ehc 114
DESCRIPTION
EHC 114 (UPM SPECIAL ISSUE)TRANSCRIPT

In men, prostate cancer is the most commonly diagnosed solid tumor malignancy in the United
States and is the second highest cancer-specific cause of death after lung cancer.1
At time of diagnosis, most indi-viduals with prostate cancer are as-ymptomatic. Screening and identifi-cation of prostate cancer is normally based on prostate-specific antigen (PSA) testing and a digital rectal examination, and the diagnosis is typically confirmed by a needle biop-sy. If the biopsy results are positive, the affected tissue is graded based on microscopic evaluation and a Glea-son score is calculated. The Gleason score is used to predict prognosis and help guide initial therapy.2
Although Gleason grading and scoring has been the gold standard of risk classification in prostate cancer for many years, there are emerging techniques that may be incorporated into the physician’s armamentarium in the future.
Today’s screening and identifica-tion techniques find most patients with prostate cancer, and only ap-proximately 5% of newly diagnosed prostate cancer patients in the United States present with meta-static disease.3
With the change in the US Preven-tive Services Task Force guidance regarding routine PSA screening in men age 50 years and older, some urologists are concerned that the percentage of newly diagnosed pa-tients with metastatic disease may begin to increase, reversing a trend whereby the incidence of newly di-agnosed patients with metastatic prostate cancer had dropped from 67 per 100,000 in 1990 to 23 per 100,000 in 2005—a 66% decrease.4,5
Herein lies the conundrum. On the one hand, some stakeholders have
Proceedings of the Prostate Cancer Steering Committee MeetingFebruary 13, 2013, Orlando, Florida
Continued on page 9
May 2013 SPeCial iSSue VoluMe 2 • NuMber 1
Urology Practice ManageMent™
process improvements to enhance patient care™
©2013 engage healthcare communications, LLc
Clinical Considerations in Treating advanced Prostate Cancer: The Changing role of the urologistby Matthew Wendling, MPH, and Neal Shore, MDMr Wendling is Medical Writer, engage Healthcare Communications and Dr Shore is Managing Partner, Carolina urologic research Center, Myrtle beach, SC
www.uroPracticeManagement.com
As the US healthcare system continues to evolve, physicians in every state and spe-cialty are attempting to comply with new
rules, expectations, and costs, and must adapt to meet new healthcare demands. In urology, these changes are being driven by a combination of clinical and economic factors, including therapeu-tic innovation, improved surgical techniques, and perhaps most prominently, a policy environment where purchasers of healthcare are increasingly focused on accountability, quality, and value. These changes are having a profound effect on the practice of urology from a business as well as a clinical perspective.
The Prostate Cancer Steering Committee was convened to discuss the current business challeng-es faced by urology practices and to understand how urology practices are changing their clinical and business models in order to thrive in today’s healthcare environment. In addition, the Steering Committee was assembled to explore clinical and practice management trends and challenges with respect to the treatment of advanced prostate can-cer, including the utilization of oral agents to treat metastatic disease. l

K P G75 M50 K75 Y50 GN M25 B C75 M75 K25 Y C50 M G25 C Y75 K50 C25 G50 Y25 R
Date: 04/12/13 Customer Code: K08Z13048 Group 360 Job #: 682403File Name: K08Z13048_682403_v1a (2-page spread) Brand: ZytigaSize: 8.125" x 10.875" Colors: CMYK Description: An Oral Option for your Urology PracticePub: Urology Practice Management (May 2013 issue)
LOCALTHERAPY† ZYTIGA®
PLUS PREDNISONEADT‡
MonthsMonthsMonthsMonths35.3333355..
K0
8Z12
1176
* Study Design: ZYTIGA®, in combination with prednisone, was evaluated in a Phase 3, randomized, double-blind, placebo-controlled, multicenter trial in patients with mCRPC who had not received prior chemotherapy (N = 1,088). Patients were using a luteinizing hormone-releasing hormone (LHRH) agonist or were previously treated with orchiectomy. In the ZYTIGA® arm, patients received ZYTIGA® 1,000 mg orally once daily + prednisone 5 mg orally twice daily. In the placebo arm, patients received placebo orally once daily + prednisone 5 mg orally twice daily. In this study, the coprimary efficacy endpoints were overall survival and radiographic progression-free survival.
†Local therapy = radiation and/or surgery.‡ For many patients with mCRPC, gonadotropin-releasing hormone (GnRH)agonist therapy typically continues throughout the disease course, and is used concomitantly with other mCRPC treatments, including ZYTIGA®. This illustration is not intended to suggest that ZYTIGA® is the only treatment option following androgen-deprivation therapy (ADT).
§ Primary endpoint.|| Secondary endpoint.
Please see brief summary of full Prescribing Information on adjacent pages.
Contraindications—ZYTIGA® is not indicated for use in women. ZYTIGA® can cause fetal harm (Pregnancy Category X) when administered to a pregnant woman and is contraindicated in women who are or may become pregnant. Hypertension, Hypokalemia, and Fluid Retention Due to Mineralocorticoid Excess—Use with caution in patients with a history of cardiovascular disease or with medical conditions that might be compromised by increases in blood pressure, hypokalemia, or fl uid retention. ZYTIGA® may cause hypertension, hypokalemia, and fl uid retention as a consequence of increased mineralocorticoid levels resulting from CYP17 inhibition. Safety has not been established in patients with LVEF < 50% or New York Heart Association (NYHA) Class III or IV heart failure (in study 1) or NYHA Class II to IV heart failure (in study 2) because these patients were excluded from these randomized clinical trials. Control hypertension and correct hypokalemia before and during treatment. Monitor blood pressure, serum potassium, and symptoms of fl uid retention at least monthly. Adrenocortical Insuffi ciency (AI)—AI was reported in patients receiving ZYTIGA® in combination with prednisone, after an interruption of daily steroids and/or with concurrent infection or stress. Use caution and monitor for symptoms and signs of AI if prednisone is stopped or withdrawn, if prednisone dose is reduced, or if the patient experiences unusual stress. Symptoms and signs of AI may be masked by adverse reactions associated
with mineralocorticoid excess seen in patients treated with ZYTIGA®. Perform appropriate tests, if indicated, to confi rm AI. Increased dosages of corticosteroids may be used before, during, and after stressful situations. Hepatotoxicity—Monitor liver function and modify, withhold, or discontinue ZYTIGA® dosing as recommended (see Prescribing Information for more information). Measure serum transaminases [alanine aminotransferase (ALT) and aspartate aminotransferase (AST)] and bilirubin levels prior to starting treatment with ZYTIGA®, every two weeks for the fi rst three months of treatment, and monthly thereafter. Promptly measure serum total bilirubin, AST, and ALT if clinical symptoms or signs suggestive of hepatotoxicity develop. Elevations of AST, ALT, or bilirubin from the patient’s baseline should prompt more frequent monitoring. If at any time AST or ALT rise above fi ve times the upper limit of normal (ULN) or the bilirubin rises above three times the ULN, interrupt ZYTIGA® treatment and closely monitor liver function. Increased ZYTIGA® Exposures With Food—ZYTIGA® must be taken on an empty stomach. No food should be eaten for at least two hours before the dose of ZYTIGA® is taken and for at least one hour after the dose of ZYTIGA® is taken. Abiraterone Cmax and AUC0-∞ (exposure) were increased up to 17- and 10-fold higher, respectively, when a single dose of abiraterone acetate was administered with a meal compared to a fasted state.
Adverse Reactions—The most common adverse reactions (≥ 10%) are fatigue, joint swelling or discomfort, edema, hot fl ush, diarrhea, vomiting, cough, hypertension, dyspnea, urinary tract infection, and contusion. The most common laboratory abnormalities (> 20%) are anemia, elevated alkaline phosphatase, hypertriglyceridemia, lymphopenia, hypercholesterolemia, hyperglycemia, elevated AST, hypophosphatemia, elevated ALT, and hypokalemia.
Drug Interactions—ZYTIGA® is an inhibitor of the hepatic drug-metabolizing enzyme CYP2D6. Avoid co-administration with CYP2D6 substrates that have a narrow therapeutic index. If an alternative cannot be used, exercise caution and consider a dose reduction of the CYP2D6 substrate. In vitro, ZYTIGA® inhibits CYP2C8. There are no clinical data on its use with drugs that are substrates of CYP2C8. Patients should be monitored closely for signs of toxicity related to the CYP2C8 substrate if used concomitantly with abiraterone acetate.Based on in vitro data, ZYTIGA® is a substrate of CYP3A4. The eff ects of strong CYP3A4 inhibitors or inducers on the pharmacokinetics of abiraterone have not been evaluated, in vivo. Strong inhibitors and inducers of CYP3A4 should be avoided or used with caution during treatment with ZYTIGA®.
Use in Specifi c Populations—Do not use ZYTIGA® in patients with baseline severe hepatic impairment (Child-Pugh Class C).
IMPORTANT SAFETY INFORMATION
For more information, please visit www.zytigahcp.com.
FOR PATIENTS WITH mCRPC WHO HAVE PROGRESSED ON ADT*
ZYTIGA® is indicated in combination with prednisone for the treatment of patients with metastatic castration-resistant prostate cancer (mCRPC).
AN ORAL OPTION FOR YOUR UROLOGY PRACTICE
Janssen Biotech, Inc.© Janssen Biotech, Inc. 20133/13 K08Z13048
ZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGA NextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNext®
Signifi cantly increased median time to opiate use for prostate cancer pain vs placebo plus prednisone (not reached vs 23.7 months, respectively)||
HR = 0.686; 95% CI: 0.566, 0.833; P = 0.0001.
Signifi cantly increased median time to chemotherapy vs placebo plus prednisone (25.2 months vs 16.8 months, respectively)||
HR = 0.580; 95% CI: 0.487, 0.691; P < 0.0001.
57% reduction in risk of radiographic progression or death vs placebo plus prednisone (median rPFS not reached vs 8.28 months, respectively)§
HR = 0.425; 95% CI: 0.347, 0.522; P < 0.0001.
35.3 months median overall survival vs 30.1 months with placebo plus prednisone§
Hazard ratio (HR) = 0.792; 95% CI: 0.655, 0.956; P = 0.0151; prespecifi ed value for statistical signifi cance not reached.
B:11.125 in
B:16.5 in
T:10.875 in
T:8.125 inT:8.125 in
S:10.375 in
S:7.625 inS:7.625 in

