femoral acetabular labral tear rehabilitation
TRANSCRIPT

IntroductionThe idea that abnormal hip morphology was a possible cause of hip degeneration and arthritis was initially suggested by Stulberg et al (1975), when they identified the ‘pistol grip deformity’ in the xray findings of abnormal head of femur (HOF) clearance from the acetabulum in patients with hip arthritis (1). This led to the idea that mechanical impingement may be one of the underlying causes of hip degeneration and hip joint pain.
Over the next few decades, with improvements in radiology and hip joint surgery, and more sophisticated clinical assessment skills, it was recognised that a number of atypical hip joint morphologies
commonly existed that may give rise to hip joint pain in athletes.
In the late 1990’s, Mayer et al (1999)(2) were the first to use the term ‘Femoro-acetabular impingement’ or ‘FAI’ to describe the morphology of the hip as being a causative factor in hip joint arthritis, and the concept of FAI was further pioneered by Reinhold Ganz(3) and colleagues during the early 2000s.
An FAI is a genuine complication for an athlete, particularly for young male athletes, as it can not only lead to hip joint pain and labral and cartilage damage, but it can also give rise to other athletic injuries such as osteitis pubis and inguinal hernias due to the detrimental effect that a lack of hip joint
rotation plays on pelvis stress injuries(4). The purpose of this Rehabilitation
Masterclass is to explain the relevant anatomy and biomechanics of the hip joint, explain the pathogenesis of FAI and offer management ideas and an in depth overview of the rehabilitation of the hip joint post-FAI surgery.
Relevant anatomy and biomechanicsThe hip joint is a ball and socket joint that enjoys a wide range of movement into all planes of motion. It can also accommodate a large weight bearing force during locomotion. The ‘normal’ hip morphology is identified as(5);
£17.99 Issue 151 February 2016
Hip impingment
Time to get hip: Femoro-acetabular impingement
In the first part of this 2-part article, Chris Mallac looks at the surgery and rehab options for Femoro-acetabular impingement (FAI), an increasingly common musculoskeletal disorder that can affect young to middle aged athletes. In part two, Chris will describe in detail the post-operative rehabilitation period required to take an athlete back to full competition
From the editorAs clinicians caring for athletes, we like to think that our treatments can help rehab and prevent sports injuries. But as Chris Mallac explains in this issue’s lead article, conservative management of femoro-acetabular impingement (FAI), an insidious condition that leads to the insidious onset of groin pain and damage to the hip joint labrum, usually fails in the young athlete. In the first of a 2-part article, Chris outlines the pathogenesis of FAI, provides differential diagnostic tests, and offers management ideas, plus an in depth overview of the rehabilitation of the hip joint post-FAI surgery.
Meanwhile, Alicia Filley looks at tendinopathy treatments. Until recently, these treatment options were predicated a r o u n d a p a t h o l o g y p a r a d i g m o f inflammation only. As Alicia explains however, a more recent understanding of the additional role of degeneration in tendonitis has changed the thinking about the best
treatment approaches – and those that evidence suggests are rather less effective.
In our third article, Pat Gilham explores the topic of hamstring injury grading and how this can help formulate a rehab plan that enables a more rapid return to play. He also describes an eccentric training programme that has been demonstrated to be particularly useful in helping athletes overcome hamstring injury and get back to full sport participation.
Rounding up the issue, I’ve taken a long, hard look at the efficacy or otherwise of platelet therapy. In theory, platelet therapy supplies extra growth factors for injured tissue, thereby aiding the repair and remodelling phase, thereby speeding recovery. However, do these theoretical benefits translate into superior outcomes in injured athletes? As always, theory and practice are not necessarily the same thing...
Hope you enjoy this issue and we look forward to seeing you next month!
Andrew Hamilton BSc Hons MRSC ACSM (commissioning editor)
In this issue
Femoro-acetabular impingement: surgery and rehab options for an increasingly common musculoskeletal disorder 1
Tendon injuries: how the inflammation and degeneration theory is shaping the latest treatment approaches 6
Hamstring rehab: how injury grading and eccentric training can hasten return to play 10
Platelet therapy: does it do what it says on the tin? 14
2 SPORTS INJURY BULLETIN No 151
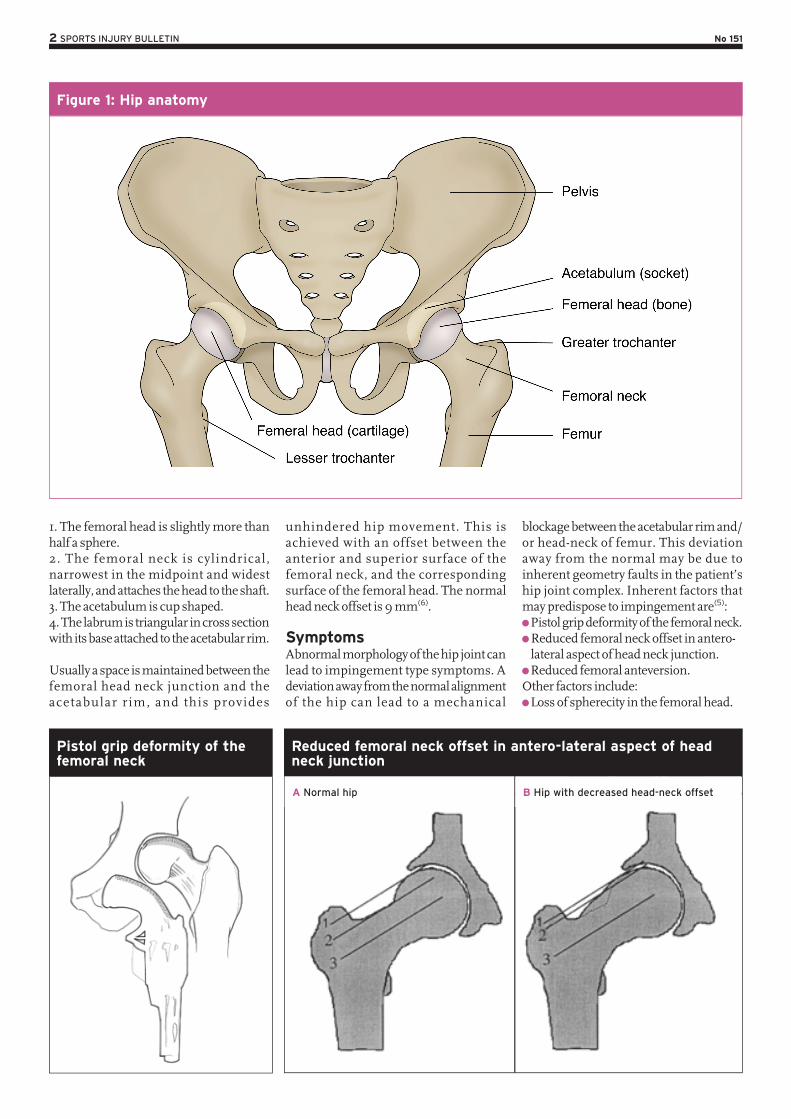
1. The femoral head is slightly more than half a sphere.2. The femoral neck is cylindrical, narrowest in the midpoint and widest laterally, and attaches the head to the shaft.3. The acetabulum is cup shaped.4. The labrum is triangular in cross section with its base attached to the acetabular rim.
Usually a space is maintained between the femoral head neck junction and the acetabular rim, and this provides
unhindered hip movement. This is achieved with an offset between the anterior and superior surface of the femoral neck, and the corresponding surface of the femoral head. The normal head neck offset is 9 mm(6).
SymptomsAbnormal morphology of the hip joint can lead to impingement type symptoms. A deviation away from the normal alignment of the hip can lead to a mechanical
blockage between the acetabular rim and/or head-neck of femur. This deviation away from the normal may be due to inherent geometry faults in the patient’s hip joint complex. Inherent factors that may predispose to impingement are(5): Pistol grip deformity of the femoral neck. Reduced femoral neck offset in antero-lateral aspect of head neck junction. Reduced femoral anteversion.
Other factors include: Loss of spherecity in the femoral head.
Figure 1: Hip anatomy
Pistol grip deformity of the femoral neck
Reduced femoral neck offset in antero-lateral aspect of head neck junction
A Normal hip B Hip with decreased head-neck offset

3 SPORTS INJURY BULLETIN No 151
Excessive coverage of acetabulum Retroversion of acetabulum (causes over-coverage and restricts flexion of the femoral neck). Coxa profunda deformity floor of the acetabulum touches the ilio-ischial line) increases the depth of the acetabulum.
FAI as an injuryAlthough some examples of hip joint impingement are caused by inherent hip joint abnormalities, FAI as an injury is an anatomical mal-alignment between the head and neck o f femur and the acetabulum. This causes compression of the labrum and articular cartilage during hip flexion manifesting as anterior hip pain and progression to early osteoarthritis of the hip. It is a condition that seems to affect younger more active people, particularly male. For example, in a radiological study of 155 young active patients 18-50 years of age with complaints of hip pain, it was found that a staggering 87% of subjects had evidence of an FAI(7).
The natural progression of an FAI to full blown hip joint disease has been postulated by McCarthy et al (2001)(8). They propose that initially an FAI causes excessive loads on the acetabular labrum at extreme ranges of movement. As the labrum frays along the articular margins, this progresses to a more consequential tear of the labrum. The articular cartilage then delaminates away from the articular margin adjacent to the labral lesion. This then leads to abnormal shear forces across the joint, which over a long term, causes more g loba l l abra l and ar t i cu lar degeneration.
Furthermore, more recent research suggests a strong link between FAI and other athletic groin pain syndromes, in p a r t i c u l a r a t h l e t i c p u b a l g i a . Economopoulos et al (2014) found that in
43 patients who underwent surgery for athletic pubalgia, 86% of them had evidence of a FAI in at least one hip, with Cam lesions being the most prevalent (see below for Cam lesion)(9). This highlights the possible interaction between forces acting across the pelvis and hip joint. Hammoud et al (2014) provide an in-depth discussion on how a FAI can possibly lead mechanical compensation patterns, which can in turn lead to a host of sports injuries such as osteitis pubis, sacroiliac joint problems, posterior hip impingement and proximal hamstring syndrome just to name a few(10).
In the context of FAI, two main manifestat ions of FAI have been described. These are ‘Cam’ and ‘Pincer’ lesions (see figure 2).
