endocrine group 10. pituitary disease panhypopituitarism which hormones are lost first? the least...
TRANSCRIPT
ENDOCRINEENDOCRINE
Group 10Group 10

Pituitary DiseasePituitary Disease
PanhypopituitarismPanhypopituitarism
Which hormones are lost first? Which hormones are lost first? The least life threatening lost first: FSH, LHThe least life threatening lost first: FSH, LH

Which pituitary disorder affects the Which pituitary disorder affects the pituitary gland itself?pituitary gland itself?Secondary disordersSecondary disorders

A patient comes to you complaining of loss A patient comes to you complaining of loss of axillary, pubic and body hair. He also of axillary, pubic and body hair. He also complains of losing his sense of smell. complains of losing his sense of smell. What is the most likely diagnosis?What is the most likely diagnosis?
Kallman’s syndromeKallman’s syndrome
True or false:True or false: In adrenal deficiency there will be In adrenal deficiency there will be
hyperpigmentation.hyperpigmentation.• FALSEFALSE
Most common tumor causing Most common tumor causing hypopituitarism in childrenhypopituitarism in children
CraniopharyngiomaCraniopharyngioma
Common signs and symptoms of a basilar Common signs and symptoms of a basilar skull fracture:skull fracture:
Bilateral ecchymosisBilateral ecchymosis
““Battle sign”-ecchymosis of mastoidBattle sign”-ecchymosis of mastoid
Clear otorrhea or rhinorrheaClear otorrhea or rhinorrhea

Patient comes in one week after delivering Patient comes in one week after delivering her baby complaining of no lactation and her baby complaining of no lactation and loss of pubic and axillary hair. What is the loss of pubic and axillary hair. What is the diagnosis?diagnosis?
Sheehan’s syndromeSheehan’s syndrome

What is the treatment of choice for a What is the treatment of choice for a pituitary adenoma?pituitary adenoma?
Transphenoidal microsurgeryTransphenoidal microsurgery
HyperprolactinemiaHyperprolactinemia
What is prolactin inhibitory factor (PIF)?What is prolactin inhibitory factor (PIF)?DopamineDopamine
Treatment of choice?Treatment of choice?Medical preferred over surgicalMedical preferred over surgical
• BromocriptineBromocriptine

Patient comes to your office complaining Patient comes to your office complaining that recently he has had trouble fitting in that recently he has had trouble fitting in his gloves, hat and shoes. Upon physical his gloves, hat and shoes. Upon physical exam you notice protrusion of the jaw and exam you notice protrusion of the jaw and enlargening of the tongue. What is your enlargening of the tongue. What is your diagnosis?diagnosis?
Acromegaly Acromegaly

True or false:True or false: Desmopressin is used for the treatment of Desmopressin is used for the treatment of
nephrogenic Diabetes insipidusnephrogenic Diabetes insipidus• FALSE- it it used for central diabetes insipidus FALSE- it it used for central diabetes insipidus
where the production of ADH is deficientwhere the production of ADH is deficient• In nephrogenic DI, ADH levels are normal, but In nephrogenic DI, ADH levels are normal, but
there is a defect in kidney tubules that interferes there is a defect in kidney tubules that interferes with water reabsorptionwith water reabsorption
Secondary causes of nephrogenic DI:Secondary causes of nephrogenic DI:
HypercalcemiaHypercalcemia
HypokalemiaHypokalemia
A euvolemic hyponatremia is common in A euvolemic hyponatremia is common in which disease?which disease?
SIADH- SIADH-
Syndrome of Inappropriate Antidiuretic Syndrome of Inappropriate Antidiuretic Hormone SecretionHormone Secretion

What is a complication of correcting What is a complication of correcting SIADH too rapidly?SIADH too rapidly?
Contraction of brain cells resulting in Contraction of brain cells resulting in demyelinationdemyelination
ADRENALADRENAL
What hormone causes reabsorption of Na What hormone causes reabsorption of Na at the level of the kidney? at the level of the kidney?
AldosteroneAldosterone
Two major causes for aldosterone release? Two major causes for aldosterone release?
Hypovolemia or hypokalemia Hypovolemia or hypokalemia

What hormone counters insulin’s effects, What hormone counters insulin’s effects, is increased with stress/trauma, with a is increased with stress/trauma, with a diurnal pattern? diurnal pattern?
CortisolCortisol
How does it counter insulin’s effects in the How does it counter insulin’s effects in the body? body?
Hyperglycemia, increases hepatic Hyperglycemia, increases hepatic gluconeogenesis.gluconeogenesis.

