evaluating the delivery of extended brief interventions in ... · evaluating the delivery of...
TRANSCRIPT

Evaluating the Delivery of Extended Brief Interventions in specialist alcohol settings: how to improve outcomes for
Higher Risk drinkers?
Laura Pechey University of Stirling
Haringey Advisory Group on Alcohol May 2011
2
Abstract
While Increasing Risk drinkers can access Brief Advice (short, structured advice) through
generalists, and High Risk/dependent drinkers can access specialist alcohol treatment, the
needs of those drinkers who fall between these two groups—known as Higher Risk
drinkers—are often overlooked by both generalist services and specialist alcohol settings.
Extended Brief Interventions (EBI)—short motivational sessions with follow-ups—have been
recommended in national guidance as a means of filling this gap in provision. The present
study sought to explore and evaluate the effectiveness of alcohol specialists delivering EBI
as a form of Brief Treatment (BT).
A literature review was conducted, focusing first on the evidence regarding the
comparative efficacy of Brief Advice (BA) and EBI, and then on comparative studies of EBI
with more intensive treatment. In reviewing the literature, it was concluded that, whilst
there is a broad consensus that BA is as effective as EBI and that BT can be as effective as
intensive treatment, it does not follow that either EBI or more intensive treatment is
ineffective or unnecessary. In spite of some patent flaws in the evidence base, EBI and BT
are legitimate modalities for Higher or High Risk individuals who require more than BA and
less than treatment proper.
In January 2011, a local alcohol service in North London, Haringey Advisory Group on
Alcohol (HAGA)—the author’s employer—introduced EBI as a new treatment option.
Under this new treatment pathway, all clients were to be screened at entry and exit using
the Alcohol Use Disorders Identification Test (AUDIT) in addition to the Treatment
Outcomes Profile (TOPS). All appropriate Higher Risk drinkers (AUDIT score 16-19) were to
be offered one to four EBI sessions instead of longer-term treatment.
The researcher undertook analysis of data relating to HAGA’s EBI client cohort (January-
March 2011), conducted semi-structured interviews with members of this cohort, and
sought commissioner perspectives on EBI through an online questionnaire
During the period under analysis, twelve individuals were allocated as EBI clients; of which
75% (n=9) received EBI. All twelve clients were approached to take part in semi-structured
interviews and 41.67% (n=5) took part; of which 80% had received EBI. The interviews
explored client’s experiences of EBI, and the advantages and disadvantages of alcohol
services providing EBI.

3
At follow-up, all EBI clients had improved AUDIT and TOPS scores, which while subject to
biasing effects, were not negligible. There was a 53.6% reduction in the mean TOPS
drinking days over the last month from entry to follow-up. This is a substantial short-term
change in cohort drinking levels. 100% of EBI clients reported either sustained abstinence
or controlled drinking.
Commissioning leads were not so much interested in debates around terminology but
rather driven by a perceived need to fill an identified gap in provision for Higher Risk and
motivated High Risk drinkers with EBI (or other BT modalities).
The provision of EBI as a form of BT in a specialist service appears to have met the needs of
the majority (80% n=4)) of the follow-up cohort assessed here. The findings of this study
further support the idea that local alcohol services should integrate EBI (and/or other BT
modalities) into their service provision. In order to reach those individuals put off by the
stigma of attending an alcohol service and less motivated to seek treatment,
commissioners should seriously consider specialist-led EBI satellites in primary care and
other settings.
A large-scale longitudinal study of the short- and long-term outcomes for treatment-
seeking Higher Risk and suitable High Risk drinkers allocated to three different study groups
who would either receive EBI as BT in an alcohol setting, receive EBI from a specialist in a
primary care setting, or remain in primary care and receive no support (or only BA) would
test these recommendations.

4
1 Introduction 1.1 Screening Identification and Brief Advice (IBA) is most often undertaken by generalists (i.e. non-
alcohol specialists) and can be either universal or targeted. Of the screening tools
developed, the Alcohol Use Disorders Identification Test (AUDIT) has the most substantial
evidence base (Saunders et al 1993) (Appendix 1). Following screening, the identified risk
level (and clinical judgment) indicates the appropriate intervention (Table 1).
AUDIT scores Risk Level Unit-based definitions (per day) 0-7 Low Risk Men: < 3-4 units
Women: < 2-3 units 8-15 Increasing
Risk
Men: > 3-4 units but not drinking at levels incurring the highest risk. Women: > 2-3 units but not drinking at levels incurring the highest risk.
16-19 Higher Risk Men: > 8 units or > 50 units per week. Women: > 6 units or > 35 units per week.
20+ Dependent Consumption at or above Higher Risk levels plus signs of dependence and/or alcohol-related harm
Table 1. Risk Levels
1.2 Brief Advice Where an individual is at Increasing or Higher Risk, Brief Advice should be delivered. Brief
Advice (BA) comprises short (five minutes), face-to-face, structured advice aimed at
motivating the individual to reduce to within Low Risk levels. BA is modelled on a
Motivational Interviewing (MI) concept: FRAMES (Feedback, Responsibility, Advice, Menu,
Empathy, Self-Efficacy). BA does, however, also involve a degree of practitioner-led
didactic advice.
1.3 Extended Brief Interventions Extended Brief Interventions (EBI) are 20-40 minute one-to-one sessions based on the
therapeutic principles of MI and health behaviour counselling (Rollnick et al. 1999; Miller &
Rollnick 1991). EBI requires significantly more intensive assessment, training and clinical skill
than BA. EBI is offered after BA to patients who:
o request further help or, in the practitioner’s view, need further help ; o and/or are ambivalent about change; o and/or are at Higher Risk (AUDIT score 16-19).
Higher Risk drinkers are likely to be experiencing physical and/or mental health alcohol-
related problems (ARP), such as dependence or injury.

5
The aim of EBI is to motivate the individual to achieve the reduction, or cessation, of
alcohol use. Unlike BA, EBI involves up to four follow-ups and is non-didactic. Practitioners
use the client’s levels of confidence and motivation to tailor sessions that promote
“change talk” (See Appendix 2). Clients are supported in developing and reviewing a
reduction plan with strategies for negotiating difficult situations. At exit, the success of the
intervention is assessed and the client either makes a planned exit or, where the desired
changes have not been achieved, is referred into higher threshold support.
1.4 Brief Treatment Brief Treatment (BT) has been defined as:
relatively briefer forms of treatment delivered by therapists or counsellors working in alcohol or addiction specialist agencies to those who are seeking, or have been mandated or persuaded to seek, help for their alcohol problems. (Heather 2004)
BT could take the form of EBI, Cognitive Behavioural Therapy (CBT), Motivational
Enhancement Therapy (MET), or other psychosocial models. Clients who are treatment-
seeking or compelled into treatment are likely to be complex, with longer alcohol misuse
histories, and mild to moderate dependence (Heather 1996, 2004, 2011). BT is classified as
a clinical ‘Tier 3’ intervention (MoCAM 2005). The often-blurred divide between EBI and BT
is explored in depth in the literature review below.
2. Literature Review A preliminary literature search was undertaken using the University of Cambridge’s online
search facility Cross-Search, limiting the journal subjects searched to “Social Sciences and
Humanities” and “Health and Medicine.” Keywords searched were “alcohol” plus either
“extended brief interventions,” “briefer treatment,” “brief treatment,” “brief lifestyle
counselling,” or “brief interventions.” Cross-referencing relevant articles supplemented this
search.
2.1 BA versus EBI trials Since the 1970s, IBA has been consistently validated by research in primary care and, to a
lesser extent, in A&E/hospital settings (Heather et al 1987; Wallace et al 1988; Anderson &
Scott 1992; Babor & Grant 1992; WHO 1992; WHO 1996; Gentilello et al 1999; Ockene et al
1999; Nilsen et al 2008). Meta-analytic reviews have corroborated this research (Bien et al
1993; Wilk et al 1997; Moyer et al 2002; Kaner et al 2007). One hugely influential review of
thirty-two controlled trials concluded that one in every eight individuals who receives BA

