fall into gi 2013 - chicago sgnachicagosgna.org/.../2014/02/objectives-for-fall-into-gi-2013.pdf ·...
TRANSCRIPT

Chicago SGNA
Fall into GI 2013 A Special "Hands-On" ERCP Clinic Station Objective Handouts
Chicago SGNA Education Committee 11/9/2013

OBJECTIVES FOR STATION #1
DESCRIBE THE ROLE OF THE RN/GI TECH IN PREPARING THE
ENDOSCOPY SUITE
Position carts and monitors in the room for easiest viewing of
monitor and fluoroscope screen by MD and assistive personnel
Work top organization should include and organizer with pockets
or clips to hold various equipment (wires tend to be long), gauze,
sterile water, normal saline and alcohol pads (to clean sticky
contrast agents off gloves)
Equipment preferences of the MD.
PPE equipment including gowns, gloves, masks, lead aprons with
thyroid collar, X-ray badges, and X-ray in use warning signs, X-ray
protective goggles
RN RESPONSIBLE FOR
drawing up and proper labeling of all medications
used during procedure, including
contrast agent 1/2 strength and full strength with
no air bubbles
Normal saline and or sterile water drawn up in
20ml syringes
glucagon available
simethicone available (not used in all institutions)
sedation used during procedure (unless general
anesthesia)
reversal meds readily available
IDENTIFY VARIOUS TYPES OF ERCP EQUIPMENT INCLUDING CANNULATOMES AND WIRES
HANDS ON DEMONSTRATION AND RETURN DEMONSTRATION OF ERCP EQUIPMENT- including
cannulatomes and wires

E ndoscopic - Looking inside with a scope
R etrograde - Backwards
C holangio - Biliary
P ancreatography – Pancreas –
using radiographic examination


Cholelithiasis: Gallstones in the
gallbladder
Cholangitis: Inflammation of the
common bile duct, often
secondary to bacterial infection
or choledocholithiasis
Cholecystitis: Inflammation of
the gallbladder secondary to
gallstones
Choledocholithiasis: Gallstones,
which have migrated from the
gallbladder to the common bile
duct


We discussed the SGNA position statements-
Ergonomics in the Gastroenterology Setting
Radiation Safety in the Endoscopy Setting
Available at www.sgna.org

OBJECTIVES FOR STATION #2
Describe the role of the RN Pre-procedure/patient assessment
RN needs to completely assess the patient prior to the procedure, and accurately
document all nursing measures, including the following:
Date/time of arrival
History obtained from
Who is accompanying the pt/who is driving home?
Ambulation
Indications for procedure- (evaluation of s/s of malignancy, acute/recurrent/chronic
pancreatitis, CBD stones, unexplained chronic abdominal pain, jaundice, possible bile
duct disease, pre or post cholecystectomy stone removal, ampulla and bile duct
manometry
Pt ID and Allergy/other Alert Bands
Previous sedation problems
Medical and surgical history
Metal implants/ICD for grounding pad placement
Current Medications
Current Physical exam including- vital sign, lungs sounds, bowel sounds, Ht and wt,
pregnancy status
NPO status
Dentures
Advanced directives
Belongings
Current Lab results
Start or check for patent IV line
Assess knowledge deficits for patient education related to ERCP
length of procedure
Positioning
use of flouro
sedation and monitoring
indications
recovery expectations
Ensure any preoperative MD orders are implemented
Identify various types of ERCP equipment including those to facilitate access and opening of the ampulla
such as a needleknife, dilators and biliary balloon dilators
HANDS ON RETURN DEMONSTRATION OF ERCP EQUIPMENT including those to facilitate access and
opening of the ampulla such as a needle knife, dilators and biliary balloon dilators

We discussed the SGNA Standards and guidelines
Guidelines for Documentation in the Gastrointestinal Endoscopy Setting
Available www.sgna.org

