endocrinol. japon. 1989, 36(2),299-314 - jst
TRANSCRIPT
Endocrinol. Japon. 1989, 36(2),299-314
The Management of Hyperthyroidism Due to Graves' Diseasein Japan in 1988
The Japan Thyroid Association; YUJI NAGAYAMA, MOTOMORI IZUMIAND SHIGENOBU NAGATAKI
The First Department of Internal Medicine, Nagasaki University School ofMedicine, Nagasaki, Japan
Abstract
The management of hyperthyroidism due to Graves' disease in Japan was the
subject of a survey of the members of the Japan Thyroid Association (JTA), and
the results were compared to those of the European Thyroid Association (ETA).
In the questionnaire, in vivo and in vitro diagnostic procedures, the choice ot
treatment and the details of the treatment for a patient with typical, moderate
and uncomplicated hyperthyroidism due to Graves' disease was at first asked,
and eight variations with a single alternative were proposed to evaluate how
each alternative would affect the choice of treatment. For the diagnostic
procedures, thyroid uptake/scintigraphy was carried out by approximately 60%
of the respondents and the isotope mainly used was 123I. The number of in
vitro tests used for diagnosis averaged 8.1•}1.8 tests. Measurements of basal
TSH and free T4 were the most frequent tests performed to confirm the
diagnosis of hyperthyroidism (94 and 80%, respectively). Determinations of
microsomal, thyroglobulin and TSH-receptor autoantibodies were also employed
by many respondents (96, 96 and 77%, respectively). On the other hand, the
free T4 index and TRH test were less frequently employed. In the teatment
of these patients, antithyroid drug treatment was the first choice, and surgery
was not, in general, regarded as a primary therapy except in a patient with
a large goiter. The frequency of the respondents who advocated radioiodine
therapy was considerably higher for patients with recurrences and old age.
No respondents proposed radioiodine therapy for young patients. Specialists
tended to favor their own specialist treatment regimens. The initial dose of
antithyroid drugs was reduced according to thyroid function, and withdrawal
of antithyroid drug treatment was determined by some specific criteria (basal
TSH in supersensitive assays, TSH-receptor autoantibodies, T3 suppression
test, etc.). The aim of radioiodine therapy and surgery was to restore
euthyroidism. The significant differences between the results from the JTA
and those from the ETA were as follows radionuclide used for thyroid
uptake/scintigraphy was mainly 123I in Japan, but 131I in Europe, the number
of diagnostic studies in Japan was more than that in Europe, and the dosage
of antithyroid drugs was reduced according to thyroid function and discontinued
based on certain specific criteria in Japan, but after fixed periods in Europe.
These results may represent actual trends in how hyperthyrodism due to
Graves' disease is managed in specialist clinics in Japan today and the
differences between the JTA and the ETA.
Received January 31, 1989