6
will reduce to Low Risk levels (Moyer et al 2002). Some counter-evidence has tempered
these positive findings (i.e. Emmen et al 2004).
Early IBA studies hypothesized that longer, repeated and more intensive interventions
would increase positive outcomes via a ‘dose-response’ effect (WHO 1992, 1996). Some
primary studies and meta-analytic reviews support the dose-response hypothesis
(Robertson et al 1986; Richmond 1995; Israel 1996; Aalto 2000; Maisto 2001; Longabaugh et
al 2001; Poikolainen 1999; Ballesteros et al 2004). One major review concluded that EBI
(differentiated here by multiple sessions) was effective for women but not men, with an
average treatment effect of -51g of alcohol per week (Poikolainen 1999). However, whilst
researchers broadly agree that extended interventions are effective, the vast majority of
reviews have found no additive effect for extended interventions over BA in either
treatment or non-treatment–seeking populations (Bien et al 1993; Freemantle et al 1993;
Moyer et al 2002; Ballesteros et al 2004; Kaner et al 2007).
In accounting for this lack of additive power, researchers have pointed to uncontrolled
factors, such as the type of sample, ‘regression to the mean,’ ‘assessment effect,’
therapist style, motivation levels on entry and the precise nature of the interventions
delivered (Hall & Heather 1991). High dropout rates (and hence low follow-up) are
perhaps the most obvious biasing effect, since compliant and motivated individuals are
likely to be over-represented in follow-up data (Ballesteros et al 2004). Recruitment via
advertisement and the exclusion in some studies of those with mental health problems,
homelessness, dependence, drug use, the unemployed or unmarried have left reviewers
questioning the real-world significance of such research (Miller et al 1993, Drummond et al
1990; WHO 1996). The calculation of treatment effect is also problematized by lengthy
and repeated screening and assessments, both of which incorporate aspects of BA (i.e.
feedback, identifying risks). What is more, definitions of BA, EBI or BT are by no means
consistent across studies. BA ranges in studies from ten to 180 minutes with up to three
follow-ups, while EBI-style interventions range from twenty to seventy-five minutes with up
to twelve follow-ups (Wilk et al 1997; Gentilello 1999; Longabaugh et al 2001; Moyer et al
2002). The range of extended intervention models—EBI, Brief Counselling, BT, MET, brief
coping skills, CBT—further complicates comparative analysis.
2.2 BT versus intensive treatment trials The consensus view that EBI has no additive effect over BA should not be misconstrued.
Heather has drawn attention to a distinct line of research that positively compares BT to
7
more intensive treatment, arguing that this serves to support the delivery of BT (which
might, for example, take the form of EBI) in specialist settings (2004, 2011).
Heather traces this research line to a 1977 study in which married males (n=100) were
assessed (three-hours) and allocated either to conventional inpatient or outpatient
treatment, or a session of couples counselling with a psychiatrist (Edwards et al 1977). At
one-, two- and twelve-year follow-up, no statistically significant differences were evident
between these groups (Edwards et al 1977 & 1983). The selection of relatively stable
employed married men and the failure to factor in any additional support accessed have
faced criticism (Mattick & Jarvis 1994; Monahan & Finney 1996). Project MATCH—an
influential 1997 study of 1726 alcohol dependent volunteers, which found no clinically
significant differences between BT (four MET sessions) and more intensive treatment
(twelve sessions)—has been subject to similar criticisms about the biasing effect of
choosing relatively motivated individuals (Peele 1997).
Other BT trials have successfully minimised such design flaws. Women and unmarried
individuals were included in a 1988 BT trial conducted at an alcohol service (Chick et al
1988). Individuals (n=152) were allocated to advice (one-off five minutes), “amplified
advice” (up to sixty minutes of psychiatrist-led MI), extended inpatient or extended
outpatient treatment. At two-year follow-up, the extended cohort had less ARP but had
not reduced their alcohol consumption more than either advice groups. In 1990,
Drummond et al sought to analyse the benefits of specialist versus primary care treatment.
A sample (n=40) of problem drinkers referred to an alcohol clinic was assessed (three-
hours) and given BA by specialists, before being randomized either to on-going outpatient
counselling in the clinic or referral to their GP for monitoring. On six-month follow-up, there
were no statistically significant differences in outcomes between groups and no benefit in
specialist support for higher pre-treatment alcohol consumption levels. The study design
should not however be taken as a realistic comparison of specialist versus GP support,
since the GP group received a highly enhanced version of GP care, involving specialist
visits to support the practitioner in patient management. ‘Assessment effect’ could again
arguably be responsible for a large part of the treatment effect in both studies.
Taking a different angle on BT, a more recent study has explored whether BT acts as a
pathway into more intensive support (Krupski et al 2010). Of 1365 BA patients referred for
BT, 20% (n=278) participated in BT within a year. BT patients were significantly more likely to
access further specialist support (regardless of previous treatment history) compared to

8
non-BT patients and were most likely to do so immediately after BT. The study’s definition
of BT is, however, questionable, since up to twelve sessions (with an average of eight) is
arguably as intense as intensive twelve-week treatment modalities. Since the researchers
do not describe any assessment beyond alcohol and drug screening and there were no
exclusions except under 18s and over 65s, this study largely eliminated two major flaws
typical of BT studies: selection bias and assessment effect. However, setting the measure
of engagement in further treatment as simply admission does not seem to be an honest
reflection of whether BT acts as a pathway into support. Moreover, it might be argued
that professional input and liaison facilitated access into treatment rather than the BT itself
(Wright et al 1998).
2.4 Conclusion Whilst there is a broad consensus that BA is as effective as EBI and that BT can be as
effective as intensive treatment, it does not follow that either EBI or more intensive
treatment is unnecessary or ineffective. In spite of flaws in the evidence base, EBI and BT
are legitimate modalities for motivated Higher Risk or High Risk individuals requiring
something more than BA and less than treatment proper and who are assessed as suitable
for motivational interventions.
3. Methodology The present study focused on those individuals allocated as EBI clients at a community
alcohol service, Haringey Advisory Group on Alcohol (HAGA), between January and
March 2011 (For HAGA pathway, see Appendix 5). Since this study is both exploratory and
evaluative, the research design incorporates qualitative and quantitative approaches. All
aspects of methodology are modeled on Matthews & Ross (2010). A word on
terminology: whilst EBI delivered in an alcohol setting constitutes a form of BT, the
intervention delivered at HAGA was a specifically EBI model and so is referred to as EBI
throughout.
3.1 Documentation/data analysis The analysis of documentation and data related to the cohort (i.e. entry and exit AUDIT
and Treatment Outcomes Profile [TOPS] scores) was the first stage of research. Designed
by the National Treatment Agency (NTA), TOPS is a twenty-item tool measuring health and
social functioning used at entry, review and exit. Both AUDIT and TOPS are evidence-
based measures of reductions in drinking and improvements in social functioning
(Saunders et al 1993; Marsden et al 2008). The use of standardised research tools allows

9
small-scale study results to be tested on a larger scale for replicability. The EBI worksheet
used at HAGA (designed by the researcher) is modeled on that used in a major on-going
trial (Appendices 2 and 3) (Coulton et al 2009).
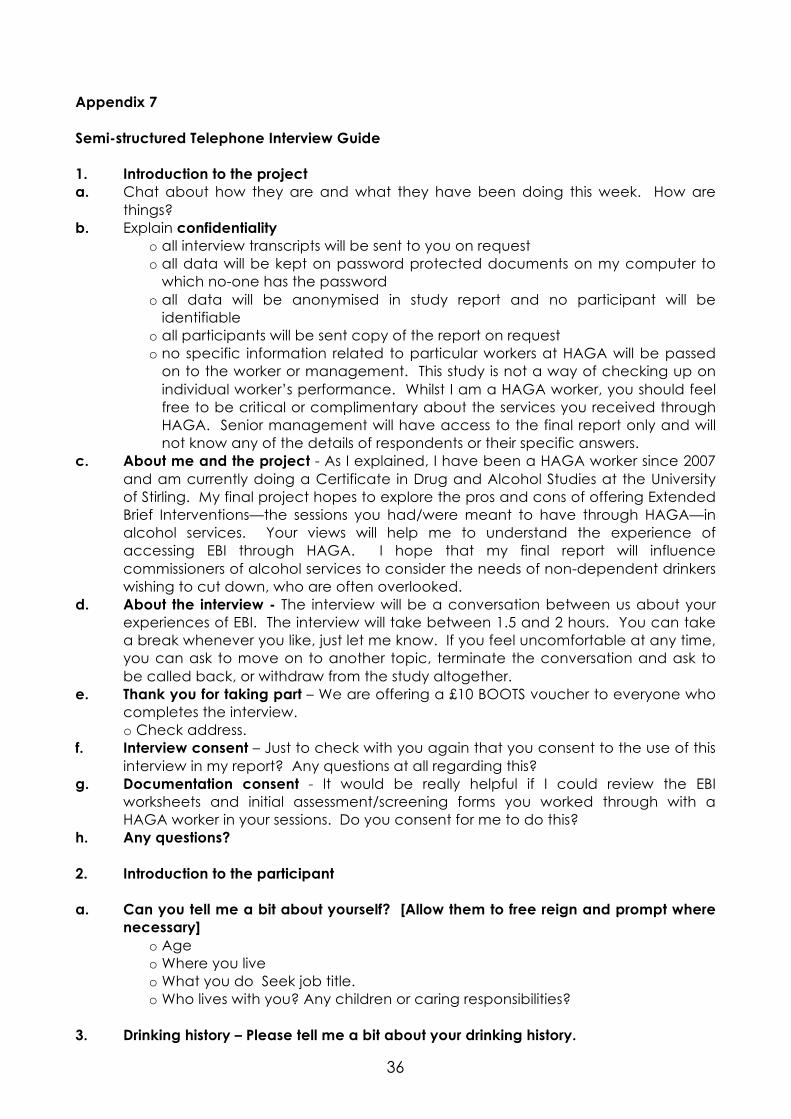
3.2 Semi-structured interviews Those individuals who were allocated as EBI clients during Quarter Four 2010-2011
(including those who did not engage) were approached to participate in the study.
Since the sample was small (n=12), semi-structured telephone interviews were considered
the best means of gleaning detailed qualitative responses. A telephone interview was
thought advisable to ensure confidentiality, reduce health and safety risks, and avoid the
biasing effect of interviews being conducted at HAGA. The interviews explored drinking
history, expectations and experiences of EBI via an alcohol service, and barriers to support
(Appendix 7). The collation of three sets of AUDIT and TOPS scores from entry, exit (both
Quarter Four 2010-2011) and at follow-up (Quarter One 2011-2012) was undertaken to
explore self-reported changes in drinking and well-being. Whilst self-reported data is not
unproblematic, this data has been shown to be accurate when checked against
biochemical data (WHO 1996).
A small, in-depth study of a self-selecting sample inevitably introduces bias and faces
potentially low response rates. To encourage participation, a £10 voucher was offered as
an incentive. Patients accessing EBI through an alcohol service are likely to be motivated
and/or have serious/complex problems. Compliant and/or motivated clients are likely to
both participate in the study and report positive outcomes. Attempts were therefore
made to recruit those clients who did not engage or made an unplanned exit. Since the
researcher’s employment at HAGA may also have introduced bias, the researcher made
it clear that respondents should be candid in their responses (Appendix 7). In a study of
this size, it was not feasible to control for all the potentially confounding factors or to
produce statistically powerful results.
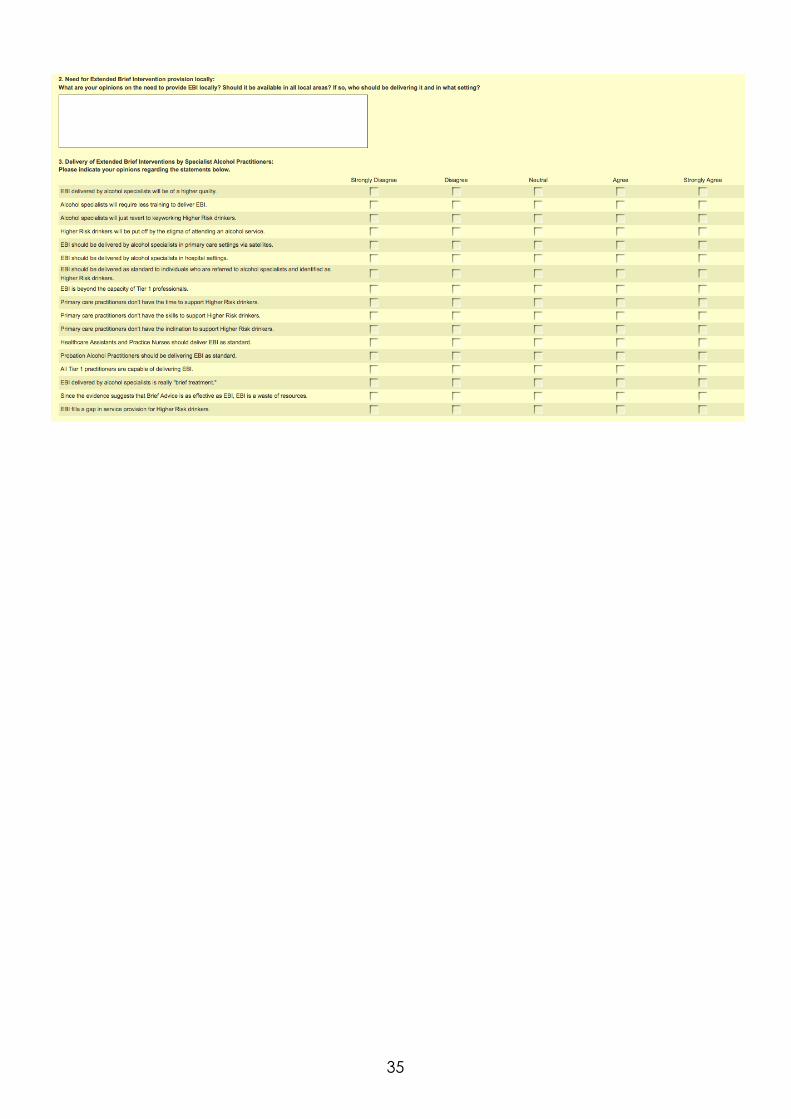
3.3 Questionnaire To scope commissioning perspectives on EBI, an online questionnaire was emailed to
commissioning leads in the thirty-three London boroughs (Appendix 6). An online survey
was considered to be the most effective means of eliciting responses from busy
professionals with daily Internet access. The questionnaire asked about the provision of
interventions in borough and explored perspectives through value statements and free
text responses.