What hormone is responsible for the What hormone is responsible for the development of secondary sex development of secondary sex characteristic? characteristic?
AndrogensAndrogens
These hormones are also neurotransmitters in These hormones are also neurotransmitters in the CNS? the CNS?
Catecholamines: Catecholamines: Epinephrine, NorepinephrineEpinephrine, Norepinephrine

MCC of hyperaldosteronism? MCC of hyperaldosteronism? Conn’s syndrome.Conn’s syndrome.
Etiology? Etiology? Unilateral adrenal aldosterone producing Unilateral adrenal aldosterone producing
adenomaadenoma
Aldosterone to renin ratio in primary Aldosterone to renin ratio in primary hyperaldosteronism? hyperaldosteronism?
Increases plasma aldosterone to renin ratioIncreases plasma aldosterone to renin ratio
How do you perform a aldosterone suppression How do you perform a aldosterone suppression test?test?
Give Na and aldosterone is not suppressed.Give Na and aldosterone is not suppressed.

Central obesity with striae and thin Central obesity with striae and thin extremities, HTN, DM, glucose extremities, HTN, DM, glucose intolerance, proximal muscle weakness? intolerance, proximal muscle weakness?
Hypercortisolism Hypercortisolism
Two additional common signs? Two additional common signs?
Moon face, buffalo hump.Moon face, buffalo hump.

Prolonged use of exogenous steroids or Prolonged use of exogenous steroids or ACTH causes? ACTH causes?
Cushing’s SyndromeCushing’s Syndrome
What causes Cushing’s Disease? What causes Cushing’s Disease? Increased pituitary secretion of ACTHIncreased pituitary secretion of ACTH
Common etiology? Common etiology? Pituitary adenomaPituitary adenoma

First diagnostic test for Cushing’s? First diagnostic test for Cushing’s? 24 hr urine cortisol 24 hr urine cortisol
Second Test? Second Test? Low dose dexamethasone for suppressionLow dose dexamethasone for suppression
Third diagnostic test? ACTHThird diagnostic test? ACTH If decreased, then? It’s adrenal. If decreased, then? It’s adrenal. Fourth diagnostic test?Fourth diagnostic test?
High dose dexamethasone. High dose dexamethasone. If it doesn’t suppress ACTH then what? If it doesn’t suppress ACTH then what? Tumor is ectopic.Tumor is ectopic.
Weight loss, salt cravings, hyperpigmentation,Weight loss, salt cravings, hyperpigmentation,
abdominal pain? abdominal pain?
Addison’s Addison’s
MCC Addison’s in US? MCC Addison’s in US?
Autoimmune Autoimmune
Worldwide? Worldwide?
TBTB
What are the two stimulation diagnostic tests What are the two stimulation diagnostic tests for Addison’s? for Addison’s?
Cosyntropin and MetyraponeCosyntropin and Metyrapone
Increased K, decreased Na, decreased Increased K, decreased Na, decreased cortisol, decreased aldosterone, cortisol, decreased aldosterone, decreased androgen, ACTH increased? decreased androgen, ACTH increased?
Primary or secondary Addison’s?Primary or secondary Addison’s?
PrimaryPrimary
Paroxysmal HTN, sweating, headache, Paroxysmal HTN, sweating, headache, palpitations, hyperglycemia, flushing, orthostatic palpitations, hyperglycemia, flushing, orthostatic hypotension? hypotension?
PheochromocytomaPheochromocytoma
Diagnostic TOC? Diagnostic TOC?
Metanephrine and vanillylmandelic acid Metanephrine and vanillylmandelic acid
TOC TOC
pre-op a-blockers and b-blockers, w/venous pre-op a-blockers and b-blockers, w/venous ligation and removal of glandligation and removal of gland
Parahyperthyroidism, pancreatic islet cell Parahyperthyroidism, pancreatic islet cell tumor, pituitary tumor tumor, pituitary tumor
MEN I- Wermer’s presentation MEN I- Wermer’s presentation
Parahyperthyroidism, adrenal tumor, thyroid Parahyperthyroidism, adrenal tumor, thyroid (medullary carcinoma) (medullary carcinoma)
MEN IIA- Sipple syndrome MEN IIA- Sipple syndrome
Mucosal/GI, Marfanoid, adrenal Mucosal/GI, Marfanoid, adrenal (pheochromocytoma), thyroid (medullary (pheochromocytoma), thyroid (medullary carcinoma) carcinoma)
MEN IIB- Mucosal and GI MEN IIB- Mucosal and GI
Increased blood Ca, increased PTH? Increased blood Ca, increased PTH?
HyperparathyroidismHyperparathyroidism
Manifestation? Manifestation?
Stones, bones, groans, psychic Stones, bones, groans, psychic overtones, and short Q-Tovertones, and short Q-T
What substance do you take into account What substance do you take into account when measuring the Ca level? when measuring the Ca level?
AlbuminAlbumin
Decreased Ca, prolonged Q-T,Decreased Ca, prolonged Q-T,
paresthesias, muscles cramps, hyperactive paresthesias, muscles cramps, hyperactive DTRs? DTRs?
HypoparathyroidismHypoparathyroidism
What special signs can you test for in PE? What special signs can you test for in PE?
Chvostek’s and Trousseau’sChvostek’s and Trousseau’s
Chovostek’s sign- is a carpal spasm with Chovostek’s sign- is a carpal spasm with use of BP cuff. True/False?use of BP cuff. True/False?
FalseFalse

