esc guidelines 2011 - ijn college — the current evidence on the best practice strategie s to...
TRANSCRIPT

ESC g
uid
elines
2011

ACC/AH
A g
uid
elines
2011

NIC
E g
uid
elines
Marc
h 2
010

MO
H C
PG
2011

NO
N S
T E
LEVATIO
N
MYO
CARD
IAL
INFA
RCTIO
N
Dr.
Akm
al Ars
had
MBChB (
Hons)
Leic
est
er,
MRCP (
UK)
IJN
Card
iolo
gy S
pR

Obje
cti
ves
�The c
urr
ent
evid
ence o
n t
he b
est
pra
cti
ce s
trate
gie
s to
reduce m
orb
idit
y a
nd m
ort
ality
in p
ati
ents
wit
h
UA/N
STEM
I.
�Str
ate
gie
s th
at
are
applicable
to o
ur
local se
ttin
g
consi
deri
ng o
ur
lim
ited h
ealt
hcare
reso
urc
es.

Bre
akdow
n o
f to
pic
s
1.
Epid
em
iolo
gy
2.
Path
ophysi
olo
gy
3.
Dia
gnosi
s
4.
Ris
k s
trati
ficati
on
5.
Managem
ent
6.
Specia
l popula
tions

Applicabilit
y o
f guid
elines
Takin
g into
account
that
our
local healt
h c
are
reso
urc
es
has
all t
he f
ollow
ings
�ECG
machin
es
�M
easu
rem
ent
of
card
iac b
iom
ark
ers
�Tr
eadm
ill st
ress
test
�Echocard
iogra
ms
�M
edic
ati
ons
appro
ved f
or
use
in M
ala
ysi
a
�Id
enti
ficati
on o
f te
rtia
ry c
ente
r ro
le

1.E
pid
em
iolo
gy
�N
ati
onal card
iovasc
ula
r dis
ease
data
base
(N
CVD
)
�In
cid
ence o
f ACS 1
41 p
er
100,0
00 p
opula
tion p
er
year
�In
pati
ent
mort
ality
rate
is
7%




