epilepsziaa kisállatpraxisban...terápiai. • cél: rohm csökkentés,qol,mellékhatások...
TRANSCRIPT

Epilepszia a kisállatpraxisban
Budapest 2018
Prof.h.c., Priv.Doz. Dr Akos Pakozdy PhD, DECVNUniversity of Veterinary Medicine, Vienna

Mi az epilepszia?
• Generalizált epilepsziás roham (klonusos)(nagy roham)
• Myoclonus: hirtelen, rövid
(100msec) akaratlan izomkontrakció
• Clonic: ismétlődő myoklonus
A.Pakozdy

Mi az epilepszia?
John Hughling Jackson
(1835-1911)Charles-Edouard Brown-Sequard
(1817-1894)
Mi az epilepszia?
Current human definitions (ILAE 2005, IVETF 2015)
• Roham:
The term can be used for any sudden, short lasting and transient event.
•Epilepsziás roham:Episodszerű tünet/tünetcsoport az agy elektromos aktivitásának túlműködése által.
•Epilepszia:Agyi megbetegedés, amely egy tartós fokozott készséggel (prediszpozíció) jár epilepsziás rohamok előfordulására.
A gyakorlatban ez 2 roham jelentkezése után mondható ki (amelyek között több mint 24 óra telt el).

Gyakorlati jelentése?
Epilepszás roham:
• Epizódszerű tünetek– Gyakran görcsök (nem mindig)
– Tudatzavar/vesztés (megítélése szubjektív)
– Szenzoros/vegetatív zavar
• Agyi elektromos túlműködés
Epilepszia
• Agyi megbetegedés
• Prediszpozíció epilepsziás rohamokra
• Diagnose ex Juvantibus – az állatorvosi praxisban
További diagnosztika
Klinikai vizsgálat

Klinikai vizsgálat
• Páciens a rohamok között– Nationale
– Klinikai vzsgálat
– Neurológia vizsgálat
– További kivizsgálás
• A roham maga– Leírás
– Video
– A tulajdonos vizsgálja meg
• A kutya fekszik az kevés
• Reszponzív?
• Járóképes?

Epilepsziás roham
• Generalizált
• Pedál automatizmus
A.Pakozdy

Epileptic seizure
• GM with pedal automatism/ lateralisation
A.Pakozdy

Epilepsziás roham
Fokális epilepsziás roham – terjedéssel -generalizáció
A.Pakozdy

Epilepsziás roham
Fokális epiepsziás roham – részleges generalizáció
A.Pakozdy

Epilepsziás roham
• Fokális epilepsziás roham generalizációval
11

Epilepsziás roham• Preiktális fázis
– 1-24h (nem nyilvánvaló)– idegesség, félősség
• Iktusz (10Sek-1h)– Konvulzió: túlzott patológiás izomkontrakció
– Tónusos: tartósan megnövekedett izomtónus
– Klónusos: ismétlődő myoklonus
– Myoclonus: hirtelen, rövid (100msec) akaratlan izomkontrakció
– Automatism: koordinált, ismétlődő motoros tevékenység (futás, ásás, oroalimentáris
– Hallucinációk– Vegetativ tünetek (vizelet, széklet, nyálzás, mydriázis)
– Tudatzavar– Komplex magatartászavar (psychomotor seizure)
• Posztiktális fázis– Általában rövidebb mint 2 h– Todds paralysis– Paresis– Ataxia, kényszermozgás, körben járás, vakság, süketsés– Nyálzás, ugatás, lihegés
A.Pakozdy

Posziktális tünetek
Gyakori a cerebrális tünet:
• Parézis, ataxia• Kényszermozgás• Zavartság
• CAVE neurovizsgálat!!!!
A.Pakozdy

A roham epilepsziás?
• Anamnézisen alapul!
• Video segít – de nem mindig
• „Not everything that shakes is epilepsy”Rothner 1989
A.Pakozdy

Epilepsziás roham?
A.Pakozdy

Epilepsziás roham?
• Myasthenia Gravis:• Epizódikus gyengesés
• Fizikai megterhelés kiváltja– generalisied/Focal/Fulminant Form
• Pihenésre eltűnik/javul
• Parézis van, konvulzió nincs
• Etiológia: – Veleszületett
– Szerzett (immun-mediert)
• Megaeosophagus gyakori
• AcCh-Rez Ab, Tensilon-Test
• Electrodiagnostic
• No response to AED
A.Pakozdy

Epilepsziás roham?
A.Pakozdy

Epilepsziás roham?
• Synkope:„rövid, ájulás-szerű tudatzavar agyi hypoperfúzió miatt“– Kardiogén– Keringési rendszer– Vasovagális
A.Pakozdy

Differenciáldiagnózis: Syncope/Epilepsziás roham (Human)
A.Pakozdy
Syncope Epilepsziás roham
Preictal seconds: vertigo, sweating Longer: behaviouralchange
Heart Bradycardy Tachycardy
Body position Álló helyzet, mozgás Alvás, nyugalmi szakasz
Motor Mild/no motor signs Automatism, convulsions
Inkontinentia rare often

Episodic Disorders
A.Pakozdy
„paroxysmal event“
Anamnézis, klinikai neurológiai vizsgálat
Szívzörej,
ritmuszavar,
cianózis
Hányás, hasmenés,
aszcites
Gyengeség,
Regurgitáció
Kiesési tün.,
Tudat/magatartás
zavar
Fájdalom
Kardiorespir. Metabolikus/
szisztémás
Myast.
gravis
Neurológiai
betegségek
Orthopédiai
problémák

