elbow arthroscopy: indications, techniques, outcomes, and
TRANSCRIPT
© 2015 AAOS Instructional Course Lectures, Volume 64 215
18
In recent years, increased understand-ing of the anatomy about the elbow and techniques of elbow arthroscopy have emerged. An increased familiarity with arthroscopy in general, and elbow
arthroscopy in particular, now allows surgeons to expand the indications for this procedure. Nevertheless, arthros-copy remains a technique with limita-tions and risks, and recognizing these
will help the surgeon understand how arthroscopy fi ts into surgical practice.
IndicationsIndications for elbow arthroscopy in-clude débridement for septic elbow ar-thritis, synovectomy for infl ammatory arthritis, débridement for osteoarthri-tis, loose body extraction, contracture release, treatment of osteochondral defects and selected fractures or insta-bility, and tennis elbow release, as well as for diagnostic purposes.1-19
ContraindicationsThe potential for neurovascular injury in elbow arthroscopy is higher than in other joints because of the proximity of neurovascular structures to portals and the working fi eld. Elbow arthroscopy ideally is considered when the surgeon has arthroscopic training or arthro-scopic experience in other joints. Prior surgical management about the elbow is, in some patients, a relative contra-indication to elbow arthroscopy. Prior
Elbow Arthroscopy: Indications, Techniques, Outcomes, and Complications
Julie E. Adams, MDGraham J.W. King, MD, MSc, FRCSC
Scott P. Steinmann, MDMark S. Cohen, MD
Dr. Adams or an immediate family member has received royalties from Arthrex, Biomet, and Innovative Medical Device Solutions; serves as a paid consultant to or is an employee of Acumed, Arthrex, Articulinx, Biomet, Elsevier, and Springer; and serves as a board member, owner, offi cer, or committee member of the American Association for Hand Surgery, the Minnesota Orthopaedic Society, and the Ruth Jackson Orthopaedic Society. Dr. King or an immediate family member has received royalties from Wright Medical Technolog y and serves as a paid consultant to or is an employee of Wright Medical Technolog y. Dr. Steinmann or an immediate family member has received royalties from Arthrex, Biomet, and Innovative Medical Device Solutions; serves as a paid consultant to or is an employee of Acumed, Arthrex, Articulinx, Biomet, Elsevier, and Springer; and serves as a board member, owner, offi cer, or committee member of the American Shoulder and Elbow Surgeons and the American Society for Surgery of the Hand. Dr. Cohen or an immediate family member has received royalties from Integra and serves as a paid consultant to or is an employee of Acumed.
AbstractElbow arthroscopy is a tool useful for the treatment of a variety of pathologies about the elbow. The major indications for elbow arthroscopy include débridement for septic elbow arthritis, synovectomy for infl ammatory arthritis, débridement for osteoarthritis, loose body extraction, contracture release, treatment of osteochondral defects and selected fractures or instability, and tennis elbow release. To achieve favorable outcomes after elbow arthroscopy, the surgeon should be aware of contraindications, technical considerations, anatomic princi-ples, and the need for proper patient positioning and portal selection.. Elbow arthroscopy is an effective procedure for the treatment of infl ammatory arthritis, osteoarthritis, and lateral epicondylitis.
Instr Course Lect 2015;64:215–224.
Shoulder and Elbow
216 © 2015 AAOS Instructional Course Lectures, Volume 64
ulnar nerve subcutaneous transposition is not necessarily a contraindication if the ulnar nerve is identifi ed. How ever, prior submuscular or intramuscular ulnar nerve transposition is generally considered a contraindication.20 Some conditions or situations are not ade-quately addressed with arthroscopy and may be better addressed with an open procedure, such as arthritis with widespread joint changes, as evidenced by pain throughout the arc of motion.
Surgical TechniqueRegional or general anesthesia may be used for the procedure. Patient posi-tioning may be supine, prone, or the lat-eral decubitus position. With the lateral decubitus position, the patient is posi-tioned on an infl atable beanbag with an axillary roll beneath the bottom arm, and the affected arm is placed in an arm holder. Care is taken to avoid pressure on or stretching of the brachial plexus, and the arm holder is positioned such that the upper arm is supported without impingement on the antecubital fossa. A tourniquet may be applied (Figure 1).
Standard knee arthroscopy equip-ment and instruments are used, such as a 30° 4.5-mm arthroscope. Solid nontrephinated cannulas are useful be-cause trephinations allow the escape of fl uid from the capsule and joint work-ing area into the soft tissues. Standard arthroscopic biters, graspers, burrs, and shavers are used during the procedure. Shaver suction tubing is, in general, not applied because even when the suction is turned off, some negative pressure is present in the tubing. Retractor de-vices are used as needed during the procedure.
Portal PlacementStandard elbow arthroscopy portals in-clude the anterolateral, antero medial, posterolateral, and direct posterior portals. Accessory portals include the
soft spot portal (direct lateral portal), the distal ulnar portal, and accessory retraction portals in the anterior joint laterally and medially (Figures 2 and 3). Portals and bony and soft-tissue land-marks, including the radiocapitellar joint, the medial and lateral epicondyles, the intramuscular septum, and the olec-ranon, are marked before the procedure begins; fl uid egress alters the surgeon’s ability to palpate these structures. The location of the ulnar nerve is marked, and any subluxation of the ulnar nerve is noted.
The tourniquet is infl ated to 200 to 250 mm Hg. Using an 18-gauge nee-dle, the joint is insuffl ated with 25 to 30 mL of saline through the direct lateral portal or at the fi rst portal site placed; accurate placement into the joint is confi rmed by slight extension of the elbow as fl uid distends the joint.
Preoperative photo-graph demonstrating a patient in the lateral decubitus position. The operative arm is positioned in an arm holder such that the arm may be draped freely to allow complete access to the elbow. (Courtesy of Scott P. Steinmann, MD, Rochester, MN.)