OBJECTIVES FOR STATION #3
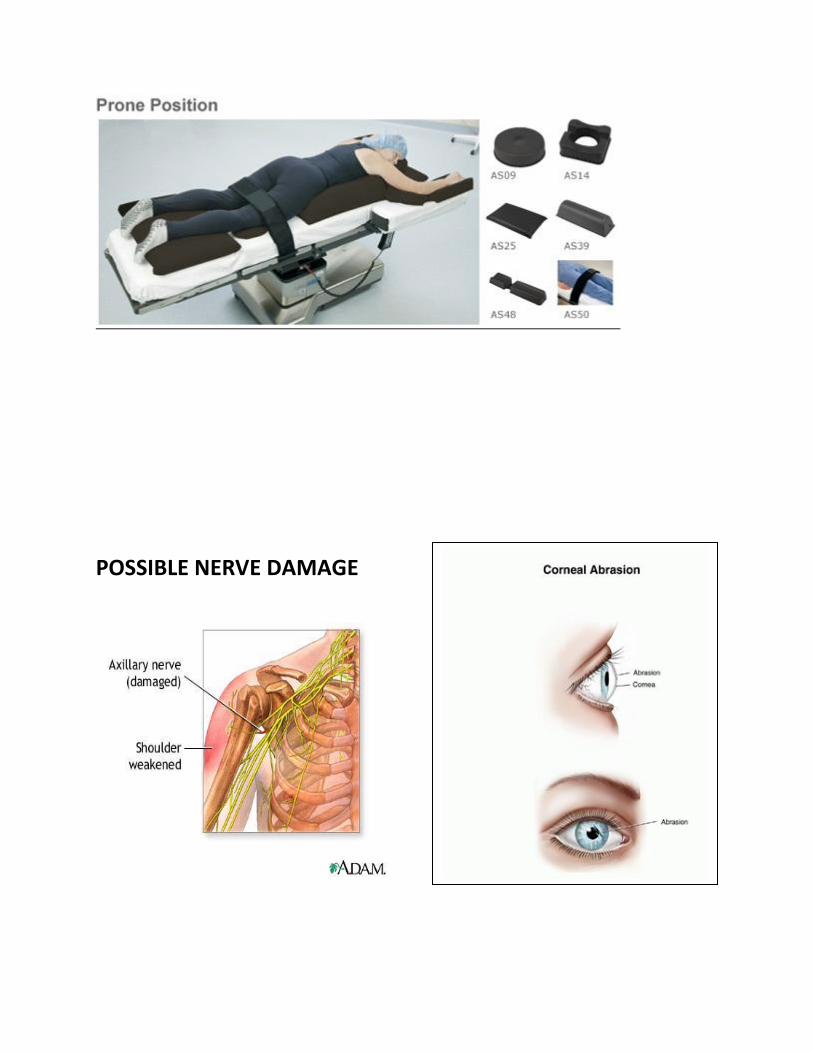
Describe the role of the RN Intra-procedure, including proper positioning and possible complications of
poor positioning of the ERCP patient
Goal is to position for patient comfort with the least chance for complications
usually prone or slight left lateral (prone is best anatomically)
if pt is to be intubated, done supine and then turned prone with a minimum
assist of 4 people
preserve cervical spine and body alignment
pad under bony prominences
pad or pillow under shins will prevent foot drop
ask ladies if their breasts are comfortable, men if their scrotum is
comfortable
arms should never be >90 degrees at the shoulder
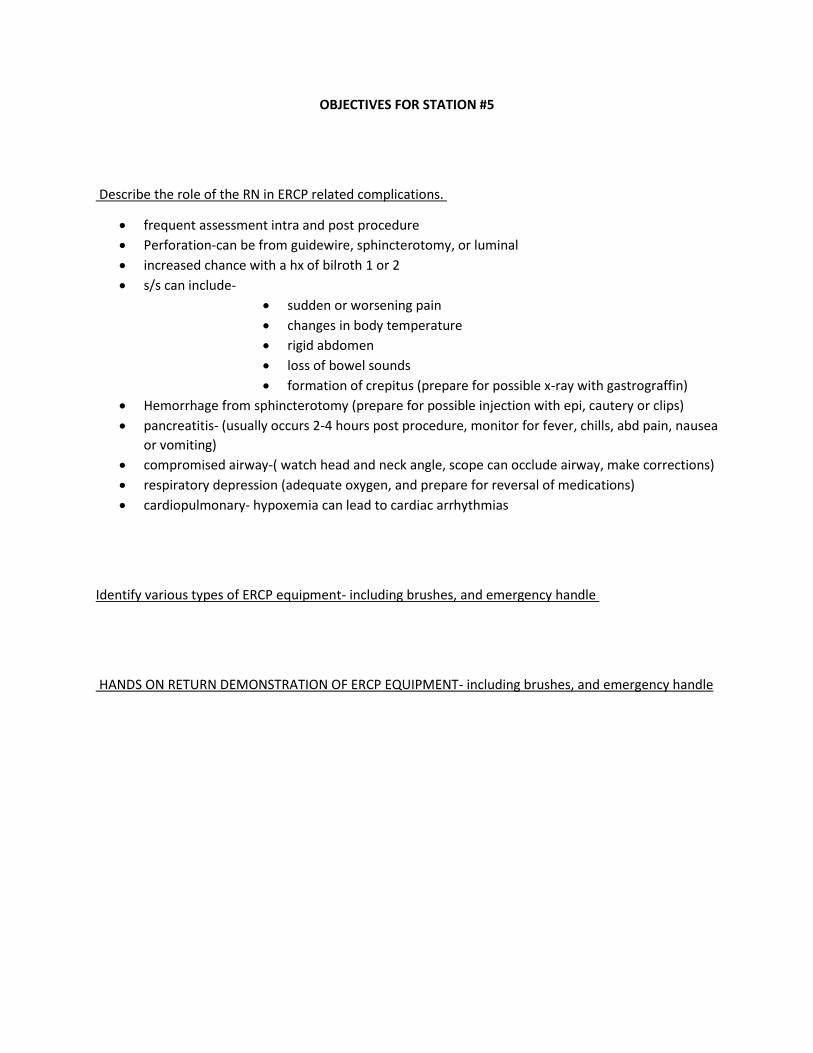
Potential Complications from poor positioning
nerve damage (axillary, radial, ulnar, peroneal or tibia nerves)
vessel compression
pressure ulcers
compartment syndrome (straps too tight)
V/Q mismatch (one lung perfusing, one lung oxygenating)
atelectasis (shallow breathing due to pressure on chest)
corneal abrasions
Identify various types of ERCP equipment for stone retrieval
Hands on return demonstration of ERCP equipment- including stone retrieval balloons and baskets

