electronic prescribing problems reported to the pharmacy and provider eprescribing experience...
TRANSCRIPT

Research in Social and
Administrative Pharmacy j (2013) j–j
Original Research
Electronic prescribing problems reportedto the Pharmacy and Provider ePrescribing Experience
Reporting (PEER) portalAna L. Hincapie, Ph.D.a,*, Terri Warholak, Ph.D.b,
Ahmed Altyar, Pharm.D.b, Rebecca Snead, B.S.Pharm.c,Tara Modisett, B.S.d
aCalifornia Northstate University, College of Pharmacy, 10811 International Dr., Rancho Cordova, CA 95670, USAbUniversity of Arizona, College of Pharmacy, Tucson, AZ, USA
cNational Alliance of State Pharmacy Associations, Richmond, VA, USAdAlliance for Patient Medication Safety, Richmond, VA, USA
Abstract
Background: Electronic prescribing (e-prescribing) may prevent medication errors caused by prescriptionillegibility; however, information technologies also may introduce different kinds of medication errors.
Objective: To identify and quantify e-prescribing problems reported through an electronic prescribingincident reporting tool in the United States.Methods: Voluntary and anonymous reports to a web-based, e-prescribing incident reporting tool were
collected during 18 months using convenience sampling. Questions in the reporting tool were designed toelicit information on pharmacists’ experiences with e-prescribing. Data were analyzed to characterize thedifferent types of e-prescribing concerns.
Results: A total of 484 reports were collected through the incident reporting tool. Out of 484 reports, 75%corresponded to electronic prescriptions received directly into pharmacies’ computers and 23% werecomputer-generated prescriptions faxed to pharmacies. Most of reports corresponded to comments,complaints or identified unsafe conditions regarding electronic prescriptions (49%), followed by incidents
that did not reach the patient (44%) and those that reached patients (6%). The majority of problemsreported involved directions (24%) and quantity selection (12%).Conclusion: The use of an incident reporting tool revealed a variety of issues regarding e-prescribing. The
majority of the issues reported in this study were related to directions and quantity selection. The findingsin this study indicate that software system changes and appropriate prescriber training are required todecrease or eliminate some of these issues.
� 2013 Elsevier Inc. All rights reserved.
Tara Modisett is employed by the Alliance for Patient Medication Safety, which provided funding for
the research reported in this article. The other authors declare no conflicts of interest or financial interests
in any product or service mentioned in this article, including grants, employment, gifts, stock holdings, or
honoraria.Funding: Partial funding for this evaluation was provided by the Alliance for Patient Medication Safety with sup-
port from the Community Pharmacy Foundation.
* Corresponding author. Tel.: þ1 916 503 1889.
E-mail address: [email protected] (A.L. Hincapie).
1551-7411/$ - see front matter � 2013 Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.sapharm.2013.08.007

2 Hincapie et al. / Research in Social and Administrative Pharmacy j (2013) 1–9
Keywords: Electronic prescribing; Community pharmacies; Error reporting system
Introduction
Electronic prescribing (e-prescribing) is a typeof health information technology that allowsprescribers to securely send electronic prescrip-
tions directly to pharmacies using specific soft-ware.1 Many benefits have been attributed toe-prescribing such as reduction in medicationerrors, streamlined refill processes, better formu-
lary management and improved efficiency for pre-scribers and pharmacists.2,3 However, severalstudies have documented e-prescribing system
challenges; e-prescription error rates may notbe lower than those for other modes of transmis-sion4 (i.e., paper, fax, telephone), and there is
some evidence that pharmacists must interveneon electronic prescriptions as often as they doon handwritten prescriptions.5,6 The Institute of
Medicine 2012 report “Health IT and PatientSafety: Building Safer Systems for Better Care”highlighted the risks to health care of health infor-mation technologies improperly designed or
implemented.7 During 2011 in the United States(US), almost two thirds of all dispensed prescrip-tions were electronically prescribed; this repre-
sents a 75% increase from the previous year.8
This increase in electronic prescriptions occurred,in part, due to the momentum generated with the
Centers for Medicare and Medicaid Services(CMS) E-prescribing Incentive Program.9 Since2009, this program has provided financial incen-tives to qualifying prescribers who transmit pre-
scriptions electronically. In 2012, the programbegan to apply penalties in form of medicarepayment adjustments for professionals not using
e-prescribing.9 Pharmacists should expect toreceive more prescriptions electronically. Thus,they should be aware of the potential unintended
consequences of e-prescribing.The Alliance for Patient Medication Safety
(APMS), a non profit institution and a federally
listed Patient Safety Organization, developedan e-prescribing incident reporting system: thePharmacy and Provider ePrescribing ExperienceReporting (PEER) data portal to identify the
problems experienced with e-prescribing.10 Themission of APMS is to foster a culture of qualitywithin the profession of pharmacy that promotes
a continuous systems analysis to develop bestpractices to reduce medication errors, improve
medication use and enhance patient care. APMS
collects the data directly using a securedweb-portal. Each report becomes part of a largedatabase of reports from many different users.