Epilepsziás roham?
21
„Fly-biting“
Stereotypia/OCD
� Therapy:
� Clomipramin 1-2mg/kg bid
� Fluoxetin 1mg/kg bid
� Behavioural therapy

Epilepsziás roham?Narkolepsia/Kataplexia
� Emotional/excitation induced
� Congenital (genetic, autosomal rezessive)
� Dobermann, Labrador, Dackel
� Hypocretin receptor disturbance
� Sporadic HYP deficiency (?)
� Aquired (autoimmune?)
� Therapy:
� Amitriptylin 1-2mg/kg bid
� Imipramin 0.5-1.5mg/kg bid
� Desipramin 3 mg/kg bid
� Methylphenidat 0.25mg/kg SID/BID
� Fluoxetin 1mg/kg sid
� Selegilin 1mg/kg sid
� Bagley and Platt 2013
� Thomas and Dewey 2008

Epilepsziás roham?
23
Exercise Induced Collaps
(Labrador, Clumber Spaniel, Corgi)
Autosomal rezessive
Excitment/Excercise-induced
� Ataxia und Paresis of thehindlimbs
� Body temperature increases
� GENTEST (DynaminMutation)
� Therapy:
� Restriktive working
� Cooling
� Sedation

Epilepsziás roham?
24
Canine Epileptoid Cramping Syndrome
In Border Terrier (Spike`s Disease)
Episods:
Ataxia/falling/stiffness
Abdominal movement/borborygma, tremor
� 2-30Min
� Conscious
� 50% vomiting or diarrhoe
Therapy
� Classic AED does not work
� Diazepam, Clorazepate,
� Buscopan, glutenfree diet� Serum increased Antitransglutaminase2 Antigladin Ab
(normalised after diet (Lowrie et al. 2015)
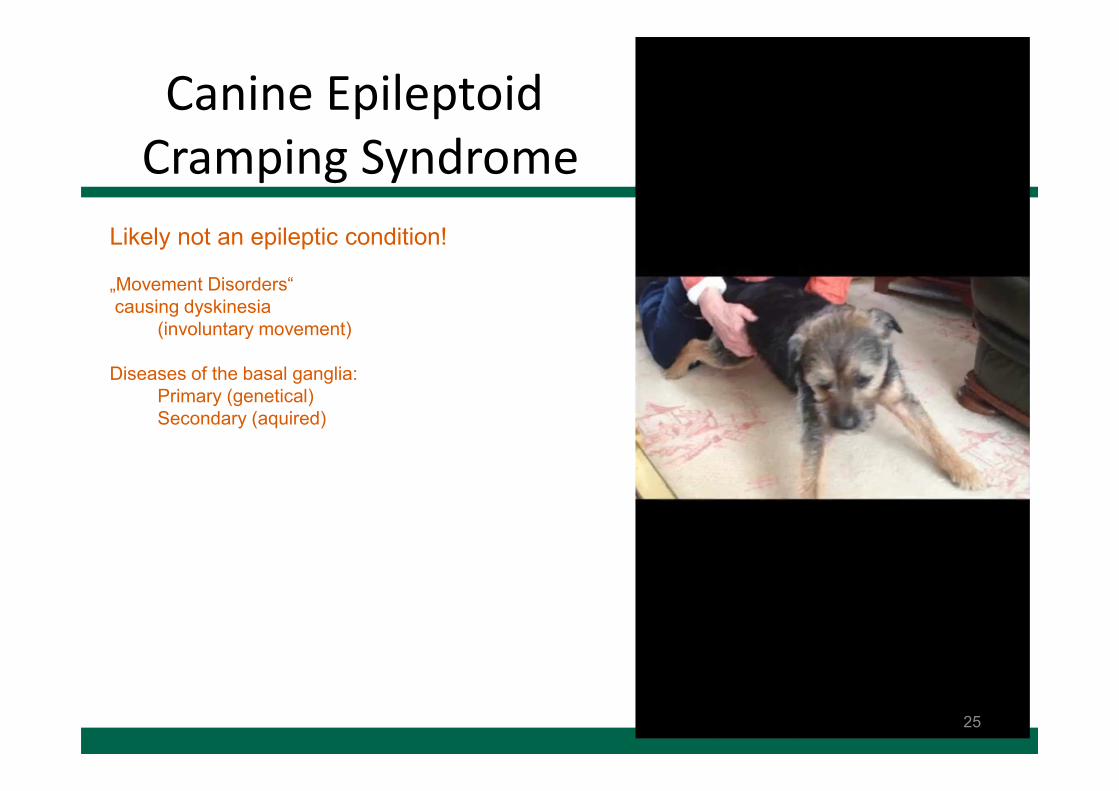
Canine EpileptoidCramping Syndrome
25
Likely not an epileptic condition!
„Movement Disorders“
causing dyskinesia
(involuntary movement)
Diseases of the basal ganglia:
Primary (genetical)
Secondary (aquired)
Epilepsziás roham?
A.Pakozdy
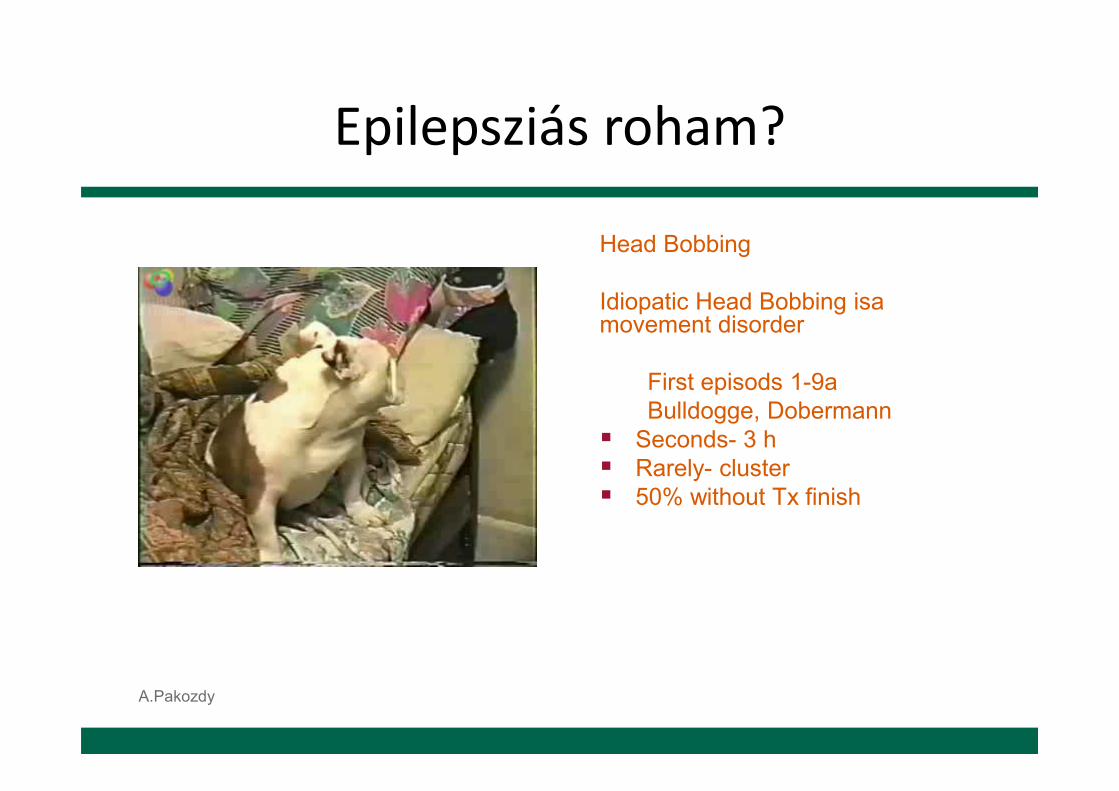
Head Bobbing
Idiopatic Head Bobbing isamovement disorder
First episods 1-9a
Bulldogge, Dobermann
� Seconds- 3 h
� Rarely- cluster
� 50% without Tx finish

