dr.murat akyildiz, md associate professor of gastroenterology istanbul bilim university, department...
TRANSCRIPT
Dr.Murat AKYILDIZ, MDAssociate Professor of Gastroenterology
Istanbul Bilim University, Department of Gastroenterology,Sisli Florence Nightingale Hospital, Organ Transplantation Center, Istanbul
/
Recipient
Donor
Living Donor Liver Transplantation:Recipient and Donor Evaluation
Road map• Case presentation
• Recipient Evaluation– General information about
recipient evaluation– Cardiac– Pulmonary– Renal– Other spesific conditions
• Donor Evaluation
Case presantation-recipient
• 57 years-old woman,
• Referred to our center for liver transplantation since she had liver cirrhosis and chronic HCV infection
Medical History-1
• She had chronic HCV infection for 12 years • Regular interferon plus ribavirin treatment were given 12
months in 1999 and HCV RNA became negative after the tretment
• Three months later after the treatment, HCV RNA became positive and she was considered as recurrence of HCV infection
• Then she was followed up from hepatology outpatients clinic without antiviral treatment until 2002
• 2002– She had vomiting and fatigue – ALT 220– AST 200– T.BIL 1– HCV RNA 1.000.000 copy/ml– HCV genotype 1– USG: no mass, no splenomegaly, no ascites
Medical History-2
• PEG-INF+Ribavirin treatment were given for 2 years– HCV RNA was found 1000 copy/ml after 3 month of
the treatment– HCV RNA was negative 6-12 and 24 month of the
treatment– However, HCV RNA again became positive after 6
months of the treatment– Then she was followed up without any spesific
treatment from the outpatients clinic
Medical History-3
• 2010
– ascites developed and she was considered decompansated liver
cirrhosis
– furosemid 40 mgday and spironolactone 100 mg/day with salt
restriction were given.
– diuretics were increased up until furosemid 160 mg and
spironolactone 400 mg/day since she had tense ascites and
peripheral eodema.
– after ten months, diuretic therapies became unanswered and
therapeutic paracentesis were done.
Medical History-4
• Large volume paracenthesis was performed periodically (weekly/bimonthly),
• She had progressive dispne – No fever– physical examination with chest X-ray showed right hepatic hydrothorax.
• Thoracenthesis was performed – fluid was similar with ascites
• There was no tumor, infection and TBC lesion on thorax CT imaging.
• She begun to hospitalized with short time distances because of massive pleural effusion and respiratory distress and drainage with thorax tube.
Medical History-5
• Surgical History– 15 years ago gynecologic operation (exisional bx
from vulva)– No hepatobiliary operation
• Family History– No other liver disease– No genetic disease– Type 2 Diabetes Mellitus (older brother)
Medical History-6
• Habits: no alcohol and smoking and drug abuse
• Treatment– Furosemid 80 mg/day– Spironolactone 200 mg/day– Ursodeoxycolic acid 1000 mg/day– Norfloxacin 1x400 mg/day