K P G75 M50 K75 Y50 GN M25 B C75 M75 K25 Y C50 M G25 C Y75 K50 C25 G50 Y25 R
Date: 04/12/13 Customer Code: K08Z13048 Group 360 Job #: 682403File Name: K08Z13048_682403_v1a (2-page spread) Brand: ZytigaSize: 8.125" x 10.875" Colors: CMYK Description: An Oral Option for your Urology PracticePub: Urology Practice Management (May 2013 issue)
LOCALTHERAPY† ZYTIGA®
PLUS PREDNISONEADT‡
MonthsMonthsMonthsMonths35.3333355..
K0
8Z12
1176
* Study Design: ZYTIGA®, in combination with prednisone, was evaluated in a Phase 3, randomized, double-blind, placebo-controlled, multicenter trial in patients with mCRPC who had not received prior chemotherapy (N = 1,088). Patients were using a luteinizing hormone-releasing hormone (LHRH) agonist or were previously treated with orchiectomy. In the ZYTIGA® arm, patients received ZYTIGA® 1,000 mg orally once daily + prednisone 5 mg orally twice daily. In the placebo arm, patients received placebo orally once daily + prednisone 5 mg orally twice daily. In this study, the coprimary efficacy endpoints were overall survival and radiographic progression-free survival.
†Local therapy = radiation and/or surgery.‡ For many patients with mCRPC, gonadotropin-releasing hormone (GnRH)agonist therapy typically continues throughout the disease course, and is used concomitantly with other mCRPC treatments, including ZYTIGA®. This illustration is not intended to suggest that ZYTIGA® is the only treatment option following androgen-deprivation therapy (ADT).
§ Primary endpoint.|| Secondary endpoint.
Please see brief summary of full Prescribing Information on adjacent pages.
Contraindications—ZYTIGA® is not indicated for use in women. ZYTIGA® can cause fetal harm (Pregnancy Category X) when administered to a pregnant woman and is contraindicated in women who are or may become pregnant. Hypertension, Hypokalemia, and Fluid Retention Due to Mineralocorticoid Excess—Use with caution in patients with a history of cardiovascular disease or with medical conditions that might be compromised by increases in blood pressure, hypokalemia, or fl uid retention. ZYTIGA® may cause hypertension, hypokalemia, and fl uid retention as a consequence of increased mineralocorticoid levels resulting from CYP17 inhibition. Safety has not been established in patients with LVEF < 50% or New York Heart Association (NYHA) Class III or IV heart failure (in study 1) or NYHA Class II to IV heart failure (in study 2) because these patients were excluded from these randomized clinical trials. Control hypertension and correct hypokalemia before and during treatment. Monitor blood pressure, serum potassium, and symptoms of fl uid retention at least monthly. Adrenocortical Insuffi ciency (AI)—AI was reported in patients receiving ZYTIGA® in combination with prednisone, after an interruption of daily steroids and/or with concurrent infection or stress. Use caution and monitor for symptoms and signs of AI if prednisone is stopped or withdrawn, if prednisone dose is reduced, or if the patient experiences unusual stress. Symptoms and signs of AI may be masked by adverse reactions associated
with mineralocorticoid excess seen in patients treated with ZYTIGA®. Perform appropriate tests, if indicated, to confi rm AI. Increased dosages of corticosteroids may be used before, during, and after stressful situations. Hepatotoxicity—Monitor liver function and modify, withhold, or discontinue ZYTIGA® dosing as recommended (see Prescribing Information for more information). Measure serum transaminases [alanine aminotransferase (ALT) and aspartate aminotransferase (AST)] and bilirubin levels prior to starting treatment with ZYTIGA®, every two weeks for the fi rst three months of treatment, and monthly thereafter. Promptly measure serum total bilirubin, AST, and ALT if clinical symptoms or signs suggestive of hepatotoxicity develop. Elevations of AST, ALT, or bilirubin from the patient’s baseline should prompt more frequent monitoring. If at any time AST or ALT rise above fi ve times the upper limit of normal (ULN) or the bilirubin rises above three times the ULN, interrupt ZYTIGA® treatment and closely monitor liver function. Increased ZYTIGA® Exposures With Food—ZYTIGA® must be taken on an empty stomach. No food should be eaten for at least two hours before the dose of ZYTIGA® is taken and for at least one hour after the dose of ZYTIGA® is taken. Abiraterone Cmax and AUC0-∞ (exposure) were increased up to 17- and 10-fold higher, respectively, when a single dose of abiraterone acetate was administered with a meal compared to a fasted state.
Adverse Reactions—The most common adverse reactions (≥ 10%) are fatigue, joint swelling or discomfort, edema, hot fl ush, diarrhea, vomiting, cough, hypertension, dyspnea, urinary tract infection, and contusion. The most common laboratory abnormalities (> 20%) are anemia, elevated alkaline phosphatase, hypertriglyceridemia, lymphopenia, hypercholesterolemia, hyperglycemia, elevated AST, hypophosphatemia, elevated ALT, and hypokalemia.
Drug Interactions—ZYTIGA® is an inhibitor of the hepatic drug-metabolizing enzyme CYP2D6. Avoid co-administration with CYP2D6 substrates that have a narrow therapeutic index. If an alternative cannot be used, exercise caution and consider a dose reduction of the CYP2D6 substrate. In vitro, ZYTIGA® inhibits CYP2C8. There are no clinical data on its use with drugs that are substrates of CYP2C8. Patients should be monitored closely for signs of toxicity related to the CYP2C8 substrate if used concomitantly with abiraterone acetate.Based on in vitro data, ZYTIGA® is a substrate of CYP3A4. The eff ects of strong CYP3A4 inhibitors or inducers on the pharmacokinetics of abiraterone have not been evaluated, in vivo. Strong inhibitors and inducers of CYP3A4 should be avoided or used with caution during treatment with ZYTIGA®.
Use in Specifi c Populations—Do not use ZYTIGA® in patients with baseline severe hepatic impairment (Child-Pugh Class C).
IMPORTANT SAFETY INFORMATION
For more information, please visit www.zytigahcp.com.
FOR PATIENTS WITH mCRPC WHO HAVE PROGRESSED ON ADT*
ZYTIGA® is indicated in combination with prednisone for the treatment of patients with metastatic castration-resistant prostate cancer (mCRPC).
AN ORAL OPTION FOR YOUR UROLOGY PRACTICE
Janssen Biotech, Inc.© Janssen Biotech, Inc. 20133/13 K08Z13048
ZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGAZYTIGA NextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNextNext®
Signifi cantly increased median time to opiate use for prostate cancer pain vs placebo plus prednisone (not reached vs 23.7 months, respectively)||
HR = 0.686; 95% CI: 0.566, 0.833; P = 0.0001.
Signifi cantly increased median time to chemotherapy vs placebo plus prednisone (25.2 months vs 16.8 months, respectively)||
HR = 0.580; 95% CI: 0.487, 0.691; P < 0.0001.
57% reduction in risk of radiographic progression or death vs placebo plus prednisone (median rPFS not reached vs 8.28 months, respectively)§
HR = 0.425; 95% CI: 0.347, 0.522; P < 0.0001.
35.3 months median overall survival vs 30.1 months with placebo plus prednisone§
Hazard ratio (HR) = 0.792; 95% CI: 0.655, 0.956; P = 0.0151; prespecifi ed value for statistical signifi cance not reached.
B:11.125 inB:16.5 in
T:10.875 inT:8.125 inT:8.125 in
S:10.375 inS:7.625 inS:7.625 in
ZYTIGA® (abiraterone acetate) TabletsBrief Summary of Prescribing Information.INDICATIONS AND USAGE ZYTIGA is a CYP17 inhibitor indicated in combination with prednisone for the treatment of patients with metastatic castration-resistant prostate cancer.CONTRAINDICATIONSPregnancy: ZYTIGA can cause fetal harm when administered to a pregnant woman. ZYTIGA is not indicated for use in women. ZYTIGA is contraindicated in women who are or may become pregnant. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, apprise the patient of the potential hazard to the fetus and the potential risk for pregnancy loss [see Use in Specific Populations].WARNINGS AND PRECAUTIONS Hypertension, Hypokalemia and Fluid Retention Due to Mineralocorticoid Excess: ZYTIGA may cause hypertension, hypokalemia, and fluid retention as a consequence of increased mineralocorticoid levels resulting from CYP17 inhibition [see Clinical Pharmacology (12.1) in full Prescribing Information]. In the two randomized clinical trials, grade 3 to 4 hypertension occurred in 2% of patients, grade 3 to 4 hypokalemia in 4% of patients, and grade 3 to 4 edema in 1% of patients treated with ZYTIGA [see Adverse Reactions].Co-administration of a corticosteroid suppresses adrenocorticotropic hormone (ACTH) drive, resulting in a reduction in the incidence and severity of these adverse reactions. Use caution when treating patients whose underlying medical conditions might be compromised by increases in blood pressure, hypokalemia or fluid retention, e.g., those with heart failure, recent myocardial infarction or ventricular arrhythmia. Use ZYTIGA with caution in patients with a history of cardiovascular disease. The safety of ZYTIGA in patients with left ventricular ejection fraction < 50% or New York Heart Association (NYHA) Class III or IV heart failure (in Study 1) or NYHA Class II to IV heart failure (in Study 2) was not established because these patients were excluded from these randomized clinical trials [see Clinical Studies (14) in full Prescribing Information]. Monitor patients for hypertension, hypokalemia, and fluid retention at least once a month. Control hypertension and correct hypokalemia before and during treatment with ZYTIGA.Adrenocortical Insufficiency: Adrenal insufficiency occurred in the two randomized clinical studies in 0.5% of patients taking ZYTIGA and in 0.2% of patients taking placebo. Adrenocortical insufficiency was reported in patients receiving ZYTIGA in combination with prednisone, following interruption of daily steroids and/or with concurrent infection or stress. Use caution and monitor for symptoms and signs of adrenocortical insufficiency, particularly if patients are withdrawn from prednisone, have prednisone dose reductions, or experience unusual stress. Symptoms and signs of adrenocortical insufficiency may be masked by adverse reactions associated with mineralocorticoid excess seen in patients treated with ZYTIGA. If clinically indicated, perform appropriate tests to confirm the diagnosis of adrenocortical insufficiency. Increased dosage of corticosteroids may be indicated before, during and after stressful situations [see Warnings and Precautions].Hepatotoxicity: In the two randomized clinical trials, grade 3 or 4 ALT or AST increases (at least 5X ULN) were reported in 4% of patients who received ZYTIGA, typically during the first 3 months after starting treatment. Patients whose baseline ALT or AST were elevated were more likely to experience liver test elevation than those beginning with normal values. Treatment discontinuation due to liver enzyme increases occurred in 1% of patients taking ZYTIGA. No deaths clearly related to ZYTIGA were reported due to hepatotoxicity events. Measure serum transaminases (ALT and AST) and bilirubin levels prior to starting treatment with ZYTIGA, every two weeks for the first three months of treatment and monthly thereafter. In patients with baseline moderate hepatic impairment receiving a reduced ZYTIGA dose of 250 mg, measure ALT, AST, and bilirubin prior to the start of treatment, every week for the first month, every two weeks for the following two months of treatment and monthly thereafter. Promptly measure serum total bilirubin, AST, and ALT if clinical symptoms or signs suggestive of hepatotoxicity develop. Elevations of AST, ALT, or bilirubin from the patient’s baseline should prompt more frequent monitoring. If at any time AST or ALT rise above five times the ULN, or the bilirubin rises above three times the ULN, interrupt ZYTIGA treatment and closely monitor liver function.Re-treatment with ZYTIGA at a reduced dose level may take place only after return of liver function tests to the patient’s baseline or to AST and ALT less than or equal to 2.5X ULN and total bilirubin less than or equal to 1.5X ULN [see Dosage and Administration (2.2) in full Prescribing Information].The safety of ZYTIGA re-treatment of patients who develop AST or ALT greater than or equal to 20X ULN and/or bilirubin greater than or equal to 10X ULN is unknown.Increased ZYTIGA Exposures with Food: ZYTIGA must be taken on an empty stomach. No food should be consumed for at least two hours before the dose of ZYTIGA is taken and for at least one hour after the dose of ZYTIGA
is taken. Abiraterone Cmax and AUC0-∞ (exposure) were increased up to 17- and 10-fold higher, respectively, when a single dose of abiraterone acetate was administered with a meal compared to a fasted state. The safety of these increased exposures when multiple doses of abiraterone acetate are taken with food has not been assessed [see Dosage and Administration (2.1) and Clinical Pharmacology (12.3) in full Prescribing Information].
ADVERSE REACTIONSThe following are discussed in more detail in other sections of the labeling:• Hypertension, Hypokalemia, and Fluid Retention due to Mineralocorticoid
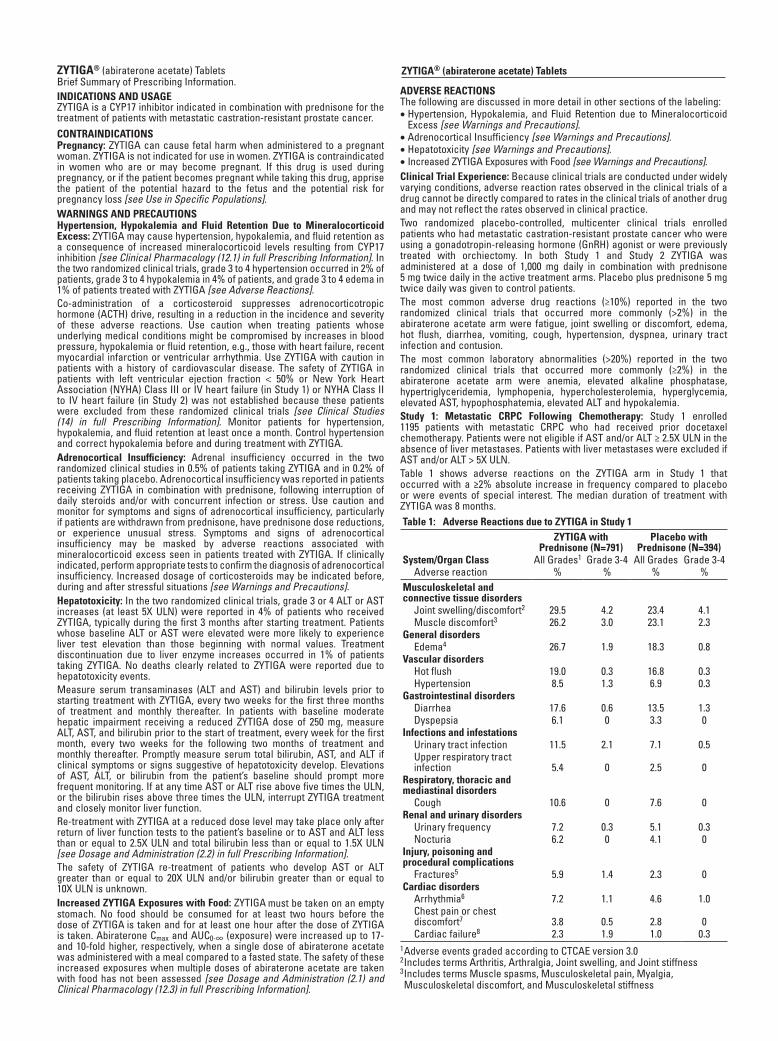
Excess [see Warnings and Precautions].• Adrenocortical Insufficiency [see Warnings and Precautions].• Hepatotoxicity [see Warnings and Precautions].• Increased ZYTIGA Exposures with Food [see Warnings and Precautions].Clinical Trial Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.Two randomized placebo-controlled, multicenter clinical trials enrolled patients who had metastatic castration-resistant prostate cancer who were using a gonadotropin-releasing hormone (GnRH) agonist or were previously treated with orchiectomy. In both Study 1 and Study 2 ZYTIGA was administered at a dose of 1,000 mg daily in combination with prednisone 5 mg twice daily in the active treatment arms. Placebo plus prednisone 5 mg twice daily was given to control patients. The most common adverse drug reactions (≥10%) reported in the two randomized clinical trials that occurred more commonly (>2%) in the abiraterone acetate arm were fatigue, joint swelling or discomfort, edema, hot flush, diarrhea, vomiting, cough, hypertension, dyspnea, urinary tract infection and contusion. The most common laboratory abnormalities (>20%) reported in the two randomized clinical trials that occurred more commonly (≥2%) in the abiraterone acetate arm were anemia, elevated alkaline phosphatase, hypertriglyceridemia, lymphopenia, hypercholesterolemia, hyperglycemia, elevated AST, hypo phosphatemia, elevated ALT and hypokalemia.Study 1: Metastatic CRPC Following Chemotherapy: Study 1 enrolled 1195 patients with metastatic CRPC who had received prior docetaxel chemotherapy. Patients were not eligible if AST and/or ALT ≥ 2.5X ULN in the absence of liver metastases. Patients with liver metastases were excluded if AST and/or ALT > 5X ULN.Table 1 shows adverse reactions on the ZYTIGA arm in Study 1 that occurred with a ≥2% absolute increase in frequency compared to placebo or were events of special interest. The median duration of treatment with ZYTIGA was 8 months.Table 1: Adverse Reactions due to ZYTIGA in Study 1
ZYTIGA with Prednisone (N=791)
Placebo with Prednisone (N=394)
System/Organ Class All Grades1 Grade 3-4 All Grades Grade 3-4Adverse reaction % % % %
Musculoskeletal and connective tissue disorders
Joint swelling/discomfort2 29.5 4.2 23.4 4.1Muscle discomfort3 26.2 3.0 23.1 2.3
General disordersEdema4 26.7 1.9 18.3 0.8
Vascular disordersHot flush 19.0 0.3 16.8 0.3Hypertension 8.5 1.3 6.9 0.3
Gastrointestinal disordersDiarrhea 17.6 0.6 13.5 1.3Dyspepsia 6.1 0 3.3 0
Infections and infestationsUrinary tract infection 11.5 2.1 7.1 0.5Upper respiratory tract infection 5.4 0 2.5 0
Respiratory, thoracic and mediastinal disorders
Cough 10.6 0 7.6 0Renal and urinary disorders
Urinary frequency 7.2 0.3 5.1 0.3Nocturia 6.2 0 4.1 0
Injury, poisoning and procedural complications
Fractures5 5.9 1.4 2.3 0Cardiac disorders
Arrhythmia6 7.2 1.1 4.6 1.0Chest pain or chest discomfort7 3.8 0.5 2.8 0Cardiac failure8 2.3 1.9 1.0 0.3
1 Adverse events graded according to CTCAE version 3.02 Includes terms Arthritis, Arthralgia, Joint swelling, and Joint stiffness 3 Includes terms Muscle spasms, Musculoskeletal pain, Myalgia, Musculoskeletal discomfort, and Musculoskeletal stiffness
ZYTIGA® (abiraterone acetate) Tablets
4 Includes terms Edema, Edema peripheral, Pitting edema, and Generalized edema
5 Includes all fractures with the exception of pathological fracture6 Includes terms Arrhythmia, Tachycardia, Atrial fibrillation, Supraventricular tachycardia, Atrial tachycardia, Ventricular tachycardia, Atrial flutter, Bradycardia, Atrioventricular block complete, Conduction disorder, and Bradyarrhythmia
7 Includes terms Angina pectoris, Chest pain, and Angina unstable. Myocardial infarction or ischemia occurred more commonly in the placebo arm than in the ZYTIGA arm (1.3% vs. 1.1% respectively).
8 Includes terms Cardiac failure, Cardiac failure congestive, Left ventricular dysfunction, Cardiogenic shock, Cardiomegaly, Cardiomyopathy, and Ejection fraction decreased
Table 2 shows laboratory abnormalities of interest from Study 1. Grade 3-4 low serum phosphorus (7%) and low potassium (5%) occurred at a greater than or equal to 5% rate in the ZYTIGA arm.Table 2: Laboratory Abnormalities of Interest in Study 1
Abiraterone (N=791) Placebo (N=394)Laboratory Abnormality
All Grades (%)
Grade 3-4 (%)
All Grades (%)
Grade 3-4 (%)
Hypertriglyceridemia 62.5 0.4 53.0 0High AST 30.6 2.1 36.3 1.5Hypokalemia 28.3 5.3 19.8 1.0Hypophosphatemia 23.8 7.2 15.7 5.8High ALT 11.1 1.4 10.4 0.8High Total Bilirubin 6.6 0.1 4.6 0
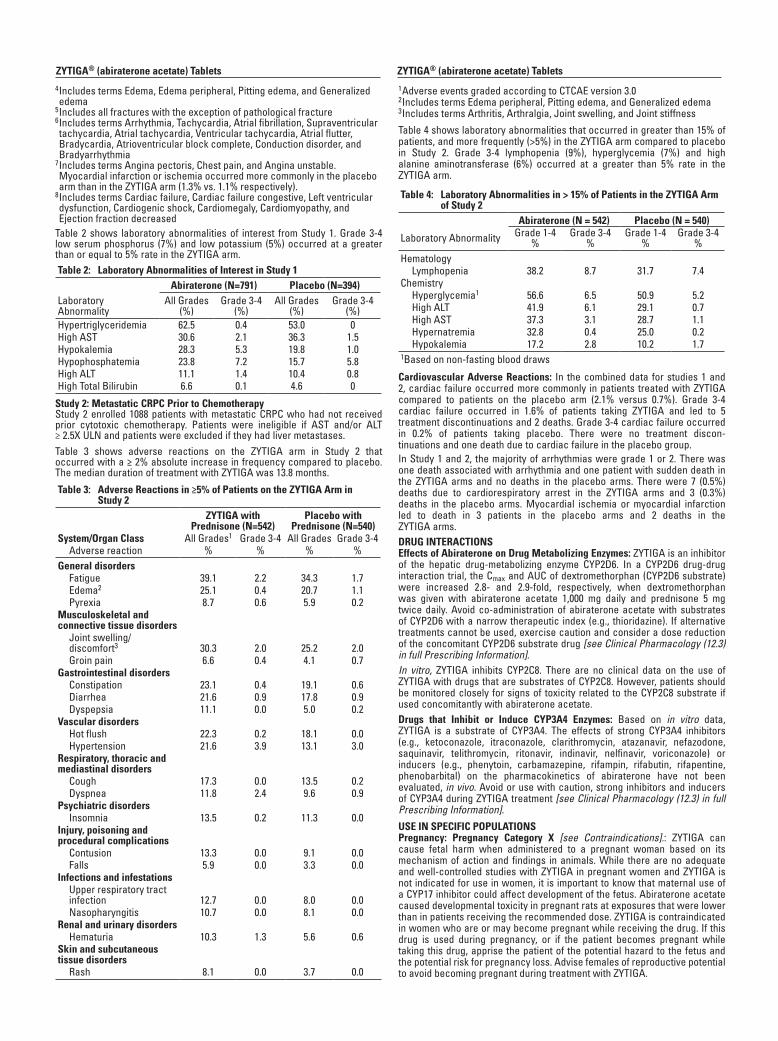
Study 2: Metastatic CRPC Prior to ChemotherapyStudy 2 enrolled 1088 patients with metastatic CRPC who had not received prior cytotoxic chemotherapy. Patients were ineligible if AST and/or ALT ≥ 2.5X ULN and patients were excluded if they had liver metastases.Table 3 shows adverse reactions on the ZYTIGA arm in Study 2 that occurred with a ≥ 2% absolute increase in frequency compared to placebo. The median duration of treatment with ZYTIGA was 13.8 months.
Table 3: Adverse Reactions in ≥5% of Patients on the ZYTIGA Arm in Study 2
ZYTIGA with Prednisone (N=542)
Placebo with Prednisone (N=540)
System/Organ Class All Grades1 Grade 3-4 All Grades Grade 3-4Adverse reaction % % % %
General disordersFatigue 39.1 2.2 34.3 1.7Edema2 25.1 0.4 20.7 1.1Pyrexia 8.7 0.6 5.9 0.2
Musculoskeletal and connective tissue disorders
Joint swelling/ discomfort3 30.3 2.0 25.2 2.0Groin pain 6.6 0.4 4.1 0.7
Gastrointestinal disordersConstipation 23.1 0.4 19.1 0.6Diarrhea 21.6 0.9 17.8 0.9Dyspepsia 11.1 0.0 5.0 0.2
Vascular disordersHot flush 22.3 0.2 18.1 0.0Hypertension 21.6 3.9 13.1 3.0
Respiratory, thoracic and mediastinal disorders
Cough 17.3 0.0 13.5 0.2Dyspnea 11.8 2.4 9.6 0.9
Psychiatric disordersInsomnia 13.5 0.2 11.3 0.0
Injury, poisoning and procedural complications
Contusion 13.3 0.0 9.1 0.0Falls 5.9 0.0 3.3 0.0
Infections and infestations Upper respiratory tract infection 12.7 0.0 8.0 0.0Nasopharyngitis 10.7 0.0 8.1 0.0
Renal and urinary disordersHematuria 10.3 1.3 5.6 0.6
Skin and subcutaneous tissue disorders
Rash 8.1 0.0 3.7 0.0
1 Adverse events graded according to CTCAE version 3.02 Includes terms Edema peripheral, Pitting edema, and Generalized edema3 Includes terms Arthritis, Arthralgia, Joint swelling, and Joint stiffness
Table 4 shows laboratory abnormalities that occurred in greater than 15% of patients, and more frequently (>5%) in the ZYTIGA arm compared to placebo in Study 2. Grade 3-4 lymphopenia (9%), hyperglycemia (7%) and high alanine aminotransferase (6%) occurred at a greater than 5% rate in the ZYTIGA arm.
Table 4: Laboratory Abnormalities in > 15% of Patients in the ZYTIGA Arm of Study 2
Abiraterone (N = 542) Placebo (N = 540)
Laboratory Abnormality Grade 1-4%
Grade 3-4%
Grade 1-4%
Grade 3-4%
HematologyLymphopenia 38.2 8.7 31.7 7.4
ChemistryHyperglycemia1 56.6 6.5 50.9 5.2High ALT 41.9 6.1 29.1 0.7High AST 37.3 3.1 28.7 1.1Hypernatremia 32.8 0.4 25.0 0.2Hypokalemia 17.2 2.8 10.2 1.7
1Based on non-fasting blood draws
Cardiovascular Adverse Reactions: In the combined data for studies 1 and 2, cardiac failure occurred more commonly in patients treated with ZYTIGA compared to patients on the placebo arm (2.1% versus 0.7%). Grade 3-4 cardiac failure occurred in 1.6% of patients taking ZYTIGA and led to 5 treatment discontinuations and 2 deaths. Grade 3-4 cardiac failure occurred in 0.2% of patients taking placebo. There were no treatment discon-tinuations and one death due to cardiac failure in the placebo group. In Study 1 and 2, the majority of arrhythmias were grade 1 or 2. There was one death associated with arrhythmia and one patient with sudden death in the ZYTIGA arms and no deaths in the placebo arms. There were 7 (0.5%) deaths due to cardiorespiratory arrest in the ZYTIGA arms and 3 (0.3%) deaths in the placebo arms. Myocardial ischemia or myocardial infarction led to death in 3 patients in the placebo arms and 2 deaths in the ZYTIGA arms. DRUG INTERACTIONSEffects of Abiraterone on Drug Metabolizing Enzymes: ZYTIGA is an inhibitor of the hepatic drug-metabolizing enzyme CYP2D6. In a CYP2D6 drug-drug interaction trial, the Cmax and AUC of dextromethorphan (CYP2D6 substrate) were increased 2.8- and 2.9-fold, respectively, when dextromethorphan was given with abiraterone acetate 1,000 mg daily and prednisone 5 mg twice daily. Avoid co-administration of abiraterone acetate with substrates of CYP2D6 with a narrow therapeutic index (e.g., thioridazine). If alternative treatments cannot be used, exercise caution and consider a dose reduction of the concomitant CYP2D6 substrate drug [see Clinical Pharmacology (12.3) in full Prescribing Information].In vitro, ZYTIGA inhibits CYP2C8. There are no clinical data on the use of ZYTIGA with drugs that are substrates of CYP2C8. However, patients should be monitored closely for signs of toxicity related to the CYP2C8 substrate if used concomitantly with abiraterone acetate. Drugs that Inhibit or Induce CYP3A4 Enzymes: Based on in vitro data, ZYTIGA is a substrate of CYP3A4. The effects of strong CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, clarithromycin, atazanavir, nefazodone, saquinavir, telithromycin, ritonavir, indinavir, nelfinavir, voriconazole) or inducers (e.g., phenytoin, carbamazepine, rifampin, rifabutin, rifapentine, phenobarbital) on the pharmacokinetics of abiraterone have not been evaluated, in vivo. Avoid or use with caution, strong inhibitors and inducers of CYP3A4 during ZYTIGA treatment [see Clinical Pharmacology (12.3) in full Prescribing Information].USE IN SPECIFIC POPULATIONSPregnancy: Pregnancy Category X [see Contraindications].: ZYTIGA can cause fetal harm when administered to a pregnant woman based on its mechanism of action and findings in animals. While there are no adequate and well-controlled studies with ZYTIGA in pregnant women and ZYTIGA is not indicated for use in women, it is important to know that maternal use of a CYP17 inhibitor could affect development of the fetus. Abiraterone acetate caused developmental toxicity in pregnant rats at exposures that were lower than in patients receiving the recommended dose. ZYTIGA is contraindicated in women who are or may become pregnant while receiving the drug. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, apprise the patient of the potential hazard to the fetus and the potential risk for pregnancy loss. Advise females of reproductive potential to avoid becoming pregnant during treatment with ZYTIGA.
ZYTIGA® (abiraterone acetate) Tablets ZYTIGA® (abiraterone acetate) Tablets