Epilepsziás roham?
27
Episodic Falling in Cavalier King Charles Spaniel (CKCS) „Hyperekplexia“
Genetic disease
(autosomal recessive)
� Episodic
� Stiffness/falling
� No autonomic signs
� No consciousness change
� Stress/exercise induced
� First episodes 2mo-5a
� GEN: BCAN mutation?
� Therapy:
� Clonazepam 0.5mg/kg tid
� Azetasolamid

Epilepsziás roham?
28
Scottie cramp
Genetic disease
� Episodic stiffness
� Stress/execice induced
� Kyphosis
� May progress into rigidity
� No consciousness change
� First episodes under 1a
� Therapy:
� Diazepam
� Acepromazin
� Fluoxetine

Epilepsziás roham?
• Chinook seizure(Hereditary idiopathic paroxysmal dyskinesia)
� Autosomal recessive
� Episods starts 2m-5a
� 1-60min, rarely-cluster
� Limbs in flexion mild movement
� Sometimes convulsive episodes too
� Therapie: not known
29

Epilepsziás roham?
• Degenerative Encephalopathy in Nova ScotiaDuck Tolling Retriever with REM Sleep Disorder(Barker et al. 2016)
• N=9, onset 2mo-5y, progressive
• Increased movement during sleep
• Noise phobias, gait abnormalities
• Neuroexam: tetraparesis, tremor, ataxia
• MRI caudate nuclei cavitation
• Histo: Malacia of CN and dystrophy in brainstemand spinal cord
– Barker et al. 2016
30

Epilepsziás roham?
31
Increased startle reaction
� Congenital
� Aquired
� Therapy:
� Clonazepam, Levetiracetam
Progressive myoclonus epilepsyin beagle (Lafora Disease)
� Congenital disease of glykogen metabolism
EPM2A or NHLRC1 mutation
� Therapy:
� Phe, KBr, Levetiracetam
� Diet (carbonhydratereduced, antioxidants)

Epilepsziás roham?
32

Epilepsziás roham?
33
Seppala et al. 2011
LGI2 Truncation Causes a Remitting Focal Epilepsy in Dogs
Benigne familial juvenile
epilepsy (BFJE) in Lagotto
romagnolo dogs
whole-body tremor
autosomal recessive
inheritance
Onset 6-7 weeks
Spontaneous remission
Nonsense mutation in
the LGI2 gene

Epilepsziás roham?
Clinical signs in ChiariMalformation• Subclinical
• Cervikal pruritus (most frequent)
• cerebrale
• cerebellare
• Brainstamm
• Cervikal– Tetraparesis
– Monoparesis
– Hyperaesthesia

