ensure a brighter future
TRANSCRIPT
ENSURE A BRIGHTER FUTURECARLISLE FAMILY YMCA2021-22 SACC Program Enrollment Packet
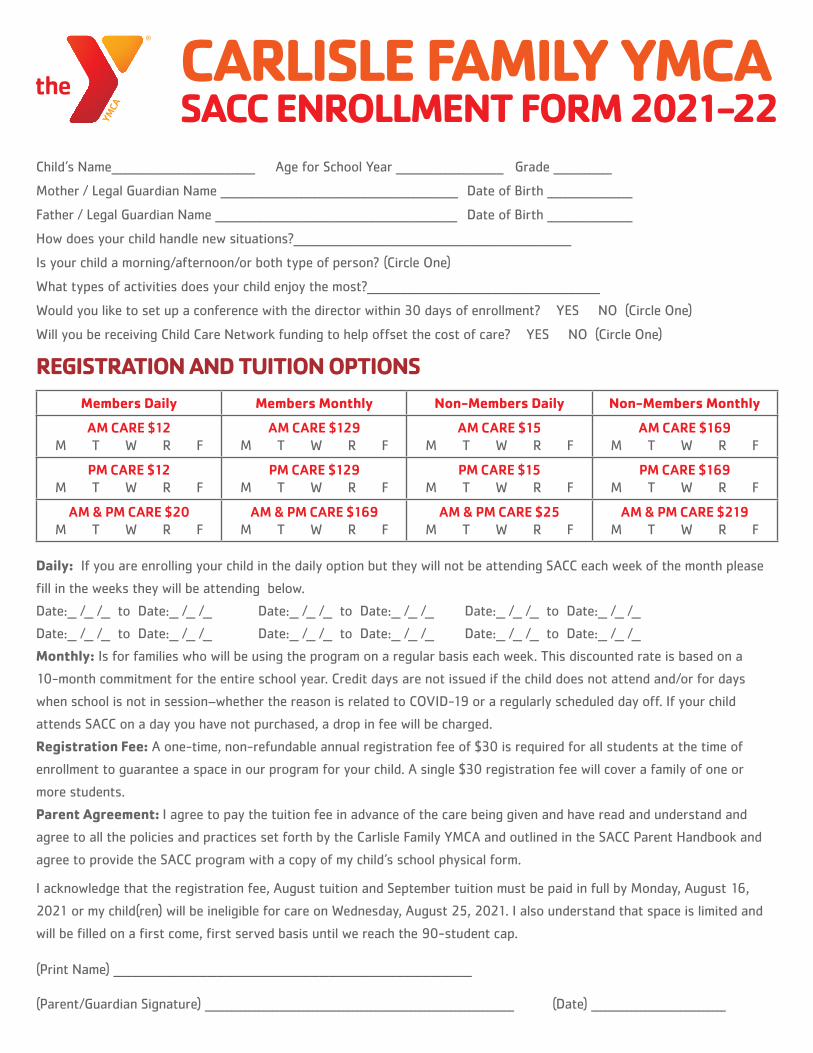
CARLISLE FAMILY YMCA SACC ENROLLMENT FORM 2021-22
Child’s Name________________________________ Age for School Year ________________________ Grade _____________
Mother / Legal Guardian Name _____________________________________________________ Date of Birth ___________________
Father / Legal Guardian Name ______________________________________________________ Date of Birth ___________________
How does your child handle new situations?______________________________________________________________
Is your child a morning/afternoon/or both type of person? (Circle One)
What types of activities does your child enjoy the most?____________________________________________________
Would you like to set up a conference with the director within 30 days of enrollment? YES NO (Circle One)
Will you be receiving Child Care Network funding to help offset the cost of care? YES NO (Circle One)
REGISTRATION AND TUITION OPTIONSMembers Daily Members Monthly Non-Members Daily Non-Members Monthly
AM CARE $12M T W R F
AM CARE $129M T W R F
AM CARE $15M T W R F
AM CARE $169M T W R F
PM CARE $12M T W R F
PM CARE $129M T W R F
PM CARE $15M T W R F
PM CARE $169M T W R F
AM & PM CARE $20M T W R F
AM & PM CARE $169M T W R F
AM & PM CARE $25M T W R F
AM & PM CARE $219M T W R F
Daily: If you are enrolling your child in the daily option but they will not be attending SACC each week of the month please
fill in the weeks they will be attending below.
