 mg QD)Rosuvastatin (10 mg QD)Rosuvastatin (10 mg QD) + Fenofibrate 200 mg (67 mg TID)Rosuvastatin (10 mg QD) + Fenofibrate 200 mg (67 mg TID)
Fenofibrate Does Not Increase Fenofibrate Does Not Increase Rosuvastatin Plasma ConcentrationsRosuvastatin Plasma Concentrations
Martin PD, et al. Clin Ther. 2003;25:459-470.
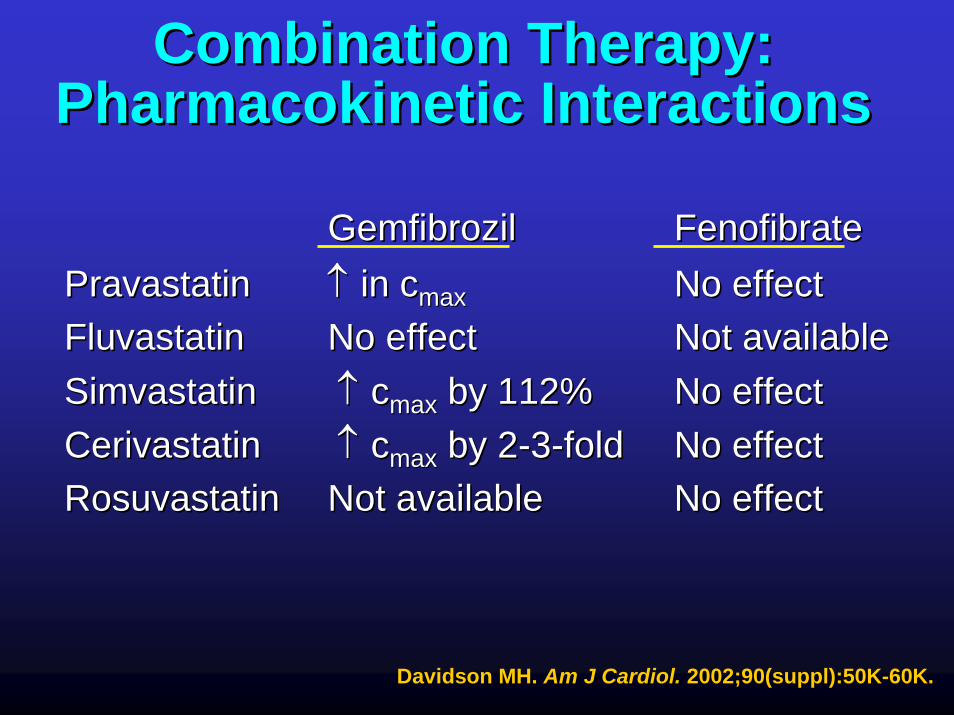
Combination Therapy: Combination Therapy: Pharmacokinetic InteractionsPharmacokinetic Interactions
GemfibrozilGemfibrozil FenofibrateFenofibratePravastatinPravastatin ↑↑ in cin cmaxmax No effectNo effectFluvastatinFluvastatin No effectNo effect Not availableNot availableSimvastatinSimvastatin ↑↑ ccmaxmax by 112%by 112% No effectNo effectCerivastatinCerivastatin ↑↑ ccmaxmax by 2by 2--33--foldfold No effectNo effectRosuvastatinRosuvastatin Not availableNot available No effectNo effect
Davidson MH. Am J Cardiol. 2002;90(suppl):50K-60K.

Statin/Fibrate Combination Therapy: Statin/Fibrate Combination Therapy: Pharmacokinetic InteractionsPharmacokinetic Interactions
Backman JT, et al. Clin Pharmacol Ther. 2002;72:685-691.Abbott Laboratories. Data on file; 2005.
Davidson MH. Am J Cardiol. 2002;90(suppl):50K-60K.Prueksaritanont T, et al. Drug Metab Dispos. 2002;30:1280-1287.
Martin PD, et al. Clin Ther. 2003;25:459-471.Bergman AJ, et al. J Clin Pharmacol. 2004;44:1054-1062.
TriCor [package insert]. Abbott Laboratories;2004.Kyrklund C, et al. Clin Pharmacol Ther. 2001;69:340-345.
Pan W-J, et al. J Clin Pharmacol. 2000;40:316-323.Backman JT, et al. Clin Pharmacol Ther. 2000;68:122-129.
Gemfibrozil FenofibrateAtorvastatin Not available No effectSimvastatin ↑ in Cmax by 2-fold No effectPravastatin ↑ in Cmax by 2-fold No effectRosuvastatin ↑ in Cmax by 2-fold No effectFluvastatin No effect No effect Lovastatin ↑ in Cmax by 2.8-fold No effectCerivastatin ↑ in Cmax by 2-3–fold No effect