10
4. Findings 4.1 Documentation/data analysis 4.1.1 Sample Twelve individuals were allocated as EBI clients during the study period. 4.1.2 Demographics The gender distribution of the sample (n=12) was 50% male (n=6) and 50% female (n=6).
Sample ethnicity was 41.67% White British (n=5), 41.67% White Other (n=5), 8.33% Black
British (n=1) and 8.33% Black Other (n=1). Ages ranged from 28 to 66 with a mean age of
42.
4.1.3 Substance history The mean age of first alcohol use was 17 and the range was 13-20. Two individuals
(16.67%) had undergone previous alcohol treatment; of which 50% (n=1) at HAGA and
50% (n=1) elsewhere. Only 16.67% (n=2) used other substances.
4.1.4 Referral
Fig. 1 Referral Sources 4.1.5 AUDIT/TOPS Of those clients allocated to EBI, 8.33% (n=1) were Increasing Risk (AUDIT score 8-15),
16.67% (n=2) were Higher Risk (AUDIT score 16-19), 58.33% (n=7) were High Risk (AUDIT score
20+) and 16.67% (n=2) did not have entry AUDIT scores recorded. The mean entry AUDIT
score (n=10) was 25.7 (High Risk).
11
For ease of reference, mean AUDIT and TOPS scores are shown in Section 4.2.3 and 4.2.4
alongside follow-up scores.
4.1.6 EBI 66.67% (n=6) of EBI clients attended one session, 22.22% (n=2) attended two sessions and
one individual (11.11%) attended four sessions. The mean number of sessions attended
was 1.16. Of the sample (n=12), 75% (n=9) engaged in EBI.
4.1.7 Assessment & discharge 33.33% (n=4) of the sample was comprehensively assessed either before or after EBI. At
the time of analysis, 83.3% (n=10) had been discharged and 16.7% (n=2) remained in
service; one of which had an intra-agency referral for counselling. Of the 11 discharges,
72.7% (8) were planned and 27.3% (n=3) unplanned.
4.2 Semi-structured interviews 4.2.1 Sample All twelve individuals were contacted via telephone to invite them to participate in the
study. 58% (n=7) agreed but only 41% (n=5) participated. Of these, 20% (n=1) had
disengaged after comprehensive assessment without receiving EBI or any other
intervention. The non-intervention individual was interviewed to ascertain reasons for non-
engagement. The mean follow-up time for all interviewees (n=5) was ten weeks (range: 8-
12).
The follow-up intervention sample (n=4) was 50% (n=2) female and 50% (n=2) male, and
75% (n=3) White Other and 25% (n=1) Black British. The mean AUDIT score for the followed
up intervention sample (n=4) was 30.75.
Gaps in entry and exit AUDIT, TOPS, and motivation/confidence scores problematised the
comparative analysis of this with follow-up data. Complete entry and exit AUDIT and TOPS
scores was available for only 16.67% (n=2) of the entry cohort (n=12). Entry and exit
confidence/motivation levels were available for 0% of the sample. Consequently, values
for entry and exit AUDIT and TOPS had to be calculated as the mean of the data
available at entry, exit and follow-up (Fig. 3 & 4).
4.2.2 EBI sessions

12
Clients described EBI sessions as “relaxed,” “optimistic,” “reassuring,” whilst also “intense.”
One respondent noted the difference between EBI and counselling, explaining:
we talked about the way things are, I could ask questions about alcohol, It was a framework I could cling to … it felt practical, felt socially orientated, made me feel part of a community.
All interviewees commented on either the “client-centred” or “non-judgmental” nature of
the sessions. One respondent, who “wouldn’t have allowed [making a six-step plan as per
the format]” described EBI as “more of an interaction” focused on “motivation and
listening not jumping through hoops.” 50% (n=2) valued some cautionary tales about the
“effects on family” from the worker’s professional experiences with severe alcohol
misusers. Respondents also valued having the same worker (50% n=2) and re-reading their
plan (50% n=2) after the session. One individual felt that the session could have been
improved by an explanation of the “framework” and theory behind it.
None of the respondents had sought other support alongside EBI but one individual had
since been attending weekly Alcoholics Anonymous (AA) meetings. Workers integrated a
variety of tools/self-help literatures (i.e. drink diaries) and Relapse Prevention (RP)
techniques—“urge-surfing,” the “three-month itch,” and “six-month itch”—into the EBI
model. 75% (n=3) of the intervention follow-up group valued such metaphorically
powerful ways of conceptualising fighting urges.
100% (n=4) of intervention group respondents rated rapport and alcohol expertise as the
most important aspects of EBI sessions, and would recommend EBI as an effective way to
help people reduce their drinking.
4.2.3 AUDIT The mean reduction in AUDIT scores from sample entry (n=10) to follow-up of the
intervention group (n=4) was 24.12% (25.7 to 19.5).

13
Fig. 2. Mean AUDIT scores at entry, exit and follow-up (y axis). For the members of the intervention group, who had entry and follow-up AUDIT scores
(n=4), the reduction was far greater: 30.75 to 19.5; a mean reduction of 37%.
4.2.4 TOPS The mean reduction in TOPS drinking days score from sample entry (n=6) to intervention
group follow-up (n=4) was 53.57%. For those of the intervention group who had entry and
follow-up drinking days scores (75% n=3), the mean reduction was 100% reduction, since
all were abstinent.
14
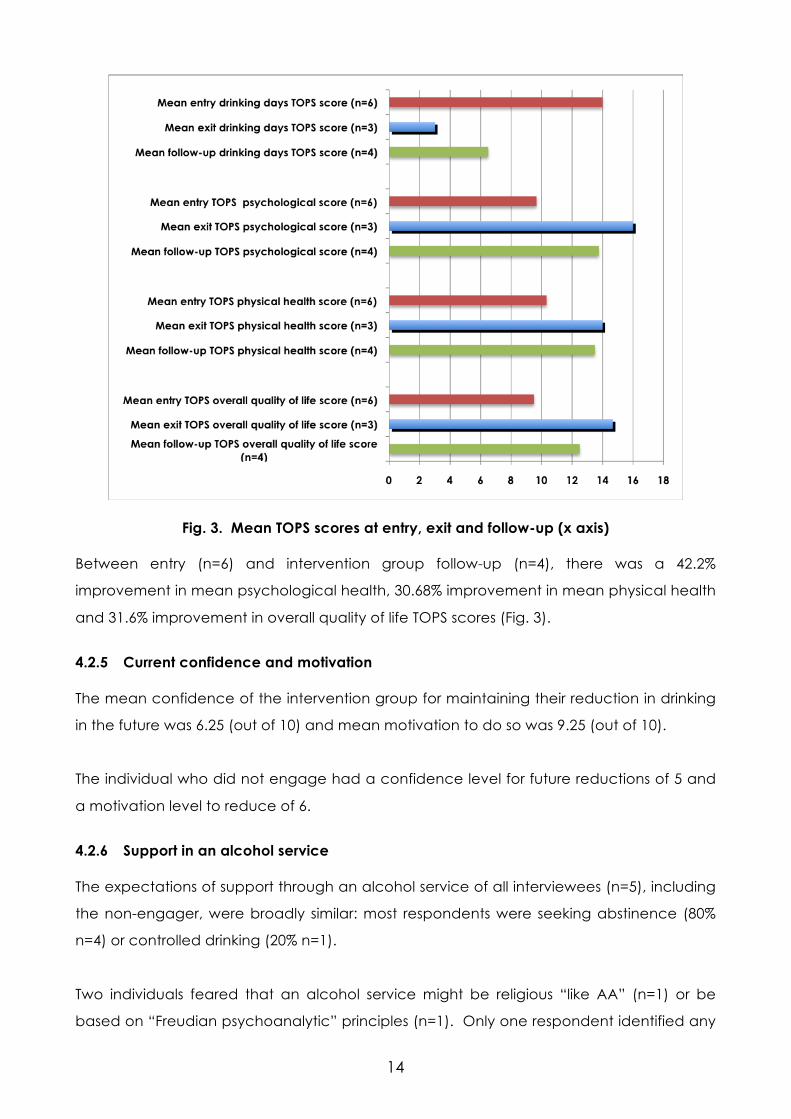
Fig. 3. Mean TOPS scores at entry, exit and follow-up (x axis) Between entry (n=6) and intervention group follow-up (n=4), there was a 42.2%
improvement in mean psychological health, 30.68% improvement in mean physical health
and 31.6% improvement in overall quality of life TOPS scores (Fig. 3).
4.2.5 Current confidence and motivation The mean confidence of the intervention group for maintaining their reduction in drinking
in the future was 6.25 (out of 10) and mean motivation to do so was 9.25 (out of 10).
The individual who did not engage had a confidence level for future reductions of 5 and
a motivation level to reduce of 6.
4.2.6 Support in an alcohol service The expectations of support through an alcohol service of all interviewees (n=5), including
the non-engager, were broadly similar: most respondents were seeking abstinence (80%
n=4) or controlled drinking (20% n=1).
Two individuals feared that an alcohol service might be religious “like AA” (n=1) or be
based on “Freudian psychoanalytic” principles (n=1). Only one respondent identified any

