drug and toxin induced liver disease hepatotoxicity from chemicals
TRANSCRIPT

Drug and toxin Induced liver Disease
hepatotoxicity from chemicals
Drug Induced liver Disease Liver is the mayor detoxifying organ in
the body. Liver is subjet to potential damage from
pharamceutical and environmental chemicals.
Injury may result from: Direct toxicity Hepatic conversion of chemical. Immune mechanisms.

Drug Induced liver Disease Liver damage from chemicals may be
immediate or take months. Forms of liver injury:
Hepatocyte necrosis Cholestasis Insidious onset of dysfunction. Drug induced chronic hepatitis is
indistinguishable from chrinc viral hepatitis

Drug Induced liver Disease
Hepatocelular damage
Chemicals
Microvesicular fatty change
Tetracycline, salicylates.
Macrovesicular fatty change
Ethanol, methrotexate.
Massive necrosis Acetaminophen, insoniazid.
Hepatitis, acute and chronic
Methyldopa, phenytoin.
Cholestasis Anabolic steroids, oral contraceptives.

Drug Induced liver Disease
Reye syndrome Mitochonrdial dysfuntion in liver and
some other organs. Predminantly in children given
acetylsalicylic acid cause of fever. Produces microvesicular steatosis
with severe liver dysfuntion.

Alcholic liver disease
(Ethanol Metabolism)

Epidemiology It develop only after a "threshold" dose 600 kg for men and 150 to 300 kg for
women. one must consume eight 6-oz beers, 1 L
of wine, daily for a period of 20 years Almost all people who exceed this
threshold dose of ethanol exhibit some biochemical or histologic abnormality suggestive of liver injury

Epidemiology
fewer than 50% of people who ingest the calculated threshold dose of ethanol eventually develop serious alcoholic liver disease (e.g., alcoholic hepatitis or fibrosis).
This suggest that the pathogenesis involves hereditary and enviromental disorders.

Metabolism Liver. 3 enzyme systems:
ADH MEOS Catalase.
There exist several isoforms of the ADH enzyme (alfa, beta and gamma) and its variation changes the metabolic rate of ethanol. Asians (beta2) 20% faster.
ADH acts alone when tissue levels do not exceed 10 mmol/L
MEOS Cytochrome P-450 2E1 (CYP2E1) also the metabolism of other drugs such
as acetaminophen, haloalkanes, and nitrosamines
Chronic ethanol consumption up-regulates CYP2E1
CYP2E1-mediated ethanol oxidation yields reactive oxygen intermediates
These are capable of provoking hepatocellular damage


Acetaldehyde is a highly reactive and potentially toxic compound. It is metabolized by the ALDH .
Half of Chinese people are deficient of this enzyme.

Gastric metabolism
Gastric ADH is implicated in first-pass metabolism of ethanol
This limit the ethanol delivery to the portal circulation
This enzyme is lower in Women.

Eventos mórbidos

Oxidant Stress
DNA is sensitive to oxidant stress. Mitochondrial DNA is more susceptible than nuclear DNA to oxidative damage because of reduced protection by histone and nonhistone proteins and because of a decreased capacity for repair
This causes deletion and mutations in DNA