PRONE POSITIONING SHOWING PROPER PADDING UNDER BONY
PROMINENCES
POSSIBLE NERVE DAMAGE

DUE TO CHEST COMPRESSION

V/Q MISMATCH
A VQ Mismatch in respiratory pathophysiology is a problem with either the Ventilation (air
going in and out of the lungs) or the Perfusion (Oxygen and Co2 diffusion at the alvioli and
the pulmonary arteries). VQ ratios compare the amount of air reaching the alveoli to the
amount of blood reaching the alveoli.
Ventilation Problems include: inadequate rate or tidal volume during respiration. For
example, the person has an adequate rate of respirations (say, 18 breaths per minute), but
the tidal volume is insufficient). This would be considered a V/Q mismatch relating to a
problem with the V side of the equation.
Alternatively, you may have a perfusion problem. For example, excess pulmonary dead
space,such as: emphasema, bronchitis, pneumonia, atelectasis, low pulmonary artery
pressures, RVF, lack of haemoglobin availability (as a result of haemorrhage or Carbon
Monoxide Poisoning).


OBJECTIVES FOR STATION #4
Describe the roles of the RN or GI tech during ERCP, intra-procedure
One RN to be considered the "circulating" RN
liason between the outside and the procedure room
administer and monitor sedation (unless general or MAC)
be responsible for accurate and thorough documentation of all nursing
measures
be able to retrieve equipment, troubleshoot, and carry out MD orders
during procedure
One RN or tech to be considered the "scrub or assist" role (some institutions may use GI techs during
ERCP)
has to be extensively familiar and competent with ERCP equipment to work with the MD
Circulating RN role
RN responsibility of accurate documentation of the following:
re-verify Pt ID and procedure during time out
verify consent form signed
all personnel involved in case
scope ID used
events or occurrences
vital signs per protocol
any specimens retrieved
therapeutic devices used (cautery, balloons, dilators)
grounding pad placement and evaluation of skin
IV fluids
fluoroscopy time
if pt was shielded
contrast media(amount and strength)
RN is responsible for monitoring of the sedated patient
medications and reversals used during endoscopic sedation
indications for and levels of sedation
sedation policies and guidelines
airway management
continuous monitoring of the sedated patient
risks and complications including cardiac, respiratory and paradoxical, precautions during
pregnancy, pediactric and elderly, difficult to sedate pt, sleep apnea.

