espen congress lisbon 2004 · espen congress lisbon 2004 pharmacists’ session specialised...
TRANSCRIPT

ESPEN Congress Lisbon 2004
Pharmacists’ Session
Specialised formulas for enteral and parenteral nutrition – A clinical reality or marketing exercise
Bruce McElroy
Specialised Formulas for Enteral and Parenteral
NutritionA Clinical Reality or Marketing Exercise?
Bruce Mc ElroyPrincipal Pharmacist
Royal Shrewsbury Hospital




Nutrition Products• Foodstuffs, Nutrition Modification, Functional
Foods-Health promoting and Maintaining• Nutritional products for medical purposes and use in
specific diseases- Enteral Nutrition and management of malnournished patients
• Parenteral Nutrition and Nutrients- management of malnutrition and treatment of specific deficiencies
• Nutraceuticals and Single Nutrient Therapy-management and treatment- medicinal claims

Nutritional products for medical purposes and use in specific diseases
Enteral Nutrition• PARNUTS Directive and Regulation- limit
composition and quantities of additives- unless proved by clinical trials and medicinal regulation
• Information on supplementation to be regulated to the general public. But allow “medical” claims, not based on medicinal regulation to Clinicians, Pharmacy and Dietetics
• Expectation of major potential growth in number and specialised enteral feeds.

Parenteral Nutrition and NutrientsManagement of malnutrition and treatment of specific deficiencies
• Parenteral Nutrition always regulated as medicinal products
• Cannot make health claims without evidence of benefit
• Required to state specific dose ranges and indications for use
• Evidence based approach

Specialised Enteral Nutrition Feeds
• Manipulation of various macronutrients and electrolyte content
• Additions of specific components- e.g. Amino Acids, Omega-3 fatty acids, antioxidants
Most targeted as disease or condition specific
Examples of Disease Specific Enteral Nutrition
• Respiratory Distress• Liver Disease• Acute Renal Impairment• Cystic Fibrosis• Wound Healing• Immune Function Enhancing

Respiratory Distress- Enteral Nutrition• Mechanically ventilated critically ill patients on
formulas with high %age of energy for Carbohydrate tend to retain CO2 & had difficulty weaning from mechanical ventilation.
• Where formulas with less Carbohydrate provided respiratory status may be improved
• Suggestion that enteral feeds with high fat content ~50-60% compared to standard of ~30% would be of benefit to weaning patients off ventilation
• Respiratory Quotient of Carbohydrate is 1.0, Fat 0.7

Respiratory Distress- Enteral Nutrition
• Fluid Restriction is often indicated in ARDS- energy dense feeds may be preferred
• Initial respiratory feeds used conventional sources of fat, recent work focuses on different fatty acids and role in lung injury
• Suggestion that significant different responses in prostaglandin and leukotriene synthesis can result and effect anti inflammatory responses
• Alter fat composition and cause less inflammatory eicosanoids- resulting in improved outcomes, decreased ventilation time and length of stay
Respiratory Distress- Enteral Nutrition
• Research also suggests reduced levels of antioxidants- vitamin C, E, retinol, ß-carotene & selenium- standard feeds are not able to correct these deficiencies
• COPD patients similar in expected requirements to ARDS and ventilated patients- energy and protein dense feeds, with vitamins and trace elements are marketed

Respiratory Distress- Enteral Nutrition• Overall evidence suggests provision of excess
energy, regardless of source leads to higher Respiratory Quotient than oxidation of Fat or CHO. Likely avoidance of any over feeding is more significant than effect of macronutrient composition.
• Standard feeds with high energy density may normally be adequate
• Effect of changes in fat and source & role of antioxidants require further studies and research to realise clinical potential

Liver Disease- Enteral NutritionPatients with co-morbidities e.g. malnutrition
• Often require increased energy and protein, but may not tolerate increases in protein
• However most patients with cirrhosis tolerate 1g Protein/kg/24hours
• Patients with severe intractable encephalopathy or hepatic failure may require protein restriction-but restrict for minimum time necessary to avoid protein malnutrition

Liver Disease- Enteral Nutrition• In hepatic failure serum concs of aromatic amino
acids (tyrosine, phenylalanine) can increase. Whilst Branched chain amino acids (BCAA) (leucine, isoleucine & valine) can decrease. Imbalance may contribute to hepatic encephalopathy.
• Suggestion of inclusion of BCAA enriched feeds may influence plasma amino acid profile and reduce incidence of encephalopathy.
• Fat content moderate with often high %age of Medium Chain Triglyercides(MCTs), low Sodium and concentrated to assist oedema and Na balance

