effects of chronic ramipril treatment in …
TRANSCRIPT

Indian J Physiol Pharmacol 1997; 41(4); 353-360
EFFECTS OF CHRONIC RAMIPRIL TREATMENT INSTREPTOZOTOCIN-INDUCED DIABETIC RATS
ZEENAT S. HAKIM, BHAGIRATH K. PATELAND RAMESH K. GOYAL*
Department of Pharmacology,L. M. College of Pharmacy,Ahmedabad - 380 009
( Received on September 22, 1996)
Abstract; The present investigation was undertaken to study the effectsof chronic oral ramipril (1 mglkg) trentment in strepto'Zotocin (STZ) induceddiabetic rats. Single tail vein injection of STZ (45 mglkg, i. v.) produced adiabetic state exhibiting all the cardinal symptoms such as loss of bodyweight, polydipsia, polyuria, glucosuria, polyphagia, hypoinsulinaemia andhyperglycaemia. The diabetic state was also found to be associated withbradycardia, hypothyroidism, cardiac depression and cardiomyopathy.Ramipril treatment prevented STZ-induced hypertension, bradycardia,hypothyroidism, hyperchosestcrolacmia and partially the cardiomayopathy.Ramipril treatment could not, however prevent STZ-induced loss of bodyweight, polyuria, polydipsia, polyphagia, hyperglycaemia, hypoinsulinaemia,hypertriglyceridaemia and cardiac depression. Our data suggests thatramipril has a few beneficial effects in the STZ-treated diabetic rats.
Key words: diabetes mellitus rnmipril strepto'Zotocin
INTRODUCTION
Hypertension is reported to be morcprevalent among diabetics than non-diabeticsubjects, and it is reported to aggravate thecardiovascular complications of diabetes (1,
2). Both hypertension and diabetes mellitusare multifaceted and dynamic expressionsof pathological disequlibria which are closelyrelated and even intermingled by commonfactOrS such as obesity, hyperinsulinaemia,micro-and macrovasulcar disease andcardiac risk factors (3).
Our laboratory is engaged in the studyof various antihypertensives on STZinduced diabetic rats. It has been reported
-Corresponding Author
that cardioselective beta-blocker atenolol,does not improve cardiac dysunfction,cardiomyopathy and other complications (4),whereas, prazosin improves cardiacdysfunction but not cardiomyopathy andhyperlipidaemia (4). Chronic nifedipinetreatment prevents STZ-inducedcardiomyopathy, hypertension, hyperlipidacmia and hypothyroidism (5). Further,Lakkad et al (6) reported that angiotensinconverting enzyme inhibitor (ACE!)enalapril prevents STZ-induccdcardiomyopathy, cardiac dysfunction andhypcrcholesterolaemia in rats. Studies withramipril suggest that it produces a reversalof left ventricular hypertrophy inhypertensive patients without any
354 Hakim et al
deterioration of pump function (7). Animalstudies have shown that ramipril improvesmyocardial metabolism, reduces myocardialnecrosis and reperfusion-inducedarryhthmias in experimental myocardialischaemia reperfijsion studies (8). ACEinhibitors are being used more and morefor the treatment of hypertension as theydo not interfere with glucose tolerance indiabetic state (9) and blood lipid profile inhypertensives with or without diabetes (10,11). They are also reported to reduce cardiacinvolvement in hypertension to induceremodelling of hypertrophied heart (12) andto improve work capacity and life expectancyin patients with severe heart failure (8).This could be particularly useful for longterm hypertensive diabetics who have ahigher incidence and greater morbidity andmortality from cardiac diseases. Sinceprevious studies with ACEI enalapril wereencouraging, the present investigation wasundertaken to study the effects of chronictreatment with ramipril in BTZ-induceddiabetes in rats.