300 NAGAYAMA et al.Endocrinol. Japon.April.1989
A survey of the management of hy-
perthyroidism due to Graves' disease wasundertaken in the European Thyroid As-sociation (ETA) in 1986 (Glinoer et al.,1987). Its purpose was (1) to obtain anaccurate pattern of how hyperthyroidismdue to Graves' disease was managed inEurope today and (2) also to delineatemore precise guidelines for future researchin thyroidology. Successively, a similarsurvey was also performed in the AmericanThyroid Association (ATA) in 1988 (Solomonet al., 1988), the results of which werecompared to those in the ETA. There-fore, for similar purposes, a survey of themembers of the Japan Thyroid Association
(JTA) was also conducted in 1988.
Methods
The contents of this survey were based on asimilar format to that used by the ETA in orderto compare trends in the management of hyper-thyroidism due to Graves' disease in differentareas (Annex); the basic case report of a typical ,moderate and uncomplicated example of hyper-thyroidism due to Graves' disease was at firstpresented, for whom in vivo and in vitro diag-nostic procedures, the choice of treatment andthe details of the treatment selected were asked ,and then, eight variations with a single altera-tive in the basic case history (age , sex, goitersize, severity, etc.) were proposed in order toevaluate how each alternative would affect thechoice of treatment.
The questionnaires were mailed to all membersof the JTA (698 including many basic scientists)at the end of 1987. The responses were givenindividually. The data analysis was performedin the First Department of Internal Medicine ,Nagasaki University School of Medicine sinceone of the authors (S.N.) was the Presidentof the JTA in 1988. Statistical analysis wasperformed by Chi square test.
Results
Responses to the surveyOne hundred and thirty eight members
(105 institutes) responded, and 95 of themwere internists, 33 were surgeons, 3 were
pediatricians and 7 were nuclear medicinephysicians. Approximately 20% of themembers responded.
Diagnostic proceduresIn vivo tests (Table 1)-Almost all
respondents (93%) carried out the workon the basic case on an out-patient basis .For in vivo tests, thyroid scintigraphy wascarried out by 58% of the respondents.1231 was used by 70% of respondents per -forming thyroid scintigraphy, followed by99mTc (20%) and 131I (15%); three res-
Table 1. Work up and in vivo diagnostic
procedures.
*Percent positive answers .
Vol.36, No.2 THE MANAGEMENT OF GRAVES' DISEASE IN JAPAN 301
pondents used two kinds of isotope forscintigraphy and one did used three kindsof isotope. Thyroid uptake measurementwas performed by 62% of the respondents.The isotope used most frequently was 123
I(70%), followed by 131I (20%) and 99mTc(10%). Of the respondents performingthyroid scintigraphy, 96% carried outthyroid uptake measurement, and of those
performing thyroid uptake measurements,90% did thyroid scintigraphy. Furthermore,four clinicians used different kinds of iso-topes for thyroid scintigraphy and thyroiduptake measurements. There was no re-spondent who determined serum PB131I. Inthe other in vivo tests, thyroid ultrasonograpywas carried out most frequently (25%).83%of ultrasonography was combined withthyroid scintigraphy, whereas ultrasono-
graphy without scintigraphy was performedless frequently (17%). Neck soft x-ray (2%),T3 suppression test (1%), basal metabolic
zrate measurement (1%), cervical computedtomography (1%), 201T1 scintigrapy (1%)and fine needle aspiration (1%) was per-formed much less frequently.
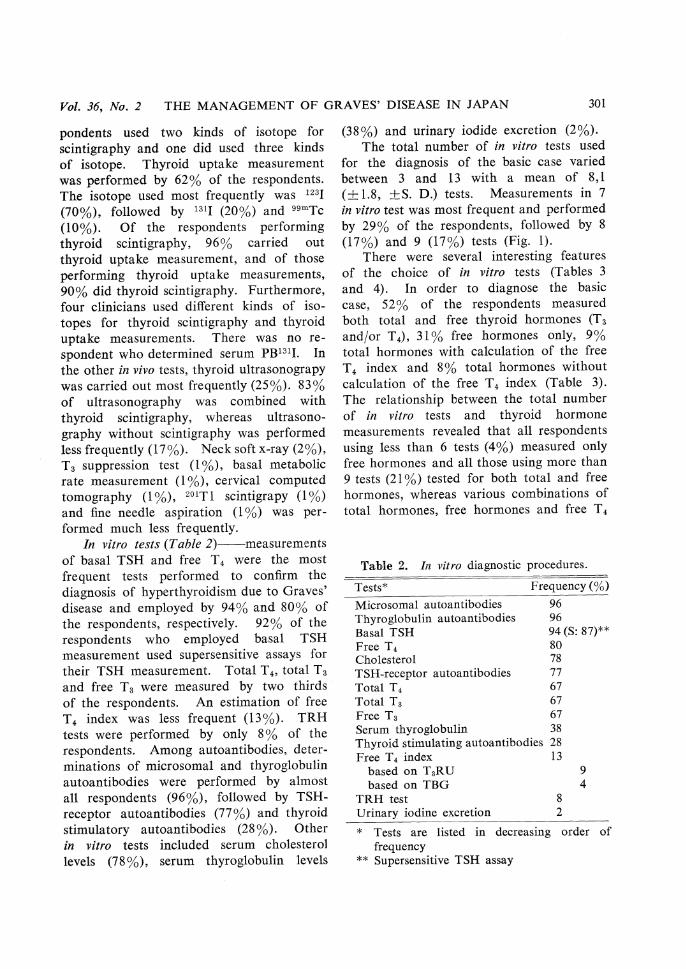
In vitro tests Table 2)-measurementsof basal TSH and free T4 were the mostfrequent tests performed to confirm thediagnosis of hyperthyroidism due to Graves'disease and employed by 94% and 80% ofthe respondents, respectively. 92% of therespondents who employed basal TSHmeasurement used supersensitive assays fortheir TSH measurement. Total T4, total T3and free T3 were measured by two thirdsof the respondents. An estimation of freeT4 index was less frequent (13%). TRHtests were performed by only 8% of therespondents. Among autoantibodies, deter-minations of microsomal and thyroglobulinautoantibodies were performed by almostall respondents (96%), followed by TSH-receptor autoantibodies (77%) and thyroidstimulatory autoantibodies (28%). Otherin vitro tests included serum cholesterollevels (78%), serum thyroglobulin levels
(38%) and urinary iodide excretion (2%).
The total number of in vitro tests used
for the diagnosis of the basic case varied
between 3 and 13 with a mean of 8,1
(•}1.8, •}S.D.) tests. Measurements in 7
in vitro test was most frequent and performed
by 29% of the respondents, followed by 8
(17%) and 9 (17%) tests (Fig. 1).
There were several interesting features
of the choice of in vitro tests (Tables 3
and 4). In order to diagnose the basic
case, 52% of the respondents measured
both total and free thyroid hormones (T3
and/or T4), 31% free hormones only, 9%
total hormones with calculation of the free
T4 index and 8% total hormones without
calculation of the free T4 index (Table 3).
The relationship between the total number
of in vitro tests and thyroid hormone
measurements revealed that all respondents
using less than 6 tests (4%) measured only
free hormones and all those using more than
9 tests (21%) tested for both total and free
hormones, whereas various combinations of
total hormones, free hormones and free T4
Table 2. In vitro diagnostic procedures.
*Tests are listed in decreasing order of
frequency**Supersensitive TSH assay