Identify various types of ERCP equipment - including biliary and pancreatic stents
HANDS ON RETURN DEMONSTRATION OF ERCP EQUIPMENT- including biliary and pancreatic stents

SEDATION SCALE (CHECK YOUR INSTITUTION GUIDELINES)

www.medscape.com
Dosage Guidelines for Adults Table 1. Commonly Used Drugs for Procedural Sedation and Analgesia in Adults(Open Table in a new window)
Drug Adult Dose Onset
of
Action
Duration
of Action*
Comments
Midazolam
(Versed)
0.02-0.1 mg/kg IV initially; if further
sedation is required, may repeat with 25%
of initial dose after 3-5 min; not to exceed
2.5 mg/dose (1.5 mg for elderly persons)
and 5 mg cumulative dose (3.5 mg for
elderly persons)
1-2 min 30-60 min Respiratory depression or hypotension may occur, particularly when rapidly
administered or combined with fentanyl (may need to decrease midazolam dose); does
not provide analgesia; action reversed by flumazenil
Fentanyl 1-2 mcg/kg slow IV push (over 1-2 min);
may repeat dose after 30 min
1-2 min 30-60 min May cause chest wall rigidity, apnea, respiratory depression, or hypotension; elicits
minimal cardiovascular depression; may cause dysphoria, nausea, vomiting, or EEG
changes; action reversed by naloxone
Etomidate
(Amidate)
0.1-0.2 mg/kg slow IV push over 30-60
sec
< 1 min 3-5 min Commonly causes myoclonus, pain upon injection, adrenal suppression (typically no
clinical significance unless repeated doses are used within a limited time span); may
cause nausea, vomiting, and lower seizure threshold; does not alter hemodynamics;
causes a slight to moderate decrease in intracranial pressure that only lasts for several
minutes; does not cause histamine release; useful for patients with trauma and
hypotension
Propofol
(Diprivan)
0.5-1 mg/kg IV loading dose; may repeat
by 0.5-mg increments q3-5min
< 1 min 3-10 min Provides rapid onset and recovery phase, and brief duration of action; has
anticonvulsant properties; can rapidly cause deepening sedation;
causes cardiovascular depression and hypotension
*Duration of action based on normal drug elimination (ie, nonelderly adult with normal renal and hepatic function)
OBJECTIVES FOR STATION #5
Describe the role of the RN in ERCP related complications.
frequent assessment intra and post procedure
Perforation-can be from guidewire, sphincterotomy, or luminal
increased chance with a hx of bilroth 1 or 2
s/s can include-
sudden or worsening pain
changes in body temperature
rigid abdomen
loss of bowel sounds
formation of crepitus (prepare for possible x-ray with gastrograffin)
Hemorrhage from sphincterotomy (prepare for possible injection with epi, cautery or clips)
pancreatitis- (usually occurs 2-4 hours post procedure, monitor for fever, chills, abd pain, nausea
or vomiting)
compromised airway-( watch head and neck angle, scope can occlude airway, make corrections)
respiratory depression (adequate oxygen, and prepare for reversal of medications)
cardiopulmonary- hypoxemia can lead to cardiac arrhythmias
Identify various types of ERCP equipment- including brushes, and emergency handle
HANDS ON RETURN DEMONSTRATION OF ERCP EQUIPMENT- including brushes, and emergency handle

Sphincterotomy bleed with clips

www.medscape.com
Post-ERCP Pancreatitis: Presentation and Management
Typically, if a patient is going to develop post-ERCP pancreatitis, the
probable diagnosis becomes apparent within a few hours of the procedure.
It is characterized by;
severe abdominal pain
frequently, back pain
nausea (with or without vomiting)
mild fever
Unfortunately, the usual 1-hour observation period after ERCP is often
insufficient for post-ERCP pancreatitis to declare itself. If the patient can be
kept under observation longer, or returns with symptoms, a 2-hour serum
or urinary amylase level (> 1000 IU/L) is highly predictive of evolving post-
ERCP pancreatitis
Patients presenting with post-ERCP pancreatitis should receive:
adequate (narcotic) analgesia
treatment for nausea (if present)
copious intravenous fluids (starting with a 1-2 L bolus of Ringer's
lactate solution and continuing with 250-300 mL/hr)
A nasogastric tube should be placed only if the patient has unrelieved
nausea or vomiting.
Urine output should be monitored and charted, with the aim of at least
50 cc/hr of urine output (100 cc/hr is better). In patients unable or
unwilling to spontaneously pass urine, placement of a urinary catheter is
necessary to monitor urine output.
Patients should be watched for signs of severe inflammatory response
syndrome, which includes:
fever (> 38˚ C)
tachycardia (> 90 beats/min)
tachypnea (> 20 breaths/min)
and low or high peripheral white blood cell count (< 4000/mm3 or >
12,000/mm3).