In an embryo-fetal developmental toxicity study in rats, abiraterone acetate caused developmental toxicity when administered at oral doses of 10, 30 or 100 mg/kg/day throughout the period of organogenesis (gestational days 6-17). Findings included embryo-fetal lethality (increased post implantation loss and resorptions and decreased number of live fetuses), fetal developmental delay (skeletal effects) and urogenital effects (bilateral ureter dilation) at doses ≥10 mg/kg/day, decreased fetal ano-genital distance at ≥30 mg/kg/day, and decreased fetal body weight at 100 mg/kg/day. Doses ≥10 mg/kg/day caused maternal toxicity. The doses tested in rats resulted in systemic exposures (AUC) approximately 0.03, 0.1 and 0.3 times, respectively, the AUC in patients.Nursing Mothers: ZYTIGA is not indicated for use in women. It is not known if abiraterone acetate is excreted in human milk. Because many drugs are excreted in human milk, and because of the potential for serious adverse reactions in nursing infants from ZYTIGA, a decision should be made to either discontinue nursing, or discontinue the drug taking into account the importance of the drug to the mother.Pediatric Use: Safety and effectiveness of ZYTIGA in pediatric patients have not been established.Geriatric Use: Of the total number of patients receiving ZYTIGA in phase 3 trials, 73% of patients were 65 years and over and 30% were 75 years and over. No overall differences in safety or effectiveness were observed between these elderly patients and younger patients. Other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.Patients with Hepatic Impairment: The pharmacokinetics of abiraterone were examined in subjects with baseline mild (n = 8) or moderate (n = 8) hepatic impairment (Child-Pugh Class A and B, respectively) and in 8 healthy control subjects with normal hepatic function. The systemic exposure (AUC) of abiraterone after a single oral 1,000 mg dose of ZYTIGA increased by approximately 1.1-fold and 3.6-fold in subjects with mild and moderate baseline hepatic impairment, respectively compared to subjects with normal hepatic function.No dosage adjustment is necessary for patients with baseline mild hepatic impairment. In patients with baseline moderate hepatic impairment (Child-Pugh Class B), reduce the recommended dose of ZYTIGA to 250 mg once daily. If elevations in ALT or AST >5X ULN or total bilirubin >3X ULN occur in patients with baseline moderate hepatic impairment, discontinue ZYTIGA treatment [see Dosage and Administration (2.1) and Clinical Pharmacology (12.3) in full Prescribing Information].The safety of ZYTIGA in patients with baseline severe hepatic impairment has not been studied. These patients should not receive ZYTIGA.For patients who develop hepatotoxicity during treatment, interruption of treatment and dosage adjustment may be required [see Dosage and Administration (2.2) in full Prescribing Information, Warnings and Precautions, and Clinical Pharmacology (12.3) in full Prescribing Information].Patients with Renal Impairment: In a dedicated renal impairment trial, the mean PK parameters were comparable between healthy subjects with normal renal function (N=8) and those with end stage renal disease (ESRD) on hemodialysis (N=8) after a single oral 1,000 mg dose of ZYTIGA. No dosage adjustment is necessary for patients with renal impairment [see Dosage and Administration (2.1) and Clinical Pharmacology (12.3) in full Prescribing Information].OVERDOSAGEThere have been no reports of overdose of ZYTIGA during clinical studies.There is no specific antidote. In the event of an overdose, stop ZYTIGA, undertake general supportive measures, including monitoring for arrhythmias and cardiac failure and assess liver function.Storage and Handling: Store at 20oC to 25oC (68oF to 77oF); excursions permitted in the range from 15oC to 30oC (59oF to 86°F) [see USP controlled room temperature].Based on its mechanism of action, ZYTIGA may harm a developing fetus. Therefore, women who are pregnant or women who may be pregnant should not handle ZYTIGA without protection, e.g., gloves [see Use in Specific Populations].PATIENT COUNSELING INFORMATIONSee FDA-approved patient labeling (Patient Information)• Patients should be informed that ZYTIGA and prednisone are used
together and that they should not interrupt or stop either of these medications without consulting their physician.
• Patients receiving GnRH agonists should be informed that they need to maintain this treatment during the course of treatment with ZYTIGA and prednisone.
• Patients should be informed that ZYTIGA must not be taken with food and that no food should be consumed for at least two hours before the dose of ZYTIGA is taken and for at least one hour after the dose of ZYTIGA is taken. They should be informed that the tablets should be swallowed whole with water without crushing or chewing. Patients should be informed that taking ZYTIGA with food causes increased exposure and this may result in adverse reactions.
• Patients should be informed that ZYTIGA is taken once daily and prednisone is taken twice daily according to their physician’s instructions.
• Patients should be informed that in the event of a missed daily dose of ZYTIGA or prednisone, they should take their normal dose the following day. If more than one daily dose is skipped, patients should be told to inform their physician.
• Patients should be apprised of the common side effects associated with ZYTIGA, including peripheral edema, hypokalemia, hypertension, elevated liver function tests, and urinary tract infection. Direct the patient to a complete list of adverse drug reactions in PATIENT INFORMATION.
• Patients should be advised that their liver function will be monitored using blood tests.
• Patients should be informed that ZYTIGA may harm a developing fetus; thus, women who are pregnant or women who may be pregnant should not handle ZYTIGA without protection, e.g., gloves. Patients should also be informed that it is not known whether abiraterone or its metabolites are present in semen and they should use a condom if having sex with a pregnant woman. The patient should use a condom and another effective method of birth control if he is having sex with a woman of child-bearing potential. These measures are required during and for one week after treatment with ZYTIGA.
Manufactured by:Patheon Inc.Mississauga, Canada
Manufactured for:Janssen Biotech, Inc.Horsham, PA 19044
© Janssen Biotech, Inc. 2012 Revised: December 2012
2000005445
K08Z121174A
ZYTIGA® (abiraterone acetate) Tablets ZYTIGA® (abiraterone acetate) Tablets