Date:__ /__ /__ to Date:__ /__ /__ Date:__ /__ /__ to Date:__ /__ /__ Date:__ /__ /__ to Date:__ /__ /__
Date:__ /__ /__ to Date:__ /__ /__ Date:__ /__ /__ to Date:__ /__ /__ Date:__ /__ /__ to Date:__ /__ /__
Monthly: Is for families who will be using the program on a regular basis each week. This discounted rate is based on a
10-month commitment for the entire school year. Credit days are not issued if the child does not attend and/or for days
when school is not in session–whether the reason is related to COVID-19 or a regularly scheduled day off. If your child
attends SACC on a day you have not purchased, a drop in fee will be charged.
Registration Fee: A one-time, non-refundable annual registration fee of $30 is required for all students at the time of
enrollment to guarantee a space in our program for your child. A single $30 registration fee will cover a family of one or
more students.
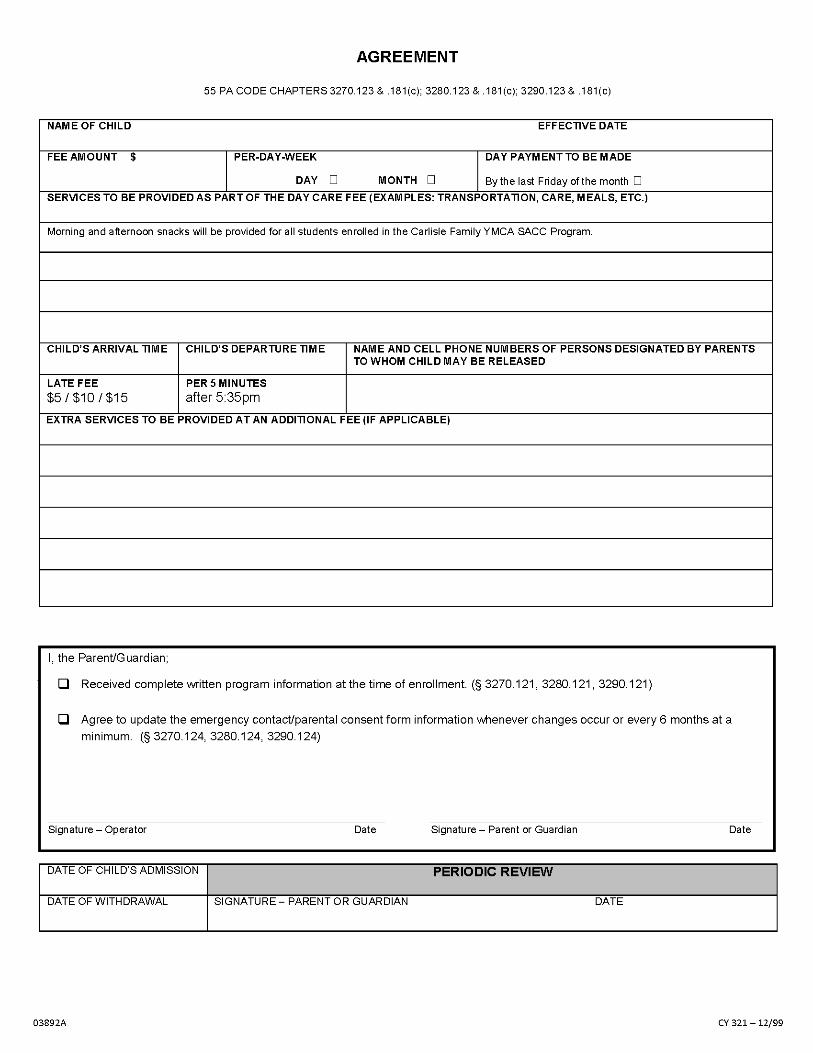
Parent Agreement: I agree to pay the tuition fee in advance of the care being given and have read and understand and
agree to all the policies and practices set forth by the Carlisle Family YMCA and outlined in the SACC Parent Handbook and
agree to provide the SACC program with a copy of my child’s school physical form.
I acknowledge that the registration fee, August tuition and September tuition must be paid in full by Monday, August 16,
2021 or my child(ren) will be ineligible for care on Wednesday, August 25, 2021. I also understand that space is limited and
will be filled on a first come, first served basis until we reach the 90-student cap.
