emergency department overcrowding and increased length of stay: identifying the causes in a...
TRANSCRIPT
0 20 40 60 80 100
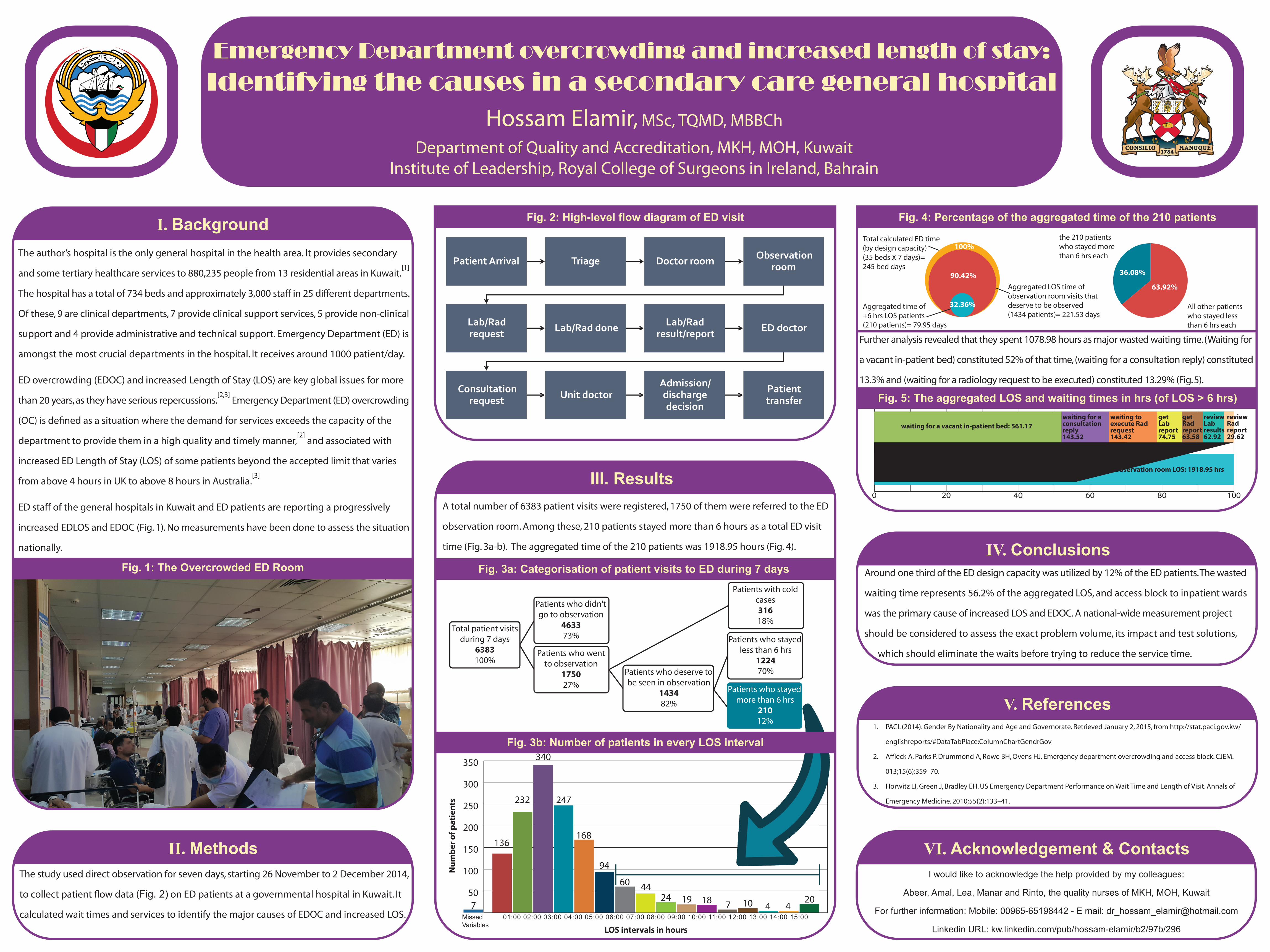
waiting for a vacant in-patient bed: 561.17
Total ED observation room LOS: 1918.95 hrsMajor waste time: 1078.98 hrs
waiting for a consultation reply143.52
waiting to execute Rad request 143.42
getLab report74.75
get Rad report 63.58
review Lab results 62.92
review Rad report 29.62
450
100
150
200
250
300
350
Missed 01:00 02:00 03:00 04:00 05:00 06:00 07:00 08:00 09:00 10:00 11:00 12:00 13:00 14:00 15:00Variables
7
136
232
340
247
168
60 4424 19 18 7 10 4
20
94
LOS intervals in hours
Num
ber o
f pat
ient
s
Emergency Department overcrowding and increased length of stay:Identifying the causes in a secondary care general hospital
Hossam Elamir, MSc, TQMD, MBBCh
Department of Quality and Accreditation, MKH, MOH, KuwaitInstitute of Leadership, Royal College of Surgeons in Ireland, Bahrain
I. BackgroundThe author’s hospital is the only general hospital in the health area. It provides secondary
and some tertiary healthcare services to 880,235 people from 13 residential areas in Kuwait.[1]
The hospital has a total of 734 beds and approximately 3,000 staff in 25 different departments.