Cam lesions The Cam lesion is attributed to an asymmetric or nonspherical portion of the femoral head or neck abutting against an
acetabular rim. This abutment is most evident in flexion and internal rotation where a shear force occurs along the anterolateral edge of the acetabulum. This deformity decreases the head neck offset, increases the femoral head radius of curvature and resul ts in re la t ive retroversion of the femoral head.
The smooth motion between the femoral head and acetabulum is lost, which causes an outside-in abrasion of the acetabular cartilage with avulsion from the l a b r u m a n d s u b c h o n d r a l b o n e (delamination). This can lead to separation of the cartilage from the antero superior aspect of the labrum(11). Labral injuries are more likely to affect the anterior region possibly due to its poor blood supply. Also, it is a mechanically weaker area of the labrum and the anter ior l abrum experiences more loads and shear than other areas of the labrum(12).
Cam lesions are common in young active men with a ratio of around 25% in
Figure 2: Cam and pincer lesions
Reduced femoral anteversion
15º Angle of FNA
Normal Femoral Neck Anteversion
Increased Femoral Neck Anteversion
Femoral Neck Anteversion
45º Angle of FNA 0º Angle of FNA
CamPincer
4 SPORTS INJURY BULLETIN No 151
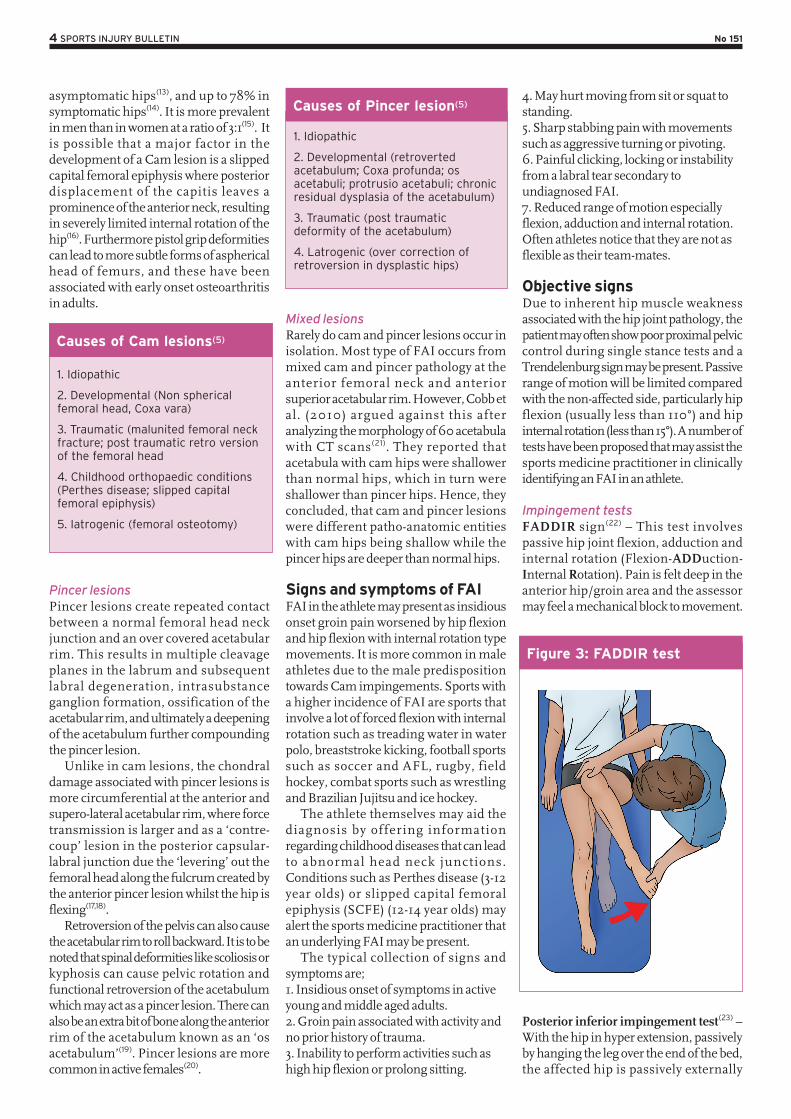
asymptomatic hips(13), and up to 78% in symptomatic hips(14). It is more prevalent in men than in women at a ratio of 3:1(15). It is possible that a major factor in the development of a Cam lesion is a slipped capital femoral epiphysis where posterior displacement of the capitis leaves a prominence of the anterior neck, resulting in severely limited internal rotation of the hip(16). Furthermore pistol grip deformities can lead to more subtle forms of aspherical head of femurs, and these have been associated with early onset osteoarthritis in adults.
1. Idiopathic
2. Developmental (Non spherical femoral head, Coxa vara)
3. Traumatic (malunited femoral neck fracture; post traumatic retro version of the femoral head
4. Childhood orthopaedic conditions (Perthes disease; slipped capital femoral epiphysis)
5. Iatrogenic (femoral osteotomy)
Pincer lesions Pincer lesions create repeated contact between a normal femoral head neck junction and an over covered acetabular rim. This results in multiple cleavage planes in the labrum and subsequent labral degeneration, intrasubstance ganglion formation, ossification of the acetabular rim, and ultimately a deepening of the acetabulum further compounding the pincer lesion.
Unlike in cam lesions, the chondral damage associated with pincer lesions is more circumferential at the anterior and supero-lateral acetabular rim, where force transmission is larger and as a ‘contre-coup’ lesion in the posterior capsular-labral junction due the ‘levering’ out the femoral head along the fulcrum created by the anterior pincer lesion whilst the hip is flexing(17,18).
Retroversion of the pelvis can also cause the acetabular rim to roll backward. It is to be noted that spinal deformities like scoliosis or kyphosis can cause pelvic rotation and functional retroversion of the acetabulum which may act as a pincer lesion. There can also be an extra bit of bone along the anterior rim of the acetabulum known as an ‘os acetabulum’(19). Pincer lesions are more common in active females(20).
1. Idiopathic
2. Developmental (retroverted acetabulum; Coxa profunda; os acetabuli; protrusio acetabuli; chronic residual dysplasia of the acetabulum)
3. Traumatic (post traumatic deformity of the acetabulum)
4. Latrogenic (over correction of retroversion in dysplastic hips)
Mixed lesionsRarely do cam and pincer lesions occur in isolation. Most type of FAI occurs from mixed cam and pincer pathology at the anterior femoral neck and anterior superior acetabular rim. However, Cobb et al. (2010) argued against this after analyzing the morphology of 60 acetabula with CT scans(21). They reported that acetabula with cam hips were shallower than normal hips, which in turn were shallower than pincer hips. Hence, they concluded, that cam and pincer lesions were different patho-anatomic entities with cam hips being shallow while the pincer hips are deeper than normal hips.
Signs and symptoms of FAIFAI in the athlete may present as insidious onset groin pain worsened by hip flexion and hip flexion with internal rotation type movements. It is more common in male athletes due to the male predisposition towards Cam impingements. Sports with a higher incidence of FAI are sports that involve a lot of forced flexion with internal rotation such as treading water in water polo, breaststroke kicking, football sports such as soccer and AFL, rugby, field hockey, combat sports such as wrestling and Brazilian Jujitsu and ice hockey.
The athlete themselves may aid the diagnosis by offering information regarding childhood diseases that can lead to abnormal head neck junctions. Conditions such as Perthes disease (3-12 year olds) or slipped capital femoral epiphysis (SCFE) (12-14 year olds) may alert the sports medicine practitioner that an underlying FAI may be present.
The typical collection of signs and symptoms are; 1. Insidious onset of symptoms in active young and middle aged adults.2. Groin pain associated with activity and no prior history of trauma. 3. Inability to perform activities such as high hip flexion or prolong sitting.
4. May hurt moving from sit or squat to standing. 5. Sharp stabbing pain with movements such as aggressive turning or pivoting.6. Painful clicking, locking or instability from a labral tear secondary to undiagnosed FAI.7. Reduced range of motion especially flexion, adduction and internal rotation. Often athletes notice that they are not as flexible as their team-mates.
Objective signsDue to inherent hip muscle weakness associated with the hip joint pathology, the patient may often show poor proximal pelvic control during single stance tests and a Trendelenburg sign may be present. Passive range of motion will be limited compared with the non-affected side, particularly hip flexion (usually less than 110°) and hip internal rotation (less than 15°). A number of tests have been proposed that may assist the sports medicine practitioner in clinically identifying an FAI in an athlete.
Impingement testsFADDIR sign(22) – This test involves passive hip joint flexion, adduction and internal rotation (Flexion-ADDuction-Internal Rotation). Pain is felt deep in the anterior hip/groin area and the assessor may feel a mechanical block to movement.
Posterior inferior impingement test(23) – With the hip in hyper extension, passively by hanging the leg over the end of the bed, the affected hip is passively externally
Figure 3: FADDIR test
Causes of Cam lesions(5)
Causes of Pincer lesion(5)

5 SPORTS INJURY BULLETIN No 151
rotated. The test is positive if it elicits similar pain as complained by the patient.
FABER test(24) – With the hip in flexion, abduction and external rotation (Flexion-ABDuction, External Rotation), abutment of the labrum and cartilage also can occur. The test is positive if it elicits similar pain as complained of by the patient,or if the distance between the lateral knee and the e x a m t a b l e d i f f e r s b e t w e e n t h e symptomatic and contra lateral hip.
RadiographsAnterior/posterior (AP) viewsWell centred AP views are necessary to view Cam lesions (due to flattened head-neck junction, pistol grip deformity), any degenerative hip joint changes (sclerosis, osteophytes, reduced joint space) and a profunda socket. AP views will also define the acetabular version such as the cross-over sign. This may also be seen indicative of a prominent anterior acetabular wall (pincer impingement). AP views will show acetabular retroversion, acetabular depth, os acetabulum and/or herniation pit in the neck of femur and/or impingement cysts may be present.
Standard Lateral ViewThis will identify subchondral bone sclerosis and cyst formation of the anterior acetabular rim.
Cross table lateral views/frog lateral viewsThis can be done in 10-15° internal hip rotation to compensate for femoral anteversion. This is best to view the Cam impingement lesion and reactive fibro cystic changes of the anterior head-neck junction. Other radiological measurements that can be made include head-neck offset(25), alpha angles(26), and anterior offset ratio(27).