Alcoholic hepatitis Hepatocyte necrosis
Infiltrate of neutrophils +/- fatty change
+/- Mallory bodies +/- bile stasis
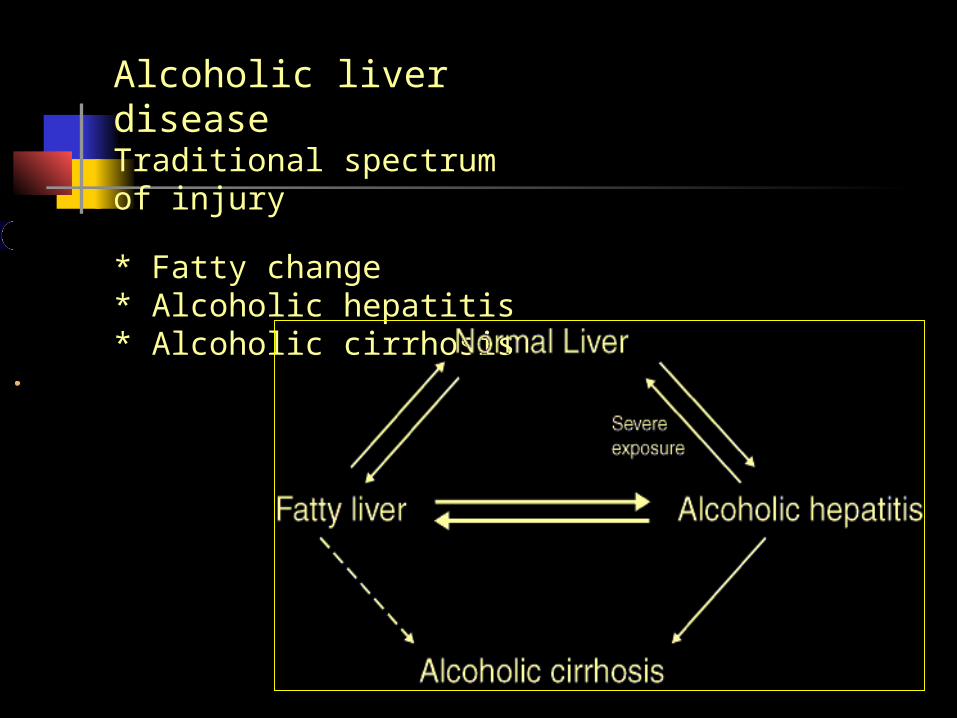
Alcoholic liver disease Traditional spectrum of injury
* Fatty change* Alcoholic hepatitis* Alcoholic cirrhosis
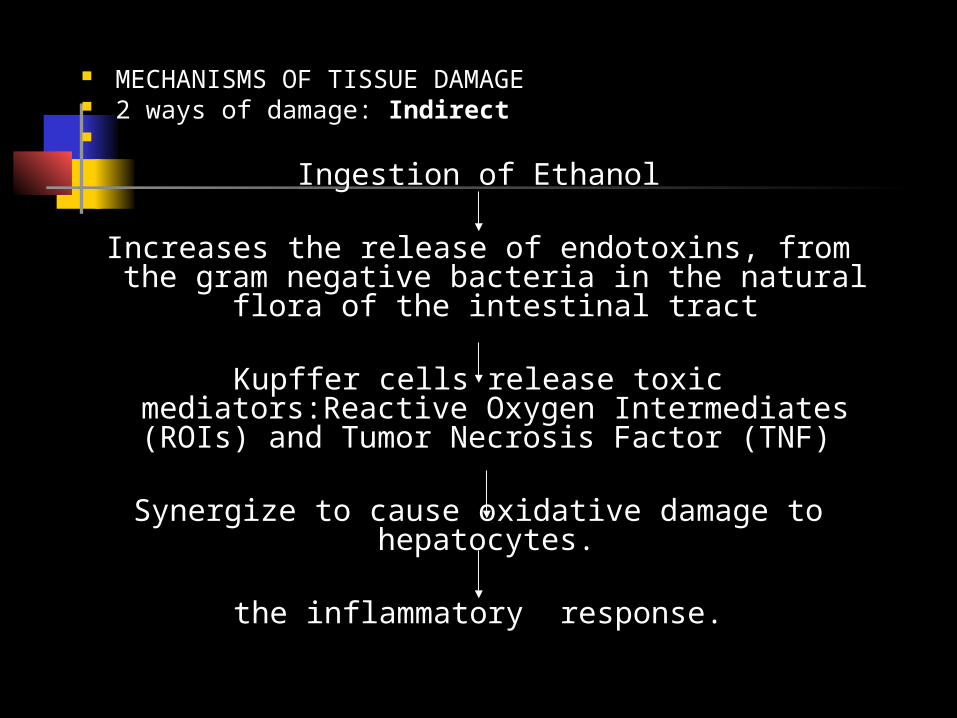
MECHANISMS OF TISSUE DAMAGE 2 ways of damage: Indirect
Ingestion of Ethanol
Increases the release of endotoxins, from the gram negative bacteria in the natural flora of
the intestinal tract
Kupffer cells release toxic mediators:Reactive Oxygen Intermediates (ROIs) and Tumor
Necrosis Factor (TNF)
Synergize to cause oxidative damage to hepatocytes.
the inflammatory response.

