efficacy and safety of pioglitazone in type 2 diabetes...
TRANSCRIPT

28
ORIGINAL ARTICLE
Acta Medica Indonesiana - The Indonesian Journal of Internal Medicine
Efficacy and Safety of Pioglitazone in Type 2 Diabetes Mellitus: a Postmarketing Observational Study
Nafrialdi1,21 Department of Pharmacology, Faculty of Medicine, Universitas Indonesia. Jl. Salemba Raya 6, Jakarta, Indonesia. 2 Clinical Study Unit, Faculty of Medicine, University of Indonesia - dr. Cipto Mangunkusumo Hospital, Jakarta,
Indonesia. Correspondence mail: [email protected].
ABSTRAKTujuan: menilai efektivitas dan keamanan pioglitazon pada populasi Indonesia penyandang diabetes
tipe 2. Metode: penelitian dilakukan mulai September 2009 sampai Desember 2010 di 23 kota di Indonesia. Penyandang DM tipe 2 yang belum diobati atau yang telah mendapat antidiabetik oral dengan gula darah yang belum terkontrol diberi pioglitazon 15 atau 30 mg/hari selama 12 minggu. Gula darah puasa (GDP) dan 2 jam posprandial (GDPP) diambil sebagai parameter efektivitas dan dinilai setiap 4 minggu. Berat badan (BB) dan indeks masa tubuh (IMT) sebagai parameter keamanan dinilai setiap 4 minggu dan GPT diukur pada awal dan akhir penelitian. Data dianalisis dengan uji Wilcoxon. Hasil: penelitian melibatkan 190 passion (92 pria dan 98 wanita) berusia 56,3 (28-80) tahun. Rerata GDP menurun dari 191,8 mg/dL (baseline) menjadi 155,9; 141,0; dan 127,3 mg/dL, pada minggu 4, 8, dan 12 (p<0,001). Rerata GDPP menurun dari 267,3 mg/dL (baseline) menjadi 209,7; 188,2; and 174,9 pada minggu 4, 8, dan 12 (p<0,001). BB sedikit meningkat (tapi statistik bermakna) dari 67,3 (40-98) kg (baseline) menjadi 67,7 (42,0-98,5) dan 67,8 (43,0-99,0) kg pada minggu 8 dan 12 (p<0.001) dan IMT dari 25,6 (16,2-38,6) kg/m2 (baseline) menjadi 25,7 (17,0-36,3) dan 25,7 (17,4-36,6) kg/m2 pada minggu 8 dan 12 (p<0,001). SGPT tidak berubah secara bermakna (35,6 U/L menjadi 35,5 U/L, p=0,93). Kesimpulan: pioglitazon efektif dalam mengendalikan gull darah tanpa efek sampling pada fungsi hati, namun terjadi sedikit peningkatan berat badan, yang mengisyaratkan kehati-hatian dalam menggunakan pioglitazon pada pasien dengan gagal jantung atau kondisi retensi cairan lainnya.
Kata kunci: diabetes melitus, pioglitazone, thiazolidinedione, retensi cairan, toksisitas pada hati.
ABSTRACTAim: to assess the effectiveness and safety profile of pioglitazone in Indonesian type 2 diabetic patients.
Methods: type 2 diabetic patients, naive or under oral antidiabetics, with uncontrolled fasting (FBG) or postprandial blood glucose (PPBG) were enrolled from September 2009 to December 2010 from 23 cities in Indonesia. Pioglitazone (Actos®) 15 mg or 30 mg daily was prescribed by the physician and performed observation for 12 weeks. Body weight (BW), body mass index (BMI), FBG and PPBG were measured every 4 weeks and serum transaminase (SGPT) was measured at the beginning and at the end of the study. Changes from baseline to each visit were analyzed using Wilcoxon-test. Results: 190 patients (92 male and 98 female) aged 56.3 (28-80) years were included. Mean FBG decreased from 191.8 mg/dL at baseline to 155.9; 141.0; and 127.3 mg/dL, at week 4, 8, and 12, respectively (p<0.001). Mean PPBG decreased from 267.3 mg/dL at baseline to 209.7; 188.2; and 174.9 at week 4, 8, and 12, respectively (p<0.001). BW slightly increased from 67.3 (range: 40-98) kg at baseline to 67.7 (42.0-98.5) and 67.8 (43.0-99.0) kg at weeks 8 and 12, respectively (p<0.001) and BMI increased from 25.6 (16.2-38.6) kg/m2 at baseline to 25.7 (17.0-36.3) and 25.7 (17.4-36.6) kg/m2 at weeks 8 and 12, respectively (p<0.001). SGPT values were not significantly changed (35.6U/L at baseline and 35.5U/L at week 12, p=0.93). Conclusion: Pioglitazone is effective in controlling blood glucose, without harmful effect

Vol 44 • Number 1 • January 2012 Efficacy and Safety of Pioglitazone in Type 2 Diabetes Mellitus
29
INTRODUCTION
Type 2 diabetes mellitus is a chronic illness with progressivity leading to micro- and macrovascular complications and constitutes a major risk factor for numerous other diseases. Pathophysiology of DM is related with development of insulin resistance in target tissues, increased hepatic glucose production, and ultimately failure of insulin secretion by pancreatic beta cell. These pathologies lead to hyperglycemia and hyperinsulinism. Within this last decade, various drugs have been marketed with excellent efficacy in controlling blood glucose levels, reducing the progress of complications, and in decreasing morbidity and mortality of DM.