7 May 2013 I www.UroPracticeManagement.com I
PUBLISHING STAFFSenior Vice President/Group Publisher
Nicholas Englezos [email protected]
Vice President, Director of Sales & Marketing
Joe Chanley [email protected]
Publisher Cristopher Pires
Editorial Director Lisa Neuman
Associate Editor Lara J. Lorton
Editorial Assistants Jennifer Brandt
Cara Guglielmon
Production Manager Marie RS Borrelli
The Lynx Group President/CEO Brian Tyburski
Chief Operating Officer Pam Rattanonont Ferris
Vice President of Finance Andrea Kelly
Associate Editorial Director, Projects Division
Terri Moore
Director, Quality Control Barbara Marino
Director, Production & Manufacturing Alaina Pede
Director, Creative & Design Robyn Jacobs
Creative & Design Assistant Lora LaRocca
Director, Digital Media Anthony Romano
Web Content Managers David Maldonado Anthony Travean
Digital Programmer Michael Amundsen
Senior Project Manager Andrea Boylston
Project Coordinators Deanna Martinez
Jackie Luma
Business Manager Blanche Marchitto
Executive Administrator Rachael Baranoski
Office Coordinator Robert Sorensen
Engage Healthcare Communications 1249 South River Road - Ste 202A
Cranbury, NJ 08512 phone: 732-992-1880
fax: 732-992-1881
ehc114
Neil Baum, MDPracticing UrologistNew Orleans, LA
Cheris Craig, MBA, CMPEChief Administrative OfficerUrology of Greater Atlanta, LLCAtlanta, GA
Rick Janss, MBA, CMPEPractice AdministratorClinical Urology Associates Gadsden, AL
John McMann, MS AdministratorAdvanced Urology Specialists, LLC Oxford, FL
Jonathan Oppenheimer, MD, FCAPMedical Director, Chief Pathologist Oppenheimer Urologic Reference Laboratory Nashville, TN
James A. Sylora, MDUrologistAUS–Midwest UrologyEvergreen Park, IL
Sean M. Weiss, CCP-P, CCA-P, ACS-EM, CPC, CPC-PVice President & Chief Compliance OfficerDecisionHealth Professional ServicesGaithersburg, MD
editorial advisory board
Clinical Considerations in Treating advanced Prostate Cancer: The Changing role of the urologist ............................................................1by Matthew Wendling, MPH; Neal Shore, MD
Panel Discussion
Developing the infrastructure to adopt Newer Therapies: in-house Specialty Clinics .............................................................................................11
a New era for urology: Practice Management Considerations ..........14by Matthew Wendling, MPH; atheer a. Kaddis, PharmD; Deepak Kapoor, MD
Panel Discussion
an interactive Discussion with Practice Managers .............................. 18
Urology Practice Management™, ISSN (requested), is published 2 times a year by Engage Healthcare Communications, LLC, 1249 South River Road, Suite 202A, Cranbury, NJ 08512. Copyright © 2013 by Engage Healthcare Communications, LLC. All rights reserved. Urology Practice Management™ is a registered trademark of Engage Healthcare Communications, LLC. No part of this publication may be reproduced or transmitted in any form or by any means now or hereafter known, electronic or mechanical, including photocopy, recording, or any informational storage and retrieval system, without written permission from the publisher. Printed in the United States of America. The ideas and opinions expressed in Urology Practice Management™ do not necessarily reflect those of the editorial board, the editors, or the publisher. Publication of an advertisement or other product mentioned in Urology Practice Management™ should not be construed as an endorsement of the product or the manufacturer’s claims. Readers are encouraged to contact the manufacturers about any features or limitations of products mentioned. Neither the editors nor the publisher assume any responsibility for any injury and/or damage to persons or property arising out of or related to any use of the material mentioned in this publication.Postmaster: Correspondence regarding subscriptions or change of address should be directed to CIRCULATION DIRECTOR, Urology Practice Management™, 1249 South River Road, Suite 202A, Cranbury, NJ 08512. Fax: 732-992-1881. Yearly subscription rates: 1 year: $99.00 USD; 2 years: $149.00 USD; 3 years: $199.00 USD.
MISSION STATEMENTUrology healthcare requires providers to focus attention on financial concerns and strategic deci-sions that affect the bottom line. To continue to provide the high-quality care urology patients deserve, providers must master the ever-changing business of urology. Urology Practice Management™ will offer process solutions for members of the urology care team—medical, surgical, and radiation urologists, as well as executives, administrators, and coders/billers—to assist them in reimbursement, staffing, electronic health records, REMS, and compliance with state and federal regulations.
In This Issue

