equine chiropractic: general principles and clinical ... · kevin k. haussler, dvm, ... tered...
TRANSCRIPT
Equine Chiropractic: General Principles andClinical Applications
Kevin K. Haussler, DVM, DC, PhD
Chiropractic techniques provide additional diagnostic and therapeutic approaches that may helpequine practitioners to identify and treat select musculoskeletal disorders. Direct measures ofchiropractic techniques in horses demonstrate substantial induced vertebral motion, usually beyondthe normal range of segmental motion that occurs during locomotion. Future studies need toevaluate the long-term functional effects of chiropractic. Author’s address: Department of Biomed-ical Sciences, College of Veterinary Medicine, Cornell University, Ithaca, New York 14853-6401.© 2000 AAEP.
Introduction
Equine practitioners have seen a recent prolifera-tion in the use of chiropractic techniques within theveterinary profession. However, since veterinari-ans do not receive a formal chiropractic education,many practitioners do not have a basic understand-ing of chiropractic principles or clinical applications.In addition, limited research has been done to eval-uate the clinical effectiveness of chiropractic tech-niques in horses. Veterinary medicine, for themost part, has been forced to acknowledge the use ofchiropractic and other non-traditional modalities byowners who have sought practitioners that use thesetechniques and have experienced their perceivedtherapeutic effects.1 If veterinarians have nottaken the time or effort to learn more about thesenon-traditional techniques, then objectively evaluat-ing its use or discussing the indications or contrain-dications for a specific treatment modality isdifficult. Therefore, owners often seek advice aboutalternative therapies or treatment from someonewho is not their regular veterinarian, often withoutthe veterinarian’s knowledge. To complicate mat-ters, some individuals claim to be “equine chiroprac-tors” but are not professionally trained nor licensedin either chiropractic or veterinary medicine. Thepurpose of this article is to describe the generalprinciples, indications, and contraindications forequine chiropractic care.
Chiropractic Principles
The word chiropractic is derived from the Greekwords cheir meaning ‘hand’ and praktike meaning‘business or to practice’. The practice of chiroprac-tic focuses on the relationship between structure(primarily the vertebral column) and function (as
coordinated by the nervous system) and how thatrelationship affects the preservation and restorationof health. Chiropractic is a form of manual therapythat uses controlled forces which are applied to spe-cific articulations or anatomic regions to induce atherapeutic response via induced changes in jointstructures, muscle function, and neurologic reflexes.The principle common to all chiropractic theories isthat joint dysfunction affects the normal neurologi-cal balance found in healthy individuals. The the-ory of a ‘bone out of place’ is outdated and notsupported by current spinal research.
Clinical Applications
The prevalence of back problems in horses variesgreatly (from 0.9–94%), depending on the specializa-tion or type of practice surveyed: general practice(0.9%); Thoroughbred racehorse practice (2%); vet-erinary school referrals (5%); mixed equine practice(dressage, show-jumpers, eventing) (13%); spinal re-search clinic (47%); or equine chiropractic clinic(94%).2 Veterinarians often have difficulties whendealing with horses that have no obvious localizedpain or have vague, unspecified lameness. Neck orback problems and lameness are often interrelated.Lower limb injuries can cause an alteration in car-riage of the affected limb and altered gait, which cansubsequently overwork or injure proximal limb mus-culature and the paraspinal musculature. Simi-larly, vertebral column injuries can produce gaitabnormalities, increased concussive forces, andlower limb lameness. The diagnostic dilemma fac-ing veterinarians is to decide whether the limb orthe vertebral column is the primary or initial causeof the horse’s clinical problem. Unless the primarycause of the neck or back pain is identified and
84 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000
treated, most horses will have recurrent back painwhen returned to work after a period of rest or trialof anti-inflammatory medications. Nonspecific backpain is most likely related to a functional impair-ment and not a structural disorder. Therefore,many back problems may be related to muscle orjoint dysfunction with resultant soft tissue irritationand pain generation.3
Chiropractic provides expertise in the evaluationof vertebral column disorders and can provide anadditional means of diagnosis and early treatmentoptions in certain types of gait abnormalities or per-formance problems. Prepurchase examinations us-ing chiropractic examination techniques can alsohelp identify horses that have chronic underlyingneck or back problems.4 Chiropractic addressessubclinical conditions or abnormal biomechanicsthat may progress to future debilitating musculo-skeletal injuries. Chiropractors are also trained inthe use of physiotherapy modalities, strength train-ing exercises, massage, stretching techniques, andother forms of musculoskeletal and nerve rehabili-tation. Equine chiropractic is a complementarymodality that can be used in veterinary medicine forthe diagnosis, treatment, and potential preventionof select musculoskeletal disorders in horses.