2.P
ath
ophysi
olo
gy

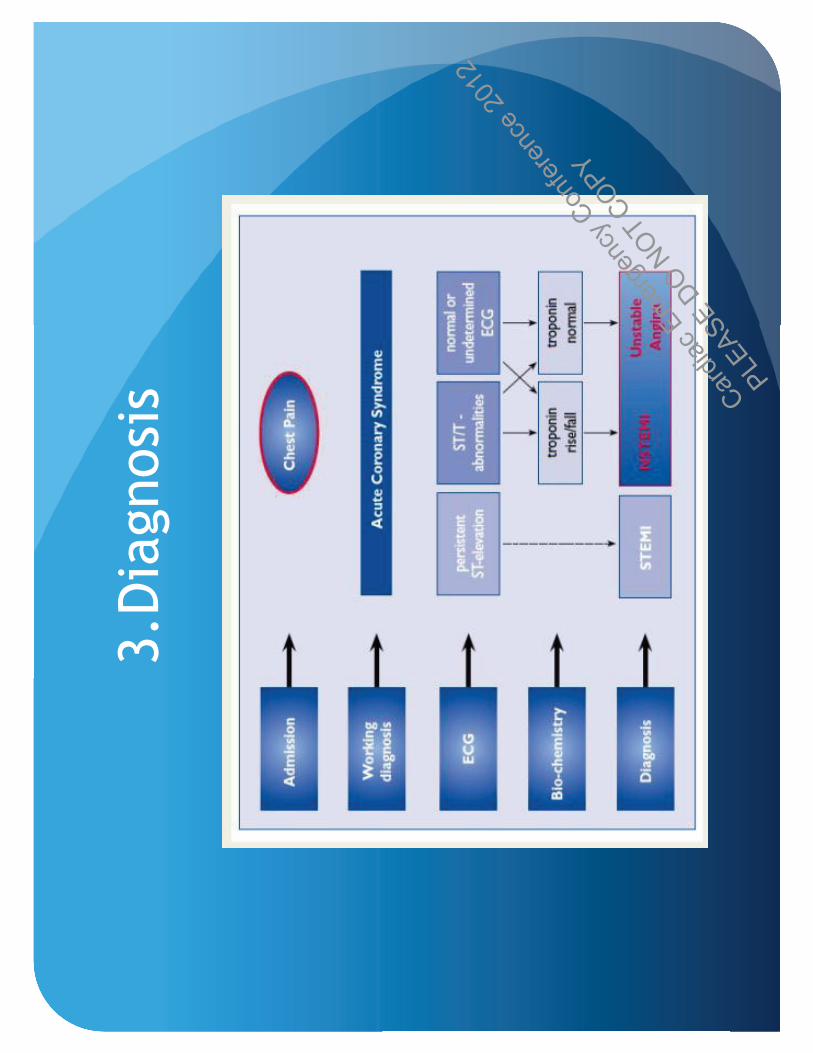
3.D
iagnosi
s

Dia
gnosi
s
�Clinic
al pre
senta
tion
�D
iagnost
ic t
ools
(Physi
cal
exam
inati
on/ECG
/Card
iac
bio
mark
ers
/card
iac im
agin
g)

Clinic
al pre
senta
tions

Physi
cal
exam
inati
ons
�Poss
ible
cause
s
�Pre
cip
itati
ng c
ause
s
�Com
plicati
ons
of
UA/N
STEM
I

Physi
cal
exam
inati
ons

Tria
ge a
ssess
ment

Dia
gnost
ic t
ools

ECG
suggest
ive o
f U
A/N
STEM
I

ECG

ECG

ECG

Card
iac b
iom
ark
ers
�Card
iac t
roponin
s (T
rop T
or
I)
�6 t
o 1
2 h
ours
fro
m t
he o
nse
t of
chest
pain
�Seri
al te
stin
g
�CK/CKM
B

Card
iac b
iom
ark
ers

Card
iac b
iom
ark
ers
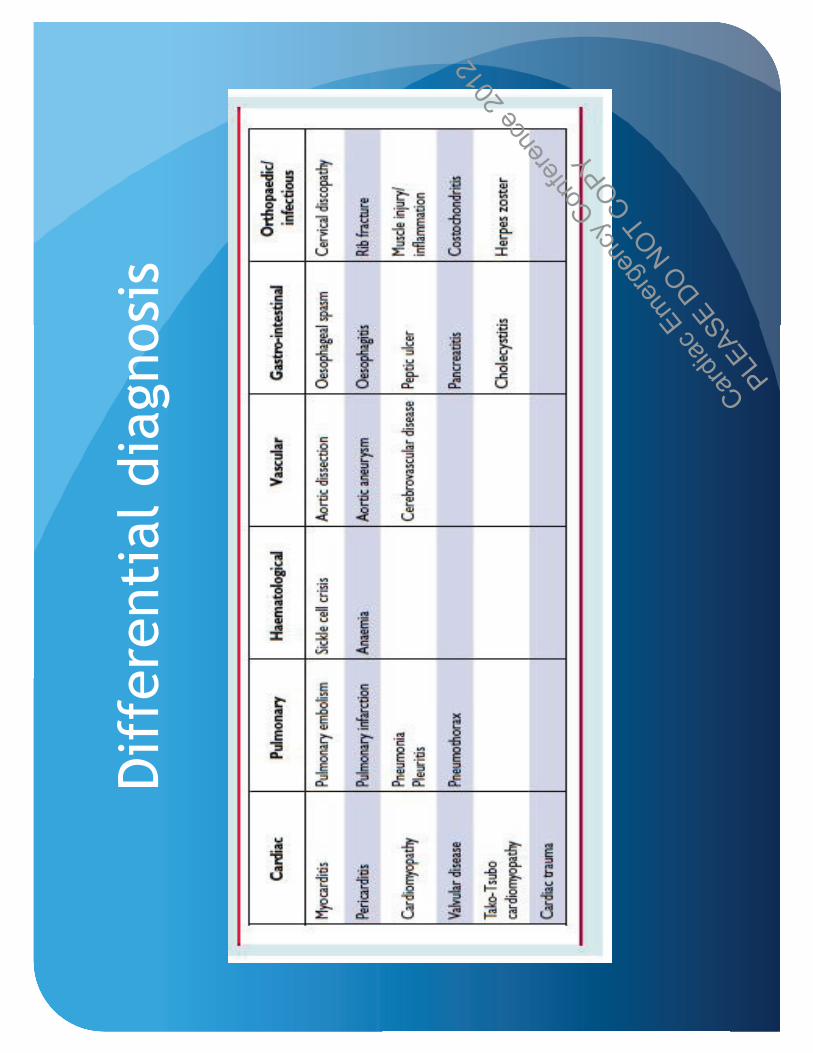
Dif
fere
nti
al dia
gnosi
s

