ergonomic analysis of surgeries with the use of … analysis of surgeries with the use of wireless...
TRANSCRIPT

361
ERGONOMIC ANALYSIS OF SURGERIES WITH THE USE OF WIRELESS BODY POSTURES MEASUREMENT SYSTEM
Joanna BARTNICKA, Agnieszka ZIĘTKIEWICZ, Grzegorz KOWALSKI Abstract: The aim of the study was the recognition of the possibilities of conducting cross-sectional ergonomic analysis in a uniform programming environment. Particularly the data about body postures were included in the ergonomic analysis which were gathered from wireless body postures measurement system. There was developed the special procedure for doing research with the use of body postures measurement system which can be implemented for such difficult working conditions like conditions in operation room while laparoscopic surgeries. The studies were executed with CAPTIV system for both capturing body positions and cross-sectional analysis. An example of how to support the ergonomic assessment of surgeon tasks was presented, particularly focusing on motion safety zonas for wrists. Key words: ergonomics, cross-sectional analysis, ergonomic data visualisation, laparoscopic surgery, body postures, wireless sensors. 1. Introduction
Conducting ergonomic analysis is an essential factor in the process of improving working conditions and reducing health hazards for workers. There are different approaches to carrying out research in the field of ergonomics, but most of known and effective of them are based on observation of workers while doing their work. The examples of observational methods are inter alia OWAS [1], RULA [2] and REBA [3]. These methods are based on the coding of the body segments position as well as external load and attribution of indicated codes for a particular category of workload. According to certain categories the occupational risk and requirements for improving the way of doing work tasks are determined.
The body position is defined in different ways and with different degree of specificity, depends on the type of method. The most common methods are here: an online observation of worker with simultaneous description of certain body posture codes or video recording of a worker and then description of codes. The great advantage of these methods is the possibility of conducting analysis based on real working environment. Unfortunately such processing is impossible or very difficult in some cases due to the specificity of work factors. To these specific factors can be included: a limited space for examination as well as access to tested objects or the specific environmental material conditions.
However, the authors have attempted to develop a methodology for ergonomic analysis which integrates three quite problematic and mentioned above elements:
1. Specific and difficult, from the point of view of research, environment; 2. Video recording of work processes; 3. Online observation and data acquisition of body postures measurements. This methodology aims at giving opportunity to do comprehensive and cross-sectional
ergonomic analysis based on real needs of workers who perform their tasks in difficult
362
working conditions. A representative of such problematic conditions is operating room. Particularly, in the article the experiences of performing research in ergonomics of laparoscopic surgeries with the use of observational method and wireless body postures capturing system are described.
Laparoscopic procedures belong to minimally invasive surgeries and are currently used in all areas of general surgery [4]. The idea of laparoscopic procedure was developed in the beginning of XX century. Fischer, Reddick and Olsen have published research, in which they compared the outcomes of laparoscopic cholecystectomy surgery with the outcomes of classical surgery. The research clearly indicated than laparoscopic method is more safety and cheaper, and its using is associated with less postoperative pain, shorter hospital stay and shorter incapacity for work [5].
A working environment of laparoscopic surgeons is chosen due to the high degree of complexity of the man-machine functioning in specific working conditions represented by:
deployment of extended medical devices with auxiliary equipment, such as cables, pipes, which reduce the effective working area [6],
construction of surgical instruments and medical devices that determines the specific, often awkward surgeons’ postures while performing by them surgical procedures,
changes in a way of doing works from the dynamic, characterized by the free maneuvers of the surgeon, to the static with restricted mobility.
The final purpose of research, where this article is a part of it, is to develop an integrated ergonomic tool which enables:
recognition of health hazards for certain segments of musculoskeletal system, a direct connection of specific risks factors with the activities performed by the
surgeon during a procedure, identification of the differences and commonalities in terms of risks factors
depending on the type of surgical procedure and creation of health hazards map for surgeons,
identification of dependencies and relationships between the various factors shaping the working conditions.