Joint Physiology
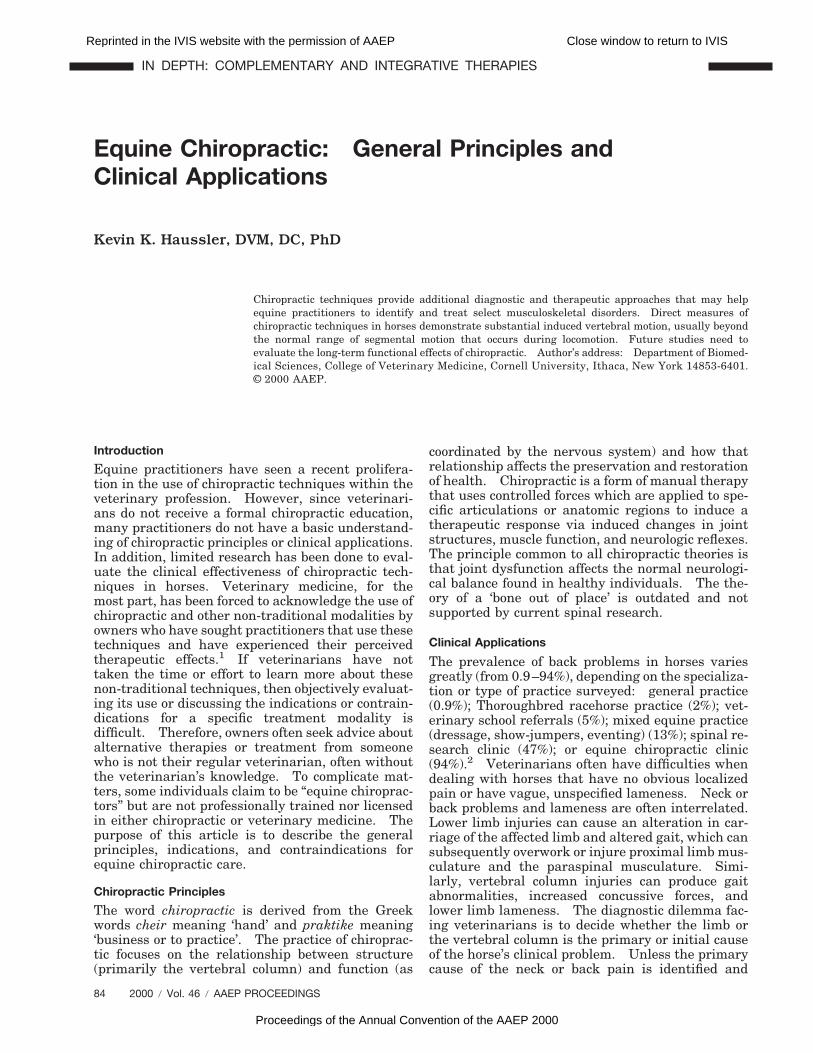
The vertebral motion segment is the functional unitof the vertebral column, which includes two adjacentvertebrae and the associated soft tissues that bindthem together. Joint motion can be categorizedinto three zones of movement: physiologic, para-physiologic, and pathologic (Fig. 1). The physiolog-ical zone of movement includes both active andpassive ranges of motion and is the site where jointmobilization occurs (Figs. 2 and 3). The paraphysi-ological zone of movement exists outside the joint’snormal elastic barrier and is the site of joint cavita-tion (i.e., noise associated with “cracking yourknuckles.”). The normal elastic barrier of the jointis a semi-restrictive anatomical barrier between thephysiologic and paraphysiologic ranges of motion.The pathological zone of movement lies outside thelimits of normal anatomic joint integrity and is char-acterized by joint injury (e.g., sprain, subluxation, or
luxation). Vertebral motion segment injury maycause altered proprioception, protective muscleguarding, altered intervertebral disc and joint bio-mechanics, and increased tension and stress in thejoint capsules and adjacent ligaments.5,6
The goal of chiropractic treatment is to restorenormal joint motion, stimulate neurologic reflexes,and to reduce pain and muscle hypertonicity. Suc-cessful manipulation requires proper technique (i.e.,correct direction, force, amplitude, and velocity) andheightened psychomotor skills.6 A thorough knowl-edge of vertebral anatomy and joint biomechanics isrequired for proper chiropractic evaluation andtreatment. During a successful adjustment, a ‘re-lease’ or movement of the restricted articulation isoften palpable. An audible ‘popping’ sound mayalso be heard during treatment as the applied forceovercomes the elastic barrier of joint resistance.7
The rapid articular separation produces a cavitationof the synovial fluid.8 Radiographic studies postad-justing have shown a radiolucent cavity within thejoint space (i.e., vacuum phenomenon) that contains
Fig. 1. Schematic representation of the three articular zones ofjoint movement. The elastic barrier and the anatomic limitmark the transitional boundaries between the three articularzones.
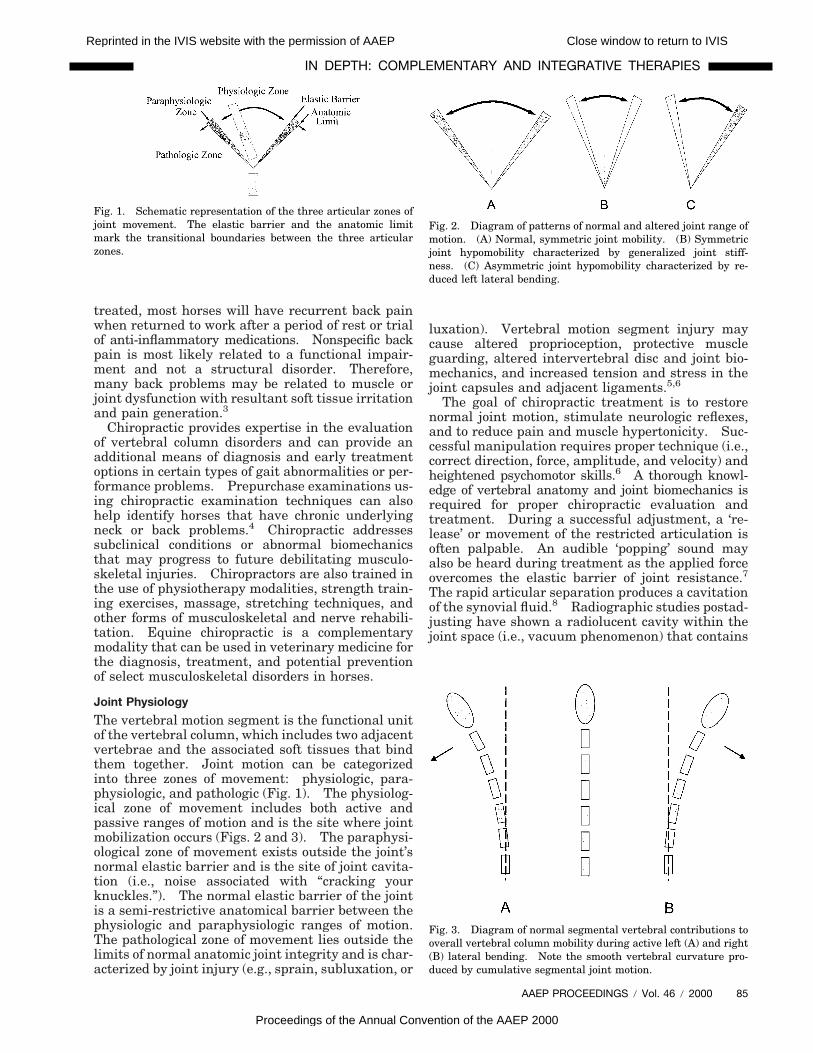
Fig. 2. Diagram of patterns of normal and altered joint range ofmotion. (A) Normal, symmetric joint mobility. (B) Symmetricjoint hypomobility characterized by generalized joint stiff-ness. (C) Asymmetric joint hypomobility characterized by re-duced left lateral bending.