4.
Ris
k s
trati
ficati
on
�Ris
k s
trati
ficati
on
�Lik
elihood o
f advers
e o
utc
om
es
�M
anagem
ent
stra
tegie
s (e
.g s
ite o
f care
)
�U
rgency o
f re
vasc
ula
rizati
on s
trate
gy

TIM
I ri
sk s
core

GRACE r
isk s
core
ww
w.m
dcalc
.com

GRACE r
isk s
core

Ris
k s
trati
ficati
on f
or
NSTEM
I
Low
ris
k
1.
No p
revio
us
angin
a
2.
No o
ngoin
g a
ngin
a
3.
No p
rior
use
of
GTN
4.
Norm
al ECG
5.
Norm
al Tro
ponin
6.
Norm
al LV
functi
on
7.
Younger
age g
roup
Medic
al th
era
py +
outp
ati
ent
ass
ess
ment
Inte
rmedia
te o
r H
igh r
isk
1.
Recurr
ent
chest
pain
2.
Dynam
ic S
T s
egm
ent
changes
3.
Ele
vate
d c
ard
iac b
iom
ark
ers
4.
Dia
bete
s m
ellit
us
5.
Haem
odynam
ically u
nst
able
6.
Depre
ssed L
V f
uncti
on
7.
Majo
r arr
yth
mia
s (V
F/VT)
Medic
al th
era
py +
tra
nsf
er
to c
entr
e
wit
h c
ath
lab f
or
angio
gra
m

5.N
STEM
I M
anagem
ent
goals
�Im
media
te r
elief
of
ongoin
g isc
haem
ia a
nd a
ngin
a
�Pre
venti
on o
f re
curr
ent
ischaem
ia a
nd a
ngin
a
�Pre
venti
on o
f se
rious
advers
e e
vents

ESC A
CS M
anagem
ent
chart

Alg
ori
thm
for
troponin
test

Init
ial
thera
peuti
c m
easu
res

Checklist
of
treatm
ents

Ora
l anti
pla
tlets
Loadin
g d
ose
M
ain
tenance d
ose
R
ecom
mendati
on
Asp
irin
300m
g s
tat
Asp
irin
75-1
50m
g O
D
(I,A
)

P2Y
12 In
hib
itor
Medic
ati
on
Dosa
ge
Recom
mendati
on
CLO
PID
OG
REL
Loadin
g d
ose
of
300 t
o
600m
g,
Main
tenance
dose
- 75m
g O
D
(I,A
)
TIC
LO
PID
INE
250m
g B
D
(II-
a,
B)
TIC
AG
RELO
R
Loadin
g d
ose
180m
g,
Main
tenance d
ose
-
90m
g B
D
(I,B
)
PRASU
GREL
Loadin
g d
ose
of
60m
g,
main
tenance d
ose
of
10m
g O
D
(I,B
)

Activate
d p
late
lets
are
centr
al to
thro
mbus
form
ation in A
CS
Pla
qu
e r
up
ture
lead
s t
o p
late
let
ad
hesio
n t
o t
he
exp
osed
su
ben
do
theli
um
Acti
va
ted
pla
tele
ts l
ead
to
th
rom
bu
s
form
ati
on
Acti
va
ted
pla
tele
ts a
gg
reg
ate
co
veri
ng
th
e t
hro
mb
us
su
rface
[Ad
ap
ted
fro
m
Dav
ies 2
000:
A]
2
1
3
Vo
rch
heim
er
DA
, et
al. M
ayo
Clin
Pro
c. 2006;8
1:5
9-6
8;
Dav
ies M
J. H
eart
. 2000;8
3:3
61-3
66.