Decreased Ca, increase PTH, short Decreased Ca, increase PTH, short stature, round face, short 4th metacarpal, stature, round face, short 4th metacarpal, and mental retardation? and mental retardation?
Pseudo- hypoparathyroidismPseudo- hypoparathyroidism
THYROID DISEASESTHYROID DISEASES

Where is TRH released from?Where is TRH released from? The Hypothalmus The Hypothalmus
Where is TSH released from? Where is TSH released from? Anterior PituitaryAnterior Pituitary
Where is T3 & T4 released from? Where is T3 & T4 released from? ThyroidThyroid
What is the major hormone secreted into What is the major hormone secreted into circulation and converted in the cell? circulation and converted in the cell? T4T4
Why is thyroid hormone critical in children? Why is thyroid hormone critical in children? Brain and musculoskeletal development. Brain and musculoskeletal development.
What happen without it? What happen without it? Growth impairment and mental retardationGrowth impairment and mental retardation
What form of hypothyroidism is this?What form of hypothyroidism is this? Congenital Congenital
Tx: Tx: prompt T4prompt T4
What substance is required to produce What substance is required to produce thyroid hormone? thyroid hormone? IodideIodide
Where do we get it? Where do we get it? SaltSalt
Iodine deficiency is the MCC of primary Iodine deficiency is the MCC of primary hypothyroidism in the US? True or Falsehypothyroidism in the US? True or False FalseFalse It is, however, the MCC worldwideIt is, however, the MCC worldwide
Patient presents with fatigue, SOB, hair Patient presents with fatigue, SOB, hair loss and cold intolerance? DX?loss and cold intolerance? DX? HypothyroidismHypothyroidism
Other symptoms include?Other symptoms include? Slow movement/speech, weight gainSlow movement/speech, weight gain
PE will reveal…PE will reveal… Delayed DTRs, non-pitting edema, cool pale Delayed DTRs, non-pitting edema, cool pale
skin, loss of lateral 1/3 of eyebrowskin, loss of lateral 1/3 of eyebrow Labs reveal: Labs reveal:
Low TSHLow TSH MCC of primary hypothyroidismMCC of primary hypothyroidism
Hashimotos’s Hashimotos’s Etiology? Etiology?
AutoimmuneAutoimmune
What is the most severe form of What is the most severe form of Hypothyroidism? Hypothyroidism? Myexedema Coma. Myexedema Coma.
Presentation? Presentation? Hypothermia, respiratory depression, Hypothermia, respiratory depression,
cardio collapsecardio collapse

