enlarge the pie: leadership and qapi€¦ · · 2017-11-11enlarge the pie: leadership and qapi...
TRANSCRIPT

Enlarge the Pie: Leadership and QAPI
Traci Treasure, MS, CPHQ, LNHA Quality Improvement Consultant
LeadingAge Washington Annual Conference 2013
2
• Qualis Health is one of the nation’s leading healthcare consulting organizations, partnering with our clients across the country to improve care for millions of Americans every day
• Serving as the Medicare Quality Improvement Organization (QIO) for Idaho and Washington
• QIOs: the largest federal network dedicated to improving health quality at the community level

3 3
Enlarge the Pie
5 5
Outline
• Identify Best Practice • QAPI • National Change Package • Qualis Health Collaborative
• Identify Opportunities • Four steps for improvement • PI model review
• Leaders’ role for transformation

6 6
PPACA Requirements
The Affordable Care Act of 2010 requires nursing homes to have an acceptable, written, QAPI plan in place within 1 year of the promulgation of a QAPI regulation.
• Nursing Homes in the US will soon be required to develop QAPI plans.
• Written plan must be unique to the facility. • QAPI is not new to the healthcare industry—it
is already required regulation in hospitals, hospice, ambulatory care, dialysis centers, transplant programs.
7 7
QAPI for Nursing Homes • QAPI is Person-Centered:
– Resident & Family input is essential
• QAPI is broad in scope and continuous: – All Staff, at All Levels, in All Departments use QAPI daily as part of
their routine job duties, it is not just a program or project!
• QAPI is about systems thinking: – Requires proactive analysis – Is data and measurement driven – Is supported by tools

8 8
The Five Elements of QAPI1
____ 1 Centers for Medicare & Medicaid Services http://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/Downloads/Survey-and-Cert-Letter-13-05.pdf
9 9
QAPI Pre-assessment Results
106 responses from homes in ID & WA

10 10
QAPI Status
• At least 3 or more homes have achieved stage 3 for every question
• The most homes at stage 3 for • “Just culture” • Governance Board support of QAPI
• The fewest homes at stage 3 for questions involving training and support of frontline caregivers in QAPI
11 11
Two Collaboratives
National • Best Practice
nursing home tour • Culture change • 7 Guiding
principles • 3 Learning event
webinars
Qualis Health • QAPI focus • AP use and
Dementia Care • Affinity groups to
support clinical changes of your choice

12 12
CMS Studied Nursing Homes
• Identify high performing nursing homes in order to learn more about their systems and processes that contribute to overall quality
• Specific focus HAI, HACs, antipsychotics • Focused on successful practices of high
performers • Consistent high CMS 5-Star rating; Good
performance on Quality Measures.
• Utilize the findings to share with any nursing home seeking to improve quality
13 13
Eligible for visits
14 14
Where they visited
15 15
Best Practice Principles
1. Lead with a sense of purpose 2. Recruit and retain a quality staff 3. Connect with residents in a celebration of
their lives 4. Nourish teamwork and communication 5. Be a continuous learning organization 6. Provide exceptional, compassionate
clinical care that treats the whole person 7. Construct solid business practices that
support your purpose

16 16
Great, but what’s that got to do with QAPI?
Five elements of QAPI • Design and scope • Governance &
Leadership • Feedback, data systems,
monitoring • Performance
Improvement Projects • Systematic analysis
and action
Best practice guiding principles
Lead with purpose Quality staff Connect with residents Teamwork/communication Continuous learning Clinical care Business practices
17 17
Changes You Can Try
CMS Best Practices Change package QAPI at a Glance
Focuses on the Five Elements and 12 Steps
Qualis Health Change Ideas Specific to our Focus Topics: AP, Falls, Pain
management, Re-hospitalization, others Sources: CMS change package, other known best
practices and literature review
www.qualishealthmedicare.org/NHCollaborative

18 18
Qualis Health Nursing Home Quality Care Collaborative
• February 2013 – July 2014 • Integrates with national collaborative • Provides local support at in-person events • Recaps content in webinars • Supports peer-to-peer sharing and
learning together • Website with best practice and peer
resources
19 19
Collaborative Activity To Date
• 133 Washington homes signed-up • 70 homes have attended at least one
learning event • 11 shared storyboards • 106 homes from ID and WA completed the
QAPI self-assessment • Action Period Reports from homes due by
June 15th!

