extraanatomische endoskopische intervention - … endoskopische... · extraanatomische...
TRANSCRIPT

Extraanatomische endoskopische Interventionan der Gallenblase und an den Gallenwegen
Georg Spaun

Disclosure
– Boston Scientific: Consultant – USGI medical: Grant and Support – Covidien Medtronic: Support – TaeWoong medical: Support – Pejcl Medizintechnik: Support – GSurg: Support
Georg Spaun, Endo Linz 2017

Endoskopische Standard Intervention an Gallenwegen
Georg Spaun, Endo Linz 2017
▪ ERCP ▪ Experten 95 % bis 97% Kanülierungs Rate ▪ wenn ERCP nicht erfolgreich
▪ ☛ Transfer zu erfahrenerem Endoskopiker ▪ Wiederholungs ERCP in „Referral Center“ in 85 % bis 98 % erfolgreich ▪ Gründe für Scheitern der ERCP bei „Experten“:
▪ veränderte Anatomie nach Chirurgie ▪ Tumorinfiltration ▪ (iuxtapapilläres Divertikel)
▪ scheitert Experte ☛ PTC oder EUS

Georg Spaun, Endo Linz 2017
▪ In the case of failed endoscopic stenting, nonsurgical options that have provided technical success rates of >80% include repeat attempt at ERCP
▪ percutaneous drainage ▪ EUS-guided cholangiography
▪ …..should be reserved to endoscopists at tertiary care centers with advanced training in both EUS and ERCP
Dumonceau J-M et al. ESGE Clinical Guideline for biliary stenting… Endoscopy 2012; 44: 277–292
extraanatomische Intervention an Gallenwegen und Gallenblase
Georg Spaun, Endo Linz 2017
▪ EUS geführtes Rendezvous mit ERCP ▪ EUS geführte Choledocho-
duodenostomie ▪ EUS geführte Hepatico-gastrostomie ▪ EUS geführte Cholecysto-duodenostomie
oder -gastrostomie

Endosonografische Drainage
Georg Spaun, Endo Linz 2017
▪ Standardtechnik: ▪ EUS Punktion mit 19 G Nadel (0,035 Führungsdraht), 22 G
Nadel (0,018 Führungsdraht) ▪ Führungsdraht unter Durchleuchtung eingebracht ▪ transmurale Ballondilatation ▪ Nadelmesser, Dilatationskatheder ▪ spezielles Zystotom (Ringmesser) ▪ Stent eingebracht

Endosonografische Drainage
Georg Spaun, Endo Linz 2017
▪ alternative Technik ▪ 1 Instrument für:
▪ Punktion des Zielorgans ▪ Schneiden und Dilatieren eines
ausreichend weiten Kanals ▪ verankern des distalen Flansches im
Zielorgan ▪ vollständiges Entwickeln des Stents ▪ abdichten der beiden Lumina und Schutz
vor Verrutschen durch zwei Flanschen

Endosonografische Drainage
Georg Spaun, Endo Linz 2017
Georg Spaun, Endo Linz 2017
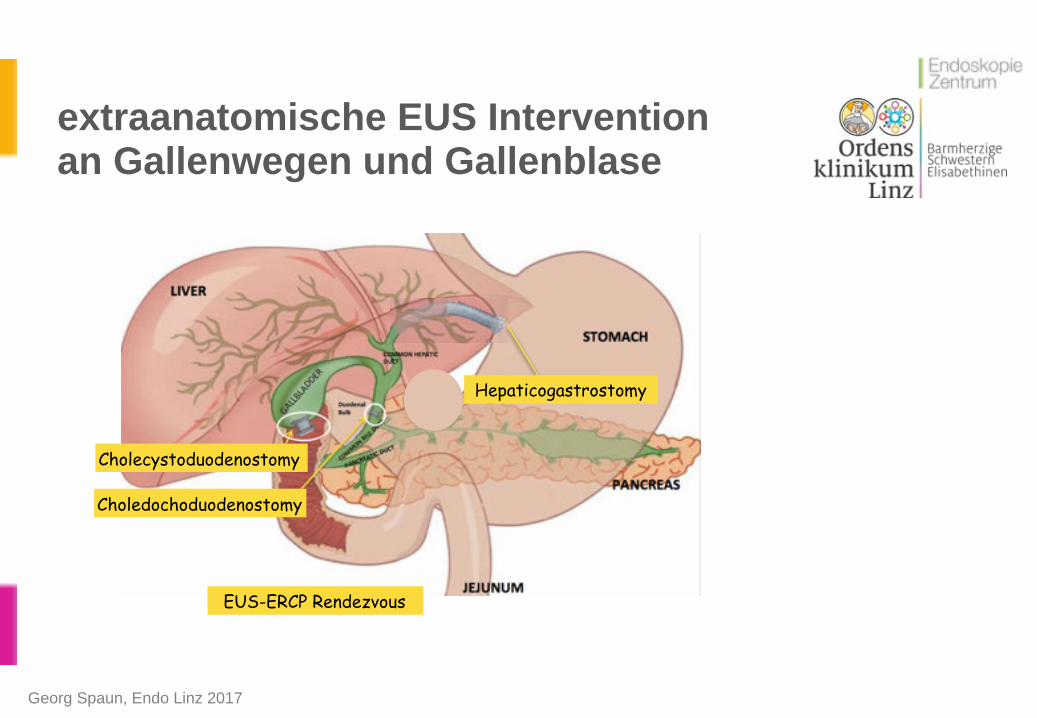
Cholecystoduodenostomy
Choledochoduodenostomy
Hepaticogastrostomy
EUS-ERCP Rendezvous
extraanatomische EUS Intervention an Gallenwegen und Gallenblase