(Print Name) ________________________________________________________________________________ (Parent/Guardian Signature) _____________________________________________________________________ (Date) ______________________________
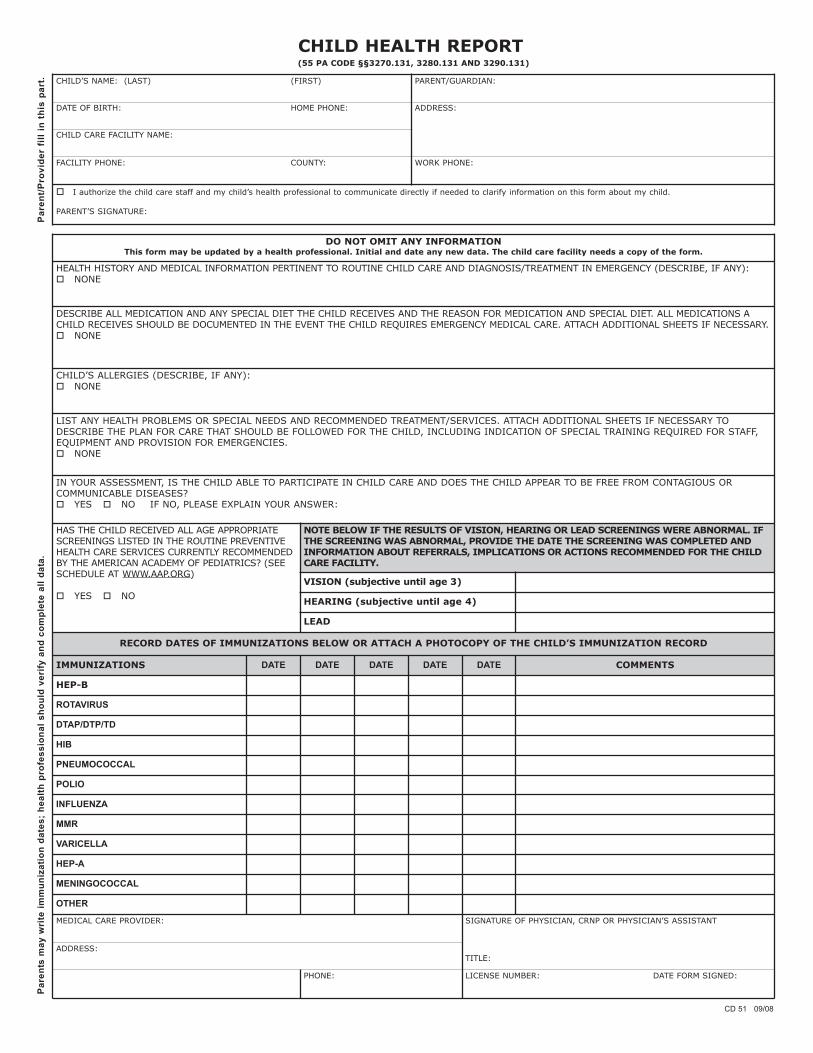
CHILD HEALTH REPORT (55 PA CODE §§3270.131, 3280.131 AND 3290.131)
Pare
nt/P
rovi
der
fill i
n th
is p
art. CHILD’S NAME: (LAST) (FIRST) PARENT/GUARDIAN:
DATE OF BIRTH: HOME PHONE: ADDRESS:
CHILD CARE FACILITY NAME:
FACILITY PHONE: COUNTY: WORK PHONE:
� I authorize the child care staff and my child’s health professional to communicate directly if needed to clarify information on this form about my child.
PARENT’S SIGNATURE:
Pare
nts
may
wri
te im
mun
izat
ion
date
s; h
ealth
pro
fess
iona
l sho
uld
veri
fy a
nd c
ompl
ete
all d
ata.
DO NOT OMIT ANY INFORMATION This form may be updated by a health professional. Initial and date any new data. The child care facility needs a copy of the form.
