espen congress lisbon 2015 espen guidelines · espen guidelines cystic fibrosis carla ... • new...
TRANSCRIPT
ESPEN Congress Lisbon 2015
Cystic fibrosisC. Colombo (IT)
ESPEN GUIDELINES
ESPEN GuidelinesCystic fibrosis
Carla Colombo
ESPEN LISBON SEPTEMBER 2015
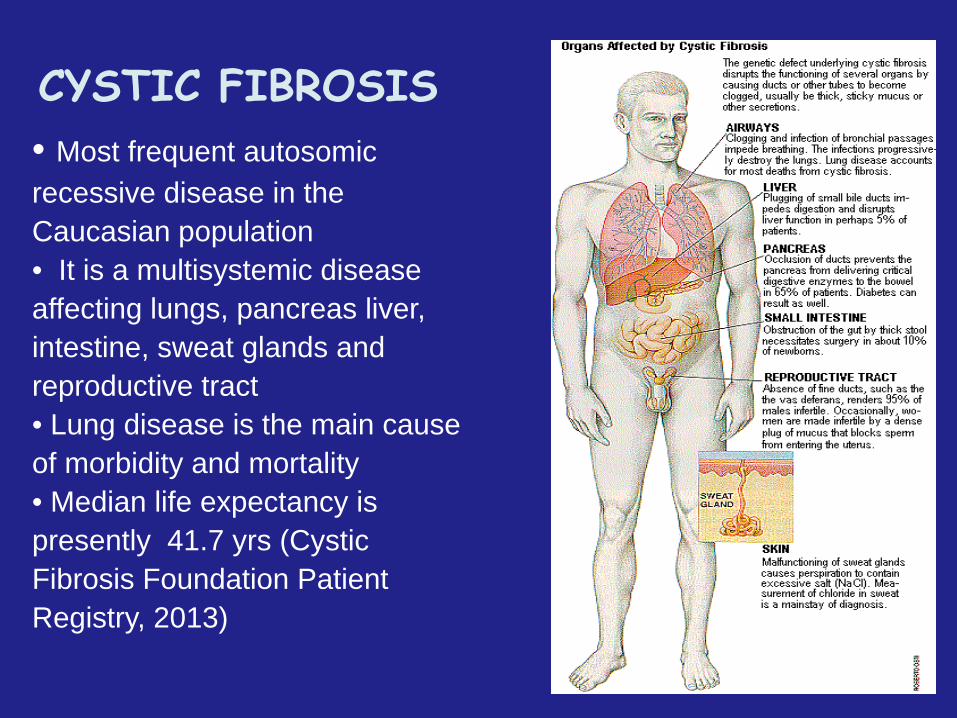
• Most frequent autosomic recessive disease in the Caucasian population• It is a multisystemic disease affecting lungs, pancreas liver, intestine, sweat glands and reproductive tract• Lung disease is the main cause of morbidity and mortality• Median life expectancy is presently 41.7 yrs (Cystic Fibrosis Foundation Patient Registry, 2013)
CYSTIC FIBROSIS

Pancreatic Enzymes
antistaphylococcal antibioticsantipseudomonal antibiotics
rhDNaseInhaled Tobramycin
Airway clearance
0
5
1015
20
25
30
35
40
1st pathologicdescription
CF geneidentified
Discoveryof high saltin sweat
Sweat chloridetest developed
1st successfulpregnancy
CF proteinidentified
AzithromycinHTS
AZLI
What next?
Age (years)
• Individual benefit is modest but cumulative• Life expectancy greatly increased
Improved Survival with Treatment InnovationIncremental Modest Benefits
Improving outcomes for CF care
• Care delivered by multidisciplinary team in specialized Centers
• Neonatal screening –best care for the screened infant
• Improvement in nutritional status• Effective treatment of infection in the early years• Transition to adult care optimal adult care• New therapies ...the importance of clinical trial networks
Toronto (1970s)
