esophagus and stomach surgical pathology 2015
DESCRIPTION
Lecture by Doc SilvaTRANSCRIPT

ESOPHAGUS and STOMACH AZESU O. SILVA, MD, DPSP (AP-CP)Surgical Pathology
ESOPHAGUS Mouth to stomach- Passage for
food and water Swallow then coordinated wave of
peristaltic contractions Motor disorders:
o “nutcracker esophagus” –Outer longitudinal and inner circular smooth muscle – lack of coordination
o Diffuse esophageal spasm –wall stress-small outpouching (pseudodiverticula = lacks true muscularis)
NORMAL hollow muscular highly distensible
tube epiglottis- (C6), GE junction-(T11 to
T12) 10-11 cm children, 25 cm adult Endoscopist- esophagus- between
15 and 45 cm from incisor/ GE junction at 40 cm
points of narrowing:1. CRICOID CARTILAGE2. ALONGSIDE AORTIC ARCH 3. PIERCINGDIAPHRAGM
NORMALLY NEGATIVE PRESSURE IN LUMEN- but with 2 higher pressure areas, contracted in resting phase:
1. IN PROXIMAL ESOPHAGUS, 3 CM SEGMENT- CRICOPHARYNGUS MUSCLE LEVEL (UES)
2. PROXIMAL TO GE JUNCTION, 2-4 CM SEGMENT- DIAPHRAGM LEVEL (LES)
* Physiologic sphincters- no anatomic landmarks
HISTOLOGY 1. MUCOSA2. SUBMUCOSA3. MUSCULARIS PROPRIA4. ADVENTITIA
MUCOSA non-keratinizing strat. sq.
epithelium (matured squamous and basal cells) * specialized cells- melanocytes, endocrine cells, dendritic cells, lymphocytes
lamina propria – areolar CT, blood vessels, leukocytes
muscularis mucosa – longitudinally arranged smooth muscle cells
SUBMUCOSA1
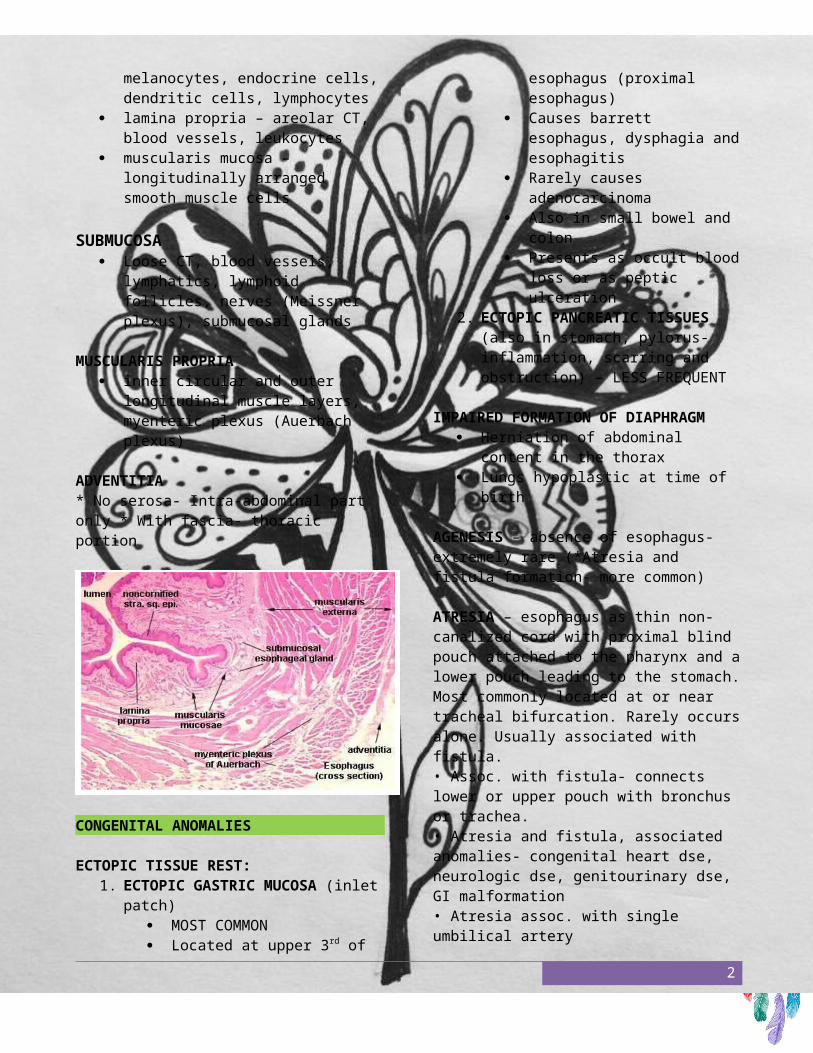
Loose CT, blood vessels, lymphatics, lymphoid follicles, nerves (Meissner plexus), submucosal glands
MUSCULARIS PROPRIA inner circular and outer
longitudinal muscle layers, myenteric plexus (Auerbach plexus)
ADVENTITIA* No serosa- Intra-abdominal part only * With fascia- thoracic portion
CONGENITAL ANOMALIES
ECTOPIC TISSUE REST: 1. ECTOPIC GASTRIC MUCOSA
(inlet patch) MOST COMMON Located at upper 3rd of
esophagus (proximal esophagus)
Causes barrett esophagus, dysphagia and esophagitis
Rarely causes adenocarcinoma
Also in small bowel and colon
Presents as occult blood loss or as peptic ulceration
2. ECTOPIC PANCREATIC TISSUES (also in stomach, pylorus- inflammation, scarring and obstruction) – LESS FREQUENT
IMPAIRED FORMATION OF
DIAPHRAGM Herniation of abdominal content in
the thorax Lungs hypoplastic at time of birth
AGENESIS – absence of esophagus- extremely rare (*Atresia and fistula formation- more common)
ATRESIA – esophagus as thin non-canalized cord with proximal blind pouch attached to the pharynx and a lower pouch leading to the stomach. Most commonly located at or near tracheal bifurcation. Rarely occurs alone. Usually associated with fistula. • Assoc. with fistula- connects lower or upper pouch with bronchus or trachea. • Atresia and fistula, associated anomalies- congenital heart dse, neurologic dse, genitourinary dse, GI malformation • Atresia assoc. with single umbilical artery • Aspiration and paroxysmal suffocation from food, hazards. Pneumonia and severe electrolyte imbalance.
ESOPHAGEAL ATRESIA AND TRACHEOSEPHAGEAL FISTULA
Type C most common Blind upper segment and fistula
between lower segment and trachea
ESOPHAGEAL MUCOSAL WEBS ledge like mucosal protrusion,
usually at UE semicircumferential, eccentric Composed of squamous mucosa
and vascular submucosa Congenital, or in long standing
2