2. Material and methods
The research material is based on 33 laparoscopic procedures which have been recorded
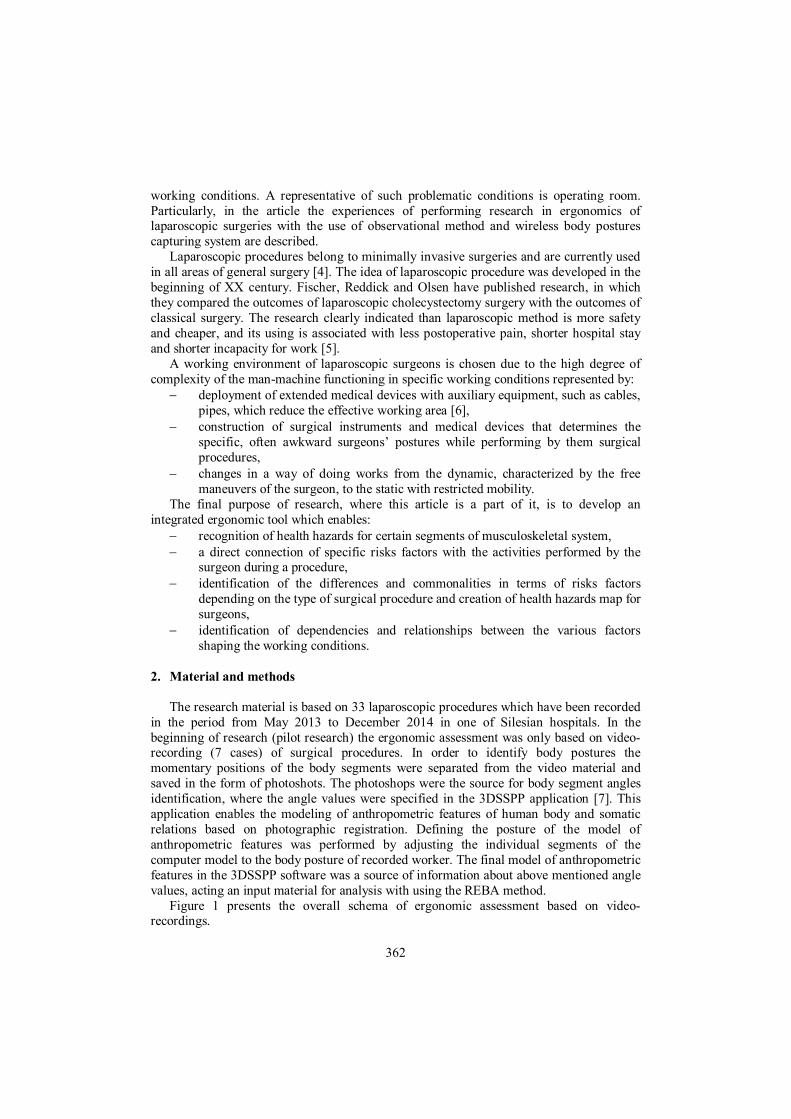
in the period from May 2013 to December 2014 in one of Silesian hospitals. In the beginning of research (pilot research) the ergonomic assessment was only based on video-recording (7 cases) of surgical procedures. In order to identify body postures the momentary positions of the body segments were separated from the video material and saved in the form of photoshots. The photoshops were the source for body segment angles identification, where the angle values were specified in the 3DSSPP application [7]. This application enables the modeling of anthropometric features of human body and somatic relations based on photographic registration. Defining the posture of the model of anthropometric features was performed by adjusting the individual segments of the computer model to the body posture of recorded worker. The final model of anthropometric features in the 3DSSPP software was a source of information about above mentioned angle values, acting an input material for analysis with using the REBA method.
Figure 1 presents the overall schema of ergonomic assessment based on video-recordings.
363
3D
SSP
PRE
BA
Figure 1. The overall schema of ergonomic assessment based
on video-recordings (own elaboration)
However, while research there were identified several limitations associated with video recording of surgeons’ operations during surgery and hence with ergonomic assessment:
a camera operator can move only in the "dirty" zone, the recommended at least two directions of video recording (front and side) of
surgeon’s operations may not be able to meet because of the barriers in the form of equipment and people involved in the surgery,
the initial location of the camera operator (or operators) may vary due to the dynamics of the surgical procedure, such as changing the surgeon’s position or location of the surgical team members,
the separation of certain snapshots was difficult and time-consuming because there

364
were no additional supporting tools for that but it was based on visual studying video recordings frame by frame,
the identification of body segment angles was estimated in 3DSSPP application with the possibility of measurement errors because of two reasons: (1) it is not possible to record surgeon in front and side directions while real surgery; (2) it is not possible to record the entire body of surgeon due to such barriers like handled surgical instruments, other medical equipment as well as the other members of the surgical team.