Invitation to Join the UPM Editorial BoardThe publishers of Urology Practice Management™ (UPM) are inviting qualified urologypractice owners and administrators to participate as members of the UPM Editorial Board.As an editorial board member, you will play an active role in helping to shape the contentof this exciting new publication.
Urology Practice Management is a novel publication focused on process solutions for urology practices. UPM is designed to provide the urology care team – medical, practiceadministrators, coders, and billers – with the knowledge and skills required to keep abreastof today’s fast-changing business environment, allowing practice professionals more timeto concentrate on high-quality patient care. Each issue of UPM will focus on variousareas of urology practice, featuring current topics such as:
• Healthcare technology• Models of care• Staffing• Reimbursement and coding
Take advantage of this unique opportunity to help your peers and enhance your professional reputation by becoming the newest member of the UPM Editorial Board.
For consideration to become an Editorial Board Member, please complete the form below and fax to: 732-992-1881 or e-mail to [email protected]
Your Information
_______________________________________________________________________________________First Name Last Name Credentials
_______________________________________________________________________________________Title Company
_______________________________________________________________________________________Address
_______________________________________________________________________________________E-mail Phone
Urology Practice Management™1249 South River Road, Suite 202A, Cranbury, NJ 08512
an affiliate of Establishing a patient-centered approach is rapidly becoming a core requirement in US medical prac-tices. Medical home models, account-able care organization (ACO) models,
and Health Information Technology for Economic and Clinical Health (HITECH) requirements all have com-ponents of engaging patients in their care. To incorporate a patient-centered
On October 1, 2014, the UnitedStates will adopt the International Classifi cation of Disease, Tenth Revision, Clinical Modifi cation/Procedure Cod-ing Sys tem (ICD-10-CM/PCS), 1 year later than we had initially reported in Urology Practice Management in September 2012. The reprieve, although welcome to many,
is less than 17 months away, during which several phases of implementation must be completed. The timeline for implement-ing the code sets is divided into 4 phases: Phase 1: Impact Assessment, fi rst quarter 2009 through second quarter 2012; Phase 2: Preparing for Implementation, fi rst quarter 2012 through second quarter 2014; Phase 3:
©2013 Engage Healthcare Communications, LLC
www.UroPracticeManagement.com
Urology PracticeManagement™MAY 2013
VOLUME 2 • NUMBER 1
PROCESS IMPROVEMENTS TO ENHANCE PATIENT CARE™
Continued on page 10
Continued on page 8
Continued on page 19
Exploring Men’s Willingness to Pay for Prostate Cancer Screening to Avoid Unnecessary Biopsys and Treatment By Rosemary Frei, MSc
Transitioning to ICD-10 By Susanne Talebian, CHBC, RMM, CMOM, CPC-I, CPC, CUA, CCS-P, PCS
Certifi ed Healthcare Business Consultant, American Health Information
Management Association—AHIMA Certifi ed ICD-10-CM/PCS Trainer
Implementing a Patient Portal in Your Urology Practice to Provide Patient-Centered CareBy Gena CookFounder and Chief Executive Offi cer Navigating Cancer, a leading provider
of oncology-specifi c patient portals
D utch researchers have peered into the minds and wallets of a group of men aged 55 to 75 years to determine what they are willing to trade for a reduced risk of prostate cancer–related death or to avoid unnec-essary procedures and treatment.Men with more education had a lower
probability of opting for prostate cancer screening. Furthermore, the men were willing to lose 2% of risk reduction in mortality related to prostate cancer, or to pay, on average, €188 (in 2010 euros—equivalent to $245 in 2010 US dollars) annually, for a 10% reduced risk of unnecessary biopsy or treatment.“Physicians should be aware that men,
PROSTATE
HEALTH
Prostate C
ancer
O
vervie
w...16
UPM_42513
UPM house ad pgs_2013_Layout 1 4/25/13 11:59 AM Page 1

Clinical Considerations
9 may 2013 i www.Uropracticemanagement.com i
Clinical Considerations in Treating…Continued from page 1
concerns that urologists may be over-screening and overdiagnosing pa-tients. On the other hand, aggressive screening has been effective in lower-ing the incidence of newly diagnosed metastatic disease. Furthermore, indi-viduals diagnosed with local or region-al early-stage disease typically have a favorable prognosis, with a 5-year sur-vival rate approaching 100%.6
Clinical management of prostate cancer depends on stage at time of diagnosis, life expectancy, and ag-gressiveness of disease. For patients with very low or low risk of recur-rence, the National Comprehensive Cancer Network (NCCN) recom-mends active surveillance for pa-tients with a life expectancy <20 years or <10 years, respectively, while radiation therapy, brachyther-apy, or radical prostatectomy are ad-ditional options for patients with longer life expectancies. Treatment recommendations for patients with intermediate risk of recurrence are also dependent upon life expectancy, and options may include active sur-veillance, radiation therapy, andro-gen deprivation therapy (ADT), brachytherapy, or radical prostatec-tomy. Active surveillance is not rec-ommended for patients with high or very high risk of recurrence, and ra-diation therapy and ADT are recom-mended for most patients, with or without brachytherapy. Radical prostatectomy also remains a treat-ment option for these patient popu-lations. ADT alone may be consid-ered in select patients with a very high risk of recurrence.7
Prostate cancer progression is sen-sitive to testosterone and androgens. Lowering androgen levels has been shown to reduce the probability of early cancer recurrence, or slow growth in advanced patients. There-fore, ADT is a mainstay for patients with advanced prostate cancer. There are a number of different agents
characterized as ADT. The most rec-ognizable brand marketed in the United States is Lupron (leuprolide acetate). In addition to ADT, urolo-gists may or may not add a secondary antiandrogen agent such as nilut-amide, bicalutamide, or flutamide.7
It is important to recognize that ADT can have a number of side ef-fects, including hot flashes and flush-ing; bone demineralization, which can lead to osteoporosis; and central weight gain and insulin resistance, which may contribute to the onset of diabetes and cardiovascular disease. In recent years, urologists have gained a better understanding of those toxicities. Even though ADT is often started early, patients are re-ceiving better nutritional and car-diovascular care than in the past.
Nonetheless, overuse of ADT re-mains a concern. It is recommended for adjuvant therapy with radiation in intermediate-, high-, and very high-risk patients, and in patients with metastatic disease.7
A number of antiandrogen thera-pies, including leuprolide, goserelin, triptorelin, and histrelin, are available in the United States for palliative treatment of advanced prostate can-
cer. Antiandrogens are frequently prescribed to patients with prostate cancer after PSA relapse, although not specifically indicated for this pop-ulation. In addition, starting ADT in patients with asymptomatic metastat-ic disease remains controversial.8-12
In castration-recurrent prostate cancer (CRPC), the patient progress-es despite primary androgen depriva-tion therapy or bilateral orchiectomy. CRPC is characterized by a rising PSA level despite a testosterone level <50 ng/dL.7,13 There are a number of treatment options for CRPC, as noted in guidance from NCCN.7
Cytotoxic chemotherapeutic agents for the treatment of patients with advanced prostate cancer include docetaxel and cabazitaxel. In 2004, Taxotere (docetaxel) was approved for use in patients with metastatic CRPC. Taxotere is administered concomitantly with prednisone. Al-though 20% to 30% of patients have grade 3 and grade 4 toxicities, the majority of patients tolerate Taxotere reasonably well. Given in combina-tion with prednisone every 3 weeks, Taxotere gives patients a 2.4-month overall survival advantage compared with mitoxantrone and prednisone.14
Jevtana (cabazitaxel), a microtu-bule inhibitor indicated in combina-tion with prednisone, was approved in 2010 for patients previously treat-ed with a docetaxel-containing treat-ment regimen. Jevtana has demon-strated a 2.4-month overall survival advantage compared with mitoxan-trone and prednisone in this patient population.15
Until recently, most patients who progressed despite ADT were given cytotoxic chemotherapy. However, the treatment landscape has been changing, and there have been sever-al new developments in treating pa-tients with metastatic CRPC (Table).
Provenge (sipuleucel-T), which was approved in 2010, is an immuno-
Continued on page 10
until recently, most patients who progressed despite aDT were given cytotoxic chemotherapy. but the treatment landscape has been changing, and there have been several new developments in treating patients with metastatic CrPC.

