eduction of tissue iron stores and normalization of serum ... fileafter he refused deferoxamine...
TRANSCRIPT

.l.
n
i: d ,, ;, ~ :c r ~ s, ."·!:
I IC
l· . .
3' A r· nt ~
' ·s.
~
18 m
is !O
cy
J: UI
~r
I G
l, n, ia
of .ic
I to :w
tn
id "
1l
f I z .
H t ,.
,_..,. f r 1.
! •
eduction of Tissue Iron Stores and Normalization of Serum Ferritin During Treatment With the Oral Iron Chelator Lt in Thalassemia Iniermedia
ncy F. Olivieri, Gideon Koren, Doreen Matsui, Peter P. Liu, Laurie Bien dis, Ross Cameron, Robert A. McClelland, and Douglas M. Templeton
In patients with thalassemia lntermedia In whom hypera!J. sorption of iron may result in serious organ dysfunction, an orally effective Iron-chelating drug would have major therapeutic advantages, especially for the many patients with thalassemia intermedia in the Third World. We report reduc. tion in tissue iron stores and normalization of serum ferritin concentration after 9-month therapy with the oral chelator 1,2-dimethyt-3-hydroxypyrid-4-one (L 11ina29-year-old man with thalassemia intermedia and clinically significant Iron overload (SF 2,174 !'g/l., transferrin saturation 100%; elevated AST and ALT, abnormal cardiac radionuclide angiogram) who was enrolled in the study with L1 75 mg/kg/day after he refused deferoxamine therapy. L 1-lnduced 24-hour urinary iron excretion during the first 6 months of therapy was (mean :t: SD, range I 53 ::!: ao (11to109) mg (O.n mg/kg), declining during the last 3 months of L 1to24 :t 14 (13-40) mg
· PROGRESSIVE ORGAN dysfunction, often leading to mortality, is a consequence of transfusional or absorp
tionaJ tissue iron loading in patients with homozygous ~-thalassemia.1 Regular chelation therapy with deferoxamine reduces hepatic iron and arrests hepatic fibrosis,2 stabilizes iron-related cardiac disease,3 and prevents gonadal failure when started before age 10 years.• Administration of standard therapy with deferoxamine is problematic, however; the drug requires prolonged nightly subcutaneous (SC) infusion, frequently associated with local irritation. Compliance with this regimen decreases dramatically during adolescence,s and many patients with cardiac iron overload still die.5-8 Moreover, the cost of deferoxamine renders it unavailable to thousands of thalassemia patients in the Third World. It has long been acknowledged9 that the added convenience of an orally available chelator would simplify treatment of patients with transfusion-dependent thalassemia, and should also simplify management of patients with sickle cell disease who are maintained on a transfusion program in an effort to prevent or arrest specific disease complications .
Although transfusion-dependent anemias have focused attention on the worldwide need for a safe, orally active iron-chelating agent, disorders of increased iron absorption should also benefit from their development. Individuals with nontransfusion-dependent thalassemia (thalassemia "intermedia ")exhibit excessive dietary iron absorption that can lead to serious iron loading by the second or third decade of life.10The cost to these patients of neglecting iron loading is the development of life-threatening tissue damage, and infrequent infusions of deferoxamine may suffice to prevent iron ac.cumulation and its complications.II An orally effective iron-chelating drug would have major therapeutic advantages for these patients, especiaHy for Third v.:orici patients with thalassemia intennedia.1:
Several orally available, iron-chelating compounds have been developed in recent years9; few have been evaluated in human trials. Among those that have, l,2-dirnethyl-3-hydroxypyrid4-one (CP20 or LJ) has been demonstrated.to
Bloocf. Vol 79, No 10 (May 15). 1992: pp 2741·2748
(0.36 mg/kg), as serum ferritin decreased steadily to normal range (present value, 251 flg/LJ. Dramatic Improvement In signal intensity of the liver and mild improvement in that of the heart was shown by comparison of T,-weighted spin echo magnetic resonance imaging with images obtained Immediately before L 1 administration was observed after 9 months of L1 therapy. Hepatic Iron concentration decreased from 14.6 mg/g dry weight of liver before L1 therapy to 1.9 mg/g liver after 9 months of therapy. This constitutes the first report of normalization of serum fettitin concentration In parallel with demonstrateq reduction in tissue iron stores as a result of treatment with L1. Use of L1 as a therapeutic option in patients with thalassemia intermedia and Iron overload appears warranted . o 1992 by The American Society of Hematology.
promote clinically significant urinary iron excretion in animal studies13·14 and in human trials in the United Kingdom,1s.16 Europe," India,18 and Canada.19 In a shortterm randomized, cross-over study, Ll's ability to induce urinary iron excretion was demonstrated to be comparable to that of SC deferoxamine and well tolerated20; recent studies have demonstrated its continued long-term efficacy.16.1?