HEALTH HISTORY AND MEDICAL INFORMATION PERTINENT TO ROUTINE CHILD CARE AND DIAGNOSIS/TREATMENT IN EMERGENCY (DESCRIBE, IF ANY): � NONE
DESCRIBE ALL MEDICATION AND ANY SPECIAL DIET THE CHILD RECEIVES AND THE REASON FOR MEDICATION AND SPECIAL DIET. ALL MEDICATIONS A CHILD RECEIVES SHOULD BE DOCUMENTED IN THE EVENT THE CHILD REQUIRES EMERGENCY MEDICAL CARE. ATTACH ADDITIONAL SHEETS IF NECESSARY. � NONE
CHILD’S ALLERGIES (DESCRIBE, IF ANY): � NONE
LIST ANY HEALTH PROBLEMS OR SPECIAL NEEDS AND RECOMMENDED TREATMENT/SERVICES. ATTACH ADDITIONAL SHEETS IF NECESSARY TO DESCRIBE THE PLAN FOR CARE THAT SHOULD BE FOLLOWED FOR THE CHILD, INCLUDING INDICATION OF SPECIAL TRAINING REQUIRED FOR STAFF, EQUIPMENT AND PROVISION FOR EMERGENCIES. � NONE
IN YOUR ASSESSMENT, IS THE CHILD ABLE TO PARTICIPATE IN CHILD CARE AND DOES THE CHILD APPEAR TO BE FREE FROM CONTAGIOUS OR COMMUNICABLE DISEASES? � YES � NO IF NO, PLEASE EXPLAIN YOUR ANSWER:
HAS THE CHILD RECEIVED ALL AGE APPROPRIATE SCREENINGS LISTED IN THE ROUTINE PREVENTIVE HEALTH CARE SERVICES CURRENTLY RECOMMENDED BY THE AMERICAN ACADEMY OF PEDIATRICS? (SEESCHEDULE AT WWW.AAP.ORG)
� YES � NO
NOTE BELOW IF THE RESULTS OF VISION, HEARING OR LEAD SCREENINGS WERE ABNORMAL. IF THE SCREENING WAS ABNORMAL, PROVIDE THE DATE THE SCREENING WAS COMPLETED AND INFORMATION ABOUT REFERRALS, IMPLICATIONS OR ACTIONS RECOMMENDED FOR THE CHILD CARE FACILITY.
VISION (subjective until age 3)
HEARING (subjective until age 4)
LEAD
RECORD DATES OF IMMUNIZATIONS BELOW OR ATTACH A PHOTOCOPY OF THE CHILD’S IMMUNIZATION RECORD
IMMUNIZATIONS DATE DATE DATE DATE DATE COMMENTS
HEP-B
ROTAVIRUS
DTAP/DTP/TD
HIB
PNEUMOCOCCAL
POLIO
INFLUENZA
MMR
VARICELLA
HEP-A
MENINGOCOCCAL
OTHER
MEDICAL CARE PROVIDER:
ADDRESS:
PHONE:
SIGNATURE OF PHYSICIAN, CRNP OR PHYSICIAN’S ASSISTANT
TITLE:
LICENSE NUMBER: DATE FORM SIGNED:
CD 51 09/08
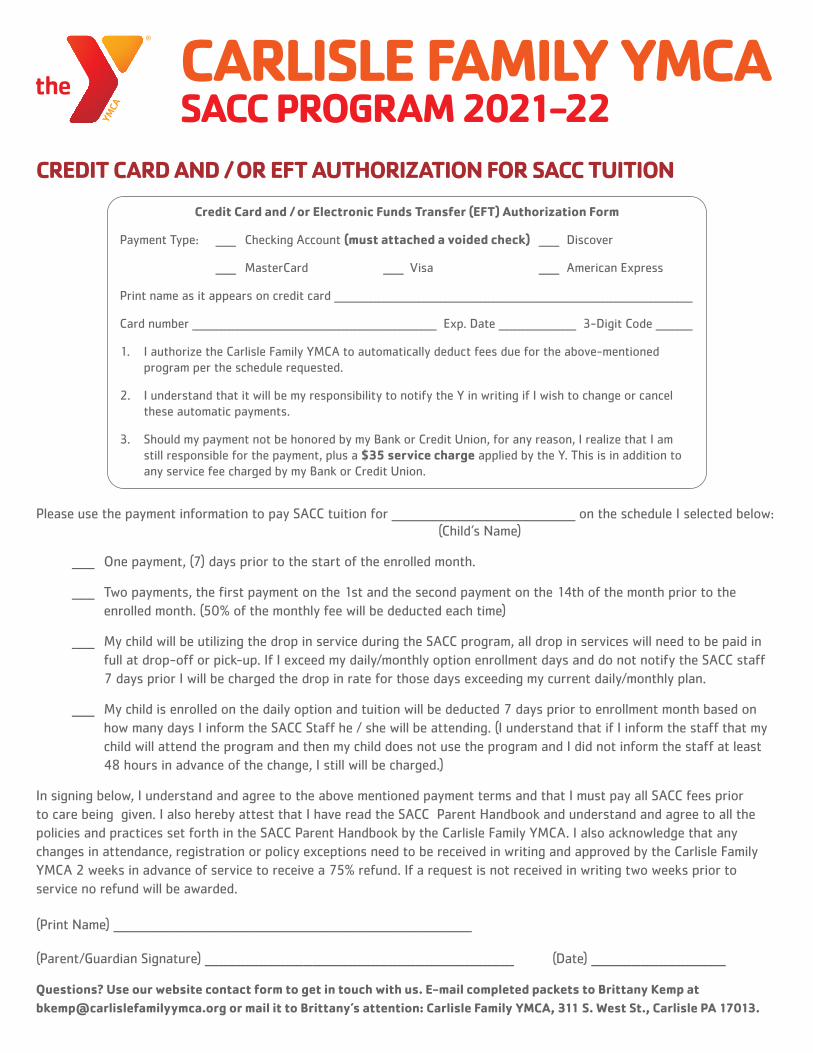
CARLISLE FAMILY YMCA SACC PROGRAM 2021-22
Please use the payment information to pay SACC tuition for _________________________________________ on the schedule I selected below: (Child’s Name)
_____ One payment, (7) days prior to the start of the enrolled month.
_____ Two payments, the first payment on the 1st and the second payment on the 14th of the month prior to the enrolled month. (50% of the monthly fee will be deducted each time)
_____ My child will be utilizing the drop in service during the SACC program, all drop in services will need to be paid in full at drop-off or pick-up. If I exceed my daily/monthly option enrollment days and do not notify the SACC staff 7 days prior I will be charged the drop in rate for those days exceeding my current daily/monthly plan.