Injury on structures of the liver
A. Mitochondria Know as “megamitochondria” 25% of the patient with AAH. B. citokines. C. Kupfer Cells
Secretes high levels of: TNF-alpha. This is a strong factor for adherence and activation of the
leucocytes. IL-8- main mediator for neutrophils atraction
D. Alterations of the hepatocelular proteinAldehide and ethanol change conformation of the surface proteins.
In such way the immune system recognizes them as “Neoantigens
E. Fibrosis Irreversible
Occurs at only 10 – 15% of the alcoholics Due to activation of the Ito Cells (Fat store cells
or perisinusoids cells) that are at Disse Spece.Function: normally stores vitamyn A, But en
presence of Ethanol miofibrobñastic cells and Hipersecretes collagen fibrosis
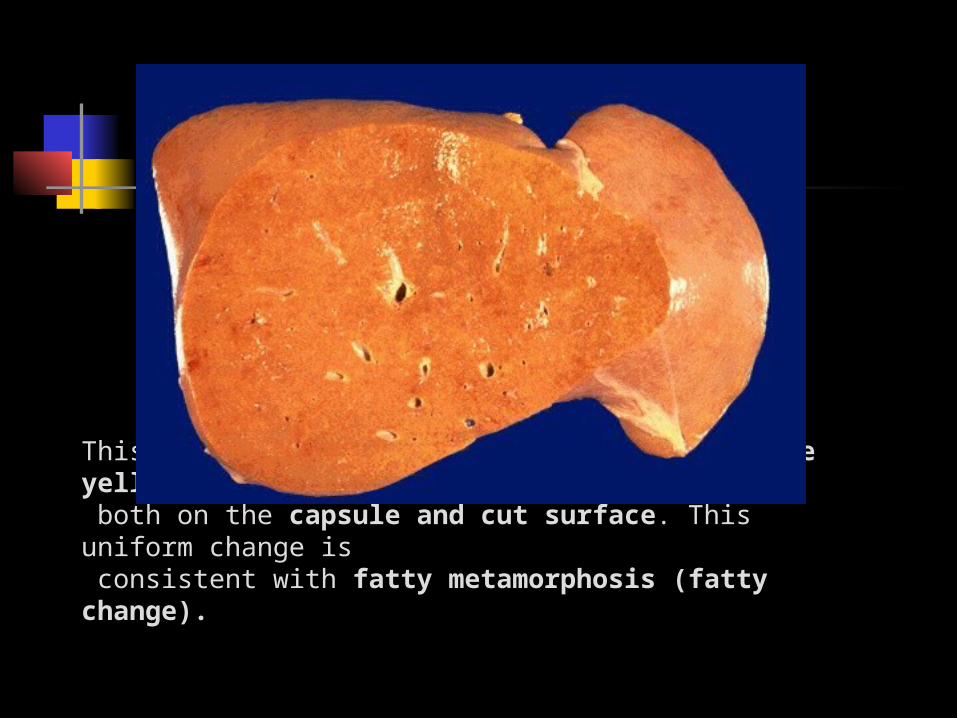
This liver is slightly enlarged and has a pale yellow appearance, seen both on the capsule and cut surface. This uniform change is consistent with fatty metamorphosis (fatty change).

Massive hepatomegaly in an elderly alcoholic; the liver weighed 2010 grams. Note the tinge of yellow.