15
disadvantages in attending an alcohol service: “I don’t think I would have gone to HAGA
if not through my GP … To walk into an alcohol centre is to kind of identify.” The
advantages of seeking support through an alcohol service were identified as expertise
(n=4) and dedication/commitment (n=3). Two respondents also discussed the sense of
“community” it brought being alongside “really long-term badly damaged people from
different walks of life. You could sense it worked but also that you could degenerate
quickly too.”
100% (n=5) of respondents—including the non-intervention respondent—would
recommend that problem drinkers contact an alcohol service.
4.3 Questionnaire 4.3.1 Response Rate The response rate according to borough was 57% (19 of 33). This may have been
adversely affected by strain on commissioners due to funding cuts, redundancies and
sector reorganisation. 30.4% (n=7) of those who started the questionnaire (n=23) did not
complete. It is evident that some respondents skipped answers where the response rates
per item are inconsistent with the rate for the whole question. In Tables 2 and 4, it was
therefore assumed that a respondent had no practitioners conducting IBA or EBI where
they didn’t give an answer and figures for “None” were adjusted accordingly. Otherwise,
response rates were calculated according to the number of survey respondents who
answered a particular question.
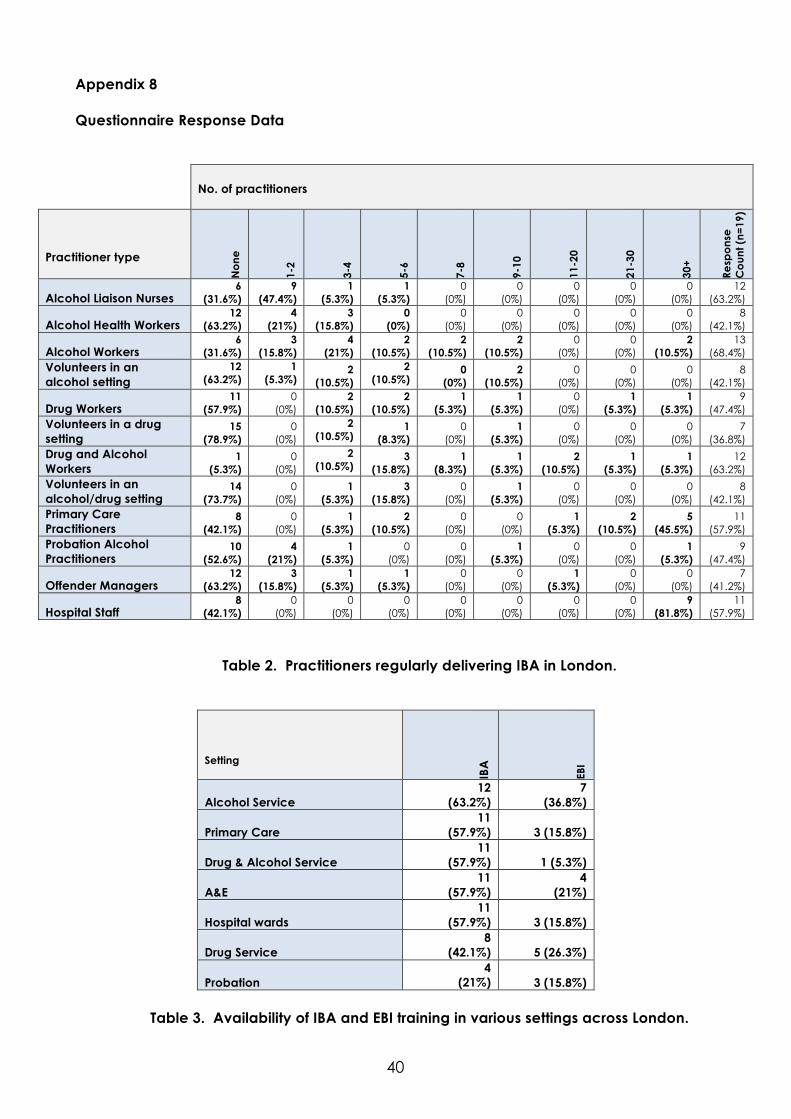
4.3.3 Commissioner’s responses The tabulated data from the questionnaire is in Appendix 8 and summarized below.
The delivery of IBA is becoming embedded across the region with respondents reporting a
range and number of IBA practitioners, predominantly in substance misuse services, and
primary and acute settings, with alcohol project workers (68.4%) taking the lead (Table 2).
Training to support IBA delivery is available in a variety of settings, most widely in alcohol
services (63.2%) (Table 3).
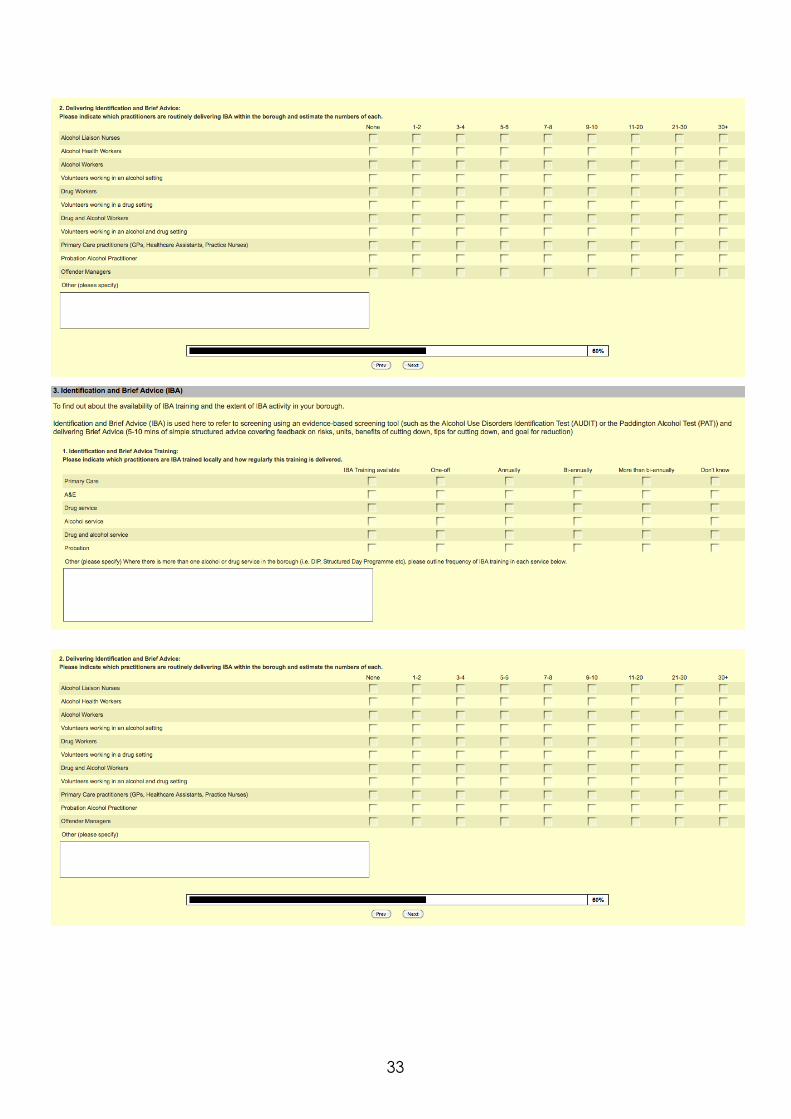
Whilst many practitioners are delivering EBI—most widely, alcohol workers (73.7%), drug
and alcohol workers (63.1%), Alcohol Liaison Nurses (57.9%), hospital staff (57.9%), and
primary care practitioners (36.8%)—the total number of practitioners is substantially less
than for IBA (Table 4). It is strikingly evident in Table 3 that EBI training is in limited supply: for