10 I UroLogy practice management i may 2013
Clinical Considerations
Clinical Considerations in Treating…Continued from page 9
therapeutic agent with a 4-week to 6-week course of therapy that is indi-cated for asymptomatic or minimally symptomatic disease. In 2 clinical studies, patients taking Provenge had a 4.1-month and a 4.5-month overall survival advantage compared with controls. In clinical trials, the most common adverse events reported in patients treated with Provenge were chills, fatigue, fever, back pain, nau-sea, joint ache, and headache. Serious adverse events included acute infu-sion reactions, cerebrovascular events, and single case reports of eosinophil-ia, rhabdomyolysis, myasthenia gra-vis, myositis, and tumor flare.16
Zytiga (abiraterone acetate), an oral agent given once daily in con-junction with prednisone, was ini-tially approved in 2011 for patients with metastatic CRPC after cyto-toxic chemotherapy, and in De-cember 2012, received US Food and Drug Administration approval for patients with metastatic CRPC prior to cytotoxic chemotherapy. In a clinical trial, patients achieved a 35.3-month median overall sur-vival with Zytiga and a near dou-bling of radiographic progres-sion-free survival. In addition, for patients taking Zytiga, median time to initiation of cytotoxic che-motherapy was 25.2 months. The side effects of Zytiga may include fluid retention, which can cause an
increase in blood pressure, and occasionally, lowering of potassi-um levels and elevation of liver functions. Liver function tests are recommended for patients receiv-ing Zytiga. In the postchemothera-py setting, the phase 3 Zytiga trial improved survival by a median time of 3.9 months in the primary survival analysis and 4.6 months in an updated survival analysis.17
Another oral agent, Xtandi (en-zalutamide), was approved as mono-therapy in September of 2012 for patients with metastatic CRPC who have previously received docetaxel. Xtandi is given once daily, and was shown to extend overall survival by 4.8 months. Side effects that require monitoring include fatigue, diarrhea, hot flushes, and headache. In a piv-otal phase 3 clinical trial, 7 patients receiving Xtandi reported seizures versus no patients in the placebo
group. Overall, however, Xtandi is regarded as a well-tolerated drug.18
Although some physicians pre-scribe secondary therapies after pro-gression on ADT, such as keto-conazole, steroids, and estrogens, these drugs all have significant side effects and none have been shown in a phase 3 trial to improve overall survival. With new therapeutic agents available, some urologists are beginning to view secondary hor-monal maneuvers as a delaying tac-tic that may adversely affect patient access to approved therapies with demonstrable survival benefit.
The approval of 3 new (not cyto-toxic) agents since 2010 is changing the way that urologists may think about advanced prostate cancer. Al-though some urologists are begin-ning to incorporate these therapies into clinical practice, panelists noted 2 primary barriers to entry. First, physicians are often slow to change their practice patterns. After a peri-od of cumulative clinical experience, they can develop a comfort level prescribing newer therapies, even for agents with new side effects, as long as toxicities are manageable and out-comes are relatively predictable. Conversely, urologists may initially have concerns about managing tox-icities for unfamiliar drugs. In addi-tion to clinical considerations, it may be necessary to dedicate staff
Table. New Agents Among Treatment Recommendations for Metastatic CRPC7,a
Symptomatic disease Asymptomatic disease Symptomatic disease after treatment with docetaxel
• Abiraterone acetate • Enzalutamide
• Sipuleucel-Tb (category 1)c
• Abiraterone acetate (category 1)c
• Enzalutamide
• Abiraterone acetate (category 1)c
• Enzalutamide (category 1)c
aUnless specified, all recommendations are category 2A, which means that, based on lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate.bAppropriate for asymptomatic or minimally symptomatic patients.cBased on high-level evidence, there is uniform NCCN consensus that the intervention is appropriate.CRPC indicates castration-recurrent prostate cancer; NCCN, National Comprehensive Cancer Network.
The approval of 3 new (not cytotoxic) agents since 2010 is changing the way that urologists may think about advanced prostate cancer.
Clinical Considerations
11 may 2013 i www.Uropracticemanagement.com i
Continued on page 12
and resources to develop the clinical and business infrastructure to sup-port adoption of new agents. Fur-thermore, practices may also need to develop expanded data collection and reporting mechanisms to pro-vide payers with information to sup-port quality initiatives or risk man-agement programs.
Although it may require an initial investment, many practices find that adoption of newer agents, including oral therapies, allows them to better serve their patients with CRPC. The urologists represented on the panel agreed that these agents are efficacious and have manageable toxicities and improved outcomes. Furthermore, there was general agreement from the panel that new oral therapies allow
the clinical practice to retain patients and provide continuity of care. l
Author Disclosure StatementMr Welz has nothing to disclose. Dr
Shore is a consultant to Amgen, Astellas, Bayer, Dendreon, Ferring, Janssen, Millennium, and Medivation.
References1. US Cancer Statistics Working Group. United States Cancer Statistics: 1999–2009 Incidence and Mortality Web-based Report. Atlanta, GA: Centers for Disease Control and Prevention, and National Cancer Institute, US Department of Health and Human Services; 2012.2. Urology Care Foundation: Official Foundation of the American Urological Association. Prostate Cancer. http:// www.urologyhealth.org/urology/index.cfm?article=146. Updated March 2013. Accessed April 22, 2013.3. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11-30.4. American Urological Association. Information Sheet: Prostate-Specific Antigen (PSA) Testing for the Early Detection of Prostate Cancer. 2012.5. Etzioni R, Gulati R, Tsodikov A, et al. The prostate cancer conundrum revisited: treatment changes and prostate cancer mortality declines. Cancer. 2012;118: 5955-5963.
6. American Cancer Society. Prostate Cancer Overview. http://www.cancer.org/cancer/prostatecancer/detailed guide/prostate-cancer-survival-rates. Updated January 17, 2013. Accessed April 22, 2013.7. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Prostate Can-cer. Version 2.2013. http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf. Accessed April 11, 2013.8. Lupron Depot [package insert]. North Chicago, IL: AbbVie Inc; 2013.9. Eligard [package insert]. Bridgewater, NJ: sanofi- aventis US LLC; 2013.10. Zoladex [package insert]. Wilmington, DE: Astra Zeneca Pharmaceuticals LP; 2012.11. Trelstar [package insert]. Parsippany, NJ: Watson Pharma, Inc; 2013.12. Vantas [package insert]. Malvern, PA: Endo Phar-maceuticals Inc; 2012.13. Abdulla A, Kapoor A. Emerging novel therapies in the treatment of castration-resistant prostate cancer.Can Urol Assoc J. 2011;5:120-133.14. Taxotere [package insert]. Bridgewater, NJ: sanofi- aventis US LLC; 2010.15. Jevtana [package insert]. Bridgewater, NJ: sanofi- aventis US LLC; 2012.16. Provenge [package insert]. Seattle, WA: Dendreon Corporation; 2011.17. Zytiga [package insert]. Horsham, PA: Janssen Biotech, Inc; 2012.18. Xtandi [package insert]. San Francisco, CA: Astellas Pharma US, Inc; 2012.
A number of practices represented on the panel have implemented or are in the process of implementing internal specialty referral mecha-nisms. These “specialty clinics” are typically staffed by a small panel of urologists interested in prescribing newer therapies for advanced prostate cancer. The following exchange be-tween several of the panelists high-lights the challenges in developing internal specialty referral programs.
Gary Kirsh (Moderator): We have hired and trained a staff person
(navigator) to review every luteinizing hormone-releasing hormone (LHRH) injection, every month, from the elec-tronic medical record (EMR). We’ve developed an entire protocol that buck-ets patients into 2 groups: CRPC with metastases, and CRPC with no metas-tases but a PSA >5.
These patients are targeted for refer-ral to a small, limited panel of 4 or 5 urologists within our practice. In terms of process, the navigator notifies the primary treating urologist that their patient qualifies for the CRPC clinic, then calls the patient and offers them
an appointment with a urologist on the panel who can provide specialty care. These urologists all have a comfort level in prescribing and managing newer therapies such as Provenge, Zytiga, and Xtandi.
Jonathan Henderson: We began implementing a very similar program about 2 months ago. We realized that we had about 3600 patients who had received LHRH therapy, yet only about 20 to 30 of them had re-ceived Provenge. From the numbers alone, we knew that we were missing
Developing the infrastructure to adopt Newer Therapies: in-house Specialty Clinics
Panel DiscussionJonathan Henderson, MDPracticing UrologistRegional Urology
Deepak Kapoor, MDChief Executive OfficerIntegrated Medical Professionals
Gary Kirsh, MDPresidentThe Urology Group
Earl WalzChief Executive OfficerThe Urology Group

12 I urology Practice ManageMent i May 2013
Panel Discussion
patients who would be eligible for Provenge and Zytiga.
The patient identification process at Regional Urology is a little differ-ent from the process outlined by Dr Kirsh. Our physician assistant re-views the charts of all patients who have been receiving LHRH therapy, and inputs CRPC and metastatic CRPC dummy codes into the EMR.
Deepak Kapoor: We recently con-ducted a pilot program in which we assigned a staff person to track every LHRH injection. It took about 2 business days to track all of the prior month’s LHRH injections. Similar to Dr Henderson’s practice, we used dummy codes M0 and M1 for CRPC and metastatic CRPC, respectively.
Kirsh: Use of dummy codes is one approach. If you are using an ancillary staff person to review and put those codes in, it works. If you rely on the urologist to put the dummy code in, the results may not be optimal.
Earl Walz: Perhaps we should start thinking about ICD-10, which
is expected to break down code 185 (malignant neoplasm of prostate), into more detail than current ICD-9-CM coding. If we’re using dummy codes, can we use dummy codes to correspond with anticipated ICD-10-CM coding?
Kapoor: Unfortunately, for most EMRs, you will need to crosswalk your dummy codes into ICD-10, be-cause we don’t really know the code architecture for ICD-10 at this time. Logistically, it may just be easier to create dummy codes using current ICD-9 coding and then crosswalk the code when your EMR is updated to ICD-10.
Kirsh: There are other issues in ad-dition to the mechanics of identifying patients. We felt that it was important to involve our clinical research depart-ment. When we began speaking with all our stakeholders, we found that there were competing goals within the organi-zation. Specifically, the research depart-ment operated somewhat independently in terms of their financial accountability to the organization. There was discus-
sion about which patients should be re-ferred to specialty urologists and which patients should be referred to the clinical trial program. We brought together all the stakeholders and worked out a pro-tocol that everybody agreed was in the best interests of the patient.
Although we recognize the challeng-es of actively redirecting care from a patient’s traditional urologist to a spe-cialty panel, we are committed to moving forward, and referring selected patients to the CRPC panel. Physi-cians participating on the CRPC panel must complete an educational orienta-tion session, and we will institute peri-odic meetings to review and adjust protocols in response to clinical experi-ence and new products as they enter the marketplace.
Henderson: Our practice has a shared compensation model, which removes any financial incentive for urologists to prescribe certain thera-pies. The panel is comprised of urol-ogists who have a clinical interest in treating patients with advanced dis-ease. So far, it is working out well for our practice. l
Developing the infrastructure to adopt…Continued from page 11

Do you have a practicemanagementsolution to share
Send us your ideas!Submit a 1,000- to 2,000-word original article, previously unpublished and submittedexclusively to Urology Practice Management, that your fellow practice managers willwant to read.
Call for submissions
In your background as a urology practice manager, it’s likely there’s onebusiness experience—and maybe more—that practice managers acrossthe nation would want to read about.
High-interest topics include: the solution you found to a practice manage-ment challenge, reimbursement, your experience with EMR, Medicare audits, a memorable encounter that shaped the way you now run yourbusiness and/or practice medicine, or how you successfully integrated ancillary products and services into your practice as a revenue-generator.
Submit to: Editorial Department Fax to: 732-992-1881 or e-mail to [email protected]
UPM_42513
??Urology PracticeManagement™
PROCESS IMPROVEMENTS TO ENHANCE PATIENT CARE™
UPM house ad pgs_2013_Layout 1 4/25/13 11:54 AM Page 3