SGNA.ORG- SEDATION AIRWAY MANAGEMENT
Go to SGNA.org
Go to issues tab, then under that tab is ‘sedationfacts.org’ – Read all about sedation and patient
management there.
Reversal Agent Indication Adult Dose Pediatric Dose Comments
Naloxone (Narcan) Reverses
opioid
agonists
Postanesthetic or
opioid dependent:
0.1-0.2 mg/kg IV;
may repeat q2-3min
prn
Opioid overdose:
0.4-2 mg IV; may
repeat q2-3min prn
Postanesthetic reversal:
0.005-0.01 mg/kg
IV/IM; may repeat q2-
3min prn
Opiate intoxication:
0.01-0.1 mg/kg dose
IV/IM; may repeat
every min; not to
exceed 2 mg/dose
Onset of action for IV is 1-3 min vs
10-15 min for IM; rebound sedation
may occur; if used in patient with
chronic opioid use, will precipitate
acute withdrawal and abrupt
sympathetic discharge possibly
leading to acute pulmonary edema

www.medscape.com- Commonly used reversal agents.
Flumazenil
(Mazicon)
Reverses
benzodiazepines
Partial antagonism
(for sedation
reversal): 0.1-0.2
mg IV infused over
15 sec; may repeat
after 45 sec and
then every min; not
to exceed total
cumulative dose of
1 mg
Complete
antagonism (for
overdose): 0.2 mg
IV infused over 30
sec; may repeat
with additional
doses of 0.5 mg
over 30 sec at 1-
min intervals; not
to exceed a total
cumulative dose of
3 mg
0.01 mg/kg/dose
IV infused over 15
sec; not to exceed
0.2 mg/dose; may
repeat every min;
not to exceed total
cumulative dose of
0.05 mg/kg or 1
mg (whichever is
lower)
Rebound sedation may occur; if
used in patient with chronic BZP
use, will precipitate acute
withdrawal; may precipitate
seizures unresponsive to BZPs