Summary data are shared with professional asso-ciations, technology groups, e-prescribing andpharmacy system vendors, and legislators.
Objective
The objective of this study was to identifyand quantify e-prescribing problems voluntarily
reported through the PEER portal.
Methods
Data collection
APMS launched the PEER portal at the end of
October 2010. The portal is available free ofcharge to anyone who has an Internet connection.State pharmacy associations worked with APMS
to promote use of the PEER portal by addinga PEER portal link on their websites and bysharing information in their electronic newsletters
and other publications. APMS also spoke aboutthe portal during member presentations, such ascontinuing education programs on medication
safety and quality assurance. Additional outreachwas made to several national pharmacists’ associ-ations, many of which also promoted the portal totheir members.
This study used convenience sampling design.Voluntary and anonymous reports to the PEERportal were collected between October 2010 and
April 2012.
Instrument
The PEER portal was intended to providepharmacists with a tool to report their e-prescribingexperience from any internet-compatible device.
The PEER reporting instrument was designedbased on investigator (TW)-published articlesin the field of e-prescribing and community
pharmacy.11 APMS assessed the PEER portal con-tent validity. The instrument can be found atwww.pqc.net/eprescribe, and a copy can be found
in the Appendix. The e-prescribing problems cate-gories used in the reporting instrument included in-cident or error, near miss, and unsafe conditions.

3Hincapie et al. / Research in Social and Administrative Pharmacy j (2013) 1–9
An incident or error was defined as the event thatreached the patient regardless of the degree ofharm or the clinical significance.12 Reaching thepatient meant that the prescription product left
the control of the pharmacy and was in the posses-sion of the patient or patient’s caregiver. A nearmiss was defined as the event that was detected
and corrected before the patient took possessionof the prescription product. Finally, an unsafe con-dition, complaint, or comment for improvement re-
fers to an event that did not involve a specificprescription order or patient. Reporters were di-rected to select this category if they wished to re-
port: a potential problem, design flaw or defectthat could result in harm in the future; a complaintabout an e-prescribing design feature thatmay indi-cate a flawor future risk; or a possible improvement
to the e-prescribing process to reduce the risk ofa future error. In accordance with the regulationsof Patient Safety Organizations, neither informa-
tion identifying the person reporting to the PEERportal nor the site type at which the reporter isworking (chain or independent pharmacy or
name or organization) are captured by the PEERportal.
Other data collected included: reporter type
(pharmacist, technician, technician, nurse, etc.);reporter’s practice site (pharmacy, hospital, med-ical clinic, long term care, other); name of com-puter system if known; name of e-prescribing
system if known; prescribed drug name; the issuewith the electric prescription (incorrect patient,dose selection, dosage form selection, route selec-
tion, SIG/directions, electronic prescription con-tains conflicting information, etc.); the person whofirst identified the problem (pharmacist, technician,
technician, nurse, patient, etc.); free text descrip-tion of the issue encountered; time in minutes spentdirectly resolving the issue; total elapsed time inhours and minutes until the issue was fully re-
solved; and type of electronic prescription (com-puter-generated fax to pharmacy, electronicprescription received directly into pharmacy com-
puter system, other). Computer-generated faxeswere included because the sending of a computer-generated fax to the pharmacy involves the use of
prescriber-side e-prescribing systems.