High-fat, high-energy diet
Normal growth and nutritional status
Better survival
1960s-1980s
Low fat diet often prescribed to control abdominal symptoms and maldigestion/malabsorption
As a consequence, most CF patients developed severe malnutrition and stunting due to energy imbalance
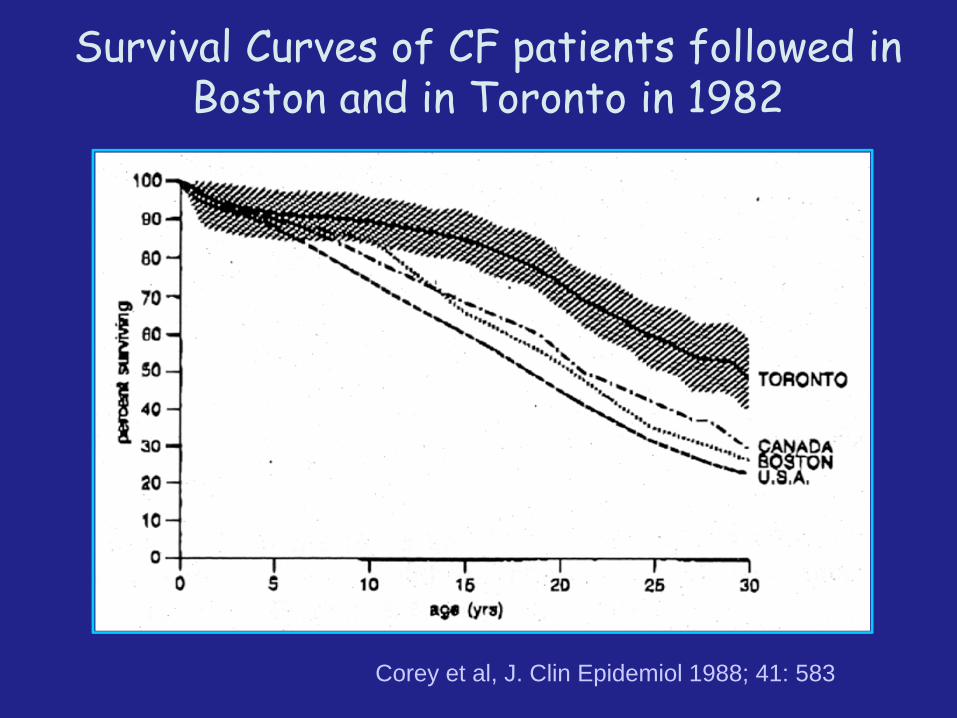
Corey et al, J. Clin Epidemiol 1988; 41: 583
Survival Curves of CF patients followed in Boston and in Toronto in 1982
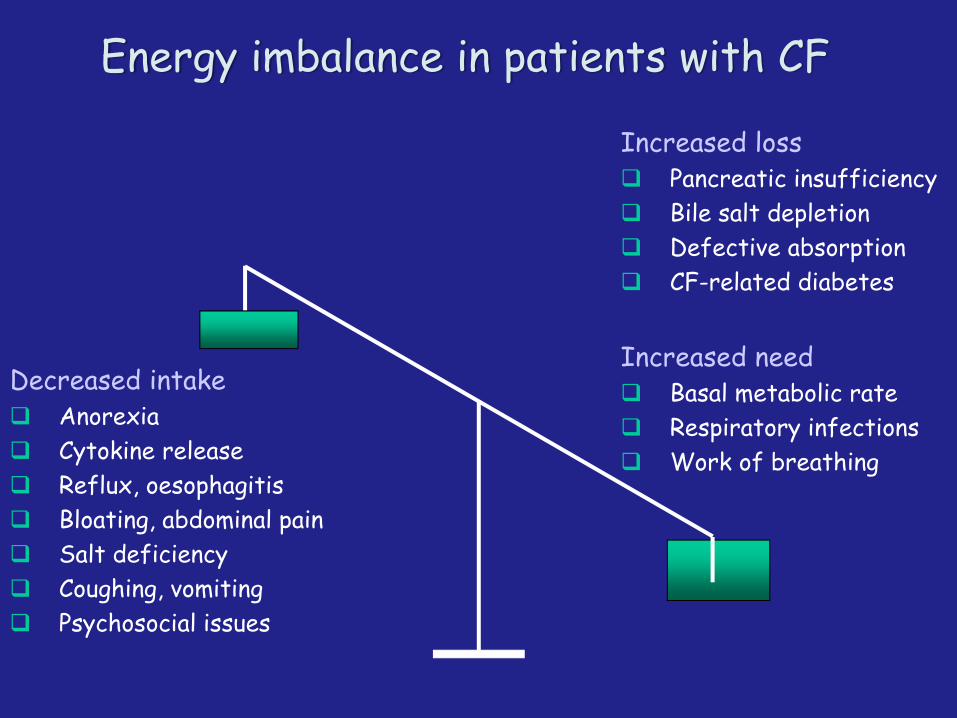
Energy imbalance in patients with CF
Decreased intakeAnorexiaCytokine releaseReflux, oesophagitisBloating, abdominal painSalt deficiencyCoughing, vomitingPsychosocial issues
Increased lossPancreatic insufficiencyBile salt depletion Defective absorptionCF-related diabetes
Increased needBasal metabolic rateRespiratory infectionsWork of breathing
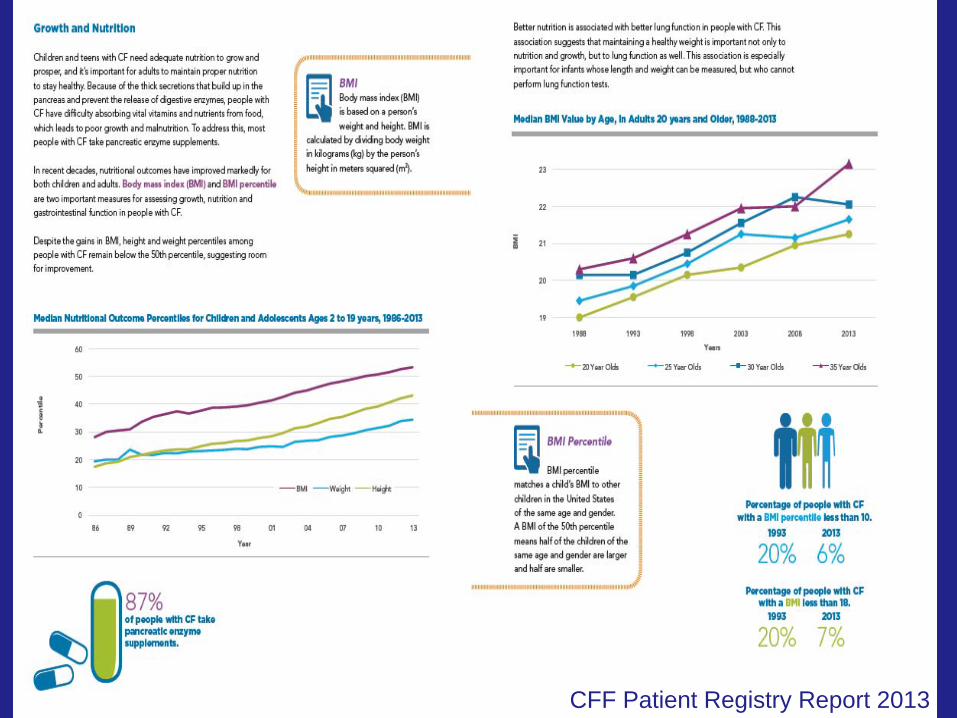
CFF Patient Registry Report 2013

ESPEN Cystic Fibrosis Guidelines Team• Christian P Braegger, MD (Switzerland)• Carla Colombo, MD (Italy)• Dimitri Declercq, MSc (Belgium)• Alison Morton, RD, BSc-Hons (UK)• Ruzha Pancheva, MD, PhD (Bulgaria)• Eddy Robberecht, MD, PhD (Belgium)• Martin Stern, MD (Germany)• Birgitta Strandvik, MD, PhD (Sweden)• Sue Wolfe, RD, BSc-Hons (UK)• Stephane M. Schneider, MD (France)• Dominique Turck, MD (France)• Michael Wilschanski, MBBS (Israel)
Currently under review by ESPGHAN and ECFS
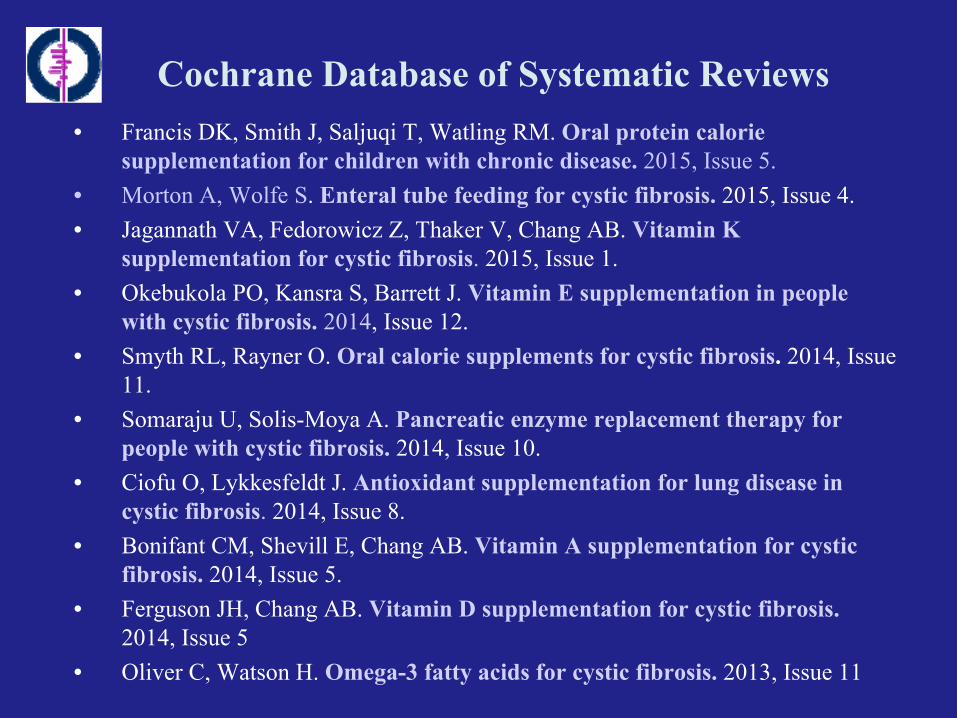
Cochrane Database of Systematic Reviews• Francis DK, Smith J, Saljuqi T, Watling RM. Oral protein calorie