METHODS
Induction of diabetes and drugtreatment: Female albino rats of Wi starstrain, weighing 200-230 g, were madediabetic by STZ (45 mg/kg, Lv.) dissolved incitrate buffer (pH 4.5). Control rats wereinjected with citrate buffer. Urine glucoselevels were measured using Glucostix 48hours after the injection and animalsshowing glucosuria (>2%) were consideredas diabetic. Both control and diabeticanimals were randomly divided intosubgroups--untreated and treated. Ramipril(l mglkg) was given daily by oral route forsix weeks. During the six weeks treatment
Indian J Physiol Pharmacal 1997; 41(4)
period, the animals were maintained onstandard rat chow and water ad libitum andthey were observed carefully for changes inwater intake, food intake, body weight,general behavior and mortality.
Blood sample collection and analysis: Atthe end of six weeks blood samples werecollected from the retro-orbital plexus ofrats. The serum was separated bycentrifugation of the whole blood at 3000rpm for 15 min. Serum glUCOse, cholesterol,triglyceride, HDL cholesterol levels weremeasured spectrophotometrically byenzymatic method using their respectivekits. Serum immunoreactive insulin wasassayed by the radioimmunoassay methodusing the kit from Monobind Costa Mesa,USA. Serum Ta and T
4were estimated by
Solid Phase Competitive Binding EnzymeImmunoassay method using the kit fromMiles India Ltd.
Measurement of blood pressure, heartrale, and cardiac functions: Blood pressureand heart rate of all the experimentalanimals were recorded before and at the endof the six week treatment using the HarvardBP Monitor. The LVDP was measured usingNeely's working heart mode. The animalwas stunned and the heart was dissectedout and mounted. The heart was perfusedwith Chenoweth-Koelle solution (pH 7.4)and aerated with carbogen at temperature37°C. The isolated heart was allowed tostabilize for 10 minutes at the perfusionpressure of 10 cm H'l0. The LVDP was thenrecorded at different atrial filling pressures(5 cm H
20 to 25 cm H
20). The atrial
pressure was changed 2.5 cm H20 each timein a stepwise manner by changing theheight of the constant level reservoir.

Indian J Physiol Pharmacol 1997; 41(4)
Histological study of organ tissue: At theend of the treatment period the heart ofeach animal was dissected out and fixed inBouin's fixative. After dehydration of thetissue, paraffin blocks were made andmicrotomy carried out. Perefectly stainedsections were observed under a lightmicroscope.
Statistical analysis: Statistical analysiswas performed using Analysis of Variancefollwed by Tukey's Test (13). Alpha level of5% was taken as the level of statisticalsignificance.
RESULTS
General features: Injection of STZ to ratsresulted in a diabetic state with an elevated
Ramipril in Diabetes-Mellitus 355
urine glucose level (>2%) throughout thestudy period. No detectable glucose waspresent in the urine of control animals.Diabetic rats showed a significant reductionin body weight, polydipsia, polyphagia(Table I), hypertension and bradycardia(Table II). Ramipril did not alter any ofthese parameters except the blood pressure,which was lowered significantly in diabetictreated rats. Diabetic rats exhibited reducedheart weight. However, the ratio of heartweight to body weight was not significantlydifferent in all the groups (Table II).
Cardiac functions: The blood pressureof diabetic rats (148.33 ± 3.46) wassignificantly higher than that of the controlanimals (120.5 ± 5.85). Ramiprit lowered theblood pressure (I15 ± 2.35) in the diabetic
TABLE I: Changes in the general conditions and mortality with ramipril treatment.
20 % 2
220 %3.0635 % 2
Control(n=7)
Body weight (g)
Wllter intake(mVday/ral)~'ood intake(g/dlly/rllt>
Mortality 0.00%
COlltrol DiabetIctreated with Diabetic treated with
Ramipril (n=5) Ramipril(n=7) (n=6)
218.75 %3.75 156.66 %4.51* 160 %3.33-
43 %2 57 %4- 68 %2*
20 % I 35 %9* 35:t1*
0.00% 13% 13%
-Significantly different from control (P<0.05)
TABLE 11 fnOuence of ramipril treatment on blood pressure and heart rate.