reflux esophagitis, chronic GVHD and blistering skin disease
If accompanied by: iron def anemia, glossitis, cheilosis = PATERSON-BROWN-KELLY OR PLUMMER-VINSON SYNDROME with risk of postcricoid esophageal carcinoma
Main symptom- dysphagia with incompletely chewed food
NORMAL WEB
ESOPHAGEAL RING or Schatzki ring concentric and thicker plates,
distal esophagus A ring- above the GE junction B ring - at the squamocolumnar
junction (with Gastric type mucosa) Mucosa, submucosa and
hypetrtophied muscularis propria, Gastric type mucosa (B ring)
NORMAL ESOPHAGEAL RING
WEBS AND RINGS common in female, 40 yo,
uncertain etiology Main symptom- episodic dysphagia Pain is infrequent
ESOPHAGEAL STENOSIS fibrous thickening, submucosa,
with atrophy of muscularis propria, thin ulcerated lining epithelium
Occasionally congenital most common cause severe injury
with inflammatory scarring (chronic GE reflux, irradiation, caustic injury)
Develops slowly in adulthood progressive dysphagia (solid then
fluid)
NORMAL STENOSIS
LESIONS ASSOCIATED WITH MOTOR DYSFUNCTION
ACHALASIA HIATAL HERNIA DIVERTICULUM MALLORY-WEISS TEAR
ACHALASIA failure to relax Major abnormalities: aperistalsis,
partial or complete relaxation of LES with swallowing, increased resting tone of LES
PRIMARY: UNCERTAIN ETIOLOGY MOSTLY
Dysfunction of inhibitory neurons containing NO2 and vasoactive intestinal peptide (VIP), neural innervation degenerative changes (vagus nerve)
SECONDARY: Chaga’s disease (T cruzi) myenteric plexus destruction, failure of peristalsis and esophageal dilatation
ACAHALASIA LIKE DISEASEo diabetic autonomic
neuropathyo Disorders of dorsal motor
nuclei- polio, surgical
3