The outcomes of the pilot research encouraged the authors to look for a new way of body posture identification and ergonomic assessment. The criteria for new solution were:
remote body posture data acquisition which allows worker to behave in a naturalistic manner and with unrestrained freedom of motion;
more automatic manner of assessing working conditions; including into ergonomic analysis a set of various factors shaping working
conditions while taking into account the relations and dependencies between them; the possibility of synchronous and comprehensive ergonomic analysis i.e. in which
the various factors creating working conditions are tested at the same intervals and in respect to a video recordings of operations performed by the surgeons;
carrying out various ergonomic tests in common software environment. Based on the above specification a computer system CAPTIV [8] was chosen for
supporting the study on integrated ergonomic assessment. CAPTIV system includes both hardware part which is wireless system for angular measurement of body positions and software part which is application for acquisition of quantitative and qualitative data, synchronization and video analysis.
The system for angular measurement is divided into following accessories: goniometer sensor for measuring flexion/extension and abduction/adduction; torsiometer sensor for measuring torsion; datalogger - a station for data acquisition. Table 1 presents the most important parameters of the indicated elements.
Table 1. Specification of angular measurement system (own elaboration)
Photo Description Goniometer
Measuring range: +/- 180° Frequency: 32Hz /channel Accuracy 2° Power supply: Li-Ion battery - 190mAh Battery life: 4hrs Recharging time: 3hrs Dimensions 52mm x 25mm x 14mm Wire length: 80mm Weight 20g Temperature: 0°C to 40°C Humidity < 60%
Torsiometer
365
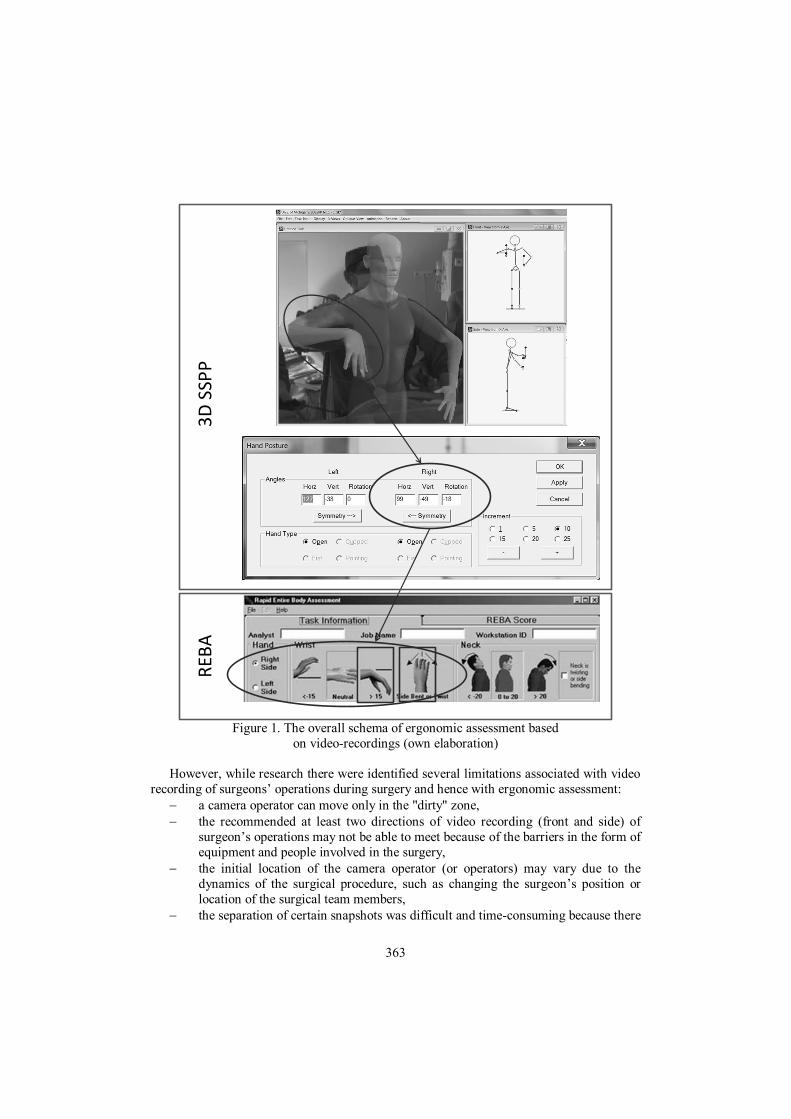
Datalogger
Memory: SD-SDHC-MMC Resolution: Up to 16 bits Screen: 2,8”, Tactile Communication with PC: USB 2.0 port Sampling rate: 16Hz to 2048Hz Bandwidth: 2048Hz Number of sensors: 1-12 Range: 6m Battery life: 12hrs Recharging time: 4hrs Dimensions: 117x73x23mm Weight: 170g
The way of affixing the sensors is presented in the Figure 2, where particularly the
Figure 2a shows the neutral and calibration position, Figure 2b position with flexion position of the wrist and Figure 2c position with extension position of the wrist.
a)
b)
c) Figure 2. The manner of affixing the measuring sensors with the sample positions of the
wrist a) neutral, b) flexion, c) extension (own elaboration)
The empirical studies with the use of CAPTIV system was divided into two parts: 1. Pilot study, where the procedure of using CAPTIV system was developed and
verify in lab conditions; 2. Main study performing while real surgeries.