Magnetic resonance imaging (MRI) and arthrography (MRA)MRI is useful if hip labral pathology is suspected in conjunction with FAI, and may show articular cartilage thinning. Increased signal on T2-weighted images in the anterior acetabulum may be indicative of subchondral edema, which may be incorrectly interpreted as a stress fracture of the anterior inferior iliac spine. It is more likely indicative of a subchondral stress reaction in the anterior acetabulum due to failure of the subjacent articular surface. Thus, anterior acetabular subchondral edema is suggestive of significant articular pathology(28).
MRA is much more sensitive for viewing intra-art icular pathology including labral lesions. This can also be useful, as the gadolinium injection associated with the MRA also has local anaesthetic that can be used as a diagnostic block for intra-articular joint pathology.
Computerised tomography (CT)CT 3D reconstructions are useful to assess the shape of the femoral head neck junction and this is considered useful for surgical resection. A new CT view has been developed by Pri tchard and O’Donnell to demonstrate FAI lesions(29). CT scanning in the position of discomfort (POD view) allows symptomatic Cam deformity to be accurately mapped in a 3-dimensional reconstruction. This procedure helps in diagnosis of the problem by visualisation and subsequent planning for surgical resection.
SurgeryDue to the mechanical nature of FAI, conservative management along with physiotherapy usually fails as ultimately, the impingement of bone on bone will prove to be restrictive to the athlete. Often conservative programs are only effective as acting as identifiers of FAI and then to prevent further mechanical symptoms by avoiding the offending movements. Gym based movements such as squats past 60° hip flexion, Bulgarian squats and leg press are avoided, or modified to be performed in external rotation. However, ultimately if pain persists then surgery is the only way to manage these problems.
Prior to the development of more advanced hip joint surgery techniques, athletes with ‘FAI’ would have lived and performed within the confines of their symptoms. They simply would have avoided movements that created hip joint
pain and if this proved too difficult to avoid, they simply would have ceased to compete.
In this current day, advancements in not only diagnosis but also both open and arthroscopic hip joint surgery has allowed simple management of these conditions. Therefore surgery is often recommended for the young athlete with FAI. The purpose of surgery is to remove the mechanical block of the proximal femur against the acetabulum and to also address any associated labral pathology and articular damage. Open and closed arthroscopic techniques have been described.
Prior to 2001, direct access into the hip joint was very difficult due to the risk of avascular necrosis, therefore most hip joint impingements were managed with labral debridement and/or labral reattachment. In 2001, Ganz et al described a surgical technique that involved surgical dislocation with a ‘trochanteric flip osteotomy’ that preserved the blood flow to the femoral head(30). This avoided the serious side effect of avascular necrosis of the femoral head associated with hip joint dislocation
Figure 4: FABER test
Figure 5: AP xray showing a prominent femoral neck
Figure 6: Alpha angle of the head neck of femur

6 SPORTS INJURY BULLETIN No 151
procedures. This technique led to better identification of FAI as a genuine hip joint pathology and correcting this surgically was now possible.
Open surgeryThis involves dislocation of the hip anteriorly using a trochanteric flap osteotomy. This allows a full view of the head neck junction. Any osseous impingement visualised can then be excised to restore the normal contour of the femoral neck junction. Retroversion of the acetabulum can be managed with resection of the prominent anterior acetabular rim. Any labral tear should be treated with excision or repair.
Ongoing groin pain following an open procedure can be caused by insufficient restoration of the femoral or acetabular morphology, advanced joint degeneration, joint space narrowing, ongoing cartilage damage, or scar adhesions between the hip joint capsule and femoral neck resection, and between the labrum and hip joint capsule(31). If this scarring is thick then they may interfere with motion between the femur and acetabulum. These can impinge during flexion and internal rotation movements.
Arthroscopic repairArthroscopic intervention is now becoming increasingly more popular. Two a r e a s c a n b e e x a m i n e d u n d e r arthroscopy(32);
1. Central compartment – the structures medial to the labrum. 2. Peripheral compartment – the structures outside the labrum but inside the hip capsule.
The arthroscopic procedure is performed with the patient lying supine or lateral decubitus. A traction device is used to separate the femur from the acetabulum to visualise the central compartment. Traction is not needed for peripheral compartment procedures. The joint is filled with saline and two to three portals are used (anterior, anterolateral and/or posterolateral).
The procedures achieved by hip arthroscopy at present include; Debridement of labral tear Repair of torn labrum Chondroplasty of acetabular lesions Drilling or micro fracture of acetabular lesions Acetabular rim excision (pincer lesions) Debridement of acetabular chondral delamination Capsular excision Femoral osteochondroplasty
Philippon et al (2007) found that at 93% of athletes returned to competitive sport following arthroscopically managed FAI(33). The small number who did not had advanced OA changes at the time of surgery.
ConclusionFAI is an increasingly more common
musculoskeletal disorder affecting the young to middle aged athlete that can lead to insidious onset groin pain and damage the hip joint labrum and lead to early OA changes. It is common in sports that require hip flexion and hip rotation positions as part of the skill execution. Cam and pincer lesions are the two varieties of FAI lesions and these can combine to form double lesions. Conservative management usually fails in the young athlete to completely manage their pain, therefore surgery, either open or arthroscopic is usually the recommended treatment.
References1. The Proceedings of the Third Open Scientific
Meeting of the Hip Society. St Louis, MO: CV
Mosby;1975:212–2.
2. Ann Surg. 2008;4:656-665
3. Clin Orthop Relat Res. 2003;417:112–20
4. Clin Ortop. 1999; 363:93–9
5. Curr Rev Musculoskelet Med. 4:23–32
6. Curr Orthop. 2008;22:300–10
7. Clin Orthop Relat Res. 2010 October; 468(10):
2710–2714
8. Clin Orthop Relat Res. 2001 Dec;(393):25-37
9. Sports Health. 2014. 6(2); pp 171-177
10. Sports Health. 2014. 6(2); pp 108-118
11. J Bone Joint [Br]. 2001;83-B:171–6
12. Curr Rev Musculoskelet Med. 2009; 2: 105–
117
13. Arthritis Care & Res. 2010;62 (9): 1319-1327
14. J Bone Joint Surg Am. 2010 Oct 20;92
(14):2436-44
15. Clin Orthop Relat Res. 2009;467:739-746
16. J Surg Orthop Adv. 2004;13(1):20-23
17. Radiology 2006;240(3):778-85
18. J Bone Joint Surg Br. 2005;87-B:1012–8
19. Hip Int. 2006;16(4):281-286
20. Arthritis Rheum. 2011;63 Suppl 10 :1077
21. Clin Orthop Relat Res. 2010; 468:2143–51
22. Knee Surg Sports Traumatol Arthrosc.
2007;15:1041–7
23. J Bone Joint Surg Br. 2005;87- B:1459–62
24. Clin Sports Med. 2006;25(2):299–308
25. Clin Orthop Relat Res. 2007;462:115–21
26. Clin Orthop. 2004;429:170–7
27. Hip Int. 2001;11:37–41
28. Sports Health. 2010. 2(4). pp 321-333
29. Singh PJ, PritchardM, O’Donnell J. The POD
CTscan—a betterway to demonstrate FAI and
early hip degeneration. Annual Scientific
Meeting. International Society for Hip
Arthroscopy; Oct 2009
30. The J of Bone and J Surgery. 83-B (8), pp
1119-1124
31. Clin Orthop Relat Res (2009) 467:769–774
32. Tech Orthop. 2005;20:156–62
33. Knee Surg Sports Traumatol Arthrosc
(2007) 15:908–914.
Figure 7: A 3-dimensional reconstruction of Cam lesion
7 SPORTS INJURY BULLETIN No 151
Tendons are bands of tough connective tissue at the ends of muscles that transfer forces between muscles and bones to move joints and maintain posture. They store kinetic energy, absorb shock, and aid in proprioception. To endure the great forces placed upon them, tendons must be strong and rigid, yet flexible enough to participate in joint movement. Tenocytes, the regulatory cells within the tendon, synthesise all the components in the extra cellular matrix, including collagen. Collagen provides the tendon’s tough yet elastic structure, through bundles of molecules formed into concentric fibrous bands.
Healing in healthy tendons is divided into three stages(1):1. The initial response after strain is inflammation, which provides clotting to ruptured vessels within the tendon, and consumes the tissue that is no longer viable. 2. In the proliferative and repair stage that follows, fibroblasts and tenocytes rush to the wound site, multiply, and rebuild the structure of the tendon. 3. The remodelling phase begins one to two months after injury, when the collagen
fibres align in the direction of stress along the tendon. Through this process, tendons adapt and grow in thickness and length.
Historically, symptomatic tendons that failed to heal were assumed stuck in a cycle of inflammation and the condition was labelled tendonitis. Subsequent research has found evidence of degeneration within s y m p t o m a t i c t e n d o n s , a n d t h e inflammatory theory was subsequently discarded in favour of the term ‘tendinosis’. More recent work suggests that both inflammation and degeneration exist in failed tendon healing, called tendinopathy.