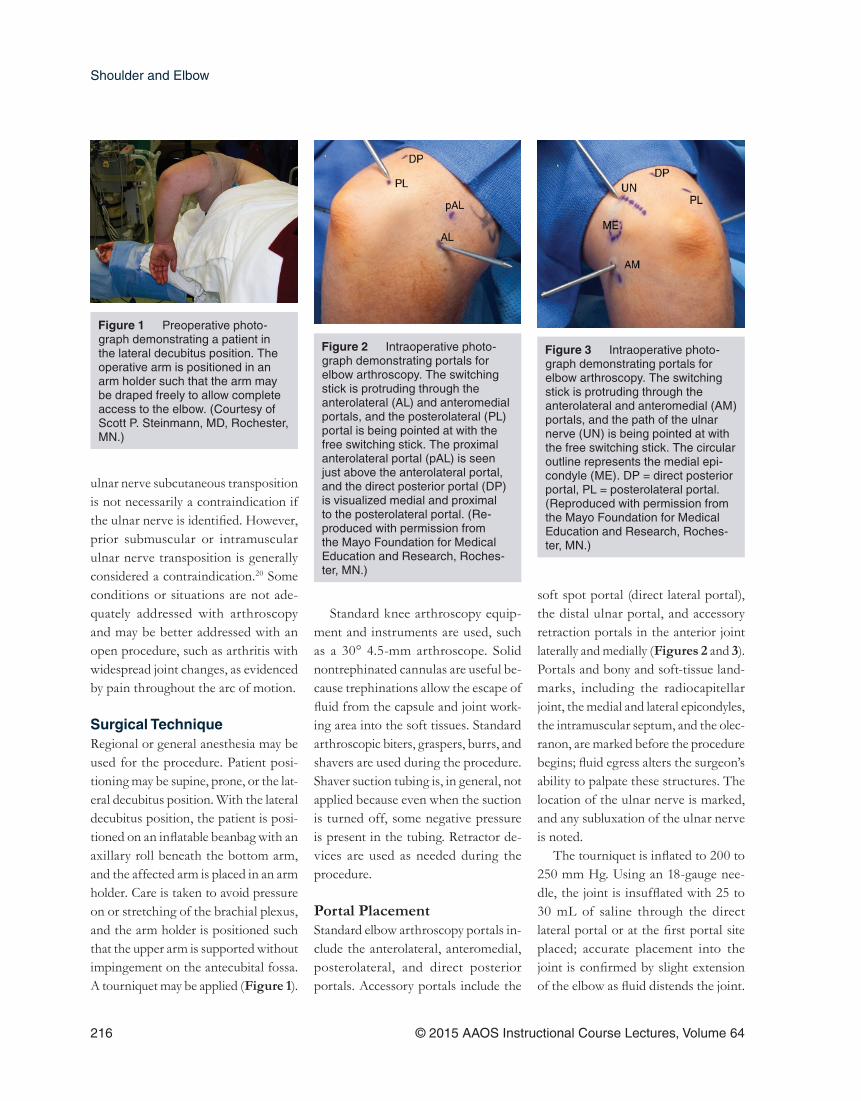
Figure 1
Intraoperative photo-graph demonstrating portals for elbow arthroscopy. The switching stick is protruding through the anterolateral (AL) and anteromedial portals, and the posterolateral (PL) portal is being pointed at with the free switching stick. The proximal anterolateral portal (pAL) is seen just above the anterolateral portal, and the direct posterior portal (DP) is visualized medial and proximal to the posterolateral portal. (Re-produced with permission from the Mayo Foundation for Medical Education and Research, Roches-ter, MN.)
Figure 2 Intraoperative photo-graph demonstrating portals for elbow arthroscopy. The switching stick is protruding through the anterolateral and anteromedial (AM) portals, and the path of the ulnar nerve (UN) is being pointed at with the free switching stick. The circular outline represents the medial epi-condyle (ME). DP = direct posterior portal, PL = posterolateral portal. (Reproduced with permission from the Mayo Foundation for Medical Education and Research, Roches-ter, MN.)
Figure 3

Elbow Arthroscopy: Indications, Techniques, Outcomes, and Complications Chapter 18
© 2015 AAOS Instructional Course Lectures, Volume 64 217
The order of portal placement depends on the preference and experience of the surgeon and the pathology to be addressed.
PortalsAnterolateral The anterolateral portal is placed just anterior to the radiocapitellar joint. More proximal placement increases the margin of safety rather than placement more distally (ie, closer to the poste-rior interosseous nerve). The antero-lateral portal has the smallest margin of safe distance from a neurovascular structure; it is reasonable to create this portal fi rst before fl uid extravasation and distention alter palpable landmarks, although many surgeons prefer starting anteromedially.
For portal placement, the skin only is incised with a No. 15 blade and then dissected bluntly down to the joint. An egress of fl uid confi rms that the joint has been entered. A blunt trocar and an arthroscopy sheath are placed at the portal site.
AnteromedialThe anteromedial portal is located 1 to 2 cm anterior and 1 to 2 cm distal to the medial epicondyle; the portal traverses the fl exor pronator mass and has a high margin of safety from neurovascular structures. This portal may be made after visualizing from the anterolateral portal and palpating to choose the ap-propriate portal site. The portal may be made by an inside-out technique by exchanging the camera for a blunt tro-car and advancing it toward the medial skin. The skin is tented at the portal site, and after the incision for the portal is made, a second sheath may be intro-duced from the medial side, thus allow-ing for this working portal to be used. A
switching stick is often useful when the viewing portal is switched from antero-lateral to anteromedial.
Accessory AnteriorAccessory portals may be placed ante-riorly for retraction. An anteromedial accessory portal is placed just anterior to the supracondylar ridge and intra-muscular septum, 2 cm superior to the medial epicondyle. An anterolateral ac-cessory portal is placed 2 cm superior to the lateral epicondyle, just anterior to the supracondylar ridge.
Direct Lateral or Soft SpotThe direct lateral portal is particularly useful to visualize and treat osteochon-dral defects. It is created through the center of a triangle made between the tips of the olecranon, lateral epicondyle, and radial head. The palpable soft spot is covered by the anconeus.