Patient presents with anxiousness, Patient presents with anxiousness, thinning hair, muscle weakness and heat thinning hair, muscle weakness and heat intolerance. DX? intolerance. DX? HyperthyroidismHyperthyroidism
Additional symptoms include?Additional symptoms include? Increased appetite and weight lossIncreased appetite and weight loss
PE reveals? PE reveals? Warm and moist skin, tachycardia, Warm and moist skin, tachycardia,
hyperreflexia, and exophthalmus hyperreflexia, and exophthalmus Initial lab indicator? Initial lab indicator?
Low TSH; Why? Low TSH; Why? negative feedback negative feedback
Second lab: Second lab: T4 high T4 high

What will be seen on radioactive iodine What will be seen on radioactive iodine uptake? uptake? Increased uptake. Increased uptake.
TOC for hyperthyroidism?TOC for hyperthyroidism? radioiodine ablationradioiodine ablation
MCC of hyperthyroidism? MCC of hyperthyroidism? Grave’s diseaseGrave’s disease
Patient presents with exaggerated Patient presents with exaggerated hyperthyroidism plus delirium, CHF, stupor hyperthyroidism plus delirium, CHF, stupor and fever. Dx? and fever. Dx? Thyroid stormThyroid storm
Tx: Tx: beta- blockersbeta- blockers anti-thyroid agentsanti-thyroid agents DexamethasoneDexamethasone
Supportive Tx:Supportive Tx: IV fluids and cooling blanketsIV fluids and cooling blankets
Can you name a rare cause Can you name a rare cause hyperthyroidism….hyperthyroidism….
Hint: it has nothing to do with the thyroid Hint: it has nothing to do with the thyroid gland? gland? Ovarian dermoid tumor containing thyroid tissue.Ovarian dermoid tumor containing thyroid tissue.
What is the most common cause of What is the most common cause of diabetic hospital admissions?diabetic hospital admissions?
Problems with the feet- peripheral neuropathyProblems with the feet- peripheral neuropathy
Stocking and glove distribution refers to Stocking and glove distribution refers to what?what?
Loss of perception of vibrations, temperature, Loss of perception of vibrations, temperature, touch, position sense, and altered pain touch, position sense, and altered pain perceptionperception

Where are the most common area for an Where are the most common area for an ulcer in diabetic patients?ulcer in diabetic patients?
Dorsal portion of toes, plantar of metatarsal Dorsal portion of toes, plantar of metatarsal heads and heelheads and heel

Your patient has just been diagnosed with Your patient has just been diagnosed with diabetes- educate the patient on changes diabetes- educate the patient on changes that may need to be made.that may need to be made.
ShoesShoes Checking feet regularly for ulcers Checking feet regularly for ulcers MoisturizersMoisturizers Glucose control Glucose control Yearly podiatry assessmentsYearly podiatry assessments
Gonadal DysfunctionGonadal Dysfunction
Total Chromosomal number and sex Total Chromosomal number and sex chromosome in femaleschromosome in females
• 46 and XX46 and XX
Total Chromosomal number and sex Total Chromosomal number and sex chromosome in males?chromosome in males?
• 46 and XY46 and XY

A tall person comes to your office with…A tall person comes to your office with… decrease facial and axillary hair decrease facial and axillary hair Gynecomastia Gynecomastia High voice High voice Decrease libidoDecrease libido Small/firm testesSmall/firm testes
What would you predict the person’s What would you predict the person’s chromosome are?chromosome are?
46 and XXX46 and XXX

What would you notice in the physical of a What would you notice in the physical of a person with turner’s syndrome?person with turner’s syndrome? Webbing of the neckWebbing of the neck Short statureShort stature Short 4Short 4thth metacarpal metacarpal Mutiple congenital abnormalites to heart and Mutiple congenital abnormalites to heart and
kidney. kidney. What you would be the treatment?What you would be the treatment?
Estrogen replacementEstrogen replacement High dose of recombinant growth hormoneHigh dose of recombinant growth hormone Cardiac and renal evaluationCardiac and renal evaluation
What is the karotype of the following?What is the karotype of the following? Female pseudohermaphroditismFemale pseudohermaphroditism
• 46XX karyotype46XX karyotype
Male pseudohermaphroditismMale pseudohermaphroditism• 46XY karyotype46XY karyotype
True hermaphoditismTrue hermaphoditism• Have both 46XX and 46XYHave both 46XX and 46XY
Upon phsical examination you notice Upon phsical examination you notice clitoral enlargement and excessive clitoral enlargement and excessive production of androgens. Your likely dx?production of androgens. Your likely dx?
• Female pseudohermaphroditismFemale pseudohermaphroditism
Is the patient able bear child?Is the patient able bear child?• YesYes
What is the likely Dx?What is the likely Dx?
Upon physical you note…Upon physical you note…• Blind vaginaBlind vagina• Sparse axillary and pubic hairSparse axillary and pubic hair• Testes are present in abdomenTestes are present in abdomen• Breast developmentBreast development
Test show..Test show..• Testosterone levelTestosterone level• Xy karotypingXy karotyping• LH high and FSH normalLH high and FSH normal