OBJECTIVES FOR STATION #6
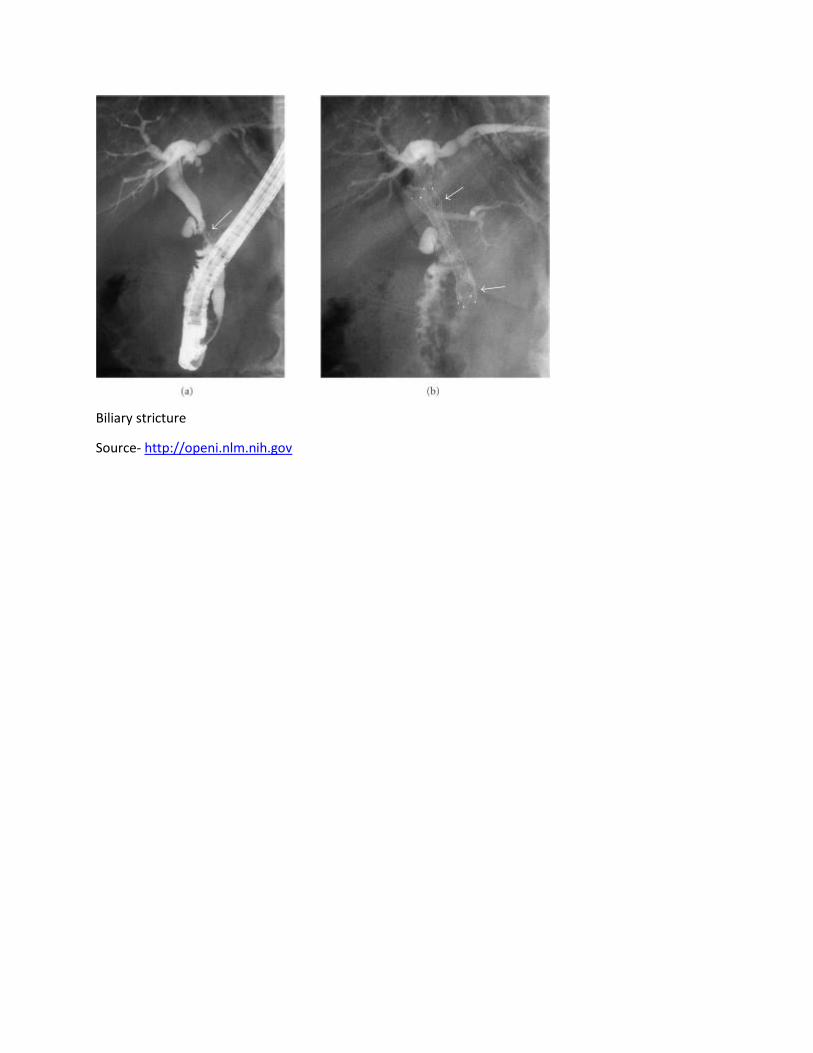
DISCUSS CASE STUDY – BILIARY STRICTURE
New onset jaundice associated with solitary biliary strictures in the elderly is concerning for a malignant
stricture such as cholangiocarcinoma.
Patient, 70 year old male
Symptoms- Painless jaundice
Labs-
His bilirubin was 7.0 mg/dl
alkaline phosphatase was 294 U/L
Ultrasound and CT scan were normal
ERCP- revealed a biliary stricture below the bifurcation of the right and left hepatic ducts, concerning for
cholangiocarcinoma – a stent was placed
Biopsies and brushings were negative
CEA and CA 19-9 were normal
One month later, repeat ERCP and cholangioscopy revealed that the stricture had resolved.
Ampullary biopsies revealed infiltration with IgG4 plasma cells
Liver function tests returned to normal
Nine months later, the patient represented with painless jaundice
Labs-
bilirubin was 8.1 mg/dl
alkaline phosphatase was 282 U/L
CT scan was normal
2nd ERCP- revealed a new stricture in the distal bile duct- concerning for a malignant stricture. The
previously seen proximal biliary stricture remained resolved.
Biopsies and brushings were negative.
Repeat CEA and CA 19-9 were normal.
Endoscopic ultrasound- revealed a mass surrounding the biliary stricture
He was treated with prednisone 20 mg, and a slow taper
His liver enzymes returned to normal
Repeat ERCP showed resolution of the biliary stricture. His liver enzymes have remained normal after
10 months of follow-up

DISCUSSION-
IgG4-Related Sclerosing Cholangitis (IgG4-SC) is a rare condition which can cause biliary strictures
mimicking malignant strictures. It is most often seen in association with autoimmune pancreatitis,
which our patient did not have.
It can also be associated with IgG4-related lymphoplasmacytic infiltration in other organs. We report a
rare case of IgG4-SC causing metachronous biliary strictures responsive to medical therapy.
This is an important differential diagnosis to consider, particularly to avoid drastic unnecessary surgery
or chemotherapy in benign disease.
DESCRIBE VARIOUS EQUIPMENT USED TO CANNULATE THE COMMON BILE DUCT
Cannula: Catheter used to gain access to CBD and/or PD. Can have
multiple lumens for injection and guide wire usage.
Guide wire: Wire placed into the CBD/PD. Can be used for cannulation.
Left into the duct to maintain access while devices are exchanged over
it.
HANDS ON DEMONSTRATION AND RETURN DEMONSTRATION OF ERCP EQUIPMENT- including
cannulatomes and wires