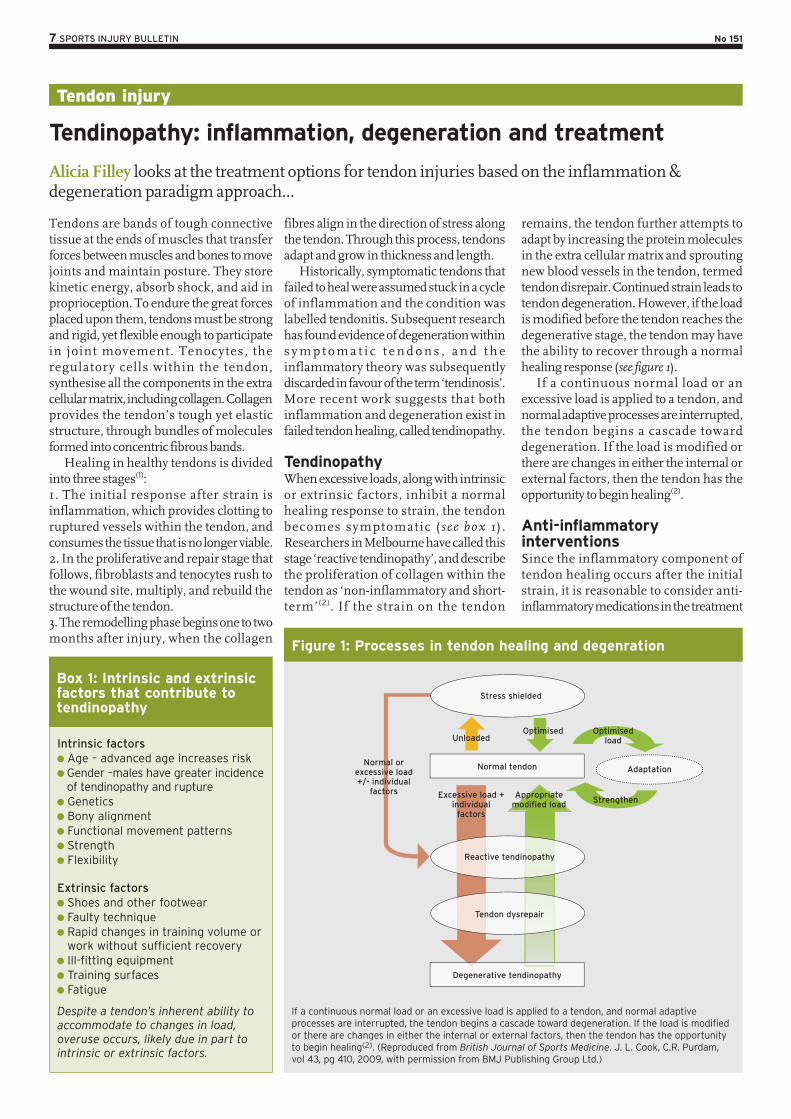
TendinopathyWhen excessive loads, along with intrinsic or extrinsic factors, inhibit a normal healing response to strain, the tendon becomes symptomatic ( see box 1 ) . Researchers in Melbourne have called this stage ‘reactive tendinopathy’, and describe the proliferation of collagen within the tendon as ‘non-inflammatory and short-term’ (2). If the strain on the tendon
remains, the tendon further attempts to adapt by increasing the protein molecules in the extra cellular matrix and sprouting new blood vessels in the tendon, termed tendon disrepair. Continued strain leads to tendon degeneration. However, if the load is modified before the tendon reaches the degenerative stage, the tendon may have the ability to recover through a normal healing response (see figure 1).
If a continuous normal load or an excessive load is applied to a tendon, and normal adaptive processes are interrupted, the tendon begins a cascade toward degeneration. If the load is modified or there are changes in either the internal or external factors, then the tendon has the opportunity to begin healing(2).
Anti-inflammatory interventionsSince the inflammatory component of tendon healing occurs after the initial strain, it is reasonable to consider anti-inflammatory medications in the treatment
Intrinsic factors Age – advanced age increases risk Gender –males have greater incidence of tendinopathy and rupture Genetics Bony alignment Functional movement patterns Strength Flexibility
Extrinsic factors Shoes and other footwear Faulty technique Rapid changes in training volume or work without sufficient recovery
Ill-fitting equipment Training surfaces Fatigue
Despite a tendon’s inherent ability to accommodate to changes in load, overuse occurs, likely due in part to intrinsic or extrinsic factors.
Tendon injury
Tendinopathy: inflammation, degeneration and treatment
Alicia Filley looks at the treatment options for tendon injuries based on the inflammation & degeneration paradigm approach...
If a continuous normal load or an excessive load is applied to a tendon, and normal adaptive processes are interrupted, the tendon begins a cascade toward degeneration. If the load is modified or there are changes in either the internal or external factors, then the tendon has the opportunity to begin healing(2). (Reproduced from British Journal of Sports Medicine. J. L. Cook, C.R. Purdam, vol 43, pg 410, 2009, with permission from BMJ Publishing Group Ltd.)
Figure 1: Processes in tendon healing and degenration
Normal tendon Adaptation
OptimisedUnloaded
Excessive load + individual
factors
Appropriate modified load
Optimisedload
Strengthen
Reactive tendinopathy
Tendon dysrepair
Normal or excessive load +/- individual
factors
Stress shielded
Degenerative tendinopathy
Box 1: Intrinsic and extrinsic factors that contribute to tendinopathy

8 SPORTS INJURY BULLETIN No 151
of tendinopathy, especially in the period soon after injury. Corticosteroid injections provide short-term pain relief from pain and swelling. Some suppose that the effect is really on the tissues surrounding the injured tendon, rather than the tendon itself(3). Understanding that corticosteroid injections are not curative but palliative is important when considering their use in treatment. While improving comfort and function in the short term, corticosteroids tend to weaken the structure of the tendon, paradoxically increasing the risk of tendon rupture.
Nonsteroidal anti-inflammatory drugs (NSAIDs), administered either orally or trans-dermally also assist with pain management. Professor Jill Cook has frequently stated that the use of Ibuprofen (and only Ibuprofen – not Celebrex or Feldene etc.) seems to drop the pain in painful tendons in the reactive stage if used short term(4). Again, some theorise that perhaps the mechanism of action is actually on the tissue surrounding the tendon. However, NSAIDs have been shown to supress tendon healing in animal studies, which would indicate a direct ac t ion upon the tendon (3). S ince inflammation is a normal part of the adaptive response, perhaps inhibiting it with NSAIDs interrupts a necessary part of the healing process.
The prolonged use of NSAIDs carries a risk of side effects related to the renal, cardiovascular and gastrointestinal systems and a review of the literature provides little to substantiate their use in the treatment of tendinopathy beyond short-term pain control(3). Therefore, the decision to recommend NSAIDs or not is based on clinical judgement. Consider the need for pain management versus the potential side effects and impact on tendon healing before advising its use.
Healing through loadingEccentric exercise is the most effective type of exercise for treating tendinopathy, though the mechanism of action is not well understood(5). During eccentric exercise (muscle lengthening), the tension within the muscle fibres is greater than when the muscles move concentrically (muscle shortening), yet the energy requirements, oxygen consumption, adenosine triphosphate (ATP) breakdown, and heat production are all less than during concentric movement. Therefore, during eccentric exercise, the muscle produces the same amount of work with less effort, and releases fewer irritating waste products.
Perhaps there is something in this eccentric equation that allows the tendon to receive the mechanical stimulation it needs to repair, while keeping the biochemical irritants at bay. Using the Melbourne model of degenerative tendinopathy, it is reasonable to expect a less stressful load, along with the modification of intrinsic and extrinsic factors, to trigger a normal adaptive response(2). Studies conducted on tendinopathic Achilles and patellar tendons show good results using an eccentric training program(3).
Guidelines for treatment with eccentric loading typically rely on the Alfredson protocol. Alfredson and colleagues conducted a landmark Swedish study that showed heavy-load eccentric calf muscle exercise to be effective in the treatment of chronic Achilles tendinopathy(6). Since then, most studies recommend a similar regimen of three sets of 12-15 repetitions, first using body weight resistance and then progressing to a 15-repetition maximum resistance, twice per day(3). Pain is tolerated during the exercise; however, if significant pain persists after the exercise, decrease the resistance. There are no contraindications to eccentric exercise.
Physiotherapy modalitiesPhysiotherapists and trainers often augment exercise prescription with various treatment modalities. While these may add to the subjective comfort of the athlete, they are not curative. For instance, cryotherapy (treating with ice) is a standard method of reducing inflammation and controlling pain. While effective for acute injuries, its efficacy in treating chronic tendinopathy in the reactive or disrepair stage is questionable. Other modalities, such as sound-assisted soft tissue massage, augmented soft tissue mobilization, ultrasound therapy, phonophoresis, and iontophoresis, lack randomised controlled clinical studies to support their use. These treatments are generally safe and have minimal side effects, but may not promote tendon healing.
The question of blood flowIncreased blood flow in damaged tendons, seen in the tendon disrepair stage, was first observed and described in the 1990s and termed neovascularisation(7). Nerves sprouting along side new blood vessels were thought to be the cause of the pain in the diseased tendon. While some saw this increased vascularity as the body’s attempt to heal and sought ways to promote it, others concluded that preventing this angiogenesis would interrupt the failed
healing cascade and also provide pain relief. Shock therapyTheoretically, the administration of shock waves to an injured tendon induces micro trauma that stimulates blood flow. Extracorporeal shock wave therapy (ESWT) targets tissue with a single-impulse acoustic wave generated using magnets, underwater electrodes, or crystals. Shock waves are uni-phasic and have a peak pressure that is nearly 1000 times greater than an ultrasound wave. Shock waves, administered as a low-energy treatment, require three weekly sessions; where as, a high-energy treatment is a single session that requires local or general anaesthesia.
Authors from Queen Mary University of London recently reviewed the literature available on the use of ESWT to treat lower limb tendinopathy and found only 13 studies with enough reliable data to analyse(7). The protocol for administration of ESWT varied between them, further complicating the ability to draw definite conclusions. That said, the researchers suggest that ESWT is more effective in the treatment of patellar tendinopathy than other conservative treatments and equal to patellar tendinopathy surgery. When treating insertional Achilles tendinopathy, they also suggest that ESWT is more effective than eccentric loading; and equally effective as eccentric loading when the tendinopathy is in the midportion of the Achilles tendon. There is some evidence that when combined, ESWT and eccentric loading provide even better outcomes(8).
Go with the flowThere are several other treatments that aim to increase blood flow to the relatively avascular tendon in an attempt to improve healing. Topical glyceryltrinitrate, administered through a topical patch, delivers nitric oxide (NO) to the tendon through the skin. The NO is thought to improve collagen production and increase vascularization. Low-level laser therapy, also known as cold or soft laser, supposedly increases tendon metabolism, collagen production, and vascularisation.
Injections of platelet rich plasma, derived from the subject’s own blood, directly into the tendon supposes that the platelets release growth factors into the damaged tissue (see Andrew Hamilton’s detailed article on platelet therapy elsewhere in this issue). These growth factors purportedly decrease inflammation and stimulate revascularisation and collagen production. Some have even attempted to

9 SPORTS INJURY BULLETIN No 151
inject whole autologous blood into diseased tendons with the same goals.
Overall, the shortage of studies on the efficacy of each of the above treatments, and the variation in protocols, study design, and sample size make it difficult to assess their usefulness with complete confidence. In addition, some of these treatments carry with them significant risks or side effects. Professional licencing boards and government agencies vary on approval of these methods, including ESWT, to manage tendinopathy; clinicians should therefore carefully assess the pros and cons of a treatment option before recommending its use for athletes.