LLipids in ipids in DDiabetes iabetes SStudy (tudy (LDSLDS))4,191 diabetic patients without known CHD and 4,191 diabetic patients without known CHD and LDLLDL--C < 160 mg/dL from 30 centers in UKC < 160 mg/dL from 30 centers in UK•• Fenofibrate 200 mg + placeboFenofibrate 200 mg + placebo•• Cerivastatin .4mg + placeboCerivastatin .4mg + placebo•• Cerivastatin.4mg + fenofibrate 200mgCerivastatin.4mg + fenofibrate 200mg•• Placebo + placeboPlacebo + placebo
Began May 1999 and closed August 2001Began May 1999 and closed August 2001Data on 1949Data on 1949 followed for a year have been followed for a year have been analyzedanalyzed•• No myositis or rhabomyolysis casesNo myositis or rhabomyolysis cases
ADA abstract 317 Neil A et al. The Endocrinologist 2003;13(suppl3):S17

Fibrate/Statin Risk of RhabdomyolysisFibrate/Statin Risk of RhabdomyolysisFibrate/Statin Risk of Rhabdomyolysis
Gemfibrozil + Any StatinGemfibrozil + Any Statin 590590 6,757,0006,757,000 87.3287.32Gemfibrozil + Cerivastatin 533 116,000Gemfibrozil + Cerivastatin 533 116,000 4,594.834,594.83Gemfibrozil + Other Statins 57Gemfibrozil + Other Statins 57 6,641,0006,641,000 8.588.58
Number of Cases of RhabdomyolysisNumber of Cases of Rhabdomyolysis
1Adverse Event Reporting System, U.S. Food and Drug Administration.2National Prescription Audit Plus report, IMS Health.
3Concomitancy Report, VERISPAN, LLC.
Fenofibrate + Any StatinFenofibrate + Any Statin 1616 3,519,0003,519,000 4.554.55Fenofibrate + Cerivastatin 14Fenofibrate + Cerivastatin 14 100,000100,000 140.00140.00Fenofibrate + Other Statins 2Fenofibrate + Other Statins 2 3,419,0003,419,000 0.580.58
MedicationMedication # Cases # Cases ReportedReported
# Rx # Rx Dispensed Dispensed 2,32,3
# Cases # Cases Reported per Reported per
Million Million 11

Jones PH & Davidson MH. A J Card 2005;95:120-122
Risk of Rhabdomyolysis Risk of Rhabdomyolysis with Fibrates and Statinswith Fibrates and Statins
1000
1500
2000
2500
3000
3500
4000
4500
5000
500
0
4600
Fenofibrate Gemfibrozil
1400.58
8.6
Fenofibrate Gemfibrozil
2
3
4
5
6
7
8
9
10
1
0No.
Cas
es R
epor
ted
per M
illio
n Pr
escr
iptio
ns
No.
Cas
es R
epor
ted
per M
illio
n Pr
escr
iptio
ns
Number of cases of rhabdomyolysis Number of cases of rhabdomyolysis reported per million prescriptions reported per million prescriptions
dispensed ofdispensed of cerivastatin in combinationcerivastatin in combinationwith fibrates. with fibrates.
Number of cases of rhabdomyolysis Number of cases of rhabdomyolysis reported per million prescriptions reported per million prescriptions
dispensed of dispensed of statins other than statins other than cerivastatincerivastatin in combinationin combination with fibrates. with fibrates.
Fenofibrate resulted in 33times lower
rhabdomyolysis reporting than did gemfibrozil
Fenofibrate resulted in 15 times lower
rhabdomyolysis reporting than did gemfibrozil
vs statins other than cerivastatin vs cerivastatin

Number of Cases of Rhabdomyolysis in Number of Cases of Rhabdomyolysis in Combination Therapy With CerivastatinCombination Therapy With Cerivastatin
Jones PH, et al. Am J Cardiol. 2005;95:120-122.
140
4600
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
Fenofibrate Gemfibrozil
No.
Cas
es R
epor
ted
per M
illio
n Pr
escr
iptio
ns

Number of Cases of Rhabdomyolysis in Number of Cases of Rhabdomyolysis in Combination Therapy With Statins*Combination Therapy With Statins*
0.58
8.6
0
1
2
3
4
5
6
7
8
9
10
Fenofibrate Gemfibrozil
No.
Cas
es R
epor
ted
per M
illio
n Pr
escr
iptio
ns
15-Fold Increase
Jones PH, et al. Am J Cardiol. 2005;95:120-122.*Excludes cases involving cerivastatin

Alsheikh-Ali, A. et al. Amer J Card 2004;59:935-938
Risk of Adverse Events with FibratesRisk of Adverse Events with Fibrates
OR 1.24*OR 2.41*
OR 10.84*
OR 0.95 OR 1.78*
0
20
40
60
80
100
120
0
Any AERs
Major A
ERs
Hepato
toxicity
Myosit
is
Rhabdomyo
sitis
GemfibrozilFenofibrate
AER
s/O
ne M
illio
n R
x
Reviewed adverse events reported to the United States Food and Drug
Administration (FDA)