Testicular feminization syndromeTesticular feminization syndrome
What would be your therapy?What would be your therapy?• EstrogenEstrogen

Diabetes Mellitus Type 1Diabetes Mellitus Type 1

Hyperglycemia is caused from?Hyperglycemia is caused from?
Low insulin secretion orLow insulin secretion or Insulin resistance and low secretionInsulin resistance and low secretion

Most common etiology is?Most common etiology is?
Autoimmune from beta islet cell Autoimmune from beta islet cell destructiondestruction
MC in Scandinavia and northern EuropeMC in Scandinavia and northern Europe Dependent on insulin for life (unlike Dependent on insulin for life (unlike
idiopathic form of DM)idiopathic form of DM)

What genetic markers predispose What genetic markers predispose you to DM 1? you to DM 1?
Human Leukocyte Antigen- 95% have Human Leukocyte Antigen- 95% have HLA DR3 or HLA DR4HLA DR3 or HLA DR4
Circulating Islet Cell Antibodies- 85% of Circulating Islet Cell Antibodies- 85% of patients test in 1patients test in 1stst week of onset week of onset
What are some common clinical What are some common clinical presentations?presentations?
*Polyphagia, polydypsia, polyuria*Polyphagia, polydypsia, polyuria *Weight loss/inability to gain weight*Weight loss/inability to gain weight Blurry visionBlurry vision Diabetic NeuropathyDiabetic Neuropathy *Ketoacidosis*Ketoacidosis Abdominal PainAbdominal Pain

What are some manifestations of What are some manifestations of ketoacidosis?ketoacidosis?
Insulin Deficiency Insulin Deficiency Lipolysis Lipolysis Free Free Fatty Acids Fatty Acids Ketonemia Ketonemia
Metabolic AcidosisMetabolic Acidosis Fruity Breath Odor (acetone)Fruity Breath Odor (acetone) Dehydration (hypotension, tachycardia)Dehydration (hypotension, tachycardia) Kussmaul’s Respiration (rapid deep Kussmaul’s Respiration (rapid deep
breathing)- corrects acid base disorderbreathing)- corrects acid base disorder

How do you treat DKA?How do you treat DKA?
0.9% NS for 1 hr 0.9% NS for 1 hr Then 0.45% NS with dextrose (prevent Then 0.45% NS with dextrose (prevent
hypoglycemia) for 3 hrshypoglycemia) for 3 hrs Insulin ReplacementInsulin Replacement K+ replacement (as needed)- from fluid K+ replacement (as needed)- from fluid
loss and intracellular shift of K+ into cells loss and intracellular shift of K+ into cells due to insulin replacementdue to insulin replacement
Tx Underlying CauseTx Underlying Cause

What is the best screening test for What is the best screening test for DM?DM?
Fasting Plasma GlucoseFasting Plasma Glucose How long do you fast for?How long do you fast for? Fast for 8 hours prior to the testFast for 8 hours prior to the test

What is the reference range of the What is the reference range of the fasting plasma glucose?fasting plasma glucose?
FPG <100mg/dl = reference rangeFPG <100mg/dl = reference range What is the impaired fasting range?What is the impaired fasting range? FPG FPG ≥ 100 mg/dl = impaired fasting ≥ 100 mg/dl = impaired fasting
glucoseglucose What is the range that is diagnostic for What is the range that is diagnostic for
DM?DM? FPG ≥ 126 mg/dl = diagnostic of DM (must FPG ≥ 126 mg/dl = diagnostic of DM (must
be done 2x)be done 2x)