14 I urology Practice ManageMent i May 2013
A New Era for Urology
a New era for urology: Practice Management Considerationsby Matthew Wendling, MPH; atheer a. Kaddis, PharmD; and Deepak Kapoor, MDMr Wendling is Medical Writer, engage Healthcare Communications; Dr Kaddis is Senior Vice President, Diplomat Specialty Pharmacy, Flint, Mi; Dr Kapoor is Chief executive officer, integrated Medical Professionals, Melville, Ny
Overall, the practice of medi-cine has been evolving in re-cent years, and the specialty
of urology has been no exception. These changes are being driven by a combination of clinical and econom-ic factors, including therapeutic inno-vation, improved surgical techniques, and perhaps most prominently, a pol-icy environment in which purchasers of healthcare are increasingly focused on accountability, quality, and value. These changes are having a profound effect on urology practice manage-ment from a business as well as a clinical perspective.
Early screening, identification, and treatment of patients with prostate cancer have had a considerable effect on the clinical course of the disease. Patients are diagnosed earlier and are living longer with prostate cancer than ever before.
As a result, prostate cancer is in-creasingly viewed as a chronic disease. This has important ramifications for purchasers of healthcare. As patients live longer, they receive treatment for a longer period of time, which in-creases the cost of care. Of course, many lower-risk prostate cancer pa-tients may be managed by active sur-veillance, and minimization of over-treatment in lower-risk patient populations may mitigate the increas-ing cost of treating advanced prostate cancer patients to some degree.
In the past, payers have been somewhat hesitant to institute utili-zation management controls in on-cology. However, in recent years, the utilization management paradigm in oncology has begun to align more closely with management approach-
es for other chronic illnesses such as diabetes, COPD, and heart failure, to name a few. Utilization management approaches currently being used by payers in oncology include prior au-thorization (PA), quantity limits, clinical treatment pathways, differ-ential tiering, and in an increasing number of categories, step edits. Fur-thermore, specialty pharmacy is play-ing a more important role in distribu-tion and management, particularly
with the newer oral agents. The en-suing discussion will focus on the practice management challenges faced by today’s urology community as well as some of the solutions that are being implemented by progres-sive practices.
Navigating Prior AuthorizationThe urology practices represented
on the Steering Committee noted
that an increasing number of pros-tate cancer agents are subject to payers’ PA requirements. Fulfilling PA requirements may be resource intensive and make it necessary that assigned staff receive proper orienta-tion and training. In support of PA requirements, practices may be re-quired to submit laboratory data, medication history, and other sup-porting information. Furthermore, the typical urology practice sees pa-tients with coverage provided by a range of commercial and Medicare insurance plans. The specific PA re-quirements may be different for each of these payers. In addition to PAs for oncology drugs, many payers re-quire precertification to establish medical necessity for radiation and surgical procedures.
The urology practices represented on the panel vary in the way they navigate payer requirements. For practices with one central location, it may be logical to assign PA/precer-tification responsibilities to a single individual. However, this approach may not be optimal for practices with a number of different offices. These practices may be better served by assigning PA responsibilities to an individual at each satellite office.
Panelists noted that PA require-ments vary by therapy as well as payer. This may also impact the deci-sion to centralize PA responsibilities to a single individual or small number of dedicated staff. In general, more complex therapies may be subject to more complicated PA requirements. For example, the PA for immuno-therapy may require urology offices to provide more information than other
early screening, identification, and treatment of patients with prostate cancer have had a considerable effect on the clinical course of the disease. Patients are diagnosed earlier and are living longer with prostate cancer than ever before.

15 May 2013 I www.UroPracticeManagement.com I
A New Era for Urology
PAs, including ECOG status, family history, and CT scans prior to approv-al. It may be logical to assign more complex PAs to a single individual, while allowing satellite office staff to process more straightforward PAs on higher-volume medications.
Working with Specialty Pharmacies
Specialty pharmacy provides com-prehensive and coordinated patient management plans for chronic ill-nesses and complex medical condi-tions. In specialty pharmacy, distri-bution focuses on drugs that are high cost and administratively and clini-cally intensive. Specialty pharmacies are involved in a continuum of ac-tivities beginning with intake man-agement through drug fulfillment (Figure 1). Underlying all of these activities is drug therapy manage-ment, a critical function that can help urology practices manage cer-tain patient populations.
Traditionally, specialty pharmacy distribution has focused primarily on self-administered oral or injectable medications. However, because of market forces and the decreasing at-tractiveness of the “buy and bill” drug purchasing model, many specialty pharmacies now have an increased role in dispensing and managing of-fice-administered drugs as well.
There is no standard definition for a specialty pharmaceutical. Howev-er, the Centers for Medicare & Med-icaid Services set a minimum cost for medications included in specialty tiers, specifically, prescriptions cost-ing more than $600 per month.1
Many other stakeholders have adopt-ed this way of characterizing special-ty drugs. Notably, there is no stan-dard designation for specialty pharmaceuticals—they are not la-beled as such by the US Food and Drug Administration (FDA) or any other regulatory body.
Specialty pharmacies are owned and operated by a number of stake-
holders in the healthcare market. The major pharmacy benefit manag-ers own the largest specialty phar-macies. Some health plans also op-erate their own specialty pharmacies. In addition, there are a number of independent specialty pharmacies. Some oncology practices dispense specialty pharmaceuticals, even oral oncolytics, which makes them a de facto specialty pharmacy. Tradition-al specialty pharmacies provide back-end support services through group purchasing organization rela-tionships with some of these large dispensing practices.
In recent years, cost trends have been minimal for traditional drugs, whereas specialty drug costs have been increasing by 15% to 25% per year. Most experts expect the trend to continue for at least the next 5 years, as shown in Figure 2. Due in large part to these cost trends, payers con-tract with specialty pharmacies to help manage the utilization and costs associated with specialty medications.
Drug pipelines are a major factor in driving specialty drug cost trends. Nearly 60% of the new FDA approv-als in 2012 were specialty drugs, and this trend is expected to accelerate in the coming years.2
A substantial proportion of the pipeline drugs are oral therapies, signifying a major shift from inject-able and infusion therapies, which have traditionally constituted the bulk of the specialty market. It should be noted that the majority of these new molecular entities are oncolytic agents, and several will
impact urology practices. An increasing number of specialty
drugs are being covered by payers’ pharmacy benefit, which is typically the domain of oral drugs. Looking specifically at prostate cancer, more and more patients are being diag-nosed at a younger age. These younger patients typically enroll in commercial, rather than Medicare Part D, coverage. This is an impor-tant distinction, because Part D benefit designs often require more patient cost-sharing than commer-cial coverage. In addition, PA and other utilization management re-quirements may be different for these 2 types of coverage.
There are 3 distribution models used for specialty drugs. The first of these is exclusive distribution, which takes place when a manufac-turer chooses to work with 1 phar-macy as a sole dispensary. This type of distribution is usually limited to drugs with a very small patient pop-ulation, for example, cabozantinib and vandetanib for medullary thy-roid cancer.
More commonly, manufacturers limit the distribution of their pro d-ucts to a handful of pharmacies or limited distribution panels. The vast majority of these limited distribution panels must meet specific require-ments that are developed by manu-facturers. In a limited distribution arrangement, manufacturers typical-ly contract with 5 to 15 specialty pharmacies to dispense a product. Many manufacturers choose limited distribution because it gives them
Intake Management Benefits Investigation Drug Fulfillment
Drug Therapy Management
Figure 1. The Role of Specialty Pharmacy
Source: Diplomat Specialty Pharmacy.
Continued on page 16

16 I urology Practice ManageMent i May 2013
A New Era for Urology
excellent control over their product, particularly when partnering with specialty pharmacies that offer com-prehensive drug therapy manage-ment programs. In other cases, the manufacturer may use specialty phar-macies to collect data in support of their risk evaluation and mitigation strategy (REMS) program, which may be mandated by the FDA when the product is approved.3-5
Drug therapy management is a valuable service provided by most specialty pharmacies. When adopt-ing new oral therapies into their treatment armamentarium, some urologists on the panel expressed concern about patient adherence to
these therapies, citing across-the-board suboptimal adherence rates for self-administered drugs in all thera-peutic categories.
Practices, as well as payers and pharmacies, employ a number of techniques in an effort to improve adherence, including telephonic out-reach. For the products they dispense, with access to real-time patient data, specialty pharmacies are perhaps best positioned to conduct telephonic outreach to patients. These calls are typically made either proactively or when it has been determined that a patient has not refilled their prescrip-tion within a predetermined window of time. If a new prescription is re-
quired, specialty pharmacies may also notify the prescriber.
Many payers have instituted split-fill programs, where a 15-day supply of a newly prescribed medication is dis-pensed and patients are monitored closely to ensure that they are tolerat-ing the drug. In split-fill programs, the specialty pharmacy is often contractu-ally responsible for conducting the telephonic outreach. These types of outreach programs, done in conjunc-tion with patient education, have been effective in promoting compli-ance with prescribed therapy, thereby impacting both the quality-of-care and cost-containment efforts, because noncompliance is costly.
Specialty pharmacies engage in other activities to support drug ther-apy management. They collect data from patients on potential side ef-fects, and are able to monitor situa-tions that may require dose adjust-ment. Specialty pharmacies can also assist urology offices in navigating payer utilization management re-quirements. As payers begin to man-age drugs to treat patients with pros-tate and other urologic cancers more aggressively through PAs, quantity limits, and differential tiering, spe-cialty pharmacy providers can help urology practices alleviate the stress around some of these barriers.
With these changes in the market-place, it becomes even more impor-tant for specialty pharmacies to dem-onstrate value to their customers.
Group Practice Integration Urology practices are being forced
to adapt to today’s rapidly changing business environment. Declining re-imbursement and increasing expens-es have forced practices to improve business efficiencies in order to thrive. The Accountable Care Act and other healthcare legislation are also driving a shift away from tradi-tional fee-for-service–based payment
a New era for urology…Continued from page 15
Source: Specialty Drug Trend Across the Pharmacy and Medical Benefit. Artemetrx —a PSG Company; 2013.
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0% 2012 2013 2014 2015 2016 2017 2018
30% 34% 38% 42% 45% 48% 50%
70% 66% 62% 58% 55% 52% 50%
Figure 2. Traditional and Specialty Drug Cost Trends
Traditional Specialty
Trend Forecast by Year and Drug Type
Drug Type 2013 2014 2015 2016 2017 2018
Traditional 2% 3% 4% 4% 5% 6%
Specialty 20% 22% 21% 19% 18% 17%
Forecasted Net Prescription Drug Spend %, Traditional and Specialty, for Commercial Plan Sponsors

Clinical Considerations
17 May 2013 I www.UroPracticeManagement.com I
A New Era for Urology
models and we are entering an era where risk-based payment may be-come the rule rather than the excep-tion. As a result, practices are en-countering an increased regulatory burden and increased pressure to standardize care.
In response to financial pressure, many urology practices have accepted acquisition offers from hospitals and health systems in their areas. Al-though urologists may realize some benefits from these arrangements in terms of guaranteed income and re-duced risk exposure, as hospital em-ployees they may also experience a loss of fiscal autonomy and clinical independence. Hospitals, like most other businesses, seek to contain their vendor expenses, and struggling urol-ogy practices may not be in the most ideal negotiating situation. Further-more, the historical payment advan-tage to hospitals is under attack, as the Medicare Payment Advisory Commission (MedPAC) continues to discuss equalization of office-based and hospital outpatient department payment rates.
Group practice integration is an-other option for today’s urology prac-tices. Consolidation helps to build the economies of scale required for urology practices to have the negoti-ating and purchasing leverage re-quired in today’s highly competitive healthcare environment. It also makes it easier for practices to obtain capital-intensive resources such as pathology laboratories, diagnostic imaging, and radiation oncology equipment and specialty staff, if they choose to do so.
Integration puts practices in a bet-ter position to assume risk. Medicare enables providers to form account-able care organizations, participate in shared savings programs, and cre-ate novel reimbursement models such as bundled payments.6 In addi-tion, integration may also allow a practice to contract directly with third-party payers, particularly if the practice can demonstrate that it of-fers an integrated suite of services for a patient.
Integrated urology practices can meet today’s regulatory challenges by developing the infrastructure to sup-port clinical standardization and en-forcing policies that member physi-cians have collectively agreed on. Clearly defined utilization review, quality management, and compliance processes are needed to generate the data requested and are sometimes re-quired by purchasers of healthcare.
Perhaps the greatest challenge for integrating group practices is to overcome the competitive internal practice environment that often ex-ists and develop a unified culture of
shared clinical risk from the begin-ning. Once consensus is reached regarding policies and processes to support clinical standardization ef-forts, it is critical for the practice to empower leadership to enforce those policies.
An integrated, well-managed, shared-risk group practice model al-lows physicians to retain their pro-fessional and economic indepen-dence. In today’s shifting healthcare treatment paradigm, it may afford urologists the best opportunity to provide optimal patient care, make independent clinical decisions, and exercise some degree of control over their financial circumstances. l
Author Disclosure StatementMr Welz has nothing to disclose.
Dr Kaddis has nothing to disclose. Dr Kapoor is on the Medical Advisory Board for Strand Diagnostics’ know error sytem.
References1. National Opinion Research Center (NORC) and Georgetown University for the Medicare Payment Advisory Commission (MedPAC). Drugs on Specialty Tiers in Part D. NORC and Georgetown University. http://www.medpac.gov/documents/feb09_drugson specialtytiers_contractor_rs.pdf. Published February 2009. Accessed March 20, 2013.2. Tharaldson A; Express Scripts Lab. 2012: Landmark Year for Drug Approvals. http://lab.express-scripts.com/prescription-drug-trends/2012-landmark-year-for-drug-approvals/. Published March 28, 2013. Accessed April 15, 2013.3. Pharmaceutical Studies Group. Understanding Spe-cialty Pharmacy Management and Cost Control. Pharma-ceutical Strategies Group, LP; June 2010.4. Sharon B. 2010 Health Care Trend Survey: Summer. Aon Consulting; 2010.5. EMD Serono. EMD Serono Specialty Digest, 7th Edition: Managed Care Strategies for Specialty Pharma-ceuticals. EMD Serono, Inc; 2011.6. Innovation Models. Centers for Medicare & Medic-aid Services (CMS) Web site. http://innovation.cms.gov/initiatives/index.html. Accessed April 23, 2013.
an integrated, well-managed, shared-risk group practice model allows physicians to retain their professional and economic independence.

