estrogens and progestins. introduction estrogens and progestins are endogenous hormones that...
TRANSCRIPT

Estrogens and ProgestinsEstrogens and Progestins

IntroductionIntroduction
Estrogens and progestins are endogenous hormones that produce numerous physiological actions
The therapeutic use of estrogens and progestins largely reflects extensions of their physiological activities
The most common uses of these agents are menopausal hormone therapy and contraception in women

IntroductionIntroduction
Estrogen- and progesterone-receptor antagonists also are available
The main uses of anti-estrogens are treatment of hormone-responsive breast cancer and infertility
The main use of anti-progestins has been for medical abortion

+
+
-
-
NE
Hypothalamus
GnRHGnRH
Anterior pitutary gland
FSHFSHLHLH
Target Tissues
Ovaries
DA, Opioid, GABA
EstrogenProgesterone
+-
-

1. Estrogens1. Estrogens

EstrogensEstrogens
The most potent endogenous estrogen is estradiol, followed by estrone & estriol
Preparations of conjugated estrogens containing sulfate esters of estrone and equilin estrogens (equilenin & equilin) obtained from pregnant mares’ urine
Ethinyl substitutions at the C17 position of estradiol (ethinyl estradiol) greatly increase oral potency by inhibiting first-pass hepatic metabolism

EstrogensEstrogens
Steroidal estrogens arise from androstenedione or testosterone by aromatization. The reaction is catalyzed by aromatase (CYP19)
In postmenopausal women, the principal source of circulating estrogen is adipose tissue stroma, where estrone is synthesized from dehydroepiandrosterone secreted by the adrenals
The placenta uses fetal dehydroepiandrosterone and its 16-hydroxyl derivative to produce large amounts of estrone and estriol
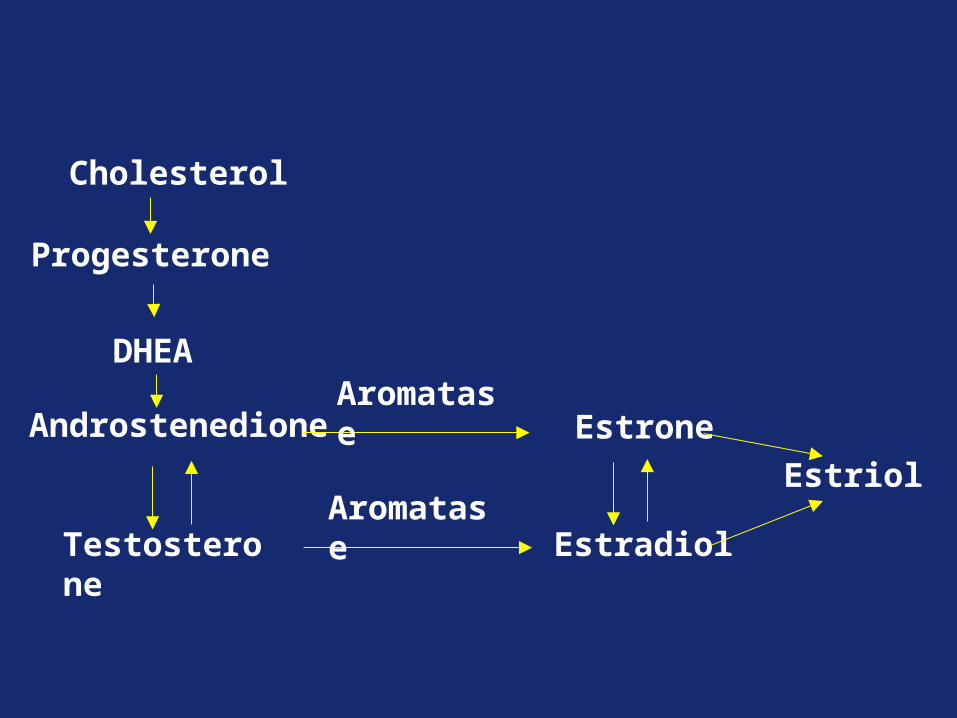
Androstenedione Estrone
Testosterone Estradiol
Aromatase
Aromatase
Progesterone
Cholesterol
DHEA
Estriol