Distal UlnarThe distal ulnar portal is particularly useful to visualize the posterior capitel-lum, especially for treatment of osteo-chondral defects (Figure 4). The distal ulnar portal is initiated in the skin 3 to 4 cm distal to the radiocapitellar joint. A blunt trocar and sleeve are placed and guided proximally along the lateral bor-der of the ulna to enter the joint.5
Direct PosteriorThe direct posterior portal is placed 2 to 3 cm above the proximal edge of the olecranon. It traverses the thick triceps and requires making an inci-sion through the skin and triceps. A blunt trocar is placed and abrades the posterior humerus to remove posterior olecranon fat to help create a visual-ization space; because this represents a potential space, removal of the fat and
synovium is necessary to create space to visualize the posterior joint. It is useful to place the shaver and blindly shave at the olecranon fossa to remove tissue, taking care to avoid orienting the shaver toward the ulnar nerve.
PosterolateralAfter creation of a working space, the posterolateral portal is used mostly for visualization. This portal is created nearly level with the proximal edge of the olecranon on the posterolateral surface. It offers a relative margin of safety provided that the position of the ulnar nerve is noted, and it has a high
Intraoperative photo-graph demonstrating use of the distal ulnar portal to visualize osteo-chondral lesions. The arthroscope is in the distal ulnar portal, and the shaver is in the direct lateral or soft spot portal. (Reproduced with permission from the Mayo Foun-dation for Medical Education and Research, Rochester, MN.)
Figure 4

Shoulder and Elbow
218 © 2015 AAOS Instructional Course Lectures, Volume 64
margin of safety away from the named neurovascular structures.
ComplicationsJoint space infection is unusual fol-lowing elbow arthroscopy. However, because of the risk of the development of fi stulae or persistent drainage from the joint, the use of sutures is recom-mended, as opposed to the use of thin adhesive strips alone, for closure of the portal sites.21
Although heterotopic ossifi cation appears to be a less common occur-rence after elbow arthroscopy than af-ter open procedures, this complication does occur. The role of, dosage of, and compliance with prophylaxis for hetero-topic ossifi cation is uncertain.12,22
Published reports document injury to all major peripheral nerves about the elbow. In one series of 473 elbow ar-throscopies, the ulnar nerve was most commonly involved, followed by the superfi cial radial nerve, posterior in-terosseous nerve, anterior interosseous nerve, and medial antebrachial cutane-ous nerve, respectively.13,21,23-25
Nerve injury is more common in pa-tients with rheumatoid arthritis because the capsule is thinned or absent, in pro-found preoperative contractures, and in distorted anatomy. Neurovascular inju-ries following elbow arthroscopy may be underreported, and even with care-ful technique, the risk of neurovascular injury cannot be entirely eliminated.13
Arthroscopic Synovectomy for Inflammatory ArthritisSynovectomy is an effective treatment of infl ammatory arthritis of the elbow that is refractory to medical manage-ment. Whereas synovectomy is tradi-tionally performed with open surgery, arthroscopic synovectomy is gaining in
popularity because of its less invasive nature. Relative to other arthroscopic procedures of the elbow, synovec-tomy for rheumatoid arthritis has an increased risk of causing nerve injury because of the distorted anatomy and the thin, weak joint capsule, which nor-mally helps protect the neurovascular structures.21
History and Physical ExaminationPain, swelling, and stiffness are commonly reported with persistent synovitis. It is important to review the underlying disease process and the treatment to date. Examination typi-cally reveals a boggy swelling postero-laterally that is the result of synovitis and effusion. Motion should be doc-umented, and the quality of the end points of motion should be evaluated. A soft end point suggests synovitis or cap-sular contracture, whereas a fi rm end point indicates osseous impingement. Limitation in rotation may be the result of radial head deformity or distal radi-oulnar joint disease. The function of the posterior interosseous and ulnar nerves should be documented because these nerves may be compressed by synovitis. It is critical to locate the ulnar nerve and evaluate it for any subluxation to help avoid injury.
ImagingEvidence of joint destruction on plain radiographs predicts the effi cacy of synovectomy for rheumatoid arthri-tis.26 In the Mayo Clinic Classifi ca-tion, grade I has no osseous changes; grade II has narrowing of the joint space with normal architecture; grade III has damage to the subchondral architecture of the joint, such as thin-ning of the olecranon or resorption of
the trochlea or capitellum; grade IV has gross destruction of the joint; and grade V is ankylosis. CT best defi nes the osseous anatomy. MRI demonstrates the extent of synovitis (Figure 5) and nonossifi ed loose bodies.
Indications and ContraindicationsRheumatoid arthritis is the most com-mon indication for arthroscopic syn-ovectomy of the elbow.26-29 Synovectomy is considered in the setting of persistent, painful synovitis despite good medical management. Patients with some pre-served articular cartilage and only mild bony deformity (Mayo grades I and II) are the best candidates for arthro-scopic synovectomy.27 Younger patients with more advanced disease (Mayo grade III) who are not candidates for elbow arthroplasty also should be con-sidered. Arthroscopic synovectomy is effective in patients with hemophilia who have recurrent elbow hemar-throses despite the use of prophylactic factor replacement.30,31 Arthroscopic sy-novectomy also may be used for psori-atic arthritis and acute septic arthritis.32
MRI demonstrating abundant synovitis in a patient with rheumatoid arthritis. (Courtesy of Graham J.W. King, MD, London, Ontario, Canada.)
Figure 5
Elbow Arthroscopy: Indications, Techniques, Outcomes, and Complications Chapter 18
© 2015 AAOS Instructional Course Lectures, Volume 64 219
Surgical TechniqueFollowing surgical setup of the patient, a nonaggressive full radius resector is used to preserve the integrity of the capsule, thus reducing the risk of nerve injury. Retractors are used as needed on the capsule or muscles to improve visualization. It is important that the shaver not be turned on until it is con-fi rmed that the instruments are within the joint because extensive synovitis may result in a poor initial view. Sy-novium is removed while the capsule is preserved (Figure 6). In infl amma-tory arthritis, the capsule is typically thin and easy to inadvertently penetrate or resect, thus lowering the margin of safety. Particular caution is used when removing the synovium anterior to the radial head because of the proximity of the posterior interosseous nerve; cau-tion also is advised in the posteromedial gutter near the ulnar nerve.