Thiazolidinediones (TZD) are a group of drugs known as insulin-sensitisers,indicated for improving glycemic control in diabetic patients, as a single agent or in combination with other medications. It works by activating the peroxisome proliferators activated receptor-g (PPAR-g),which facilitates and strengthens intracellular signaling cascade after binding of insulin to its receptor.1 Some literature indicates that thiazolidinediones increase the expression of insulin receptor in fat tissue and hepatocytes, but seems to have minor contribution in skeletal muscle. Improvement of pancreatic beta cells has led this drug to be used for prevention of DM.2,3 In addition, activation of PPAR-g receptors have beneficial effects on vascular endothelial cells4,5 suggesting that this drug would be good for diabetic patients with cardiovascular disease. However, the use of thiazolidinediones is associated with water retention which can be harmful to patients with heart failure.6
The first drug in TZD group, troglitazone, has been withdrawn from the market due to liver toxicity,7 and followed by withdrawal of rosiglitazone several years later due to cardiovascular side effects.8
Pioglitazone is another member of TZD which has been approved by National Agency of Drug and Food Control of Indonesia since 2001
and still in use until nowadays. By restricting its indication for type 2 diabetic patients without heart failure, until now no study has been reporting on the increase of cardiovascular events in patients taking pioglitazone. Regarding liver toxicity,inconsistent results of increased transaminases have been reported.6,9
This postmarketing study represents the first one to evaluate the efficacy and safety of pioglitazone (Actos®) in Indonesian population with type2 diabetes mellitus.
METHODSThis is a multicenter postmarketing
observational study conducted on type 2 diabetic patients in 23 cities in Indonesia, involving about 50 private clinics from September 2009 to December 2010. The study protocol was approved by the Ethics Committee of the Faculty of Medicine, University of Indonesia.
Inclusion criteria were male or female diabetic patients aged 18 years or above. Treatment-Naive patients with fasting blood glucose (FBG) of >126 mg/dL or 2-hour postprandial blood glucose (PPBG) of >200 mg/dL, or patients under oral antidiabetic drug (OAD) with uncontrolled blood glucose (FBG of >100 mg/dL, and/or PPBG of >145 mg/dL),were recruited. Written informed consent was obtained from each patient before entering the study. Pioglitazone (Actos®) 15 mg or 30 mg once daily was prescribed by the physician, and we performed the observation for 12 weeks.
Those with the following criteria are excluded: history of hypersensitivity to thiazolidinedione, history or current heart failure (NYHA class I-IV), liver dysfunction with serum glutamic pyruvic transaminase (SGPT) of >2.5 upper normal level, renal dysfunction with serum creatinine of >2 mg/dL, pregnancy or breast feeding woman, taking diabetic drugs other than metformin or sulphonylurea, and other conditions which, according to the opinion of the treating physician, will affect safety and efficacy evaluation.
on the liver. However, there was a slight but statistically significant increase in body weight, that mandates the precaution when using this drug in patients with heart failure or other conditions with water retention.
Key words: diabetes mellitus, pioglitazone, thiazolidinedione, water retention, liver toxicity.