ablation (amputation, excision) –
o Infiltrative disorder- malignancy, amyloidosis, sarcoidosis
Treatment Myotomy, pneumatic balloon
dilatation Botulinum toxin (botox)- inhibits
LES cholinergic neurons
MORPHOLOGY Progressive dilatation above LES,
wall with normal thickness Absent myenteric ganglia, but may
or may not be reduced at LES area Ulcer, inflammation or fibrotic
thickening above the LES Development of SQUAMOUS CELL
CARCINOMA (5% OF CASES)
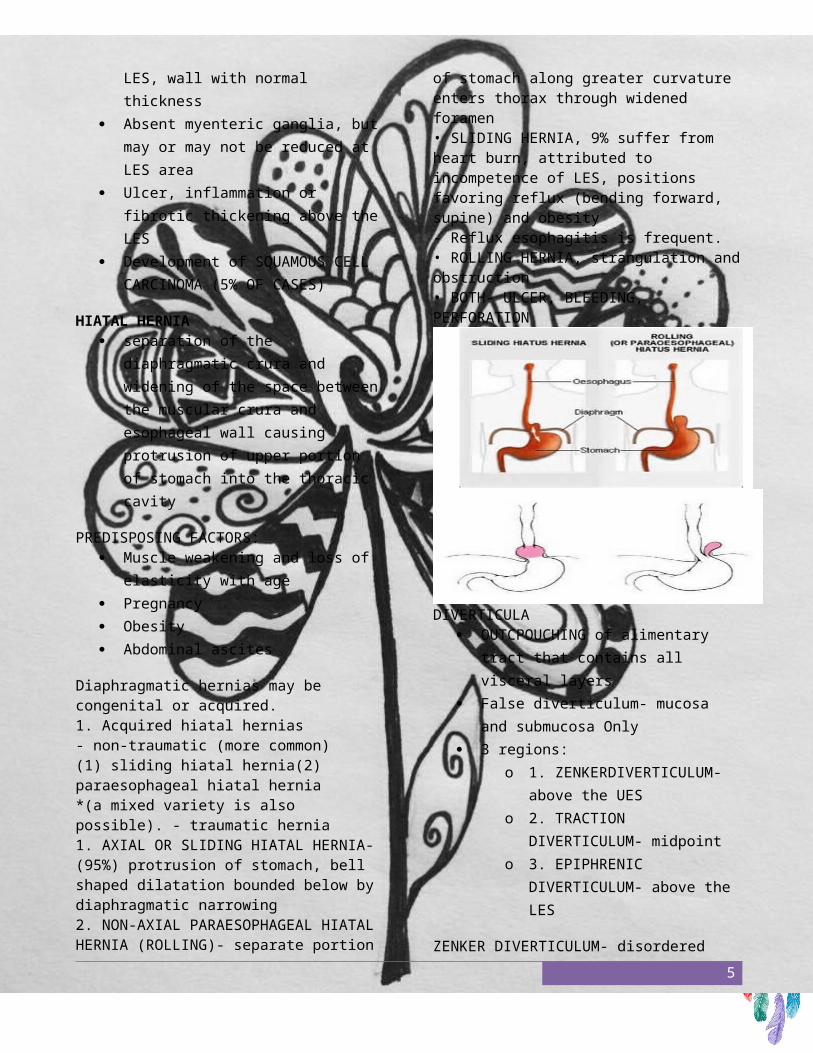
HIATAL HERNIA separation of the diaphragmatic
crura and widening of the space between the muscular crura and esophageal wall causing protrusion
of upper portion of stomach into the thoracic cavity
PREDISPOSING FACTORS: Muscle weakening and loss of
elasticity with age Pregnancy Obesity Abdominal ascites
Diaphragmatic hernias may be congenital or acquired. 1. Acquired hiatal hernias- non-traumatic (more common) (1) sliding hiatal hernia(2) paraesophageal hiatal hernia *(a mixed variety is also possible). - traumatic hernia 1. AXIAL OR SLIDING HIATAL HERNIA- (95%) protrusion of stomach, bell shaped dilatation bounded below by diaphragmatic narrowing 2. NON-AXIAL PARAESOPHAGEAL HIATAL HERNIA (ROLLING)- separate portion of stomach along greater curvature enters thorax through widened foramen • SLIDING HERNIA, 9% suffer from heart burn, attributed to incompetence of LES, positions favoring reflux (bending forward, supine) and obesity - Reflux esophagitis is frequent. • ROLLING HERNIA, strangulation and obstruction • BOTH- ULCER, BLEEDING, PERFORATION
4
DIVERTICULA OUTCPOUCHING of alimentary
tract that contains all visceral layers
False diverticulum- mucosa and submucosa Only
3 regions:o 1. ZENKERDIVERTICULUM-
above the UESo 2. TRACTION
DIVERTICULUM- midpointo 3. EPIPHRENIC
DIVERTICULUM- above the LES
ZENKER DIVERTICULUM- disordered cricopharyngeal motor dysfunction w/ or w/o GERD and diminished luminal size of UES.
TRACTION DIVERTICULUM- Scarring sec to lymphadenitis (TB), causes traction to esophagus.
EPIPHRENIC DIVERTICULUM- Discoordinated peristalsis and LES relaxation.
ZENKER’S DIVERTICULUM
ESOPHAGITIS • LACERATIONS (MALLORY WEISS SYNDROME)
- longitudinal tears in the esophagus at the esophago-gastric junction or gastric cardia, severe retching or vomiting, in alcoholics - relaxation fails to occur during prolonged vomiting - Underlying hiatal hernia is a predisposing factor - Infection may lead to inflammatory ulcer or to
5