Liver Disease- Enteral Nutrition• Most standard Protein enteral formulas can be
sufficient to maintain Nitrogen balance and avoid encephalopathy.
• Most randomized trials have not shown benefit in hepatic failure patients receiving BCAA enriched formulas.
• BCAA enriched formulas may be of benefit to patients with protein intolerance linked with encephalopathy.
• Value of BCAA enriched Enteral feeds not definitively established, but may prove of value in specific patient groups

Acute Renal Impairment- EnteralNutrition
• Fluid and Electrolyte Restrictions result in energy dense enteral nutrition (~2Kcals/ml)
• Feeds should maintain adequate levels of protein • Feeds often now provide supplementational levels of
Electrolytes due to the improved clearance by newer methods of dialysis
• Early work suggested changes to amino acid profile, provide low protein with high %age of essential amino acids, to allow for non-essential Amino acids to be synthesised via transamination to reduce nitrogenous waste. Not definitely demonstrated and probably no longer recommended

Cystic Fibrosis-Enteral Feeding
• High Energy Requirements- 130-150% of calculated expected requirements
• Considered to require energy dense feeds• Possible benefit of high fat ratio• Possible benefit of essential fatty acid provision
However need for more studies- no conclusive benefits clearly demonstrated for highly specialised feeds in large studies-more data needed

Wound Healing- Enteral Nutrition• Wound healing & pressure sores requires adequate
provision of nutrients, if inadequate the process is slow and healing is impaired.
• Adequate energy is required for tissue maintenance, repair and cell synthesis. Patients with large/severe wounds often require increased energy input
• Protein is required for cell synthesis, collagen and connective tissue formation, enhanced Protein provision may be of benefit
• Micronutrients provision is of significance to wound healing, Zinc, Vitamin A,E, C, K, thiamine and riboflavin all reported as necessary

Wound Healing- Enteral Nutrition
• Provision of specific amino acids may promote wound healing- Arginine often included in specific enteral feeds
• Effect of Arginine linked to its regulation of nucleic acid synthesis and effect on IGF-1 and role in nitric oxide and its influence on immune response.
• Optimum level of Arginine to promote wound healing is not known and feeds vary widely in provision

Wound Healing- Enteral Nutrition• Feeds are sometimes energy rich to ensure adequate
energy provision- 30-35Kcal/kg/day, often with protein up to 1.5g/kg/24hours
• Feeds invariably contain Arginine, but no consensus over dosing and overall provision
• Feeds often rich in Micronutrients in excess of normal levels of supplementationOverall nutrition is only one part of the wound healing process, good O2 in the wound, viable wound, absence of necrotic tissue, vascular sufficiency, diabetes, obesity, age, immune function all are major factors and equally important

Immune Function Enhancing(IFE)-Enteral Feeds
• Area of largest number of publications of any specialised enteral feed
• Postulated that by nutrient modulation the immune response can be normalised or enhanced
• Often known as “Nutra-Cocktails” and contain a wide variety of nutrient in combination
• Principal nutrients include, Arginine, Omega 3 fatty acids and nucleotides
• But, controversy remains & doubt of universal benefit