COil trot Diabe/icControl treated with Diabetic treated with
(n=7) Ramipril (0=5) Ramiprit(n=7) (n:6)
Blood pressure 120.5 %5.85 118.12 ±2.78 148.33 :i: 3.46- 115 ± 2.35*-(0101 Hg)
Heart rate 334.5 %5.16 348%3.8 311.66 %3.66* 340%6.1*-(beatlllmin)
Wet heart 4.08%0.1 4.67 %0.46 3.65 :t 0.5* 3.8 %0.2*Wl.Ibody wt.(mg/g)
*Significantly different from control (P<0.05)--Significantly different from diabetic control (P<0.05)

356 Hakim et al Indian J Physiol Pharmacol 1997; 41(4)
group (Table II). The heart rate of thediabetic rats (311.66 ± 3.6) was significantlylower when compared to that of the controlrats (334.5 ± 5.16). Ramipril prevented STZinduced bradycardia (Table II).
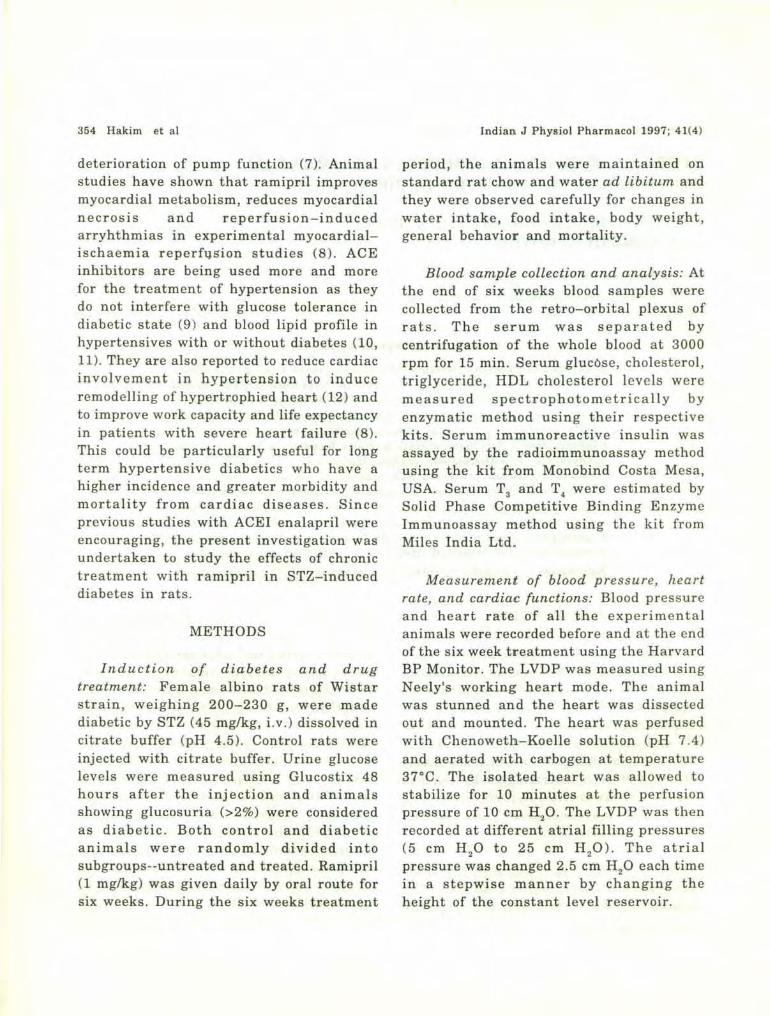
Increase in left atrial filling pressureproduced a gradual increase in LVDP andthis was significantly lower in STZ-treatedrats (Fig.D. Ramipril treatment of thediabetic rats did not alter the LVDP at anyof the filling pressures (Fig. 1).