20 20
Qualis Health Activity to Date
• In-person education and webinar series for Learning Session 1
• QM data reports X3 • QAPI pre-assessment report • Organized affinity groups for clinical topics • Enhanced website
www.qualishealthmedicare.org/NHCollaborative
• In-person and webinar events for Learning Session 2
21 21
Table Talk with Tip Sheets

22 22
Four Steps for Improvement
• Use your data and observe current practices
• Identify the gap from best practice • Match the change to test to the gap/cause • Train and support front line staff to do PI
23 23
1.a. Use Your Data
• Monitored QM rates not meeting goal • Adverse event tracking
• New infection, pressure ulcer, fall, other HAC • Unplanned readmission • Incident report • Survey citation • Near-miss events • Medication errors
• Resident/staff satisfaction scores
24 24
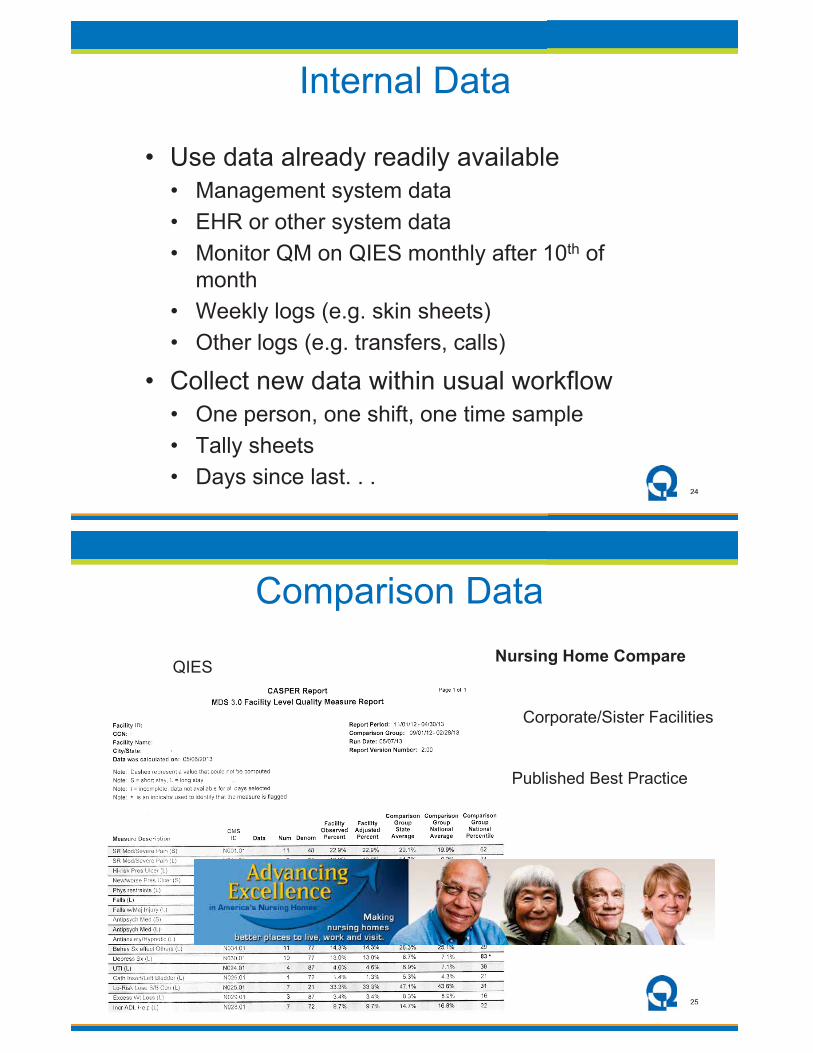
Internal Data
• Use data already readily available • Management system data • EHR or other system data • Monitor QM on QIES monthly after 10th of
month • Weekly logs (e.g. skin sheets) • Other logs (e.g. transfers, calls)
• Collect new data within usual workflow • One person, one shift, one time sample • Tally sheets • Days since last. . .
25 25
Nursing Home Compare QIES
Comparison Data
Corporate/Sister Facilities
Published Best Practice
26 26
Speed of Improvement
• Gather just enough data one step faster than needed outcome • Hourly • By shift • Daily • Weekly • Monthly • Quarterly • Annually
27 27
1.b. Observe Current Practice
• Go to the gemba • Ask 5 people for an objective view of what
usually happens and how standardized the process now is
• Use gap & cause—system assessments • May use RCA