Immune Function Enhancing-Arginine
• Studies suggest it has a potential role in immunostimulation
• Enhances depressed immune response in trauma patients, results in improved lymphocyte response, increases T-cell function *
• Enhanced effect on wound healing*• Shown to retard tumour growth and diminishes
tumour metastasis* similar effects observed at identical doses 30g/day
in healthy subjects
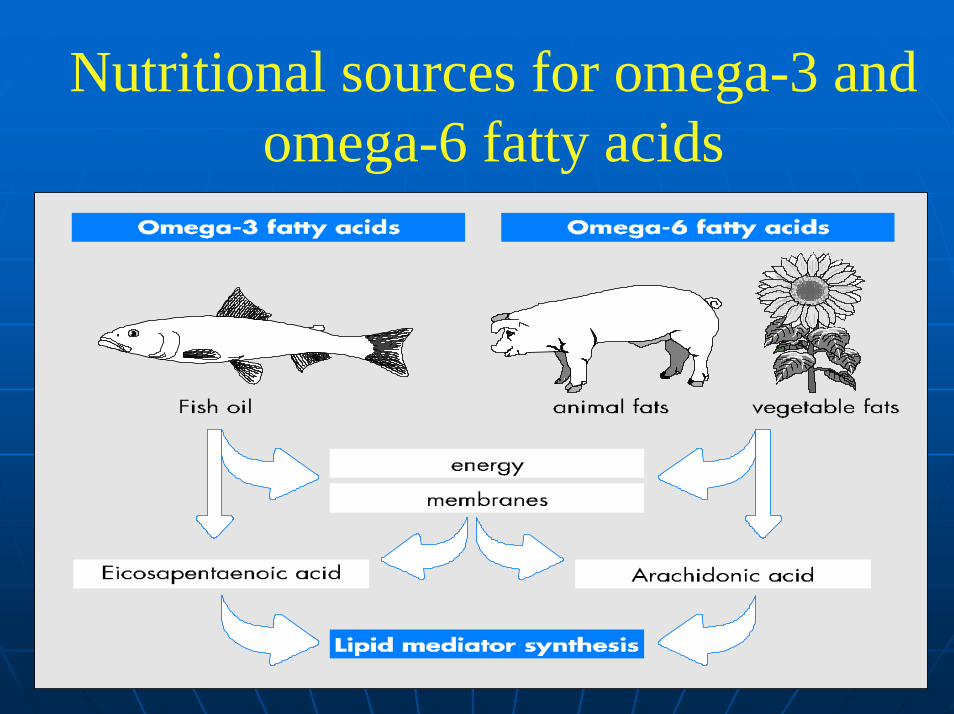
Nutritional sources for omega-3 and omega-6 fatty acids

Functions of n−3 & n−6 Fatty Acidsn−3 Fatty Acids n-6 Fatty AcidsFunctions of n−3 & n−6 Fatty Acidsn−3 Fatty Acids n-6 Fatty Acids
• Precursors of the 2 series prostaglandins, prostacylinsand thromboxanes and leukotrienes of the 4-series
• These are known inducers of inflammation and immunosuppression
• Useful in tissue graft suppression, autoimmune and inflammatory diseases, eg. Multiple sclerosis, rheumatoid arthritis ?
• Precursors of the 2 series prostaglandins, prostacylinsand thromboxanes and leukotrienes of the 4-series
• These are known inducers of inflammation and immunosuppression
• Useful in tissue graft suppression, autoimmune and inflammatory diseases, eg. Multiple sclerosis, rheumatoid arthritis ?
• Precursors of the 3 series prostaglandins, prostacylins and thromboxanes and leukotrienesof the 5 series
• These are less inflammatory and immunosuppressive & they competitively inhibit the formation of n-6 eiconsanoids
• Can therefore by inhibiting n-6 eiconsanoids stimulate the immune system, eg. Use in immunocompromised patients ?
• Precursors of the 3 series prostaglandins, prostacylins and thromboxanes and leukotrienesof the 5 series
• These are less inflammatory and immunosuppressive & they competitively inhibit the formation of n-6 eiconsanoids
• Can therefore by inhibiting n-6 eiconsanoids stimulate the immune system, eg. Use in immunocompromised patients ?

Nucleotides & NucleosidesNucleotides & Nucleosides
• Nucleotides serve as major structural units in DNA, RNA & ATP etc.
• They account for between 10-20% of non-protein Nitrogen or 5% of the total nitrogen in human milk
• Not generally regarded as essential since they are synthesized de novo from amino acids and other small molecules
• Most enteral feeds lack nucleotides
• Nucleotides serve as major structural units in DNA, RNA & ATP etc.
• They account for between 10-20% of non-protein Nitrogen or 5% of the total nitrogen in human milk
• Not generally regarded as essential since they are synthesized de novo from amino acids and other small molecules
• Most enteral feeds lack nucleotides

Nucleotides & NucleosidesNucleotides & Nucleosides
• Studies suggest that in certain circumstances de novo synthesis may be insufficient to meet requirements
• Nucleotide supplementation in experimental studies suggests they are essential to maintain immune function
• Nucleotide-free diets suppress production of helper T-cells and IL-2 whereas T-cells & macrophage populations benefit from RNA supplementation
• Studies suggest that in certain circumstances de novo synthesis may be insufficient to meet requirements
• Nucleotide supplementation in experimental studies suggests they are essential to maintain immune function
• Nucleotide-free diets suppress production of helper T-cells and IL-2 whereas T-cells & macrophage populations benefit from RNA supplementation

Immune Function Enhancing-EnteralFeeds Why controversy?• Most feeds are combination feeds- difficult to
attribute effects as single nutrient studies have not being done
• The amounts and doses adminstered, particularly of Arginine differ widely
• There may be sub sets of patients who benefit and those whose outcome may be deteriously effected
• There is “no cure all” basis for immune enhancement