mediastinitis - Distal esophageal rupture, “BOERHAAVE SYNDROME”
MALLORY-WEISS TEAR
ESOPHAGEAL VARICES • prolonged or severe portal
hypertension due to formation of collateral bypass channels wherever portal and caval system communicate
• Develops in 90% of cirrhotic patients - Alcoholic cirrhosis - Hepatic schistosomiasis
• Dilated veins- in submucosa of distal esophagus and proximal stomach
• Also dilated venous channels beneath the esophageal epithelium
ESPHAGEAL VARICES
• Clinically- no symptoms until they rupture • half of cirrhotic patients die from rupture of varices. ESOPHAGITIS • Normally submucosal glands-
bicarbonate and mucin- mucosal protection
• inflammation of esophageal mucosa • physical chemical and biological agents
• REFLUX ESOPHAGITIS associated with the clinical condition-GERD- - decreased efficiency of esophageal anti-reflux mechanisms, LES tone- CNC depressant, pregnancy - In Sliding hiatal hernia - Inadequate slowed esophageal clearance or refluxed material - Delayed gastric emptying and increased gastric volume - Reduction of reparative capacity by protracted exposure to gastric acid. - Gastric juice and bile (severe cases) from duodenum
Morphology
6

• Hyperemia- inflamm cells (N,E,L) in squamous epithelial layer • Basal zone hyperplasia >20 % of wall thickness • elongation or lamina propria papillae with capillary congestion
REFLUX ESOPHAGITIS-GERD
REFLUX ESOPHAGITIS-GERD
• EOSINOPHILS-EARLYHISTOLOGICABNORMALITY • NEUTROPHILS-MORESEVEREINJURY,INULCER • Most common in adults 40 yo • Infant and children also • Dysphagia, heart burn, regurgitation of sour tasting gastric content (less
frequently) • Complications: ulceration, hematamesis, melena, stricture, barrett esophagus BARRETT ESOPHAGUS • Complication of long standing GERD • In 10% of symptomatic GERD patients • Simple most important risk factor for
ESOPHAGEAL ADENOCARCINOMA. • Distal squamous mucosa is replaced by
metaplastic columnar epithelium as response to injury.
• Criteria:1. Endoscopic evidence of columnar epithelial lining above the GE junction 2. Histologic evidence of intestinal metaplasia of columnar epithelium
• Classification: 1. 2. • • LONG SEGMENT – extending cephalad more than 3 cm from the manometric GE junction SHORT SEGMENT- extending less than 3cm cephalad. Pathogenesis is unclear but it appears to be as a result of alteration in the differentiation of the stem cells of the esophageal mucosa. Esophageal squamous epithelium is replaced by metaplastic epithelium- Goblet cells and intestinal columnar cells. • Important is to search also for
dysplasia, low grade or high grade.
• 50% of patient with High grade dysplasia may already have adenocarcinoma
• Clinical- 40-60 yo, white males, local ulceration, bleeding, stricture
• Long segment- 30-40 fold inc risk for Adenocarcinoma
• Short segment- unknown risk BARRETT ESOPHAGUS
7