We report reduction in tissue iron in the liver and heart, as demonstrated by magnetic resonance imaging (MRI) of both organs, and pe.rcutaneous liver biopsy, after 9 months of therapy with L1 in a patient with thalassemia intermedia at high risk of progressive iron-induced morbidity. nus constitutes the first report of normalization of serum ferritin concentration and demonstrated reduction of tissue iron stores as a result of treatment with Ll.
MATERIALS AND METHODS
Case Report In 1989, a 29-year-old Italian male was evaluated for liver
disease, presumed to be scoondary to iron overload. The son of
From IM Diviswnsof Hamratology/Oncolcgyand Clinical Pharmacology, The Hospital for Sick Childnn; Divisions of Haematology, Canliolcgy, Gastroentuolcgy, and Pathology, The Toronto Hospital; and the DepartmQlls of Pediatrics, Medicine, Pathology, Chemistry, and Clinical Biochemistry, The University of Toronto, Toronto, Canada.
Submitted November 19, 1991; accepted January 16, 1992. Suppot1ed by Grant No. MA 10601 from the Medical Researr;h
Council of Canada. N.F.O. and G.K art Carter Scientists of the Ontario Ministry of Health.
Address rtprint requests to Dr Nancy Oliv~ri, Division of Haematology/ Oncology, The Hospital for Sick Children, Room 6'324, 555 UniversilyAve, Toronto, Canada M5G I X8. J · Tnc publicatior. costs o,,~. tili.; a."11d~ wer~ aefraycd'\ir. par. o:~.r}iig'r-'· charge payment. This article must therefort be hereby maf!<t:d "advertisement" in accordanu with 18 U.S.C. section 1734 solely to indicate this fact.
c 1992 by The American Society of Hematology . 0006-4971192/7910-0032$3.00/0
2741
1 of 8
Taro Pharmaceuticals, Ltd. Exhibit 1005

2742
nonconsanguinous pare.nts from Calabria, he bad been diagnosed with homozygous P thalassemia and had undergone a splenecrorny in 1964 at age 3 years. In 1980, he underwent cbolcc:ystcctomy after repeated episodes of abdominal pain associated with radiologic demonstration of gallstones; RBC transfusions were administered before both opcratiollS. He had never re<:cived transfusions since then. Io 1980, observation of abnormal IC't'Cls of AST and ALT and an inc:rcased serum ferritin oonccntration prompted initiation of a program of nightly SC dcferoxamine therapy; the patient complied with this erratically and discontinued it after 6 months, although the risk of potential iron-related morbidity had been explained to him. He administered no iron-chelating therapy in the next 10 years.
In 1990, he sought medical attention because of worsening fatigue. Physical examination showed bim to be deeply pigmented and icteric, with mild muscle wasting. The liver was enlarged and firm. Height was at the fiftieth percentile for an adult male11;
external genitalia were fully developed. Laboratozy hematologic studies were consistent with previous assessments of steady-state hemoglobin concentrations of 15 to 85 g/L, increased total WBC and platelet oounts, and a hemoglobin electrophoresis demonstrating 98% hemoglobin F and 2% hemoglobin Al. consistent with p0
th!ilassemia. Fasting glucose, testosterone, TSH. thyroxine, calcium, phosphate and PTH measurements were within normal limits. Serum AST and ALT levels were increased at 139 and 98 U/L, respectively (normal for both <40 U/L); prolbrombin time, PlT, total protein, and albumin were within normal limits. Transfcrrin saturation was 95% to 100%; serum fcrritin oonceotratioo was 2,000 JLg/L (normal < 300 µ.g/L). Analysis of DNA from peripheral blood lymphocytes (PBL) demonstrated homozygosity for the codon 39 C~T mutation respoI1S1l>le for po thalasscmia, a normal et-globin gene cluster, and bomozygosity for the presence of the C to T substitution at position 158 S' to the (Ty gene.n Resting electrocardiogram demonstrated atrial bigeminy; radionuclide angiogram of the heart showed a normal resting ejection fraction (EF), but no increase in EFwitb exercise, and mild abnormalities oC diastolic function.
The evidence for and risk of progression of iron-related organ damage was explained in full to the patient, who nevertheless declined to resume SC deferoxamine or to begin a program of continuous intravenous (IV) defcroxamine infusions; 9 months later, be was offered enrollment in the Canadia~ trial of the oral iron ehelator Ll. At this time, serum ferritin concentration was increased at 2,174 JLg/L; transferrin saturation was increased at '100% (normal <30%); serum AST and ALT were increased at 126 and 94 U/L, respectively; and serum triglyceride level was in· creased at 3.74 mmol/L (nonnal 0.34 to 1.58 mmol/L). Antinuclear anti~y and rheumatoid factor were negative. ACTH stimulation testing demoO.Strated normal baseline ACTII and cortisol, normal oonisol lcvcls 30 and 60 minutes after ACTII stimulation, and two normal urinazy free cortisol quantitations. Baseline 2~hour urinary iron excretion was 2.9 mg. After undergoing baseline MRI of the liver and heart and percutaneous liver biopsy, the patient began therapy with Lt at 75 mg/leg body weight per day, administered in three divided doses at 8-hour intervals in the fasting state.