28 28
2. Identify Best Practice
• Use a standardized system assessment • Pressure ulcer system self-assessment • QAPI self-assessment • Others
• Use literature • Change package best practice ideas • Qualis Health website change ideas
• Use your own best-practice leaders
29 29
3. Match Change to Test
• Include people closest to the process in decisions about which changes to try
• Identify which best practice change ideas most closely match the system issues you identified in step 1
• Make a short list of ideas to consider for testing in your organization
30 30
Selecting Changes to Test
• Requirements • Repercussions • Breadth of contributing factors • Complexity of system • Time & resources available • Biggest impact • Easy and low cost
31 31
A Few Models for PI
• IHI Model for Improvement • Shewhart’s PDSA Cycle • Lean • Just Culture • Root Cause Analysis
Any or all may be used in building your QAPI
capacity

32 32
The Institute for Healthcare Improvement (IHI) Model for Improvement2
What are we trying
to accomplish?
How will we know that a change is an
improvement?
What change can we make that will result in improvement?
____ 2 http://www.ihi.org/knowledge/Pages/HowtoImprove/default.aspx
33 33
PDSA Cycle for Learning Improvement
Plan Charter your Team! Make Predictions -
Who, What, When, Where?
Do Carry out the plan… use
Lean? Document problems,
unexpected observations. Begin analysis.
Study
Complete the analysis of the data and compare to
predictions. Summarize learning.
Act Adopt, Adapt, or Abandon?
What changes are to be made?
Next cycle?

34 34
Definition of Lean in Healthcare
•An organization’s cultural commitment to applying the scientific method to designing, performing, and continuously improving the work delivered by teams of people leading to measurably better value for patients and other stakeholders
John Toussaint, MD ThedaCare Center for Healthcare Value
35 35
Title: What you are talking about. Background
Current Situation
Goal
Analysis
Recommendations
Plan
Follow - up
Why are you talking about it?
Where do we stand?
Where we need to be? What is the specific change you want to accomplish now?
-What is the root cause(s) of the problem?
-
What is your proposed countermeasure(s)?
What activities will be required for implementation and who will be responsible for what and when?
How we will know if the actions have the impact needed? What remaining issues can be anticipated?
Verble/Shook
�What’s the problem?
36 36
Lean Healthcare Six Principles
1.Value creation for patients 2.Unity of purpose (True North) 3.Continuous improvement (pursuing
perfection) 4.Visual management 5.Standard work 6.Respect for people
Excerpted from John Toussaint “The Promise of Lean for Healthcare” accepted for publication Mayo Clinic Proceedings July 2012
37 37
The Just Culture
•Designing systems to prevent errors from causing harm •Encouraging transparency about errors and error
reporting –Creating a learning organization
•Developing appropriate responses to errors and harms: the CULTURE is “JUST”
•Does not mean lack of accountability Implementing Just Culture is a core element of QAPI!

38 38
Human Error
Product of our current system design and behavioral choices Manage through changes in: •Choices •Processes •Procedures •Training •Design •Environment
Console
At-Risk Behavior A Choice: risk believed insignificant or justified Manage through: •Removing incentives
for at-risk behaviors •Creating incentives for
healthy behaviors •Increasing situational
awareness
Reckless Behavior
Conscious disregard of substantial and unjustifiable risk Manage through: •Remedial action •Punitive action
Coach Punish
Thanks to the Just Culture Community and David Marx for this content
The Just Culture
39 39
Root Cause Analysis?