302 NAGAYAMA et al.Endocrinol. Japon.
April 1989
index were employed by those using 6-9 tests
(75%). The relationship between the totalnumber of in vitro tests and measurementsof autoantibodies was also examined (Table4). Measurement of autoantibodies was
clearly related to the total number of invitro tests; autoantibodies were measured
by all respondents using more than 9 tests,
but not by more than half of the respon-
dents using less than 6 tests. Obvious
Fig. 1. Total number of in vitro tests used for the evaluation of a patient with hyperthy-
roidism due to Graves' disease.
Table 3. Relationship between the total number of in vitro test carried out and
thyroid hormone measurements.
* FT4I, Free T4 index.
Table 4. Relationship between the total number of in vitro tests carried out and
measurements of autoantibodies.
* Auto -Ab , Autoantibodies

Vol.36, No.2 THE MANAGEMENT OF GRAVES' DISEASE IN JAPAN 303
relationships between the total number of
in vitro tests and TSH measurement, and
thyroid hormone measurements and TSHmeasurement were not observed.
Therapeutic choicesFor the management of the patient with
typical, moderate and uncomplicated hy-
perthyroidism due to Graves' disease, most
respondents recommended treatment withantithyroid drugs (88%). Radioiodinetherapy was proposed by 11% of res-
pondent and surgery by only one respondent(Fig. 2). Among the three groups, i. e. in-ternists (including pediatricians), surgeons andnuclear medicine physicians, the last tendedto prefer radioiodine therapy. In eightvariations with a single alternative, the
TOTAL
CASE 1
2
3
4
5
6
7
8
9
Fig. 2. Frequency of therapeutic options using antithyroid drugs, surgery or radioiodine
for the basic case of Graves' disease (case 1) and for patients with single alternations
(case 2 to 9).•¡, •¡ and •¡ represent medical treatment, surgery and radioiodine
therapy, respectively.