Methods
This study was approved by The Hospital for Sick Children's Human Subject Re& \\ ·:::Ommme~ and tile Health Protection Branch, Health and Welfare CanltGa (File No. 9427-Hl117-41C. HPB, Ottawa. Canada). Writte; informed consent was obtained from the patient. Lt was synthesized according lo previously published methodsD by the direct reaction in aqueous solution of methylamine and mahol, as described previously. 202'
OLIVIERI El
Hepo/U iron quaflliJ.ation. Pcrcutan'eous liver biopsy specirr were divided with a wooden splint and weighed immediate~ determine fresh weighL One portion was then overdried (10~ hours), reweighed and wet-ashed with hot concentrated HJ (Suprapur; Mercie, Dannstadt) in a sc:rew-<ap Teflon vcssc~ analysis of total iron by Zeeman-corrected clectrothermal ato absorption (Varian SpectrAA·300; Techtron Ply, Ud, Malgr Australia). The other portion was homogenized with a pb pestle in a microcentrifuge tube in 0.50 mL cold 0.25 m< sucrose/3 mmol/L imida:zole Ha, pH 7.2 Total iron reoovere the homogenate, as compared with that determined in the d sample, was 89% to 90%. After sonication (Branson Sot W-350; power setting 3, 15 pulses at 20% duty cycle), a 100· aliquot was applied to a carboxymethylcellulose oolumn and ch in stepwise fashion according to the method of Selden and Pete Fractions eluting in the order of transferrin, ferritin, hemoprot1 and hemosiderin were analyzed for iron by atomic absorption.
Histok>gic t:XJtmination of the liver. Cores of liver tissue v fixed in 10% buffered formalin, embedded in paraffin, and stai witb Prussian blue for iron. Tissue was fixed in universal fua (2% glutaraldehyde plus 4% fonnaldehyde) and processed u standard methods for transmission electron microscopy usu Phillips 400 electron microscope.
Magnetic resonance imaging. The patient underwent magr resonance imaging (MRI) in a I.ST superconducting magnet u a spin-echo technique.26 The patient was positioned supine · simultaneous cardiac and respiratory gating. Initial coronal ITansverse images were talc.en to determine the Euler angle image the heart, liver, and peripheral muscle simultaneously a the cardiac short axis. Ti-weighted spin echo was perfonncd u cardiac gated sequence oonsisting of R-R interval/20/ 2 (TR (1 of pulse repetition)/TE (time to ecbo)/numbcr of ~uisiti spanning &om the apex to the base of the heart at 1-cm centei center separations and 7-mm slice thiclcness.
A midbcart slice position was then selected as the referena the T :-weighted spin echo acquisition. This was a gated multi1 sequence consisting of [x R-R/20-40-60-80/2 (TR/TE)/ numb! acquisitions]. Finally, the slice was angled so that it also trave both left and right lobes of the liver and the shoulder !"usdes.
Image analysis. The signal intensities from the cardiac scp1 posterior wall, liver, and peripheral muscle were calculated I identically positioned slices of the T1-weighted spin echo gradient echo images. A 0.25-cmZ of the region of interest applied over these organs, and ai;i average signal intensity obtained. The ratio of signal intensities between. the heart peripheral muscle and the liver and peripheral muscle were 1
subsequently for comparison. Image-derived Tz values were tained by fining the signal intensities from each echo of multiecho sequence to an exponential function: SI = SO · e- 1
where SI is signal intensity, SO is nondecayed signal intensity, lE is time to echo. The signal intensities were first correcte< variation in image field site and receiver attenuation when app ble.n
RESULTS
Efficacy of LI
Urinary iron excretion. Urinary iron excretion durinf first 6 months of LI therapy varied becween 113 and l~ iron excre ted in 24 hours, with a mean excretion of 53.3 equal to a mean urinary iron of 0. 77 mg/ leg body weight day. During the next 6 months of Ll administration, patient's urinary iron excretion varied be tween 4.6 and mg in a 24-hour period, with a mean excretion of
2 of 8
Taro Pharmaceuticals, Ltd. Exhibit 1005
'·
>
)
I : .