Immune Function Enhancing-EnteralFeeds Why controversy?
• Several meta analysis studies have been completed, but with slightly different conclusions, mostly due to Arginine
• IFE feeds seem to benefit most surgical and trauma related patients-reduction in infections, shortened hospital stay
• IFE feeds seem of no benefit to medical, non septic ITU patients
• Use of IFE feeds in septic critically ill patient may be linked to an increase in mortality
Common Themes- SpecialisedEnteral Feeds
• The hard science and clinical outcome data is usually sporadic and can be confusing
• No specialised feed outweighs the benefit of otherwise good dietetic assessment, advice & feed selection
• Specialised Feeds tend to be more expensive • The choice of exact feeds is difficult to ascertain due to
the number of feeds on the market- all with subtle differences
• More definitive, large case studies are often required

A Clinical Reality or Marketing Exercise? Or Both?
• Application of good sciencific principles required• Clear need for good trials and regulation of claims• Evidence of benefit in certain disease states
demonstrated, but needs defining• Cocktail combinations of feeds have confused the
situation• Good basic nutrition, choice and use of feeds must
be paramount, otherwise...“You pays your money and takes your choice!”
Specialised Parenteral Nutrition Feeds
• Glutamine• Lipid Emulsion

Efficacy of L-Glutamine Supplemented TPNGriffiths et al 1997 84 Patients APACHEII
>11• No major clinical differences reported during the
patients ITU stay• 6 month survival significantly improved, after 6
months 57% vrs 33%• Total ITU costs reduced (25%) (patients either left
ITU quicker or died)• Total hospital costs reduced (15%), significantly
lower cost per ITU admission, probably due to shorter hospital stay and lower infection rates

Parenteral L-Alanyl-L-Glutamine improves 6 month outcome in critically ill patients Goeters C et al Crit Care Med 2002 Vol 30• 144 patients randomised to received 0.2g
Glutamine/kg/day, 95patients treated >5days, 68 patients >9 days, included acute renal and liver impairment
• Glutamine supplementation well tolerated in renal and temporary hepatic failure patients
• No difference in outcome if < 5 days glutamine TPN AND <9 days
• No differences in length of ITU & hospital stay • If Glutamine TPN supplementation >9 days, 6 month
mortality significantly reduced (40% vrs 66.7% control)

Glutamine Supplementation in serious illnessNovak et al Critical Care Med 2002 30 2022
• 14 RCT, 737 patients surgical/critically ill• Parenteral but not enteral glutamine- mortality risk ratio
(RR 0.71 Confidence Interval (CI)(0.51 to 0.99) • High Dose Glutamine >0.2g/kg/d (but not low dose)
reduced mortality (RR 0.73, CI 0.53 to 1.00)• Infectious complications (RR 0.81 CI(0.64-1.00)• Shorter hospital stay in surgical patients
(-3.5 days (-5.3 to-1.7 days)• Hypothesis Forming & no evidence of harm in any
study• Need to separate patient groups- clinical care/surgical?
Differences between lipid emulsions
• Triglycerides- LCT • soybean oil (Intralipid, Ivelip) • olive oil (ClinOleic)• MCT/LCT (Lipofundin,
- STG (Structolipid)• fish oil (Omegaven)
• Emulsifiers- egg phospholipids
• Additional components• Sodium Oleate-Ivelip• Vitamin E content• Particle size distribution• Mean particle diameter• PL/TG ratio• Effect on plasma lipids• Documented experience

Controversies with LCT SoyabeanOil Emulsions
• Utilization of Fat sources in the critically ill?• Development of hyperlipaemia associated with
fat deposition in the lungs and RE- controversial• Hypertriglyceridaemia occurs if metabolic
capacity to clear fat is exceeded• Source and composition of base oil?• Effects on immune function?• Effects on liver function?

Olive Oil Emulsions- Clinoleic ®• A lipid emulsion based on 80% Olive Oil, 20%
Soya bean oil• Main component ∴ Oleic Acid- mono-unsaturated
fatty acids + 20% essential fatty acids• Aim to reduce the proportion of essential fatty
acids, in particular linoleic acid to optimize metabolic functions
• Thereby production of eicosanoids, lipid mediators of inflammatory and immune response may be better balanced

Structured Triglyceride Emulsions Structolipid®
• Structolipid is a random mix of MCFA & LCFA, esterified onto the same glycerol molecule.
• Rapid source of energy for the critically ill (MCT/LCT)
• Controlled plasma triglyceride and MCFA levels
• Equivalent tolerance (of LCT : Intralipid)
• Improved protein economy