The radial head usually can be re-tained. Excision is reserved for patients with a stable elbow and a radial head deformity that is impeding rotation. Im-pinging osteophytes are removed with a burr or an osteotome. The anterior and/or posterior capsule is released or resected if the patient desires improved motion and has persistent stiffness fol-lowing synovectomy and osteophyte débridement. A bulky soft dressing is applied for comfort.
Postoperative ManagementSynovectomy alone is performed as an outpatient procedure, followed by management consisting of early active range of motion. The patient is in-structed to remove the bulky dressing 48 hours postoperatively and apply light dressings on the portal sites. Sutures are removed at 10 days, and physical therapy is initiated if motion recovery
is slow. Patients undergoing a concom-itant capsulectomy are admitted for 48 hours for early active and passive mo-tion with a continuous brachial plexus block. Management of selected patients with more severe stiffness consists of using a continuous passive motion ma-chine to facilitate the recovery of joint motion. A nighttime static progressive extension splint is used for 12 weeks to retain extension.
ResultsA paucity of data documents the out-comes of arthroscopic synovectomy for rheumatoid arthritis, and there is even less information for other conditions. Arthroscopic synovectomy is less in-vasive than open synovectomy, which may speed recovery and reduce post-operative pain.33,34 Elbow arthroscopy allows the experienced surgeon to bet-ter visualize all areas of the elbow and address intra-articular pathology. Non-randomized reports suggest that the outcomes of arthroscopic synovectomy are comparable to those of open syn-ovectomy. The results deteriorate with time26,27,29 and are better in patients who have preserved articular cartilage and no signifi cant osseous destruction.26,27
Using arthroscopic synovectomy for hemophilic arthropathy de creases the frequency of recurrent hemar-throsis.30,31,35 Nerve injuries, recur-rent synovitis, and persistent pain have been reported after arthroscopic synovectomy.7,21,26-29
Arthroscopic synovectomy, while technically demanding, is a safe and effective treatment for patients with elbow synovitis. The outcome depends on the arthroscopic experience of the surgeon, the disease process and sever-ity, and the use of disease-modifying medications.
Arthroscopic Débridement for OsteoarthritisArthroscopic treatment of elbow osteoarthritis is becoming more prev-alent.5,10,12,13,36,37 Although the elbow joint is more technically demanding than other joints, results for treatment of osteoarthritis are encouraging.2
IndicationsArthroscopy is helpful for patients with signifi cant loss of motion at the end range of extension and fl exion. Most patients with osteoarthritis of the elbow report loss of motion more frequently than they do pain. Pain typically occurs only when there is osteophyte impinge-ment at the end of motion. Mid-arc pain generally is not reported because carti-lage is often preserved at the ulnohu-meral articulation. Signifi cant loss of cartilage often occurs at the radiocap-itellar joint, but patients often do not report pain with pronation or supina-tion. On the basis of these fi ndings, ra-dial head excision should be performed sparingly in patients with osteoarthritis.
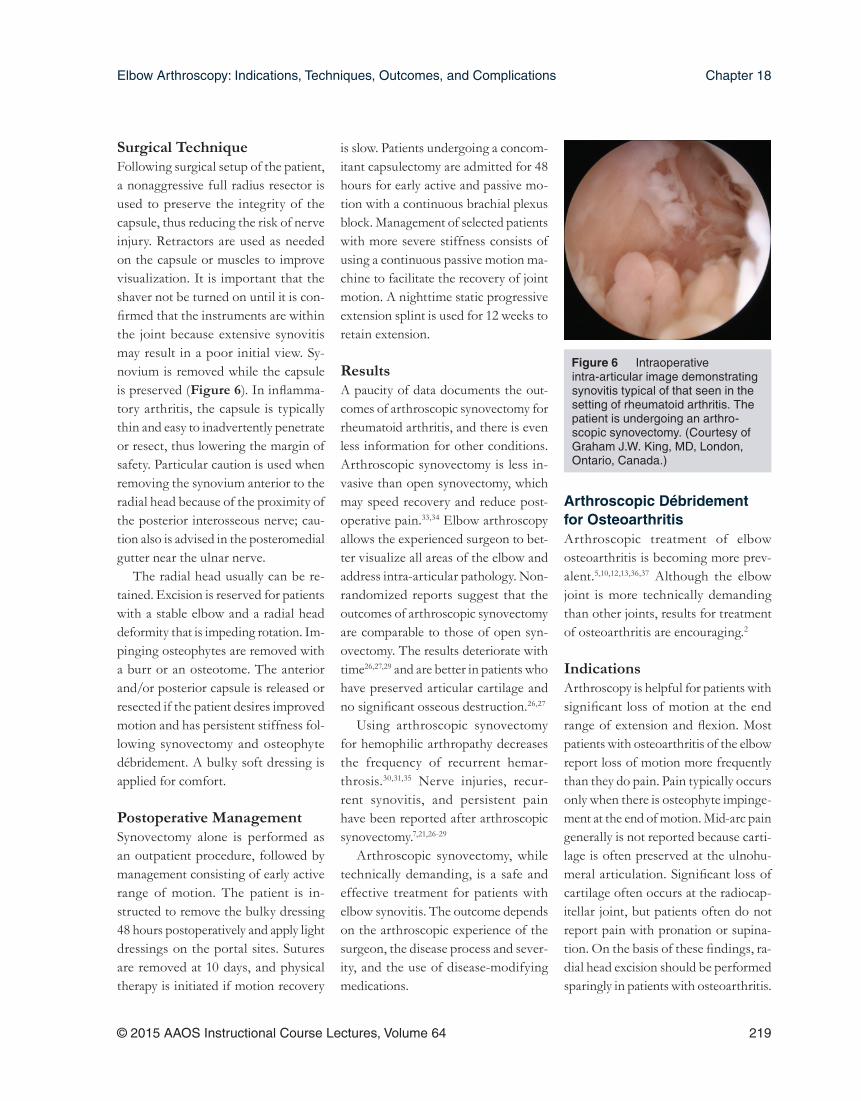
Intraoperative intra-articular image demonstrating synovitis typical of that seen in the setting of rheumatoid arthritis. The patient is undergoing an arthro-scopic synovectomy. (Courtesy of Graham J.W. King, MD, London, Ontario, Canada.)