supplementation for children with chronic disease. 2015, Issue 5. • Morton A, Wolfe S. Enteral tube feeding for cystic fibrosis. 2015, Issue 4.• Jagannath VA, Fedorowicz Z, Thaker V, Chang AB. Vitamin K
supplementation for cystic fibrosis. 2015, Issue 1.• Okebukola PO, Kansra S, Barrett J. Vitamin E supplementation in people
with cystic fibrosis. 2014, Issue 12.• Smyth RL, Rayner O. Oral calorie supplements for cystic fibrosis. 2014, Issue
11.• Somaraju U, Solis-Moya A. Pancreatic enzyme replacement therapy for
people with cystic fibrosis. 2014, Issue 10. • Ciofu O, Lykkesfeldt J. Antioxidant supplementation for lung disease in
cystic fibrosis. 2014, Issue 8. • Bonifant CM, Shevill E, Chang AB. Vitamin A supplementation for cystic
fibrosis. 2014, Issue 5. • Ferguson JH, Chang AB. Vitamin D supplementation for cystic fibrosis.
2014, Issue 5• Oliver C, Watson H. Omega-3 fatty acids for cystic fibrosis. 2013, Issue 11

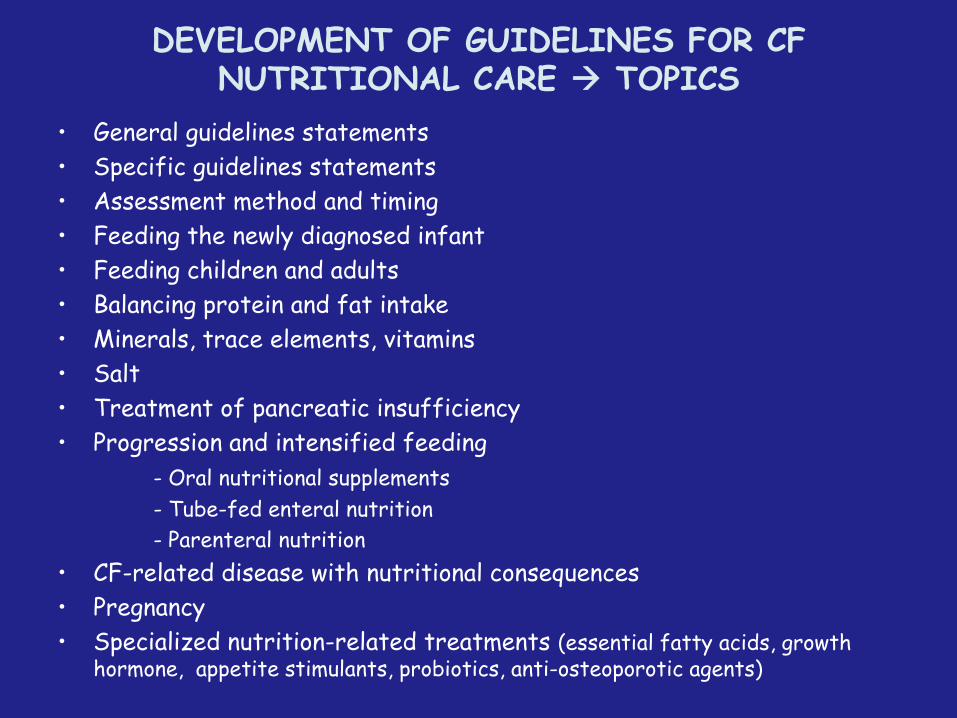
DEVELOPMENT OF GUIDELINES FOR CF NUTRITIONAL CARE TOPICS
• General guidelines statements• Specific guidelines statements• Assessment method and timing• Feeding the newly diagnosed infant• Feeding children and adults• Balancing protein and fat intake• Minerals, trace elements, vitamins• Salt• Treatment of pancreatic insufficiency• Progression and intensified feeding
- Oral nutritional supplements- Tube-fed enteral nutrition- Parenteral nutrition
• CF-related disease with nutritional consequences• Pregnancy• Specialized nutrition-related treatments (essential fatty acids, growth