BARRETT ESOPHAGUS
INFECTIOUS AND CHEMICAL ESOPHAGITIS ORIGINS: • Mucosalirritants-
alcohol,corrosivealkaliand acid and heavy smoking
• Cytotoxic anticancer therapy • Infection followed by bacteremia or
Viremia: HSV, CMV (common offenders in immunocompromised patients)
• Fungal infection candidiasis, mucormycosis, aspergillosis
• Uremia in setting of renal failure
• following irradiation, systemic GVHD, autoimmune dse, desquamative dermatologic conditions, Chron disease
Morphology • Final common pathway is severe acute
inflammation, superficial necrosis and ulceration with granulation tissue formation and eventual fibrosis
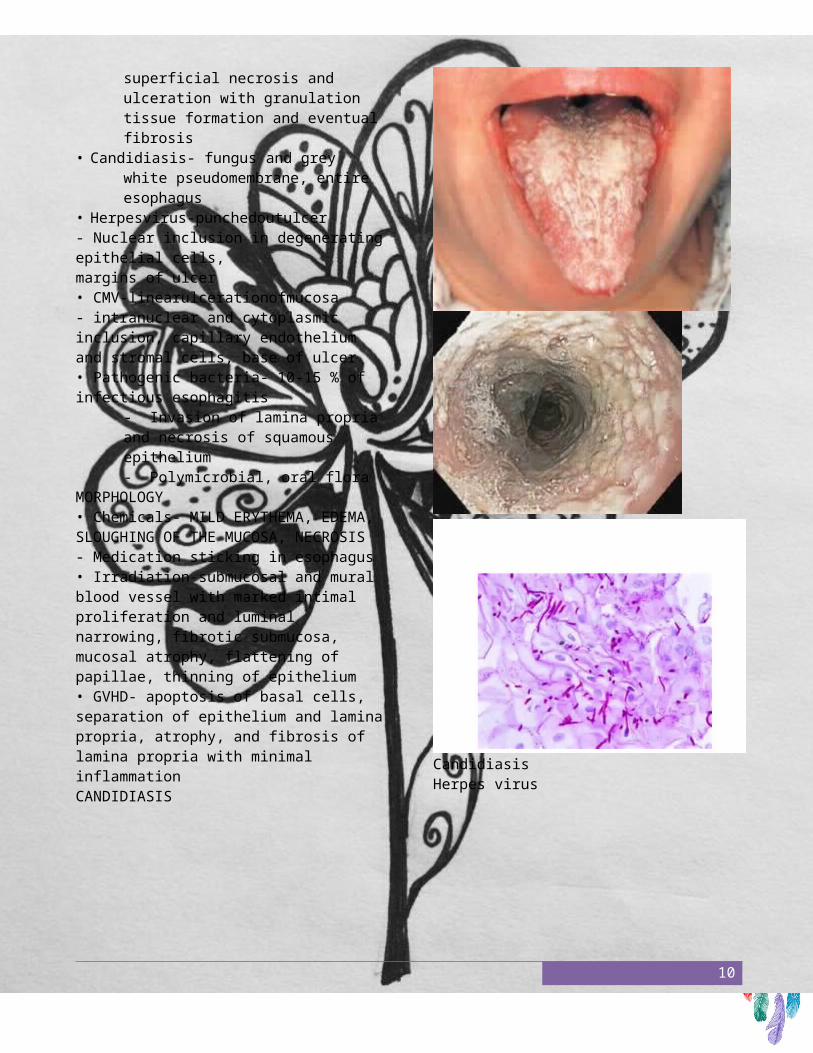
• Candidiasis- fungus and grey white pseudomembrane, entire esophagus
• Herpesvirus-punchedoutulcer - Nuclear inclusion in degenerating epithelial cells, margins of ulcer • CMV-linearulcerationofmucosa - intranuclear and cytoplasmic inclusion, capillary endothelium and stromal cells, base of ulcer • Pathogenic bacteria- 10-15 % of infectious esophagitis
- Invasion of lamina propria and necrosis of squamous epithelium - Polymicrobial, oral flora
MORPHOLOGY • Chemicals- MILD ERYTHEMA, EDEMA, SLOUGHING OF THE MUCOSA, NECROSIS - Medication sticking in esophagus • Irradiation-submucosal and mural blood vessel with marked intimal proliferation and luminal narrowing, fibrotic submucosa, mucosal atrophy, flattening of papillae, thinning of epithelium • GVHD- apoptosis of basal cells, separation of epithelium and lamina propria, atrophy, and fibrosis of lamina propria with minimal inflammation CANDIDIASIS
8

Candidiasis Herpes virus
CMV
9
TUMORS • ADENOCARCINOMA (western) AND SQUAMOUS CELL CARCINOMA (worldwide) ADENOCARCINOMA • arises in the background of BARRET
ESOPHAGUS and long standing GERD
• Increased risk: Documented dysplasia, tobacco use, obesity, prior radiation therapy
• Decreased risk: fruit and vegetable diet
• Distal third, and may invade distal gastric cardia
• Mucin production, gland formation (intestinal type), signet ring cells (gastric cancer like), small poorly differentiated cells (like small cell CA in lung)
• Pain, difficulty in swallowing, progressive weight loss, hematamesis, chest pain, vomiting (already with submucosal lymphatic invasion) • 5 year survival:
- Mucosa and submucosa- 80 % - Deeper or advanced- <25 %
SQUAMOUS CELL CARCINOMA • RISK FACTORS:
- Plummer-Vinson syndrome, alcohol, tobacco use, previous radiation exposure (10 years) - HPV infection (in high risk)
• In middle third of esophagus usually • In situ- then Polypoid exophytic, diffuse
or ulcerative • Lymph node metastasis: - Upper third- cervical - Middlethird-mediastinal,paratracheal, tracheobronchial - Lower third- gastric and celiac • Dysphagia, odynophagia, obstruction • Weight loss, hemorrhage, sepsis
10

STOMACH AZEUS O. SILVA, MD, DPSP (AP-CP) CASE #1 CLINICAL HISTORY: - MALE, 50 Y.O.- Massive hematamesis, epigastric pain, nausea - Alcohol intake, previous- Heavy smoker- Aspirin for Rheumatoid Arthritis • Endoscopy: hyperemic with focal hemorrhage, inflammation with superficial sloughing of gastric mucosa
• Biopsy: neutrophilic infiltrates within epithelium, (+) superficial mucosal erosion (without crossing of the muscularis mucosa), fibrinous exudate in glandular lumen, H. pylori (-), atrophy (-), Intestinal metaplasia (-)
DIAGNOSIS:
• ACUTE GASTRITIS
• ACUTE EROSIVE HEMORRHAGIC GASTRITIS PATHOGENESIS • Considerations: inc acid secretion, dec
bicarbonate buffer production, reduced blood flow, disruption of adherent mucus layer, direct damage to the epithelium
• Mucosal insults: bile acid and lecithin regurgitation from proximal duodenum, inadequate synthesis of prostaglandin
11