40 40
Gap and Cause—System Analysis
•Less formal and structured than Root Cause Analysis
•May use a formal system assessment tool •May use standard questioning to collect
organizational knowledge
41 41
System Assessments
•Use evidence-based best practice instruments •Examples
•Pressure Ulcer System Assessment •Emory Falls Management Self-Assessment •TeamSTEPPS Readiness Assessment •CLIP •WHO Surgery Checklist •Project RED

42 42
Go to the Gemba
•What happened to create the negative result?
•What usually happens? •How standardized is the process now? •What is in place to reduce risk of errors? •Who/where in your organization has the
best results? •How do you share the learning from
success with others throughout the organization?
43 43
Process Flow Diagram
•Answers the question “what happened?” •Shows GAP not CAUSE
Put bread on plate
Spread peanut butter
Spread jelly
Put bread pieces
together

44 44
5 Whys Method
Root Cause
Event
Why?
Why?
Why?
Why?
Why?
Root Cause
Why?
Why?
Root Cause
45 45
Six-Factors for Human Performance
Howard Sommerfeld

46 46
New Approach to RCA
1.Is this really a person or a system issue (apply “Just Culture”)?
2.Identify System Issue 3.Gap and Cause Analysis 4.Quality Improvement
47 47
4. Train and Support Front Line Staff
•Include PI tools in orientation •Train & competency test for PI skills yearly •Identify front-line staff PI champions •Create space in schedules for PI activities •Provide resources
•Computer •Bulletin board •Meeting space & time •Materials •Learning circles/sharing boards

48 48
Four Steps for Improvement
•Use your data and observe current practices
•Identify the gap from best practice •Match the change to test to the gap/cause •Train and support front line staff to do PI
49 49
How Do I Empower Front-line Staff?

50 50
The single most important critical factor missing in healthcare organizations is a
management system that supports improvement
A way to do it right the first time
John Toussaint, ThedaCare Center for
Healthcare Value
51 51
Most of what we call management consists of making it difficult for people to get their
work done
-Peter Drucker

52 52
Management by objectives: It nourishes short term performance, annihilates long
term planning, builds fear, and demolishes teamwork.
It leaves people bitter, crushed, bruised, battered, desolate, and despondent.
- W. Edwards Deming
53 53
Management by Process
•A3 thinking—define the problem first •Daily status sheet •Daily performance and defect review
huddle •Unit-based leadership teams •Standard work for leaders and supervisors •Standard work audits •Visual progress tracking
Lean Enterprise Institute: Toussaint webinar “A Roadmap to Lean Healthcare Success” originally presented: April 16, 2013
54 54
Change in Leader Behaviors
•All knowing •“In charge” •Autocratic •“Buck stops here” •Impatient •Blaming •Controlling
•Humility •Curiosity •Facilitator •Teacher •Student •Communicator •Perseverance
55 55
Can you say “Yes” every day?
•Are staff and doctors treated with dignity and respect by everyone in our organization?
•Do staff and doctors have the training and encouragement to do work that gives their life meaning?
•Have I recognized my staff and doctors for what they do?

56 56
“The No Meeting Zone”
•Theda Care best practice •Create scheduled white space •Use time for purposeful rounding at the
front line •Learn from front-line staff •Use standard-work for leaders
56
57 57
Daily Stat Sheets - Alignment

58 58
Monthly Scorecard Alignment
59 59
Summary
•Identify Best Practice •QAPI •National Change Package •Qualis Health Collaborative
•Identify Opportunities •Four steps for improvement •PI model review
•Leaders’ role for transformation

60 60
How will you enlarge your pie?
61 61
Online References •Canadian RCA Framework
http://www.patientsafetyinstitute.ca/English/toolsResources/rca/Pages/default.aspx
•Sommerfeld, H. (Feb 2011) Lean Production, Quality, Change and Training – Take a System Approach. Automated Learning Corporation. http://www.automatedlearning.com/resources/LPPerfSystem.pdf
•Lean Enterprise Institute: Toussaint webinar “A Roadmap to Lean Healthcare Success” originally presented: April 16, 2013 http://www.lean.org/events/webinarhome.cfm?utm_source=iContact&utm_medium=email&utm_campaign=Chet%20Messages&utm_content=April26webarch#hcroadmap
•A3 Template www.lean.org/downloads/A3_ppt_templates.ppt
•Qualis Health Nursing Home Collaborative www.qualishealthmedicare.org/NHCollaborative

62 62
Traci Treasure, MS, CPHQ, LNHA Quality Improvement Consultant
[email protected] 208-383-5947
For more information: www.QualisHealthMedicare.org/NHCollaborative
This material was prepared by Qualis Health, the Medicare Quality Improvement Organization for Idaho and Washington, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. ID/WA-C7-QH-1116-05-13
Questions?