hormone, appetite stimulants, probiotics, anti-osteoporotic agents)
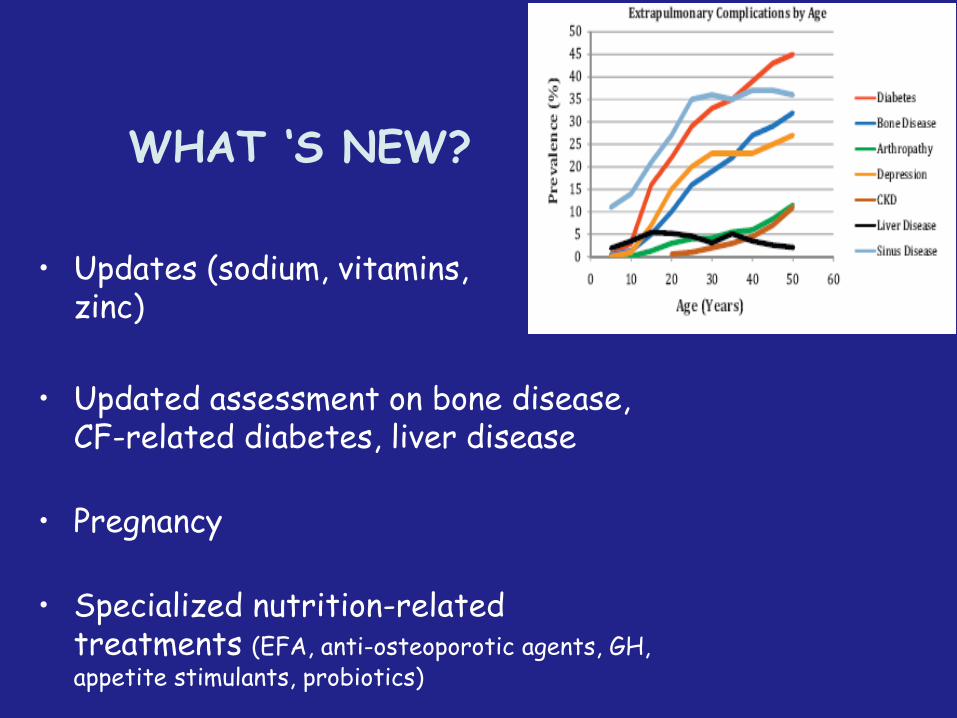
WHAT ‘S NEW?
• Updates (sodium, vitamins, zinc)
• Updated assessment on bone disease, CF-related diabetes, liver disease
• Pregnancy
• Specialized nutrition-related treatments (EFA, anti-osteoporotic agents, GH, appetite stimulants, probiotics)

Screen all newborns for CF, and initiate nutrition care early.
Monitor nutritional status by routine assessment of relevant anthropometric parameters.
Prevent or delay onset of nutrition deficits by nutrition counseling, high-energy intake, supplemental vitamins and minerals, and PERT.
Advise parents/patients on balanced macronutrient intake, especially adequate protein and fat.
Manage under-nutrition by diagnosing inadequacy, treating underlying causes, and compensating specific deficiencies.
General recommendations for 2015 CF nutrition care
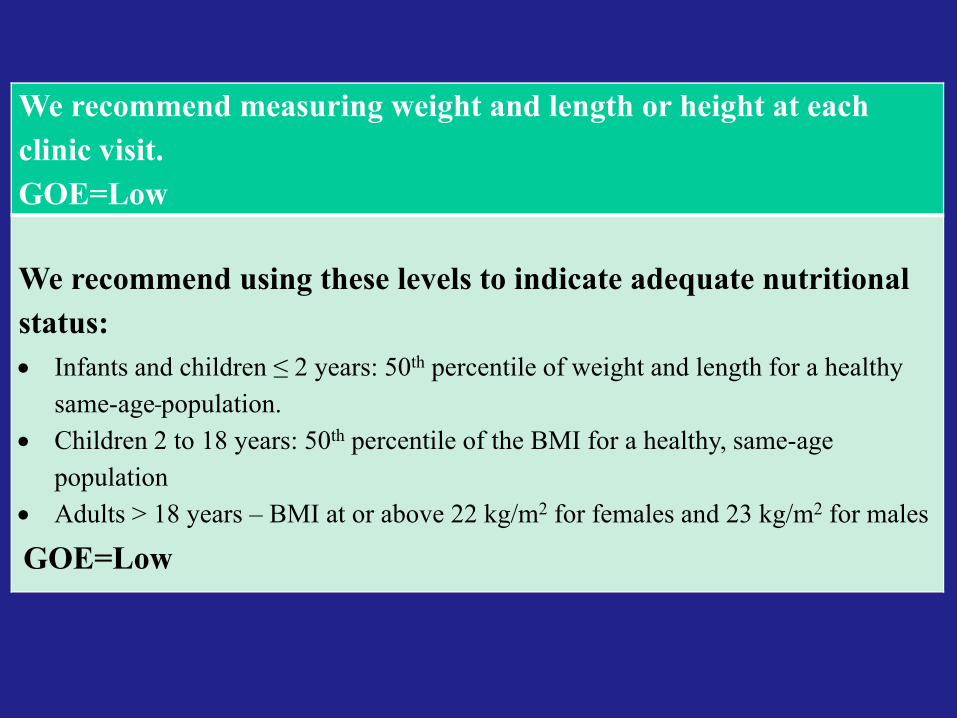
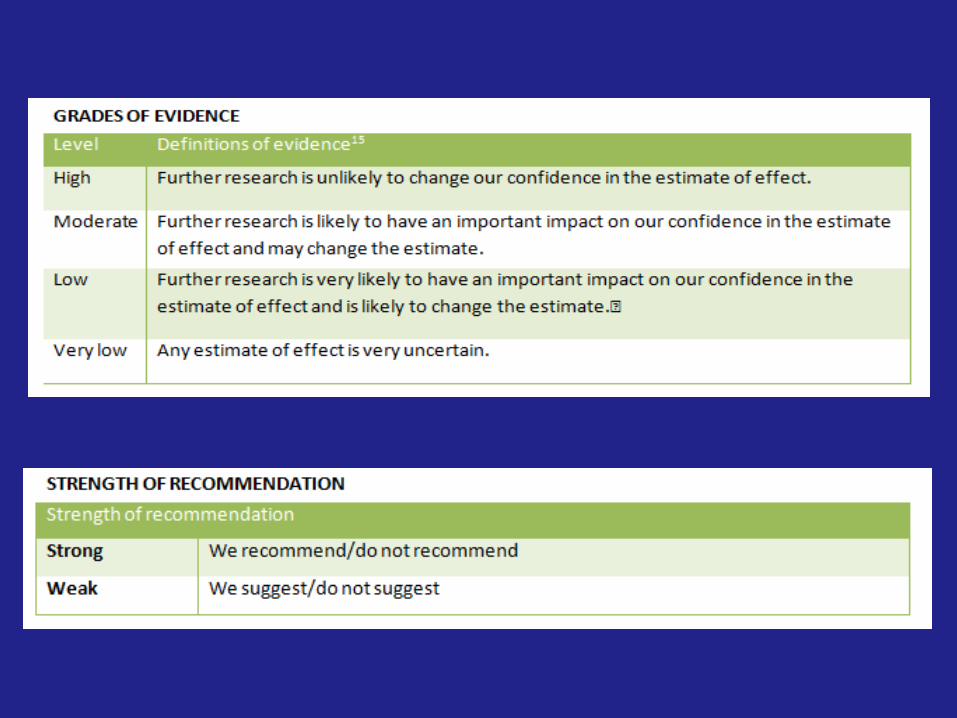
We recommend measuring weight and length or height at each clinic visit. GOE=Low
We recommend using these levels to indicate adequate nutritional status: • Infants and children ≤ 2 years: 50th percentile of weight and length for a healthy
same-age population. • Children 2 to 18 years: 50th percentile of the BMI for a healthy, same-age
population• Adults > 18 years – BMI at or above 22 kg/m2 for females and 23 kg/m2 for males
GOE=Low
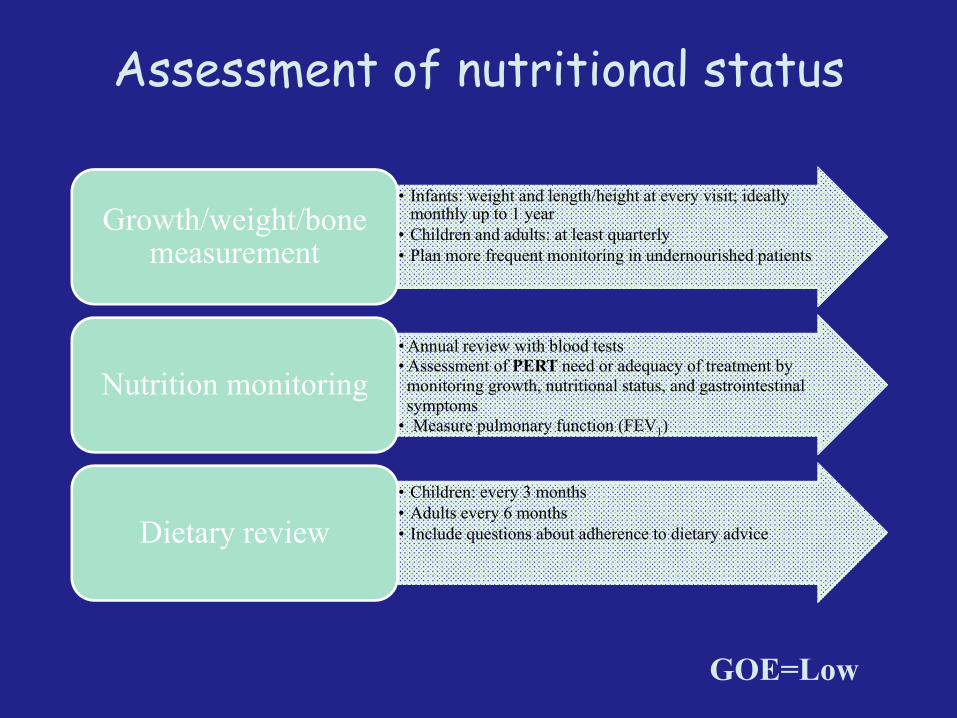
