arthroscopy of the hip for labral pathology and fai: indications and technique
TRANSCRIPT

Arthroscopy of the Hip for Labral Pathology and FAI: Indications and Technique
Cherry Blossom Seminar Sports Medicine and the Aging Athlete
2014
Andrew B. Wolff, MDWashington Orthopaedics and Sports Medicine
Washington, DC

Femoroacetabular Impingement: a risk factor for hip pathology and pain
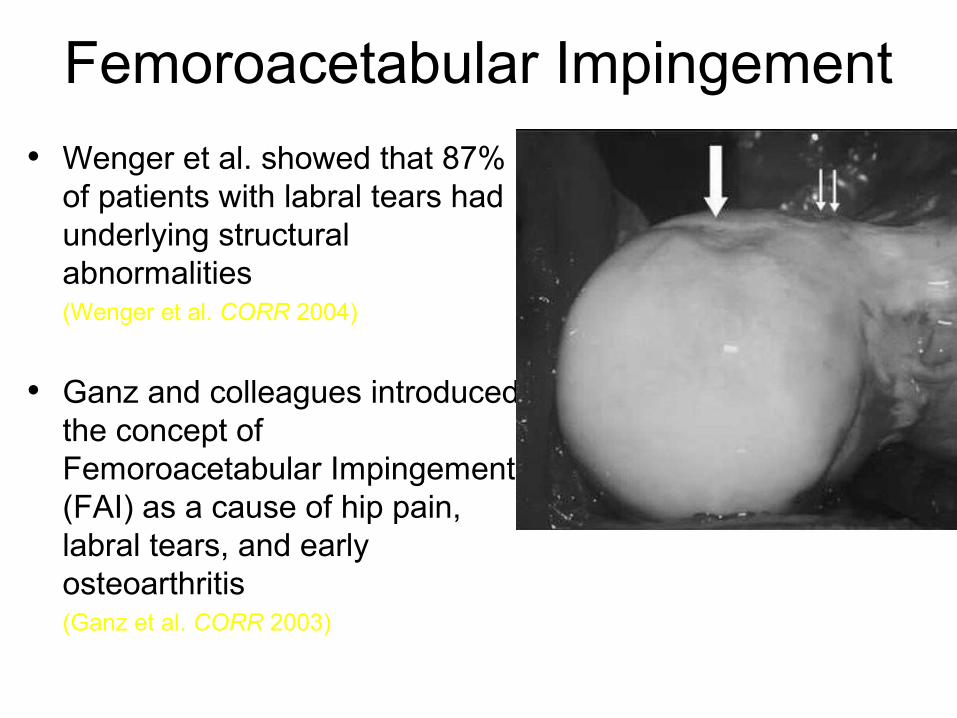
Femoroacetabular Impingement
• Wenger et al. showed that 87% of patients with labral tears had underlying structural abnormalities (Wenger et al. CORR 2004)
• Ganz and colleagues introduced the concept of Femoroacetabular Impingement (FAI) as a cause of hip pain, labral tears, and early osteoarthritis(Ganz et al. CORR 2003)

CAM & PINCER ImpingementCAM & PINCER Impingement
PincerCAM
Espinosa et al J Bone Joint Surg 2006; 88-A: 225-239

Acetabular Labrum• Extends the
acetabulum beyond the bony socket
• Is present around the entire lunate surface of the acetabulum
• Is continuous with the transverse acetabular ligament inferiorly

FAI: FAI: Pincer TypePincer Type





contre-coup

contre-coup



FAI: FAI: Cam TypeCam Type














Indications
Is my diagnosis correct?

Is my diagnosis correct?
• History and Physical are critical
• Understand concomitant disease (i.e., core muscle injury, lumbar spine pathology, muscle strains, etc.)
• Understand that there is often a mixed picture of symptoms such as sacroillitis, peri-pelvic tendinitis, ischial or troch bursitis

• Traumatic vs. Insidious– Twisting or torqueing
– Subluxation
– Dislocation, associated fracture
• Congenital / Developmental– DDH, Perthes, SCFE
• Other– Infection, PVNS, Osteonecrosis, Synovial
Chondromatosis
History
32

Confirming the source of pain
• History
– Is it predominately lateral or posterior?
– Or is it in the groin?
– Pain and/or numbness going down the leg?