What is the best test to diagnose What is the best test to diagnose DM?DM?
Oral Glucose Oral Glucose Tolerance TestTolerance Test
Can you fill in this Can you fill in this chart?chart?
Value after 1 hr of Fasting(fasting plasma glucose)
Value after 2 hrs of glucose(Glucose Load)
Reference Range
Impaired Glucose Tolerance
Dx DM
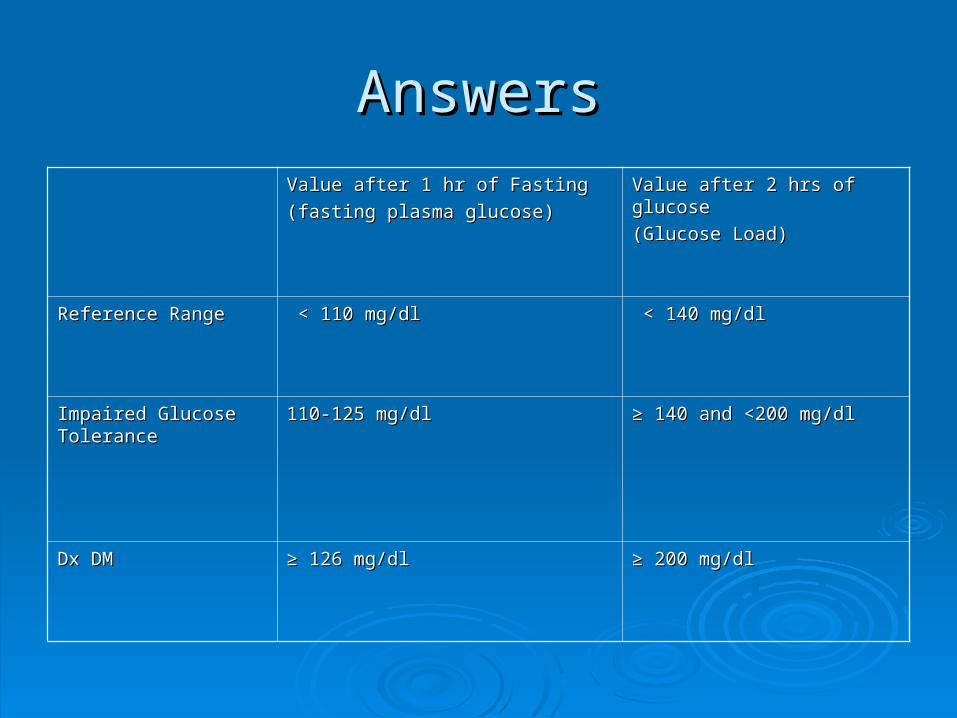
AnswersAnswersValue after 1 hr of FastingValue after 1 hr of Fasting
(fasting plasma glucose)(fasting plasma glucose)
Value after 2 hrs of glucoseValue after 2 hrs of glucose
(Glucose Load)(Glucose Load)
Reference RangeReference Range < 110 mg/dl< 110 mg/dl < 140 mg/dl< 140 mg/dl
Impaired Glucose Impaired Glucose ToleranceTolerance
110-125 mg/dl110-125 mg/dl ≥ ≥ 140 and <200 mg/dl140 and <200 mg/dl
Dx DMDx DM ≥ ≥ 126 mg/dl126 mg/dl ≥ ≥ 200 mg/dl200 mg/dl

What is measured as a screening What is measured as a screening tool for DM to log glycemic control?tool for DM to log glycemic control? Hemoglobin A1C (not diagnostic)Hemoglobin A1C (not diagnostic) What percent saturation should a diabetic What percent saturation should a diabetic
patient strive for with Hgb A1C?patient strive for with Hgb A1C? Should be saturated < 6.5%Should be saturated < 6.5%
What are some lab findings of DM What are some lab findings of DM 1?1?
MicroalbuminuriaMicroalbuminuria KetonuriaKetonuria Glucose in UrineGlucose in Urine Anti-insulin AntibodiesAnti-insulin Antibodies HypoinsulinemiaHypoinsulinemia
InsulinInsulin
What are 2 names of a “rapid form” of insulin?What are 2 names of a “rapid form” of insulin? Rapid- Lispro and AspartRapid- Lispro and Aspart What is a name of a “short acting” insulin?What is a name of a “short acting” insulin? Short- RegularShort- Regular What is a name of an “intermediate acting” insulin?What is a name of an “intermediate acting” insulin? Intermediate- NPH and LenteIntermediate- NPH and Lente What is a name of a “long acting” insulin?What is a name of a “long acting” insulin? Long- UltralenteLong- Ultralente What is the most commonly used combination amounts What is the most commonly used combination amounts
of NPH and Regular?of NPH and Regular? MC Combination- 70 NPH/30 Regular MC Combination- 70 NPH/30 Regular