_____ My child is enrolled on the daily option and tuition will be deducted 7 days prior to enrollment month based on how many days I inform the SACC Staff he / she will be attending. (I understand that if I inform the staff that my child will attend the program and then my child does not use the program and I did not inform the staff at least 48 hours in advance of the change, I still will be charged.)
In signing below, I understand and agree to the above mentioned payment terms and that I must pay all SACC fees prior to care being given. I also hereby attest that I have read the SACC Parent Handbook and understand and agree to all the policies and practices set forth in the SACC Parent Handbook by the Carlisle Family YMCA. I also acknowledge that any changes in attendance, registration or policy exceptions need to be received in writing and approved by the Carlisle Family YMCA 2 weeks in advance of service to receive a 75% refund. If a request is not received in writing two weeks prior to service no refund will be awarded.
(Print Name) ________________________________________________________________________________
(Parent/Guardian Signature) _____________________________________________________________________ (Date) ______________________________
Questions? Use our website contact form to get in touch with us. E-mail completed packets to Brittany Kemp [email protected] or mail it to Brittany’s attention: Carlisle Family YMCA, 311 S. West St., Carlisle PA 17013.
CREDIT CARD AND / OR EFT AUTHORIZATION FOR SACC TUITION
Credit Card and / or Electronic Funds Transfer (EFT) Authorization Form
Payment Type: _____ Checking Account (must attached a voided check) _____ Discover
_____ MasterCard _____ Visa _____ American Express
Print name as it appears on credit card ________________________________________________________________________________________
Card number ____________________________________________________________ Exp. Date ___________________ 3-Digit Code _________
1. I authorize the Carlisle Family YMCA to automatically deduct fees due for the above-mentioned program per the schedule requested.
2. I understand that it will be my responsibility to notify the Y in writing if I wish to change or cancel these automatic payments.
3. Should my payment not be honored by my Bank or Credit Union, for any reason, I realize that I am still responsible for the payment, plus a $35 service charge applied by the Y. This is in addition to any service fee charged by my Bank or Credit Union.