366
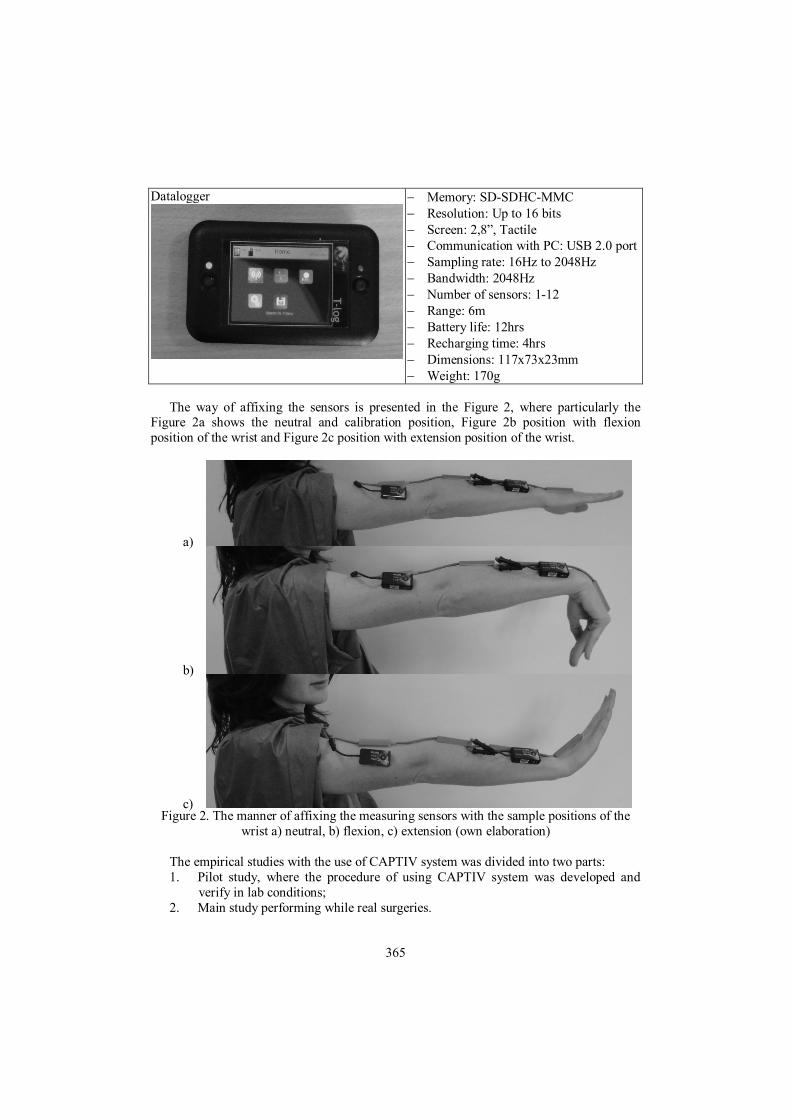
In particular the pilot study was performed in a form of surgery simulation with the use of the dummy representing a patient. Two kinds of surgical procedure were simulated: cholecystectomy and bariatric surgery. In the Figure 3 there is presented the surgeon with the affixed sensors simulated operational activities of bariatric procedure.