Interrupting blood flowWhile some treatments attempt to increase the blood flow to the damaged tendon, others try to stop it. In sclerotherapy, a chemical agent injected into the tendon, causes thrombosis and deterioration of the newly formed vessels and nerves. Electrocoagulation uses a radiofrequency probe to transfer thermal energy to the diseased tendon and destroy the neovascular bundle. Injection with hypertonic glucose and lidocaine, called prolotherapy, works toward the same end while inducing an inflammatory response. The ability to test whether these treatments have the effect they intend is difficult. Studies showing their impact on function and pain are inconclusive(9,10).
Researchers from Qatar, Italy, and England questioned the validity of the theory of angiogenesis (new blood vessel growth) as a source of either healing or pain in a joint review of the literature on the subject(7). Conflicting evidence exists as to the presence of neovessels in symptomatic Achilles tendons. In fact, studies show neovascularisation in asymptomatic athletes and test subjects after strenuous exercise(7). The question then arises as to whether the new vessels are part of a normal physiological response or a pathologic one?
The researchers concluded that the presence or absence of neovessels bears no significance on the diagnosis, prognosis, or magnitude of pain experienced by those with tendinopathy. Therefore, the treatments that attempt to influence neovasculature one way or the other, while initially promising, may prove to be ineffective with well designed, randomised and controlled research. Until research provides better conclusions, recommendation of these treatments to athletes is not worth the potential risks associated with them.
Surgical optionsTendon surgery is generally considered a last resort for those who fail conservative treatment. Surgery removes the areas of d iseased tendon, a long wi th the accompanying neovascularisation, and stimulates a new healing process. This is accomplished through either ultrasound guided percutaneous tenotomy, sometimes called needling, or tendon debridement and repair via arthroscopic or open procedures.
Success rates following surgery vary, depending on the type of procedure, the tendon treated, and the level of injury within the tendon. Rehabilitation and return to sport can take upwards of 12 months, depending again on the type of procedure and severity of injury. Most notably, 20% to 30% of surgical treatments fail to improve the symptoms(10).
Future treatmentsPioneered in veterinary medicine to treat horses, stem cell transplantation for tendinopathic tendons in humans is now under preliminary investigation. Autologous stem cells, derived from the subject’s own bone marrow, fat tissue, or tendon is either injected directly into the tendon, or introduced into the tendon along with a scaffolding matrix that promotes the differentiation of the stem cells into tenocytes.
Another potential treatment is the injection of cultured tenocyte-like cells, taken from the subject’s own skin, into the injured tendon. These cells produce collagen and thus are thought to promote healing. Preliminary studies show promise, but placebo-controlled trials are needed to confirm efficacy.
Biomaterials, constructed from naturally occurring substances, have potential benefit in the treatment of tendinopathy. These biomaterials mimic native tendon structure and therefore, drive cell production toward alignment as normal tendon. In preliminary stages of investigation, this type of tendon grafting has proved beneficial in canine subjects(11). Animal studies also show promise using the injection of growth factors directly into the tendon(11).
Recommendations for cliniciansTendinopathy is among the most difficult sporting injuries to treat, and clinicians and athletes will grasp at nearly anything with promise to stop the pain and return the player to sport.
Anti-inflammatory medications, used immediately after injury or the onset of symptoms, reduce pain but possibly deter
healing. Physiotherapy modalities may subjectively help with pain management but lack evidence that they are curative. Many other treatments, although theoretically sound, need more research and development, and carry with them significant risks.
Modifying the load on the tendon through eccentric exercise and providing the tendon with sufficient rest through the alteration of contributing intrinsic or extrinsic factors, gives the tendon the best opportunity to heal itself when in the reactive and disrepair stages (see Box 2). The tendon may bear the load for a weak link in the kinetic chain; be overworked since starting twice-a-day practices; or become strained from abnormal positioning while sleeping (because the athlete’s dog insists on sleeping on the bed with its head on the athlete’s knee). Play detective until you find and remove the cause of strain. Only then will the tendon get the rest it needs and begin the healing process (see Box 2)!
References1. Birth Defects Res C Embryo Today. 2013
Sept;99(3):203-22
2. Br J Sports Med. 2009;43:409-16
3. Clin Sports Med. 2015;34:363-74
4. http://physioedge.com.au/wp-content/
uploads/2011/10/Podcast-5-Jill-Cook.pdf
5. Int J Sports Phys Ther. 2011 Mar;6(1):27-44.
6. Am J Sports Med. 1998 May-Jun;26(3):360-6
7. Knee Surg Sports Traumatol Arthrosc. 2012
Oct;20(10):1891-4
8. Am J Sports Med. 2015 Mar;43(3):752-61
9. Clin Orthop Surg. 2015 Mar;7(1):1-7
10. Prim Care. 2013 Jun;40(2):453-73.
11. Adv Drug Deliv Rev. 2014 Nov 21. [Epub ahead
of print]
Athletes require a team approach to examine everything including:
Training schedules; Amount and quality of sleep; Movement patterns; Strength in functional positions; Flexibility during movement, not just static positions;
Equipment; Shoes; Sleeping posture and mattress; Habitual postures during driving, studying, or working;
Structural alignment; Limb length.
Box 2: Additional intrinsic and extrinsic factors that can cause tendon strain

10 SPORTS INJURY BULLETIN No 151
Sporting activities involving high demands of sprinting or excessive stretching (kicking, sliding, split positions) have been found to influence the incidence of acute hamstring injuries. Hamstring injuries are diverse in nature consisting of differing injury types, location and size. This makes recommendations regarding rehabilitation and prognosis about healing time and return-to-play notoriously difficult. It has been suggested that return-to-play timescales vary between 28-51 days following acute hamstring injuries depending on the biomechanical cause, site, and grading of soft tissue injury(1). However, this is a contentious issue, which this article will explore.
Following a return to sport, the risk of re-injury is high within the first 2 weeks(2). The causes have been linked with initial hamstring weakness; fatigue; a lack of flexibility, and a strength imbalance between the hamstrings (eccentric) and the quadriceps (concentric)(2). The highest contributory factor however, is believed to be an inadequate rehabilitation program, which coincides with a premature return to sport(3). More evidence is now highlighting the benefit of primarily using eccentric strengthening exercises in hamstring rehabilitation performed at high loads at longer musculotendon lengths(1,4).
S e m i t e n d i n o s u s ( S T ) , Semimembranosus (SM), and Biceps
femoris long and short heads (BFLH and BFSH) make up the hamstring muscle group. They are involved with extension of the hip, flexion of the knee as well as providing multi-directional stability of the tibia and pelvis. All three muscles cross the posterior aspect of both hip and the knee joints making them biarticular. As a result, they have to continuously respond to large mechanical forces created by upper limb, trunk and lower limb locomotion via concentric and eccentric contractions. These forces are greatly increased during sporting activity, which is a likely culprit for their high injury frequency.
In a s tudy at the Universi ty of Melbourne, biomechanical analysts quantified the biomechanical load (ie musculotendon strain, velocity, force, power, and work) experienced by the hamstrings across a full stride cycle during over-ground sprinting, and compared the biomechanical load across each individual hamstring muscle(4).
Firstly, the hamstrings undergo a stretch-shortening cycle during sprinting, with the lengthening phase occurring during the terminal swing and shortening phase commencing just before foot strike, and continuing throughout the stance. Secondly, the biomechanical load on the biarticular hamstring muscles was found to be greatest during the terminal swing.
B F L H h a d t h e l a r g e s t p e a k musculotendon strain, ST displayed the greatest musculotendon lengthening velocity, and SM produced the highest musculotendon force as well as absorbing
Hamstring rehab
Acute Hamstring Injury Rehab – Get eccentric!
Patrick Gillham explores the benefits of using eccentric strengthening in rehabilitation for a quicker return-to-play following acute hamstring injuries…
Hamstring anatomy
Biomechanics during sprinting
11 SPORTS INJURY BULLETIN No 151
and generating the most musculotendon power. This has ties in with other similar research, which distinguishes peak musculotendon strain as a large contributor to eccentric muscle damage, ie hamstring injury, rather than peak muscle force(1); hence the recommendation of eccentric strengthening for acute hamstring rehabilitation.
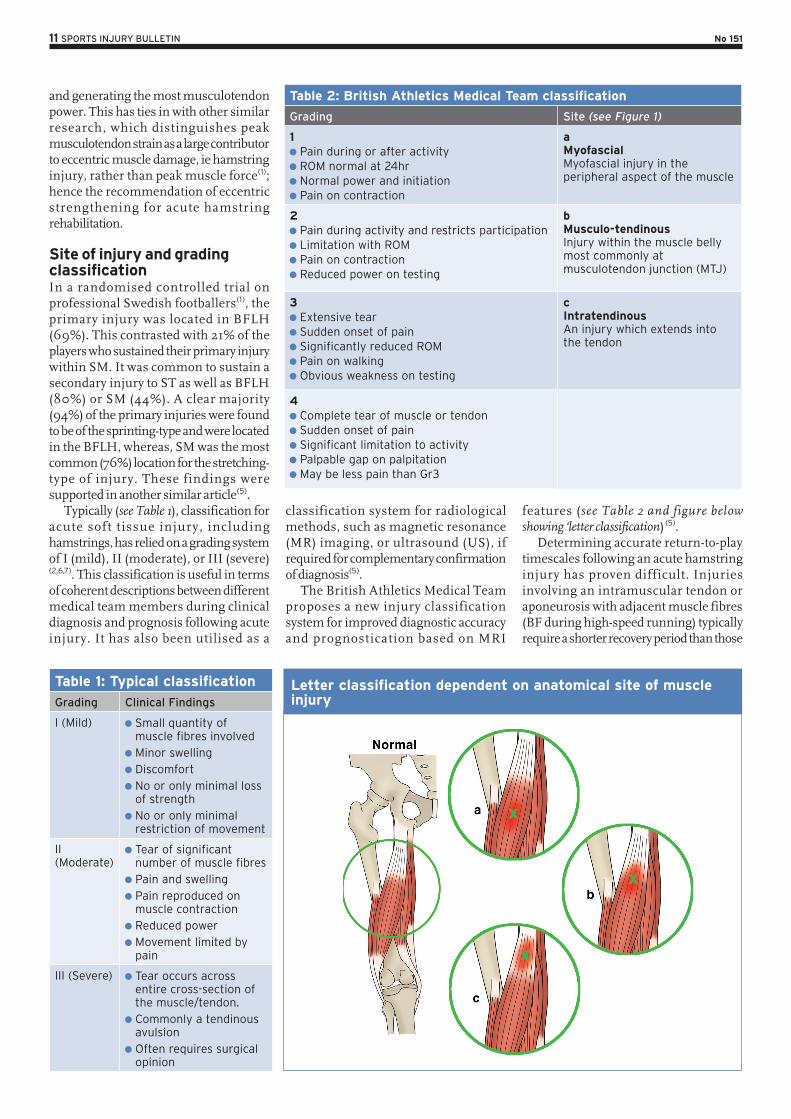
Site of injury and grading classificationIn a randomised controlled trial on professional Swedish footballers(1), the primary injury was located in BFLH (69%). This contrasted with 21% of the players who sustained their primary injury within SM. It was common to sustain a secondary injury to ST as well as BFLH (80%) or SM (44%). A clear majority (94%) of the primary injuries were found to be of the sprinting-type and were located in the BFLH, whereas, SM was the most common (76%) location for the stretching-type of injury. These findings were supported in another similar article(5).