Neuro.1-JGT
� Chiari I Malformation
� Caudale Occipitale
Malformation

Patophysiologia: Chiari Malformation
• „Overgrowding“ von FossaCaudalis – dynamic druckchange
• Cerebellar herniation throughForamen Magnum
• Secondary hydrocephalus
• Hydromyelia in cervikal region(rarely more caudal)
• Cavalier King Charles Spaniel
• Yorkshire/Maltese/Pekinese

Therápia: ChiariMalformation
• On demand:– Prednisolon 0,5mg/kg/nap– Gabapentin 5-10mg/kg TID– Pregabalin 3-4mg/kg TID– Omeprazol 0,5 mg/kg SID– NSAID
• Meloxicam (Metacam)• Carprofen (Rimadyl)• Fibrocoxib (Previcox)
– Other painkillers
• Fentanyl patch– Furosemid– May be:
– Ketamin– Amytriptilin
– Operation
37

Epilepsziás roham?
38

Epilepsziás roham?
39
Generalized myoclonic epilepsy in Rhodesian Ridgeback
� Myoclonus (sudden, brief involuntary contraction)
� Onset 6Weeks-18Mo
� Myoclonus trunk, proximal limb, cervicalmuscles
� May progress into GTCS
� Photosensitivity
� EEG 4-5Hz SW
� DIRAS1 gen (AcCh)
� MR: ventricle assymetria
� Histo: WNL
� Therapy:
� LEV, KBr the best
� Wielaender et al. 2017

40

Epilepsziás roham?
41
Painful orthopedic disorders, are rare differentials

Az epilepsziák etiológiája• Idiopáthiás epilepszia
– Functional disease – no „great“ structural changes
• Strukturális epilepsziák– Intracranial disorders (VITAMIND)
• Vascular (Ischemia, haemorrhage)• Inflammatory (Infect): distemper, FSME, bakterial, cryptococc)• Inflammatory (non-infect) (GME, NME, NLE, EME)• Traumatic• Anomalia: hydrocephalus, Chiari-Malformation, Supracollicular cyst• Neoplastic• Degenerative (storage disease, genetic disease)
– Extracranial disorders (reaktiv epilepsziás rohamok)• Hypoglycaemia• Hepatic encephalopathy: PSS, cirrhosis/fibrosis• Renale Encephalopathy• Electrolyte disturbances (Hypocalcaemie, Hypernatraemie)• Intoxication (Carbamat, organophosphat, metaldehyd etc)• Hypoxia/hypoxaemia/anaemia• Erythrocytosis/leucocytosis/thrombocytosis
• Kryptogén epilepszia/Epilepsy of unknown origin– Lesion strongly suspected, but no lesion can be confirmed– After head trauma, post-anaesthesia, post-encephalitis
A.Pakozdy

Az epilepsziák etiológiája
• Idiopathic epilepsy (kizárásos diagnózis)– Genetic cause confirmed
• Lagotto Romagnolo LGI2• Belgischer Schäffer ADAM23• Rhodesian Ridgback DIRAS
– Genetic cause suspected (family historyKlick, breed, age)– Unklarer Genese
• Strukturális epilepszia– Intracranial causes (VITAMIND)
A.Pakozdy

Saját eredmények (Pakozdy et al. 2008)
Ursache der Krampfanfälle beim Hund
Ano
mal
ie; 1
0D
egene
rativ
; 9
Hyp
ogly
käm
ie; 7
Vas
cula
r; 7
Traum
a; 3U
räm
ie; 3
prim
äre E
pile
psie; 1
15
Neopla
sie;
39
Enz
ephal
itis;
23
Toxico
se; 9
Hep
athoen
zeph
.; 8
ande
re E
xtra
crani
al; 5
Ele
ctro
lytv
ersc
hieb.;
2
0
20
40
60
80
100
120
1
A.Pakozdy

Idiopáthiás epilepszia(ák)
Genetic factors
– Breed predisposition• Beagle (1968)
• Golden Retriever (1994)
• Labrador Retriever (1997)
• Tervueren (1997)
• Berner Sehnenhund (1998)
• Mischlinge (1998)
• Vizsla (2003)
• Border Collie (2009)!
– Well controlled with therapy (80%)
– 1. seizure (6Mo-6 Jahre)
A.Pakozdy

46
Ekenstedt
et al. 2012

Idiopathic vs structural epilepsy
Croft
(1965)
n=260
Jaggy
(1998)
n=235
Pakozdy
(2008)
n=240
Idiopathisch 64% 53% 48%
Symptomatisch 36% 47% 52%

IE versus SE
• Anamnézis: milyen a roham?– Epilepsziás vagy nem epilepsziás?
– Focal seizure is more frequent in focal brain disease(3.25times more frequent in SE)
– Status epilepticus (2.16times more frequent in SE)
– Cluster Anfall (1.57times more frequent in SE)
– Seizures in sleep (3.2times more frequent in IE)
A.Pakozdy

További kivizsgálás?
• Blood work + urinalysis is routine
• CT/MRT
• Liquor
• EEG
• Genetic tests?A.Pakozdy

Vérvizsgálat
• HK ↕• Leucocytes↕• Glucose• Azotaemia (creatinine, BUN)• Hepathopathy (bile acid, ammonia)• Na• Ca• Hyper/Hypo-osmolarity• Acidosis-Alkalosise• Urinalysis (haemolysis, haematurie, glucosuria, gravity)
A.Pakozdy