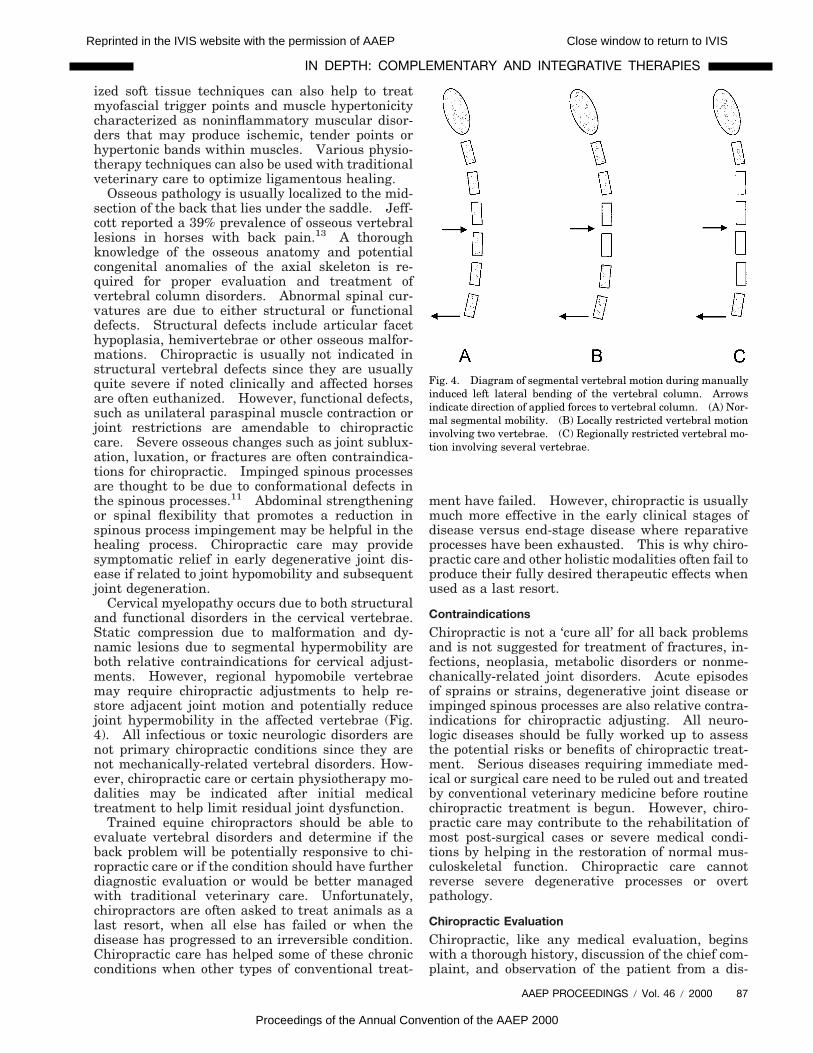
Fig. 3. Diagram of normal segmental vertebral contributions tooverall vertebral column mobility during active left (A) and right(B) lateral bending. Note the smooth vertebral curvature pro-duced by cumulative segmental joint motion.
AAEP PROCEEDINGS / Vol. 46 / 2000 85
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

80% carbon dioxide and lasts for 15–20 min.9 Asecond attempt to recavitate the joint will be unsuc-cessful and potentially painful until the intra-artic-ular gas has been reabsorbed (the refractory period).
Joint Dysfunction
The basic elements of joint dysfunction include al-tered articular neurophysiology, biochemical alter-ations, joint capsule pathology, and articulardegeneration.5,6 Vertebral segment dysfunction(chiropractically defined subluxation) is a vertebrallesion characterized by 1) asymmetric or loss of nor-mal joint motion in one or more planes (Figs. 4 and5); 2) an altered point tenderness or diminished painthreshold to pressure in the adjacent paraspinaltissues or osseous structures; 3) abnormal paraspi-nal muscle tension; and 4) visual or palpatory signsof active inflammatory processes or chronic tissuetexture abnormalities (i.e., edema, fibrosis, hyper-emia, or altered temperature).5 Multiple theorieshave been proposed and tested over the years toexplain the pathophysiology of vertebral segmentdysfunction and its interactions and influences onthe neuromusculoskeletal system.5,6 Altered me-chanical and biochemical processes influence theneuromusculoskeletal system in the following ways:altered joint mobility (hypomobility, hypermobility),altered articular neurophysiology and pain sensa-tion (inhibition, facilitation), altered muscle func-tion (hypertonicity, atrophy), connective tissuechanges (fibrosis), and vascular alterations (isch-emia, hyperemia).5,6 Additionally, the inflamma-tory process influences all these components toproduce biochemical and cellular changes that re-sult in distinct vertebral histopathology. The ver-tebral subluxation complex is a theoretical model ofvertebral segmental dysfunction that incorporatesthe complex interaction of pathological changes innervous, muscular, articular, ligamentous, vascular,and connective tissues.10 Alterations in articularneurophysiology from mechanical or chemical inju-ries can affect both mechanoreceptor and nociceptorfunction via increased joint capsule tension andnerve ending hypersensitivity. Mechanoreceptorstimulation induces reflex paraspinal musculaturehypertonicity and altered local and systemic neuro-logic reflexes. Nociceptor stimulation results in alowered pain threshold, sustained afferent stimula-tion (i.e., facilitation), reflex paraspinal musculaturehypertonicity, and abnormal neurologic reflexes.
Back Problems
Any vertebral column disorder can have serious ef-fects on a horse’s ability to perform. Back problemscan be classified into three basic types of injuriesinvolving either the muscles, tendons and ligaments(soft tissue injuries), bones and joints (osseous inju-ries) or nervous system (neurologic disorders). How-ever, multiple concurrent injuries have beenreported in 17% of horses with back pain.11
Diagnosis of the underlying vertebral pathology in
horses with back pain is important for the appropri-ate treatment and management of these disorders.Primary vertebral injuries usually affect theparaspinal musculature or vertebral articulations.Chiropractic conditions in performance horses usu-ally have a history of a traumatic event or injuryrelated to overexertion.12 Trauma may occur as asingle event such as a trailer accident, falling overbackwards, or dramatic falls over jumps (macro-trauma). Severe injuries may gradually improvebut never totally resolve or subsequently developdebilitating arthritis or soft tissue fibrosis.Chronic, overuse injuries (microtrauma) are usuallyassociated with poor saddle fit, improper riding tech-niques, inadequate shoeing, or faulty conformation.Long periods of confinement, inconsistent trainingprograms, overuse syndromes, or stresses andstrains related to athletic activities may also predis-pose horses to musculoskeletal injuries and reducedperformance. Older horses, like elderly humans,are susceptible to loss of vertebral column flexibility,joint degeneration, and loss of muscle strength.Aged horses also have increased healing times andincreased chances of having chronic conditions orabnormal musculoskeletal compensations fromprior injuries.