Nafrialdi Acta Med Indones-Indones J Intern Med
30
FBG and PPBG were measured every 4 weeks for a period of 12 weeks as parameters of efficacy, and body weight (BW in kg) as well as body mass index (BMI in kg/m2) were taken as safety parameters. In addition, SGPT was measured before and after 12 weeks of pioglitazone treatment. Concomitant drugs previously taken by the patients can be continued and noted in the case report form. Every patients is given the option to continue or withdraw his/her participation in the study.
Data AnalysisData of fasting and postprandial blood
glucose at baseline and after 12 weeks of treatment were compared by paired t-test or Wilcoxon test as appropriate. Weekly variation of blood glucose was analyzed by using ANOVA repeated measures or by Friedman test as appropriate. P value of <0.05 was considered statistically significant.
RESULTS
In the present study, 190 patients aged from 28 to 80 years have been recruited consisting of 92 males (48.4%) and 98 females (51.6%). Among them,181 patients (95.26%) completed the study, while 9 patients (4.7%) dropped out (1 patient due to side effect, 1 patient moved to another city, and 7 patients were lost to follow up).
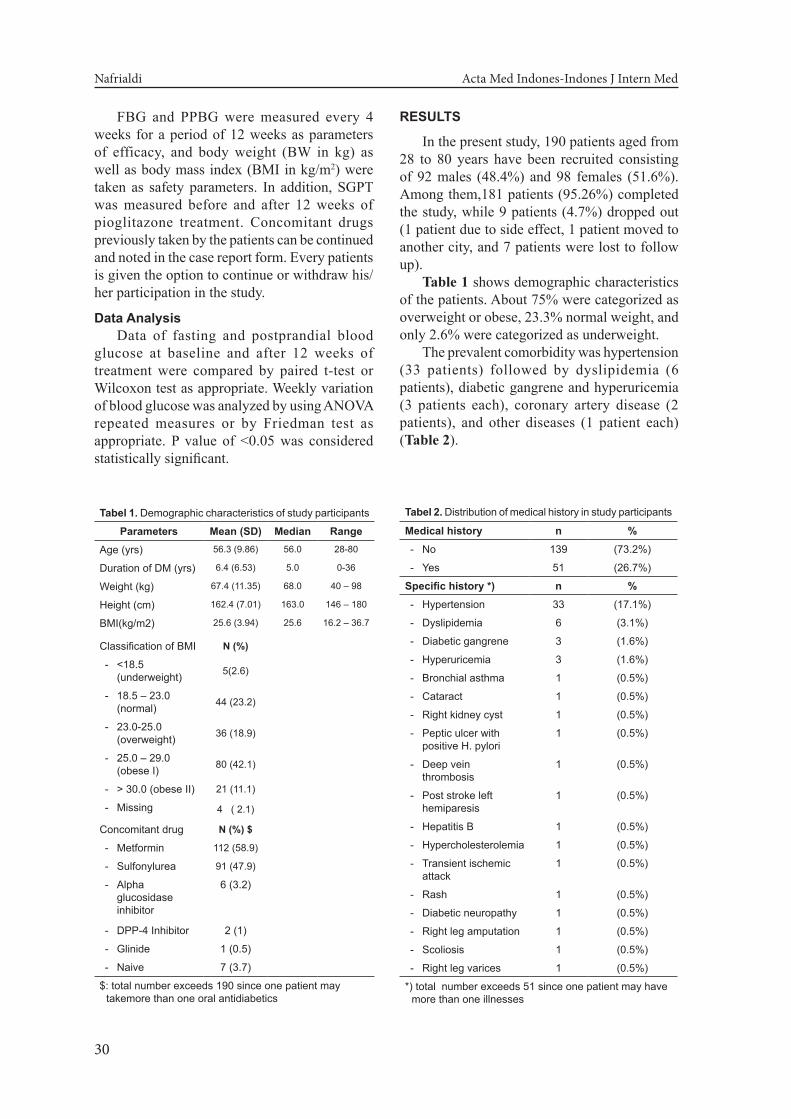
Table 1 shows demographic characteristics of the patients. About 75% were categorized as overweight or obese, 23.3% normal weight, and only 2.6% were categorized as underweight.
The prevalent comorbidity was hypertension (33 patients) followed by dyslipidemia (6 patients), diabetic gangrene and hyperuricemia (3 patients each), coronary artery disease (2 patients), and other diseases (1 patient each) (Table 2).