Best Practices Tip Sheet
DRAFT May 1, 2013 Qualis Health
Dementia Care and Appropriate Antipsychotic Medication Use
Lead: Traci Treasure [email protected] 208-383-5947
Educate staff and family on different types of dementia, and approaches to care, including medication use, in order to reduce/eliminate the use of anti-psychotic medications.
View “disruptive” behaviors as attempts to communicate needs. Explore patterns, times, potential causes to help understand the needs that are being communicated.
Involve direct care staff on all shifts in identifying and sharing approaches that work for behavior disorders. For example, meet with nursing assistants to gather creative ideas and ways they have identified and met resident needs without the use of anti-psychotics.
Provide individualized care based upon the resident’s response. Empower the nursing assistants to use their best judgment and knowledge of the resident when caring for them.
When anti-psychotic medications are used, document the specific reason for use. For example, instead of stating paranoia, describe specific symptoms such as not eating because of fear of being poisoned by food.
Encourage staff to meet the resident’s needs rather than accepting behaviors as typical.
Promote an environment that has been proven to be supportive: quiet; normal routine of home, familiar areas, consistent staff, etc.
Sources:
National Nursing Home Quality Care Collaborative Change Package, Strategy 6.d. Change Concepts 29-35, page 35 http://www.qualishealthmedicare.org/sites/default/files/NHChangePackageV1.2.pdf
CMS Partnership to Improve Dementia Care http://www.nhqualitycampaign.org/star_index.aspx?controls=dementiaCare
Advancing Excellence Campaign – Medications goal http://www.nhqualitycampaign.org/star_index.aspx?controls=medicationsexploregoal
Qualis Health Focus Topic web page on Dementia Care http://www.qualishealthmedicare.org/healthcare-providers/nursing-homes/quality-care-collaborative/focus-topics/dementia-care
This material was prepared by Qualis Health, the Medicare Quality Improvement Organization for Idaho and Washington, under a
contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human
Services. The contents presented do not necessarily reflect CMS policy. ID/WA-C7-QH-1113-05-13