Parenteral Fish Oil Emulsions Potential Clinical Applications
• Trauma patients• Surgical patients• In early stages of sepsis/SIRS• In risk of hyper-inflammatory processes• To support immune function• Inflammatory bowel diseases
(Crohn´s disease, ulcerative colitis)
• Preterm infants

Future Lipid emulsions • Series of designer structured triglycerides combining all
the best features of LCT and MCT lipid emulsions• Protein Economy in Critically ill?• Enhancements to use the most appropriate base oils,
delivering optimal balance?• Treatment of diseases where chronic and progressive
inflammation and wasting occur, e.g. Immunomodulation & Cancer
• Lipid emulsions may be considered therapeutic as well as supportive therapy….
Common Themes- SpecialisedParenteral Feeds
• The hard science and clinical outcome data is usually similar to drug therapy, but power of small studies remains an issue
• New parenteral feeds are likely to be regulated as medicines and be pharmaceutically marketed
• Clinical trials in small numbers are a major restraint on parenteral nutrition feeds
• Specialised Feeds tend to be more expensive, but cost analysis should be compared to drug therapy
Glutamine- Is it worth the Cost?• The daily cost of an ITU patient is between ~1200-2500
Euro • The daily cost for ward patient is ~300-500 Euro • The weekly drug costs per ITU bed space is ~1800 Euro • The daily drug cost of antibiotics is Ciprofloxacin 90
Euro Primaxin 90 Euro, Vancomycin 45 Euro, Teicoplanin 78 Euro , Cef+Met 45 Euro
• The drug cost of inotopes basic support 60 Euro per day, high dose +120 Euro
• Dialysis session ~90-270 Euro • Sedation Propofol 70-140 Euro per day • Recombinant Activated Protein C ~7500-12000 Euro per
patient, Mortality Reduction 24.7% vrs 30.8%

A Clinical Reality or Marketing Exercise? Or Both?
• Application of good sciencific principles required• Evidence of benefit in certain disease states
demonstrated, but needs defining• Marketing is restricted due to regulation as medicinal
products• The expense of clinical trials and regulatory issues for
medicines may slow the development of nutritional therapy
• The cost of nutritional therapy should be considered as in drug utilisation reviews

Regulation of NutritionFoodstuffs, Nutrition Modification, Functional Foods
• EU wide Regulation of Health Claims and Promotions to be increased - Proposed EU Directive
• EU wide Regulation of composition and quantity of additives e.g Vitamins, Minerals, Amino Acids- EU Directive on Food Supplements (FSD)
• PARNUTS EU Directive and Regulation 2004 Intent to limit the medical claims, composition and number of additives (5000 reducing to ~300) and increasing regulatory control



Benefits of RegulationBenefits of Regulation
Cessation of unsubstantiated product claimsFull scale clinical trialsProof of efficacySide effects and toxicity limits ascertainedSpecific indications for useDose/Responses defined
Cessation of unsubstantiated product claimsFull scale clinical trialsProof of efficacySide effects and toxicity limits ascertainedSpecific indications for useDose/Responses defined

Risks of Over-RegulationRisks of Over-Regulation
• Reduction in research activity establishing the functional roles of nutrients
• Loss of vitality in developing nutritional support
• Limitation of corporate research due to increased R & D costs
• Manufacturers lose interest due to high cost of regulation in a limited market
• New Product Development time lengthen considerably
• Reduction in research activity establishing the functional roles of nutrients
• Loss of vitality in developing nutritional support
• Limitation of corporate research due to increased R & D costs
• Manufacturers lose interest due to high cost of regulation in a limited market
• New Product Development time lengthen considerably
Current problems with Regulation• Public perception that many products should be not
be regulated or regarded as medicines• Resistance from commercial companies and concern
over over-regulation, Market valued in 100s millions of Euros per year
• The “www” effect- difficult to legislate and control• Indifferent regulation of claims and availability• Apparent differences between over the counter
preparations, nutrition products marketed to healthcare professions and full medicinal products

Specialised Formulas for Enteraland Parenteral Nutrition
A Clinical Reality or Marketing Exercise?
• Parenteral Feeds due to regulation are based on clinical trials and proven clinical data- but slow to develop
• Enteral Feeds are increasingly regulated, this may require further restriction on medical claims for some products and need clinical trails to ensure the clinical benefits are realised
• Clinical Nutrition is perhaps unique in its regulation • Regulation is a friend and a foe of scienific clinical
nutrition, but ultimately essential