ACUTE GASTRIC ULCERATION • focal, acutely developing gastric mucosal defect- NSAID TX COMPLICATION (cyclooxygenase inhibition) TYPES • Stress ulcers- shock, sepsis and severe trauma • Curling ulcers- severe burns and trauma - proximal duodenum* Splanchnic vasoconstriction inc Hcl • Cushing ulcer- intracranial disease (stimulation of vagal nuclei, inc acid secretion) - gastric, duodenal, esophageal - high incidence of perforation
Prostaglandin IMPORTANCE:• Favors production of mucus and bicarbonate• Inhibits acid secretion by parietal cells• Vasodilatory action, PGE and I improves mucosal blood flow Gross
Shallow erosion superficial to deep • Less
than 1 cm in diameter (acute)• Ulcer base- brown to black - extravasated blood (acid digestion) - transmural infiltration- local serositis • Can be found anywhere in stomach • Rugal folds- normal• Non-indurated base and margins• Single or Multiple mostly • Sharply demarcated- normal adjacent mucosa
Microscopy • NECROTIC AREA• INFLAMMATORY CELLS • GRANULATION TISSUE • FIBROSIS * Heals with complete re-epithelialization CASE #2 CLINICAL HISTORY: - FEMALE, 40 Y.O. - NAUSEA, VOMITTING, UPPER ABDOMINAL DISCOMFORT - Normal to inc serum Gastrin level GASTRIN • is a peptide hormone that stimulates secretion of gastric acid (HCl) by the parietal cells ofthe stomach • aids in gastric motility • released by G cells in the antrum of the
stomach, duodenum, and the pancreas.
1.Gastrin binds to cholecystokinin B receptors to stimulate the release of histamines in enterochromaffin-like cells, and it induces the
insertion of K+
/H+
ATPase pumps into the apical membrane of parietal cells (which in turn
increases H+
release into the stomach cavity).
2.Its release is stimulated by peptides in the lumen of the stomach.
• Endoscopy: antral-body-fundic mucosa (Pangastritis), reddened, coarse
12

PANGASTRITIS
Biopsy: lymphocytes and plasma cells in
lamina propria, thin and flattened , Non- invasive H. pylori (+), atrophy (+), Intestinal metaplasia (+), lymphoid aggregates with germinal centers within mucosa, intraepithelial neutrophils and pit abscess, subepithelialplasma cells
Regenerative changes- mitotic figures in gland neck, EC enlargement, hyperchromatic nuclei, high N:C ratio, mucus depletion
Parietal cells are prominent but decreased in number
G cell hyperplasia
13

DIAGNOSIS: - CHRONIC GASTRITIS WITH HELICOBACTER PYLORI INFECTION - CHRONIC ATROPHIC GASTRITIS WITH INTESTINAL METAPLASIA HELICOBACTER PYLORI, PRESENT
NOTE
• Check for dysplasia or neoplasia, WHY? LONG STANDING CHRONIC GASTRITIS Metaplasia Dysplasia In-situ Carcinoma GASTRIC CANCER - associated with autoimmune gastritis and H. pylori assoc. Chronic gastritis
CHRONIC GASTRITIS • less severe but more persistent Nausea and upper abdominal discomfort vomiting (sometimes), hematamesis
(uncommon) Most common cause of CG is infection
(H. pylori) Most common cause of CG without H.
pylori infection- autoimmune gastritis- most common cause of ATROPHIC GASTRITIS
CHRONIC GASTRITIS • Other causes: 1. RADIATION • CHRONIC BILE REFLUX • MECHANICAL INJURY • SYSTEMIC DISEASES- CHRON DISEASE,
AMYLOIDOSIS, GVHD Helicobacter pylori • Non-spore forming curvilinear gram neg rod, 3.5 x 0.5 um Does not invade mucosa, intense inflamm
reaction and immune response. Inc production of proinflamm cytokines (IL-1, TNF -from epith cells, PMN recruitment)
Produces bacterial products that cause epithelial injury and induces inflammation (urease, phospholipase)
Enhances gastric acid secretion Some of its protein are immunogenic (T
and B cells) - causes T cell-driven activation of B-cells- GASTRIC LYMPHOMA
•HUMANS ARETHEONLYKNOWNHOST• ORAL-ORAL, FECAL-ORAL, ENVIRONMENTAL SPREAD H. PYLORI • VIRULENCE: • - FLAGELLA- motility in
mucus • - UREASE- generates
ammonia from endogenous urea, elevates local gastric pH
• - ADHESINS- adherence to foveolar cells
• - TOXINS- cytotoxin-associated gene A (CagA) maybe associated with ulcer and cancer development by poorly defined mechanism.
predominantly antral gastritis with high acid production, despite hypogastrinemia
increased risk of duodenal cancer IMBALANCE IN GASTRODUODENAL
MUCOSAL DEFENSE AND DAMAGING FORCES THAT OVERCOME THOSE DEFENSES
CASE #3 CLINICAL HISTORY: - FEMALE, 45 Y.O.
14