Assessment of nutritional status
• Infants: weight and length/height at every visit; ideally monthly up to 1 year
• Children and adults: at least quarterly• Plan more frequent monitoring in undernourished patients
Growth/weight/bone measurement
• Annual review with blood tests• Assessment of PERT need or adequacy of treatment bymonitoring growth, nutritional status, and gastrointestinalsymptoms
• Measure pulmonary function (FEV1)
Nutrition monitoring
• Children: every 3 months• Adults every 6 months• Include questions about adherence to dietary adviceDietary review
GOE=Low
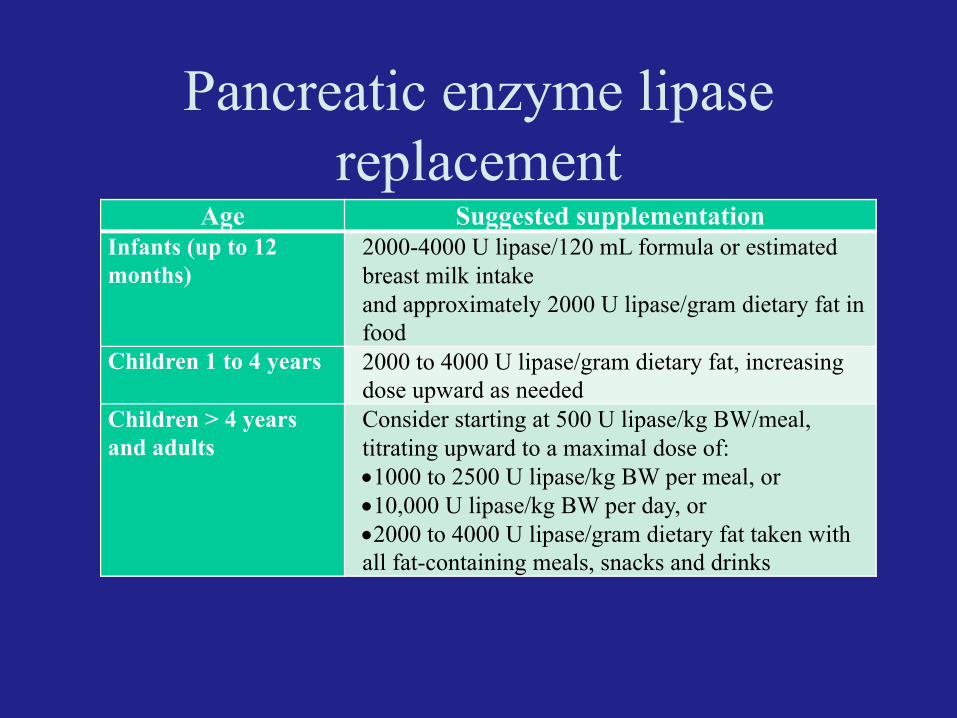
Pancreatic enzyme lipase replacement
Age Suggested supplementationInfants (up to 12 months)
2000-4000 U lipase/120 mL formula or estimated breast milk intake and approximately 2000 U lipase/gram dietary fat in food
Children 1 to 4 years 2000 to 4000 U lipase/gram dietary fat, increasing dose upward as needed
Children > 4 years and adults
Consider starting at 500 U lipase/kg BW/meal, titrating upward to a maximal dose of:•1000 to 2500 U lipase/kg BW per meal, or •10,000 U lipase/kg BW per day, or•2000 to 4000 U lipase/gram dietary fat taken with all fat-containing meals, snacks and drinks
The self-management of enzyme replacement in the European cysticfibrosis (CF) patients by means of a mobile application (APP) that allows fora personalised and accurate control and monitoring of pancreaticinsufficiency thanks to the interaction between patients and healthprofessionals.