Non-Drug Management of Problem Behaviors and Psychosis in Dementia
STEP 1: Assess And Treats Contributing Factors
FOCUS on one behavior at a time• Note how often, how bad, how long, & document specific details • Ask: What is really going on? What is causing the problem behavior? What is making it worse?
IDENTIFY what leads to or triggers problems• Physical: pain, infection, hunger/thirst, other needs?• Psychological: loneliness, boredom, nothing to do?• Environment: too much/too little going on; lost?• Psychiatric: depression, anxiety, psychosis?
REDUCE, ELIMINATE things that lead to or trigger the problems• Treat medical/physical problems• Offer pain medications for comfort or to help cooperation• Address emotional needs: reassure, encourage, engage • Offer enjoyable activities to do alone, 1:1, small group• Remove or disguise misleading objects• Redirect away from people or areas that lead to problems• Try another approach; try again later• Find out what works for others; get someone to help
DOCUMENT outcomes• If the behavior is reduced or manageable, go to Step 3• If the behavior persists, go to Step 2 STEP 2: Select and Apply Interventions
CONSIDER retained abilities, preferences, resources• Cognitive level• Physical functional level• Long-standing personality, life history, interests• Preferred personal routines, daily schedules• Personal/family/facility resources
DEVELOP a Person-Centered plan• Adjust caregiver approaches• Adapt/change the environment• Select/use best evidence-based interventions tailored to the person’s unique needs/interests/abilities
This material was prepared by University of Iowa and Agency for Healthcare Research and Quality, which has granted permission to duplicate for educational purposes. This copy has been provided by Qualis Health, the Medicare Quality Improvement Organization for Idaho and Washington, under a contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. ID/WA-C7-QH-1081-03-13
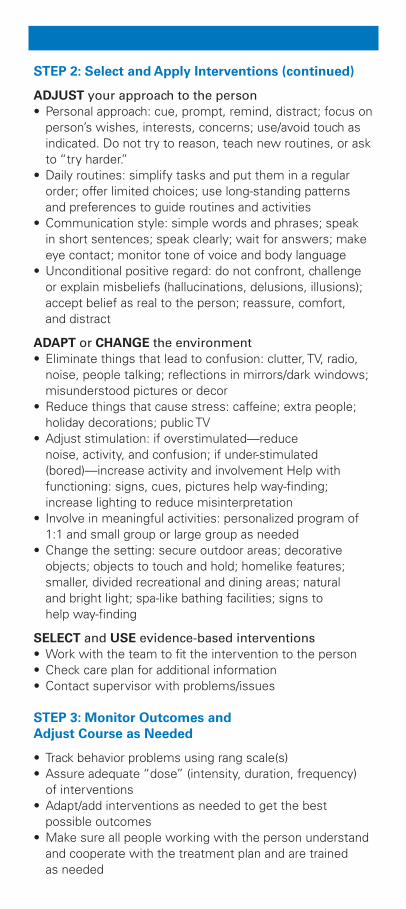
STEP 2: Select and Apply Interventions (continued)
ADJUST your approach to the person• Personal approach: cue, prompt, remind, distract; focus on
person’s wishes, interests, concerns; use/avoid touch as indicated. Do not try to reason, teach new routines, or ask to “try harder.”
• Daily routines: simplify tasks and put them in a regular order; offer limited choices; use long-standing patterns and preferences to guide routines and activities
• Communication style: simple words and phrases; speak in short sentences; speak clearly; wait for answers; make eye contact; monitor tone of voice and body language
• Unconditional positive regard: do not confront, challenge or explain misbeliefs (hallucinations, delusions, illusions); accept belief as real to the person; reassure, comfort, and distract
ADAPT or CHANGE the environment• Eliminate things that lead to confusion: clutter, TV, radio,
noise, people talking; reflections in mirrors/dark windows; misunderstood pictures or decor
• Reduce things that cause stress: caffeine; extra people; holiday decorations; public TV
• Adjust stimulation: if overstimulated—reduce noise, activity, and confusion; if under-stimulated (bored)—increase activity and involvement Help with functioning: signs, cues, pictures help way-finding; increase lighting to reduce misinterpretation
• Involve in meaningful activities: personalized program of 1:1 and small group or large group as needed
• Change the setting: secure outdoor areas; decorative objects; objects to touch and hold; homelike features; smaller, divided recreational and dining areas; natural and bright light; spa-like bathing facilities; signs to help way-finding
SELECT and USE evidence-based interventions• Work with the team to fit the intervention to the person• Check care plan for additional information• Contact supervisor with problems/issues STEP 3: Monitor Outcomes and Adjust Course as Needed
• Track behavior problems using rang scale(s)• Assure adequate “dose” (intensity, duration, frequency) of interventions• Adapt/add interventions as needed to get the best possible outcomes• Make sure all people working with the person understand and cooperate with the treatment plan and are trained as needed

DSA
P
Set Aim
Study High Performers
Recruit Faculty
Develop
Framework and Changes
Enroll
Participants
Prework
LS3Fall 2013
AP3Summative
Congresses and Publications
Feb 2014
LS1Feb 2013
AP1 LS2Apr/May
2013
AP2
DSA
P DSA
P
Learning Session
Supports:Email • Visits • Phone Conferences • Team Reports • Assessments
Action PeriodDSA
PPlan-Do-Study-Act
QUALIS HEALTH Nursing Home Quality Care CollaborativeWebinar recordings, materials, tools, news and progress and updates on learning sessions are available at www.qualishealthmedicare.org/NHCollaborative.
This material was prepared by Qualis Health, the Medicare Quality Improvement Organization for Idaho and Washington, under a contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. ID/WA-C7-QH-1127-05-13
DSA
P
Set Aim
Study High Performers
Recruit Faculty
Develop
Framework and Changes
Enroll
Participants
Prework
LS3Fall 2013
AP3Summative
Congresses and Publications
Feb 2014
LS1Feb 2013
AP1 LS2Apr/May
2013
AP2
DSA
P DSA
P
Learning Session
Supports:Email • Visits • Phone Conferences • Team Reports • Assessments
Action PeriodDSA
PPlan-Do-Study-Act
QUALIS HEALTH Nursing Home Quality Care CollaborativeWebinar recordings, materials, tools, news and progress and updates on learning sessions are available at www.qualishealthmedicare.org/NHCollaborative.
This material was prepared by Qualis Health, the Medicare Quality Improvement Organization for Idaho and Washington, under a contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. ID/WA-C7-QH-1127-05-13