• - NAUSEA, VOMITTING, UPPER ABDOMINAL DISCOMFORT
• - CBC-dec HGB, dec HCT, dec RBC
• - PBS- macrocytic anemia with hypersegmented polymorphonuclear cells
• - inc Gastrin level • - Hyperchlorhydria or
achlorhydria or hypergastrinemia Gross • Diffuse mucosal damage, body and fundus • Thin and rugal fold almost lost• Incomplete mucosal atrophy• Multiple small polyps and nodules
Microscopy - Parietal and chief cells, severe loss or absent- G cell hyperplasia- Enterochromaffin like cell hyperplasia - PERSISTING GLANDS, CYSTIC DILATATION
Diagnosis:
• CHRONIC GASTRITIS
• AUTOIMMUNE TYPE OF CHRONIC GASTRITIS
ASSOCIATIONS
ACID PRODUCTION
Epithelial cells damage
OTHER LESION
MUCOSAL DAMAGE
PEPTIC ULCER
GASTRIC LYMPHOMA
CARCINOID TUMOR (ECL hyperplasia)
ASSOCIATIONS
Pro-inflammatory cytokine production
Epithelial cells damage
Inflam cells
SEROLOGY Characteristics: Reduced pepsinogen I concn. Antral endocrine cell hyperplasia Vit B 12 def Defective gastric acid secretion
(achlorhydria) Autoantibodies- against COMPONENTS
OF GASTRIC GLAND PARIETAL CELLS, ACID PRODUCING ENZYME (H-K-ATPase), GASTRIN RECEPTORS, INTRINSIC FACTOR
15

• Pernicious anemia + autoimmune gastritis- Assoc with hashimoto thyroiditid, Type I DM etc. UNCOMMON FORMS OF GASTRITIS • ALLERGIC GASTROENTEROPATHY- antral, mucosa only, children • LYMPHOCYTIC GASTRITIS- body,
Immune mediated, CD8 cells, mucosa and lamina propria
• GRANULOMATOUS GASTRITIS- antral, intramucosal, CHRON disease, Sarcoidosis, TB, Histoplasmosis, Anisakiasis, foreign body reaction, systemic vasculitis
UNCOMMON FORMS OF GASTRITIS • EOSINOPHILIC- antral and pyloric, all layers of stomach, middle aged women • REACTIVE GASTROPATHY- edema, glandular hyperplasia, regenerative changes, - NSAID, bile reflux • GVHD- lamina propria lymphocytes, bone marrow transpalntation • REACTIVE GASTROPATHY-mucosal histologic changes (foveolar hyperplasia, loss of mucin, glandular regenerative changes etc) without neutrophils PEPTIC ULCER DISEASE • A BREACH IN THE MUCOSA OF THE ALIMENTARY TRACT THAT EXTEND THROUGH THE MUSCULARIS MUCOSA INTO THE SUBMUCOSA OR DEEPER. *Erosion- (-) muscularis mucosa breach• Commonly involves duodenum and stomach • Acute and chronic ulcers
CHRONIC • PEPTIC ULCER- solitary, any portion exposed to acid/peptic juice • Locations: • Duodenum, first portion • Stomach, usually antrum • GE junction in GE reflux or Barrett
disease • Margins of gastrojejunostomy • Duodenum, stomach and/or jejunum-
ZOLLINGER- ELLISON syndrome • Within or adjacent to an ileal Meckel
diverticulum that contain ectopic gastric mucosa
They often appear without any precipitating factor – becomes active – heals spontaneously
Imbalance bet gastroduodenal defense and damaging forces (gastrin and pepsin)
Hyperacidity is not a prerequisite Ulceration occurs: mucosal defense
fails ( dec mucosal blood flow, delayed gastric emptying, impaired epithelial restitution
Tendency to recur due to infection with H. pylori
• Thrombotic occlusion- bacterial platelet activating factor • Damage of cells- leakage of nutrient- sustained bacillus
16