Fig. 1: Effects of streptozotocin diabetes and ramipriltreatment on Left Ventricular DevelopedPressure on rat heart. (a) indicates control:( 0 ldepicts control ramipril treated: (.)represents diabetic control; (.) indicatesdiabetic treated with ramipril. Each point andthe bar represents mean ± SEM of 5-7experiments.
Biochemical parameters: Hyperglycemiaand hypoinsulinaemia were observed indiabetic rats (Table III). These remainedunaltered after ramipril treatment. Serumcholesterol and triglyceride levels werefound to be significantly high in diabeticrats (Table III). In addition, a significantdecrease in T 3 levels was also seen indiabetic rats. The six-weeks ramipriltreatment did not alter STZ-inducedhypertrigIyceridaemia. However, it produceda significant decrease in the serumcholesterol, LDL cholesterol and levels andalso increased the serum T
3levels thereby
improving hypothyroidism.
Effects on myocardium: The single tailvein injection of STZ caused distortion ofmyocaridial fibres. The nuclei wereclustered, intercalations disrupted and
<>-0_o---oClll<lOOl_-.rI~--...-... ~_,I11U")
•
•
•
•
,.,.
TABLI': III Effect of ramipril treatment on various biochemical parameters.
Control DiabelicControl treated with Diabetic treated luith
(n=7) Ramipril (n=5) Ramipril(n=7) (n=6)
Glucose (mg/dll 84.12:t2.70 84.79:t 7.67 520.88 :t 3.92* 528.20 :t 8.56*
Insulin (uU/ml) 41.2:t6.9 22.12:t 0.26· 15.38:t 1.77- 15 :t 4.36-
T, (ng/ml) 1.58:t 0.19 L92:t 0.38· 0.64 :t 0.07· 1.2:t 0.01'"
Cholesterol (mg/dl) 83.67:t5.01 49.05:t 4.54· 129.86:t 5.71- 64.40 :t 2.2**
Triglycerides (mg/dl) 78.72:t1.31 79.55:t 1.72 153.21 :t 3- 155.19 ± 2.68·
LDL (mg/dll 37.88:tl.30 3.96:t 1.21 70.39 :t 2.95· 48.8:t 1.35**
*Significantly different from control (PeO.OS)**Significantly different from diabetic control (PeO.05)

Indian J Physiol Pharmacol 1997; 41(4) Ramipril in Diabetes-Mellitus 357
Junod et al (14) reported thatdiabetogenic effects of STZ are dosedependent, ranging from a mild diabetesfollowing a dose of 35 mg/kg to a severeketotic state, leading to death within 2-3days after a dose of 100 mg/kg. Whentreated with intermediate doses of STZ (55and 65 mg/kg), rats fail to gain weight anddevelop blood glucose levels 3-4 timeshigher than normal, survive without insulinsupplementation do not develop ketosis. Inthe present investigation a single tail veininjection of 45 mg/kg STZ was used toinduce diabetes. At this dose, rats showedcharacteristic symptoms of diabetes mellituslike polydipsia, polyuria, polyphagia, weightloss, and glucosuria. Hofteizer andCarpenter (15) suggested that the loss ofbody weight could be due to dehydrationand the catabolism of fats and proteins seenduring diabetes mellitus. Treatment withramipril could not prevent the weight lossin diabetic animals.
Diabetic rats exhibited glucosuria (>2%)48 hr after the injection of STZ (45 mglkg)and this persisted throughout thetreatment. At the end of six weeks serumglucose levels of the diabetic treated ratswere significantly higher than those of thecontrol animals (Table III). A correspondingdecrease was observed in the serum insulinlevels of the diabetic animals as comparedto the control untreated animals. It wasinteresting to note a decrease in the seruminsulin levels in the control treated animals(Table III), the mechanism for whichremains obscure. Lakkad et al (6) alsoreported similar finding with enalapriltreatment. Although the serum insulin
DISCUSSION
~-=:......._.
vacuoles were formed (Fig. 28). The sixweek ramipril treatment partially preventedthese disruptions (Fig. 2C).