Estrogen pharmacokineticsEstrogen pharmacokinetics
Estradiol is extensively bound to SHBG
Estradiol is converted primarily by the liver to estrone and estriol, the major urinary metabolite
Estradiol undergo enterohepatic recirculation via (1) sulfate and glucuronide conjugation in the liver, (2) biliary secretion of the conjugates into the intestine, and (3) hydrolysis in the gut (largely by bacterial enzymes) followed by reabsorption

Estrogen preparationsEstrogen preparations
For many uses, preparations are available as an estrogen alone or in combination with a progestin
All of the estrogens produce almost the same hormonal effects, their potencies vary both between agents and depending on the route of administration

Estrogen preparationsEstrogen preparations
Oral administration is common and may utilize estradiol, conjugated estrogens, esters of estrone and other estrogens, and ethinyl estradiol
Tansdermal patches provides slow, sustained release of the hormone, systemic distribution, and more constant blood levels than oral dosing
Estradiol and conjugated estrogen creams also are available for topical administration to the vagina

Commonly Used EstrogensPreparation Average Replacement Dosage
Ethinyl estradiol 0.005–0.02 mg/dMicronized estradiol 1–2 mg/dEstradiol cypionate 2–5 mg every 3–4 weeksEstradiol valerate 2–20 mg every other weekEstropipate 1.25–2.5 mg/d
Conjugated, esterified, or mixed estrogenic substances: Oral 0.3–1.25 mg/d
Injectable 0.2–2 mg/d Transdermal Patch
Quinestrol 0.1–0.2 mg/week
Chlorotrianisene 12–25 mg/dMethallenestril 3–9 mg/d
Physiological effectsPhysiological effects
1. Growth and Development
2. Neuroendocrine Control of the Menstrual Cycle
3. Endometrial Effects
Physiological effectsPhysiological effects
4. Metabolic Effects:
a) Decrease bone resorption rate
b) Increase HDL levels and a slight decrease in LDL , a reduction in total plasma cholesterol, and a slight increase in TG levels
c) Increase plasma levels of CBG, TBG, & SHBG
d) Enhance the coagulability of blood: increase circulating levels of factors II, VII, IX, and X and decrease antithrombin III

Therapeutic uses of estrogensTherapeutic uses of estrogens
Menopausal Hormone therapy (MHT)
Benefits of estrogen therapy include amelioration of vasomotor symptoms and the prevention of bone fractures and urogenital atrophy
MHT with estrogens should use the lowest dose and shortest duration necessary to achieve an appropriate therapeutic goal

Therapeutic uses of estrogensTherapeutic uses of estrogens
2. Menopausal Hormone therapy (MHT)
Optimal management of the postmenopausal patient requires careful assessment of her symptoms as well as consideration of her age and the presence of (or risks for) cardiovascular disease, osteoporosis, breast cancer, and endometrial cancer
ERT in postmenopausal women is associated with an increased incidence of endometrial carcinoma; this led to the use of HRT to reduces the risk of this cancer

Therapeutic uses of estrogensTherapeutic uses of estrogens
2. Menopausal Hormone therapy (MHT)
For women who have undergone a hysterectomy, endometrial carcinoma is not a concern, and it is most prescribe estrogen (conjugated estrogens or ethinyl estradiol)
Oral estrogen should be avoided in women with hypertriglyceridemia, liver disease, and gallbladder disease. For these women, transdermal administration is a safer approach

Therapeutic uses of estrogensTherapeutic uses of estrogens
2. Menopausal Hormone therapy (MHT)
a) Vasomotor symptoms: hot flashes may alternate with chilly sensations, inappropriate sweating, and (less commonly) paresthesias
Treatment with estrogen is specific and is the most efficacious pharmacotherapy for these symptoms

Therapeutic uses of estrogensTherapeutic uses of estrogens
2. Menopausal Hormone therapy (MHT)
b) Osteoporosis:
Osteoporosis is an indication for estrogen therapy, which clearly is efficacious in decreasing the incidence of fractures
Estrogens are most effective if treatment is initiated before significant bone loss occurs, and their maximal beneficial effects require continuous use; bone loss resumes when treatment is discontinued