OAAl IRON CHELATION IN THAl.ASSEMIA INTcRMEDIA
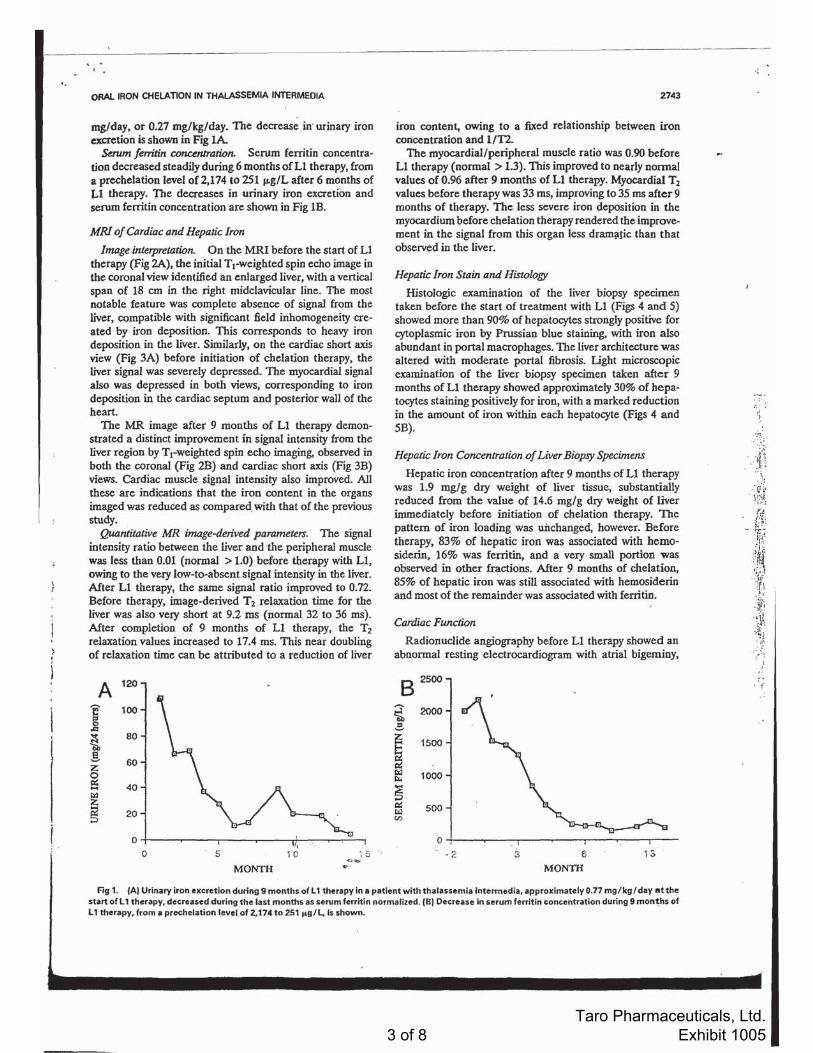
mg/day, or 0.27 mg/kg/day. The decrease in· urinary iron excretion is shown in Fig lA
Serum Jerri/in concetµradon. Serum ferritin concentra· tion decreased steadily during 6 months of LI therapy, from a prechelation level of 2,174 to 251 µ.g/L after 6 months of Ll therapy. The decreases in urinary iron excretfon and serum ferritin concentration are shown in Fig lB.
MRI of Cardiac and Hepatic Tron
Image inLerpreJati.on. On the MRI before the start of LI therapy (Fig 2A), the initial Ti-weighted spin echo image in the coronal view identified an enlarged liver, with a venical span of 18 cm in the right midclavicular line. The most notable feature was complete absence of signal from the liver, compatible with significant field inhomogeneity created by iron deposition. This corresponds to heavy iron deposition in the liver. Similarly, on the cardiac shon axis view (Fig 3A) before initiation of chelation therapy, the liver signal was severely depressed. The myocardial signal also was depressed in both views, corresponding to iron deposition in the cardiac septum and posterior wall of the bean.
The MR image after 9 months of Ll therapy demonstrated a distinct improvement in signal intensity from the liver region by Trwcighted spin echo imaging, observed in both the coronal (Fig 2B) and cardiac short axis (Fig 3B) views. Cardiac muscle signal intensity also improved. All these arc indications that the iron content in the organs imaged was reduced as compared. with that of the previous study.
Quantila.tive MR image-derived parameters. The signal intensity ratio between the liver and the peripheral muscle was less than 0.01 (normal > 1.0) before therapy with Ll, owing to the very low-to-absent signal intensity in the liver. After L1 therapy, the same signal ratio improved to 0. 72. Before therapy, image-derived T 2 relaxation time for the liver was also very short at 9.2 ms (normal 32 to 36 ms). After completion of 9 months of Ll therapy, the T2
relaxation values increased to 17.4 ms. This near doubling of relaxation time can be attributed to a reduction of liver
A 120
c :s
100 0 ,Q
~ 80
g 60 z
0 ex: .... 40 ll:l z .... ~ 20 ;:i
0 I
0 5 10 : 5 .. ~ ...
MONTH ..
2743
iron content, owing to a fixed relationship between iron concentration and l/T2.