AIM of the Project
www.mycyfapp.eu

Assess body composition (dual-energy X-ray absorptiometry, DXA), including bone health, for all patients ≥ 8 years old.
Assess calcium intake at least annually
Screen all CF patients ≥ 10 years for glucose tolerance.
For women with CF who are or plan to become pregnant, we recommend increasing the frequency of monitoring and continuing after delivery.
Assess pancreatic function yearly in pancreatic sufficientpatients by fecal elastase-1, with the test repeated if growth is
inadequate.
Specific recommendations for 2015 CF nutrition care
GOE=Low
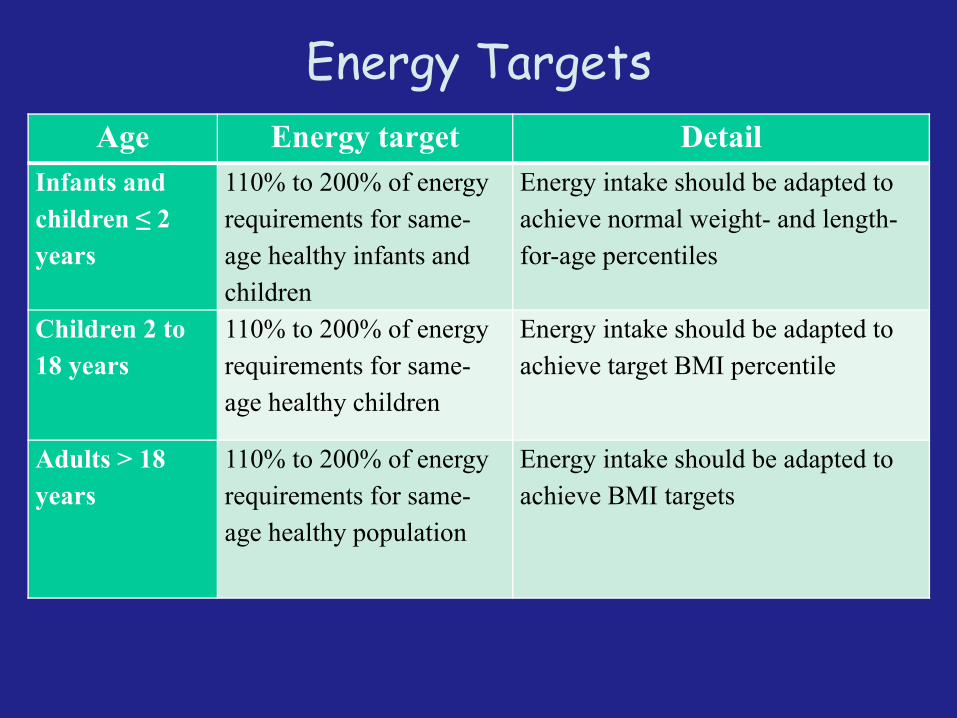
Energy TargetsAge Energy target Detail
Infants and children ≤ 2 years
110% to 200% of energy requirements for same-age healthy infants and children
Energy intake should be adapted to achieve normal weight- and length-for-age percentiles
Children 2 to 18 years
110% to 200% of energy requirements for same-age healthy children
Energy intake should be adapted to achieve target BMI percentile
Adults > 18 years
110% to 200% of energy requirements for same-age healthy population
Energy intake should be adapted to achieve BMI targets
Curr Opin Clin Nutr Metab Care 2014;17:515-520.

Sodium supplementation Europe vs US
AgeSodium
supplement*Detail
Breastfed infants 0 to 6 months
1–2 mmolper kg bw/day
For infants at risk of sodium deficiency give salt in small portions throughout the day, diluted in water or fruit juice.
For infants with special considerations
Up to 4 mmol per kg bw/day
Increase intake for infants living in hot ambient temperatures; or for those with increased fluid loss due to vomiting, fever, diarrhea, or tachypnea; or infants with ostomies.
Older children through adults
Salty foods or sodium chloride capsules or vials
Supplement in stress situations when excessive sweating is expected (i.e., fever, exercise/sports, hot weather).