Figure 6

Shoulder and Elbow
220 © 2015 AAOS Instructional Course Lectures, Volume 64
Arthroscopy may often improve mo-tion after an extensive débridement but, similar to open release, it cannot restore the elbow range of motion to normal. In patients who lack only a few degrees of fl exion or extension, nonsurgical management should be pursued, and the patient should be counseled accord-ingly. In addition, patients who have pain throughout the arc of motion may have widespread joint changes that may be better addressed with an alternative procedure, such as joint resurfacing.
Preoperative Examination and ImagingMotion is documented, and the status of the major peripheral nerves is as-sessed. Patients are specifi cally queried about pain throughout or at the end of the arc of motion, if there is locking or catching (suggestive of loose bodies),
and any ulnar nerve symptoms. Provoc-ative maneuvers at the cubital tunnel are performed because patients may be un-aware of concomitant ulnar neuropathy.
Radiographs are obtained to help determine the overall extent of ar-thritic changes. CT, particularly three- dimensional reconstructions, is helpful to view the location of osteophytes for surgical planning. If most of the osteo-phyte formation is posterior, then the surgical procedure is best started in the olecranon fossa, followed by anterior débridement.
TechniqueIn most patients, the preferred tech-nique is to start anteriorly because there is often more osteophyte formation at this location. In addition, the radial nerve is the neurovascular structure closest to the work area, and it is best to complete anterolateral débridement before the development of joint swell-ing from arthroscopic fl uid. Anteriorly, osteophytes in the coronoid and ra dial head fossae are removed according to the preoperative CT through an an-teromedial working portal while vi-sualizing from the anterolateral portal (Figure 7). The capsule may be released or excised. Once the medial half of the joint has been addressed, a switching stick is used to move the camera to the medial side of the joint, and osteophytes and loose bodies are removed from the lateral side. Care should be taken not to excise the capsule over the area of the radial nerve and the posterior inter-osseous nerve. Osteophytes should be removed from the tip and the medial aspects of the coronoid.
After the anterior aspect of the joint is completed, a posterior approach can be performed. A direct posterior portal located at the midproximal margin of
the olecranon fossa provides an excel-lent working portal for the placement of a shaver or burr. Visualization of the posterior fossa is often diffi cult initially until a portion of the fat pad is removed with the shaver. During this débridement, the shaver should avoid the me dial aspect of the joint to prevent contact with the ulnar nerve. After re-moval of the synovium and fat to allow visualization, viewing is usually con-ducted from the direct posterior portal, and the posterolateral portal is used as a working portal located just lateral to the olecranon; this allows for good visuali-zation of the olecranon fossa.
In the posterior joint, in addition to the obvious bony spur on the tip of the olecranon, bone formation occurs on the sides of the olecranon. This can be diffi cult to resect. On the medial side of the joint, the ulnar nerve is at risk. During work in the area, the ulnar nerve may be protected by a retractor; if the patient has coexisting ulnar neurop-athy, then an open, in situ release of the nerve allows for direct protection. Use of a burr in this area has the potential to wrap up soft tissue quickly and should be considered with caution.
In the olecranon fossa, a thick osteo-phyte often divides the fossa into two parts and acts as a block to extension. A burr working directly through a pos-terolateral portal may be used to remove this common osteophyte.
Ulnar Nerve ReleaseDuring arthroscopy of the osteoar-thritic elbow, the ulnar nerve may need to be addressed. In the patient with preoperative ulnar neuropathy, a small incision is made at the begin-ning of the procedure, and an in situ release of the ulnar nerve is performed. When mild neuropathy is present, an
CT scan with three- dimensional reconstruction that defi nes the areas of osteophyte formation to be addressed to restore motion. The circled area and the arrow identify areas that should be addressed for removal of osteophytes. (Courtesy of Julie E. Adams, MD, Minneapolis, MN.)
Figure 7

Elbow Arthroscopy: Indications, Techniques, Outcomes, and Complications Chapter 18
© 2015 AAOS Instructional Course Lectures, Volume 64 221
all- arthroscopic release of the nerve can be performed.38 In patients who preop-eratively cannot fl ex past 90°, an open ulnar release is advocated. There is no consensus of opinion on this addition-al procedure in asymptomatic patients, but it is recognized that surgical release of the ulnar nerve itself is not without risk.
Postoperative CareAfter surgery, a soft compressive dress-ing is applied from the midarm to the wrist. Patients are instructed to rest the elbow and return in 48 hours for removal of the dressing. Management then consists of instructing patients to move the elbow; if they are able to do so through at least a 45° arc of motion, they are given hinged static splints to help stretch and maintain the range of motion gained at surgery. A small per-centage of patients will have too much pain to be able to move the elbow; these patients are candidates for an axillary block and continuous passive motion for 48 hours.
At 48 hours after surgery, patients are instructed to use the elbow for all activities of daily living. If in the fi rst 2 or 3 postoperative weeks patients are unable to maintain the gains in motion achieved in the operating room, then gentle manipulation under anesthesia has proven to be an effective option.39
The results of elbow arthroscopy for osteoarthritis are generally favor-able. Most studies demonstrate im-provements in motion and function; it should be anticipated, however, that full restoration of motion is unlikely, particularly terminal extension. Like-wise, series suggest diffi culty with res-toration of pronosupination. No studies have shown advantages compared with open treatment. Unfortunately, the risk
of nerve injury cannot be eliminated, and neurovascular complications may occur with either open or arthroscopic elbow surgery.23,24
Arthroscopic Treatment of Lateral EpicondylitisThe origin of the extensor carpi radialis brevis (ECRB) has been implicated as the source of pathology in lateral epi-condylitis.40 Surgical treatment is most commonly directed at excision of the pathologic tissue.41-46
AnatomyFor arthroscopic management, it is important to understand the anatomy of the extensor tendon origins at the humeral epicondyle; the location of the ECRB tendon origin has been defi ned relative to intra-articular landmarks.17
At the elbow, the extensor carpi ra-dialis longus (ECRL) overlies the prox-imal portion of the ECRB such that the ECRL must be elevated anteriorly to visualize the superfi cial surface of the ECRB. A thin fi lm of areolar connec-tive tissue separates the two structures.