Therapeutic uses of estrogensTherapeutic uses of estrogens
2. Menopausal Hormone therapy (MHT)
c) Vaginal dryness and urogenital atrophy:
These include dryness and itching of the vagina, dyspareunia, swelling of tissues in the genital region, pain during urination, a need to urinate urgently or often, and sudden or unexpected urinary incontinence
When estrogens are being used solely for relief of vulvar and vaginal atrophy, local administration as a vaginal cream, ring device, or tablets may be considered

Therapeutic uses of estrogensTherapeutic uses of estrogens
2. Menopausal Hormone therapy (MHT)
d) Cardiovascular events
Epidemiological studies consistently showed an association between estrogen use and reduced CV disease in postmenopausal women
However, estrogens promote coagulation and thromboembolic events
Transdermal or vaginal administration of estrogen may be associated with decreased CV risk
Adverse EffectsAdverse Effects
1) Nausea and vomiting
2) Breast tenderness: minimized by using the smallest effective dose
3) Postmenopausal uterine bleeding
4) Increased frequency of migrane headache
5) Cholestasis and gallbladder disease

Adverse EffectsAdverse Effects
5) Cancer
a. Increase risk of endometrial cancer The risk seems to vary with the dose and duration
of treatment: 15 times greater in patients taking large doses of estrogen for 5 or more years
The concomitant use of a progestin prevents this increased risk and may in fact reduce the incidence of endometrial cancer

Selective Estrogen Receptor Modulators (SERMs)
Selective Estrogen Receptor Modulators (SERMs)
Class of estrogen-related compounds with tissue-selective actions
Their pharmacological goal is to produce beneficial estrogenic actions in certain tissues (e.g., bone) but antagonist activity in others (e.g., breast and endometrium)

Tissue Dependent Action
Antagonistic Effects(uterus, breast)
Agonistic Effects (bone)
Selective Estrogen Receptor Modulator
(SERM)
ER = Estrogen ReceptorBMD = Bone Mineral Density
ERER
• Increase BMD and reducethe risk of vertebral fractures

Tamoxifen Tamoxifen It is a partial estrogen agonist in breast and is
used as a palliative treatment and chemopreventative for breast cancer in high-risk women
It is a full agonist in bone and endometrium, and prolonged use of tamoxifen leads to a fourfold to fivefold increase in the incidence of endometrial cancer
ADEs: nausea, vomiting, hot flushes, & increases the risk of venous thrombosis

Decreased cancer risk
Tamoxifen Estrogen
Uterine receptor activated
Estrogen receptor in uterine endometrial cell
Endometrial cell proliferation
Breast receptor not activated
Estrogen receptor in breast cell
blocked
No breast cell proliferation
Increased cancer risk

RaloxifeneRaloxifene
It is an estrogen agonist in bone and is approved for the prevention of osteoporosis in postmenopausal women
Like tamoxifen, it has antagonist effects in breast tissue and reduces the incidence of breast cancer in women who are at very high risk
Unlike tamoxifen, the drug has no estrogenic effects on endometrial tissue
ADEs: hot flushes, leg cramps, & increased risk of DVT

ClomipheneClomiphene
Partial estrogen agonist
Interfere with the negative feedback of estrogen on the hypothalamus: GnRH secretion becomes more pulsatile, which results in increased pituitary gonadotropin (FSH, LH) release
Uses: Infertility associated with anovulatory cycles
Adverse effects: headache, nausea, hot flushes, visual disturbances, & ovarian enlargement

Estrogen-Synthesis Inhibitors: Aromatase inhibitors
Estrogen-Synthesis Inhibitors: Aromatase inhibitors
Aromatase is the enzyme required for estrogen synthesis
Agents:
1) Irreversible steroidal inhibitors: Exemestane
2) Reversible Non-steroidal inhibitors: anastrozole & letrozole
• These agents may be used as first-line treatment of breast cancer or as second-line drugs after tamoxifen

Androstenedione Estrone
Testosterone Estradiol
Aromatase
Aromatase
Progesterone
Cholesterol
DHEA Aromatase Inhibitors