Data analysis
Reports were received in tabular form. In-vestigators AH and AA analyzed the data. Uni-
variate summary statistics were calculated for thereports and analyzed using STATA 11.0. Thisstudy received IRB approval from the Office for
the Responsible Conduct of Research at theUniversity of Arizona.
Results
From October 1, 2010 until April 1, 2012,a total of 484 reports were collected throughthe PEER portal. Pharmacists reported 85%
(n ¼ 412) of incidents, technicians 11% (n ¼ 54),pharmacy students 3% (n ¼ 16), physicians0.2% (n ¼ 1) and, nurses 0.2% (n ¼ 1). The
majority of incident reports (98% n ¼ 474) camefrom pharmacies, 1% (n ¼ 7) from medical officesand two reports came from other unspecified set-
tings. In accordance with the regulations ofPatient Safety Organizations, the PEER portaldoes not capture the name or type of the site atwhich the reporter is working. Therefore, it is
not possible to tell how many pharmacies or dif-ferent pharmacists contributed to this data set.
Type of electronic prescription
Of 484 reports, 75% (n ¼ 364) corresponded to
electronic prescriptions received directly intopharmacies’ computers and 23% (n ¼ 110) in-volved computer-generated prescriptions faxed
to pharmacies. In ten reports, the prescriptionswere computer-generated and hard copies werebrought into pharmacies.
Type of e-prescribing problem
Nearly half of the e-prescribing problems
reported through the PEER portal (n ¼ 239) werecategorized as comments, complaints, or unsafeconditions regarding electronic prescriptions.
Forty-four percent, the second most common typeof error, were near misses (n ¼ 215). In 6% of re-ports (n ¼ 30), the incident reached the patient.
This percentage distribution was similar by pre-scription type (data not shown). A review of thecomments received in this category revealed the po-tential of harm to patients. For example, a pharma-
cist indicated that a patient with elevated levels ofserum creatinine received two fills of the inappro-priate medication strength. The reporter indicated
that the root cause of this error was a mismatch ofthe drug naming formats between the prescriber’se-prescribing system and the pharmacy system.
Person identifying error
Pharmacists identified more than two thirdsof e-prescribing problems reported (n ¼ 355) fol-lowed by pharmacy technicians (n ¼ 99). When
4 Hincapie et al. / Research in Social and Administrative Pharmacy j (2013) 1–9
the problem reached the patient (n ¼ 30), the pa-tient himself was first identified the error in 47%of reports (n ¼ 14) while pharmacists identified
the issue in 30% of these reports (n ¼ 9).
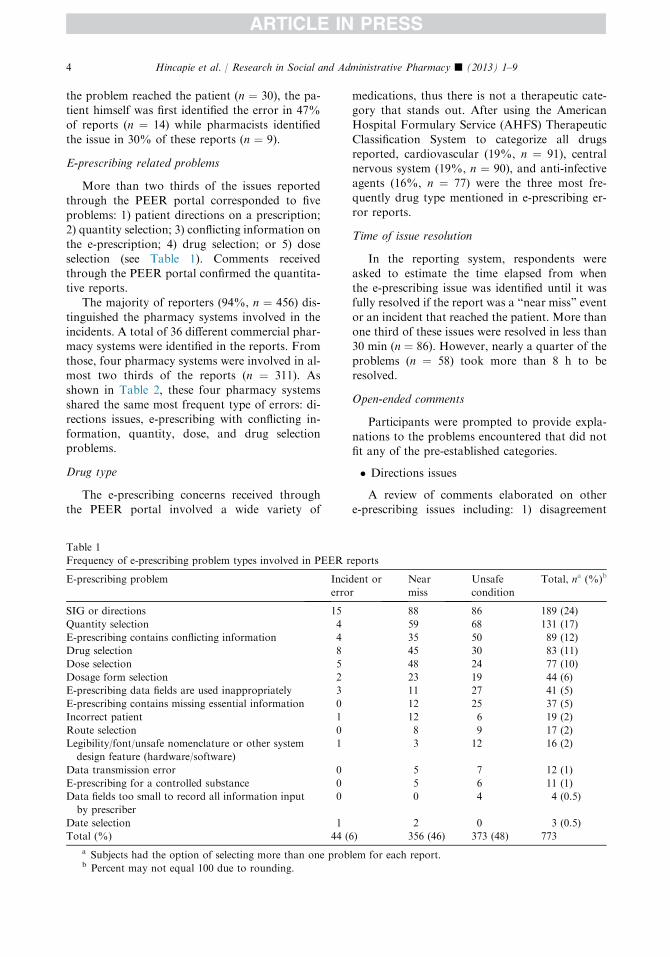
E-prescribing related problems
More than two thirds of the issues reportedthrough the PEER portal corresponded to five
problems: 1) patient directions on a prescription;2) quantity selection; 3) conflicting information onthe e-prescription; 4) drug selection; or 5) doseselection (see Table 1). Comments received
through the PEER portal confirmed the quantita-tive reports.