“C” Sign
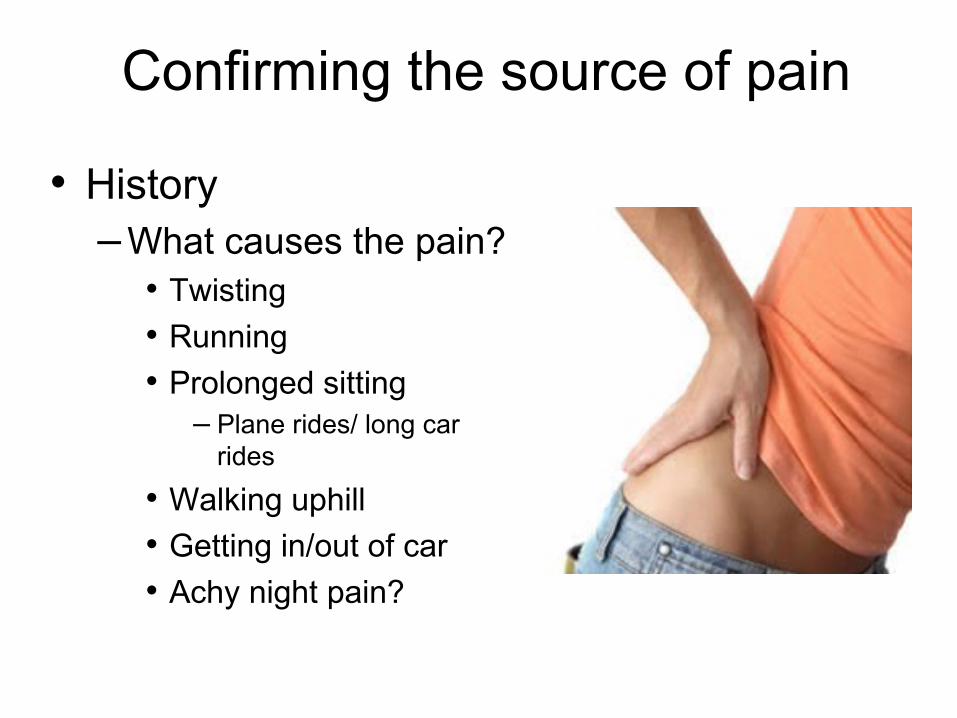
Confirming the source of pain
• History – What causes the pain?
• Twisting
• Running
• Prolonged sitting– Plane rides/ long car
rides
• Walking uphill
• Getting in/out of car
• Achy night pain?

Confirming the source of pain
• Many patients don’t follow the textbook– Combined back and
groin pain
– Troch and groin pain
– Butt and groin pain
– Groin pain but negative anterior impingement sign
– Achy night pain

“Anterior Impingement Test”Passive flexion to 90°
followed by forced adduction and IR
Leunig et al. Op Tech Orthop 2005

FABER Test
Vad et al. Am J Sports Med 2004
Confirming the source of pain
• Diagnostic injections
– Physical exam
– Inciting activities
– Pain diary

Indications
Is my diagnosis correct?
Do the patient’s current symptoms/limitations warrant surgical
intervention?

Do the patient’s current symptoms/limitations warrant
surgical intervention?
•If it doesn’t hurt, don’t operate

Do the patient’s current symptoms/limitations warrant
surgical intervention?
•No evidence for prophylactic FAI correction
•Possible exception of SCFE

Indications
Is my diagnosis correct?
Do the patient’s current symptoms/limitations warrant surgical
intervention?
Does this patient have osteoarthritis?

Osteoarthritis
• Cannot be cured with arthroscopy
• 2 mm rule (Philippon et al AJSM 2010)– Not applicable to women– Is it applicable at all?– High resolution MRI
• Role for chondral restorative procedures in chondral defects

Indications
Is my diagnosis correct?
Do the patient’s current symptoms/limitations warrant surgical
intervention?
Does this patient have osteoarthritis?
Does this patient have dysplasia?

Dysplasia
• Undercovered hips cannot be cured arthroscopically– Measure LCEA, ACEA, acetabular inclination
and femoral neck shaft angles on all patients • Consider acetabular and femoral version
– Definite role for arthroscopic treatment of borderline dysplastics
– How much dysplasia is too much?

Pincer correction with labral repair

Correction of cam type FAI

Some are easier…
Pre-op Post-op

…than others
Pre-op Post-op

Conclusions
• In 2014, much can be accomplished in the hip arthroscopically
• Not all FAI and labral tears need to be fixed
• With the right indications, modern techniques yield reproducibly good results

Conclusions
• In depth understanding of the hip joint is paramount
• Advanced imaging is very helpful
• Equally important: advanced history and physical
• Use diagnostic injections
• BEWARE osteoarthritis and dysplasia!