16
example, whilst alcohol workers are delivering EBI in 73.7% of areas, only 36.8% of local
areas have EBI training available for alcohol workers.
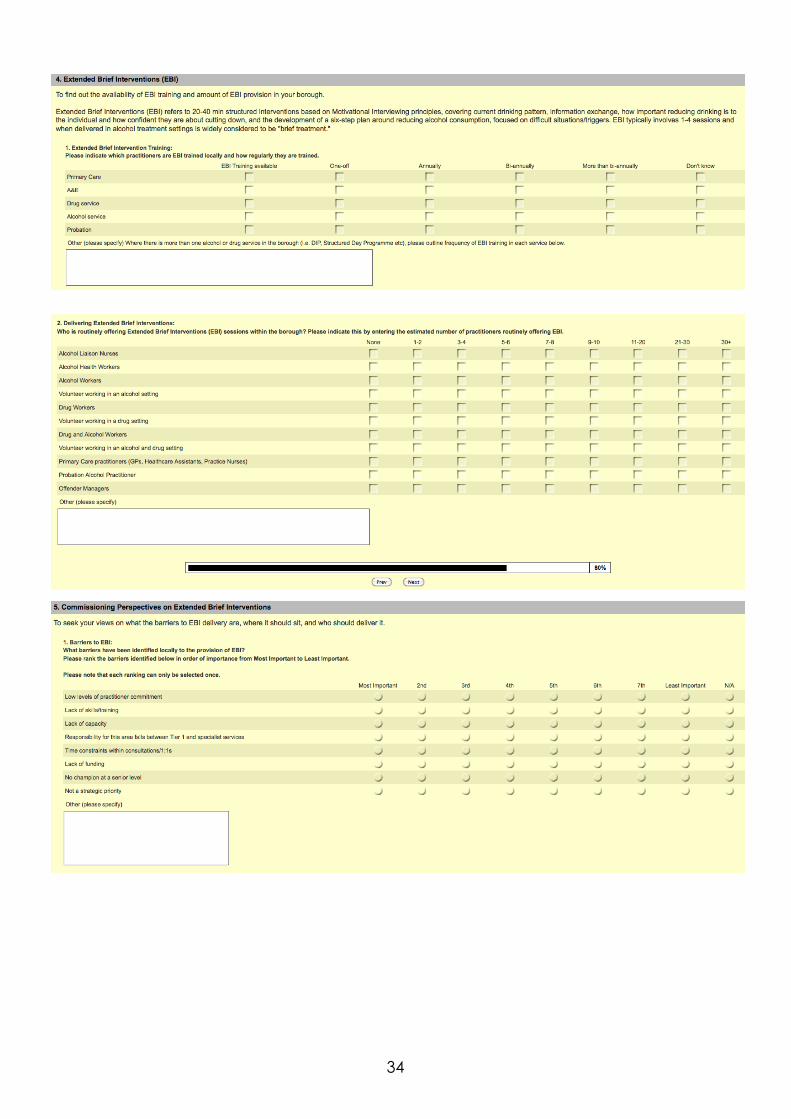
Lack of capacity was identified by 50% (n=6) of respondents as the biggest barrier to EBI
implementation, while 25% (n=3) felt lack of funding was the primary factor. The
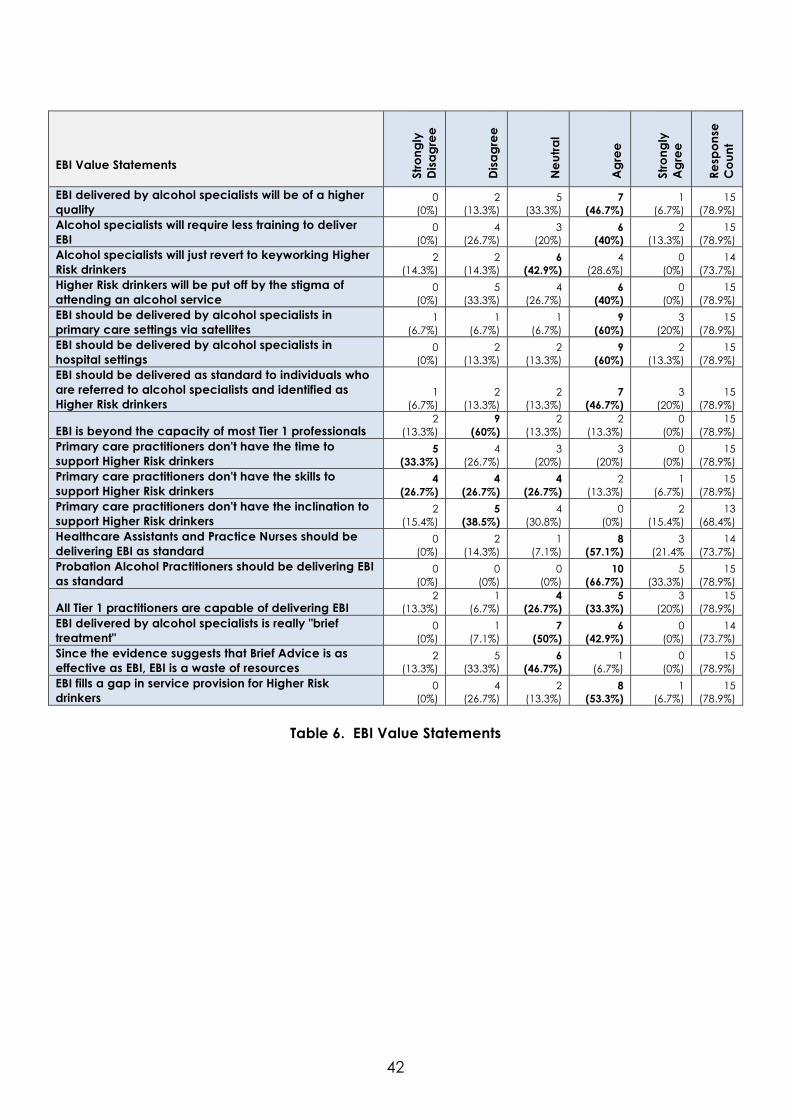
importance of Tier 1 for EBI delivery was widely acknowledged with 60% (n=9) disagreeing
with the notion that EBI is beyond Tier 1 practitioners’ capability. Support for developing
EBI activity in Tier 1 was tempered by cautions that non-specialists need close-working
relationships with alcohol specialists. There was also considerable reference to the
importance of individual practitioners’ skills in ensuring positive outcomes and the related
need for high quality rolling MI training (mentioned by almost half of respondents (n=6)).
Many respondents 53.3% (n=8) acknowledged that the gap in provision for Higher Risk
could be filled by EBI. The need to fully embed IBA before EBI can be developed was,
however, also expressed. 46.7% (n=7) agreed that EBI should be delivered to individuals
referred to alcohol services and identified as Higher Risk. Since 60% (n=9) felt that Higher
Risk drinkers would be put off by the stigma of attending an alcohol service, many
respondents agreed that alcohol specialist-led satellites in primary care (60% n=9) and
hospital settings (60% n=9) were the answer to EBI delivery.
5. Discussion 5.1 EBI client profile The EBI cohort’s gender (50/50) and ethnicity (84% White/16% Black, Asian, Minority, Ethnic
and Refugee (BAMER)) are not representative of the service as a whole, which is over-
represented by men (70/30) and more ethnically diverse (70/30). The cohort’s ethnicity
may be attributable to on-going primary care IBA pilots in an area of the borough with a
smaller BAMER community. The over-representation of women in the cohort is perhaps
due to relatively lower levels of consumption amongst women compared to men. The
high level of EBI-appropriate GP referral (50%) is again perhaps due to local IBA activity,
especially the GP IBA pilots (Fig. 1).
Only 16.67% of the cohort had undergone previous alcohol treatment (n=2). It is
consistent with best-practice guidance and evidence of good care-planning (based on
the principle of “stepped care”) that treatment-naïve clients were allocated to a lower
threshold interventions, such as EBI (Sobell & Sobell 2000).

17
Entry-level AUDIT scores are of particular interest. It was hypothesized that the introduction
of EBI into the range of interventions available in an alcohol treatment service would serve
to meet the needs of Higher Risk drinkers. However, only 16.67% (n=2) of the cohort scored
as Higher Risk. 8.33% (n=1) of the entry cohort scored at the top end of Increasing Risk and
was assessed as requiring something beyond BA. The remaining 75% (n=9) scored as High
Risk but were considered suitable for EBI, most likely on the basis of their presenting
motivation levels. It seems that EBI served alcohol specialists as a means of meeting the
needs of highly motivated Higher and High Risk individuals. The client notes of the non-
engager interviewed suggest that EBI was considered a means (unsuccessful in this
instance) of motivating an individual ambivalent about engaging in more intensive
support.
5.2 Client perspectives and outcomes It is fully recognised that those clients who agree to follow-up are likely to be the more
compliant and therefore more likely to report positive outcomes. This, along with the
small, self-selecting nature of the cohort as a whole, introduces clear bias into the findings
of the present study, which did not have the capacity to set up comparative control
groups.
The EBI sessions described by clients—client-centred, non-judgmental, and focused on the
present and future—were largely faithful to the spirit of EBI. However, whilst some clients
appreciated not being subjected to cautionary tales about the harms of alcohol, others
specifically requested that practitioners tell them such stories from their professional
experience of alcohol-related harm. Didactic advice of this nature may seem to fly in the
face of EBI or MI theory. However, since clients elicited these stories, stories of this type
appear to have been motivational for particular individuals.
There were notable improvements in AUDIT and TOPS scores between entry and follow-up
(Fig, 2 & 3). Entry and follow-up scores are the most reliable as similar numbers are
represented (although only intervention clients are included in follow-up scores). The exit
scores for both should, however, be viewed with caution as the individuals represented
therein (n=3) made planned exits and hence were most likely to be highly motivated and
stable. Since AUDIT scores include historical measures of drinking behaviours in the last
year (five questions) and lifetime incidence (two questions), twelve month follow-up would
have been required to get an accurate reflection of any long-term changes. The 53.6%

18
reduction in TOPS drinking days score (based on the last month) is more indicative of the
short-term changes in drinking reported.
The high number of EBI clients followed up who had achieved abstinence (50% n=2) was
in line with client’s goals on entry. 50% (n=2) of the intervention follow-up sought
abstinence as a goal. One respondent did not feel, however, that she had personally
chosen abstinence over controlled drinking. It is possible that alcohol practitioners used to
working with severely dependent or complex clients urge abstinence as the goal of
treatment without sufficiently exploring client’s own goals.
It is unsurprising that at follow-up EBI clients were more motivated to maintain change
(9.25) in drinking than they were confident (6.25) about achieving this. The absence of
data around entry confidence and motivation levels means comparison with follow-up is
not possible. The minimal contact time required by most of the EBI clients was particularly
striking; of the follow-up intervention group, only one individual engaged in four sessions,
one individual attended two and two others attended a single session. This possibly
reflects high levels of entry motivation.
The extent to which clients’ valued alcohol expertise—in particular their specialist ability to
provide metaphorically powerful ways of conceptualizing alcohol urges—and the special
dedication of alcohol practitioners to alcohol misuse, supports the need for alcohol
specialists to deliver EBI. It was not anticipated that, when asked to focus on the pros and
cons of seeking support in an alcohol service, two individuals would value a sense of
“community” with other alcohol users, specifically dependent/complex cases. This was
notably, however, an advantage realised only in retrospect and not something
anticipated by respondents pre-entry. The stigma related to attending an alcohol service
therefore remains a significant barrier to even the more motivated Higher Risk or High Risks
drinkers accessing EBI in this setting.
5.3 Commissioning perspectives IBA is high on the commissioning agenda and increasingly well-embedded across London.
Many respondents openly acknowledged that their knowledge of the exact extent of EBI
activity in borough is currently hazy. Worringly, the provision of EBI training is lagging well
behind EBI activity. There is nevertheless a strong commitment to extending EBI provision.
Commissioners remained neutral about debates around terminology, focusing instead on

19
the need to fill an identified gap in provision for Higher Risk and motivated High Risk
drinkers.
5.4 Conclusions The commissioning perspective on EBI is no doubt influenced by recommendations that
local areas explore EBI and BT provision (MoCAM 2005; Dept. of Health 2009; NICE 2010;
NICE 2011). Whilst the small-scale nature of this study reduces the reliability of its findings,
the fact that 100% of the EBI group followed up had achieved controlled drinking or
abstinence should not be devalued. In accordance with the pragmatic line taken in a
recent article by Heather, the provision of EBI to Higher Risk and suitable High Risk drinkers
is supported by this study (2011). Where BA is not successful, a higher-level modality not
equal to intensive treatment is required on the basis of ‘stepped care’. Alcohol specialists
seem best placed to deliver these interventions, clients clearly value specialist input. The
provision of EBI as a form of BT in a specialist service appears to have met the needs of a
motivated treatment-seeking client group. The findings of this study therefore support the
idea that local alcohol (and, for that matter, substance misuse) services should integrate
EBI (or other BT treatment modalities) into their service provision. In order to reach those
individuals put off by the stigma of attending an alcohol service, commissioners should
seriously consider specialist-led EBI satellites in primary care and other settings. A large-
scale longitudinal study of the short- and long-term outcomes for groups of treatment-
seeking Higher Risk and mildly dependent High Risk drinkers allocated to three different
study groups who would either receive EBI as BT in an alcohol setting, receive EBI from a
specialist in a primary care setting, or remain in primary care and receive no support (or
only BA) would test these recommendations.