Targ
et
for
pla
tele
t in
hib
itio
n

Gene
tic p
oly
morp
his
ms m
ay c
ontr
ibute
to
clo
pid
og
rel re
sp
on
se
vari
abili
ty

Adapte
d f
rom
Schom
ig A
. N
Engl J M
ed
. 2009;3
61:1
108–
11
11.
Tic
agre
lor:
Does
NO
T r
equir
e
meta
bolic a
cti
vati
on t
o
becom
e a
cti
ve d
rug
Clo
pid
ogre
l:
A p
rodru
g;
requir
es
meta
bolism
to
becom
e a
cti
ve d
rug
CY
P-d
ep
en
den
t
oxid
ati
on
CY
P1A
2
CY
P2B
6
CY
P2C
19
CY
P-d
ep
en
den
t
oxid
ati
on
CY
P2C
19
CY
P3A
4/5
CY
P2B
6
Acti
ve c
om
po
un
d
Inte
rmed
iate
meta
bo
lite
Pro
dru
g
Tic
ag
relo
r
Clo
pid
og
rel
Bin
din
g
P2Y
12
Tic
agre
lor:
Does N
ot
Require H
epatic
Meta
bolis
m for A
ctivation
Pla
tele
t

PL
AT
O:
Prim
ary
Effic
acy E
ndp
oin
t
(Com
po
site o
f C
V D
eath
, M
I, o
r S
troke)

Intr
avenous
anti
pla
tlet
thera
py
�Abcix
imab
�Tir
ofi
ban
�Epti
fibati
de
�These
agents
may b
e u
sed in h
igh r
isk p
ati
ents
aw
ait
ing
transf
er
to a
PCI fa
cilit
y f
or
an e
arl
y invasi
ve s
trate
gy.

Anti
coagula
nt
thera
py
�U
nfr
acti
oned h
epari
n (
I,A)
�Low
mole
cula
r w
eig
ht
hepari
n (
I,A)
�Anti
Xa inhib
itor-
Fondapari
nux (
I,A)
�Anti
IIa
inhib
itors
- Biv
aliru
din
(I,
A)

Dosi
ng R
egim
en
Agent
NST
EM
I D
uri
ng P
CI
UFH
In
itia
l IV
bolu
s 60
IU/kg (
max 4
000 IU
)
follow
ed b
y infu
sion
to m
ain
tain
APTT 1
.5-
2.0
Em
pir
ical lo
adin
g d
ose
of
5000-1
0,0
00 i
u
EN
OXAPA
RIN
In
itia
l 30m
g IV b
olu
s,
then 1
5 m
inute
s la
ter -
s/c 1
.0 m
g/kg e
very
12 h
ours
(<75 y
ears
)
0.5
-0.7
5m
g/kg IV
bolu
s (n
o p
rior
use
)
FO
ND
APA
RIN
UX
2.5
mg s
/c O
D
Addit
ional 50-6
0 IU
/kg
of
UFH

Anti
isc
haem
ic d
rug t
hera
py
�N
itra
tes-
Consi
der
IV w
hen t
here
is
nor
relief
of
sym
pto
ms
wit
h S
/L
GTN
, D
ynam
ic E
CG
changes,
LV
failure
and h
igh b
lood p
ress
ure
�Beta
blo
ckers
- sh
ould
be a
dm
inis
tere
d e
arl
y
�Calc
ium
channel blo
ckers
- conti
nuin
g a
ngin
a d
esp
ite
bein
g o
n n
itra
tes
and b
eta
blo
ckers
. Printzmetal’s
angin
a

Dosi
ng r
egim
e f
or
Nit
rate
s
Com
pound
Route
D
osa
ge
GTN
Sublingual
0.3
-0.6
Mg (
3-5
min
ute
s)
IV
5-2
00 m
icro
gra
m/m
in
ISO
SO
RBID
E D
INIT
RATE
IV
2-1
2 m
g/hour
ora
l 10-2
0m
g t
ds
ISO
SO
RBID
E
MO
NO
NIT
RATE
ora
l 30-6
0m
g o
d

Dosi
ng r
egim
e f
or
beta
blo
ckers
Type
Init
iati
on d
ose
Targ
et
dose
METO
PRO
LO
L
25 M
G B
D
100M
G B
D
BIS
OPRO
LO
L
1.2
5 M
G O
D
10M
G O
D
CARVED
ILO
L
3.1
25 M
G B
D
25M
G B
D

Dosi
ng r
egim
e f
or
calc
ium
channel blo
ckers
Dru
g
Dose
Dilti
azem
30-9
0m
g t
ds
Vera
pam
il
40-8
0m
g t
ds
Am
lodip
ine
2.5
-10m
g
Nif
edip
ine
SR 3
0-9
0 m
g o
d