Indications
Chiropractic provides additional diagnostic ap-proaches that are not currently available in veteri-nary medicine. The principal indications forequine chiropractic evaluation are back or neckpain, localized or regional joint stiffness, poor per-formance, and an altered gait that is not associatedwith overt lameness. A thorough diagnostic workupis required to identify soft tissue and osseous pathol-ogy, neurologic disorders, or other lameness conditionsthat may not be responsive to chiropractic care. Theprimary clinical signs that equine chiropractors lookfor are localized musculoskeletal pain, muscle hyper-tonicity, and restricted joint motion. This triad ofclinical signs can be found in a variety of lower limbdisorders, but is most evident in neck or backproblems. Chiropractic care can help manage themuscular, articular, and neurologic components ofselect musculoskeletal injuries in performancehorses. Musculoskeletal conditions that are chronicor recurring, not readily diagnosed, or are not re-sponding to conventional veterinary care may beindicators that chiropractic consultation is needed.
Soft tissue injuries have been noted in 39% ofhorses with back pain.11 The most commonly re-ported injuries included longissimus muscle strainand supraspinous and sacroiliac ligament sprains.Jeffcott reported a complete recovery rate of 73%and recurrence of 25% in horses with soft tissueinjuries.13 Chiropractic care is usually contraindi-cated in the acute stages of soft tissue injury. How-ever, as the soft tissue injury heals, chiropractic hasthe potential to help restore normal joint motion,thus limiting the risk for future reinjury.3 Special-
86 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000
ized soft tissue techniques can also help to treatmyofascial trigger points and muscle hypertonicitycharacterized as noninflammatory muscular disor-ders that may produce ischemic, tender points orhypertonic bands within muscles. Various physio-therapy techniques can also be used with traditionalveterinary care to optimize ligamentous healing.
Osseous pathology is usually localized to the mid-section of the back that lies under the saddle. Jeff-cott reported a 39% prevalence of osseous vertebrallesions in horses with back pain.13 A thoroughknowledge of the osseous anatomy and potentialcongenital anomalies of the axial skeleton is re-quired for proper evaluation and treatment ofvertebral column disorders. Abnormal spinal cur-vatures are due to either structural or functionaldefects. Structural defects include articular facethypoplasia, hemivertebrae or other osseous malfor-mations. Chiropractic is usually not indicated instructural vertebral defects since they are usuallyquite severe if noted clinically and affected horsesare often euthanized. However, functional defects,such as unilateral paraspinal muscle contraction orjoint restrictions are amendable to chiropracticcare. Severe osseous changes such as joint sublux-ation, luxation, or fractures are often contraindica-tions for chiropractic. Impinged spinous processesare thought to be due to conformational defects inthe spinous processes.11 Abdominal strengtheningor spinal flexibility that promotes a reduction inspinous process impingement may be helpful in thehealing process. Chiropractic care may providesymptomatic relief in early degenerative joint dis-ease if related to joint hypomobility and subsequentjoint degeneration.
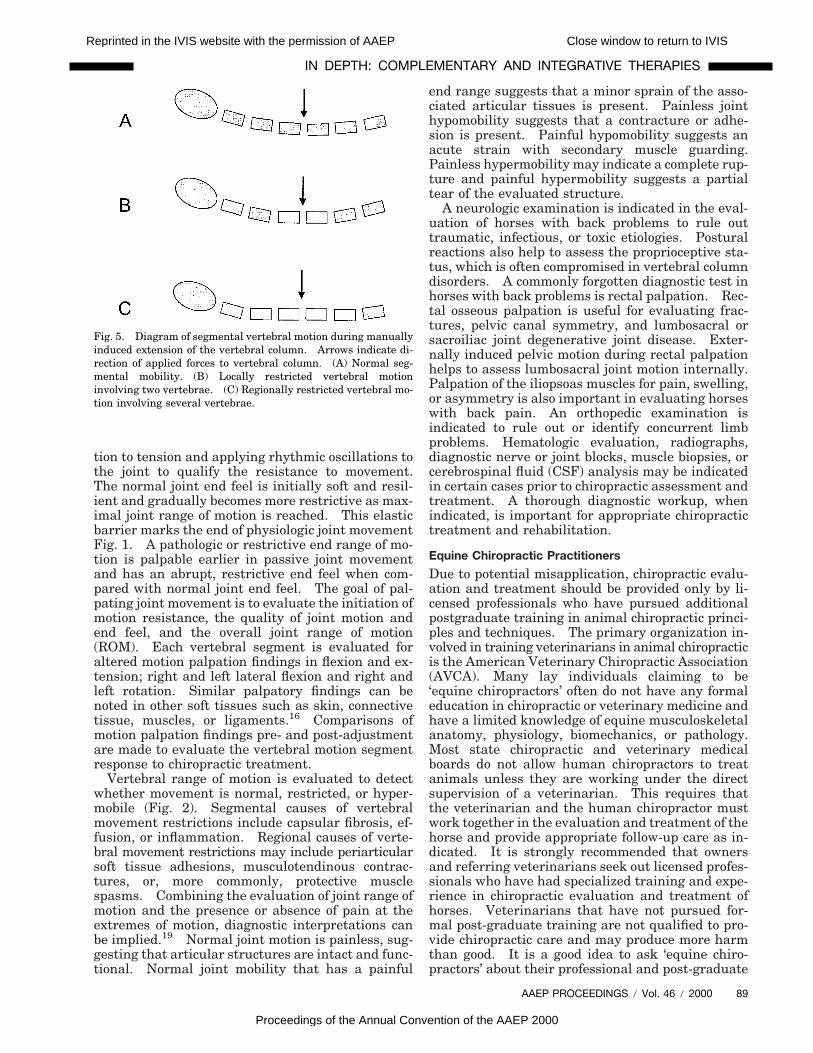
Cervical myelopathy occurs due to both structuraland functional disorders in the cervical vertebrae.Static compression due to malformation and dy-namic lesions due to segmental hypermobility areboth relative contraindications for cervical adjust-ments. However, regional hypomobile vertebraemay require chiropractic adjustments to help re-store adjacent joint motion and potentially reducejoint hypermobility in the affected vertebrae (Fig.4). All infectious or toxic neurologic disorders arenot primary chiropractic conditions since they arenot mechanically-related vertebral disorders. How-ever, chiropractic care or certain physiotherapy mo-dalities may be indicated after initial medicaltreatment to help limit residual joint dysfunction.