Fig. 2: Representative histological view of rntmyocardium from control (A), diabetic: (8) anddiabetic trealed with ramipril (Cl.

358 Hakim et al
levels (22.12 ± 0.26) in the control treatedgroup were lowered, the serum glucoselevels (84.79 ± 7.67) were not significantlyhigher than those of the control untreatedgroup (84.12 ± 2.70). This suggests anincrease in insulin sensitivity in the controltreated group.
There are several reports on genesis ofhypertension in STZ-induced diabetesmellitus rat model. Kawashima et al (6)
were the first to report that rats treatedwith STZ developed hypertension. Sincethen many other workers have observedraised blood pressure in STZ treated rats(17,18). In the present study we observedsimilar changes in blood pressure. Ramipriltreatment prevented the rise in blood pressurein the STZ-treated animals (Table II).
Jackson and Carrier (19) reported theoccurrence of bradycardia when diabetes isinduced by STZ in normotensive rats.Savarese and Berkowitz (20) suggested thatthe decrease in heart rate could be due toa decrease in beta receptor binding sites inthe diabetic heart. According to Garber etal (21) another possible mechanism forbradycardia could be the hypothyroid stateof the animal. Ciaraldi and Marinetti (22)reported that hypothyroidism is known tocause a reduction in the density of bothalpha and beta receptors in the cardiactissue. Additional evidence for the role ofhypothyroidism in producing bradycardiawas provided by the observation that T1
treatment of STZ-induced diabetic ratsprevented bradycardia (23). In the present.study the heart rate of diabetic rats weresignificantly less than that of the controlrats. Ramipril treatment could prevent STZinduced bradycardia (Table II). Ramipriltreatment increased the T
3levels (Table III)
Indian J PhYliol Pharmacal 1991; 41(4)
as well in the diabetic treated group, thussupporting the hypothesis thathypothyroidism could be one of the causesof diabetes induced bradycardia in STZtreated rats. Although ramipril treatmentprevented STZ-induced hypothyroidism, thecardiac function was found to be depressedat higher filling pressures (Fig. 1).Histological study of the myocardiumrevealed that STZ-induced diabetes mellituscauses degeneration of fibres, loss of fibreintactness and vacuolization. Althoughramipril treatment prevented thisderangement the cardiac depression athigher filling pres!jures remained unaltered.This suggests involvement of other factorsin the pathogenesis of cardiomyopathy inthe present study.
Cardiac depression in the diabetic statecould be a result of microangiopathicchanges, altered cardiac autonomicfunctions (24), increased stiffness ofventricular wall (25) and changes insubcellular organelles such as sarcoplasmicreticulum (26), membrane pumps andenzymes in the sarcolemma (27, 28).Hyperlipidaemia may also lead to cardiacdepression. It has been reported thatWistar-Kyoto diabetic rats archyperglycaemic and hypoinsulinaemic butthey do not develop hypcrlipidaemia orcardiac depression (29). In the presentinvestigation STZ-treatment produced anincrease in serum triglyceride level (TableIII). Ramipril treatment did not alter theincrease in these levels. This suggests thatthe cardiac depression observed in thepresent investigation may be a result of thehigh serum triglyceride levels.
In the present investigation we foundan increase in the serum cholesterol levels

Indian J Physiol Pharmacol 1991: 41{4)
in the STZ-treated group. This increase inthe cholesterol levels was prevented byramipril (Table Ill). Increase in serum lipidsindicates either the defective removal orover-production of one or more lipoproteins.Insulin plays a role in both production andremoval of triglyceride rich proteins whichcould be the cause of lipid disorders ofdiabetes. Probably there is defective removalof triglyceride rich lipoproteins in theinsulin deficient state (30-33). Insulinadministration restores normal conditions.[n the present study we observed anincrease in the serum cholesterol levels withsimultaneous decrease in insulin levels inthe STZ-treated group. Ramipril treatmentreduced the cholesterol level with furtherdecrease in insulin levels in the control anddiabetic animals. This again indicates anincrease in the insulin receptor sensitivity.