The ECRL origin is entirely muscu-lar along the lateral supracondylar ridge of the humerus. The muscle origin has a triangular confi guration with the apex pointing proximally. In contrast, the origin of the ECRB is entirely tendi-nous. Whereas the ECRB blends with the origin of the extensor digitorum communis when dissected from a dis-tal-to-proximal direction using the ten-don undersurface, it can be separated from the extensor digitorum commu-nis back to the humerus. The anatomic origin of the ECRB is located just be-neath the distal-most tip of the lateral supracondylar ridge. The footprint is diamond shaped and measures approx-imately 13 mm by 7 mm (Figure 8). At
the level of the radiocapitellar joint, the ECRB is intimate with the underlying anterior capsule of the elbow joint, but it is easily separable at this level.17 Using these data, an arthroscopic technique was designed for lateral epicondylitis.
TechniqueThe patient is positioned in the lateral decubitus position. It is often helpful to start with portal placement on the anteromedial side because it allows for visualization of the lateral joint, and a modifi ed anterolateral portal is estab-lished using an inside-out technique. This portal is placed 2 to 3 cm above and anterior to the lateral epicondyle, slightly more proximal than a standard anterolateral portal. The purpose of the modifi ed placement is to allow for instrumentation down to the tendon origin, rather than entering the joint through the ECRB tendon itself.
Any lateral synovitis is débrided with a resector. The lateral capsule is then released. Occasionally, a disruption of the underlying capsule from the hu-merus is identifi ed. More commonly, the capsule is intact although small linear tears may be present. It is easier to release the lateral soft tissues in lay-ers using a monopolar thermal device. With this method, the capsule is fi rst incised or released from the humerus. When it retracts distally, the ECRB ten-don is visualized posteriorly, and the ECRL, which is principally muscular, is visualized more anterior. As stated, the ECRB tendon spans from the top of the capitellum to the midline of the radiocapitellar joint.
After the capsule is adequately re-sected, the ECRB origin is released from the epicondyle (Figures 8 and 9), starting at the top of the capitellum and carried posteriorly. The lateral collateral
Shoulder and Elbow
222 © 2015 AAOS Instructional Course Lectures, Volume 64
ligament is not at risk if the release is kept above the midline of the radio-capitellar joint.45 On average, adequate resection of the ECRB must include approximately 13 mm of tendon origin from anterior to posterior.17 Care is tak-en to drive the scope in adequately to view the release down to the midline of the radiocapitellar joint. Typically, the entire ECRB retracts distally away from the humerus.
Care is taken not to release the ex-tensor aponeurosis that lies behind the ECRB tendon. This structure is visualized as a striped background of
transversely (longitudinally) oriented tendon and muscular fi bers much less distinct than the ECRB. It is located posterior to the ECRL. If the aponeu-rosis is violated, débridement will alter the subcutaneous tissue about the lat-eral elbow.
ResultsIn recent years, interest in the arthro-scopic treatment of lateral epicondylitis has increased.41-46 However, the results of arthroscopic treatment of this con-dition have been variable across series, possibly as a result of increased diffi culty
in identifying the ECRB origin through the arthroscope.41,44,46 In one study, a consecutive series of 36 patients with recalcitrant lateral epicondylitis were treated with arthroscopic release.18 On average, patients required 4 weeks to return to regular activities and 7 weeks to return to full work duties. Ten pa-tients (28%) reported continued pain with strenuous activities and repetitive use of the affected arm, and the treat-ment was considered a failure in two patients (6%) who continued to have substantial pain.18
Arthroscopic release of the ECRB appears to be an effective option for the surgical treatment of chronic lateral epi-condylitis that has failed to respond to nonsurgical management. Knowledge of the anatomy, including the extensor tendon origins as visualized from an intra-articular perspective, is essential for effective surgical release. Further series will determine how this treatment option fi ts into the armamentarium for management of this condition.