Trained equine chiropractors should be able toevaluate vertebral disorders and determine if theback problem will be potentially responsive to chi-ropractic care or if the condition should have furtherdiagnostic evaluation or would be better managedwith traditional veterinary care. Unfortunately,chiropractors are often asked to treat animals as alast resort, when all else has failed or when thedisease has progressed to an irreversible condition.Chiropractic care has helped some of these chronicconditions when other types of conventional treat-
ment have failed. However, chiropractic is usuallymuch more effective in the early clinical stages ofdisease versus end-stage disease where reparativeprocesses have been exhausted. This is why chiro-practic care and other holistic modalities often fail toproduce their fully desired therapeutic effects whenused as a last resort.
Contraindications
Chiropractic is not a ‘cure all’ for all back problemsand is not suggested for treatment of fractures, in-fections, neoplasia, metabolic disorders or nonme-chanically-related joint disorders. Acute episodesof sprains or strains, degenerative joint disease orimpinged spinous processes are also relative contra-indications for chiropractic adjusting. All neuro-logic diseases should be fully worked up to assessthe potential risks or benefits of chiropractic treat-ment. Serious diseases requiring immediate med-ical or surgical care need to be ruled out and treatedby conventional veterinary medicine before routinechiropractic treatment is begun. However, chiro-practic care may contribute to the rehabilitation ofmost post-surgical cases or severe medical condi-tions by helping in the restoration of normal mus-culoskeletal function. Chiropractic care cannotreverse severe degenerative processes or overtpathology.
Chiropractic Evaluation
Chiropractic, like any medical evaluation, beginswith a thorough history, discussion of the chief com-plaint, and observation of the patient from a dis-
Fig. 4. Diagram of segmental vertebral motion during manuallyinduced left lateral bending of the vertebral column. Arrowsindicate direction of applied forces to vertebral column. (A) Nor-mal segmental mobility. (B) Locally restricted vertebral motioninvolving two vertebrae. (C) Regionally restricted vertebral mo-tion involving several vertebrae.
AAEP PROCEEDINGS / Vol. 46 / 2000 87
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

tance for conformation, posture, and signs oflameness. Horses with conditions that may be re-sponsive to chiropractic care present with a widevariety of non-specific or vague complaints (Table1). The focus of the chiropractic exam is placed onevaluating static and dynamic characteristics of themusculoskeletal system. Initially, the horse’s gen-eral attitude and behavior are monitored for signs ofpain or discomfort. Vertebral column conformationis then evaluated for proper alignment and symme-try with special attention to the top line, shape andheight of the withers, and osseous pelvic symme-try. It is thought that short-coupled horse have ahigher incidence of osseous disorders whereas long-backed horses are more prone to soft tissueinjuries.14 Conformation is a structural relation-ship of body segments, whereas postural analysisdeals more with functional relationships. Thehorse is stood on a hard, level surface and evaluatedfor a preferred or shifting stance, head and neckcarriage, vertebral curvatures, and muscular sym-metry. Chiropractic gait analysis focuses on eval-uating regional vertebral mobility and pelvic motionsymmetry, in addition to the typical lameness as-sessment. Gait analysis may help to rule out lowerlimb disorders and rule in vertebral dysfunction,although limb lameness has been reported in about85% of horses with back problems.15 Motion asym-metries, restricted vertebral or pelvic mobility, nottracking straight, or lack of propulsion are a fewcharacteristics that are evaluated. Tape on the
vertebral column midline or tuber coxae may help tovisualize subtle motions. Evaluation of the re-sponse to placing a saddle and being ridden is im-portant for a complete assessment of horses withback problems. Inspection of the tack for properuse and fit are always suggested on initial examina-tion. Saddles and restraint devices should be eval-uated for proper fit, padding, and positioning on thehorse.
The physical examination is used to rule out othermore common causes of lameness or neurologicaldisorders. When indicated, a traditional orthope-dic and neurologic evaluation is used. The chiro-practic spinal examination focuses on evaluatingand localizing segmental vertebral dysfunction.Palpation is reliable to localize and identify softtissue and osseous structures for changes in texture,tissue mobility, or resistance to pressure.14,16 Thetissue layers are evaluated from superficial to deepby increasing digital pressure and also shiftingattention with discrete palpatory movements.Shapes of structures, transitions between struc-tures, and attachment sites may also be palpated.3
Soft tissue texture and mobility can be comparedbetween the skin, subcutaneous tissue, muscle, andthoracolumbar fascia. Patient response to palpa-tion is important especially in evaluating tendernessor hypersensitivity. The hallmarks of segmentalvertebral dysfunction include abnormal paraspinalmuscle tonicity, pain and edematous tissues.10
Osseous palpation involves evaluating osseousstructures for pain, morphology, asymmetries, andalignment. Individual thoracic, lumbar, and sacralspinous processes are palpated for a painful re-sponse and the tuber sacrale is palpated for heightasymmetries. Individual spinous process deviationis common but it is not usually associated with spi-nous process fracture or vertebral malposition (i.e.,bone out of place), as is commonly thought. Over-lapping or malaligned dorsal spinous processes areoften caused by spinous process impingement, devel-opmental asymmetries in the neural arch, or iso-lated dorsal spinous process deviation of unknownetiology.17,18
Motion palpation is used to evaluate each individ-ual vertebra for loss of normal joint motion andoverall resistance to induced motion (Figs. 4 and5). Vertebral segments with altered motion palpa-tion findings can occur with or without localizedmuscle hypertonicity and pain. To utilize palpa-tion in the evaluation of the musculoskeletal systemfully, there has to be an understanding of how jointmotion is assessed.3 Moving an articulation from aneutral position first involves evaluating a range ofmotion that has minimal, uniform resistance. Asthe articulation is moved toward the end of thatrange of motion there is a gradual increase in theresistance to movement (i.e., joint end feel). Endrange of motion starts when any change in resis-tance to passive joint manipulation is palpable.Joint end feel is evaluated by bringing the articula-
Table 1. Potential clinical indications for chiropractic evaluationand treatment.12
Poor performanceBack or neck painReduced neck or back flexibilityNot able to raise or lower head and neckLocalized muscle tightnessVague lamenessUneven or asymmetric gaitRecent change in spinal conformationDifficult or improper saddle fitDiscomfort with saddle placementResents tightening of the cinch or girthStiff and slow to warm upBucks or pins ears when riddenLame only when riddenConstantly on one rein or lineDifficulty with a lead or gait transitionRefuses jumpsResists collectionDifficulty with turning in one directionConsistently stumbles or drags a toeMuscle mass asymmetryPelvic asymmetryNot stand squarely on all four limbsDifficulty standing for the farrierHolds tail to one sideResents being groomedBehavior or avoidance problem
88 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000
tion to tension and applying rhythmic oscillations tothe joint to qualify the resistance to movement.The normal joint end feel is initially soft and resil-ient and gradually becomes more restrictive as max-imal joint range of motion is reached. This elasticbarrier marks the end of physiologic joint movementFig. 1. A pathologic or restrictive end range of mo-tion is palpable earlier in passive joint movementand has an abrupt, restrictive end feel when com-pared with normal joint end feel. The goal of pal-pating joint movement is to evaluate the initiation ofmotion resistance, the quality of joint motion andend feel, and the overall joint range of motion(ROM). Each vertebral segment is evaluated foraltered motion palpation findings in flexion and ex-tension; right and left lateral flexion and right andleft rotation. Similar palpatory findings can benoted in other soft tissues such as skin, connectivetissue, muscles, or ligaments.16 Comparisons ofmotion palpation findings pre- and post-adjustmentare made to evaluate the vertebral motion segmentresponse to chiropractic treatment.