Figure 3. Simulation of bariatric surgery (own elaboration)
The analysis of simulated surgeries has allowed developing the procedure for using
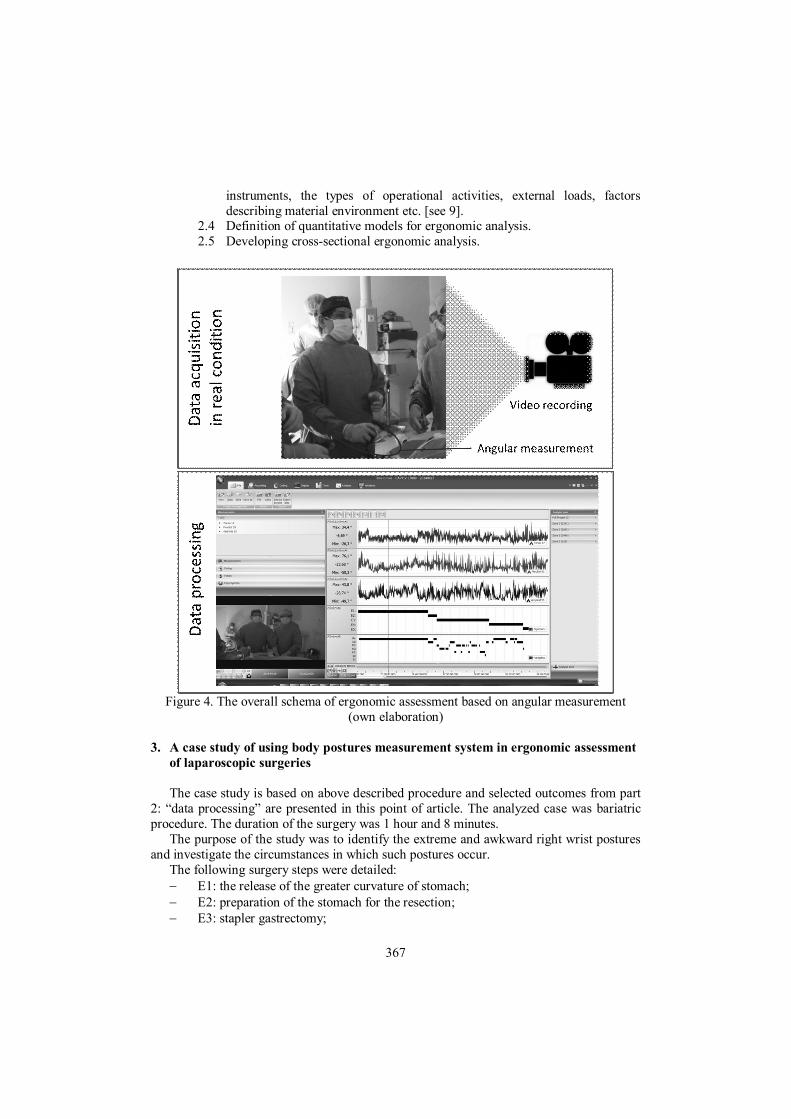
CAPTIV system in ergonomic assessment taking into account surgeon work conditions. The procedure includes two basic parts [Figure 4]:
1. Data acquisition which enrolls all actions performed in real conditions and with the use of angular measurement and video system: 1.1 Preparation of video cameras and measuring system including time
synchronization of all devices: cameras and datalogger. 1.2 Installation of the measuring sensors on the certain surgeon’s body. 1.3 Starting and verification of the correctness of the measuring sensors and
cameras. 1.4 Sensors calibration and synchronization with the cameras. 1.5 Angular measurement and video recording of surgeon while laparoscopic
procedure. 2. Data processing:
2.1 Implementation of video material and measuring data to CAPTIV software. 2.2 Synchronization of video material and measurement data in CAPTIV
software. 2.3 Definition of codes for all of the attributes describing working conditions
which are be used in ergonomic assessment, e.g. the types of surgical
367
instruments, the types of operational activities, external loads, factors describing material environment etc. [see 9].
2.4 Definition of quantitative models for ergonomic analysis. 2.5 Developing cross-sectional ergonomic analysis.
Figure 4. The overall schema of ergonomic assessment based on angular measurement
(own elaboration) 3. A case study of using body postures measurement system in ergonomic assessment
of laparoscopic surgeries
The case study is based on above described procedure and selected outcomes from part 2: “data processing” are presented in this point of article. The analyzed case was bariatric procedure. The duration of the surgery was 1 hour and 8 minutes.
The purpose of the study was to identify the extreme and awkward right wrist postures and investigate the circumstances in which such postures occur.