Typically (see Table 1), classification for acute soft tissue injury, including hamstrings, has relied on a grading system of I (mild), II (moderate), or III (severe)(2,6,7). This classification is useful in terms of coherent descriptions between different medical team members during clinical diagnosis and prognosis following acute injury. It has also been utilised as a
classification system for radiological methods, such as magnetic resonance (MR) imaging, or ultrasound (US), if required for complementary confirmation of diagnosis(5).
The British Athletics Medical Team proposes a new injury classification system for improved diagnostic accuracy and prognostication based on MRI
features (see Table 2 and figure below showing ‘letter classification) (5).
Determining accurate return-to-play timescales following an acute hamstring injury has proven difficult. Injuries involving an intramuscular tendon or aponeurosis with adjacent muscle fibres (BF during high-speed running) typically require a shorter recovery period than those
Table 1: Typical classification
Grading Clinical Findings
I (Mild) Small quantity of muscle fibres involved
Minor swelling Discomfort No or only minimal loss of strength
No or only minimal restriction of movement
II (Moderate)
Tear of significant number of muscle fibres
Pain and swelling Pain reproduced on muscle contraction
Reduced power Movement limited by pain
III (Severe) Tear occurs across entire cross-section of the muscle/tendon.
Commonly a tendinous avulsion
Often requires surgical opinion
Table 2: British Athletics Medical Team classification
Grading Site (see Figure 1)
1 Pain during or after activity ROM normal at 24hr Normal power and initiation Pain on contraction
aMyofascialMyofascial injury in the peripheral aspect of the muscle
2 Pain during activity and restricts participation Limitation with ROM Pain on contraction Reduced power on testing
bMusculo-tendinousInjury within the muscle belly most commonly at musculotendon junction (MTJ)
3 Extensive tear Sudden onset of pain Significantly reduced ROM Pain on walking Obvious weakness on testing
cIntratendinousAn injury which extends into the tendon
4 Complete tear of muscle or tendon Sudden onset of pain Significant limitation to activity Palpable gap on palpitation May be less pain than Gr3
Letter classification dependent on anatomical site of muscle injury

12 SPORTS INJURY BULLETIN No 151
involving a proximal free tendon and/or MTJ (SM during dance or kicking)(2).
There are also links between MRI findings as well as the area of injury, and return-to-play. More specifically, it has been hypothesised that the shorter the distance between the proximal pole of the injury and the ischial tuberosity (ie more intratendinous in nature) found on MRI findings (determined by the presence of oedema), the longer the time to return(1). Likewise, the length of oedema shows a similar effect on recovery time – ie the longer the length, the longer the recovery(1). In addition, the position of peak pain upon palpation following acute injury is also linked with increased recovery periods(1).
Furthermore, there have been attempts to clarify the link between grading of acute hamstring injury and return-to-play. In a prospect ive cohort s tudy on 207 professional footballers with acute hamstring injuries, 57% were grade I, 27% were grade II, and 3% were grade III. Grade I injuries returned to play within an average of 17 days. Grade II was 22 days, and grade III was 73 days. Eighty four percent of these injuries affected the BF, 11% SM, and 5% ST, but there was no significant difference in lay-off time for injuries to the three different muscles(5). This has been compared to 5-23 days with grade I-II injuries, and 28-51 days for grade I-III in other studies respectively (1,8).
Rehabilitation – eccentric strengtheningSeveral researchers have argued the benefits of eccentric strengthening following an acute hamstring injury versus concentric when aiming to reduce timeframes for return-to-play(1-5,9). The crux of this argument is that with the majority of acute hamstring injuries occurring during eccentric loading (terminal swing or stretching), the rehabilitation ‘should mirror the particular situation that lead to the injury’(1). This quotation was taken from a study, which showed a significant difference between an eccentric and concentric rehabilitation programme following acute hamstring injuries in elite and non-elite footballers.
This study was a randomised controlled clinical trial on 75 footballers in Sweden, which reported that using eccentric strengthening versus concentric the time to return-to-play was reduced by 23 days. This was irrespective of the type of injury or the site of injury. The outcome measure was the number of days to return to full–team training and availability for match
selection. This article will now explore this study in greater depth.
Two rehabilitation protocols were used, and initiation began five days following injury. All players had sustained a sprinting-type (high speed running/acceleration) or stretching-type injury (high kicking, split positions, glide tackling). Exclusion criteria included previous hamstring injuries, trauma to posterior thigh, ongoing history of low back problems, and pregnancy.
Al l p layers underwent an MRI investigation 5 days following the injury, to expose the severity and site of injury. A player was judged to be fit enough to return to full-team training using the active ‘Askling H-test’ (see below). A positive test is when a player experiences any insecurity or apprehension when performing the test. The test should be completed without full dorsiflexion of the ankle.
Seventy two percent of players sustained sprinting-type injuries, whilst
28% were stretching-type. Of these, 69% sustained injury to BFLH, whereas 21% was located in the SM. Injuries to ST were only sustained as secondary injuries (48% with BFLH, and 44% with SM). Ninety four percent of sprinting-type injuries were located in the BFLH, while SM was the most common (76%) location for the stretching-type injury.
The two rehabilitation protocols used were label led L-protocol and the C-protocol. One aimed at loading hamstr ings dur ing l eng thening (L-protocol), and the other consisted of e x e r c i s e s w i t h n o e m p h a s i s o n lengthening (C). Each consisted of three exercises which could be performed anywhere and were not dependent of advanced equipment. They also aimed at targeting flexibility, trunk/pelvic stability as well as specific strength training to the hamstrings. All were performed in the sagittal plane with speed and load progressed throughout.
The Askling H-test

13 SPORTS INJURY BULLETIN No 151
C-Protocol L-Protocol
Standing contract/relax hamstring stretch – twice every day, 3 sets x 4 repetitions.
‘The Extender’ on injured limb (slow knee extensions to the point just before pain) – Twice daily, 3 sets x 12 repetitions.
‘The Diver’ standing on injured limb (performed slowly with simultaneous upper and lower limb movement) – Once every other day, 3 sets x 6 repetitions.
‘The Glider’ with injured leg in front using friction sock/ sliding matt for sliding leg (movement back to standing is completed using the arms. Progression with distance of slide and speed performed) – Once every 3rd day, 3 sets x 4 repetitions.
Standing cable/resistance band hip extension with injured limb – once every day, 3 sets x 6 repetitions.
Supine single-leg pelvic lift using body weight on injured limb – Once every 3rd day, 3 sets with x8 repetitions.

14 SPORTS INJURY BULLETIN No 151
Platelet therapy
Platelet therapy: a faster route to recovery?In recent years, there’s been an increasing interest in platelet therapy as a treatment for speeding injury healing. But just how strong is the evidence for its use? Andrew Hamilton looks at the latest research...
Of all the injuries suffered by athletes participating in sport, those involving muscle tissue are among the commonest injuries – accounting for up to 50% of reported injuries(1,2). Many muscle injuries result from excessive strain on muscle, during sprinting, jumping or other explosive contractions but they may also be the result of direct blows, or excessive eccentric contraction, when the muscle develops tension while lengthening. In this type of injury, the myotendinous junction of the superficial muscles involved is often affected –eg the rectus f e m o r i s , s e m i t e n d i n o s u s , a n d gastrocnemius muscles.
Despite the high frequency of muscle injury in athletes, there’s still considerable debate among clinicians as to what constitutes the ‘best’ method of its treatment. Much of course will depend on the diagnosis and grading of muscle injury – usually gained from a thorough clinical assessment. Imagining can provide a d d i t i o n a l g u i d a n c e f o r t h e physiotherapist, although this often requires a referral involving additional cost and time.
Despite these caveats above, few clinicians would argue against the merits of some basic early treatment options to
hasten the athlete’s return to sport practice. The most commonly used of these include rest, ice, compression and elevation (RICE) with a short period of immobilisation during the early post-injury phase. In addition, the short-term use of non-steroidal anti-inflammatory (NSAIDs), corticosteroid medications is often recommended(3-8).
More than medicationWhile medications such as NSAIDs and corticosteroids have their place in the early stages of muscle injury treatment, there’s been an increasing interest in the use of autologous (cells and tissues derived from self) of biological products as an alternative or additional treatment for muscle injury. One such treatment is the use of blood platelets (blood cells whose function, along with the coagulation factors, is to stop bleeding) as used in platelet therapy.
Why platelets? When a muscle is injured and damaged, it undergoes a number of processes as part of the healing/repair process (see figure 1). During this process, there are two main phases: The early phase of destruction
(inflammatory phase), where affected
cells including muscles, blood vessels, connective tissues and intramuscular nerve undergo death and breakdown. The repair and remodelling phase, in
which undifferentiated satellite cells (in response to various growth factors) proliferate and differentiate into mature myoblasts in an effort to replace the injured muscle fibre tissue.
In the in f l ammatory phase , the inflammation occurring after muscle injury usually leads to the accumulation of inflammatory cells, neutrophils and macrophages. In addition, blood platelet cells in the vicinity of the injured site become activated. These activated platelets undergo ‘degranulation’ releasing various substances, including growth factors (see box 1), which are stored in the alpha (α) granules wi thin p la te le ts (9). The accumulation of platelets in the vicinity of a muscle injury should therefore in theory provide more growth factors for the tissue, thereby aiding the repair and remodelling phase. In addition, platelets contain other important substances need for tissue repair and regeneration, such as adhesive proteins, clotting factors and their inhibitors, proteases, cytokines and membrane glycoproteins.