Tabel 1. Demographic characteristics of study participants
Parameters Mean (SD) Median RangeAge (yrs) 56.3 (9.86) 56.0 28-80
Duration of DM (yrs) 6.4 (6.53) 5.0 0-36
Weight (kg) 67.4 (11.35) 68.0 40 – 98
Height (cm) 162.4 (7.01) 163.0 146 – 180
BMI(kg/m2) 25.6 (3.94) 25.6 16.2 – 36.7
Classification of BMI N (%)
- <18.5 (underweight) 5(2.6)
- 18.5 – 23.0 (normal) 44 (23.2)
- 23.0-25.0 (overweight) 36 (18.9)
- 25.0 – 29.0 (obese I) 80 (42.1)
- > 30.0 (obese II) 21 (11.1)
- Missing 4 ( 2.1)
Concomitant drug N (%) $
- Metformin 112 (58.9)
- Sulfonylurea 91 (47.9)
- Alpha glucosidase inhibitor
6 (3.2)
- DPP-4 Inhibitor 2 (1)
- Glinide 1 (0.5)
- Naive 7 (3.7)
$: total number exceeds 190 since one patient may takemore than one oral antidiabetics
Tabel 2. Distribution of medical history in study participants
Medical history n % - No 139 (73.2%)
- Yes 51 (26.7%)
Specific history *) n % - Hypertension 33 (17.1%)
- Dyslipidemia 6 (3.1%)
- Diabetic gangrene 3 (1.6%)
- Hyperuricemia 3 (1.6%)
- Bronchial asthma 1 (0.5%)
- Cataract 1 (0.5%)
- Right kidney cyst 1 (0.5%)
- Peptic ulcer with positive H. pylori
1 (0.5%)
- Deep vein thrombosis
1 (0.5%)
- Post stroke left hemiparesis
1 (0.5%)
- Hepatitis B 1 (0.5%)
- Hypercholesterolemia 1 (0.5%)
- Transient ischemic attack
1 (0.5%)
- Rash 1 (0.5%)
- Diabetic neuropathy 1 (0.5%)
- Right leg amputation 1 (0.5%)
- Scoliosis 1 (0.5%)
- Right leg varices 1 (0.5%)