The majority of reporters (94%, n ¼ 456) dis-
tinguished the pharmacy systems involved in theincidents. A total of 36 different commercial phar-macy systems were identified in the reports. From
those, four pharmacy systems were involved in al-most two thirds of the reports (n ¼ 311). Asshown in Table 2, these four pharmacy systems
shared the same most frequent type of errors: di-rections issues, e-prescribing with conflicting in-formation, quantity, dose, and drug selectionproblems.
Drug type
The e-prescribing concerns received throughthe PEER portal involved a wide variety of
Table 1
Frequency of e-prescribing problem types involved in PEER r
E-prescribing problem Incid
erro
SIG or directions 15
Quantity selection 4
E-prescribing contains conflicting information 4
Drug selection 8
Dose selection 5
Dosage form selection 2
E-prescribing data fields are used inappropriately 3
E-prescribing contains missing essential information 0
Incorrect patient 1
Route selection 0
Legibility/font/unsafe nomenclature or other system
design feature (hardware/software)
1
Data transmission error 0
E-prescribing for a controlled substance 0
Data fields too small to record all information input
by prescriber
0
Date selection 1
Total (%) 44 (
a Subjects had the option of selecting more than one probb Percent may not equal 100 due to rounding.
medications, thus there is not a therapeutic cate-gory that stands out. After using the AmericanHospital Formulary Service (AHFS) Therapeutic
Classification System to categorize all drugsreported, cardiovascular (19%, n ¼ 91), centralnervous system (19%, n ¼ 90), and anti-infectiveagents (16%, n ¼ 77) were the three most fre-
quently drug type mentioned in e-prescribing er-ror reports.
Time of issue resolution
In the reporting system, respondents were
asked to estimate the time elapsed from whenthe e-prescribing issue was identified until it wasfully resolved if the report was a “near miss” event
or an incident that reached the patient. More thanone third of these issues were resolved in less than30 min (n ¼ 86). However, nearly a quarter of the
problems (n ¼ 58) took more than 8 h to beresolved.
Open-ended comments
Participants were prompted to provide expla-
nations to the problems encountered that did notfit any of the pre-established categories.
� Directions issues
A review of comments elaborated on othere-prescribing issues including: 1) disagreement
eports
ent or
r
Near
miss
Unsafe
condition
Total, na (%)b
88 86 189 (24)
59 68 131 (17)
35 50 89 (12)
45 30 83 (11)
48 24 77 (10)
23 19 44 (6)
11 27 41 (5)
12 25 37 (5)
12 6 19 (2)
8 9 17 (2)
3 12 16 (2)
5 7 12 (1)
5 6 11 (1)
0 4 4 (0.5)
2 0 3 (0.5)
6) 356 (46) 373 (48) 773
lem for each report.

Table 2
E-prescribing problems by pharmacy systems
Pharmacy system
(no. of problemsa)
Top four most common e-prescribing
problems
Frequency (%)
System A (n ¼ 173) SIG 41 (24)
Dose selection 23 (13)
E-prescribing with conflicting information 19 (11)
Quantity selection 18 (10)
System B (n ¼ 150) SIG 44 (29)
E-prescribing with conflicting information 23 (15)
Quantity selection 19 (13)
Drug selection 17 (11)
System C (n ¼ 102) SIG 26 (25)
Quantity selection 19 (19)
E-prescribing with conflicting information 16 (16)
Drug selection 10 (10)
System D (n ¼ 40) Quantity selection 13 (32)
SIG 10 (25)
Drug selection 6 (15)
Dose selection 5 (12)
SIG ¼ patient directions on a prescription.a Subjects had the option of selecting more than one problem for each report.