FindingsThe time to return was significantly shorter in the L-protocol compared with the C-protocol, averaging 28 days and 51 days respectively. Time to return was also significantly shorter in the L-protocol than in the C-protocol for injuries of both sprinting-type and stretching-type, as well as for injuries of different injury classification. There are questions, however, over whether the C-protocol is specific enough for hamstring activation to create a legitimate comparison.
Summary and clinical implicationsAcute hamstring injuries most commonly occur during sprinting (terminal swing) or stretching (kicking, sliding, lunging/split
positions). BFLH is involved more often in sprinting-type injuries as a result of terminal swing. This is possibly due to its a b s o r p t i o n o f t h e l a r g e s t p e a k musculotendon strain across all four hamstring muscles.
Injuries can be classified from Grade I-III or perhaps more specifically Grade 1-4 for severity and a-c depending on site of injury. This based on MRI findings. The closer the site of injury is to the proximal hamstring tendon, the longer the return-t o - p l a y p e r i o d . U s i n g e c c e n t r i c strengthening exercises in rehabilitation programmes will promote a faster return-to-play. For example, ‘The Extender’, ‘The Diver’, or ‘The Slider’.
To enable a thorough rehabilitation process, clinicians need to take into
account the initial hamstring weakness, any lack of flexibility, previous hamstring injuries, age, fatigue, and strength imbalances between hamstring (eccentric) and quadriceps (concentric) contraction.
References1. Br J Sports Med 2013; 47: 953-959
2. J Orthop Sports Phys Ther 2010; 40(2): 67-81
3. Sports Med 2004; 34: 681-695
4. Med Sci Sports Exerc 2012; 44(4): 647-658
5. Br J Sports Med 2012; 46: 112-17
6. Musc Lig Tend J 2013; 3(4): 337-345
7. Brukner, P. in: Khan K. 2007 (3rd ed). Clinical
Sports Medicine. Sydney. PA: McGraw-Hill
Companies.
8. Sports Phy Ther 2011; 3(6): 528-533
9. J Biomech 2007; 40: 3555-3562
15 SPORTS INJURY BULLETIN No 151
Theory and practiceGiven the discovery that platelets play a vital role in muscle tissue repair, it wasn’t long before researchers wondered if platelet-rich plasma (PRP) injections into the site of an injured muscle could accelerate recovery time and thus hasten the return to sport of an injured athlete. These platelet-rich therapies are produced by centrifuging a quantity of the patient’s own blood and extracting the active, platelet-rich, fraction.
A 2009 study using an animal model showed that an autologous PRP injection significantly hastened tibialis anterior
muscle recovery (from 21 days to 14 days(12). Indeed, prior to this, Sanchez et al presented a similar finding at the 2005 World Congress on Regenerative Medicine. They noted that athletes receiving PRP injection under ultrasound guidance gained full recovery within half of the expected time(13).
However, in 2010, the International Olympic Committee concluded that ‘currently there is very limited scientific evidence of clinical efficacy and safety profile of PRP use in athletic injuries’(14). This stance was underlined by a systematic review article published the following year,
reporting ‘there has been no randomised clinical trials of PRP effects on muscle healing’(15). Fast forward to 2015 and what does the research about the efficacy or otherwise of PRP injections?
Latest evidenceIn the last 2-3 years, a flurry of papers has been published on the use of PRP therapy for muscle injury. A 2013 study on 30 professional athletes with acute local muscle injury seemed to provide positive evidence for PRP therapy(16). Prior to the intervention, all the athletes underwent and ultrasound and sonoelastography (a form of ultrasound imaging that reveals mechanical propert ies of t issue) examination. Patients were then randomly assigned to 2 groups: Group A received targeted PRP
injection under ultrasound guidance plus and additional conservative treatment Group B received conventional
conservative treatment only
Pain was assessed according to visual analogue scale (0 to 10), while muscle function was assessed according to pain on resisted flexion or strength, and range of motion. Both groups were further evaluated in the days 1, 7, 14, 21, and 28 after commencing treatment.
Overall, the degree of pain relief was greater in group A compared to group B throughout the intervention. At the end of 28-day observation, 93 % of pain regression was declared by patients in group A vs. 80 % of regression of pain in group B. Also, at 7 and 14 days, significant improvements in strength and range of motion for PRP treatment group were observed. By the end of the study, subjective global function scores improved significantly in group A compared with group B – as evidenced by the average return-to-sport times – 10 days in group A and 22 days in group B.
A 2014 systematic review meanwhile produced less encouraging findings on the value of PRP(17). The authors searched the literature for studies assessing the effects (benefits and harms) of platelet-rich therapies for treating musculoskeletal soft tissue injuries and where the primary outcomes were functional status, pain and adverse effects. The review included data from 19 trials totalling 1088 participants that compared platelet-rich therapy with placebo, autologous whole blood, dry needling or no platelet-rich therapy. These trials covered eight clinical conditions:
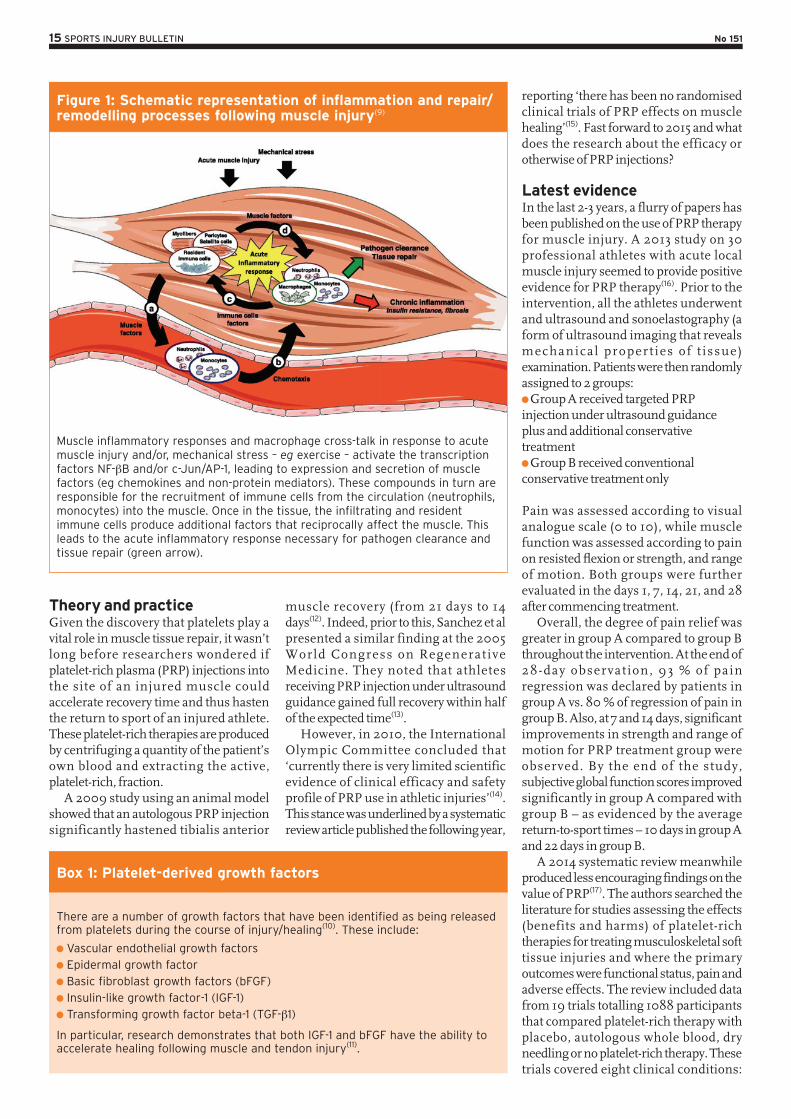
Figure 1: Schematic representation of inflammation and repair/remodelling processes following muscle injury(9)
Muscle inflammatory responses and macrophage cross-talk in response to acute muscle injury and/or, mechanical stress – eg exercise – activate the transcription factors NF-βB and/or c-Jun/AP-1, leading to expression and secretion of muscle factors (eg chemokines and non-protein mediators). These compounds in turn are responsible for the recruitment of immune cells from the circulation (neutrophils, monocytes) into the muscle. Once in the tissue, the infiltrating and resident immune cells produce additional factors that reciprocally affect the muscle. This leads to the acute inflammatory response necessary for pathogen clearance and tissue repair (green arrow).
There are a number of growth factors that have been identified as being released from platelets during the course of injury/healing(10). These include:
Vascular endothelial growth factors Epidermal growth factor Basic fibroblast growth factors (bFGF) Insulin-like growth factor-1 (IGF-1) Transforming growth factor beta-1 (TGF-β1)
In particular, research demonstrates that both IGF-1 and bFGF have the ability to accelerate healing following muscle and tendon injury(11).
Box 1: Platelet-derived growth factors
16 SPORTS INJURY BULLETIN No 151
rotator cuff tears (arthroscopic repair) (six trials); shoulder impingement syndrome surgery (one trial); elbow epicondylitis (three trials); anterior cruciate ligament (ACL) reconstruction (four trials), ACL reconstruc t ion (donor gra f t s i te applicat ion) ( two tr ials) , patel lar tendinopathy (one trial) , Achilles tendinopathy (one trial) and acute Achilles rupture surgical repair (one trial). The results were as follows: Medium-term function data at six
months from five trials showed no difference between PRP and control groups;. Long-term function data at one year
pooled from 10 trials showed no difference between PRP and the control condition; Data pooled from four trials that
assessed PRP in three clinical conditions showed a small reduction in short-term pain in favour of PRT but the clinical significance of this result was marginal; Seven trials reported an absence of
adverse events following PRP therapy but four trials reported adverse events; Pooled data for long-term function
from six trials during rotator cuff tear surgery showed no statistically or clinically significant differences between PRP and control groups; The evidence for all primary outcomes
was judged as being of very low quality not least because the methods of preparing platelet-rich plasma varied and lacked standardisation and quantification of the plasma applied to the patient;
Fast forward a year and a 2014 study investigated the effect of a single PRP injection in the treatment of grade 2 hamstring muscle injuries(18). Twenty-eight patients diagnosed with an acute hamstring injury were randomly allocated to autologous PRP therapy combined with a rehabilitation program or a rehabilitation program only. The primary outcome of this study was time to return to play. In addition, changes in pain severity and pain interference scores over time were examined.