20
References Aalto, M., R. Saksanen, P. Laine, R. Forsstrom, M. Raikaa, M. Kiviluoto, K. Seppä, & P. Sillanaukee, (2000) “Brief intervention for female heavy drinkers in routine general practice: a 3-year randomized, controlled study,” Alcoholism: Clinical and Experimental Research, 24:11, 1680–6. Anderson, P. & E. Scott, (1992) “Randomized controlled trial of general practitioner intervention in men with excessive alcohol consumption,” British Medical Journal, 87, 891-900. Babor, T. F., & M. Grant, (1992) WHO Collaborating Investigators Project on identification and management of alcohol-related problems. Combined analyses of outcome data: the cross-national generalizability of brief interventions. Report on phase II: a randomized clinical trial of brief interventions in primary health care, WHO: Copenhagen. Ballesteros, J, J. C. Duffy, I. Querejeta, J. Ariño, & A. González-Pinto, (2004) “Efficacy of Brief Interventions for Hazardous Drinkers in Primary Care: Systematic Review and Meta-Analyses,” Alcoholism: Clinical and Experimental Research, 28:4, 608–618. Bien, T, W.R. Miller, & J. S. Tonigan, (1993) “Brief interventions for alcohol problems: A review,” Addiction, 88, 315- 336. Chick, J., B. Ritson, J. Connaughton, & A. Stewart, (1988) “Advice versus extended treatment for alcoholism: a controlled study,” British Journal of Addiction, 83, 159-170. Coulton, S., K. Perryman, M. Bland, P. Cassidy, M. Crawford, P. Deluca, C. Drummond, E. Gilvarry, C. Godfrey, N. Heather, E. Kaner, J. Myles, D. Newbury-Birch, A. Oyefeso, S. Parrott, T. Phillips, D. Shenker, & J. Shepherd, (2009) “Screening and brief interventions for hazardous alcohol use in accident and emergency departments: a randomised controlled trial protocol,” BMC Health Services Research, 9:114. Department of Health, (2009) Local Routes: Guidance for developing alcohol treatment pathways. Drummond, D.C., B. Thom, C. Brown, G. Edwards & M. J. Mullan, (1990) “Specialist versus general practitioner treatment for problem drinkers,” The Lancet, 336, 915-918. Edwards, G., A. Duckitt, E. Oppenheimer, M. Sheehan, & C. Taylor, (1983) “What happens to alcoholics?” The Lancet, 30 Jul., 269-271. Edwards, G., J. Orford, S. Egert, A. Hawker, C. Hensman, C. Mitcheson, E. Oppenheimer, & C. Taylor, “Alcoholism: a controlled trial of “treatment” and “advice,” Journal of Studies on Alcohol, 38, 1004-31. Emmen, M.J., G.M. Schippers, G. Bleijenberg, & H. Wollersheim, (2004) “Effectiveness of opportunistic brief interventions for problem drinking in a general hospital setting: systematic review,” British Medical Journal, doi:10.1136/bmj.37956.562130.EE, Last accessed: 2nd May 2011 Freemantle, N., P. Gill, C. Godfrey, A. Long, C. Richards, T.A. Sheldon, F. Song, & T. Webb, (1993) “Brief interventions and alcohol use,” Quality in Health Care, 2, 267-273.

21
Gentilello, L. M., F.P. Rivara, D.M. Donovan, G.J. Jurkovich, E. Daranciang, C.W. Dunn, A. Villaveces, M. Copass, & R.R. Ries, (1999) “Alcohol interventions in a trauma center as a means of reducing the risk of injury recurrence,” Annals of Surgery, 230, 473–483. Hall, W. & N. Heather, (1991) “Issue of statistical power in comparative evaluation of minimal and intensive controlled drinking interventions,” Addictive Behaviors, 16, 83-87. Heather, N. (1996) “The Public Health and Brief Interventions for Excessive Alcohol Consumption: The British Experience,” Addictive Behaviours, 21:6, 857-868. Heather, N., (2004) “Brief Interventions,” in The Essential Handbook of Treatment & Prevention of Alcohol Problems, Eds. Heather & Tim Stockwell, Chicester, John Wiley, 1301-38. Heather, Nick, (2011) “The Case for Extended Brief Interventions,” Slovenian Journal of Public Health, 50:1, 1-11. Heather, N., P. D. Campion, R. G. Neville & D. MaCabe, (1987) “Evaluation of a controlled drinking minimal intervention for problem drinkers in general practice (the DRAMS scheme),” Journal of the Royal College of General Practitioners, 37, 358-363. Israel, Y., O. Hollander, M. Sanchez-Craig, S. Booker, V. Miller, & R. Gingrich, (1996) “Screening for problem drinking and counseling by the primary care physician-nurse team,” Alcoholism: Clinical & Experimental Research, 20:8, 443-450. Kaner E, F. Beyer, H. Dickinson, E. Pienaar, F. Campbell, C. Schlesinger, N. Heather, J. Saunders, & B. Bernand, (2007) Brief interventions for excessive drinkers in primary health care settings, Cochrane Database of Systematic Reviews, Issue 2. Art No.: CD004148 DOI: 10.1002/14651858.CD004148.pub3, Last accessed 29th April 2011. Krupski, A., J. Sears, J. Joesch, S. Estee, L. He, C. Dunn, A. Huber, P. Roy-Byrne, & R. Ries, (2010) “Impact of brief interventions and brief treatment on admissions to chemical dependency treatment,” Drug and Alcohol Dependence, 110: 1-2, 126-136. Longabaugh, R., R.F. Woolard, T.D. Nirenberg, A.P. Minugh, B. Becker, P.R. Clifford, K. Carty, Licsw, F. Sparadeo, & A. Gogineni, (2001) “Evaluating the effects of a brief motivational intervention for injured drinkers in the emergency department,” Journal of Studies on Alcohol, 62, 806–816. Maisto, S. E., J. Conigliaro, M. McNeil, K. Kraemer, R.L. Conigliaro, & M.E. Kelley, (2001) “Effects of two types of brief intervention and readiness to change on alcohol use in hazardous drinkers,” Journal of Studies on Alcohol, 62:5, 605-614. Marsden J, M. Farrell, C. Bradbury, A. Dale-Perera, B. Eastwood, M. Roxburgh, & S. Taylor, (2008) “Development of the Treatment Outcomes Profile,“ Addiction, 103:9, 1450-60. Matthews, B. & L. Ross, (2010) Research Methods: A practical guide for the social sciences, Harlow: Pearson. Mattick, R.P. & T. Jarvis, (1994) “Brief or minimal intervention for ‘alcoholics’? The evidence suggests otherwise,” Drug & Alcohol Review, 13, 137–144. Miller, W.R., (1999) Enhancing motivation for change in substance abuse treatment, U.S. Department of Health and Human Services, Rockville, MD.
22
Miller, W.R. & S. Rollnick, (1991) Motivational Interviewing, New York: Guilford Press. Monahan, S. C. & J.W. Finney, (1996) “Explaining abstinence rates following treatment for alcohol abuse: a quantitative synthesis of patient, research design and treatment effects,” Addiction, 91, 787–805. Moyer A., J.W. Finney, C.E. Swearingen, & P. Vergun, (2002) “Brief interventions for alcohol problems: a meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations,” Addiction, 97, 279-292. NICE, (2010) Preventing the Development of Hazardous and Harmful Drinking, NICE Public Health Guidance 24. NICE, (2011) Alcohol use disorders: diagnosis, assessment and management of harmful drinking and alcohol dependence, NICE Public Health Guidance 115. National Treatment Agency, (2005) Models of Care for Alcohol Misusers, London. Nilsen, P, J. Baird, M.J. Mello, T. Nirenberg, R. Woolard, P. Bendtsen, & R. Longabaugh, (2008) “A systematic review of emergency care brief alcohol interventions for injury patients,” Journal of Substance Abuse Treatment, 35:2,184-201. Ockene, J. K., A. Adams, T. Hurley, E. Wheeler, & J. R. Hebert, (1999) “Brief physician- and nurse practitioner-delivered counseling for high-risk drinkers: does it work?” Archives of Internal Medicine, 159, 2198–2205. Peele, S., (1997), “Bait and switch in project MATCH: What NIAAA research actually shows about alcohol treatment,” PsychNews International, 2, http://www.peele.net/lib/projmach.html Last accessed: 3rd May 2011. Poikolainen, K. (1999) “Effectiveness of brief interventions to reduce alcohol intake in primary health care populations: A meta-analysis,” Preventive Medicine: An International Journal Devoted to Practice & Theory, 28, 503–550. Project MATCH Research Group, (1997) “Matching alcoholism treatments to client heterogeneity: project MATCH post-treatment drinking outcomes,” Journal of Studies on Alcohol, 58, 7–29. Richmond, R., N. Heather, A. Wodak, L. Kehoe, I. & Webster, (1995) “Controlled evaluation of a general practice-based brief intervention for excessive drinking,” Addiction, 90, 119–132. Robertson, I., N. Heather, A. Dzialdowski, J. Crawford, & M. Winton, (1986) “A comparison of minimal versus intensive controlled drinking treatment interventions for problem drinkers,” British Journal of Clinical Psychology, 25, 185–194. Rollnick, S., P. Mason, & C.C. Butler, (1999) Behaviour change: a guide for health care professionals, 8th ed., London, Churchill Livingstone. Saunders, J. B., O.G. Aasland, T. F. Babor. J.R. de la Fuente, & M. Grant, (1993) “Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative

23
Project on Early Detection of Persons with Harmful Alcohol Consumption—II,” Addiction, 88:6, 791-804. Sobell, M. B. & L. C. Sobell, (2000) “Stepped Care as Heuristic Approach to the Treatment of Alcohol Problems,” Journal of Consulting & Clinical Psychology, 68:4, 573-579. Wallace, P., S. Cutler, & A. Haines, (1988) “Randomised controlled trial of general practitioner intervention in patients with excessive alcohol consumption,” British Medical Journal, 297, 663-668. WHO, (1996) “A Cross-National Trial of Brief Interventions with Heavy Drinkers,” American Journal of Public Health, 86:7, 948-955. WHO, (1992) Project on Identification and Management of Alcohol-Related Problems. Report on Phase I: A Randomized Clinical Trial of Brief Interventions in Primary Health Care, Eds. T.F. Babor & M. Grant, Geneva: World Health Organization. Wilk, A., N. Jensen, & T. Havighurst, (1997) “Meta-analysis of randomized control trials addressing brief interventions in heavy alcohol drinkers,” Journal of General Internal Medicine, 12, 274-283, 1997. Wright, S., L. Moran, M. Meyrick, R. O’Connor, & R. Touquet, (1998) “Intervention by an alcohol health worker in an accident and emergency department,” Alcohol & Alcoholism, 33:6, 651-6.

24
Appendix 1 Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al 1993)

25
Appendix 2 Screening and Intervention Programme for Sensible Drinking (SIPS) Brief Lifestyle Intervention Tool (Coulton et al 2009)

26

27
Appendix 3 Extended Brief Intervention Worksheet in use at HAGA (January 2011-current)
28

29

30
Appendix 4 Treatment Outcomes Profile (TOPS) (Marsden et al 2008)

31
Appendix 5 HAGA Pathway

32
Appendix 6 Extended Brief Interventions Survey
33
Blah
34
35
36
Appendix 7 Semi-structured Telephone Interview Guide 1. Introduction to the project a. Chat about how they are and what they have been doing this week. How are
things? b. Explain confidentiality
o all interview transcripts will be sent to you on request o all data will be kept on password protected documents on my computer to
which no-one has the password o all data will be anonymised in study report and no participant will be
identifiable o all participants will be sent copy of the report on request o no specific information related to particular workers at HAGA will be passed
on to the worker or management. This study is not a way of checking up on individual worker’s performance. Whilst I am a HAGA worker, you should feel free to be critical or complimentary about the services you received through HAGA. Senior management will have access to the final report only and will not know any of the details of respondents or their specific answers.
c. About me and the project - As I explained, I have been a HAGA worker since 2007 and am currently doing a Certificate in Drug and Alcohol Studies at the University of Stirling. My final project hopes to explore the pros and cons of offering Extended Brief Interventions—the sessions you had/were meant to have through HAGA—in alcohol services. Your views will help me to understand the experience of accessing EBI through HAGA. I hope that my final report will influence commissioners of alcohol services to consider the needs of non-dependent drinkers wishing to cut down, who are often overlooked.
d. About the interview - The interview will be a conversation between us about your experiences of EBI. The interview will take between 1.5 and 2 hours. You can take a break whenever you like, just let me know. If you feel uncomfortable at any time, you can ask to move on to another topic, terminate the conversation and ask to be called back, or withdraw from the study altogether.
e. Thank you for taking part – We are offering a £10 BOOTS voucher to everyone who completes the interview. o Check address.
f. Interview consent – Just to check with you again that you consent to the use of this interview in my report? Any questions at all regarding this?
g. Documentation consent - It would be really helpful if I could review the EBI worksheets and initial assessment/screening forms you worked through with a HAGA worker in your sessions. Do you consent for me to do this?
h. Any questions? 2. Introduction to the participant a. Can you tell me a bit about yourself? [Allow them to free reign and prompt where
necessary] o Age o Where you live o What you do Seek job title. o Who lives with you? Any children or caring responsibilities?
3. Drinking history – Please tell me a bit about your drinking history.

37
o Age started drinking o Current drinking – it would be useful if I could screen you using the standard
screening tools used when you entered and exited the service, would that be ok?
o AUDIT – TO BE COMPLETED o TOPS – TO BE COMPLETED
4. First recognition of drinking as an issue – it will be useful for me to know a little bit
about the first time that you sought support for your alcohol use. If HAGA is first source of support, then skip questions 4, 5 and 6.
a. When and how did you first recognise that your drinking was becoming or had
become a problem? o Screening? By who? When? Did they receive Brief Advice, EBI or referral? o Accident/hospitalisation? o Medical condition? o Family/friend comment? o Saw parallel with family/friend who has/had alcohol issues? o Problems at work? o Problems in relationship with partner/family/friends? o Really big session/serious hangover?
b. How soon after beginning to feel it was a problem, did you seek support with your
drinking? o Where did you go for support? i.e. family, friend or formal service/practitioner,
such as GP, alcohol service, counselling o What sort of support did you want? o What worried you about accessing support? o What barriers were there to accessing support around your drinking? o What was the outcome of your first attempt to seek support?
5. Service use history – it would be useful for me if you could outline the support that
you have accessed since then and before your recent referral to HAGA? What, if any, other support for your drinking have you accessed during this period (i.e. counselling, detoxification, 1:1, GP, etc). If you have accessed various different types of support over the years, it might be good to start with the earliest support you remember and work towards the present.
o What sort of services? o How often? Daily, weekly, monthly, bi-monthly, bi-annually, annually? o Over what time period/dates? o How did you find the experience of this type of support around your alcohol
use? Did you reduce your drinking? How long did you sustain this reduction? o On a scale of 1 (very poor) to 10 (very good), how would you rate this form of
support around your alcohol use?
6. REPEAT for each support service accessed prior to HAGA. 7. Referral and preconceptions: could you tell me a bit about how you came to
HAGA this year? o Who referred you or how did you hear about it? o Were you screened by the referrer?

38
o If so, did you receive Brief Advice (5-10 mins advice around what risks of drinking at Higher Risk levels, units, tips for cutting down, benefits of cutting down and making a goal for cutting down, usually accompanied by a leaflet or booklet)?
o What were your expectations and hopes for getting support around alcohol? o What were your fears about accessing support through an alcohol service? o What did you know about the sort of support on offer before you attended? o Did you think then that alcohol services could support someone drinking at your
level? 8a. Non-engagement in EBI – it would be useful for me if you could outline why you did
not choose to have the EBI sessions. o Assessment including TOPS o Location o Practitioner o HAGA itself o Didn’t think they needed it o Didn’t think EBI sounded right for them o Stopped drinking
SKIP TO QUESTION 13 IF DID NOT ENGAGE IN EBI SESSIONS 9. EBI sessions - Please describe your experience of the EBI sessions.
o How many sessions did you attend? o If less than 4, find out whether discontinued engagement. If disengaged, ask
why they decided to end the sessions? What could have been done differently? Have you sought alternative support? If so, seek details.
o Frequency of sessions o Length of sessions o Did you have the same worker each time? o What did you learn about alcohol/drinking from the sessions? o How did you feel about coming to your first session? o Views on completing screening tools (AUDIT and TOPS) – Intrusive? Useful? o Which of the following was important to you on a scale of one to ten where 1 is
not at all important and 10 is very important: o Content of the sessions themselves:
Being screened at beginning of each session Rating how important cutting down is Rating level of confidence about cutting down Pros and cons of cutting down Six-step plan Reviewing the six-step plan in follow-up sessions
o Re-reading the plan between sessions o Having the same worker each session o Level of alcohol expertise o Rapport with the worker o Time of sessions (i.e. appt time) o Length of sessions
10. Good and not so good aspects of EBI – it would be really interesting to hear your
views on the positive and negative aspects of receiving EBI. o What were the good aspects of the sessions? o What were the not-so-good aspects of the sessions?