304 NAGAYAMA et al.Endocrinol. Japon.
April 1989
absence of goiter (case 3) and a change ofsex from female to male (case 7) made nomarked difference to practice. It was incase 2 with a large goiter that the numberof respondents who advocated surgery in-creased most remarkably; 27% of therespondents chose surgery. However, noneof the unclear medicine physicians recom-mended surgery; 71% of them used radio-iodine therapy and 29% antithyroid drugtreatment. In case 4 with severe hyper-thyroidism, a majority of the respondents
(81%) still recommended antithyroid drugtreatment, although the number of therespondents who proposed surgery increasedslightly (8%). Cases 5 and 6 dealt withthe problem about recurrence after antithy-roid drug treatment and thyroidectomy,respectively. In the former, the numberof respondents who proposed radioiodinetherapy or surgery increased considerably
(28% and 11%, respectively). More thantwo thirds of the nuclear medicine physiciansrecommended radioiodine therapy (71%).On the other hand, the increase in thenumber of respondents who advocatedradioiodine therapy was most evident inthe latter (52%). The last two cases con-cerned the problem of age. In case 8 (oldage), three fourths of the respondents pro-
posed antithyroid drug treatment, althoughthe proportion of radioiodine therapy in-creased considerably (24%), whereas in case9 (young age), 10% of the respondentschanged from radioiodine therapy to surgeryand no respondent advocated radioiodinetherapy.
On the average, antithyroid drug treat-ment represented 75% of the total options,radioiodine therapy 18% and surgery 7%.Specialists tended to favor their own in-dividual treatment regimens.
Methods of Treatment
Antithyroid drug administration-Methods
of antithyroid drug treatment were analysed
for the basic case and also for all the
variations. In the basic case, a majority
of the respondents (84%) chose methimazole
(MMI) as the drug for initial treatment,
and the remaining (16%) propylthiouracil
(PTU) (Table 5). Treatment was mainly
started with 30mg/day MMI (89%) or 300
mg/day PTU (89%). The initial dose of
MMI was reduced by 20mg/day (59%),
and PTU 200mg/day (41%) or 150mg/day
(41%), according to thyroid function (80%)
or after fixed periods of 2 to 12 weeks
(18%). Of the respondents who reduced the
initial dose of antithyroid drugs according
to thyroid function, 74% of them continued
it until thyroid hormone levels were reduced
to the normal range, 4% continued it until
the levels were below the normal range,
5% reduced it before the thyroid hormone
levels had normalized, and 10% reduced it
after basal TSH levels were measurable in
supersensitive assays. More than two thirds
of the respondents (72%) determined the
time of modification of treatment based on
the basis of both laboratory data and
clinical findings. However, a quarter of
the respondents judged by laboratory data
alone, and a few (3%) by clinical findings
alone. Answers to the question regarding
preference for use of antithyroid drugs alone
and adjustment of dosage in order to
maintain euthyroidism, or the use of com-
bination therapy of antithyroid drugs and
thyroid hormones showed that almost all
respondents chose the former (93%). Com-
bination therapy consisted of various doses
of antithyroid drugs (5-15mg/day MMI or
100-300mg/day PTU) and thyroid hormones
(25-75ƒÊg/day T3 or 25-100ƒÊg/day T4).
Beta-blocking agents were prescribed by
80% of the respondents during initial
treatment, and 3% employed them through-
out medical treatment, but 17% did neither.
Iodides were employed by a few respondents
(4%) only during the severe state.
Concerning the criteria for withdrawing
antithyroid drug treatment, a majority of
the respondents (93%) proposed to use

Vol.36, No.2 THE MANAGEMENT OF GRAVES' DISEASE IN JAPAN 305
Table 5. Methods of treatment-antithyroid
drug administration
*ATD, Antithyroid drug
various combinations of some specific criteria.The commonest criteria were normalizationof basal TSH in supersensitive assays (59%),of TSH-receptor autoantibodies (51%) andof the results of the T3 suppression test(47%). Normalization of the TRH testresults (18%), of thyroid stimulating auto-antibodies (16%) and serum thyroglobulinin the normal range (14%) were less fre-
quently adopted. No obvious differenceswere found among the results in 8 varia-tions.
Table 6. Methods of treatment - radioiodine
therapy

306 NAGAYAMA et al.Endocrinol.Japon.
APril 1989
Radioiodine therapy-The data resultingfrom the analysis of the basic case andcase 6 for whom this therapy was proposedby most of the respondents are presented
(Table 6). All the respondents used 131Ibut not 125I in order to restore euthyroidism.No respondent advocated the use of anablative dose of radioiodine to destroy thethyroid gland. The radioiodine dosagedelivered was estimated mainly on the basisof the thyroid uptake and gland size (ap-proximately 60%). Furthermore, approxi-mately 20% of the respondents calculatedthe radiation dose by also determining theeffective half-life of radioiodine in the neck.More than 80% of the respondents adoptedsingle administration of radioiodine, andrepetitive administration was uncommon.Medical treatment was performed beforeradioiodine therapy by approximately twothirds of the respondents and after radio-iodine therapy by approximately 80%. Inmedical treatment before radioiodine therapy,the frequency of antithyroid drug admistra-tion (alone or combined with beta-blockingagents or iodides) was two to three times
that of beta-blocking agents alone. Onlytwo respondents used LiCO3. After radio-iodine therapy, treatment consisted of anti-thyroid drug administration in over 90%of the respondents; half to two thirds ofthem used an antithyroid drug alone andthe others used a combination of antithyroiddrugs and beta-blocking agents or iodides.Antithyroid drug treatment after radioiodinetherapy was usually continued for 4-36months, or occasionally until euthyroidism.When the patient was not cured by thekfirst radioiodine administration, the second
radioiodine administration was performedafter a period of 6-12 months in over 80%of the respondents.
Surgery The data presented here werefor case 2 with a large goiter, because itwas the case for which most respondents
proposed this treatment (Table 7). Pre-operative medical treatment in order toachieve euthyroidism consisted of a com-bination of antithyroid drug with iodide(73%) or beta-blocking agents (27%). 76%of the respondents performed the operationafter euthyroidism had been reached, and
Table 7. Methods of treatment-surgery