Estrogen-Synthesis Inhibitors: Aromatase inhibitors
Estrogen-Synthesis Inhibitors: Aromatase inhibitors
Unlike tamoxifen, they do not increase the risk of uterine cancer or VTE
ADEs: related to reduce circulating and local levels of estrogens (e.g. hot flushes and significant bone loss)

2. Progestins2. Progestins

ProgestinsProgestins
Natural progestins: Progesterone
It is secreted by the corpus luteum in the second part of the menstrual cycle, and by the placenta during pregnancy
Small amounts are also secreted by testis and adrenal cortex

Progestins pharmacokineticsProgestins pharmacokinetics
Progesterone is rapidly absorbed following administration by any route
It undergoes rapid first-pass metabolism, with a t1/2 of 5 minutes
Progesterone is metabolized primarily in the liver to pregnanediol and its sulfate and glucuronide conjugates are eliminated in the urine

PreparationsPreparations
1) Naturally occurring hormone and its derivatives
• They display limited binding to glucocorticoid, androgen, and mineralocorticoid receptors, a property that probably accounts for some of their nonprogestational activities
• Progesterone undergoes rapid first-pass metabolism, and is orally inactive
• Other preparations of progesterone are available for oral administration (micronized), intramuscular injection, or administration via the vagina or rectum
• Hydroxyprogesterone caproate and MPA are available for IM administration

PreparationsPreparations
B. Testosterone derivatives “19-nortestosterones”
• Can be given orally
• These compounds have progestational activity and retain some androgenic activity
• Norethisterone and norgestrel have androgenic activity
• Newer progestogens without androgenic activity include desogestrel, norgestimate, and gestodene

Properties of Some Progestational Agents.Route Duration of
ActionActivities1
Estrogenic Androgenic Antiestrog, Antiandrog . Anabolic Progesterone and derivatives
Progesterone IM 1 day – – + – –Hydroxyprogesterone caproate
IM 8–14 days sl sl – – –
Medroxyprogesterone acetate
IM, POTabs: 1–3 days; injection: 4–12 wks
– + + – –
Megestrol acetate PO 1–3 days – + – + –17-Ethinyl testosterone derivatives
Dimethisterone PO 1–3 days – – sl – –19-Nortestosterone derivatives
Desogestrel PO 1–3 days – – – – –Norethynodrel2 PO 1–3 days + – – – –Lynestrenol3 PO 1–3 days + + – – +Norethindrone2 PO 1–3 days sl + + – +Norethindrone acetate2 PO 1–3 days sl + + – +Ethynodiol diacetate2 PO 1–3 days sl + + – –L-Norgestrel2 PO 1–3 days – + + – +1Interpretation: + = active; – = inactive; sl = slightly active. Activities have been reported in various species using various end points and may not apply to humans.2See Table 40–3.3Not available in USA.
Effects of ProgesteroneEffects of Progesterone
1. Neuroendocrine action: Progesterone produced in the luteal phase
of the cycle decreases the frequency of GnRH pulses
2. Reproductive tract: Decrease estrogen-driven endometrial
proliferation and induces a secretory endometrium

Effects of ProgesteroneEffects of Progesterone
3) CNS: Increases basal body temperature
Progesterone also may have depressant and hypnotic actions in the CNS

Effects of ProgesteroneEffects of Progesterone
4) Progesterone stimulates lipoprotein lipase activity and favor fat disposition
5) Increases basal insulin levels and the insulin response to glucose
6) In the liver, it promotes glycogen storage by facilitating the effect of insulin
7) Decreases the plasma levels of many a.as and leads to increased urinary nitrogen excretion
8) Decreases Na+ reabsorption in the kidney

Therapeutic uses of Progestins Therapeutic uses of Progestins
1) Hormone replacement treatment: in combination with estrogen for hormone therapy of postmenopausal women
2) Contraception: either alone or with an estrogen
3) Test for estrogen secretion and for responsiveness of the endometrium
4) Decrease the occurrence of endometrial hyperplasia and carcinoma caused by unopposed estrogens