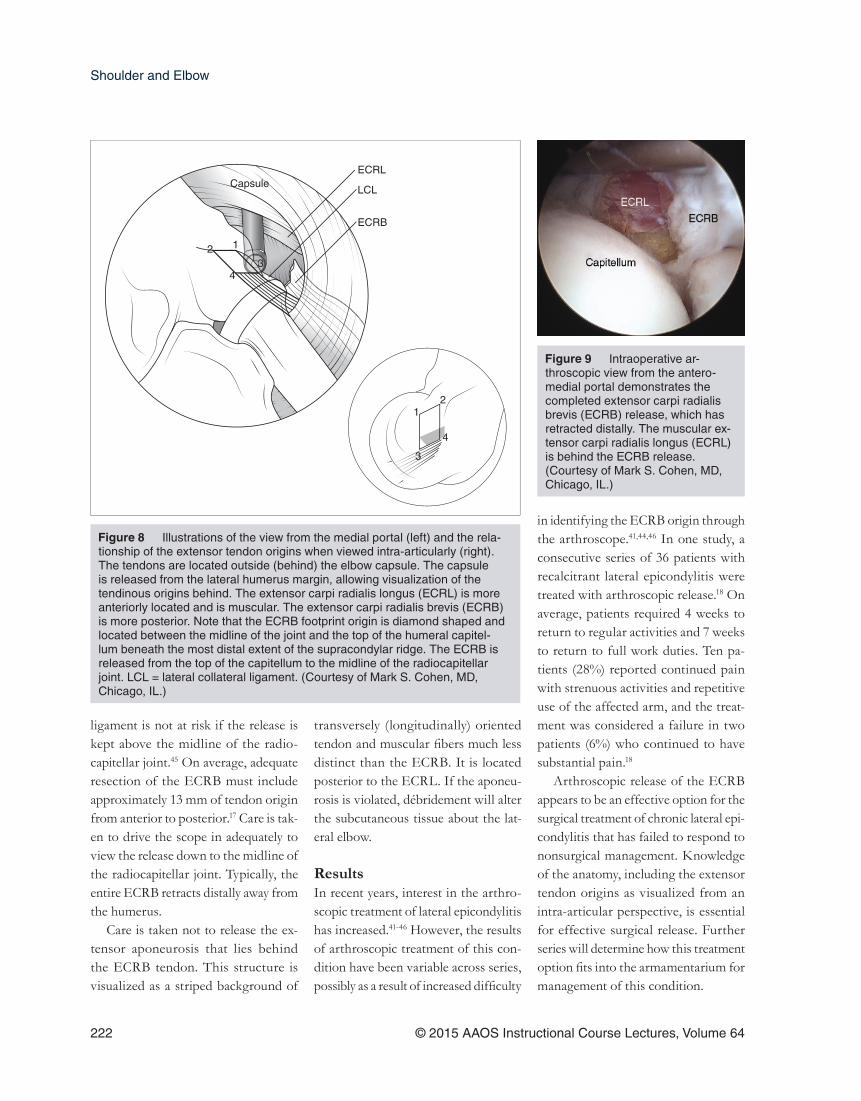
Illustrations of the view from the medial portal (left) and the rela-tionship of the extensor tendon origins when viewed intra-articularly (right). The tendons are located outside (behind) the elbow capsule. The capsule is released from the lateral humerus margin, allowing visualization of the tendinous origins behind. The extensor carpi radialis longus (ECRL) is more anteriorly located and is muscular. The extensor carpi radialis brevis (ECRB) is more posterior. Note that the ECRB footprint origin is diamond shaped and located between the midline of the joint and the top of the humeral capitel-lum beneath the most distal extent of the supracondylar ridge. The ECRB is released from the top of the capitellum to the midline of the radiocapitellar joint. LCL = lateral collateral ligament. (Courtesy of Mark S. Cohen, MD, Chicago, IL.)
CapsuleECRL
LCL
ECRB
123
4
12
3
4
Figure 8
Intraoperative ar-throscopic view from the antero-medial portal demonstrates the completed extensor carpi radialis brevis (ECRB) release, which has retracted distally. The muscular ex-tensor carpi radialis longus (ECRL) is behind the ECRB release. (Courtesy of Mark S. Cohen, MD, Chicago, IL.)
Figure 9

Elbow Arthroscopy: Indications, Techniques, Outcomes, and Complications Chapter 18
© 2015 AAOS Instructional Course Lectures, Volume 64 223
SummaryElbow arthroscopy is a useful tool to address pathology about the elbow; published studies to date document its effectiveness to address infl ammatory and degenerative arthritis and lateral epicondylitis. It is important to under-stand the limitations of this technique, as well as potential complications and alternative procedures.
References 1. Adams JE, Reding MT: Hemophilic
arthropathy of the elbow. Hand Clin 2011;27(2):151-163, v.
2. Yeoh KM, King GJ, Faber KJ, Glazebrook MA, Athwal GS: Evidence-based indications for elbow arthroscopy. Arthroscopy 2012;28(2):272-282.
3. Miyake J, Masatomi T: Arthroscopic debridement of the humeral capitel-lum for osteochondritis dissecans: Radiographic and clinical outcomes. J Hand Surg Am 2011;36(8):1333-1338.
4. Tucker SA, Savoie FH III, O’Brien MJ: Arthroscopic management of the post-traumatic stiff elbow. J Shoulder Elbow Surg 2011;20(suppl 2):S83-S89.
5. van den Ende KI, McIntosh AL, Adams JE, Steinmann SP: Osteo-chondritis dissecans of the capi-tellum: A review of the literature and a distal ulnar portal. Arthroscopy 2011;27(1):122-128.
6. Savoie FH III, O’Brien MJ, Field LD, Gurley DJ: Arthroscopic and open radial ulnohumeral ligament recon-struction for posterolateral rotatory instability of the elbow. Clin Sports Med 2010;29(4):611-618.
7. Kang HJ, Park MJ, Ahn JH, Lee SH: Arthroscopic synovectomy for the rheumatoid elbow. Arthroscopy 2010;26(9):1195-1202.
8. Savoie FH III, VanSice W, O’Brien MJ: Arthroscopic tennis elbow release. J Shoulder Elbow Surg 2010;19(suppl 2):31-36.
9. Savoie FH III: Guidelines to becom-ing an expert elbow arthroscopist. Arthroscopy 2007;23(11):1237-1240.
10. Krishnan SG, Harkins DC, Pen-nington SD, Harrison DK, Burkhead WZ: Arthroscopic ulnohumeral arthroplasty for degenerative arthritis of the elbow in patients under fi fty years of age. J Shoulder Elbow Surg 2007;16(4):443-448.
11. Steinmann SP, King GJ, Savoie FH III; American Academy of Orthopae-dic Surgeons: Arthroscopic treatment of the arthritic elbow. J Bone Joint Surg Am 2005;87(9):2114-2121.
12. Adams JE, Wolff LH III, Merten SM, Steinmann SP: Osteoarthritis of the elbow: Results of arthroscopic osteo-phyte resection and capsulectomy. J Shoulder Elbow Surg 2008;17(1):126-131.
13. Steinmann SP: Elbow arthroscopy: Where are we now? Arthroscopy 2007;23(11):1231-1236.
14. Adams JE, Merten SM, Steinmann SP: Arthroscopic-assisted treatment of coronoid fractures. Arthroscopy 2007;23(10):1060-1065.
15. Hausman MR, Qureshi S, Goldstein R, et al: Arthroscopically-assisted treatment of pediatric lateral humeral condyle fractures. J Pediatr Orthop 2007;27(7):739-742.
16. Hsu JW, Gould JL, Fonseca-Sabune H, Hausman MH: The emerging role of elbow arthroscopy in chronic use injuries and fracture care. Hand Clin 2009;25(3):305-321.