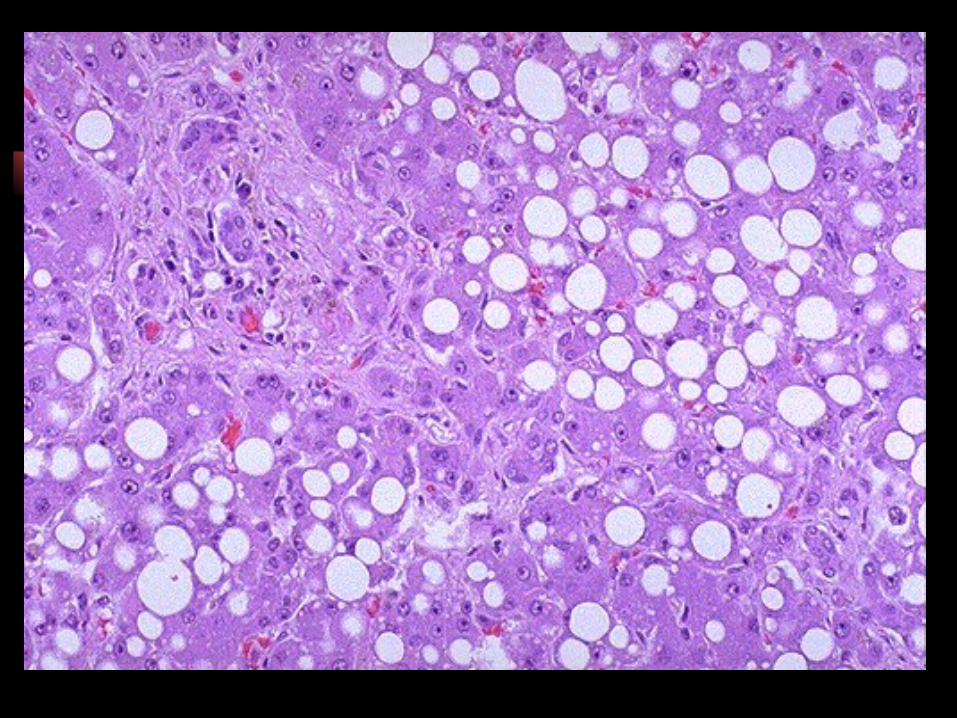
Micro
ballooning degeneration of hepatocytes, inflammation with neutrophils near mallory bodies Mallory bodies (abnormal perinuclear aggregations of cellular intermediate
filament proteins “citokeratin”).
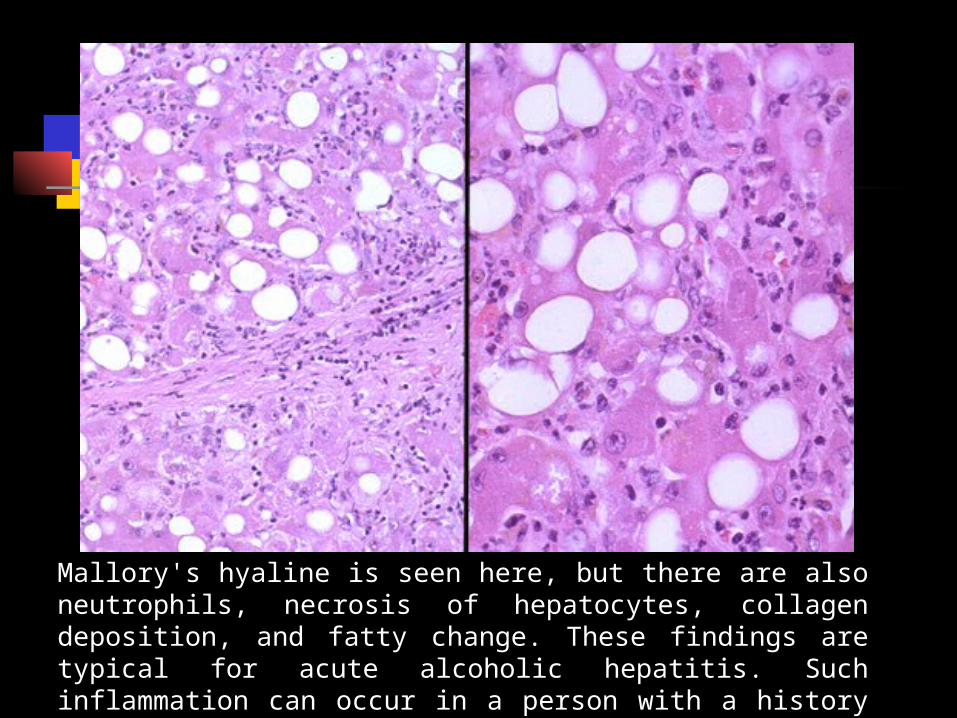
Mallory's hyaline is seen here, but there are also neutrophils, necrosis of hepatocytes, collagen deposition, and fatty change. These findings are typical for acute alcoholic hepatitis. Such inflammation can occur in a person with a history of alcoholism who goes on a drinking "binge" and consumes large quantities of alcohol over a short time.
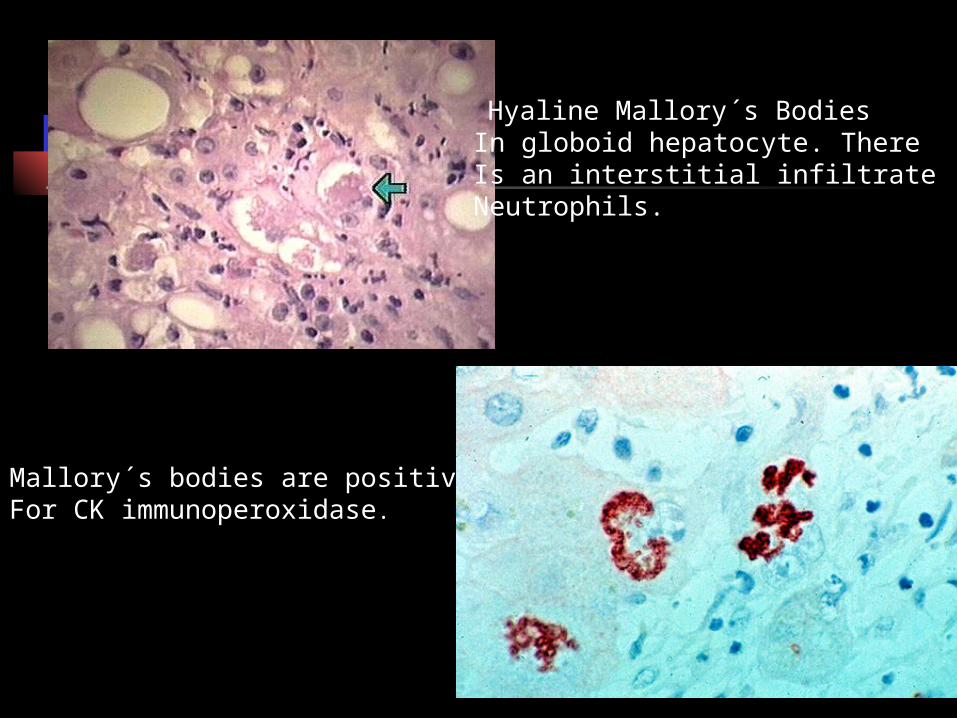
Hyaline Mallory´s Bodies In globoid hepatocyte. ThereIs an interstitial infiltrate ofNeutrophils.
Mallory´s bodies are positiveFor CK immunoperoxidase.
Clinical manifestations Vomiting Diarrhea Jaundice Psychological disturbances. Hepatic encephalopathy Ascites Bleeding esophageal Varices (varicose veins in the esophagus),
abnormal blood clotting and coma.

Main Reason for consulting:
Pathologically, it results in an enlarged liver
Painful to palpation. Enlargement is due to the accumulation
of fat and the swelling of liver cells, and to the accumulation of proteins that are normally secreted.
Lab AST to ALT ratio = 2:1 Alkaline Phosphatase elevated Gamma glutamyl transferase (GGT) Hypoalbuminemia
Management Alcohol Cessation Increased caloric and protein intake Vitamin supplementation
(Thiamine) Corticosteroids
Prognosis
Mortality 10-15% from acute hepatitis
Cirrhosis develops in 50% of alcoholic hepatitis Alcoholic liver disease
Immediate causes of death:* massive gastrointestinal* variceal haemorrhage* hepatic coma* infection* hepatorenal syndrome
Alcoholic Liver Disease.
The End.