*) total number exceeds 51 since one patient may have more than one illnesses
Vol 44 • Number 1 • January 2012 Efficacy and Safety of Pioglitazone in Type 2 Diabetes Mellitus
31
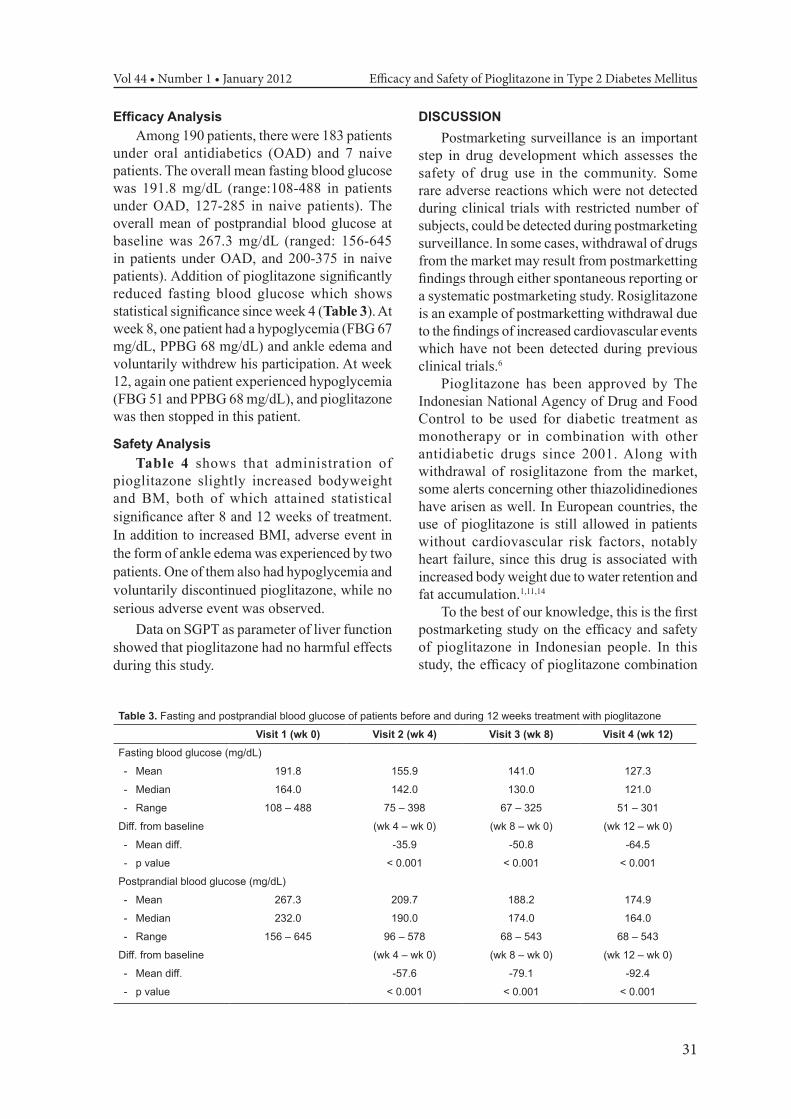
Efficacy AnalysisAmong 190 patients, there were 183 patients
under oral antidiabetics (OAD) and 7 naive patients. The overall mean fasting blood glucose was 191.8 mg/dL (range:108-488 in patients under OAD, 127-285 in naive patients). The overall mean of postprandial blood glucose at baseline was 267.3 mg/dL (ranged: 156-645 in patients under OAD, and 200-375 in naive patients). Addition of pioglitazone significantly reduced fasting blood glucose which shows statistical significance since week 4 (Table 3). At week 8, one patient had a hypoglycemia (FBG 67 mg/dL, PPBG 68 mg/dL) and ankle edema and voluntarily withdrew his participation. At week 12, again one patient experienced hypoglycemia (FBG 51 and PPBG 68 mg/dL), and pioglitazone was then stopped in this patient.
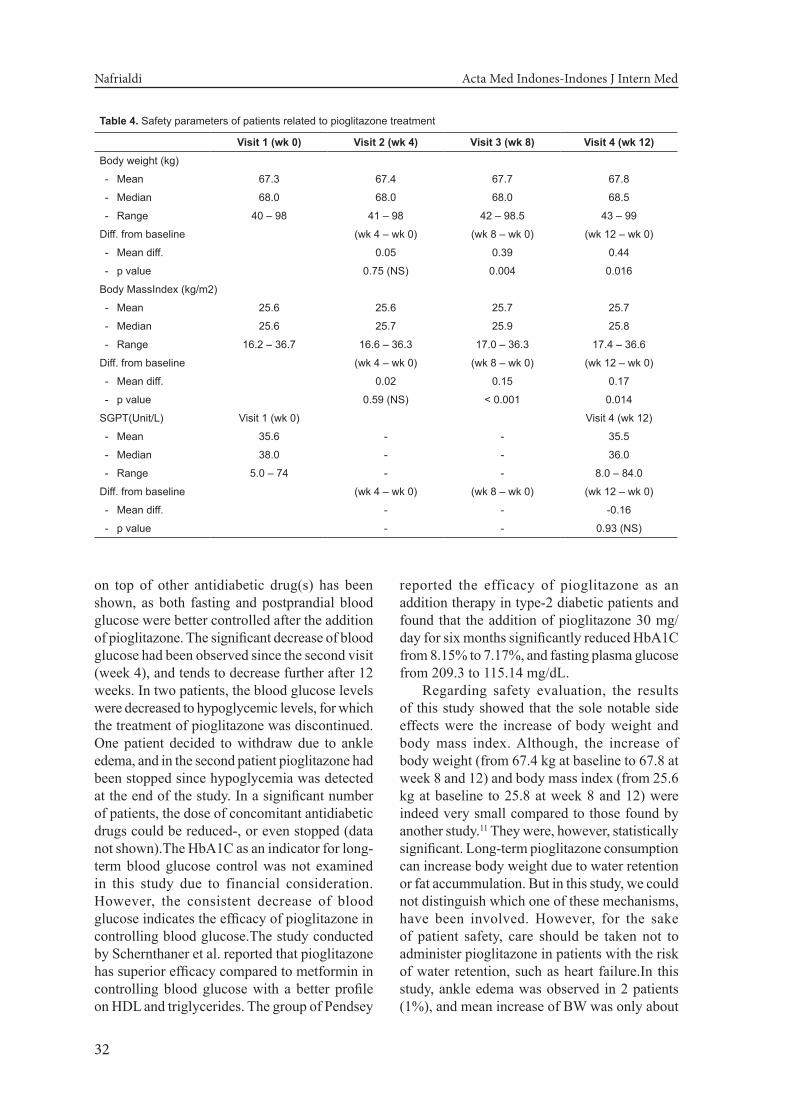
Safety AnalysisTable 4 shows that administration of
pioglitazone slightly increased bodyweight and BM, both of which attained statistical significance after 8 and 12 weeks of treatment. In addition to increased BMI, adverse event in the form of ankle edema was experienced by two patients. One of them also had hypoglycemia and voluntarily discontinued pioglitazone, while no serious adverse event was observed.