The myocardial/peripheral muscle ratio was 0.90 before Ll therapy (normal > 1.3). This improved to nearly nonnal values of 0.96 after 9 months of LI therapy. Myocardial T2
values before therapy was 33 ms, improving to 35 ms after 9 months of therapy. The less severe iron deposition in the myocardium before chelation therapy rendered the improvement in the signal from this organ less dram;lfic than that observed in the liver.
Hepatic Iron Stain and Histology
Histologic examination of the liver biopsy specimen taken before the start of treatment with Ll (Figs 4 and S) showed more than 90% of hepatocytes strongly positive for cytoplasmic iron by Prussian blue staining, with iron also abundant in portal macrophages. The liver architecture was altered with moderate portal fibrosis. Light microscopic examination of the liver biopsy specimen taken after 9 months of Ll therapy showed approximately 30% of hepatocytes staining positively for iron, with a marked reduction in the amount of iron within each hepatocyte (Figs 4 and SB).
Hepatic Iron Concentration of Liver Bi.opsy Specimens
Hepatic iron concentfation after 9 months of Ll therapy was 1.9 mg/g dry weight of liver tissue, substantially reduced from the value of 14.6 mg/g dry weight of liver immediately before initiation of chelation therapy. The pattern of iron loading was unchanged, however. Before therapy, 83% of hepatic iron was associated with hemosiderin, 16% was ferritin, and a very small portion was observed in other fractions. After 9 months of chelation, 85% of hepatic iron was still associated with hemosiderin and most of the remainder was associated with ferritin.
Cardiac FWlction
Radionuclide angiography before Ll therapy showed an abnormal resting electrocardiogram with atrial bigeminy,
B 2soo
~ 2000 .:,
~ 0:
1500
~ 1000
~ 0: 500 Czl Cl)
0 . 2 3 6 13
MONTII
Ag 1. (A) Urinary iron excretion during 9 months of L 1 therapy in• patient with thalassemla lntennedia, approximately0.77 mg/kg/ day at the start of L 1 therapy, decreased during the last months as serum ferrit ln normalized. (Bl Decrease In serum ferTitln concentration during 9 mon~hs of L 1 therapy, from a prechelation level of 2, 174 to 251 i<g/L. ls shown.
· : ,I ·~
3 of 8
Taro Pharmaceuticals, Ltd. Exhibit 1005

-....... .
2744
rcvcrti111: In 1111rmal :;inus rhvthnl tlurinl! cXt:r<"i~e·. The· ldl ,·c111ri,·uJar EF (l.VEF) wa~ i, l '~i· a[ rcsl.·~·ilh 1111 im:n.::1se· a1 pe·~k c~i.:rci~c. Mild righ l v\1nlrirnla r di la1a1i11n. and mild ;1iinormali11i.:s in tlia-;1niic fu11~·1 i', ;ri (pl:·a i.. lilii11g r:1ll". time· to pl·ak lillinc,. and alri;il con1rihutio111 \\l"t~·°';ih~L:rvi.:d.
l\f1cr ') monlhs of I.I therapy. Iii.- n:~tin!! 1.VEF remained normal I 57~"i. ). with a n1>rmal incr.:;1\c ( 111 <>.;~ ·; 1
OLIVIERI ET A
Fig 2. MAI of hepatic iron IA) before l 1 therapy. Initial r,.welghted spin echo MRI in the coronal view Identified an enlarged liver with• vertical span of 18 cm In the right mldclavlcufar Une. Complete absence of signal lrorn the liver i$ compatible w ith significant field inhomogeneity crHted by Iron deposition. (Bl Aller 9-month t 1 therapy. T1-welghted spin echo MRI In the coronal view demonstrated improvement In signal intensity from the liv1n. Indicating lhal the Iron content was reduced 1s compued with that In th• pr~vious study.
11m,· ohse·1-v1:d :11 pi.: :1~ ncffi'". Thi.: a h1111r111:di1 ;,., 111' ri!tlll v.:111ricul:1r dilat:ition :rntl ahnum1alit il·' in dia,111li<: luni.:· li<IU did 111>1 r fl :1ll [!L" dur ing ! .I lhrrapy. 1.:~<"Cpl fm :1 ' li!!hl i111pn11·i.:111cn1 in atrial l·11111rihll1ion ( 1-l ' ·; :1fln I.I the·r;1py. :is wmparl·d wilh 17"; hcfurl" 1hc1-.1py ).
Sc(/i-ty cf I.I. The· pa1iL·nt v..;is rc\'icw.:d in th.: i.:linii.: wi.:ddy. I k tuli.:rakd I .I wdl. and rqwrwd 1111 j11i111 p;1in or
4 of 8
Taro Pharmaceuticals, Ltd. Exhibit 1005

•. ORAL IRON CHELATION IN THAl.ASSEMIA INIERMEDIA
Fig 3. MRI of cardiac iron before l 1 therapy (A). lnitlal T 1-welghted spln echo MAI in the cardiac short axis view demonstrated a depressed myoc•rdial signal. (B) After 9-month L 1 therapy, T 1·weighted spin echo MRI in the cardiac short axis view demonstrated improvement, indicating that the iron content was reduced as compared whh that in the previous study.