The results showed that patients in the PRP group achieved full recovery significantly earlier than controls. The mean time to return to play was 42.5 days in the control group and 26.7 days in the PRP group. Significantly lower pain severity scores were observed in the PRP group throughout the study. However, no significant difference in the pain interference score was found between the
2 groups. The authors concluded: ‘A s ingle autologous PRP inject ion combined with a rehabilitation program is significantly more effective in treating hamstring injuries than a rehabilitation program alone’.
Conflicting evidenceLater the same year however, a rigorous double-blind, placebo-controlled trial on the effectiveness of PRP injections for acute hamstring injury drew very different conclusions(19). The researchers randomly assigned 80 competitive and recreational athletes with acute hamstring muscle injuries (as confirmed on magnetic r e s o n a n c e i m a g i n g ) t o r e c e i v e intramuscular injections of PRP or isotonic saline as a placebo. Importantly, the patients, clinicians, and physiotherapists were a l l unaware of s tudy-group assignments.
Each patient received two 3-ml injections with the use of a sterile ultrasound-guided technique; the first injection was administered within 5 days after the injury and was followed 5 to 7 days later by the second injection. Patients in the two study groups performed an
identical, daily, progressively phased, criteria-based rehabilitation program, which was based on the best available evidence (detailed in the study). The rate of re-injury within 2 months after the resumption of sports activity was assessed as a secondary outcome measure.
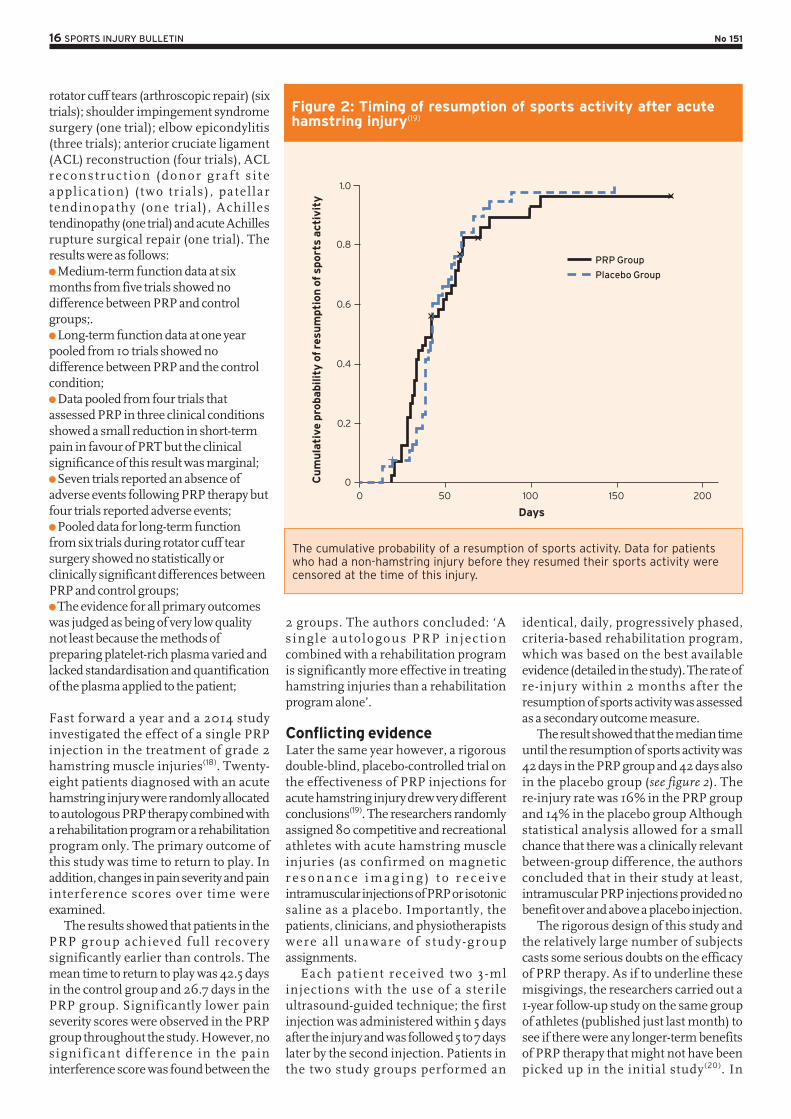
The result showed that the median time until the resumption of sports activity was 42 days in the PRP group and 42 days also in the placebo group (see figure 2). The re-injury rate was 16% in the PRP group and 14% in the placebo group Although statistical analysis allowed for a small chance that there was a clinically relevant between-group difference, the authors concluded that in their study at least, intramuscular PRP injections provided no benefit over and above a placebo injection.
The rigorous design of this study and the relatively large number of subjects casts some serious doubts on the efficacy of PRP therapy. As if to underline these misgivings, the researchers carried out a 1-year follow-up study on the same group of athletes (published just last month) to see if there were any longer-term benefits of PRP therapy that might not have been picked up in the initial study(20). In
Figure 2: Timing of resumption of sports activity after acute hamstring injury(19)
The cumulative probability of a resumption of sports activity. Data for patients who had a non-hamstring injury before they resumed their sports activity were censored at the time of this injury.
00
0.2
0.4
0.6
0.8
1.0
50 100
Days
Cu
mu
lati
ve p
roba
bilit
y o
f re
sum
pti
on
of sp
ort
s act
ivit
y
150
PRP Group
Placebo Group
200

17 SPORTS INJURY BULLETIN No 151
Contributors to this issue
Chris Mallac has worked as Head of Performance at London Irish Rugby, Head of Sports Med at Bath Rugby and Head Physio at Queensland Reds Super 14. He is currently teaching globally on Rehab Trainer Courses.
Alicia Filley PT, MS. lives in Houston, Texas and has 25 years experience working in rehabilitation. She is currently vice president of DISC Spine Center
Patrick Gillham is a musculoskeletal physiotherapist at Pure Sports Medicine in London who specialise in the prevention, diagnosis, treatment and rehabilitation of sports injuries and musculoskeletal problems
Andrew Hamilton BSc Hons, MRSC, ACSM is a member of the Royal Society of Chemistry, the American College of Sports Medicine and a consultant to the fitness industry, specialising in sport and performance nutrition: www.andrewmarkhamilton.co.uk
Sports Injury Bulletin is published by Green Star Media Ltd, Meadow View, Tannery Lane, Bramley, Guildford GU5 0AB, UK. Telephone +44 (0)1483 892894
Commissioning editor Andrew Hamilton
Technical editor Chris Mallac
Managing Director Andrew Griffiths
Customer Services Duncan Heard [email protected]
Marketing Gina Edwards [email protected]
© Green Star Media Ltd. All rights reserved.
To subscribe to Sports Injury Bulletin call Duncan Heard on +44 (0)1483 892894
particular, they sought to establish the re-injury rates at one year following PRP, and any secondary outcomes such as alterations in clinical and MRI parameters, subjective patient satisfaction and the hamstring outcome score. Analysis of the data showed that just as at 2 months, one year later there were no significant between-group differences in the 1-year re-injury rate, or any other secondary outcome measure.
Another very recent study into the efficacy of PRP therapy was published just a few months ago. Researchers pooled the data from 19 previous randomised controlled trials, which had compared PRP therapy in patients with acute or chronic musculoskeletal soft tissue injuries with placebo, autologous whole blood, dry needling, or no PRP(21). The authors concluded: ‘While several in -vitro studies have shown that platelet-derived growth fac tors can promote the regeneration of bone, cartilage, and tendons, there is currently insufficient evidence to support the use of platelet-rich therapy for treating musculoskeletal soft tissue injuries’. And as in the 2013 study highlighted earlier(17), they also pointed o u t t h a t t h e r e i s a n e e d f o r t h e standardisation of PRP preparation
methods. The final conclusion was that the only circumstance where PRP therapy might offer tangible benefits is when conservative treatment has failed and the next treatment option is an invasive surgical procedure.
Conclusions and practical advice for the clinicianWhen a clinician has an athlete in their care, minimising the recovery time so that return to sport can take place as soon as possible is an important goal of any treatment. In theory, PRP therapy should speed healing and recovery and indeed, a few earlier studies seemed to suggest that PRP is a worthwhile adjunct alongside conventional treatment. However, larger and more rigorously constructed studies have failed to find solid evidence for the benefits of PRP, either in the short or longer term. One possible reason for the confusing picture is that the preparation of PRP is far from standardised, which means that the biologically active components in a PRP treatment might vary tremendously from study to study. As clinicians, our goal is to employ evidence-based practice and on this basis, we have to conclude that (as yet) there is simply insufficient evidence for the use of PRP
therapy in the treatment of sports-related muscle injuries.
References1. Am J Sports Med 2001, 29:300–303
2. Br J Sports Med 2001, 35:435–439
3. Curr Sports Med Rep 2009, 8:308–314
4. Sports Med 2004, 25:588–593
5. Clin J Sport Med 2003, 13:48–52
6. Br J Sports Med 2004, 38:372–380
7. J Bone Joint Surg Am 1983, 65:1345–1347
8. J Am Acad Orthop Surg 1996, 4:287–296
9. Thromb Haemost 2011, 105(Suppl 1):S13–S33
10. Br J Sports Med 2008, 42:314–320
11. J Bone Joint Surg Br 2000, 82-B:131–137
12. Am J Sports Med 2009, 37:1135–1142
13. ‘Application of autologous growth factors
on skeletal muscle healing’: Presented at 2nd
World Congress on Regenerative Medicine, May
18–20, 2005
14. Br J Sports Med 2010, 44:1072–1081
15. Expert Opin Biol Ther 2011, 11(4):509–518
16. Med Ultrason. 2013 Jun;15(2):101-5
17. Cochrane Database Syst Rev. 2014 Apr
29;4:CD010071
18. Am J Sports Med. 2014 Oct;42(10):2410-8
19. N Engl J Med 2014; 370:2546-2547
20. Br J Sports Med. 2015 May 4. pii:
bjsports-2014-094250
21. Clin Podiatr Med Surg. 2015 Jan;32(1):99-10