További kivizsgálás
• MR/CT – Anomalia
• Hydrocephalus• Chiari-Malformation
– Lesions (focal structural change)• Granuloma (GME)• Neoplasia• Bleeding• Ischaemia• Cysts
• Liquor– Meningitis– Meningoencephalitis– Neoplasia– Bleeding
• Serum– Phenobarbital (20-40μg/ml = 86-173 μmol/l)– KBr (1000-3000 μg/ml = 1-3mg/ml = 100-300mg/dl)
A.Pakozdy

MRI
A.Pakozdy

MRI
53

MRI
A.Pakozdy

55

CT
A.Pakozdy

Liquor citológia
A.Pakozdy

Liquor citológia
A.Pakozdy

EEG kutyán és macskán
• Tisztázható, hogy a roham epielsziás? (ritkán 10-65% )
• Tisztázható az etiológia (nem, nincs etiológia specifikus mintázat)
• Fontos-e a terápia szempontjából hogy generalizált vagy fokális (nem)
• Van prognosztikai jelentősége? (nincs)
• A gyakorlati haszna kevés
A.Pakozdy

EEG

EEG
61

Terápia I.
• Cél: rohm csökkentés, QoL, mellékhatások – (ritka a rohammentesség, Fe!))– Gyakoriság– Súlyosság– Tartam
• Mikor kezdjük a kezelést?– Individuális döntés
• Fő faktorok– Status epilepticus fordult elő, melynek kiváltó oka ismeretlen– Strukturális epilepsziában, amely nem gyógyítható– Ismételt rohamok 2-6 havonta– Kluster rohamok 12 hónapon belül– Súlyos posztiktális tünetek– Fej trauma után 1 héten belül jelentkező rohamok
• Befolyásoló faktorok– Realitás? (Tulaj?, macska? költség?, monitoring?)– Súlyosbító (sérülésveszély, apnoe, ccianózis, hányás)
– Általában élethosszig!
A.Pakozdy

Terápia II. (Podell et al. 2015)
63

Terápia III.
• Fenobarbital– 2-5mg/kg BID per os
– GABA agonist, Ca channal blockink
– T1/2: 40-90hrs
– Cél: antiepilepsziás hatás a terápiás sávban 20-40µg/ml
– Szérumszint – 3-4 héttel a terápiakezdés után (6 havonta)
– Mellékhatások: sedation, ataxia, paraparesis, PU/PD hepatic enzymes inducing (not in cats!)
– Ritkán: cirrhosis, necr. pankreatitis, bone marrowsupression↓
A.Pakozdy

Therápia IV.• Imepitoin
– New antiepileptic drug (2013)
– Developed for veterinary use
– Imidazol derivate
– Benzodiazepine agonist (partial, low-affinity)
– Experimental and clinical data
– Löscher et al. 2004: n=111, 10mg/kg bid up to 30mg/kg bid compared withphenobarbital (n=44)
– Duration 6-7mo
– Similar efficay than phenobarbital less adverse effects
– Rieck et al. 2006: Effective and less adverse effect than phe
65

Terápia V.
• 2. Brom (Kaliumbromid/NatriumBromid)– If Phe/Ime resistent seizures– „add on“ oder MonoTx– Cl- (Hyperpolarisation)– 20-40 mg/kg BID po– Serum: 1-3mg/ml
– T 1/2: 24 days!!! (Cat: 10T)– Renal elimination– Steady state in 80-120 days (cats: 40-50T)– Adverse effects: „bromism“, vomiting, paraparesis,
pancreatitis, pruritus, cat- bronchitis– Loading-Dosis: 400-600mg/kg within 24 h
A.Pakozdy

Prognózis idiopatikus epilepsziában
• Jól kontrollált:
– 70-80% (2-6 roham/év)
– Enyhe mellékhatások (compliance)
• Élethosszig tartó kezelés
– Ha az okot sikeről megszűntetni
– Hosszú rohammentesség (0.5-3 év)
• Hirtelen megvonás veszélyes (St epilepticus, Imepitoin?)
A.Pakozdy

Mi tehetünk a terápiarezisztens esetekért?
• Therapieresistent– ca. 20% in IE
• Serum concentration
• Diagnosis?
• Add on Therapie with second-line drugs
• Ketogenic diet? (GABA increasing)
• Stimulation of vagal nerve (costs)
A.Pakozdy

Phenobarbital 3times daily? (Stabile et al. 2017)
• N=10 dogs
• PHE tid instead of bid (daily dose similar)
– tid 8-16mg/kg/Tag <- bid 7-16mg/kg/Tag
• Response
– 9/10 dogs
– 8/10 3times longer interictal period
• Effective in dogs with very short T1/2
(below 20 hrs)
69

Imepitoin and Phenobarbital (Royaux et al.
2017.)
• N=27 refractory IE on IME 30mg/kg bid
• 14 Hunde PHE add-on - 13 Hunde KBr add-on
• Responders: 79% - 69%
• Adverse effects: acceptabel PU/PD/PP, sedation
• Seizure frequency/mo– 4.25->1.6 3.5-
>0.5
70