Oth
ers
�Lip
id m
odif
yin
g d
rugs
�ACEi/
ARB

6.
Specia
l popula
tion
�N
STEM
I in
wom
en
�N
STEM
I in
Chro
nic
kid
ney d
isease
pati
ents
�N
STEM
I in
the e
lderl
y

NSTEM
I in
Wom
en

0.0
%
5.0
%
10.0
%
15.0
%
20.0
%
25.0
%
30.0
%
1999
2000
2001
2002
2003
2004
2005
2006
CV
Dis
eas
eA
ll C
an
ce
rs
Death
am
ong w
om
en d
ue t
o C
ard
iovasc
ula
r D
isease
*
and a
ll C
ancers
Com
bin
ed *
in M
ala
ysi
a**
(1999 –
2005)
CV
Dis
ease
26.8
%
27.5
%
26.7
%
25.9
%
26.4
%
25.9
%
25.4
%
26.1
%
All
Can
cers
10.1
%
10.5
%
10.6
%
10.9
%
11.4
%
11.3
%
11.8
%
11.9
%
Ab
ou
t 2
5%
of
fem
ale
de
ath
s in
gove
rn
me
nt
ho
sp
ita
ls
(a
bo
ut
1 in
4)
is d
ue
to
CV
D
W
om
en’s
He
art H
ealt
h A
wa
re
ne
ss
Pro
gra
m I
n M
ala
ysia

NSTEM
I in
wom
en
�Aty
pic
al pre
senta
tion
�Pra
sugre
l is
ass
ocia
ted w
ith m
ore
ble
edin
g in w
om
en
who w
eig
h less
than 6
0kg (
I,B)
�M
eta
analy
sis
indic
ate
s a lack o
f benefi
t of
GPIIb/IIIa
inhib
itors
in w
om
en.
The b
leedin
g r
isk is
hig
her
(I,B
)

NSTEM
I in
Chro
nic
kid
ney d
isease
�In
cre
ase
d r
isk o
f ble
edin
g.
Fondapari
nux s
eem
to b
e
ass
ocia
ted w
ith less
ble
edin
g t
hat
hepari
n/enoxapari
n
(I,B
)
�M
eta
analy
sis
show
ed t
hat
pati
ent
wit
h C
KD
- earl
y
invasi
ve s
trate
gy h
ad b
ett
er
outc
om
es.
(IIa,B
)
Loadin
g d
ose
M
ain
tenance d
ose
UFH
N
o c
hange
No c
hange
Enoxapari
n
30m
g IV
1m
g/kg s
/c e
very
24
hours
if
CrC
l
<30m
l/m
in
Fondapari
nux
Avoid
if
CrC
l
<30m
l/m
in
Avoid
if
CrC
l
<30m
l/m
in

NSTEM
I in
dia
bete
s
�D
iabeti
cs
should
be t
reate
d a
ggre
ssiv
ely
�Pra
sugre
l fo
und t
o b
e m
ore
eff
ecti
ve in d
iabeti
cs
(I,B
)
�Earl
y invasi
ve a
ppro
ach (
I,A)

NSTEM
I in
the e
lderl
y
�Aty
pic
al pre
senta
tion
�Pra
sugre
l sh
ould
be a
void
ed in p
ati
ents
old
er
than 7
5
years
old
(I,
B)
�Eld
erl
y h
ave m
ore
ble
edin
g c
om
plicati
ons

Sum
mary
�The d
iagnosi
s of
UA/N
STEM
I is
base
d o
n h
isto
ry +
/-
dynam
ic
ECG
changes
(Wit
hout
pers
iste
nt
ST e
levati
on)
+/-
rais
ed
card
iac b
iom
ark
ers
�Ris
k s
trati
ficati
on is
import
ant
for
pro
gnosi
s and t
o g
uid
e
managem
ent
�In
itia
l m
anagem
ent
should
inclu
de o
xygen,
asp
irin
, clo
pid
ogre
l or
ticagre
lor,
UFH
or
LM
WH
or
Fonda.
�In
term
edia
te o
r hig
h r
isk p
ati
ent
should
be c
onsi
dere
d f
or
transf
er
to c
ard
iac c
entr
e w
ith a
ngio
gra
phy f
acilit
y.
�O
pti
miz
ati
on o
f anti
angin
al su
ch a
s nit
rate
s, b
eta
blo
ckers
, calc
ium
channel blo
ckers
.
�Consi
dera
tion in s
pecia
l popula
tions

Thank y
ou
Dr.
akm
al@
ijn.c
om
.my
htt
p:/
/w
ww
.facebook.c
om
/re
sist
anth
ypert
ensi
on