EUS Gallengangsdrainage
Georg Spaun, Endo Linz 2017 Iwashita, Clin J Gastroenterol (2014) 7:94–102

EUS ERCP Rendezvous
Georg Spaun, Endo Linz 2017 Weilert, Surg Endosc (2014) 28:3193–3199

EUS geführte Choledochoduodenostomie
Georg Spaun, Endo Linz 2017

Hot Axios Choledochoduodenostomie
Georg Spaun, Endo Linz 2017
EUS-guided CBD puncture Contrast verification Insertion of guidewire

Hot Axios Choledochoduodenostomie
Georg Spaun, Endo Linz 2017
Distal release of Hot Axios
CBD puncture with Hot Axios
Guidewire loop in CBD

Georg Spaun, Endo Linz 2017
EUS geführte Hot Axios Choledochoduodenostomie

EUS geführte Hepaticogastrostomie
Georg Spaun, Endo Linz 2017

EUS geführte Hepaticogastrostomie
Georg Spaun, Endo Linz 2017

Georg Spaun, Endo Linz 2017
▪ 96 patients (mean age 66years, female 45%, pancreatic cancer 55%) EUS-BD ▪ 5 US, 5 European, 1 Asian, and 1 South American: between October 2012 and
November 2014 ▪ Stent placement (technical success): 92 (95.8 %) pat. (metallic 84, plastic 8) ▪ Mean procedure time: 40 minutes ▪ Clinical success in 86 (89.5 %) patients ▪ 10 (10.5 %) adverse events occurred:
▪ pneumoperitoneum (n=2), sheared wire (n=1) ▪ bleeding (n=1), bile leak (n=3) ▪ cholangitis (n=2), unintentional perforation (n=1)
▪ 4 graded as mild, 4 moderate, 1 severe, and 1 fatal (due to perforation).
Khashab et al., Endoscopy International Open 2016; 04: E487–E496

Georg Spaun, Endo Linz 2017
▪ Stable outpatients without complaints were discharged home after 3 hours of observation
▪ symptomatic (abdominal pain, vomiting, fever) ☛ hospital for observation ▪ 5-day AB ▪ Clinical success: reduction in bilirubin by 50% at 2 weeks, below 3mg/dL at 4 weeks ▪ phone call: day 1, day 7, day 30 ▪ Liver tests:
▪ before the procedure ▪ 2 weeks ▪ 4 weeks after
Khashab et al., Endoscopy International Open 2016; 04: E487–E496

Georg Spaun, Endo Linz 2017
▪ median patient survival: 167 days (95 %CI 112–221) ▪ 6-month stent patency rate was 95% (95 %CI 94.94–95.06 %) ▪ 1-year stent patency was 86% (95 %CI 85.74–86.26%) ▪ extrahepatic approach resulted in 52% decreased risk of adverse events ▪ 36 pat: intrahepatic approach ▪ 56 pat: extrahepatic approach
Khashab et al., Endoscopy International Open 2016; 04: E487–E496

Hepaticogastrostomy or choledochoduodenostomy for distal malignant biliary obstruction after failed ERCP
Georg Spaun, Endo Linz 2017 Artifon at al., Gastrointest Endosc. 2015 Apr;81(4):950-9.
▪ prospective randomized Trial ▪ 25 vs 24 pat. ▪ technical success rate: 96% HPG / 91% CD ▪ clinical success rate: 91% HPG / 77% CD ▪ mean procedural time: 47.8 minutes HPG / 48.8 minutes CD ▪ mean scores of quality of life were similar during follow-up ▪ adverse event rate was 16.3% (20% HPG group and 12.5% CD group) ▪ bile leak required percutaneous bilioma drainage ▪ no statistical difference between the 2 techniques ▪ no difference with regard to survival time