OBJECTIVES FOR STATION #7
Discuss Case Study- Primary Sclerosing Cholangitis
52 year old with history of Htn and hyperlipidemia
Current symptoms-
Progressive fatigue
Pruritis
Labs- rising bilirubin
Tests-
Diagnosis of PSC typically does not require ERCP
ERCP is reserved for treatment of dominant stricture or sampling to rule out
cholangiocarcinoma
Can be diagnosed with MRCP
ERCP was performed with stent placement in hepatic stricture
Liver biopsy performed to confirm “onion skin” or fibrosis in hepatic tissue
Considerations with PSC
Consider in patients with IBD, unexplained cholestasis, and normal MRCP
6% overlap with autoimmune hepatitis
ERCP is done for patients with PSC and worsening
symptoms to evaluate for dominant main duct disease→ concern for cholangiogram
Dilation or dilation + stenting are both effective to treat strictures
dilation + stenting associated with more infectious complications
No randomized control trial comparing dilation to dilation + stenting Risk of cholangiocarcinoma
is 1-2% per year
As with all indeterminate biliary strictures, yield of brushing is poor. Slightly improved with
biopsy, however, overall sensitivity is still suboptimal
DESCRIBE VARIOUS EQUIPMENT USED FOR OPENING AND ACCESSING THE COMMON BILE DUCT
SPHINCTEROTOME: Catheter used to gain access to common bile duct (CBD) and/or pancreatic
duct (PD) and perform sphincterotomy. Can have multiple lumens for injection and guidewire
usage.
DILATION BALLOON: Balloon catheter used to open the ampulla. Commonly done following a
sphincterotomy. Dilation balloon can also be used to open up strictures within the CBD and PD.

NEEDLE KNIFE: A slender surgical knife with a needle point, used to gain access of the CBD.
Needle is advanced into the tissue, heat is applied to cut through mucosa and gain access.
HANDS ON DEMONSTRATION AND RETURN DEMONSTRATION OF ERCP EQUIPMENT including
those to facilitate access and opening of the ampula such as a needleknife, dilators and biliary
balloon dilators.
OBJECTIVES FOR STATION #8
Discuss case study- choledocholithiasis
35 year old with no past medical history
Current symptoms
epigastric abdominal pain
nausea and vomiting x 48 hours
Labs-
liver enzymes elevated 2x ULN
bilirubin 2.0
Lipase is normal
Ultrasound is ordered which reveals dilated intra and extrahepatic ducts with no stone in
the CBD.
Choledocholithiasis is suspected on the basis of clinical symptoms and initial laboratory
evaluation
Normal liver enzymes have a negative predicitive value of 97% for choledocholithiasis
RUQ ultrasound has a sensitivity of 22-50% for choledocholithiasis

Guidelines from ASGE-The Role of Endoscopy in the Evaluation of
Suspected Choledocholithiasis
Gastrointest Endosc 2010;71:1-9 1. We recommend that the initial evaluation of suspected choledocholithiasis should include serum liver
biochemical tests and a transabdominal US of the right upper quadrant. These tests should be used to
risk-stratify patients to guide further evaluation and management.
2. We recommend that patients with symptomatic cholelithiasis who are surgical candidates and have a
low probability of choledocholithiasis proceed to cholecystectomy without additional biliary evaluation
3. We recommend that patients with an intermediate probability of choledocholithiasis undergo further
evaluation with preoperative EUS or MRC or an IOC. In this group of patients, we suggest that ERC be
deferred unless EUS, MRC, and IOC are unavailable, given the less favorable risk profile of ERC.
4. We recommend that patients with a high probability of choledocholithiasis undergo an evaluation of
the bile duct with therapeutic capability, generally preoperative ERC. When available, laparoscopic bile
duct exploration can serve as an alternative to ERC.
5. We suggest that EUS or MRC be considered in the diagnostic evaluation of postcholecystectomy
patients suspected of having choledocholithiasis when initial laboratory and US data are abnormal yet
nondiagnostic.
6. We recommend against early ERC in the evaluation and management of patients with mild ABP in the
absence of clear evidence of a retained stone.
7. We recommend early ERC in patients with acute biliary pancreatitis and concomitant cholangitis,
given the observed benefits in morbidity and mortality.
8. We suggest that patients with acute biliary pancreatitis and clinical evidence of biliary obstruction be
considered for early ERC. We cannot recommend for or against early ERC in patients with predicted
severe acute biliary pancreatitis in the absence of overt biliary obstruction or cholangitis, given the lack
of consensus in the available data.
9. As patients with acute biliary pancreatitis are at least at intermediate risk for choledocholithiasis, we
suggest pre-operative EUS or IOC be considered for these patients when cholangitis or biliary
obstruction are absent.
Patient had cholecystectomy without complications.
Identify and describe various equipment used during ERCP for stone retrieval