The following surgery steps were detailed: E1: the release of the greater curvature of stomach; E2: preparation of the stomach for the resection; E3: stapler gastrectomy;
368
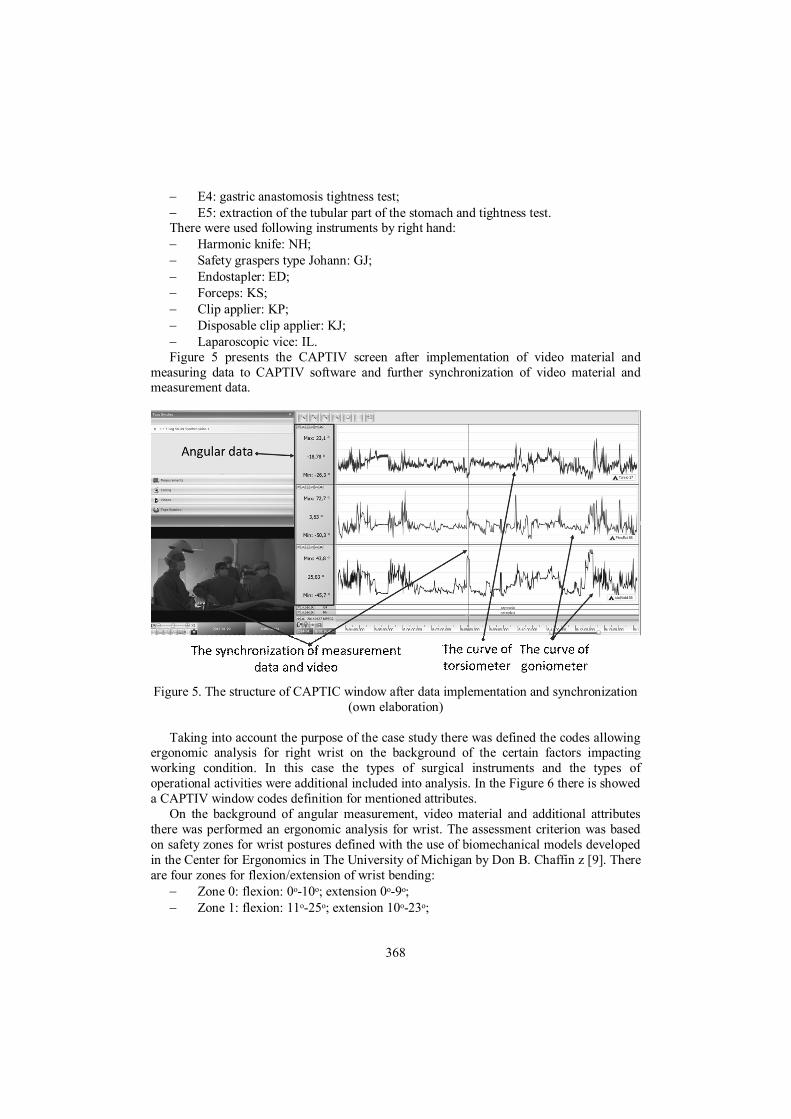
E4: gastric anastomosis tightness test; E5: extraction of the tubular part of the stomach and tightness test. There were used following instruments by right hand: Harmonic knife: NH; Safety graspers type Johann: GJ; Endostapler: ED; Forceps: KS; Clip applier: KP; Disposable clip applier: KJ; Laparoscopic vice: IL. Figure 5 presents the CAPTIV screen after implementation of video material and
measuring data to CAPTIV software and further synchronization of video material and measurement data.
Figure 5. The structure of CAPTIC window after data implementation and synchronization
(own elaboration) Taking into account the purpose of the case study there was defined the codes allowing
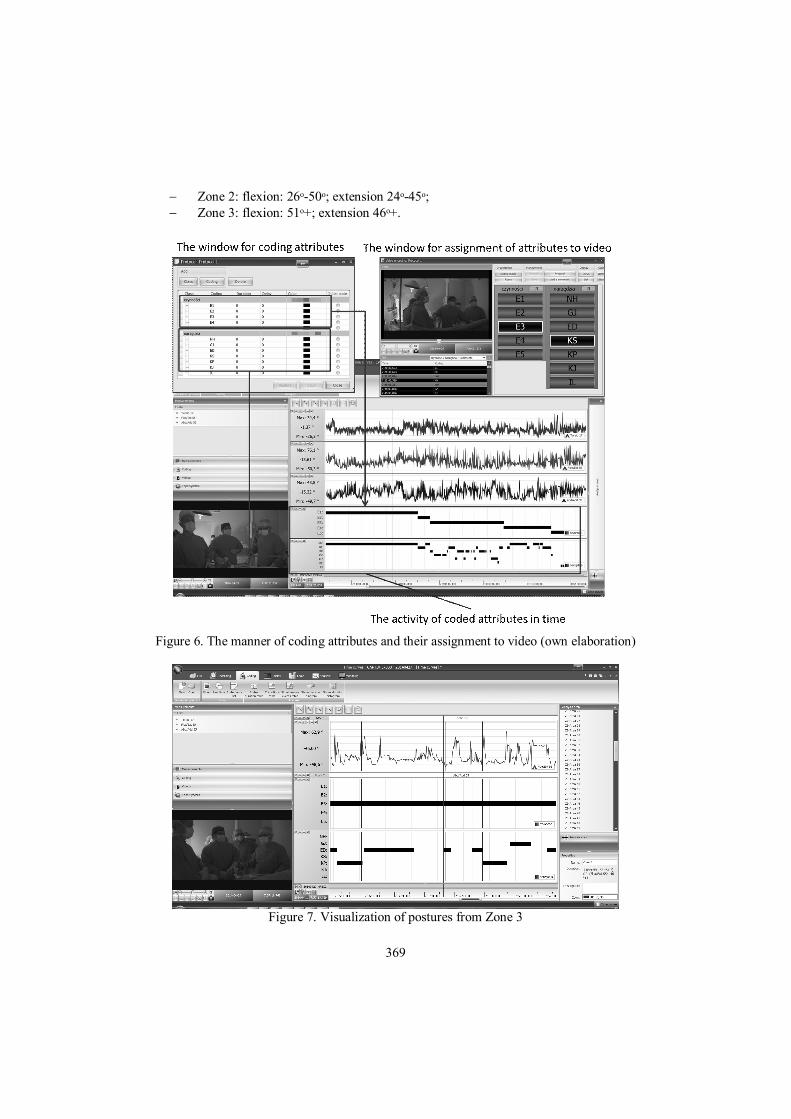
ergonomic analysis for right wrist on the background of the certain factors impacting working condition. In this case the types of surgical instruments and the types of operational activities were additional included into analysis. In the Figure 6 there is showed a CAPTIV window codes definition for mentioned attributes.