Vertebral range of motion is evaluated to detectwhether movement is normal, restricted, or hyper-mobile (Fig. 2). Segmental causes of vertebralmovement restrictions include capsular fibrosis, ef-fusion, or inflammation. Regional causes of verte-bral movement restrictions may include periarticularsoft tissue adhesions, musculotendinous contrac-tures, or, more commonly, protective musclespasms. Combining the evaluation of joint range ofmotion and the presence or absence of pain at theextremes of motion, diagnostic interpretations canbe implied.19 Normal joint motion is painless, sug-gesting that articular structures are intact and func-tional. Normal joint mobility that has a painful
end range suggests that a minor sprain of the asso-ciated articular tissues is present. Painless jointhypomobility suggests that a contracture or adhe-sion is present. Painful hypomobility suggests anacute strain with secondary muscle guarding.Painless hypermobility may indicate a complete rup-ture and painful hypermobility suggests a partialtear of the evaluated structure.
A neurologic examination is indicated in the eval-uation of horses with back problems to rule outtraumatic, infectious, or toxic etiologies. Posturalreactions also help to assess the proprioceptive sta-tus, which is often compromised in vertebral columndisorders. A commonly forgotten diagnostic test inhorses with back problems is rectal palpation. Rec-tal osseous palpation is useful for evaluating frac-tures, pelvic canal symmetry, and lumbosacral orsacroiliac joint degenerative joint disease. Exter-nally induced pelvic motion during rectal palpationhelps to assess lumbosacral joint motion internally.Palpation of the iliopsoas muscles for pain, swelling,or asymmetry is also important in evaluating horseswith back pain. An orthopedic examination isindicated to rule out or identify concurrent limbproblems. Hematologic evaluation, radiographs,diagnostic nerve or joint blocks, muscle biopsies, orcerebrospinal fluid (CSF) analysis may be indicatedin certain cases prior to chiropractic assessment andtreatment. A thorough diagnostic workup, whenindicated, is important for appropriate chiropractictreatment and rehabilitation.
Equine Chiropractic Practitioners
Due to potential misapplication, chiropractic evalu-ation and treatment should be provided only by li-censed professionals who have pursued additionalpostgraduate training in animal chiropractic princi-ples and techniques. The primary organization in-volved in training veterinarians in animal chiropracticis the American Veterinary Chiropractic Association(AVCA). Many lay individuals claiming to be‘equine chiropractors’ often do not have any formaleducation in chiropractic or veterinary medicine andhave a limited knowledge of equine musculoskeletalanatomy, physiology, biomechanics, or pathology.Most state chiropractic and veterinary medicalboards do not allow human chiropractors to treatanimals unless they are working under the directsupervision of a veterinarian. This requires thatthe veterinarian and the human chiropractor mustwork together in the evaluation and treatment of thehorse and provide appropriate follow-up care as in-dicated. It is strongly recommended that ownersand referring veterinarians seek out licensed profes-sionals who have had specialized training and expe-rience in chiropractic evaluation and treatment ofhorses. Veterinarians that have not pursued for-mal post-graduate training are not qualified to pro-vide chiropractic care and may produce more harmthan good. It is a good idea to ask ‘equine chiro-practors’ about their professional and post-graduate
Fig. 5. Diagram of segmental vertebral motion during manuallyinduced extension of the vertebral column. Arrows indicate di-rection of applied forces to vertebral column. (A) Normal seg-mental mobility. (B) Locally restricted vertebral motioninvolving two vertebrae. (C) Regionally restricted vertebral mo-tion involving several vertebrae.
AAEP PROCEEDINGS / Vol. 46 / 2000 89
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

training or certification, horse experience, and thetypes of techniques that they use (e.g., hands onlyvs. hammers, mallets or mechanical devices).
Chiropractic Techniques
Chiropractic provides important therapeutic ap-proaches that are not currently available in veteri-nary medicine. Most of what we know aboutequine chiropractic has been borrowed from humanchiropractic techniques, theories, and research andadapted to our animal patients. Therapeutic trialsof chiropractic adjustments are often used since wecurrently have limited knowledge about the effectsof chiropractic care in animals. Chiropractic ad-dresses mechanically-related disorders of the mus-culoskeletal and nervous systems and provides aconservative means of treatment and prevention forhorses with back problems. Chiropractic tech-niques involve a controlled force applied to a specificanatomical region or osseous structure to produce adesired therapeutic response (i.e., restore joint mo-tion and reduce pain). Chiropractic adjustmentsare applied to areas of vertebral segment dysfunc-tion and the horse’s condition is closely monitored asthe neuromusculoskeletal system responds to theapplied treatment. The applied treatment influ-ences both mechanoreceptor and nociceptor functionvia mechanical and biological mechanisms.5 The‘therapeutic dosage’ of chiropractic adjusting is con-trolled by the number of vertebral levels adjusted,the amplitude of the applied force, and the frequencyof treatment.