Morphology • 98 % of peptic ulcer are located In the
1st
portion of the duodenum • Wall penetration, adheres to pancreas, omental fat or liver• ACTIVE ULCER- Base and margins, Necrotic fibrinoid
necrosis Non-specific inflammatory infiltrates,
neutrophil predominance Active granulation tissue formation Fibrous scar
• Chronic gastritis is universal among patients with PUD • Always positive for H. pylori• Gastritis remains after ulcer has healed• Recurrence of the ulcer not related to gastritis *in acute erosive gastritis or stress ulcer- adjacent mucosa is generally normal
ACUTE GASTRIC ULCERATION • NSAID medication, stress ulcer • Located mainly in stomach and
occasionally in the duodenum • Ranges from erosion to ulceration • Commonly encountered in shock,
extensive burns, sepsis or severe trauma; in intracranial injury raising intracranial pressure; following intracranial surgery
• Curling ulcer- Proximal duodenum associated with severe burns trauma • Cushing ulcer- gastric, esophageal and duodenal arising in patient with intracranial injury, operation or tumor • Factors are shared with acute gastritis- impaired oxygenation, NSAID medication, decreased prostaglandin
17

• Intracranial injury- direct stimulation of vagal nerve- inc acid• STRESS- splanchnic vasoconstriction(Splanchnic vessels are blood vessels supplying and draining viscera. MORPHOLOGY • Stress ulcers- LESS THAN 1 CM USUALLY• Circular, brown base (extruded acid digested blood)• Margin and base are not indurated• Gastric rugal mucosa is essentially normal• Suffusion of blood and inflammatory reaction maybe noted • No scarring and no thickened blood vessels• healing
• Healing with complete re-epithelialization days to several weeks Complications of PUD • Bleeding• Perforation• Obstruction from edema or scarring *See table Tumors • Benign:1. Polyp- nodule or mass - mucosal polyp- non- neoplastic and neoplastic - gastric polyp are uncommon, but found incidentally in biopsy Non-neoplastic Polyps
• HYPERPLASTIC (90 %) - mixture of hyperplastic foveolar and cystic, inflammatory cells glandular epithelium, seen frequently in chronic gastritis • Adenoma/Adenomatous- proliferative dysplastic epithelium, malignant potential - Sessile (without a stalk) or pedunculated (with stalk) – commonly antral location • Uncommon: fundic gland polyp, Peutz- jeghers polyp, juvenile polyp, hamartomatous polyp, inflammatory fibroid polyp (eosinophilic granuloma) • Check for carcinoma bec. 40 % of gastric adenoma contains focus of carcinoma, specially larger lesions GASTRIC CARCINOMA • MOST COMMON AND MOST IMPORTANT MALIGNANT TUMOR OF THE STOMACH • Lauren classification: • Intestinal type- glandular structures • Diffuse type- poorly diff discohesive
malignant cells FEATURES Intestinal type
Precursor lesion (+)
Morphology Glandular
Incidence 65. y.o./ male
Occurrence (*same now) More common Pathogenesis • H. pylori infection- initially causes chronic gastritis followed by atrophy intestinal metaplasia, dysplasia, carcinoma - Increased genomic mutation and DNA damage • HOST (AUTOIMMUNE GASTRITIS)- WHO HISTOLOGIC CLASSIFICATION OF GASTRIC TUMORS • EPITHELIAL TUMOR- Adenoma,
Adenocarcinoma, Small cell carcinoma
• NON-EPITHELIAL- Leiomyoma , Schwannoma
• MALIGNANT LYMPHOMA • Check on table- • Also FACTORS ASSOCIATED WITH
INCREASED INCIDENCE OF GASTRIC CARCINOMA.
MORPHOLOGY • PYLORUS AND ANTRUM- (50-60%)• Cardia (25 %), body and fundus
18

(remainder)• Lesser curvature antropyloric region- favored site• Greater curvature- less common- most likely malignant • Early lesion-mucosa and submucosa• Advanced lesion- deeper (through muscular wall • Exophytic flat or depressed excavated
• Exophytic linitis plastica excavated • Intestinal type- neoplastic glands resemble colonic adenocarcinoma, cells with apical mucin vacuole and abundant mucin in gland lumen • Diffuse type- no glands, individual cells scattered (variant-signet ring) *if signet ring cells are >50% of the tumor –signet ring cell carcinoma
• Most common site for metastasis-
Virchow (supraclavicular sentinel) nodes
• Metastasis to periumbillical area- subcutaneous nodule (SISTER MARY JOSEPH NODULE)
• Metastasis to one or both ovaries- KRUKENBERG TUMOR
• PROGNOSIS: depends on depth of invasion extent of nodal and distant metastasis
Other Tumors Gastric lymphoma – usually B Cell of
MALT, associated with chronic gastritis and H. pylori
GASTROINTESTINAL STROMAL TUMOR-mesenchymal
• - nerve cells- Schwannoma • - GIST( more common)-
from interstitial cells of Cajal (controls gastrointestinal peristalsis) - c- KIT and CD 34
Gastric Neuroendocrine Cell (Carcinoid) Tumors from Enterochromaffin-like cells (ECL) in the oxyntic mucosa- HYPERGASTRINEMIC STATE
Lipoma- SUBMUCOSA Metastatic carcinoma- systemic
lymphomas - lung and breast CA metastasis mimics LINITIS PLASTICA
__END__
19