17. Cohen MS, Romeo AA, Hennigan SP, Gordon M: Lateral epicondylitis: Anatomic relationships of the exten-sor tendon origins and implications for arthroscopic treatment. J Shoulder Elbow Surg 2008;17(6):954-960.
18. Lattermann C, Romeo AA, Anbari A, et al: Arthroscopic debridement of the extensor carpi radialis brevis for recal-citrant lateral epicondylitis. J Shoulder Elbow Surg 2010;19(5):651-656.
19. van den Ende KI, Steinmann SP: Arthroscopic treatment of septic arthritis of the elbow. J Shoulder Elbow Surg 2012;21(8):1001-1005.
20. Sahajpal DT, Blonna D, O’Driscoll SW: Anteromedial elbow arthroscopy portals in patients with prior ulnar nerve transposition or subluxation. Arthroscopy 2010;26(8):1045-1052.
21. Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83(1):25-34.
22. Gofton WT, King GJ: Heterotopic ossifi cation following elbow arthros-copy. Arthroscopy 2001;17(1):E2.
23. Adams JE, Steinmann SP: Nerve injuries about the elbow. J Hand Surg Am 2006;31(2):303-313.
24. Ruch DS, Poehling GG: Anterior interosseous nerve injury follow-ing elbow arthroscopy. Arthroscopy 1997;13(6):756-758.
25. Verhaar J, van Mameren H, Brandsma A: Risks of neurovascular injury in elbow arthroscopy: Starting antero-medially or anterolaterally? Arthroscopy 1991;7(3):287-290.
26. Lee BP, Morrey BF: Arthroscopic syn-ovectomy of the elbow for rheumatoid arthritis: A prospective study. J Bone Joint Surg Br 1997;79(5):770-772.
27. Horiuchi K, Momohara S, Tomatsu T, Inoue K, Toyama Y: Arthroscopic synovectomy of the elbow in rheu-matoid arthritis. J Bone Joint Surg Am 2002;84(3):342-347.
28. Nemoto K, Arino H, Yoshihara Y, Fujikawa K: Arthroscopic synovec-tomy for the rheumatoid elbow: A short-term outcome. J Shoulder Elbow Surg 2004;13(6):652-655.
29. Tanaka N, Sakahashi H, Hirose K, Ishima T, Ishii S: Arthroscopic and open synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am 2006;88(3):521-525.
30. Dunn AL, Busch MT, Wyly JB, Sul-livan KM, Abshire TC: Arthroscopic synovectomy for hemophilic joint disease in a pediatric population. J Pediatr Orthop 2004;24(4):414-426.
31. Tamurian RM, Spencer EE, Wojtys EM: The role of arthroscopic synovectomy in the management of hemarthrosis in hemophilia patients: Financial perspectives. Arthroscopy 2002;18(7):789-794.
32. Jerosch J, Hoffstetter I, Schröder M, Castro WH: Septic arthritis: Ar-throscopic management with local antibiotic treatment. Acta Orthop Belg 1995;61(2):126-134.

Shoulder and Elbow
224 © 2015 AAOS Instructional Course Lectures, Volume 64
33. Gendi NS, Axon JM, Carr AJ, Pile KD, Burge PD, Mowat AG: Syn-ovectomy of the elbow and radial head excision in rheumatoid arthri-tis: Predictive factors and long-term outcome. J Bone Joint Surg Br 1997;79(6):918-923.
34. Ferlic DC, Patchett CE, Clayton ML, Freeman AC: Elbow synovec tomy in rheumatoid arthritis: Long-term results. Clin Orthop Relat Res 1987;220:119-125.
35. Verma N, Valentino LA, Chawla A: Arthroscopic synovectomy in haemophilia: Indications, technique and results. Haemophilia 2007;13(suppl 3):38-44.
36. Keener JD, Galatz LM: Arthroscopic management of the stiff elbow. J Am Acad Orthop Surg 2011;19(5):265-274.
37. Ogilvie-Harris DJ, Gordon R, Mac-Kay M: Arthroscopic treatment for posterior impingement in degenera-tive arthritis of the elbow. Arthroscopy 1995;11(4):437-443.
38. Kovachevich R, Steinmann SP: Ar-throscopic ulnar nerve decompression in the setting of elbow osteoarthritis. J Hand Surg Am 2012;37(4):663-668.
39. Araghi A, Celli A, Adams R, Morrey B: The outcome of examination (manipulation) under anesthesia on the stiff elbow after surgical con-tracture release. J Shoulder Elbow Surg 2010;19(2):202-208.
40. Kraushaar BS, Nirschl RP: Tendinosis of the elbow (tennis elbow): Clinical features and fi ndings of histological, immunohistochemical, and electron microscopy studies. J Bone Joint Surg Am 1999;81:259-278.
41. Baker CL Jr, Murphy KP, Gottlob CA, Curd DT: Arthroscopic classifi ca-tion and treatment of lateral epicon-dylitis: Two-year clinical results. J Shoulder Elbow Surg 2000;9(6):475-482.
42. Cohen MS, Romeo AA: Lateral epicondylitis: Open and arthro-scopic treatment. J Am Soc Surg Hand 2001;1:172-176.
43. Kuklo TR, Taylor KF, Murphy KP, Islinger RB, Heekin RD, Baker CL Jr: Arthroscopic release for lateral epicondylitis: A cadaveric model. Arthroscopy 1999;15(3):259-264.
44. Peart RE, Strickler SS, Schweitzer KM Jr: Lateral epicondylitis: A com-parative study of open and arthro-scopic lateral release. Am J Orthop (Belle Mead NJ) 2004;33(11):565-567.
45. Smith AM, Castle JA, Ruch DS: Arthroscopic resection of the common extensor origin: Anatomic considerations. J Shoulder Elbow Surg 2003;12(4):375-379.
46. Stapleton TR, Baker CL Jr: Ar-throscopic treatment of lateral epi-condylitis: A clinical study. Arthroscopy 1996;12:365-366.
Video Reference Steinmann SP: The Stiff Elbow: Arthroscopic Management of Elbow Arthritis and Elbow Arthrofi brosis [video excerpt]. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2014.