Halálokok IE
Alive 81Chronic renal failure 1
Status epilepticus 3 Demencia 1
Refractory seizures 3 Lymphoma 1
Hepatic cirrhosis 2 Pleuritis 1
Necrotising pankreatitis 2 Arthrosis 1
Gastrointestinal signs 1 Chronic otitis 1
Liver carcinoma 1Cardiacinsufficiency 1
A.Pakozdy
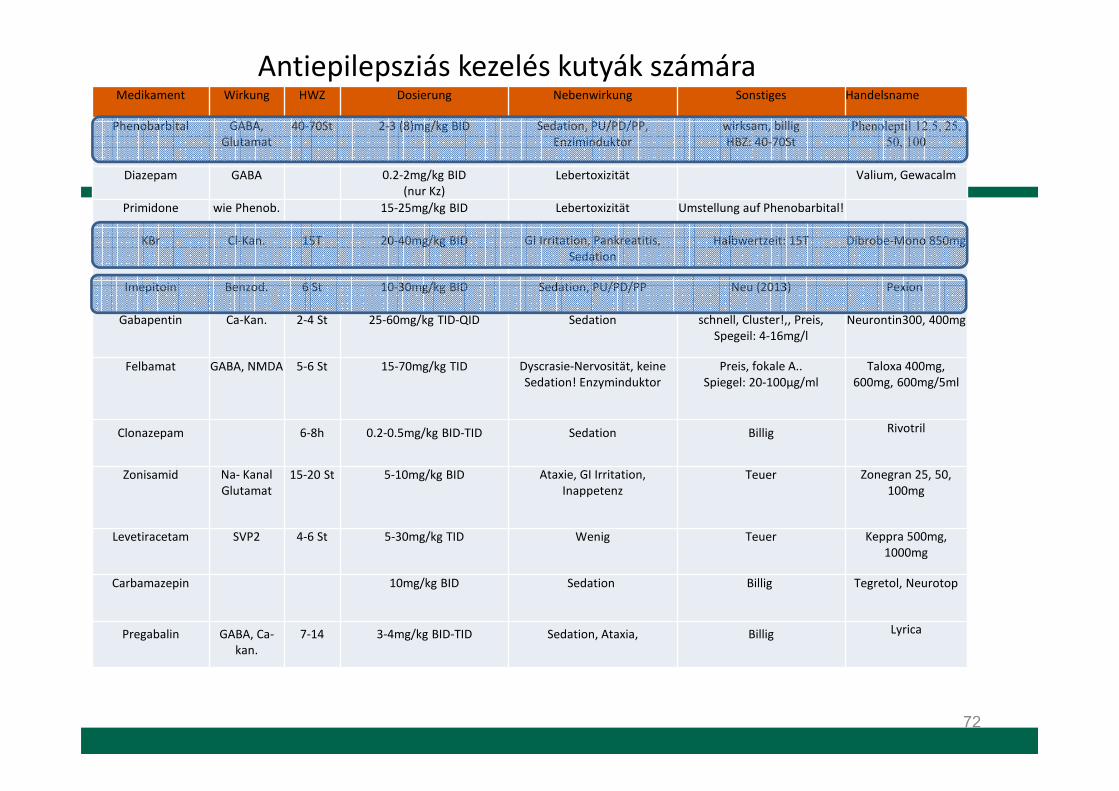
Antiepilepsziás kezelés kutyák számára
72
Medikament Wirkung HWZ Dosierung Nebenwirkung Sonstiges Handelsname
Phenobarbital GABA, Glutamat
40-70St 2-3 (8)mg/kg BID Sedation, PU/PD/PP, Enziminduktor
wirksam, billigHBZ: 40-70St
Phenoleptil 12.5, 25,
50, 100
Diazepam GABA 0.2-2mg/kg BID(nur Kz)
Lebertoxizität Valium, Gewacalm
Primidone wie Phenob. 15-25mg/kg BID Lebertoxizität Umstellung auf Phenobarbital!
KBr Cl-Kan. 15T 20-40mg/kg BID GI Irritation, Pankreatitis, Sedation
Halbwertzeit: 15T Dibrobe-Mono 850mg
Imepitoin Benzod. 6 St 10-30mg/kg BID Sedation, PU/PD/PP Neu (2013) Pexion
Gabapentin Ca-Kan. 2-4 St 25-60mg/kg TID-QID Sedation schnell, Cluster!,, Preis, Spegeil: 4-16mg/l
Neurontin300, 400mg
Felbamat GABA, NMDA 5-6 St 15-70mg/kg TID Dyscrasie-Nervosität, keine Sedation! Enzyminduktor
Preis, fokale A..Spiegel: 20-100μg/ml
Taloxa 400mg, 600mg, 600mg/5ml
Clonazepam 6-8h 0.2-0.5mg/kg BID-TID Sedation Billig Rivotril
Zonisamid Na- KanalGlutamat
15-20 St 5-10mg/kg BID Ataxie, GI Irritation, Inappetenz
Teuer Zonegran 25, 50, 100mg
Levetiracetam SVP2 4-6 St 5-30mg/kg TID Wenig Teuer Keppra 500mg, 1000mg
Carbamazepin 10mg/kg BID Sedation Billig Tegretol, Neurotop
Pregabalin GABA, Ca-kan.
7-14 3-4mg/kg BID-TID Sedation, Ataxia, Billig Lyrica
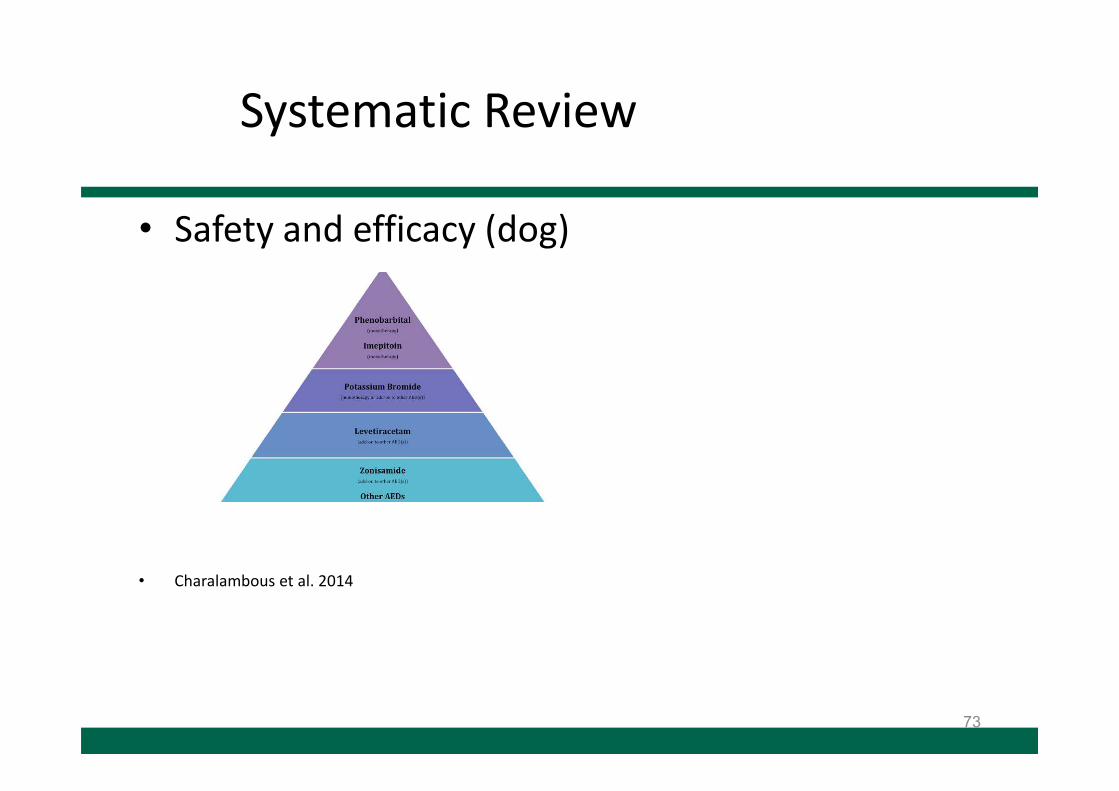
Systematic Review
• Safety and efficacy (dog)
• Charalambous et al. 2014
73