Veterinarians and clients often ask how a 1200pound horse can be adjusted. The answer is onevertebral segment at a time. Recent equine chiro-practic research has demonstrated that forces ap-plied to instrumented vertebral segments do inducesubstantial vertebral motion, usually beyond thenormal range of segmental motion that occurs dur-ing locomotion.20 At the L6-S1 vertebral segments,chiropractic adjustments induced 3.0 6 1.2° of dor-soventral flexion, 2.7 6 0.4° of lateral bending, and2.7 6 0.5° of axial rotation. Segmental vertebralmotion characteristics induced during chiropractictreatment in horses are similar to those reported inhumans.21 The induced vertebral motion supportscurrent theories on the effects of chiropractic manip-ulations on joint physiology. Future studies needto evaluate the long term mechanical and neuro-physiologic effects of chiropractic techniques inhorses. Knowledge of normal segmental vertebralmotion and response to manual therapies will fur-ther our future understanding of the pathophysiol-ogy, clinical diagnosis and treatment of backproblems in horses.
In a relaxed horse, the mass (vertebral segment)that is affected by a rapidly applied adjustive thrustis proportionately smaller than the mass of the prac-titioner applying the treatment. However, if thehorse does not relax the paraspinal musculature,then the mass that is affected increases dramati-
cally from the mass of a few vertebral segments tothe mass of the entire vertebral region or potentiallyentire horse. In this situation it is nearly impossi-ble to induce any vertebral movement and chiropracticadjustments are futile. An effective adjustmentcannot be applied to a nervous, tense horse withoutrisk of injury to the horse or the practitioner. Un-educated individuals that do not understand thisconcept and do not have thorough understanding ofjoint physiology, vertebral anatomy, biomechanics,or chiropractic principles will resort to overly ag-gressive and forceful means of applying an externalforce (e.g., sledge hammers and two-by-fours, threestrong men and a twitch, or tractors). Small, rap-idly applied adjustments are easier to control andhave much less risk of soft tissue or osseous injurythan more forceful types of manipulation. Chiro-practic adjustments are usually done without anysedation or other medications, but may occasionallyby done under anesthesia if indicated.22 A goodrule of thumb is, if it does not look like somethingthat you would be willing to have done to yourself,then maybe you should not have it done to a horse.
Chiropractic Treatment
Horses are usually held by a trained handler on aloose lead during the chiropractic treatment. Thecervical vertebrae (Fig. 6), sacrum, and extremitiesare evaluated and adjusted as needed from groundlevel. However, the thoracolumbar vertebrae(Figs. 7 and 8) and pelvis often require an elevatedsurface to stand on for effective adjustments andproper doctor positioning to limit potential injury tothe doctor. Equine chiropractic is physically de-manding and requires significant mental concentra-tion. The horse must be relaxed and focused onwhat the practitioner is doing. The practitionermust also be relaxed and focused on the horse to
Fig. 6. Photograph of a typical chiropractic adjustment in thecervical vertebral region.
90 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000
adjust a specific vertebral segment without causinginjury to the surrounding tissues or to the practitio-ner themselves. Environmental distractions arecounterproductive to effective chiropractic care.
Muscle relaxation allows the specified joints to bebrought to tension before adjusting and to evaluatethe elastic barrier of the joint. Motion palpation isused to evaluate joint motion restrictions so that theadjustive thrust can be applied correctly. Stabili-zation of adjacent joints or vertebral segments isrequired for the application of a proper adjustivethrust. Chiropractic adjustments involve rapid,small amplitude forces applied to specific musculo-skeletal structures with the intent of evoking a ther-apeutic response.
The principal indications for chiropractic treat-ment are localized pain, muscle hypertonicity andrestricted segmental joint motion. Typically, animmediate reduction in pain and an increase in seg-mental vertebral motion is noted. Most horses willalso have increased muscle relaxation, but othertherapies (e.g., acupuncture or stretching) are oftenused in conjunction with chiropractic adjustment tocompletely resolve any remaining muscle hyperto-nicity. In general, conditions with an acute onsetrespond rapidly, whereas chronic conditions usuallytake long-term treatment or rehabilitation. Chiro-practic is a conservative modality that may be ap-plied repetitively over a set time period as the
patient’s own recuperative abilities are used in thehealing process to restore normal joint motion andneurologic function. This is often a confusing con-cept for most traditional practitioners accustomed toa ‘one-time-fix’ by utilizing potent medications orsurgical procedures. Post-adjustment recommen-dations for actively training horses usually includestall rest or pasture turnout for one day. This pro-vides an opportunity for the horse’s body to respondto the applied treatment without being exposed topotential inciting factors of the vertebral segmentdysfunction. The horse is asked to return to nor-mal work the next day unless other musculoskeletalinjuries are present, then appropriate supportivecare is recommended. If stiffness or soreness isnoted postadjusting, then an additional day of rest issuggested. If severe or continued discomfort isnoted for two days then re-examination and appro-priate referral, medical treatment, or physiotherapyshould be prescribed.
Complications or Adverse Effects
Potential adverse effects from properly applied chi-ropractic treatments include a transient stiffness orworsening of the condition after adjusting (i.e., ag-gravated complaint, worsening of preexisting state,regional soreness, or lameness).6 Adverse reac-tions from chiropractic adjustments are uncommon,
Fig. 8. Photograph of a typical chiropractic adjustment in thelumbar vertebral region.
Fig. 7. Photograph of a typical chiropractic adjustment in thecranial thoracic (withers) vertebral region.
AAEP PROCEEDINGS / Vol. 46 / 2000 91
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

but may occur immediately postadjusting or insidi-ously within the next 6–12 hr. The undesired ef-fects usually last less than 24–48 hr. If moreserious reactions are noted that last longer than oneto two days, a thorough re-examination and appro-priate treatment should be pursued. If the condi-tion does not improve with conservative care, thenreferral for more aggressive diagnostic or therapeu-tic modalities is recommended. Potential harmfuleffects from improperly applied manipulation fromuntrained individuals may include permanent artic-ular damage or loss of function (i.e., torn ligaments,injured muscles, luxated joints, fractures, or paral-ysis if severe underlying pathology is present).