Of these, 9 are clinical departments, 7 provide clinical support services, 5 provide non-clinical
support and 4 provide administrative and technical support. Emergency Department (ED) is
amongst the most crucial departments in the hospital. It receives around 1000 patient/day.
ED overcrowding (EDOC) and increased Length of Stay (LOS) are key global issues for more
than 20 years, as they have serious repercussions.[2,3]
Emergency Department (ED) overcrowding
(OC) is defined as a situation where the demand for services exceeds the capacity of the
department to provide them in a high quality and timely manner,[2]
and associated with
increased ED Length of Stay (LOS) of some patients beyond the accepted limit that varies
from above 4 hours in UK to above 8 hours in Australia.[3]
ED staff of the general hospitals in Kuwait and ED patients are reporting a progressively
increased EDLOS and EDOC (Fig. 1). No measurements have been done to assess the situation
nationally.
The study used direct observation for seven days, starting 26 November to 2 December 2014,
to collect patient flow data (Fig. 2) on ED patients at a governmental hospital in Kuwait. It
calculated wait times and services to identify the major causes of EDOC and increased LOS.
Fig. 1: The Overcrowded ED Room
Fig. 2: High-level flow diagram of ED visit
Fig. 3a: Categorisation of patient visits to ED during 7 days
Fig. 3b: Number of patients in every LOS interval
Fig. 4: Percentage of the aggregated time of the 210 patients
Fig. 5: The aggregated LOS and waiting times in hrs (of LOS > 6 hrs)
IV. Conclusions
V. References
II. MethodsI would like to acknowledge the help provided by my colleagues:
Abeer, Amal, Lea, Manar and Rinto, the quality nurses of MKH, MOH, Kuwait
For further information: Mobile: 00965-65198442 - E mail: [email protected]
Linkedin URL: kw.linkedin.com/pub/hossam-elamir/b2/97b/296
1. PACI. (2014). Gender By Nationality and Age and Governorate. Retrieved January 2, 2015, from http://stat.paci.gov.kw/
englishreports/#DataTabPlace:ColumnChartGendrGov
2. Affleck A, Parks P, Drummond A, Rowe BH, Ovens HJ. Emergency department overcrowding and access block. CJEM.
013;15(6):359–70.
3. Horwitz LI, Green J, Bradley EH. US Emergency Department Performance on Wait Time and Length of Visit. Annals of
Emergency Medicine. 2010;55(2):133–41.
Around one third of the ED design capacity was utilized by 12% of the ED patients. The wasted
waiting time represents 56.2% of the aggregated LOS, and access block to inpatient wards
was the primary cause of increased LOS and EDOC. A national-wide measurement project
should be considered to assess the exact problem volume, its impact and test solutions,
which should eliminate the waits before trying to reduce the service time.
VI. Acknowledgement & Contacts
A total number of 6383 patient visits were registered, 1750 of them were referred to the ED
observation room. Among these, 210 patients stayed more than 6 hours as a total ED visit
time (Fig. 3a-b). The aggregated time of the 210 patients was 1918.95 hours (Fig. 4).
III. Results
Total patient visits during 7 days
6383100%
Patients who didn't go to observation
463373%
Patients who went to observation
175027%
Patients who deserve to be seen in observation
143482%
Patients with cold cases31618%
Patients who stayed less than 6 hrs
122470%
Patients who stayed more than 6 hrs
21012%
Patient Arrival Triage Doctor room Observation room
Lab/Rad request Lab/Rad done Lab/Rad
result/report ED doctor
Consultation request Unit doctor
Admission/ discharge decision
Patient transfer
Further analysis revealed that they spent 1078.98 hours as major wasted waiting time. (Waiting for
a vacant in-patient bed) constituted 52% of that time, (waiting for a consultation reply) constituted
13.3% and (waiting for a radiology request to be executed) constituted 13.29% (Fig. 5).
Total calculated ED time(by design capacity)(35 beds X 7 days)=245 bed days
Aggregated LOS time ofobservation room visits that deserve to be observed(1434 patients)= 221.53 days
Aggregated time of+6 hrs LOS patients (210 patients)= 79.95 days
the 210 patients who stayed more than 6 hrs each
All other patients who stayed less than 6 hrs each
100%
90.42%
32.36%
36.08%
63.92%