Vol.36, No.2 THE MANAGEMENT OF GRAVES' DISEASE IN JAPAN 307
24% after euthyroidism had been reached
and maintained for 1-4 (2.4•}1.3, mean•}
S.D.) weeks. The aim of the surgery was
to keep the patient euthyroid without
medication in 97% of all respondents and
the decision to render the patient definitely
hypothyroid after surgery was proposed in
only 3%. After surgery, follow-up was
carried out in most of the specialist clinics
(97%). The organization of the follow-up
after surgery did not influence the surgical
strategy chosen.
Discussion
The survey of the management of hy-
perthyroidim due to Graves' disease, alreadyundertaken in the ETA and the ATA, wascarried out among the members of theJapan Thyroid Association (JTA). Theresponse rate was not high because question-naires were sent to all members of the JTAincluding many basic scientists. However,the results of this survey represent actualtrends in how hyperthyroidism due toGraves' disease is managed in specialistclinics in Japan today.
One of the purposes of the presentsurvey is, of course, to compare the resultsin Japan to those in other countries. Theresults of the survey in Europe have alreadybeen published (1), whereas those in the
United State were presented at the annualmeeting of the American Thyroid Associa-tion (2) but have not been published yet.Therefore, the results of the present surveyin Japan are mainly compared to those inEurope. A summary of the major differencesbetween the results in the JTA and in theETA is shown in Table 8. For in vivotests, the frequency of thyroid uptake/scintigraphy carried out in Japan was almostthe same as that in Europe, although theuse of 123I is more frequent in Japan thanin Europe. Thyroid ultrasonography was
performed by 20-25% of the respondentsin Japan and Europe and was mainlycombined with thyroid scintigraphy (morethan 80%). Concerning in vitro tests, thetotal number of in vitro tests was greaterin Japan than in Europe. Measurementsof microsomal, thyroglobulin and TSH-receptor autoantibodies, basal TSH and freethyroid hormones were performed morefrequently and the free T4 index and TRHtest were employed less frequently in Japanthan in Europe. In therapeutic choice,antithyroid drug treatment was found tobe a primary therapy in Japan and Europe.Futhermore, in both Japan and Europe, theselection of radioiodine therapy remainedlimited to recurrent and older patients,suggesting that in these areas there is stilla reluctance to use radioiodine therapy.Surgery was not regarded as a primary
Table 8. Summary of the major differences between the results in the JTA and the ETA.
* Statistically significant, p<0.05
** T .H., Thyroid hormones.
308 NAGAYAMA et al.Enaiocrinol. Japon.April 1989
therapy in either area, except in a patientwith a large-size goiter. For methods oftreatment, the most frequently used antithy-roid drug was MMI in both Japan andEurope. The initial dose of antithyroiddrugs was the same in both areas, and wasreduced according to thyroid function inJapan but after a fixed period in Europe.Almost all the respondents in Japan usedantithyroid drugs alone and adjusted thedosage of the drugs in order to maintaineuthyroidism, while half of the respondentsin Europe used a combination of antithyroiddrugs and thyroid hormones. Furthermore,almost all respondents in Japan used somespecific criteria for withdrawal of antithy-roid drugs, but many in Europe discontinuedantithyroid drugs after a fixed period. Theaims of radioiodine therapy and surgerywere mainly to restore euthyroidism in bothares.
In conclusion, these results representactual trends in methods of managementof hyperthyroidism due to Graves' diseasein specialist clinics in Japan and may be
useful in providing more precise guidelines
for future research in thyroidology.
Acknowledgements
We express our deep gratitude to all the
respondents among the members of the Japan
Thyroid Association for answering the question-
naire, Misses Yumi Tanaka and Yumi Takahara
for their excellent secretarial service and Dr. C.
J. Eastman for revising the manuscript.
References
Glinoer, D., D. Hesch, R. Lagasse and P.Laurberg (1987). The management of hyper-thyroidism due to Graves' disease in Europein 1986: results of an international survey.Acta Endocrinol 115, Suppl, 1-25.
Solomon, B., D. Glinoer, R. Lagasse and L.Wartofsky (1988). Management of hyperthy-roidism due to Graves' disease: results of asurvey of members of the ATA. 63th Meetingof American Thyroid Association (Montreal)T-34 (Abstract).