Therapeutic uses of Progestins Therapeutic uses of Progestins
5) Treatment of dysmenorrhea , endometriosis, and bleeding disorders when estrogens are contraindicated

Adverse EffectsAdverse Effects
Major effects: headache, fluid retention, depression, weight gain, & changes in libido
Progestins with androgenic activity (19-nortestosterone derivatives):
1) Plasma lipids: increase LDL and cause either no effect or modest reduction in serum HDL levels
2) Acne
3) Hirsutism
Antiprogestin: MifepristoneAntiprogestin: Mifepristone
• It effectively competes with progesterone for binding to PR
• Mifepristone decreases endogenous progesterone coupled with blockade of progesterone receptors in the uterus increases uterine prostaglandin levels and sensitizes the myometrium to their contractile actions
• Mifepristone also causes cervical softening, which facilitates expulsion of the detached blastocyst

Antiprogestin: MifepristoneAntiprogestin: Mifepristone
• Clinical uses:
1) Early termination of pregnancy (abortificant): in combination with misoprostol or other prostaglandins
2) Emergency postcoital contraceptive
3) Control high blood sugar levels (hyperglycemia) in adults with endogenous Cushing’s syndrome
• ADEs: Prolonged vaginal bleeding (major), abdominal pain, uterine cramps, & NVD

Selective Progesterone Receptor Modulators (SPRMs)
Selective Progesterone Receptor Modulators (SPRMs)
Exert clinically relevant tissue-selective progesterone agonist, antagonist, or partial (mixed) agonist/antagonist effects on various progesterone target tissues
Ulipristal acetate (UPA): approved by FDA in June 2010 for use as an emergency contraceptive
SEs: abdominal pain and menstrual disorders (irregular vaginal bleeding, premenstrual syndrome and uterine cramps)

Hormonal contraceptionHormonal contraception
Types of hormonal contraceptivesTypes of hormonal contraceptives
1. Combined hormonal contraceptive
2. Progestin-only contraceptives
3. Postcoital or emergency contraceptives

Combined oral contraceptiveCombined oral contraceptive
• The most frequently used agents containing both an estrogen and a progestin
• Their theoretical efficacy is considered to be 99.9%
• Combination oral contraceptives are generally provided in 21-day packs with an additional 7 pills containing no active hormone

Combined oral contraceptiveCombined oral contraceptive
• The U.S. FDA approved Beyaz tablets, an estrogen/progestin combined oral contraceptive that also contains a folate (levomefolate calcium 0.451 mg)
• Further divided into:
I. Monophasic: constant dosage of both components during the cycle
II. Multiphasic: dosage of one or both components is changed during the cycle

Multiphasic vs Monophasic Preparations*
Multiphasic vs MonophasicPreparations*
Day of pill cycle
Norethindrone
(mg)Endogenous progesterone
(ng/mL)
18
10
5
0 7 14 2128
1.0
0.75
0.5
0.4
0
Monophasic (Ovcon 35)Multiphasic (Ortho Novum 7/7/7)Endogenous progesterone level
*Ethinyl estradiol content is constant (35 µg) for both preparations.
Adapted from Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 3rd ed. 1996:1416.
20
menses

Combined oral contraceptiveCombined oral contraceptive
The estrogen in most combined preparation is ethinyl estradiol, though a few preparations contain mestranol instead
Progestins are 19-nor compounds that have varying degrees of androgenic, estrogenic, and antiestrogenic activities that may be responsible for some side effects
The most common progestins are norethindrone, norethindrone acetate, norgestrel, levonorgestrel, desogestrel, norgestimate, and drospirenone

Combined oral contraceptiveCombined oral contraceptive
The estrogen content of current preparations ranges from 20µg to 50 µg; most contain 30-35 µg
The dose of progestin is more variable because of differences in potency of the compounds used

Combined oral contraceptiveCombined oral contraceptive
Additional options for combined hormonal contraceptives include:
1.Transdermal patch containing ethinyl estradiol and norelgestromin: applied weekly for 3 weeks. Week 4 is patch-free, and withdrawal bleeding occurs
2.Vaginal ring containing ethinyl estradiol and etonogestrel: is used for 3 weeks. Week 4 is ring-free, and withdrawal bleeding occurs
Efficacy, contraindications, and ADEs similar to those of oral contraceptives