5Hincapie et al. / Research in Social and Administrative Pharmacy j (2013) 1–9
between directions and drug route; 2) strengths
that do not match the directions; and 3) packagesize that conflicts with the directions. Addi-tionally, respondents indicated that, due to limi-
tations in provider-side e-prescribing systems,compounded medication prescriptions often aresent to pharmacies with insufficient informationregarding the final concentration desired and
prescriptions for dosage forms such as inhalersare frequently transmitted with incorrect packagesizes. Specifically, reporters suggested that these
errors occur because default directions are avail-able but prescribers may not verify them beforetransmitting the e-prescription. Also, reporters
indicated that prescribers might be allowingimproperly trained medical staff to send refillprescriptions, which may increase the likelihoodof error.
� Duplicate prescriptions
Twenty-three (6%) reporters indicated that
receiving duplicate e-prescriptions is a commonproblem faced by pharmacies, which createsadditional work for staff. Electronic prescriptions
sent to the wrong pharmacy were also a concernfor respondents.
� Matching prescriptions
This study revealed problems with the patientmatching process used by some e-prescribing
systems. Reporters indicated that patients’ de-
mographic data in pharmacy computer systemsand prescriber computer systems are often differ-ent, which makes patient matching difficult. In
addition, reporters indicated that prescribers oc-casionally select the incorrect patient when send-ing an e-prescription.
� E-prescription format
It was reported that some pharmacies fre-quently received e-prescriptions that look indis-
tinguishable from emails where data were outlinedin different formats depending on the prescribers’system. In this situation, pharmacy staff reported
spending more time finding and verifying pre-scription information. Additionally, participantsindicated that many prescriptions are sent withoutprescribers’ license information or phone number.
Finally, some pharmacies reported not receivingallergy information on the e-prescriptions andtherefore additional time was spent gathering
such data.Through the reporting system, it was noticed
that some systems do not facilitate the compliance
of e-prescriptions laws for controlled substances,thus prescribers are still sending e-prescriptionsthat do not meet regulations. A reporter indicated
that in his/her state it is required to handwrite“brand necessary” when required. Therefore, whenprescriptions requiring brand-name medications

6 Hincapie et al. / Research in Social and Administrative Pharmacy j (2013) 1–9
are e-prescribed it is necessary to contact thephysician to send a handwritten prescription tomeet state requirements. Also, it was revealed that
some systems do not contain updated formularyinformation; often these formularies containedmedications that are no longer available on themarket or whose name has changed.
� Human-system interaction
Finally, auto-population capacity on prescriber-
side systems may allow providers to select incorrectmedications. A common mistake reported in thisstudy was the inability to discriminate between
different salts of the same drug.
Discussion
Over 400 reports were submitted to the PEERportal during the study period. The most com-
monly reported e-prescribing problem was re-lated to patient directions on the e-prescription.This problem may be related to the variability in
how directions can be sent to pharmacies; thismay prompt the pharmacist to ask for clarifica-tion in order to prevent a medication error (e.g.,
nasal spray directions populated as inhale twotimes by mouth daily). This finding is consistentwith those of previous investigations5,6 and sug-
gests that direction auto-population feature ofprescriber systems may contribute to these prob-lems. It also appears that when directions arechanged during prescribing, the quantity is also
erased in some systems and prescribers may failto notice. This may explain why some e-prescrip-tions for refills are sent with missing quantities.
Standards issued by a national organizationsuch as the Office of the National Coordinatorfor Health Information Technology to increase
the consistency of prescription directions andmedication names (Structured and Codified SIGand Rx Norm) may help decrease the percentage
of missing prescription information transmittedto the pharmacy.
Other commonly reported problems with e-prescriptions interventions were quantity, drug,
dose selection, and dose issues, which are in linewith previous research.6,11,13–19 These problemswere prevalent in the most common e-prescribing
system used suggesting that improvements in themajor e-prescribing vendor systems would havea significant impact on medication safety. This
study revealed that duplicate e-prescriptions area common problem for pharmacists. There is lim-ited evidence documenting this problem in the
literature.15 Thus, future research should exploreprevalence of this issue and its root causes. Partic-ipants suggested that duplications might occur
because, in some occasions, prescribers transmitthe same prescription via several different convey-ance methods to ensure delivery (i.e., e-prescrip-tion plus either and fax or phone). Prescription
insurance might sometimes detect these dup-licate claims during adjudication but if patientspay cash they could get multiple fills of the
same medication. This could be prevented if alle-prescribing systems could generate a messageto prescribers when the prescription is received
and being processed or if prescribers knew howto access these logs.