Ramipril in Diabetes-Mellitus 359
In conclusion, chronic ramipriltreatment prevented STZ-inducedrise in blood pressure, bradycardia,hypercholestcrolaemia, and hypothyroidism.However, loss of body weight, rise in serumtriglyceride, and glucose levels remainedunaffected with ramipril treatment. Ourdata suggests that ramipril has a fewbeneficial effects in STZ-induced diabetesand that it may be a preferredantihypertensive in diabetic hypertensivepatients.
ACKNOWLEDGEMENTS
The present investigation was supportedby a Research Grant from the Council ofScientific and Industrial Research, NewDelhi for which the authors are thankful tothe Council.
REFERENCES
J. Barrett-Connor E, Criqui MH. Klauber MR,Holdbrook ,'1-1. Diabetes and hypertension in acommunity of older adults. Am J Epidem 1981;113:263-284.
2. Christilieb AR. Diabetes and hypertensive vasculardisease. Am J Cardiol 1913: 32: 52-606.
3. Reaven GlI..1. Role of insulin resistance in humandisease. Diabetes 1988;31: 1592-1601.
4. Goyal RK, Bangaru RA, Lakkad NB, Ran fo.IV.Effect of chronic treatment with atenolol andprazocin in streptoztocin induced diabetic nHS.IlldicHl J Physiol Pharmacol 1996;40:220-224.
5. Shah TS, Satia MC, Gandhi TP, Bangaru RA,Goyal RK. Effect of chronic Ilifedipine treatmenton streptozotocin-induced diabetic rats. J CoriuascPharmacol 1995;26:6-12.
6. Lakkad NB, Bangaru RA, Rao MV, Goyal RK.Studies on the chronic treatment of enalapril :lOdprazocin on diabetes induced cardiac depressionand other complications. Pharm Reu COIllIll 1991:9: 133-139.
1. Ball SG, Robertson JIS. Clinical pharmacology oframipril. Am J Cardiol 1981;59:23D-21D.
8. Linz KW, Scholkens BA, Han YF. Benefici effectsof converting enzyme inhibitor, ramipril, inischemic rat hearts. J Cardiouasc Pharmacol1986:(SUIlPI 10);591-599.
9. Struthers AD. The choice of antihypertensivetherapy in diabetic patients. Pos/grad/wte Med J1985: 61: 563-569.
10. Prince MJ, Stuart CA, Papin M, Bandi Z, Hol13ndB. Metabolic effects of enalapril andhydrochlorthiazide during treatment ofhypertensive diabetic patients; enaillpril forhypertensive diabetics. Arch Jill Med 1988: 148:2363-2368.
11. Amery A, Fagard R, Staessen J. Recent data onchanges in lipid metaolism induced byantihypertensive drugs. Cllrr Opi/lion Cardial1981;2:169-114.
12. Tarazi RC. Zanchetti AC. Prospectives forangiotensin converting enzyme inhibiton in heartdisease. J Hypertension 1985;3:599-5103.
13. Bolten S. In: Pharmaceutical Statistics: Practicaland clinical application. Marcell Dekker Series onDrugs and Pharmaceutical Sciences. Vol 251984;p231-232., Marcell Dekker Inc. Now York,USA.

360 Hakim et al
14. Junod A, Lambert AE, Stauffadhei W, Renold AE.Diabetogenic action of streptozotocin: relation~hip
of dose of metabolic response. J Clin Invut1969;48:2129-2139.