What is the pathophysiology of the What is the pathophysiology of the Somogyi Effect?Somogyi Effect?
DM 1 patient takes insulin at night DM 1 patient takes insulin at night Patient becomes hypoglycemic Patient becomes hypoglycemic Counter-Regulatory hormones cortisol and Counter-Regulatory hormones cortisol and glucagon are releasedglucagon are released
Glucagon Glucagon releases glucose from liver releases glucose from liver Cortisol Cortisol increases insulin resistance increases insulin resistance Patient awakens with hyperglycemiaPatient awakens with hyperglycemia What is the treatment?What is the treatment? Treatment- Reduce night insulin doseTreatment- Reduce night insulin dose
What is the Dawn Phenomenon?What is the Dawn Phenomenon?
Increase in plasma glucose levels between 5 Increase in plasma glucose levels between 5 and 9 a.m., without preceding hypoglycemiaand 9 a.m., without preceding hypoglycemia
Which type of DM does this affect?Which type of DM does this affect? DM Type 1 and 2DM Type 1 and 2 Why is there hyperglycemia?Why is there hyperglycemia? Attributed to desensitization effects of growth Attributed to desensitization effects of growth
hormone and insulin on tissueshormone and insulin on tissues May cause mild hyperglycemia or may add to May cause mild hyperglycemia or may add to
the Somgyi Effectthe Somgyi Effect
What are some Microvascular What are some Microvascular Complications of DM 1?Complications of DM 1?
RetinopathyRetinopathy NephropathyNephropathy NeuropathyNeuropathy

What are some Macrovascular What are some Macrovascular Complications of DM 1?Complications of DM 1?
Cardiovascular DiseaseCardiovascular Disease Cerebrovascular DiseaseCerebrovascular Disease Peripheral Vascular DiseasePeripheral Vascular Disease

Type II DiabetesType II Diabetes

What are some of the clinical features that What are some of the clinical features that are associated with DM 2?are associated with DM 2?
polydipsiapolydipsia polyuriapolyuria Blurry visionBlurry vision Age: greater than 30Age: greater than 30 Race: African American, Native Race: African American, Native
American, Hispanics, AsiansAmerican, Hispanics, Asians Associated with HTN, DyslipidemiaAssociated with HTN, Dyslipidemia

A pregnant 28 y.o presents to your A pregnant 28 y.o presents to your office with elevated glucose levelsoffice with elevated glucose levels
What is the DX?What is the DX?
-Gestational Diabetes-Gestational Diabetes
What are some of theWhat are some of the
Complications associatedComplications associated
with this disease?with this disease?
-Birth defects,-Birth defects,
-Fatal macrosomnia-Fatal macrosomnia
-Birth trauma-Birth trauma
-Resp. distress-Resp. distress

What are some dermatological What are some dermatological findings associated with DM 2?findings associated with DM 2?
Acanthosis nicgricansAcanthosis nicgricans Xanthomas Xanthomas UlcerationsUlcerations GangreneGangrene Necrobiosis LipoidicaNecrobiosis Lipoidica

What would you expect to see on a What would you expect to see on a urine dip stick?urine dip stick? GlycosuriaGlycosuria ProteinuriaProteinuria Very little ketoneuriaVery little ketoneuria
What are some complications that What are some complications that are associated with DM 2?are associated with DM 2?
Peripheral neuropathyPeripheral neuropathy AtherosclerosisAtherosclerosis RetinopathyRetinopathy PVDPVD Nephropathy Nephropathy
A patient presents with the A patient presents with the following symptoms:following symptoms:
Chronic watery diarrhea Chronic watery diarrhea Weight loss Weight loss Colickly abdominal pain Colickly abdominal pain *FLUSHING and Dehydration**FLUSHING and Dehydration*
What is the Dx? VipomaWhat is the Dx? Vipoma