This study found problems related with in-correct patient name matching for e-prescriptions.
This may occur because some pharmacy computersystems do not allow the linking of incomingelectronic prescriptions to the patients’ current
pharmacy profile if validation is not completedusing the US Social Security Number. However,Social Security Numbers are not easily collected
due to the current social environment and con-cerns for patient privacy. Without an exact match,the incorrect patient can be easily selected; such
a mistake may go unnoticed by pharmacy staff.It is important to highlight that only 6% of
the 484 e-prescribing problems reported reachedpatients. This suggests that pharmacists are iden-
tifying and intervening on many e-prescriptionproblems before they reach the patient; this maypositively impact patient health and safety. Addi-
tional research concerning the severity and extentof patient harm prevented from pharmacists’interventions on e-prescribing related issues is
needed.One might wonder if the problems identified
in this analysis exist with prescribing vendorsoftware, if they are caused by problems with
the interface between the e-prescribing system andthe pharmacy system, or if they are artifactsof pharmacy information systems. While deter-
mining the root cause or causes are importantfor eliminating the problems, the first step isto recognize and report problems, as without
this the root causes will never be identified.Therefore, it is imperative that all who identifyproblems with the e-prescribing system report
them. While the vendor names are not reportedin this manuscript, the PSO reports data to thevendors aggregated and stratified by vendor sothat vendors can use this information to improve
their systems.

Table 3
Five recommendations to identify or prevent e-prescrib-
ing errors
1. Pharmacists should always ask patients about the
intended reason for use of each medication during
counseling. This information can help pharmacists
identify drop-down menu selection errors on the
prescriber side that might not be otherwise detectable
without a diagnosis.
2. Pharmacists and management staff should work to-
gether to anticipate direction problems and alert all
pharmacy staff to this possibility; policies and pro-
cedures to check and eliminate these errors should be
developed
3. Pharmacists should contact provider practices and
inform them about the error types most commonly
seen from their practices; this is especially relevant for
problems that can be resolved by end-user training.
4. Pharmacists should send messages electronically to
prescribers via pharmacy software systems when re-
questing authorization to make prescription changes
in order to streamline the process. If pharmacists are
unsure whether their system has this feature, they
should contact their software vendor.
5. Pharmacists should report e-prescribing problems
directly to software vendors or via official company
approved channels, provide specific examples of
problematic prescriptions, and follow-up until issues
are resolved. If problems are not reported the systems
will not be fixed on a systems level.
7Hincapie et al. / Research in Social and Administrative Pharmacy j (2013) 1–9
While e-prescribing systems are being im-proved continuously, the current study’s resultsare important because they demonstrate thatreporting systems to a PSO have a critical impact.
That is, the PSO serves as a platform forreporting and aggregating problems so thate-prescribing system root causes can be identified
and resolved. It is important for all health careproviders to understand that reporting platformsexist, to know how to use them, and to see that
results are being filtered back to the technologycompanies so that system improvements canbe made. Seeing this positive change can help
those reporting the problems understand thatthese data do not just fall “into a black hole,”but rather are used to produce improvementsfor the systems we all use. It is hoped that
evidence such as that gleaned from this studywill increase e-prescribing problem identificationand reporting.
Despite the increasing adoption of e-prescrib-ing, problems remain that can potentially affectpatients’ safety and decrease of pharmacists’
efficiency at work. Improvements need to bemade to e-prescribing systems (both prescriberand pharmacy-side systems) to prevent errors
such as those presented from this study. Recom-mendations for e-prescribing software improve-ment have been previously issued.14 From theresults in this study, the design of some systems
still facilitates errors. While awaiting systems im-provements, front-line pharmacists may prevente-prescribing errors in different ways (see
Table 3). The PEER portal will remain open aftergrant funding ends and data collected through itwill be compared to data coming from other
patient safety organizations and the largest e-pre-scribing network operator in order to develop bestpractice recommendations and to work with tech-nology vendors to make system improvements.