We recommend assessing infants’ needs for sodium supplementation on an individual basis, taking climate and sodium losses into consideration, by measuring fractional excretion of sodium (FENa) or urinary sodium: creatinine ratio

Daily zinc supplementation
AgeRecommended
supplementationRecommended dosing
period
Infants and children < 2 years and at risk of zinc insufficiency
1 mg/kg/day(max 15 mg/day)
6 months
Children 2 to 18 years andat risk of zinc insufficiency
15 mg/day 6 months
Adults > 18 years andat risk of zinc insufficiency
25 mg/day 6 months
We suggest zinc supplementation for people with CF who are at risk of zinc insufficiency (e.g., growth retardation, increased susceptibility to infections, delayed sexual maturation, eye problems, and anorexia).GOE=Low
Fat Soluble Vitamins
Vitamin A
Vitamin D
Vitamin E
Vitamin K
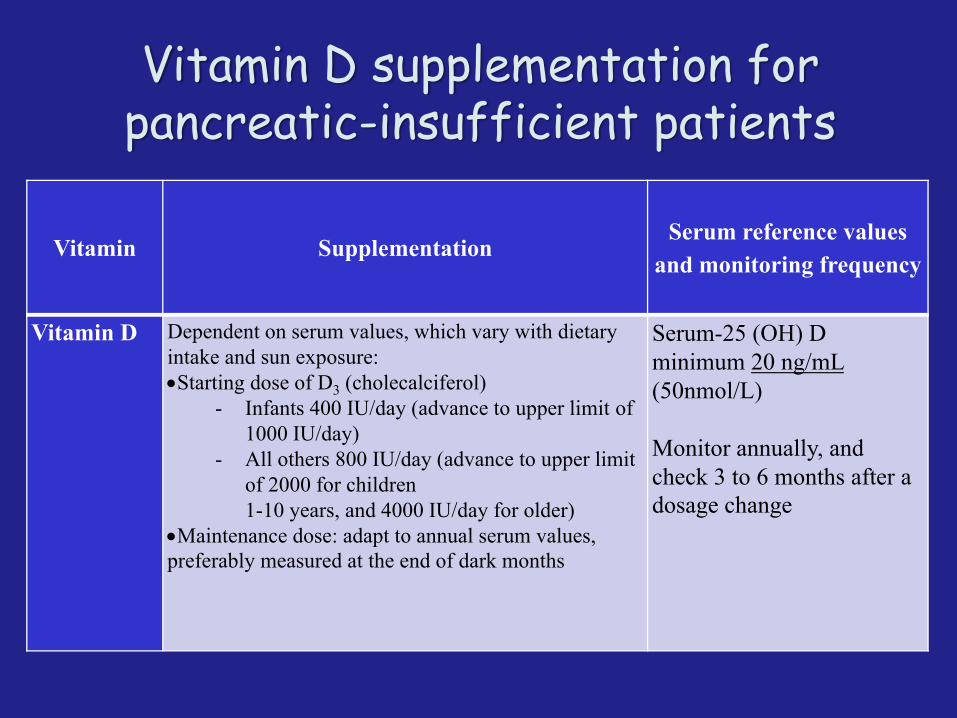
Vitamin D supplementation for pancreatic-insufficient patients
Vitamin SupplementationSerum reference values
and monitoring frequency
Vitamin D Dependent on serum values, which vary with dietary intake and sun exposure:•Starting dose of D3 (cholecalciferol)
- Infants 400 IU/day (advance to upper limit of 1000 IU/day)
- All others 800 IU/day (advance to upper limit of 2000 for children 1-10 years, and 4000 IU/day for older)
•Maintenance dose: adapt to annual serum values, preferably measured at the end of dark months
Serum-25 (OH) Dminimum 20 ng/mL (50nmol/L)
Monitor annually, and check 3 to 6 months after a dosage change
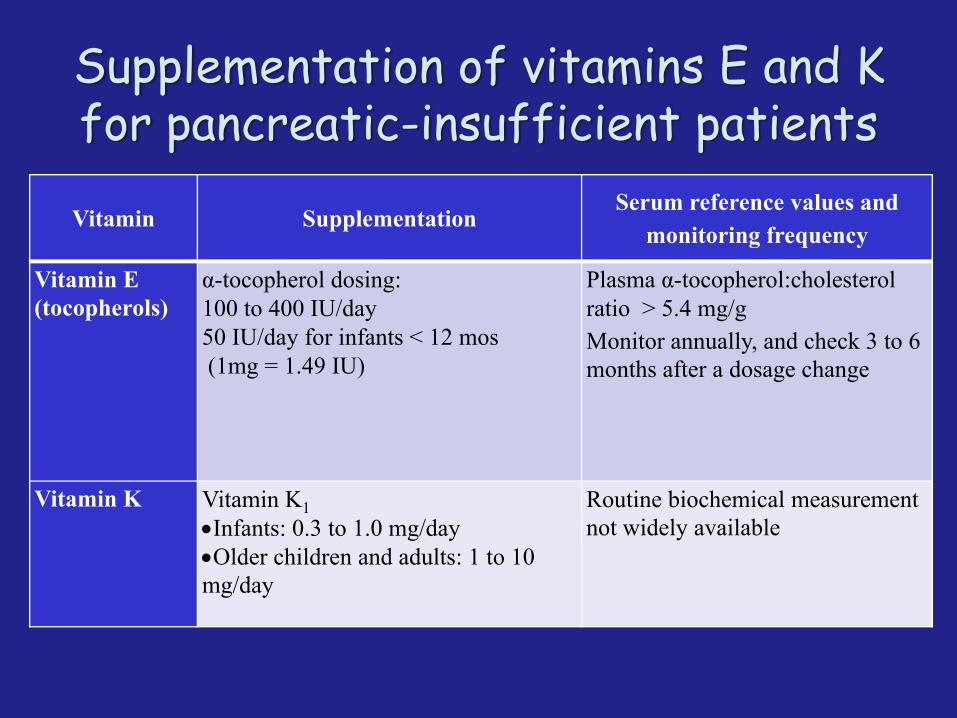
Supplementation of vitamins E and K for pancreatic-insufficient patients
Vitamin SupplementationSerum reference values and
monitoring frequency
Vitamin E (tocopherols)
α-tocopherol dosing:100 to 400 IU/day 50 IU/day for infants < 12 mos(1mg = 1.49 IU)
Plasma α-tocopherol:cholesterol ratio > 5.4 mg/g Monitor annually, and check 3 to 6 months after a dosage change
Vitamin K Vitamin K1•Infants: 0.3 to 1.0 mg/day•Older children and adults: 1 to 10 mg/day
Routine biochemical measurement not widely available
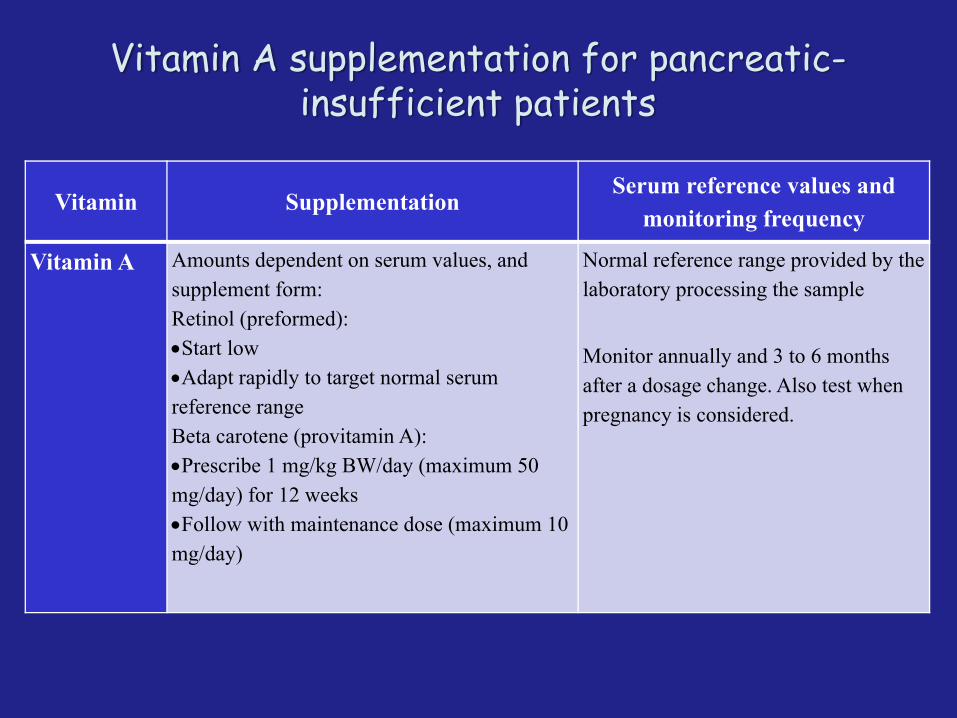
Vitamin A supplementation for pancreatic-insufficient patients
Vitamin SupplementationSerum reference values and
monitoring frequency