,1jff111:~s.:• "' ~ll ch:lll!!l' in hi.:01:1111l111!il· or hi11chc111icd paranic1•·rs was nb~c;,.·c:d <lurill)! •/ 1~1t1111hs ,,f 1Jt,.:,1py. ;\CTI I 1c,1in)! rcpt·:1tnl 4 nllllllh' :1flc:r ha,t·li1w ~lmwctl n11
d1;J11j.ll' in th.: \'al11c~ nhscr\'cd hl'l'or•· I.I ;1d111i11is1ratiou. A111inurk;ir an1ih11dy ;1ml rhc11111a1nid fac:t11r ha\'.: ri.: · 111aincc.J nc::gati,·c.
2745
DISCUSSION Thousand~ o f Thiru World pa tie nts w it h 111aj<>1
.,tJ;alassc:mia S)'nclmmcs. induding those who develop irn11-., rl'lall'd !c>xil'ity in asS<><:iation wilh gastrnintcMinal hypcrab
~<•rption uf irnn. 11 .:xhihit scriou:; inn1-rc::latc:d nwrhidity and ruortality. F<•r lh~·sc palicnl'-, ;111 orally ~t·tivi.: iron ·
'• '
5 of 8
Taro Pharmaceuticals, Ltd. Exhibit 1005

....... , - .
2746
chclnling agent would provide life-sa~ing. chdati<•n thi:rapy. Fnr palicnts of the <lcvd0pcd world. freedom from nightly. 11f1,·n p<1inful infusions w.rnld represent a wck(lme normaliz<iiion of lifestyle. An nwlly availahlc iron-d1clalin~ :1gc11t has thus been souchl at·li,·ci\· for more lhan.a dcc;idc.
The l>idcntalc h)•drm:ypyrid1•ncs show t:onsidcrahk potential as orally availahlt: iron chl"l~h•rs . t\dmini~tratinn Pl l.2-tlimc1hyl-:\-hydrnxypyriJ·-l-1iril0 or 1.1 1' · : 11 n:sull..:<l in urinary iron cxcrctinn comparable 1111hal 11h~l'incJ with SC dcfcroxaminc.: in thalassc.:rnic p:iticms. Although conllicting ohsc:rva1ions of acutc toxicity have hecn rc:pnr1l·d wilh usc
OUV!ERI ET AL
Fig 4. Hepatic Iron stain and histology at low and high power IA) before l 1 therapy. Histology of the liver showed more then 90'1. olhepatocvtes strongly pos· ltive for cytoplasmic Iron by Prussian blue sulnlng. Iron was also abundant In groups of portal macrophages; liver architecture was altered with moderate por· tal fibrosis. (8) After 9 months of L 1 therapy. light and electron microscopic examination of the liver showed approximately 30% of hepatocytes staining posl· tively for Iron, with • marked reduction in the amount of Iron in each hepotocyte.
of LI in animals.·" ·'~ administration t1f tlll." drui: ha' been <t!\SO<:iatcd with infrcqu..:nt bul s..:ri<HI' t:11111plica1io11!-. in hum;i111ri<1b. including agr;111ulnc.:ytosis and 1hro111ho<:ywpl."· nia which rc.:\'l"rsc:d :1f1-c·r wirhdraw;tl of I.I." ;111<l in lnng· te rm <:linit·:il lriab l11:111atolo~k par:11111."lcrs will h;i\l" t11 he m1•ni1orc:d l·:1rcfully to tktt· rminl" thL· risk ,,r aµran11!11,)'h•si, and wh..:1111.:r 1hc <l rtrl! is ;Kn·ptahl\' :oak lc1r dinit'al u,c.
\Ve.: repc>rt ll<>rmalizaiinn uf Sl'rtl01° krritin n111ccntra1ion and rcdl•l'ti••n in tissue.: iron ston:s in .1 p:llil."nl with lhalasscniia in1cr111l·dia 111;iint:ti1wd on I . I f1>r •J months. Like lhis p:i1ic111. indi<idu:ol< with th:il:i~"l"1lli:1 i111c·rm~·Jia
6 of 8
Taro Pharmaceuticals, Ltd. Exhibit 1005

ORAL IRON CHFLA TION IN THALASSEMIA INTEAMEOIA
Fig S. Hep•tlc; Iron stain and histology (Al before l 1 therapy and (8) after 9 months of l 1 therapy. w ith a marked reduction In nalnable Iron.