Macska: Epilepsziás rohamok

Anfälle bei KatzenParoxysmal events Important features for differentiation
Generalized epileptic seizure Complex motor episodes or/with tonic-clonic
seizure with impaired consciousness
Focal epileptic seizure Very variable, may include drooling, vocalization,
abnormal head and limb movement (secondary
generalization possible)
Temporal lobe seizure
(FEPSO)
Orofacial automatism: salivation, facial twitching, lip
smacking, chewing, licking, swallowing (secondary
generalization possible)
Feline audiogenic reflex seizure
(FARS)
Late onset, myoclonic seizures, can be triggered by
high-frequency sound
Neuromuscular collapse Exercised-induced
Cardiac syncope Arrhythmia, Evidence of heart disease
Neck pain Pain on neck manipulation
Compulsive disorders No loss of consciousness
Feline estrus behavior Howling, rolling, lordosis
Vestibular disease Nystagmus, Head tilt, Falling
Increased intracranial pressure No sudden start and termination
Feline orofacial pain syndrome
(FOPS)
Acute oral discomfort and automutilation
Feline hyperesthesia syndrome
(FHS)
Rolling skin on the lumbal region, (unclear etiology,
may be epileptic)

Macska epilepsziás roham?FEPSO (Feline Partial Seizure withOrofacial Involvement)
• Clinical signs:– Episodic facial twiching, mastication– Swallowing– Lip smacking
• Etiology– Epileptic activity within the temporallobe due to different etiology
Pakozdy et al. 2010

Macska epilepsziás roham?
FOPS(Feline Orofacial Pain Syndrome) Mainly in Burmese catsAny age• Clinical signs:
– Episodic oral discomfort, tonguemutilation
– Usually unilateral– Triggers: mouth
movements/eating/stress• Possible etiology
– History of oral lesions– Sensitisation of trigeminal nerve
• Treatment:
– Dental care– Phenobarbital/Diazepam– NSAID– Corticosteroids– Tricyclic antideppressants
• Amitripriptyline– Enviromental stress reduction
Rusbridge et al 2010

Macska epilepsziás roham?FHS(Feline Hyperaesthesia Syndrome)• Well-known phenomenon• Unclear entity• Clinical signs:
– Episodic twiching, rolling skin over the lumbar area– Agitation, agression– Licking or biting of the flank, back, tail– Several times daily
• Possible etiology– Epileptic seizure?– Obsessive-compulsive disorder?– Myopathy?– Previous dermatitis?– Spinal cord or nerve compression?– Intracranial disease?– May be heterogenous etiology
• Treatment:
– Corticosteroid/NSAID (initial)– Flea control– Tricyclic antidepressants
• Amitripriptyline 2mg/kg sid• Clomipramine 1-5mg/ca sid-bid
– SSRI• Fluoxetine 0.5-4mg/cat sid• Paroxetine 0.5mg/kg sid
– Antiepileptic drugs– Enviromental stress reduction
Bagley and Platt 2013