Data on SGPT as parameter of liver function showed that pioglitazone had no harmful effects during this study.
DISCUSSIONPostmarketing surveillance is an important
step in drug development which assesses the safety of drug use in the community. Some rare adverse reactions which were not detected during clinical trials with restricted number of subjects, could be detected during postmarketing surveillance. In some cases, withdrawal of drugs from the market may result from postmarketting findings through either spontaneous reporting or a systematic postmarketing study. Rosiglitazone is an example of postmarketting withdrawal due to the findings of increased cardiovascular events which have not been detected during previous clinical trials.6
Pioglitazone has been approved by The Indonesian National Agency of Drug and Food Control to be used for diabetic treatment as monotherapy or in combination with other antidiabetic drugs since 2001. Along with withdrawal of rosiglitazone from the market, some alerts concerning other thiazolidinediones have arisen as well. In European countries, the use of pioglitazone is still allowed in patients without cardiovascular risk factors, notably heart failure, since this drug is associated with increased body weight due to water retention and fat accumulation.1,11,14
To the best of our knowledge, this is the first postmarketing study on the efficacy and safety of pioglitazone in Indonesian people. In this study, the efficacy of pioglitazone combination
Table 3. Fasting and postprandial blood glucose of patients before and during 12 weeks treatment with pioglitazone
Visit 1 (wk 0) Visit 2 (wk 4) Visit 3 (wk 8) Visit 4 (wk 12)Fasting blood glucose (mg/dL)
- Mean 191.8 155.9 141.0 127.3
- Median 164.0 142.0 130.0 121.0
- Range 108 – 488 75 – 398 67 – 325 51 – 301
Diff. from baseline (wk 4 – wk 0) (wk 8 – wk 0) (wk 12 – wk 0)
- Mean diff. -35.9 -50.8 -64.5
- p value < 0.001 < 0.001 < 0.001
Postprandial blood glucose (mg/dL)
- Mean 267.3 209.7 188.2 174.9
- Median 232.0 190.0 174.0 164.0
- Range 156 – 645 96 – 578 68 – 543 68 – 543
Diff. from baseline (wk 4 – wk 0) (wk 8 – wk 0) (wk 12 – wk 0)
- Mean diff. -57.6 -79.1 -92.4
- p value < 0.001 < 0.001 < 0.001
Nafrialdi Acta Med Indones-Indones J Intern Med
32
on top of other antidiabetic drug(s) has been shown, as both fasting and postprandial blood glucose were better controlled after the addition of pioglitazone. The significant decrease of blood glucose had been observed since the second visit (week 4), and tends to decrease further after 12 weeks. In two patients, the blood glucose levels were decreased to hypoglycemic levels, for which the treatment of pioglitazone was discontinued. One patient decided to withdraw due to ankle edema, and in the second patient pioglitazone had been stopped since hypoglycemia was detected at the end of the study. In a significant number of patients, the dose of concomitant antidiabetic drugs could be reduced-, or even stopped (data not shown).The HbA1C as an indicator for long-term blood glucose control was not examined in this study due to financial consideration. However, the consistent decrease of blood glucose indicates the efficacy of pioglitazone in controlling blood glucose.The study conducted by Schernthaner et al. reported that pioglitazone has superior efficacy compared to metformin in controlling blood glucose with a better profile on HDL and triglycerides. The group of Pendsey
reported the efficacy of pioglitazone as an addition therapy in type-2 diabetic patients and found that the addition of pioglitazone 30 mg/day for six months significantly reduced HbA1C from 8.15% to 7.17%, and fasting plasma glucose from 209.3 to 115.14 mg/dL.