Limitations
This study had several limitations. The in-strument used was only content-validated; there-
fore, the results might be subject to measurementerror. The reporting methodology required phar-macists or prescribers to take the time to docu-
ment e-prescribing problems. Given thenotoriously hectic practice environments for phar-macists and prescribers, it is likely that significant
underreporting occurred. Because most of thereports received for this study were from commu-nity pharmacies, it is possible that some
problematic e-prescriptions were identified by
clinical systems at the prescriber site or by anintermediary (e.g., claims processor) before theirreceipt by the pharmacy. Finally, the sample size
for this study is relatively small compared to thenumber of e-prescriptions submitted annually inthe US.8 Additional research to quantify the trueincidence of prescribing problems occurring with
e-prescriptions should consider these issues whendesigning study methodology.
Conclusion
The use of an incident reporting tool revealed
a variety of issues with e-prescribing. The majorityof the issues reported in this study were related topatient directions and quantity selection. The
findings in this study reinforce that softwaresystem changes and appropriate prescribers train-ing are required to decrease or eliminate some of
these issues, and pharmacists should be aware ofthe potential errors generated by e-prescribingsystems.

8 Hincapie et al. / Research in Social and Administrative Pharmacy j (2013) 1–9
References
1. Surescripts. A Clinician’s Guide to E-prescribing,
2011. Available at: http://www.surescripts.com/
media/647028/final_clinicians_guide_for_distribution_
download.pdf. Accessed 13.06.13.
2. Corley ST. Electronic prescribing: a review of costs
and benefits. Top Health Inf Manage 2003;24:29.
3. Ammenwerth E, Schnell-Inderst P, Machan C,
Siebert U. The effect of electronic prescribing
on medication errors and adverse drug events:
a systematic review. J Am Med Inform Assoc 2008;
15:585–600.
4. Koppel R, Metlay JP, Cohen A, et al. Role of com-
puterized physician order entry systems in facilitating
medication errors. JAMA 2005;293:1197.
5. Warholak TL, Rupp MT. Analysis of community
chain pharmacists’ interventions on electronic pre-
scriptions. J Am Pharm Assoc 2009;49:59–64.
6. Gilligan AM, Miller K, Mohney A, Montenegro C,
Schwarz J, Warholak TL. Analysis of pharmacists’
interventions on electronic versus traditional pre-
scriptions in 2 community pharmacies. Res Soc
Adm Pharm 2012;8:523–532.
7. IOM. Health IT and Patient Safety: Building Safer
Systems for Better Care. The National Academy
Press; 2011.
8. Surescripts. The National Progress Report on E-
prescribing and Interoperable Health Care, 2011.
Available at: http://www.surescripts.com/about-e-
prescribing/progress-reports/national-progress-reports.
aspx.
9. Kan JT. 2012 Electronic Prescribing Incentive Pro-
gram. J Oncol Pract 2012;8:121–123.
10. Hincapie AL, Warholak TL. Electronic prescribing
errors: do they exist? J Am Pharm Assoc 2012;52:
302–303.
11. Rupp MT, Warholak TL. Evaluation of e-prescrib-
ing in chain community pharmacy: best-practice rec-
ommendations. J Am Pharm Assoc 2008;48:364–370.
12. World Health Organization. The Conceptual Frame-
work for the International Classification for Patient
Safety. World Health Organization; 2009;1–149.
13. Clauson KA, Alkhateeb FM, Lugo KD,
Khanfar NM. E-prescribing: attitudes and percep-
tions of community pharmacists in Puerto Rico. Int
J Electron Healthc 2011;6:34–46.
14. Grossman JM, Cross DA, Boukus ER, Cohen GR.
Transmitting and processing electronic prescriptions:
experiences of physician practices and pharmacies.
J Am Med Inform Assoc 2012;19:353–359.
15. Lapane KL, Waring ME, Schneider KL, Dube C,
Quilliam BJ. A mixed method study of the merits of
e-prescribing drug alerts in primary care. J Gen Intern
Med 2008;23:442–446.
16. OdukoyaO, ChuiMA.Retail pharmacy staff percep-
tions of design strengths and weaknesses of electronic
prescribing. J Am Med Inform Assoc 2012;19(6):
1059–1065.