RETRIEVAL BALLOON: catheter with a balloon on the end. Balloon is inflated in the proximal CBD and
pulled through the duct to remove stones. Device can be placed into the duct over a guidewire and can
have an injection port.
RETRIEVAL BASKET: catheter with a basket on the end. Basket is opened and closed by manipulating the
handle. When opened inside the duct the basket can grasp stones. Stones can be crushed inside the
duct or pulled out. Baskets can be used with or without a guidewire and may have a lumen for injection.
HANDS ON DEMONSTRATION AND RETURN DEMONSTRATION OF ERCP EQUIPMENT- including stone
retrieval balloons and baskets
OBJECTIVES FOR STATION #9
Discuss Case study- Bile leak
48 year old with intermittent RUQ pain presents with fever and severe RUQ pain.
Ultrasound reveals acute cholecystitis.
The patient is taken to the OR for cholecystectomy where dense adhesions are noted. Laparoscopic
procedure converted to open and only partial cholecystectomy was able to be performed.
Bile leak is a common surgical complication
Laparoscopic > Open
Severe inflammation and adhesion is also a risk factor.
Bile leak is suspected with pain post cholecystectomy with imaging revealing biloma
If JP drain is placed, bilious output is diagnostic
HIDA scan can make diagnosis, but does not provide detailed anatomic information
Therapy for bile leak involves
percutanous drainage of the existing leak
ERCP to prevent further leak
Goal of ERCP is to reduce the transpapillary pressure gradient → not necessary to “bridge” the
leak for simple leak
Stenting is better than sphincterotomy alone, however, unclear if stenting plus sphincterotomy is
better than stenting alone

ERCP with CBD stent was placed, pt symptoms resolved over time
Identify and describe various equipment used for stenting the common bile duct and pancreatic duct.
BILIARY PLASTIC STENTS: a plastic tube that is inserted into a bile duct to relieve narrowing of the duct (also called bile duct stricture). Comes in center bend, duodenal bend & double pigtail shapes. Can be placed in CBD or PD BILIARY METAL STENTS: a metal tube that is inserted into a bile duct to relieve narrowing of the duct (also called bile duct stricture). Can be fully covered, partially covered, or uncovered. Design can be open or closed cell
HANDS ON DEMONSTRATION AND RETURN DEMONSTRATION OF ERCP EQUIPMENT- including biliary and pancreatic stents
Source- American Journal of Gastroenterology- www.nature.com - Am J Gastroenterol 2010; 105:100–
105; doi:10.1038/ajg.2009.546; published online 22 September 2009
Assessment of Need for Repeat ERCP During Biliary Stent Removal After Clinical Resolution of Postcholecystectomy Bile Leak

OBJECTIVES FOR STATION #10
Discuss case study- Pancreatic head mass
58 year old with history of CAD presents with progressive jaundice, weight loss and anorexia.
CT reveals a 3.9 cm pancreatic head mass with associated biliary dilatation and pancreatic duct
dilatation.
EUS confirmed a 3-4cm mass in the head of the pancreas. Portal vein was not involved and
the mass was not adjacent to splenic artery.
EUS-FNA revealed adenocarcinoma
ERCP with brushings of pancreatic duct
Pt referred for whipple procedure due to no evidence of metastasis found on CT scan
Since surgery couldn’t be done immediately, a pancreatic stent was placed
From The American Society For Gastrointestinal Endoscopy
The role of endoscopy in the evaluation and treatment of patients with pancreaticobiliary malignancy
Identify and describe various equipment used during ERCP for collection of cells for diagnoses

Cytology Brush: catheter with a brush on the end. Brush is operated by opening and closing the handle
of the device. Used to collect cells from the CBD/PD to diagnose diseases.
SpyGlass Cholangioscopy: Four way steering catheter with four lumens allows for direct visualization of
the duct. EHL and laser probes can be passed to fragment large stones. Biopsy forceps can be passed for
direct visualization biopsies
Hands on demonstration and return demonstration of ERCP brushes and possible Spyglass probes
Note- pancreatic head mass is usually diagnosed through EUS/FNA. This case study was put at
this station randomly, not because brushings or Spyglass is used as a primary method for
diagnosis.