Mechanism of actionMechanism of action
1. Estrogen: inhibits secretion of FSH via negative feedback on the anterior pituitary, and thus suppresses development of the ovarian follicle
2. Progestin:
a) Inhibits secretion of LH and thus prevents ovulation
b) Induces viscous mucus that reduces sperm penetration and induces an endometrium that is not receptive to implantation
Clinical usesClinical uses
1) Contraception
2) Endometerosis when dysmenorrhoea is the major symptoms: long term treatment with estrogen and progestins

Adverse effectsAdverse effects
1. Cardiovascular Effect:
Relatively low and is determined by the specific compound and combination used
For nonsmokers without other risk factors such as hypertension or diabetes, there is no significant increase in the risk of CV events
Oral contraceptives increase the risk of various CV disorders, especially in women ≥35 years who are heavy smokers (with predisposing risk factors)

CV Mortality Risk with Smoking & OC UseCV Mortality Risk with Smoking & OC Use
Oral contraceptive user
Oral contraceptive nonuser
Smoker Nonsmoker Smoker Nonsmoker
< 35 years of age ≥ 35 years of age
Cas
es p
er
100,
000
Wo
man
-Yea
rs
Attributable Risk/100,000 User-Years
0.06 1.73 3.03 19.4
Sherif K. Am J Obstet Gynecol. 1999;180(Pt 2):S343-S348.

Adverse effectsAdverse effects
1. Cardiovascular Effect:
a. VTE (e.g. PE) :
Risk is related to the estrogen but not the progestin content of oral contraceptives
Postmarketing epidemiologic studies indicate that women using transdermal contraceptives have a higher than expected exposure to estrogen and are at increased risk for the development of venous thromboembolism

Adverse effectsAdverse effects
1. Cardiovascular Effect:
b. MI:
• The use of oral contraceptives is associated with a slightly higher risk of MI in women who are obese, have a history of preeclampsia or hypertension, or have hyperlipoproteinemia or diabetes
• The risk depends on the specific composition of the pill used and the patient's susceptibility to the particular effects

Adverse effectsAdverse effects
2. Cancer
Combined oral contraceptives reduce the risk of endometrial and ovarian cancer. This is due to the inclusion of progestins which opposes estrogen-induced proliferation, throughout the entire 21 days
Their ability to induce neoplasms is controversial
Adverse effectsAdverse effects
2. Metabolic effects:
a. Weight gain: more common with the combination agents containing androgen-like progestins
b. Serum lipids:
Estrogen causes an increase in HDL and a decrease in LDL
Progestins antagonize the beneficial effect of estrogen (particularly the 19-nortestosterone derivative)
Estrogen-dominant preparations are best for individuals with elevated serum cholesterol

Adverse effectsAdverse effects
3. Miscellaneous Effects
a) Nausea, mastalgia, and edema: related to the amount of estrogen
b) Breakthrough bleeding:
Occur if the estrogen-to-progestin ratio is too low to produce a stable endometrium
May be prevented by switching to a pill with a higher ratio or using biphasic and triphasic oral contraceptives

Adverse effectsAdverse effects
c) Mild headache and migraine headaches
d) Increased skin pigmentation, acne, and hirsutism: mediated by the androgenic activity of the 19-nor progestins
e) Cholestatic jaundice & increase the incidence of symptomatic gallbladder disease (e.g. cholecystitis and cholangitis)
f) Amenorrhea in some patients following cessation of administration of oral contraceptives
g) Vaginal infections and bacteriuria

ContraindicationsContraindications1) The presence or history of thromboembolic disease,
cerebrovascular disease, MI, CAD, or congenital hyperlipidemia
2) Known or suspected carcinoma of the breast
3) Carcinoma of the female reproductive tract
4) Estrogen-dependent/responsive neoplasias
5) Abnormal undiagnosed vaginal bleeding
6) Pregnancy
7) Past or present liver tumors or impaired liver function
8) Women over 35 years of age who smoke heavily (e.g., >15 cigarettes/day)
Drug interactionsDrug interactions
1. CYP450 enzyme inducers (e.g. rifampin, barbiturates, and phenytoin): may result in contraceptive failure
2. Antibiotics (e.g. amoxicillin): reduce estrogen enterohepatic recycling and may decrease the effectiveness of oral contraceptives