Regarding safety evaluation, the results of this study showed that the sole notable side effects were the increase of body weight and body mass index. Although, the increase of body weight (from 67.4 kg at baseline to 67.8 at week 8 and 12) and body mass index (from 25.6 kg at baseline to 25.8 at week 8 and 12) were indeed very small compared to those found by another study.11 They were, however, statistically significant. Long-term pioglitazone consumption can increase body weight due to water retention or fat accummulation. But in this study, we could not distinguish which one of these mechanisms, have been involved. However, for the sake of patient safety, care should be taken not to administer pioglitazone in patients with the risk of water retention, such as heart failure.In this study, ankle edema was observed in 2 patients (1%), and mean increase of BW was only about
Table 4. Safety parameters of patients related to pioglitazone treatment
Visit 1 (wk 0) Visit 2 (wk 4) Visit 3 (wk 8) Visit 4 (wk 12)Body weight (kg)
- Mean 67.3 67.4 67.7 67.8
- Median 68.0 68.0 68.0 68.5
- Range 40 – 98 41 – 98 42 – 98.5 43 – 99
Diff. from baseline (wk 4 – wk 0) (wk 8 – wk 0) (wk 12 – wk 0)
- Mean diff. 0.05 0.39 0.44
- p value 0.75 (NS) 0.004 0.016
Body MassIndex (kg/m2)
- Mean 25.6 25.6 25.7 25.7
- Median 25.6 25.7 25.9 25.8
- Range 16.2 – 36.7 16.6 – 36.3 17.0 – 36.3 17.4 – 36.6
Diff. from baseline (wk 4 – wk 0) (wk 8 – wk 0) (wk 12 – wk 0)
- Mean diff. 0.02 0.15 0.17
- p value 0.59 (NS) < 0.001 0.014
SGPT(Unit/L) Visit 1 (wk 0) Visit 4 (wk 12)
- Mean 35.6 - - 35.5
- Median 38.0 - - 36.0
- Range 5.0 – 74 - - 8.0 – 84.0
Diff. from baseline (wk 4 – wk 0) (wk 8 – wk 0) (wk 12 – wk 0)
- Mean diff. - - -0.16
- p value - - 0.93 (NS)

Vol 44 • Number 1 • January 2012 Efficacy and Safety of Pioglitazone in Type 2 Diabetes Mellitus
33
0.4 kg and increase of BMI was 0.15 kg/m2, while the study of Pendsey et al.11 reported the incidence of edema in 33.3%, with the mean increase in BW and BMI of 2.43 kg and 0.64 kg/m2, respectively in patients receiving pioglitazone. This difference was most likely due to the diffecrence in the duration of the study, in which they administered pioglitazone for six months.
It is interesting to note that even though TZD is known to cause fluid retention and concerns have arisen on the risks of cardiovascular events, some studies suggest the cardiovascular safety of pioglitazone. In accordance with laboratory studies which show that pioglitazone has antiinflammatory and antiateriosclerotic effects,12 an interesting study on 5000 patients receiving pioglitazone for a period of 2.5 years revealed a good safety profile of pioglitazone. The patients recruited had a well established cardiovascular risks in which almost 50% of patients had previous history of myocardial infarction, and 20% had a prior history of stroke. The results showed that patients treated with pioglitazone had a lower death rate, nonfatal myocardial infarction, stroke, leg amputation, and acute coronary syndrome.13 Other studies also reported that pioglitazone reduced vascular risk and inflammatory markers, and improved carotid intima media thickness independent of its glycemic effect. When compared with rosiglitazone, pioglitazone is associated with a reduction in the risk of hospitalization for acute myocardial infarction.14
Apart from body weight and body mass index, we also would like to evaluate the effect of pioglitazone on liver function.In this study, SGPT as a parameter of liver function was practically unchanged during the study (35.8 vs 35.1), indicating that pioglitazone is not harmful for the liver. A case report from May et al.9 depicted a rare adverse event in the form of mixed hepatocellular and cholestatic jaundice in one patient after taking pioglitazone for 6 months. Improvement of liver function after discontinuation of pioglitazone, indicated a strong causal association of this side efect. Other study by Belfort et al.15 even reported an improvement of liver function after administration of pioglitazone compared to placebo. In this study, fifty five patients with nonalcoholic steatohepatosis were treated with pioglitazone. Plasma aspartate aminotransferase (AST) levels
was reported to normalized in significantly higher number (40%)of pioglitazone group compared to placebo group (21%). Normalization of alanine aminotransferase (ALT) levels was observed in 58% vs. 34%,and decreased hepatic fat content was observed in 54% vs. 0%. Histologic findings with regard to steatosis, ballooning necrosis, and inflammation, were also reported to improve.