Macska epilepsziás roham?
FARS(Feline Audiogenic Reflex Seizures)Late onset (median 15 years)
• Clinical signs:– Myoclonic episodes– Triggered by high-frequency sound– Usually non-progressive– Hearing impairment (50%)
• Possible etiology– Unknown– degenerative
• Treatment:
– Levetiracetam 20-25mg/kg tid
– Phenobarbital 3-5mg/kg bid
Lowrie et al. 2015

Macska epilepsziás roham?
Syncope
– High grade atrioventricular dysfunction
Penning et al 2009

Etiology of epileptic seizures
Idiopathic Epilepsy
Structural Epilepsy
Reactive epileptic seizures
Unknown origin
IVETF 2015

Van idiopathikus epilepszia macskán!
• Schwartz-Porsche (1989)• Idiopathic Epilepsy 59%
(n=42?)• Rusbridge (2005)
• Idiopathic Epilepsy 54%(n=?)
• Schriefl et al. (2008)• Idiopathic Epilepsy 25%
(n=91)• Pakozdy et al. (2010)
• Idiopathic Epilepsy 37% (n=125)
• Wahle et al. (2014)• EUC 22%
(n=81)
Raimondi et al (2017)• Idiopathic Epilepsy 88%
(n=188)
• Quesnel et al. (1997)Idiopathic Epilepsy 0%
(n=30)

Etiology– Cats (Pakozdy et al. 2010)
A.Pakozdy

Hippocampale Necrosis
Fatzer et al. 2000• n=38• 1-6a• Clinical signs:
– Complex partial seizures - usually– Cluster, status epilepticus - usually– Behavioural changes - frequently– Therapyresistant/fatal
• Histopathology: degeneration+inflammation– Hippocampus>L.piriformis– Gyrus dentatus , CA large pyramidal cells– Shrunken, ischemic neuron, central chromatolysis, with
eccentric pyknotic nucleus, capillary proliferation– Perivascular lymphoid infiltration– Microgliosis, astrocytosis– Neuronal loss + fibrillary astrocytes
• Etiology:– Probably toxic?

MRI in hippocampale necrosis
• Schmied (2008)
• n=4
• Clinical signs:– acute generalized/focal seizures
– behavioural changes• aggression, hypersalivation, polyphagia
• MRI:– T2 hyper, T1 hypointense
– Histology: necrosis in hippocampus/l. piriformis

Clinical work-up
• Complex Partial Cluster Seizures in Cats with Orofacial Involvement
(FEPSO)
• Adult otherwise healthy cats!• Fever 5/17!
» Pakozdy et al. J Fel Med Surg 2011

Clinical work-up II.
• Pathological changes:– In hippocampus most severe (11)
– Neuronal loss (necrosis)
– Gliosis (sclerosis)
– Vascular sprouting (inflammation)

HN/HS ist not an etiological category
(Klang et al. 2015)
Category Disease/Etiology References
Vascular Stroke, Hypoxia, Ischemia, Anesthetic procedure
Schmid-Kastner et al. 1990Jurk et al 2001Altay et al 2011
Inflammatory Limbic encephalitis, FIV Mitchell et al. 1999Pakozdy et al 2013
Toxic Jodoxychinolin, Kainic acid Tanaka et al. 1982
Anomaly Dentate gyrus dysgenesis Klang et al. 2015
Idiopathic Unknown Pakozdy et al. 2014
Neoplastic Brain neoplasia Vanhaesebrouck et al. 2012
Seizure itself may cause HS/HN Fors et al. 2015

Antiepilepsziás terápia macskák számára
Treat underlying disease when present!
Corticosteroid can be beneficial in the acute stage of Limbic encephalitis

Imepitoin (Pexion) for cats too?(2017 Odilo et al.)
• 30 control cats received Imepition BID 30, 40 or 80 mg/kg for 30 days
• Sporadical vomiting
• 8 epileptic cats (IE) Imepitoin BID 30 mg/kg for 30 days.
– 4 seizurefree over 8 Wo
– Side effects: apathia, inappetence, vomiting only at the beginning

Outcome in idiopathic epilepsy in cats
• High seizure-freedom!
– 40-50% Pakozdy et al. 2012
– 44% Wahle et al. 2014
• Therapy finish cause recurrence
• Resistent cases occur!

Köszönöm a figyelmet!
Aknowledgement: radiology, Zlab, colleagues, owners, patients!

Literatur
•
•
• Berendt, M; Farquhar, RG; Mandigers, PJ; Pakozdy, A; Bhatti, SF; De Risio, L; Fischer, A; Long, S; Matiasek, K; Muñana, K; Patterson, EE; Penderis, J; Platt, S; Podell, M; Potschka, H; Pumarola, MB; Rusbridge, C; Stein, VM; Tipold, A; Volk, HA. International veterinary epilepsy task force consensus report on epilepsy definition, classification and terminology in companion animals. BMC Vet Res. 2015; 11(1):182
•
• Bhatti, SF; De Risio, L; Muñana, K; Penderis, J; Stein, VM; Tipold, A; Berendt, M; Farquhar, RG; Fischer, A; Long, S; Löscher, W; Mandigers, PJ; Matiasek, K; Pakozdy, A; Patterson, EE [and 5 others](2015): International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Vet Res. 2015; 11(1):176
•
• De Risio, L; Bhatti, S; Muñana, K; Penderis, J; Stein, V; Tipold, A; Berendt, M; Farqhuar, R; Fischer, A; Long, S; Mandigers, PJ; Matiasek, K; Packer, RM; Pakozdy, A; Patterson, N [and 6 others] (2015): International veterinary epilepsy task force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Vet Res. 2015; 11(1):148
•
•
93