On the background of angular measurement, video material and additional attributes there was performed an ergonomic analysis for wrist. The assessment criterion was based on safety zones for wrist postures defined with the use of biomechanical models developed in the Center for Ergonomics in The University of Michigan by Don B. Chaffin z [9]. There are four zones for flexion/extension of wrist bending:
Zone 0: flexion: 0ᵒ-10ᵒ; extension 0ᵒ-9ᵒ; Zone 1: flexion: 11ᵒ-25ᵒ; extension 10ᵒ-23ᵒ;
369
Zone 2: flexion: 26ᵒ-50ᵒ; extension 24ᵒ-45ᵒ; Zone 3: flexion: 51ᵒ+; extension 46ᵒ+.
Figure 6. The manner of coding attributes and their assignment to video (own elaboration)
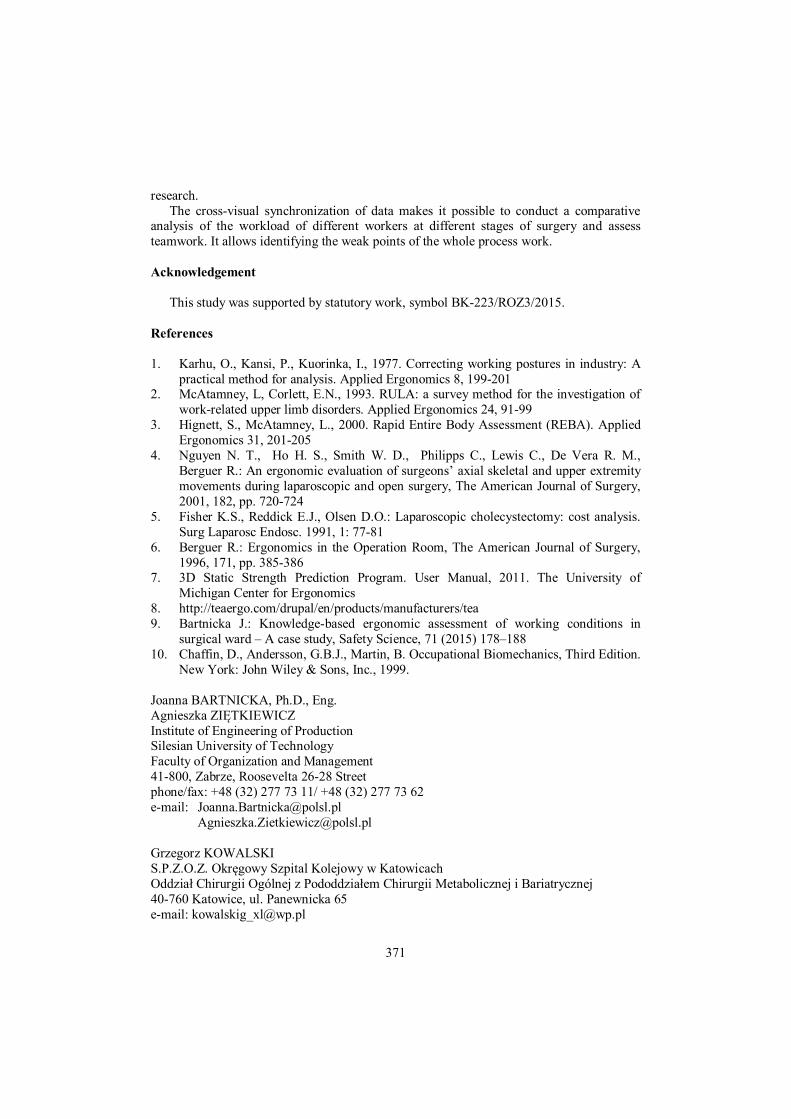
Figure 7. Visualization of postures from Zone 3

370
Zone 0 and Zone 1 are preferred for most movements, while Zones 2 and 3 should be avoided. Particularly the movements including into Zone 3 indicate extremely postures for muscles and joints which can cause musculoskeletal disorder. All movement in Zones was found according to defined equations, where in Zone 0 there is 2231 postures, Zone 1 is 2091 postures and Zone 3 is 126 postures. In the figure 7 there is presented a map of surgery course with a visualization of all postures from Zone 3 in the form of black vertical lines.