Vitamin A Amounts dependent on serum values, and supplement form:Retinol (preformed):•Start low•Adapt rapidly to target normal serum reference range Beta carotene (provitamin A):•Prescribe 1 mg/kg BW/day (maximum 50 mg/day) for 12 weeks•Follow with maintenance dose (maximum 10 mg/day)
Normal reference range provided by the laboratory processing the sample
Monitor annually and 3 to 6 months after a dosage change. Also test when pregnancy is considered.
Guidelines: Nutrition intervention
• We recommend nutrition intervention based on a full review of nutrition status, including a detailed review of pancreatic enzyme replacement therapy (PERT), and correction of any underlying medical conditions.GOE=High
• We recommend using age-appropriate BMI-related thresholds for deciding when to advance nutrition intervention. GOE=High
• We recommend a progressive approach to intensification of nutrition interventions as needs increase: preventive nutritional counseling, dietary modification and/or oral nutrition supplements, and enteral tube feeding. GOE=Low
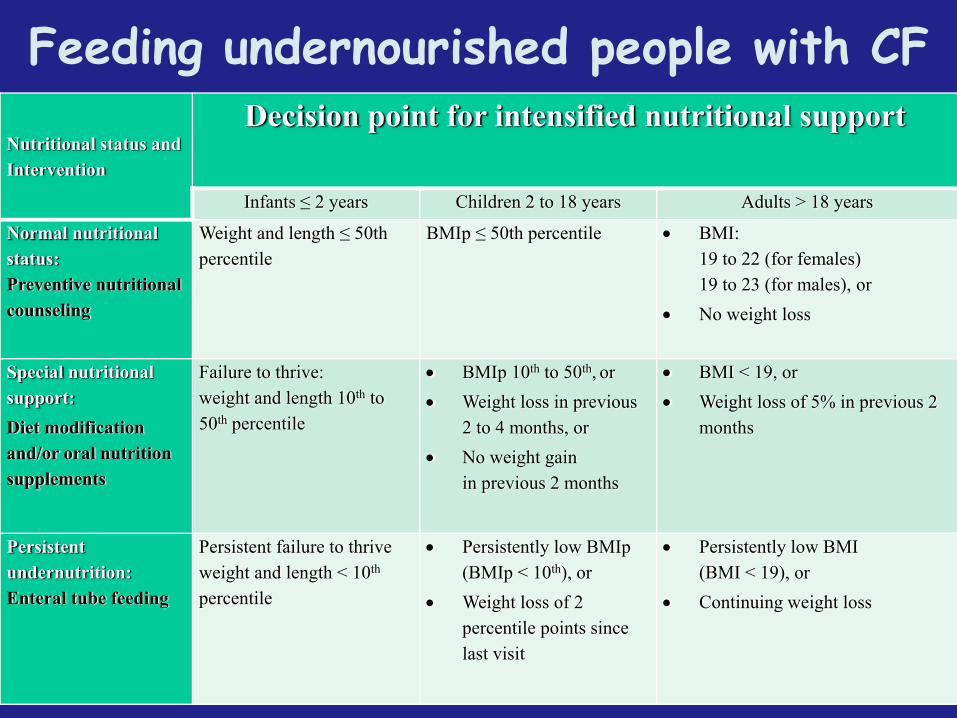
Nutritional status and Intervention
Decision point for intensified nutritional support
Infants ≤ 2 years Children 2 to 18 years Adults > 18 years
Normal nutritional status: Preventive nutritional counseling
Weight and length ≤ 50th percentile
BMIp ≤ 50th percentile • BMI:19 to 22 (for females)19 to 23 (for males), or
• No weight loss
Special nutritional support: Diet modification and/or oral nutrition supplements
Failure to thrive:weight and length 10th to 50th percentile
• BMIp 10th to 50th, or• Weight loss in previous
2 to 4 months, or• No weight gain
in previous 2 months
• BMI < 19, or• Weight loss of 5% in previous 2
months
Persistent undernutrition:Enteral tube feeding
Persistent failure to thriveweight and length < 10th
percentile
• Persistently low BMIp (BMIp < 10th), or
• Weight loss of 2 percentile points since last visit
• Persistently low BMI(BMI < 19), or
• Continuing weight loss
Feeding undernourished people with CF

Acknowledgements• The systematic review and grading of the evidence were
performed by Prof Leonard Leibovici and DrVeredZarezky from Rabin Medical Centre, Beilinson Hospital and Sackler Faculty of Medicine, Tel-Aviv University, Ramat-Aviv, Israel.
• We thank Cecilia Hofmann, PhD, for her valued assistance with compilation of the medical literature and with editing this English-language guideline.