Adjunctive Recommendations and Prognosis
Chiropractic care is often supplemented with mas-sage, physiotherapy modalities, and stretching orstrengthening exercises to help soft tissue rehabili-tation and to help restore normal vertebral jointmotion. These concurrent therapies also help toencourage owner participation in the healing pro-cess and provide close monitoring of the patient’sprogress. Other recommendations may includechanges in training schedules or activities, correc-tive shoeing, or tack changes. Many repetitive usedisorders may benefit from cross-training activities.Many practitioners have also reported synergistictherapeutic effects with the combined use of chiro-practic, acupuncture, and other holistic modalitiesin equine patients. Usually, conditions with anacute onset respond rapidly and have a good prognosisfor return to function, whereas chronic conditions usu-ally take long-term treatment or rehabilitation. Pa-tients with chronic injuries may gain only short-termimprovement of restricted motion, pain or muscle hy-pertonicity. This corresponds to current research onjoint immobilization and spinal learning.3 Chronicconditions usually require a series of adjustments toeffect a more lasting improvement. Musculoskeletalhealth depends on movement and use. Scientific ev-idence suggests that long-term rest is contraindicatedfor back pain.23
Summary
A thorough knowledge of equine vertebral columnanatomy, biomechanics, and pathology is required tounderstand the principles and theories behindchiropractic and to apply its techniques properly.Chiropractic provides additional diagnostic andtherapeutic means that may help equine practitio-ners to identify and treat the primary cause of lame-ness or poor performance. Chiropractic providesspecialized evaluation and treatment of joint dys-function and conservative treatment of neuromus-culoskeletal disorders that are currently lacking intraditional veterinary medicine. However, limitedresearch is currently available on equine chiroprac-tic and other nontraditional modalities in veterinary
medicine. In 1996, the AVMA’s Committee on Al-ternative and Complementary Therapies suggestedthat the research community should be encouragedto prioritize avenues of research and to allocate re-search funds to projects that will provide furtherscientific evaluation of these modalities.24 The useof chiropractic principles and techniques on animalsis dependent on future research into the clinicaleffectiveness and indications for management ofback problems in horses.
For more information on equine chiropractic orpost-graduate seminars contact the American Vet-erinary Chiropractic Association (AVCA), 623 MainStreet, Hillsdale, IL 61257 Office: (309) 658-2920,Fax: (309) 658-2622, E-mail: [email protected],Web site: http://www.AnimalChiro.com
References1. Wynn SG. Wherefore complementary medicine? J Am Vet
Med Assoc 1996;209:1228–1233.2. Jeffcott LB. Guidelines for the diagnosis and treatment of
back problems in horses, in Proceedings. Am Assoc EquinePract 1980;26:381–387.
3. Liebenson C. Rehabilitation of the spine. 1st ed. Balti-more, MD: Williams & Wilkins, 1996.
4. Willoughby SL. Equine chiropractic care, in Proceedings.Am Assoc Equine Pract 1993;39:31–32.
5. Leach RA. The chiropractic theories: principles and clini-cal applications. 3rd ed. Baltimore, MD: Williams &Wilkins, 1994.
6. Haldeman, S. Principles and practice of chiropractic. 2nded. Norwalk, CT: Appleton & Lange, 1992.
7. Reggars JW, Pollard HP. Analysis of zygapophyseal jointcracking during chiropractic manipulation. J ManipulativePhysiol Ther 1995;18:65–71.
8. Herzog W, Zhang YT, Conway PJW, et al. Cavitationsounds during spinal manipulative treatments. J Manipu-lative Physiol Ther 1993;16:523–526.
9. Unsworth A, Dowson D, Wright V. Cracking joints: a bio-engineering study of cavitation in the metacarpophalangealjoint. Ann Rheum Dis 1971;30:348–358.
10. Gatterman MI. Foundations of chiropractic. St. Louis:Mosby-Year Book, Inc., 1995.
11. Jeffcott LB. Disorders of the thoracolumbar spine of thehorse—a survey of 443 cases. Equine Vet J 1980;12:197–210.
12. Willoughby SL. Equine chiropractic care. 1st ed. PortByron, IL: Options for Animals Foundation, 1991.
13. Jeffcott LB. Back problems in the horse—a look at past,present and future progress. Equine Vet J 1979;11:129–136.
14. Cauvin E. Assessment of back pain in horses. In Practice1997;19:522–533.
15. Steckel RR, Kraus-Hansen AE, Fackelman GE, et al. Scin-tigraphic diagnosis of thoracolumbar spinal disease inhorses: a review of 50 cases, in Proceedings. Am AssocEquine Pract 1991;37:583–591.
16. Chaitow L. Palpation skills. New York, NY: ChurchillLivingston, 1997.
17. Jeffcott LB. Radiographic features of the normal equinethoracolumbar spine. Vet Radiol 1979;20:140–147.
18. Haussler KK, Stover SM, Willits NH. Pathology of the lum-bosacral spine and pelvis in Thoroughbred racehorses.Am J Vet Res 1999;60:143–153.
19. Kessler RM, Hertling D. Assessment of musculoskeletaldisorders. In: Hertling D, Kessler RM, eds. Managementof common musculoskeletal disorders: Physical therapyprinciples and methods. 2nd ed. Philadelphia: J. B. Lip-pincott, 1990;68–71.
92 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

20. Haussler KK, Bertram JEA, Gellman K. In-vivo segmentalkinematics of the thoracolumbar spinal region in horses andeffects of chiropractic manipulations, in Proceedings. AmAssoc Equine Pract 1999;45:327–329.
21. Gal JM, Herzog W, Kawchuk GN, et al. Movements of ver-tebrae during manipulative thrusts to unembalmed humancadavers. J Manipulative Physiol Ther 1997;20:30–40.
22. Ahern TJ. Cervical vertebral mobilization under anesthetic
(CVMUA): a physical therapy for the treatment of cervico-spinal pain and stiffness. J Equine Vet Sci 1994;14:540–545.
23. Allan DB, Waddell G. A historical perspective on low backpain and disability. Acta Orthop Scand Suppl 1989;60:1.
24. Smith CA, Tessier GJ. AVMA at work: houses approvesguidelines on alternative, complementary medicine. J AmVet Med Assoc 1996;209:1026.
AAEP PROCEEDINGS / Vol. 46 / 2000 93
IN DEPTH: COMPLEMENTARY AND INTEGRATIVE THERAPIES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000