Vol.36, No.2 A SURVEY ON THE MANAGEMENT OF GRAVES' DISEASE 309
Annex: Accompanying Letter and Questionnaire
A survey on the management of Graves' disease
A survey on management of Graves' disease has been performed among themembers of th European, American and Latin American Thyroid Associations. Thistime, it was decided to conduct a similar survey in Japan.
The basic case report of a typical example of hyperthyroidism due to Graves'
disease was at first presented, for whom in vivo and in vitro diagnostic procedures, thechoice of treatment and details of the treatment selected were asked. 3 kinds of
questionnaires about medical treatment, surgery and radioiodine therapy were prepared.Answers concerning each medical treatment before or after surgery or radioiodinetherapy were noted on the questionnaire sheet. Next, eight variations with singlealternatives were proposed. In the case of the application of other treatment, the
questionnaire about treatment for those cases can be answered.
Respondent Name:Name of Clinic:
Address of Clinic:
A representative in the clinic answers the following questions:
1) The total number of patients with Graves' disease now under medicalent in your clinic:
2) The total number of patients with untreated Graves' disease for whom
medical treatment is started in your clinic in a year:
3) The total number of patients with Grave's disease receiving radioiodinetherapy in your clinic in a year:
4) The total number of patients with Graves' disease undergoing thyroid-ectomy in your clinic in a year:
Case I: A 43-yr-old woman has had moderate but overt signs and symptoms of hyper-thyrodism for 2-3 months (pulse rate regular 105/min). She is healthy and does nottake any medication. She has an active working life. She has 2 children 5 and 10
years of age and does not plan on being pregnant again. This is her first episode ofhyperthyroidism. She has a diffuse goiter weighing 40-50 grms. She has typical, butminimal, eye signs.Clinical impression: uncomplicated Graves' disease.How do you examine this patient?Answer the following questions (Check one)

310 NAGAYAMA et al.Endocrinol. Japon.April 1989
You will find sheets correponding to the 3 treatment strategies . Fill in only theappropriate sheet corresponding to the basic therapy you decided on .

Vol.36, No.2 A SURVEY ON THE MANAGEMENT OF GRAVES' DISEASE 311
CASE 1
If you have selected surrery for the basic case, fill in this sheet.
CASE 1
If you have selected medical treatment for the basic case, fill in this sheet.

312 NAGAYAMA et al.Endocrinol. Japon.April 1989
If Yes,

Vol. 36, No. 2 A SURVEY ON THE MANAGEMENT OF GRAVES' DISEASE 313
CASE 1
If you have selected radioiodine for the basic case, fill in this sheet.
Questionnaire for eight variations with single alternations
Single alternations include age, sex, severity, size of goiter and first episode orrecurrence, and are in parentheses. Answer the questions about these 8 cases in the
next page.

314 NAGAYAMA et al.
Endocrinol. Japon.
April 1989
* Severe: pulse rate is 150/min; the patient has lost 7 kg during the last 5 weeks .** Recurrence: in this case the patient has been treated 2 years before with ATD for
1 years.*** Recurrence: in this case the patient has been treated 4 years before by subtotal
thyroidectomy, leaving 10-15 grams of thyroid tissue after surgery.
If your answer is yes (i. e., you would apply the same therapeutic approach) checkYES for each variation that applies. If your answer is no (i. e., you would apply adifferent therapeutic approach) check NO for the therapeutic option you would choosefor that variation.
For every"NO", Please fill out the following pages for the therapeutic option you have
chosen.
Please write in the variation number in the blank provided at the top of each page.
Pages 10-13 have been omitted because they are the same as 4-7.