EUS ERCP Rendezvous
Georg Spaun, Endo Linz 2017 Iwashita, Clin J Gastroenterol (2014) 7:94–102
Erfolgsrate: 81 % (215/267)
Komplikationen: 11%

EUS Hepaticogastrostomie
Georg Spaun, Endo Linz 2017 Iwashita, Clin J Gastroenterol (2014) 7:94–102
Erfolgsrate: 87 % (137/158)
Komplikationen: 27%

EUS Choledochoduodenostomie
Georg Spaun, Endo Linz 2017 Iwashita, Clin J Gastroenterol (2014) 7:94–102
Erfolgsrate: 94 % (282/300)
Komplikationen: 19%

Georg Spaun, Endo Linz 2017 Weilert, Surg Endosc (2014) 28:3193–3199
▪ 21 Pat (2,2 % aller Pat für ERCP) ▪ erfolglose ERCP 18/21 (86%) ▪ erfolglose PTC 2/21 (9,5%) ▪ Cholangiogram 21 (100 %) ▪ Procedural success 20 (95.2 %) ▪ Clinical success 19 (90.4 %)

Georg Spaun, Endo Linz 2017 Weilert, Surg Endosc (2014) 28:3193–3199
▪ Anterograde intervention (n = 20) ▪ Anterograde transpapillary SEMS 6 (30 %) ▪ Hepato-gastrostomy SEMS 8 (40 %) ▪ Hepato-gastrostomy plastic 1 (5 %) ▪ Rendezvoux SEMS 3 (15 %) ▪ Transduodenal SEMS 1 (5 %) ▪ Anterograde sphincteroplasty 1 (5 %)
Georg Spaun, Endo Linz 2017 Weilert, Surg Endosc (2014) 28:3193–3199
▪ 1/21 erfolglos (hiläre Obstruktion bei primär sklerosierender Cholangitis) ▪ Führungsdraht durch Papille 10/20 50% ▪ Führungsdraht in kontralateralen Gallengang 10/20 (50%) ▪ Dilatation mit Katheder 17/20 (85%), Needle Knife 3/20 (15%) ▪ Anterograde Interventionen 16/20 (80%) ▪ crossover to rendezvous 3/20 (15%) ▪ Choledocho-duodenostomie 1/20 (5%)

Georg Spaun, Endo Linz 2017 Weilert, Surg Endosc (2014) 28:3193–3199
▪ 16 maligne - 5 Pat mit benigner bilärer Obstruktion ▪ 1 Roux-Y- gastric bypass ▪ 1 chronische Pankreatitis
▪ procedure time: 35 min (range 21-74 min) ▪ 2/20 (9,5%) Galle Leak und Schmerzen (Roux-Y- gastric bypass)
▪ 1 OP Revision (inkomplette Steinentferung ☛ Galle Leak) ▪ adverse event Rate: 9,5%

Zusammenfassung Gallengang
Georg Spaun, Endo Linz 2017
▪ ERCP ist Goldstandard für Gallenwegsintervention ▪ in 2% bis 3% der Fälle ERCP unmöglich, hier EUS Intervention interessante
Alternative zu PTC oder Operation ▪ Unterschied Malignom / benigner Verschluss ▪ Tricks für sichere Intervention:
▪ 2 cm „Lebervorlauf“ ▪ Galle vor Kontrastierung absaugen ▪ „low profile dilatation“ (4 - 5 French)
▪ minimal Needle Knife Einsatz (Park et al., Risk Faktor für adverse events, odds ratio 12.4; P = 0.01)
▪ für Magen unnötig, fibröse Septen um Gallengänge, falls Katheder nicht gleitet)

Endoskopische Intervention an der Gallenblase
Georg Spaun, Endo Linz 2017
▪ akute Cholecystitis ▪ Goldstandard lap Cholecystektomie ▪ Pat unfit für Chirurgie: ▪ perkutane Pigtaildrainage ▪ endoskopische Techniken:
▪ endoskopische transpapilläre Gallenblasen Drainage ▪ Sonderform: Naso-zystische Drainage
▪ EUS geführte Gallenblasendrainage

Endoskopische Intervention an der Gallenblase bei akuter Cholecystitis
Georg Spaun, Endo Linz 2017
▪ Jahr 2004 bis 2013: Cornell University et Columbia University, New York ▪ 139 pat: endoscopic gallbladder drainage ▪ 94 benign ▪ 45 malignant indications ▪ overall success rate: 92% ▪ cystic duct stenting: 117 of 128 cases (91%) ▪ EUS-guided gallbladder drainage: 11 of 11 cases (100%)
Widmer, Kahaleh et al., Clin Endosc 2015;48:411-420
Endoskopische Intervention an der Gallenblase bei akuter Cholecystitis
Georg Spaun, Endo Linz 2017
▪ Complications: 11 cases (8%) ▪ pain (n=3) ▪ stent migration (n=2) ▪ fever (n=2) ▪ pancreatitis (n=1) ▪ sphincterotomy bleed (n=1) ▪ perforation of the gallbladder/bile duct requiring PTC (n=1) ▪ sepsis (n=1)
▪ 9 of the complications: benign indications, 2 in patients with malignancies
Widmer, Kahaleh et al., Clin Endosc 2015;48:411-420