According to visualization of different kind of data in one place there is possible to do cross-sectional ergonomic analysis looking for relationships between them. For example, despite the fact that harmonic knife NH was the most often used during surgery (57,88% of surgery time, see Figure 8), the extreme positions from Zone 3 were mostly noted during the another tool endostapler ED (used only in 10,1% of surgery time).
Figure 8. The percent of time duration of surgery steps and surgical tools
The numbers of extreme positions with the division of surgical tools are as follows: Harmonic knife NH: 30 Safety graspers type Johann GJ: 13 Endostapler ED: 52 Forceps KS: 2 Clip applier KP: 0 Disposable clip applier KJ: 0 Laparoscopic vice IL: 16. This above described quite simple research procedure shows that it is possible to obtain
practical information in the process of improving working condition, in this particular case concerning the process of surgical tools designing with respect of ergonomic factors.
4. Conclusion
The cross-sectional analysis including various elements of ergonomic assessment and factors creating working conditions can provide new knowledge in the area of organization and ergonomics, which would be difficult to identify in the case of doing particular
371
research. The cross-visual synchronization of data makes it possible to conduct a comparative
analysis of the workload of different workers at different stages of surgery and assess teamwork. It allows identifying the weak points of the whole process work.
Acknowledgement
This study was supported by statutory work, symbol BK-223/ROZ3/2015.
References 1. Karhu, O., Kansi, P., Kuorinka, I., 1977. Correcting working postures in industry: A
practical method for analysis. Applied Ergonomics 8, 199-201 2. McAtamney, L, Corlett, E.N., 1993. RULA: a survey method for the investigation of
work-related upper limb disorders. Applied Ergonomics 24, 91-99 3. Hignett, S., McAtamney, L., 2000. Rapid Entire Body Assessment (REBA). Applied
Ergonomics 31, 201-205 4. Nguyen N. T., Ho H. S., Smith W. D., Philipps C., Lewis C., De Vera R. M.,
Berguer R.: An ergonomic evaluation of surgeons’ axial skeletal and upper extremity movements during laparoscopic and open surgery, The American Journal of Surgery, 2001, 182, pp. 720-724
5. Fisher K.S., Reddick E.J., Olsen D.O.: Laparoscopic cholecystectomy: cost analysis. Surg Laparosc Endosc. 1991, 1: 77-81
6. Berguer R.: Ergonomics in the Operation Room, The American Journal of Surgery, 1996, 171, pp. 385-386
7. 3D Static Strength Prediction Program. User Manual, 2011. The University of Michigan Center for Ergonomics
8. http://teaergo.com/drupal/en/products/manufacturers/tea 9. Bartnicka J.: Knowledge-based ergonomic assessment of working conditions in
surgical ward – A case study, Safety Science, 71 (2015) 178–188 10. Chaffin, D., Andersson, G.B.J., Martin, B. Occupational Biomechanics, Third Edition.
New York: John Wiley & Sons, Inc., 1999. Joanna BARTNICKA, Ph.D., Eng. Agnieszka ZIĘTKIEWICZ Institute of Engineering of Production Silesian University of Technology Faculty of Organization and Management 41-800, Zabrze, Roosevelta 26-28 Street phone/fax: +48 (32) 277 73 11/ +48 (32) 277 73 62 e-mail: [email protected] [email protected] Grzegorz KOWALSKI S.P.Z.O.Z. Okręgowy Szpital Kolejowy w Katowicach Oddział Chirurgii Ogólnej z Pododdziałem Chirurgii Metabolicznej i Bariatrycznej 40-760 Katowice, ul. Panewnicka 65 e-mail: [email protected]