who maintain a hi!lh pc:riphcral hcmoglohin conccntrMion without regular RDC transfusions may show variable degrees of exc:es.~iv.: food iron ahsorpli<>n which may lead to serious iron loading f:iy middle life.11 TI1c~c· patients represcnl a major puhl ic health pn1hlcm in populations in which lhal:t ~i;emia is w mmou.1! Although the <k grce of iron owrlo:ul is less in suc:h patknt~ than in patknts with tr:111sf11si11n-dep<:ndl·nt thaht~scmia .11 nur patient hnd cvi· <lcn.:c of inm-rclaktl nrgan wxicity with carF:i- hepatic: cirrhosis :111d mi(.! eardi;ic: dias tolic (lysfunl·tion with la.:k nr systolic incrca'c: with c~l·rt"i'l' . I.I thl·rapy ha~ rcduc:c:d hi~ ti~~11e irnn fo;1tf suhManti:1lly. a~ dcmon~t ra t e<.l hy reduction in tran~fcrrin ~;1t11ra t i1111 and ~c:rum krritin conc:cntration. i111pruvc111c111 in lin·r l111wt ion. and inc:rca<c in I. vr:r with •·xcrci~.: aftl·r ''·11111111h I.I thc1ap) . impro,cml·nt in /v!RI of J.
1
2747
cardiac and hepatic iron, and reduction in hepatic iron conccnlnition. Omtinucd monitoring of urinary iron cxcrctfon and 1rc11ds in scrum fcrritin conccnrrntion in response lo a reduced daily dllSc of LI will be necessary in t11fa patient to prevent further iron-related organ damage.
Our reporl is the first to present cvitlcncc in hum:ms for LI -induced rcJuction of iron in the liver unJ heart, the organs involvc1I in th..: most ~crinu~ iron-rclntcJ morbidity :mu m!lrtali ty. Although the :>afcty and dlic:acy of long-term use of LI has hl'l'll the suhjcct ,,f much ddiatc.~'-.':
governmental appnwal frn c:li11i.:al 11 ials t\f LI is "'"' forthcoming. in !'cvt•r:1I crn1111rk~. indudin~ the U11i1c:d Stales. ;tnd ~hould he wpportcd hy the c:nt·ouragin!! result ohSC:f'\cd in'"" pal icnt.
REFERENCES .....
Coh,·n 1\. l ':o.:.1t.11rir hcm:11itl••c\ . I lr111a111I On.·111 Clin N11r1h ,\111 (::\:::I. l'IX' • •
,;. ll.1rr~ ,\I. Fl~ 1111 I>. Lt·t'~~ I:. l(i-.l11n k1\: I ""!: r.:11n d1clJ ti11n
llu.·rary Ill th:ila"cnua nMJtlf l ~fh:t·1 un livl·r 1r,1n c:c111l"l .. Ulration.
Ii\ er hi''"'"!!) .rn.t dtni.-:11 prllftC>'. llr Med) =::tl'I. 1'17-1
.1. \Volf,· LC Oli< 1cri NF. !>:111,111 Dl.. Pr11rr•·r RD. Frcc,lm;111
.• '•·
" . 1 . ... l.'.
: '~
7 of 8
Taro Pharmaceuticals, Ltd. Exhibit 1005

... 2748
MH, Nathan DG: Tbe prevention of cardiac disease by subcutaneous deferoxamine in patients with thalassemia major. N Engl J Med 312:1600, 1985
4. Bronspigel-Weintrob N, Olivieri NF, Tyler BJ, Andrews D, Freedman MH, Holland FJ: Effect of age at the start of iron chelation therapy on gonadal function in P-thalasscmia major. N Engl J Med 323:713, 1990
5. Olivieri NF, McGee A. Liu P, Koren G, Freedman MH, Benson LN: Cardiac disease-free survival in patients with thalassemia major treated with subcutaneous deferoxamine: .An update of the Toronto cohort. Ann NY Acad Sci 612:585, 1990
6. Aldouri MA, Wonke B; Hoffbrand AV, Flynn DM, Ward SE, Agnew JE, Hilson AJW: High incidence of cardiomyopathy in beta-thalassemia patients receiving transfusion and iron chelation: Reversal by intensified chel.ation. Acta Haematol 84:113, 1990
7. Ehlers KH, Giardina PJ, Lesser ML, Engle MA, Hilgartner MW: Prolonged survival in patients with beta-thalassemia major treated wi.th deferoxamine. 1 Pediatr 118:540, 1991
8. Lerner N, Blei F, Bierman F, Johnson L, Piomelli S: Chelation therapy and cardiac status in older patients with thalasscmia major. Am J Pediatr Hematol Oncol 12:56, 1990
9. Hershko C. Weatherall DJ: Iron-chelating therapy. CRC Crit Revain Lab Sci 26:303, 1988
10- Pippard MJ, Rajagopalan B, Callender ST, Weatherall DJ: Iron loadi.ng. chronic anemia, and etythroid hyperplasia as determinants of the clinical features of j:l-tbalassemia intermedia, in Weatherall DJ, Fiorelli G, Gorini S (eds): Advances in Red Cell Biology. New York, NY, Raven, 1982, p 103
11. Pippard MJ, Weatherall DJ: Iron absorption in nontransfused iron-loading anemias: Prediction of risk for iron loading, and response to iron chelation treatment, in j:l-thalassemia · intermedia and congenital sideroblastic anemias. Haematologica 17:404, 1984
12 Weatherall DJ, Clegg JB: The Thalassemia Syndromes. Oxford, UK, Blackwell Scientific Publications, Oxford University Press, 1981
13. Kontoghiorghes GJ, Hoflbrand AV: Orally active a-ketohydroxypyridine iron chelators: Studies in 'mice. Mo! Pharma.col 30:70, 1986 .