Progestin only contraceptivesProgestin only contraceptives
1. Minipills:
• As effective as combination pills
• Continuous progestin therapy without concomitant administration of estrogens
• Agents: norethisterone, levonorgestrel, or ethynodiol
• Particularly suited for use in patients for whom estrogen administration is undesirable
• ADEs: irregular bleeding episodes, headache, weight gain, and mood changes

Progestin only contraceptivesProgestin only contraceptives
2. Progestin Implant
A subdermal implant (4-cm capsule) containing etonogestrel offers long-term contraception (~ 2-4 yrs)
Low failure rate (does not rely on patient compliance)
3. Progestin intrauterin device
A T-shaped levonorgestrel-releasing intrauterine system that provide contraception for up to 5-years

Progestin only contraceptivesProgestin only contraceptives
4. Medroxyprogesterone acetate (MPA)
Administered IM every 3 months
Major disadvantage is the prolonged time required in some patients for ovulatory function to return after cessation of therapy
It should not be used for patients planning a pregnancy in the near future
MPA for contraceptive injection increase the risk of osteoporosis

Postcoital or emergency Contraceptives Postcoital or emergency Contraceptives
Should be administered within 72 hours of unprotected intercourse
· PREVEN (The combined regimen): uses large doses of both estrogen and progestin, taken as two doses seperated by 12-hours
· PLAN B (Progestin only regimen): two doses of levonorgestrel “minipill” separated by 12 hours
· A single oral dose of mifepristone followed by a single dose of a prostaglandin (Misoprostol) 48 hours later

Postcoital or emergency Contraceptives Postcoital or emergency Contraceptives
4. Ulipristal acetate (PLAN C):
Its efficacy is maintained through a five day period following exposure , making ulipristal a more versatile emergency contraceptive
Unlike levonorgestrel, is not approved for over the counter use

Postcoital or emergency Contraceptives Postcoital or emergency Contraceptives
Nausea and vomiting are the main untoward effects and may be severe
Emergency contraceptives are contraindicated in the case of confirmed pregnancy

Choice of Contraceptive PreparationsChoice of Contraceptive Preparations
For a given individual, both the efficacy and side effects of hormonal contraceptives may vary considerably among preparations
Risks for serious side effects as enumerated earlier should be considered before initiating contraceptives in any individual patient
Treatment should generally begin with preparations containing the minimum dose of steroids that provides effective contraceptive coverage

Choice of Contraceptive PreparationsChoice of Contraceptive Preparations
Typically a pill with 30-35 µg of estrogen, but preparations with 20 µg may be adequate for lighter women or >40 years of age with perimenopausal symptoms
In women for whom estrogens are contraindicated or undesirable, progestin-only contraceptives may be an option (e.g., nursing mothers and women >40 years of age, in whom fertility may be decreased)

Choice of Contraceptive PreparationsChoice of Contraceptive Preparations
The choice of a preparation also may be influenced by the specific 19-nor progestin component because this component may have varying degrees of androgenic and other activities
These side effects are greatly reduced in newer low-dose contraceptives that contain progestins with little to no androgenic activity
Noncontraceptive Health BenefitsNoncontraceptive Health Benefits
1. Significantly reduce the incidence of ovarian and endometrial cancer within 6 months of use, and the incidence is decreased 50% after 2 years of use
2. Depot MPA injections also reduce very substantially the incidence of uterine cancer for up to 15 years after oral contraceptive use is discontinued
3. Decrease the incidence of ovarian cysts and benign fibrocystic breast disease
Noncontraceptive Health BenefitsNoncontraceptive Health Benefits
4. Benefits related to menstruation: more regular menstruation, reduced menstrual blood loss and less iron-deficiency anemia, and decreased frequency of dysmenorrhea
5. Decreased incidence of pelvic inflammatory disease and ectopic pregnancies, and endometriosis