18 I urology Practice ManageMent i May 2013
Panel Discussion
Management of a urology office—large or small—is fraught with chal-lenges, particularly in an era of rap-idly evolving regulatory and fiscal environments. Increasing costs and decreasing reimbursements have forced practices to adapt by offering new products and services, maximiz-ing business efficiencies, and forming strategic alliances. The following in-teractive discussion highlights the challenges and outlines potential solutions for the issues faced by to-day’s urology practices, especially in adopting new treatment options for advanced prostate cancer.
Gary Kirsh (Moderator): As practice administrator, what would you say are the foremost practice manage-ment challenges in the CRPC land-scape right now?
Debbie Barnes: My biggest chal-lenge is non–physician staffing—not having enough time to do all the things we need to do for our CRPC patients. Our staff is currently over-whelmed, so we need to look at our staffing models to see if we can real-locate anyone. Another option may be to hire more staff.
Kirsh: Sharon, is your group facing similar challenges in treating CRPC?
Sharon Rouleau: We’re a rela-tively large practice, and we really haven’t had too much of a challenge
with staffing. I think our biggest challenge is in our relationships with the (medical) oncology providers in our area, particularly with regard to treatment recommendations. There are local oncologists who also see some of our patients. They are advis-ing some of these patients to choose a different course of therapy than what was recommended by our pro-viders. Unfortunately, we are finding that the oncologists don’t communi-cate their recommendations to our physicians—instead we hear about them from the patients. In my opin-ion, that’s been our biggest hurdle in treating CRPC patients.
Kirsh: Kathy, what has been your most important challenge in adopting newer therapies?
Kathy Hille: We’re an 18-urolo-gist group, and we do not have a physician champion in the oncology arena. Our compensation model is not set up to encourage internal re-ferrals. Even if we had a physician champion or two, I fear there would still be reluctance to refer within the group and let that patient go. That’s how I see it from an administrative perspective.
Kirsh: Kathy, I think your candid comment applies to many of the large urology groups in the country. It’s an extremely important concept, and the reluctance to make specialty internal
referrals may hamper groups from pro-gressively embracing new therapies as well as the new reimbursement models that we’re going to see.
What about challenges when you first begin adoption of some of the newer therapies that have become available for advanced prostate cancer?
Rouleau: Manufacturer support is critical, and overall, they have done a good job in supporting us. First impressions are also very important when it comes to reimbursement for a new product. The one thing you don’t want as a practice is to have a bad experience with reimbursement early on, because once you have a bad experience, then adoption of the product gets shut down before it can begin. Fortunately, we really haven’t had any such problems.
Carol Sather: When the office first begins prescribing a new ther-apy, it’s important for the practice manager to closely monitor the ther-apy and not delegate this task to of-fice staff. You really have to watch the first couple of prescriptions that come through so you can inform your physicians, and your vendors, if any problems arise.
Hille: I agree. In our practice, the business office manager takes on new therapies personally, handling the first 4 or 5 cases, and then delegating to a select supervisor within the
an interactive Discussion with Practice Managers
Panel DiscussionDebbie Barnes, CMPEPractice AdministratorUrology Associates of Central Missouri
Kathy Hille, PhDChief Executive OfficerHouston Metro Urology
Deepak Kapoor, MDChief Executive OfficerIntegrated Medical Professionals
Gary Kirsh, MDPresidentThe Urology Group
Sharon RouleauPractice ManagerUrology Specialists, PC
Carol SatherPractice AdministratorAdvanced Urology Associates
Earl WalzChief Executive OfficerThe Urology Group

Clinical Considerations
19 May 2013 I www.UroPracticeManagement.com I
group. So I think use of these new therapies requires very close atten-tion until the process works like a really well-oiled machine. Occasion-ally we will encounter challenges with very needy patients who ask detailed clinical questions that we have to refer back to the satellite office. Sometimes it can be a chal-lenge to communicate clearly with these patients and handle their needs with sensitivity.
Kirsh: I wonder if you can provide some additional insights regarding op-erational issues. For example, are the PAs done by satellite office staff? Are the copays collected across the organi-zation the same way?
Barnes: We have a single location, so the process is very simple opera-tionally. I have 1 person responsible for PAs for the entire practice.
Hille: Our PAs are done by loca-tion. We have ancillary services in our corporate office where I am, but
all of the general urology locations are in the periphery. There is 1 per-son in each office who gets the PAs and follows through on them. If it is a 1- or 2-physician office, PAs are probably not a big part of that per-son’s job. However, if there are 6 physicians in the office, that person is devoting a considerable part of their time getting PAs approved.
Sather: We have 3 offices. For sur-gical procedures, each office handles its own PAs. For a new product such as Provenge, I became personally in-volved with all requests at first, be-cause the payers were requesting a lot of information and it made sense to have a single point of contact.
Earl Walz: For Provenge, we also centralized the process into the cor-porate office. When you start talking about PAs, you need to distinguish between more sophisticated medi-cations and the usual OAB [overac-tive bladder] drugs, BPH [benign prostate hyperplasia] drugs, and ED
[erectile dysfunction] drugs. These more common medications have more routine patient requirements and the PAs are done in our satel-lite offices.
Kirsh: What about consistency—are PAs relatively standard for different payers or do you need to provide 5 sets of data for 5 different payers?
Sather: We see different PA and medical necessity requirements for different payers.
Kirsh: It’s all over the board?
Sather: Yes
Hille: I agree with that.
Deepak Kapoor: In addition, the requirements are different for Medi-care patients.
Kirsh: Thank you for providing those insights. Clearly this is an impor-tant issue for urology practices. l
Panel Discussion
SECOND ANNUAL CONFERENCE
GLOBAL BIOMARKERS CONSORTIUM™
Clinical Approaches to Targeted Technologies™
October 4-6, 2013 • The Seaport Boston Hotel • 1 Seaport Lane • Boston, MA 02210
REGISTER TODAY AT www.globalbiomarkersconsortium.com
GBC_2013Conf_horizontalV291312_Layout 1 9/13/12 12:22 PM Page 1

YOUR COMPLIMENTARY SUBSCRIPTION IS ONLY A CLICK AWAY
Receive timely information on the latest developments in urology practice management to assist you in your daily roles and responsibilities. Sign up now for Urology Practice Management.
Establishing a patient-centered approach is rapidly becoming a core requirement in US medical prac-
tices. Medical home models, account-able care organization (ACO) models,
and Health Information Technology for Economic and Clinical Health (HITECH) requirements all have com-ponents of engaging patients in their care. To incorporate a patient-centered
On October 1, 2014, the UnitedStates will adopt the International Classifi cation of Disease, Tenth
Revision, Clinical Modifi cation/Procedure Cod-ing Sys tem (ICD-10-CM/PCS), 1 year later than we had initially reported in Urology Practice Management in September 2012. The reprieve, although welcome to many,
is less than 17 months away, during which several phases of implementation must be completed. The timeline for implement-ing the code sets is divided into 4 phases: Phase 1: Impact Assessment, fi rst quarter 2009 through second quarter 2012; Phase 2: Preparing for Implementation, fi rst quarter 2012 through second quarter 2014; Phase 3:
©2013 Engage Healthcare Communications, LLC
www.UroPracticeManagement.com
Urology PracticeManagement™
MAY 2013 VOLUME 2 • NUMBER 1
PROCESS IMPROVEMENTS TO ENHANCE PATIENT CARE™
Continued on page 10
Continued on page 8Continued on page 19
Exploring Men’s Willingness to Pay for Prostate Cancer Screening to Avoid Unnecessary Biopsys and Treatment By Rosemary Frei, MSc
Transitioning to ICD-10 By Susanne Talebian, CHBC, RMM, CMOM, CPC-I, CPC, CUA, CCS-P, PCSCertifi ed Healthcare Business Consultant, American Health Information Management Association—AHIMA Certifi ed ICD-10-CM/PCS Trainer
Implementing a Patient Portal in Your Urology Practice to Provide Patient-Centered CareBy Gena CookFounder and Chief Executive Offi cer Navigating Cancer, a leading provider of oncology-specifi c patient portals
Dutch researchers have peered into the minds and wallets of a group of men aged 55 to 75
years to determine what they are willing to trade for a reduced risk of prostate cancer–related death or to avoid unnec-essary procedures and treatment.
Men with more education had a lower probability of opting for prostate cancer screening. Furthermore, the men were willing to lose 2% of risk reduction in mortality related to prostate cancer, or to pay, on average, €188 (in 2010 euros—equivalent to $245 in 2010 US dollars) annually, for a 10% reduced risk of unnecessary biopsy or treatment.
“Physicians should be aware that men,
PROST
ATE H
EALTH
Prosta
te C
ancer
O
vervi
ew...16
SIGN UP TODAY!To sign up, visit www.UroPracticeManagement.com
UPM_42513
Urology PracticeManagement™
PROCESS IMPROVEMENTS TO ENHANCE PATIENT CARE™
Urology PracticeManagement™
PROCESS IMPROVEMENTS TO ENHANCE PATIENT CARE™
E stablishing a patieapproach is rreq
O n October 1, 2014, the United
States will adopt the International
Classifi cation of Disease, Tenth
Revision, Clinical Modifi cation/Procedure Cod-
ing Sys tem (ICD-10-CM/PCS), 1 year later
than we had initially reported in Urology
Practice Management in September 2012.
The reprieve, although welcome to many,
is less than 17 months away, during which
several phases of implementation must be
completed. The timeline for implement-
ing the code sets is divided into 4 phases:
Phase 1: Impact Assessment, fi rst quarter
2009 through second quarter 2012; Phase 2:
Preparing for Implementation, fi rst quarter
2012 through second quarter 2014; Phase 3:
www.UroPracticeManagement.com
Urology PracticeManagement ™
MAY 2013
VOLUME 2 • NUMBER 1
PROCESS IMPROVEMENTS TO ENHANCE PATIENT CARE™
Continued on page 10
Contin
Exploring Men’s Willingness to Pay
for Prostate Cancer Screening to Avoid
Unnecessary Biopsys and Treatment
By Rosemary Frei, MSc
Transitioning to ICD-10
By Susanne Talebian, CHBC, RMM, CMOM, CPC-I, CPC, CUA, CCS-P, PCS
Certifi ed Healthcare Business Consultant, American Health Information
Management Association—AHIMA Certifi ed ICD-10-CM/PCS Trainer
Implementing a Patient Portal in
Your Urology Practice to Provide
Patient-Centered Care
By Gena CookFounder and Chief Executive Offi cer Navigating Ca
of oncology-specifi c patient portals
D utch researchers have peered
into the minds and wallets of
a group of men aged 55 to 75
years to determine what they are willing
to trade for a reduced risk of prostate
cancer–related death or to avoid unnec-
essary procedures and treatment.
Men with more education had a lower
probability of opting for prostate cancer
screening. Furthermore, the men were
willing to lose 2% of risk reduction in
mortality related to prostate cancer,
or to pay, on average, €188 (in 2010
euros—equivalent to $245 in 2010 US
dollars) annually, for a 10% reduced risk
of unnecessary biopsy or treatment.
“Physicians should be aware that men
UPM house ad pgs_2013_Layout 1 4/25/13 11:59 AM Page 2