Endoskopische transpapilläre Gallenblasendrainage
Georg Spaun, Endo Linz 2017
▪ retrospective studies: pooled technical success rate of 80.9%.
Widmer, Kahaleh et al., Clin Endosc 2015;48:411-420

Endoskopische transpapilläre Gallenblasendrainage
Georg Spaun, Endo Linz 2017 Widmer, Kahaleh et al., Clin Endosc 2015;48:411-420

EUS geführte extraanatomische Gallenblasendrainage
Georg Spaun, Endo Linz 2017 Widmer, Kahaleh et al., Clin Endosc 2015;48:411-420

Georg Spaun, Endo Linz 2017 Widmer, Kahaleh et al., Clin Endosc 2015;48:411-420
▪ case series: technical success rate of 84% - 100%
EUS geführte extraanatomische Gallenblasendrainage

Georg Spaun, Endo Linz 2017
▪ EUS-guided transmural gallbladder drainage: plastic stents ▪ 22 cases: technical success: 100 % ▪ adverse events: 0 to 37.5 % ▪ pooled adverse event: 18.2 % (4/22)
Anderloni et al., Surg Endosc (2016) 30:5200–5208

Georg Spaun, Endo Linz 2017
▪ EUS-guided transmural gallbladder drainage: SEMS ▪ 10 pat (13.6 %): fully covered SEMS (CSEMS) ▪ 63 pat (86.4 %): partially covered SEMS (PCSEMS) ▪ Clinical success rate: PCSEMS vs CSEMS (98 vs 70 %, p= 0.001) ▪ adverse events: 0 to 33.3 %
▪ pooled adverse event rate: 12.3 % (9/73) ▪ adverse events: more CSEMS (33.3 vs 11.2 %, p = 0.34)
Anderloni et al., Surg Endosc (2016) 30:5200–5208

Georg Spaun, Endo Linz 2017
▪ EUS-guided transmural gallbladder drainage: LAMS (lumen apposing metal stents)
▪ technical and clinical success: 91.5 % ▪ adverse events: 0 to 15.4 % ▪ pooled adverse events: 9.9 % (7/71)
Anderloni et al., Surg Endosc (2016) 30:5200–5208

Endoskopische Intervention an der Gallenblase bei Cholecystolithiasis
Georg Spaun, Endo Linz 2017
▪ case series (n=7) ▪ Shenyang, China ▪ EUS-guided
cholecystoduodenostomy or cholecystogastrostomy
▪ double-flanged fully covered metal stent
▪ ERCP, sphincterotomy: common bile duct stones
▪ 48 h nü
Ge et al. BMC Gastroenterology (2016) 16:9

Endoskopische Intervention an der Gallenblase bei Cholecystolithiasis
Georg Spaun, Endo Linz 2017
▪ 1 week: stent removed ▪ endoscope into gallbladder via
fistula ▪ cholecystolithotomy or polyp
resection ▪ nasobiliary drainage 24 h ☛ DL ▪ ☛ 24 h Gastro ▪ 6/7 fistula closed
Ge et al. BMC Gastroenterology (2016) 16:9

Endoskopische Intervention an der Gallenblase bei Cholecystolithiasis
Georg Spaun, Endo Linz 2017
▪ 1/7 closure ☛ OTSC Clip ▪ US exam: 1, 3, 6 and 12 months ▪ 4 week: gallbladder ejection fraction
was estimated ranging from 80 to 91% (86% on average)
▪ satisfactory functioning at Level 1 ▪ follow up of 3-20months: no stone
recurrence
Ge et al. BMC Gastroenterology (2016) 16:9 DOI 10.1186/s12876-016-0420-9

Zusammenfassung Gallenblase
Georg Spaun, Endo Linz 2017
▪ EUS Gallenblasendrainage ist interessante Alternative zur Cholezystektomie und perkutanen transhepatischen Pigtaildrainage bei Pat. unfit für Chirurgie und akuter Entzündung
▪ Intervention bei fehlender Entzündung dzt. experimentell ▪ Vermeidung externer Drainage ist Vorteil ▪ technischer und klinischer Erfolg sind vergleichbar ▪ Stent Selektion ist entscheidend für Erfolg und niedrigere Komplikationsrate ▪ vergleichende, kontrollierte Studien sind notwendig bzg. Langzeiterfolg und
Kosteneffektivität