15. Horteizer V, Carpenter AM. Comparison ofstreptozotocin-induced diabetes in the rat,including volumetric quantitation of the pancreaticislets. Diabetologia 1973;9:178-184.
16. Kawashima H, Igarashi T, Nakajima Y, AkiyamaY, Ysukui K, Ohtake S. Chronic hypertensioninduced by streptozotocin in rats. NounynSchmiedebergs Arch Pharmacol 1978;305: 123-126.
17. Rodrigues B, Goyal RK, McNeill JH. Effects ofhydralazine on IItreptozotocin-induced diabeticralS: prevention of hyperlipidimia and improvementof cardiac function. J Pharmacal Exp Ther1986;237:292-299.
18. Fein FS, Miller B, Florcs Z, Mortan E. Myocardialadaptation to chronic propranolol therapy indiabetic rats. J Cardiovasc Pharmocol 1991;17:846-853.
19. Jackson CV, Carrier GO. Influence of short termexperimental diabetes on blood pressure and heartrate in response to norepinephrine and angiotensin11 in the conscious rat. J Cardiovasc Phormacol1983;5:260-265.
20. Savarese JJ, Berkowitz BA. Beta adrenoceptordecrease in diabetic ral heart. Life Sci1979;25:2075-2078.
21. Garber ow, Everett AW, Neely JR. Cardiacfunction and myosin ATPase in diabetic ratstreated with insulin, T, and T•. Am J Physiol1983;244:H592-H598.
22. Ciarnldi TP, Marrinetti GV. Thyroxine andproplylthiouracil effects in vivo on alpha and betaadrenergic receptors in rat heart. Biochem BiophysRes Commull 1977; 78:984-991.
23. Goyal RK, Rodrigues B, McNeill JH. Effect oftriiodothyronine on cardiac responses to
Indian J Physiol Pharmacol 1997; 41(4)
adrenergic-agonists in streptozotocin-induceddiabetic rats. Gen Pharmacol 1987;18:357-362.
24. Hulper B, Wilmes B. In: Gries FA, Freud F, RabeF, & Berger H eds. Aspects of autonomicneuropathy in diabetes. Stultgart:George ThiemeVerlag 1908; 77.
25. Reagen TL, Lyona MM, Ahmed SS. Evidence forcardiomyopathy in familial diabetes mellitus. J ClinInvest 1977;60:885.
26. Buccino RA, Spann JF, Pool PE, Sonnenblick EH,Braunwald E. InOuence of the thyroid state on theintrinsic cintractile properties and energy staruof myocardium. J CUn invest 1967; 46;1669-1682.
27. Lopaschuck GO, Tahiliani AG, Vadlamudi RVSV,Kstz 5, McNeill JH. Cardiac sarcoplasmicreticulum fundion in insulin or carnitine treateddiabetic rats. Am J Physiol1983; 245:969H-976H.
28. Dillman WHo Diabetes millitus induces changes incardiac myosin of the rat. Diabetes 1980;29:579582.
29. Rodriguu B, McNeill JH. Cardiac function inspontaneously hypertensive diabetic rats. Am JPhysiol 1986;250:4571-4580.
30. New MI, Roberts TN, Bierman EL, Reader GG.The significance of blood lipid alterations indiabetes mellitus. Diabetes 1963; 12:208-212.
31. Nikkila EA, Hormila P. Serum lipids andlipoproteins in insulin-treated diabetes:demonstration of increased high density lipoproteinconcentrstions. Diabetu 1978; 27;1078-1086.
32. Sosenko JM, Breahw JL, Miettimen QS, Gabbay KH.Hyperglycemia and pluma lipid levels: a prospectivestudy of young insulin-dependent diabetic patienls.N Engl J Med 1980; 302:650-654.
33. Albrink MJ, Lavietes PH, Man EB. Vasculr disesseand serum lipids in diabetes mellitus: observationsover thirty years (1931-1961). Arch Intern Med1963;58:305-323.