17. Nanji KC, Rothschild JM, Salzberg C, et al.
Errors associated with outpatient computerized pre-
scribing systems. J Am Med Inform Assoc 2011;18:
767–773.
18. Flynn EA, Barker KN, Berger BA, Lloyd KB,
Brackett PD. Dispensing errors and counseling qual-
ity in 100 pharmacies. J Am Pharm Assoc 2009;49:
171–180.
19. James KL, Barlow D, McArtney R, Hiom S,
Roberts D, Whittlesea C. Incidence, type and causes
of dispensing errors: a review of the literature. Int J
Pharm Pract 2009;17:9–30.
Appendix
Pharmacy and Provider ePrescribing ExperienceReporting Portal (PEER portal)
This portal collects your experiences with
e-prescribing technologies in a confidentialmatter. All comments – whether suggestions forimprovement or complaints about the process –
are welcome. The purpose is to allow the Alliancefor Patient Medication Safety (APMS), a patientsafety organization, to gather detailed informa-tion that may be used to improve the quality and
effectiveness of electronic prescribing technolo-gies. There are 12 questions that can be completedin less than 3 min.
*Unless noted otherwise all fields are required.
1) Type of report
B Incident/error (i.e., event reached the pa-tient with or without harm)
B Near miss (i.e., event did not reach thepatient)
B Unsafe condition/complaints/commentsfor improvement
2) Reporter information
B Pharmacist O Medical office staffB Technician O Nurse practitioner/physi-
cian’s assistant
B Physician O StudentB Nurse O Other
3) Reporter’s practice siteB Pharmacy (including retail, mail-order,
outpatient clinic) O Medical office/clinicB Long-term care/skilled nursing facility/
home care practice O Hospital (inpatientsetting)
B Other:
Reporter’s state/territory: reporter’s zip code(optional):

9Hincapie et al. / Research in Social and Administrative Pharmacy j (2013) 1–9
4) Name of pharmacy computer system, ifknown:
5) Name of e-prescribing system, if known:6) Prescription information: prescribed drug
name: _____7) Type of electronic prescription (please choose
one):
B Computer-generated fax to pharmacyB Electronic prescription received directly
into pharmacy computer
B Other:
8) Please categorize your issue(s) with the elec-tronic prescription you are reporting on(check all that apply):B Incorrect patient (e.g., wrong name, mis-
spelled name, wrong patient)B Controlled substanceB Dose selection
B Dosage form selectionB Quantity selectionB Date selection
B Drug selectionB SIG/directionsB E-prescription contains conflicting infor-
mation
B E-prescription missing essential infor-mation
B E-prescription data fields are used
inappropriatelyB Legibility/font/unsafe nomenclature or
other system design feature (hardware/
software) that increases risk for errorB Data fields too small to record all infor-
mation input by prescriber
B Data transmission error that affects thequality or safety of patient care
B Other:
9) Who first identified the error, near miss or un-safe condition:
B Physician O Nurse practitioner/physi-cian’s assistant
B Nurse O StudentB Pharmacist O Patient/caregiver/family
memberB Technician O Other/unknownB Medical office staff
10) Description of issue encountered – please
provide as much detail as possible (do notrecord the names of any individual, otherpatient identifiers or PHI)
Related files: (optional)If you have files related to this issue you canupload them here. Please do not attempt
to upload files larger 1 GB (1024 MB in to-tal size.
Questions 11 and 12 ask how this event hasaffected your time.
11) Enter the time in minutes (00–99 min) spent
“on task” directly resolving the e-prescribingissue reported above:
Minutes:_____12) Enter the total elapsed time (hours and/or
minutes) from when you first identified thee-prescribing issue until the issue was fullyresolved for that patient:
Hours: _____ Minutes: ______By submitting this form, I understand that theinformation provided to APMS is confidential
and will not be disclosed by APMS to the extentprotected by law, except in a de-identified oraggregated form or in the form of feedback,
such as best practices or systems improvementsthat could result in improved quality of care. Tolearn more about the confidentiality protections,
go to http://www.pso.ahrq.gov/ following day, fora total of 25 h and 30 min (alternatively you couldenter 24 h and 90 min).