39
11. How effective is EBI? – moving on from the good and bad aspects of EBI, what is your overall opinion of EBI as a way to support people to make changes to their drinking? o How would you rate EBI overall as a way of helping people reduce their drinking
on a scale of 1 (very poor) to 10 (very good)? o What changes in your drinking have come about as a result of the EBI sessions? o If there has been a change, what in your opinion is the key aspect of EBI which
caused this? o Have the EBI sessions had an effect on any other aspect of your life? i.e . work,
relationships, psychological well-being o Have you accessed any other support (i.e. counselling, medication, emotional
support from a friend) at the same time as or since attending the EBI sessions? o On a scale of 1 to 10, how confident are you about maintaining change in your
drinking/or, where indicated they have not reduced, how confident are you about reducing your drinking in the future?
o On a scale of 1 to 10, how motivated are you to maintain reduction in your drinking/or, where indicated they have not reduced, to reduce your drinking in the future?
12. Support for Higher Risk drinkers in an alcohol setting – as you will know, your initial
screening indicated that you were drinking at Higher Risk levels. Alcohol services typically support dependent, chaotic or very high drinkers rather than Higher Risk drinkers (who typically drink double the recommended limits more than twice a week). o What were the pros and cons for you of getting support from an alcohol service? o Has EBI changed your ideas about what alcohol services do/can offer? How?
13. Your recommendation for how we can support Higher Risk drinkers
o What sort of support do you think is required by Higher Risk drinkers? o Changes that could be made to the support you had o Would you recommend EBI to other people seeking to reduce their drinking? o Would you recommend that other Higher Risk drinkers contact their alcohol
service for support? 14. Any other comments or questions? 15. Check address for voucher NOTES: If a participant’s AUDIT score or their comments suggest that they need further support (i.e. drinking not reduced or drinking increased or another related issue arises), the researcher will discuss what support HAGA can give them and where necessary signpost them to other agencies for other types of support.
40
Appendix 8 Questionnaire Response Data
No. of practitioners
Practitioner type N
on
e
1-2
3-4
5-6
7-8
9-10
11-2
0
21-3
0
30+
Resp
ons
e
Co
unt (
n=19
)
Alcohol Liaison Nurses 6
(31.6%) 9
(47.4%) 1
(5.3%) 1
(5.3%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 12
(63.2%)
Alcohol Health Workers 12
(63.2%) 4
(21%) 3
(15.8%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 8
(42.1%)
Alcohol Workers 6
(31.6%) 3
(15.8%) 4
(21%) 2
(10.5%) 2
(10.5%) 2
(10.5%) 0
(0%) 0
(0%) 2
(10.5%) 13
(68.4%) Volunteers in an alcohol setting
12 (63.2%)
1 (5.3%)
2 (10.5%)
2 (10.5%)
0 (0%)
2 (10.5%)
0 (0%)
0 (0%)
0 (0%)
8 (42.1%)
Drug Workers 11
(57.9%) 0
(0%) 2
(10.5%) 2
(10.5%) 1
(5.3%) 1
(5.3%) 0
(0%) 1
(5.3%) 1
(5.3%) 9
(47.4%) Volunteers in a drug setting
15 (78.9%)
0 (0%)
2 (10.5%)
1 (8.3%)
0 (0%)
1 (5.3%)
0 (0%)
0 (0%)
0 (0%)
7 (36.8%)
Drug and Alcohol Workers
1 (5.3%)
0 (0%)
2 (10.5%)
3 (15.8%)
1 (8.3%)
1 (5.3%)
2 (10.5%)
1 (5.3%)
1 (5.3%)
12 (63.2%)
Volunteers in an alcohol/drug setting
14 (73.7%)
0 (0%)
1 (5.3%)
3 (15.8%)
0 (0%)
1 (5.3%)
0 (0%)
0 (0%)
0 (0%)
8 (42.1%)
Primary Care Practitioners
8 (42.1%)
0 (0%)
1 (5.3%)
2 (10.5%)
0 (0%)
0 (0%)
1 (5.3%)
2 (10.5%)
5 (45.5%)
11 (57.9%)
Probation Alcohol Practitioners
10 (52.6%)
4 (21%)
1 (5.3%)
0 (0%)
0 (0%)
1 (5.3%)
0 (0%)
0 (0%)
1 (5.3%)
9 (47.4%)
Offender Managers 12
(63.2%) 3
(15.8%) 1
(5.3%) 1
(5.3%) 0
(0%) 0
(0%) 1
(5.3%) 0
(0%) 0
(0%) 7
(41.2%)
Hospital Staff 8
(42.1%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 9
(81.8%) 11
(57.9%)
Table 2. Practitioners regularly delivering IBA in London.
Setting IB
A
EBI
Alcohol Service 12
(63.2%) 7
(36.8%)
Primary Care 11
(57.9%) 3 (15.8%)
Drug & Alcohol Service 11
(57.9%) 1 (5.3%)
A&E 11
(57.9%) 4
(21%)
Hospital wards 11
(57.9%) 3 (15.8%)
Drug Service 8
(42.1%) 5 (26.3%)
Probation 4
(21%) 3 (15.8%)
Table 3. Availability of IBA and EBI training in various settings across London.

41
No. of practitioners
Practitioner type N
on
e
1-2
3-4
5-6
7-8
9-10
11-2
0
21-3
0
30+
Resp
ons
e
Co
unt
(n=1
9)
Alcohol Liaison Nurses 8
(42.1%) 11
(57.9%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 13
(68.4%)
Alcohol Health Workers 13
(68.4%) 4
(21%) 1
(5.3%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 1
(5.3%) 8
(42.1%)
Alcohol Workers 6
(31.6%) 5
(26.3%) 5
(26.3%) 0
(0%) 0
(0%) 0
(0%) 2
(10.5%) 0
(0% 1
(5.3%) 14
(73.7%) Volunteers in an alcohol setting
15 (78.9%)
1 (10.5%)
3 (15.8%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
8 (42.1%)
Drug Workers 15
(78.9%) 0
(0%) 0
(0%) 2
(10.5%) 0
(0%) 0
(0%) 1
(5.3%) 1
(5.3%) 0
(0%) 8
(42.1%) Volunteers in a drug setting
18 (94.7%)
0 (0%)
0 (0%)
0 (0%)
1 (5.3%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
7 (36.8%)
Drug and Alcohol Workers
7 (36.8%)
2 (10.5%)
1 (5.3%)
3 (15.8%)
1 (5.3%)
0 (0%)
3 (10.5%)
1 (5.3%)
1 (5.3%)
14 (73.7%)
Volunteers in an alcohol/drug setting
18 (94.7%)
1 (5.3%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
8 (42.1%)
Primary Care Practitioners
11 (57.9%)
1 (5.3%)
1 (5.3%)
1 (5.3%)
1 (5.3%)
0 (0%)
0 (0%)
1 (5.3%)
2 (10.5%)
10 (52.6%)
Probation Alcohol Practitioners
12 (63.2%)
7 (36.8%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
0 (0%)
11 (57.9%)
Offender Managers 14
(73.7%) 1
(5.3%) 1
(5.3%) 0
(0%) 0
(0%) 1
(5.3%) 0
(0%) 0
(0%) 2
(10.5%) 10
(52.6%)
Hospital Staff 8
(42.1%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 0
(0%) 11
(57.9%) 13
(68.4%)
Table 4. Delivery of EBI across London.
Barriers Mo
st
imp
ort
an
t
2nd
3rd
4th
5th
6th
7th
Lea
st
Imp
ort
an
t
Resp
ons
e
Co
unt
Low levels of practitioner commitment
1 (8.33%)
2 (16.7%) 0 (0%) 0 (0%)
2 (16.7%)
4 (33.3%) 0 (0%)
1 (8.33%)
10 (52.6%)
Lack of skills/training 0 (0%) 3
(25%) 1
(8.33%) 4
(33.3%) 2
(16.7%) 0 (0%) 2
(16.7%) 0 (0%) 12
(63.2%)
Lack of capacity 6
(50%) 2
(16.7%) 2
(16.7%) 1
(8.33%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 11
(57.9%) Responsibility for this area falls between Tier 1 and specialist services
2 (16.7%) 0 (0%) 0 (0%)
2 (16.7%)
2 (16.7%)
2 (16.7%)
1 (8.33%) 0 (0%)
10 (52.6%)
Time constraints within consultation/1:1s 0 (0%)
3 (25%)
4 (33.3%)
1 (8.33%)
1 (8.33%) 0 (0%) 0 (0%) 0 (0%)
10 (52.6%)
Lack of funding 3
(25%) 2
(16.7%) 0 (0%) 2
(16.7%) 2
(16.7%) 0 (0%) 1
(8.33%) 2
(16.7%) 10
(52.6%) No champion at a senior level
1 (8.33%)
1 (8.33%)
2 (16.7%) 0 (0%) 0 (0%) 0 (0%)
3 (25%)
1 (8.33%)
8 (42.1%)
Not a strategic priority 0 (0%) 0 (0%) 1
(8.33%) 0 (0%) 0 (0%) 2
(16.7%) 1
(8.33%) 2
(16.7%) 7
(36.8%)
Table 5. Barriers to EBI
42
EBI Value Statements St
ron
gly
D
isa
gre
e
Dis
ag
ree
Ne
utr
al
Ag
ree
Stro
ng
ly
Ag
ree
Resp
on
se
Co
un
t
EBI delivered by alcohol specialists will be of a higher quality
0 (0%)
2 (13.3%)
5 (33.3%)
7 (46.7%)
1 (6.7%)
15 (78.9%)
Alcohol specialists will require less training to deliver EBI
0 (0%)
4 (26.7%)
3 (20%)
6 (40%)
2 (13.3%)
15 (78.9%)
Alcohol specialists will just revert to keyworking Higher Risk drinkers
2 (14.3%)
2 (14.3%)
6 (42.9%)
4 (28.6%)
0 (0%)
14 (73.7%)
Higher Risk drinkers will be put off by the stigma of attending an alcohol service
0 (0%)
5 (33.3%)
4 (26.7%)
6 (40%)
0 (0%)
15 (78.9%)
EBI should be delivered by alcohol specialists in primary care settings via satellites
1 (6.7%)
1 (6.7%)
1 (6.7%)
9 (60%)
3 (20%)
15 (78.9%)
EBI should be delivered by alcohol specialists in hospital settings
0 (0%)
2 (13.3%)
2 (13.3%)
9 (60%)
2 (13.3%)
15 (78.9%)
EBI should be delivered as standard to individuals who are referred to alcohol specialists and identified as Higher Risk drinkers
1 (6.7%)
2 (13.3%)
2 (13.3%)
7 (46.7%)
3 (20%)
15 (78.9%)
EBI is beyond the capacity of most Tier 1 professionals 2
(13.3%) 9
(60%) 2
(13.3%) 2
(13.3%) 0
(0%) 15
(78.9%) Primary care practitioners don't have the time to support Higher Risk drinkers
5 (33.3%)
4 (26.7%)
3 (20%)
3 (20%)
0 (0%)
15 (78.9%)
Primary care practitioners don't have the skills to support Higher Risk drinkers
4 (26.7%)
4 (26.7%)
4 (26.7%)
2 (13.3%)
1 (6.7%)
15 (78.9%)
Primary care practitioners don't have the inclination to support Higher Risk drinkers
2 (15.4%)
5 (38.5%)
4 (30.8%)
0 (0%)
2 (15.4%)
13 (68.4%)
Healthcare Assistants and Practice Nurses should be delivering EBI as standard
0 (0%)
2 (14.3%)
1 (7.1%)
8 (57.1%)
3 (21.4%
14 (73.7%)
Probation Alcohol Practitioners should be delivering EBI as standard
0 (0%)
0 (0%)
0 (0%)
10 (66.7%)
5 (33.3%)
15 (78.9%)
All Tier 1 practitioners are capable of delivering EBI 2
(13.3%) 1
(6.7%) 4
(26.7%) 5
(33.3%) 3
(20%) 15
(78.9%) EBI delivered by alcohol specialists is really "brief treatment"
0 (0%)
1 (7.1%)
7 (50%)
6 (42.9%)
0 (0%)
14 (73.7%)
Since the evidence suggests that Brief Advice is as effective as EBI, EBI is a waste of resources
2 (13.3%)
5 (33.3%)
6 (46.7%)
1 (6.7%)
0 (0%)
15 (78.9%)
EBI fills a gap in service provision for Higher Risk drinkers
0 (0%)
4 (26.7%)
2 (13.3%)
8 (53.3%)
1 (6.7%)
15 (78.9%)
Table 6. EBI Value Statements