Alsheikh-Ali, A. et al. Amer J Card 2004;59:935-938
Risk of Adverse Events with FibratesRisk of Adverse Events with Fibrates
Cerivastatin Available
1994 1995 1996 1997 1998 1999 2000 2001 2002
Year
GemfibrozilFenofibrate
AER
s/O
ne M
illio
n R
x
20
40
60
80
100
0
EzetimibeEzetimibe had had no clinically significantno clinically significant effect on effect on the the pharmacokineticspharmacokinetics (e.g. (e.g. absorbtionabsorbtion, , metabolism and excretion) or metabolism and excretion) or pharmacodynamicspharmacodynamics (e.g. binding action of the (e.g. binding action of the drug to certain receptors and consequent effects drug to certain receptors and consequent effects on CNS, GI tract and other CV parameters) of on CNS, GI tract and other CV parameters) of fenofibrate or vice versafenofibrate or vice versa. .
Ezetimibe Ezetimibe -- Fenofibrate Fenofibrate Pharmacokinetic StudyPharmacokinetic Study
www.sch-plough.com/news/2001/research/20010521.html

Ezetimibe Ezetimibe -- Fenofibrate Fenofibrate Pharmacokinetic StudyPharmacokinetic Study
**PP≤≤0.03 vs placebo or either drug.0.03 vs placebo or either drug.
--30%30%
Mean % Mean % Change Change
From From BaselineBaseline
--36%*36%*
--32%32%ZetiaZetia
LDL-C TG (median) HDL-C
TriCorTriCor
0%0%
--20%20%
ComboCombo
PlaceboPlacebo
32 patients with hypercholesterolemia for 14 days: on strict die32 patients with hypercholesterolemia for 14 days: on strict diett

Fenofibrate Fenofibrate –– Ezetimibe Pharmacodynamic Ezetimibe Pharmacodynamic and Pharmacokinetic Interaction Studyand Pharmacokinetic Interaction Study
Kosoglou T et al. Curr Med Res & Opin 2004;20:1185-1195
-40
-30
-20
-10
-50
0
10
20
30
TC LDL-C HDL-C TG
Cha
nge
from
Bas
elin
e (%
)
Placebo (n = 8)Ezetimibe 10 mg (n = 8)Fenofibrate 200 mg (n = 8)Fenofibrate 200mg + Ezetimibe 10 mg (n = 8)
Patients have no physical activity and are on a high carbohydrate low fat diet
which lowers HDL-C
Mean (SE) percentage change from baseline in serum lipids on day 14 following oral administration of fenofibrate monotherapy, ezetimibe monotherapy, fenofibrate-ezetimibe co-
administration therapy or placebo once daily to 14 healthy subjects with hypercholesterolemia

Fenofibrate Fenofibrate –– Ezetimibe Pharmacodynamic Ezetimibe Pharmacodynamic and Pharmacokinetic Interaction Studyand Pharmacokinetic Interaction Study
Kosoglou T et al. Curr Med Res & Opin 2004;20:1185-1195
-40
-30
-20
-10
-50
0
10
20
30
Cha
nge
from
Bas
elin
e (%
)
Placebo (n = 8)Ezetimibe 10 mg (n = 8)Fenofibrate 200 mg (n = 8)Fenofibrate 200mg + Ezetimibe 10 mg (n = 8)
LDL-IIILDL-C LDL-1 LDL-IILarge Intermed Small
Combination therapy produced significantly greater reductions in LDL-C and in small
LDL-III
Levels of apoCIII were also reduced greater
than monotherapy with either drug

Fenofibrate Fenofibrate –– Ezetimibe Pharmacodynamic Ezetimibe Pharmacodynamic and Pharmacokinetic Interaction Studyand Pharmacokinetic Interaction Study
Kosoglou T et al. Curr Med Res & Opin 2004;20:1185-1195
Tota
l Eze
timib
e C
onc
(ng/
ml)
Ezet
imib
e C
onc
(ng/
ml)
0 4 8 12 16 20 24 0 4 8 12 16 20 24Time (hr) Time (hr)
60
80
100
40
20
120
140
160
180
Ezetimibe 10 mg (n = 8)Fenofibrate 200mg + Ezetimibe 10 mg (n = 8)
Ezetimibe 10 mg (n = 8)
Fenofibrate 200mg + Ezetimibe 10 mg (n = 8)
0
1.0
0
1.0
3.0
4.0
5.0
6.0
7.0
8.0
Mean (+SD) plasma concentration-time profiles of total ezetimibe (ezetimibe + ezetimibe glucuronide) and ezetimibe on day 14 following multiple dose, once-daily oral administration of either ezetimibe alone or co-administered with fenofibrate
Concomitant fenofibrate administered as a 200 mg micronized capsule formulation resulted in a significant (~50%) increase in the steady state total ezetimibe exposure. However, this exposure is probably not clinically important. The increased plasma total ezetimibe appear to be due to an
increase in ezetimibe bioavailability rather than inhibition of clearance