14. Kontoghiorghes OJ: Dose response studies using desfenioxamine and orally active chelators in a mouse model. Scand J Haematol 37:63, 1986
15. Kontoghiorghcs GJ, AJdouri MA, Hoflbrand AV, Barr J, Wonke B, Kourouclaris T, Sheppard I.; Effective chelation of iron in P-thalassemia with the oral chelator LI. Br Med J 295:1509, 1987
16. Kontoghiorghes 01, Bartle$$ AN, Hoflbrand AV, Goddard JG, Sheppard L, Barr J, Nortey P: Long-tenn trial with the oral iron chelator 1,2-dimethyl-3-hydroxypyrid-4-one (Ll ). Br I Haematol 76:295, 1990
17. Tondury P, Kontoghiorghes GJ, Ridolfi-Luthy A. Hirt A, Hofibrand AV, Lotennbach AM, Sonderegger T, Wagner HP: LI
J, .
OLIVIERI ET Al
(1,2-dimethyl-3·hydroicypyrid-4-one) for orai" iron chelation in patients with beta-thalassemia major. Br I Haematol 76:550, 1990
18. Agarwal MB, Viswanathan C, Ramanathan J, Massi! DE, Shah S,Supte SS, Vasandani D, Puniyani RR: Oral iron chelation wilh LI. Lancet 335:601, 1990
19. Olivieri NF, Koren G, KleinJ, Freedman MH, Hermann C, Matsui D, Oiung D, Templeton DM: Oral iron chelat.ion with 1,2-dimethyl-3-hydroxypyrid-4-one (Ll) in thalassemia major: pharmacokinetics, safety and iron excretion. Blood 76:72, 1990 (abstr)
20. Olivieri NF, Koren G, Hermann C. ~ral: Evaluation of the oral iron cbelator LI in iron loaded patients. Lancet 336:1275, 1990
21. Tanner JM, Whitehouse RH: Oinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child 51:170, 1976
22. Miller BA. Olivieri NF, Salameh M, Ahmed M, Aatogoetti G, Nathan DO, Orkin SH: Molecular analysis of the high F phenotype in Saudi Arabian sickle cell anemia. N Engl I Med 316:244, 1987
23. Kontoghiorghcs GJ, Sheppard L: Simple synthesis of the potent iron chelators· l-alk:yl-3-bydroxy-2-methylpyrid-4-ones. lnorg Chim Acta 136:L11, 1987
24. Olivieri NF, Koren G, Herman C. St Louis P, Bentur Y, Oiung D, Klein J, McClelland RA, Templeton DM: Studies of the oral chelator L1 in thalassemia patients. Semin Hematol 27:101, 1990
25. Selden C. Peters TJ: Separation and assay of iron proteins in needle biopsy specimens of human liver. Oin Otim Acta 98:47, 1979
26. Johnston DL, Liu PP: Evaluation of myocardial ischemia and infarction by nuclear magnetic resonance techniques. Can J Cardiol 4:116, 1988
27. Frahm J, Haase A. Matthaei D: Rapid 3-dim.ensional MR imaging using the Fl.ASH techniques. 1 Comput Assist Tomog 10:363, 1986
28. Mehta J, Singhal S, Revankar R, Walvalkar A, Olablaoi A, Mehta BC: Fatal systemic lupus ef)'tl!ematosus in patient taking oral iron chelator Ll. Lancet 337:298, 1991
29. Berdoukas VA: Antinuclear antiOodies in patients taking Ll. Lancet 337:672, 1991
30. Olivieri NF, Koren G, Freedman MH, Roitman C: Rarity of systemic lupus erytbematosus after oral iron cb~lator LI. Lancet 337:924, 1991
31. Kontoghiorghes GJ: Safety of oral iron chelator Ll. Lancet 2:457, 1989
32. Porter JB, Hoyes KP, Abeysinghe R, Huehns ER, Hider RC: Animal toxicology of iron chelator Lt. Lancet 2:156, 1989
33. Hofibrand AV, Bartlett AN, Veys PA, O'Connor NT, Kontoghiorghes GI: Agranulocytosis and thrombocytopenia in a patient with Diamond-Blackfan anemia during oral chCtator trial. Lancet2:457, 1989
8 of 8
Taro Pharmaceuticals, Ltd. Exhibit 1005