Our present study has some limitations including low subject numbers, the lack of control group, a relatively short period of observation (12 weeks),and lack of other safety parameters such as lipid profile. However, our findings concerning efficacy and safety parameters seem to be in accordance with other studies.
CONCLUSIONFrom the above results we may conclude that
pioglitazone has excellent efficacy in controlling blood glucose and has a good safety profile regarding liver function. However, there was a slight but statistically significant increase in body weight, that mandates the precaution when using this drug in patients with heart failure or other conditions with water retention.
ACKNOWLEDGEMENT We are grateful for the support of PT. Takeda
Indonesia for laboratory costs. The design of the study and data analysis were supported by the Clinical Study Unit, Faculty of Medicine, University of Indonesia. We also thank all physician that has participated in recruiting the patients and providing the data.
REFERENCES1. Hannele Yki-Järvinen. Thiazolidinediones. N Engl J
Med. 2004;351:1106-18.2. De Fronzo RA, Tripathy D, Schwenke DC, et al.
Pioglitazone for diabetes prevention in impaired glucose tolerance. N Engl J Med. 2011;364:1104-15.
3. De Fronzo RA, Banerji M, Bray GA, et al. Actos now for the prevention of diabetes (ACT NOW) study. BMC Endocr Disord. 2009;9:17.
4. Gastaldelli A, Ferrannini E, Miyazaki Y, Matsuda M, Mari A, DeFronzo RA. Thiazolidinediones improve beta-cell function in type 2 diabetic patients. Am J Physiol Endocrinol Metab. 2007;292:E871-83.
5. Gaillard V, Casellas D, Seguin-Devaux C, et al. Pioglitazone improves aortic wall elasticity in a rat model of elastocalcinotic arteriosclerosis. Hypertension. 2005;46:372-9.
6. Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardialinfarction and death from cardiovascular
Nafrialdi Acta Med Indones-Indones J Intern Med
34
causes. N Engl J Med. 2007;356:2457-71.7. Diabetes drug rosiglitazone withdrawn over heartfears.
http://besthealth.bmj.com/x/news/541024/news-item.html.
8. Center for Drug Evaulation and Research. Approval package: Avandia (rosiglitazonemaleate) tablets. Company: SmithKline Beecham Pharmaceuticals. Application no. 21-071. Approval date: 5/25/1999. Available at http://www.fda.gov/cder/foi/nda/99/21071_Avandia.htm . Accessed December 28, 2011.
9. May LD, Lefkowitch JH, Kram MT, Rubin DE. Mixed hepatocellular–cholestatic liver injury after pioglitazone therapy. Annal Intern Med. 2002;19(136):449-52.
10. Schernthaner G, Matthews DR, Charbonnel B, Hanefeld M, Brunetti P; Quartet [corrected] study group. Efficacy and safety of pioglitazone versus metformin in patients with type 2 diabetes mellitus: a double-blind, randomized trial. J Clin Endocrinol Metab. 2004;89(12):6068-76. Avaialble at www.ncbi.nlm.nih.gov/pubmed/15579760. Accessed January 3, 2012.
11. Pendsey SP, Dhanvijay VP, Joshi PP. Efficacy of pioglitazone as an add on drug with insulin, glibenclamide and metformin in patients with uncontrolled type 2 diabetes mellitus. Diabetologia Croatia 2002;31:51-7. Available at: www.idb.hr/diabetologia/o2no1-3. Accessed January 3, 2012.
12. Ishibashi M, Egashira K, Hiasa K, et al. Antiinflammatory and antiarteriosclerotic effects of pioglitazone. Hypertension. 2002;40:687-93.
13. Dormandy JA, Charbonnel B, Eckland DJA, et al. PRO active investigators. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitazone clinical trial in macro vascular events): a randomised controlled trial. Lancet. 2005;366:1279-89.
14. Derosa, Giuseppe. Efficacy and tolerability of pioglitazone in patients with type 2 diabetes mellitus: Comparison with other oral antihyperglycaemic agents. Drugs. 2010;70:1945-61.
15. Belfort R, Harrison SA, Brown K, et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Eng J Med. 2006;355: 2297-307.