Medical History-7
Physical Examination• Height 155 cm, Weight 59 kg, BMI 24.5• She was oriented, cooperation was normal,• She was subicteric and there was temporal muscle atrophy,
multiple spider angiomas, palmar erythema. • Blood pressure was 110/70 mmHg, heart rate 82/min/R, S1
and S2 were normal, no S3.• Respiratory sounds were decreased on the inferior and
middle zones of the right lung.• Abdomen: There was remarkable ascites around the 3 cm-
above umblical line, umblical hernia, Traube area was closed, 1 cm splenomegaly. There was (++) pretibial pitting edema
• No flapping tremor and other spesific findings
Laboratory
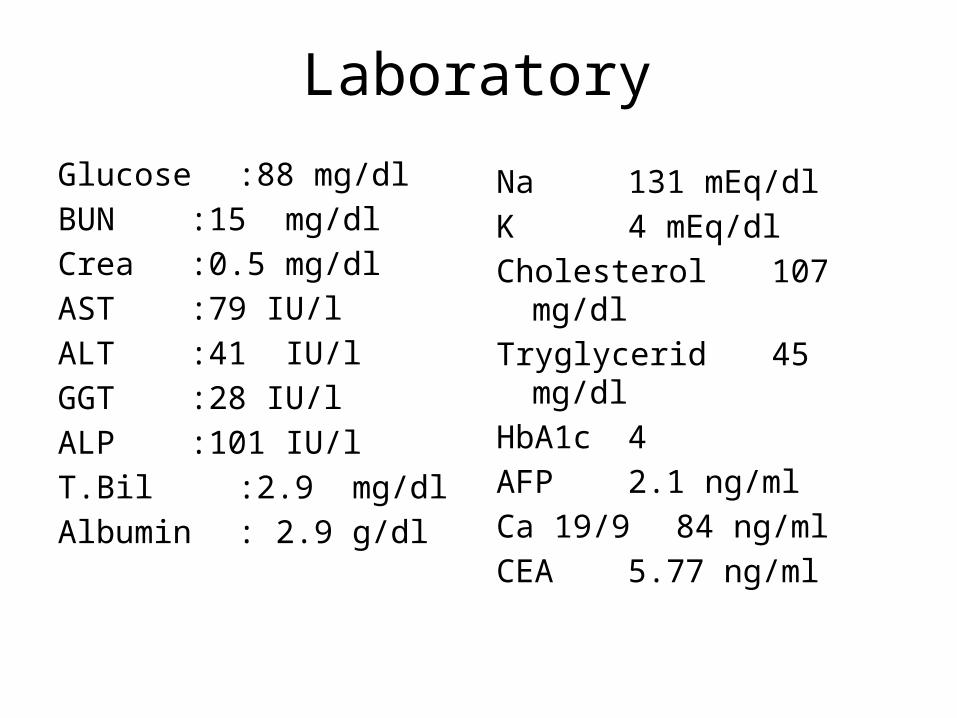
Glucose :88 mg/dlBUN :15 mg/dlCrea :0.5 mg/dlAST :79 IU/lALT :41 IU/lGGT :28 IU/lALP :101 IU/lT.Bil :2.9 mg/dlAlbumin : 2.9 g/dl
Na 131 mEq/dlK 4 mEq/dlCholesterol 107 mg/dlTryglycerid 45 mg/dlHbA1c 4AFP 2.1 ng/mlCa 19/9 84 ng/mlCEA 5.77 ng/ml
INR 1.52Hb 12 WBC 3300 PLT 88000 Blood type AB Rh(-)sT4 1.74TSH 2.15Ascites
SAAG>1.1WBC 100Culture was steril
HBs Ag (-)Anti-HBS (-)Anti-HBC IgG (+)AntiHAV IgG (+)HBV DNA (-)Anti-HCV (+)HCV-RNA:373.0000 Genotype: 1b
Laboratory
• Urinalysis: 2-3 wbc, no protein, no RBC
• Upper Endoscopy: no varices, portal hypertensive gastropathy
• Colonoscopy: internal hemoroid
Laboratory
Summary• 57 years old woman• Decompansated liver cirrhosis because of chronic HCV
infection• Refractory ascites • Hepatic hydrothorax• Child-Pugh B, score 9• MELD score 15• TX Indication:
– refractory ascites and hepatic hydrothorax– decompansated liver cirrhosis
Imaging• Thorax CT
– Bilateral pleural effusion– Atelectasia of the right lung– No active infltration or spesific lesion
• Abdomen CT+CT angiography– Liver cirrhosis– Portal hypertension– Ascites– No PVT
• Mamography– normal
Consultations• Cardiology
– Mild operational risk– EF: 63%– SPAP: 28 mmHg– Tal scannig: normal
• Infectious Disease– Rectal and urinary
cultures were normal.– No additional
recommendation
• Pulmonary – Moderate restrictive and
obstructive disease– Thoracentes fluid analysis
• similar with ascites– Albumin 0.3, LDH 61,
protein 0.6, WBC 200/mm3
• Transudative and culture was negative
• Gynecology– No spesific lesion and
smear was normal
Donor• 36 years-old, healthy woman, • Relationship: daughter of the recipient• Blood type AB Rh (+)• Height 160 cm• Weight 53 kg• BMI 21• Social status
– married, – has a 2 years old healthy child – she is house wife
Donor-2
• There was no pathology on phsysical examination
• No previous surgery• No habits• No drug using• No history of thrombosis• No previous systemic disease
Donor-3• BUN 11 mg/dl• Cr 0,4 mg/dl• Na 137 mEq/dl• K 4,4 mEq/dl• Gluc 93 mg/dl• HBA1C 4.6• HOMA-IR 2,17• Chol 185 mg/dl• Tg 82
• AST 15 IU/l• ALT 12 IU/l• ALP 83 IU/l• GGT 13 IU/l• T.Prot 8,2 g/dl• Albumin 5 g/dl• T. Bil 0,48 mg/dl• TSH 3.48• sT4 1.47• B-HCG <0.01
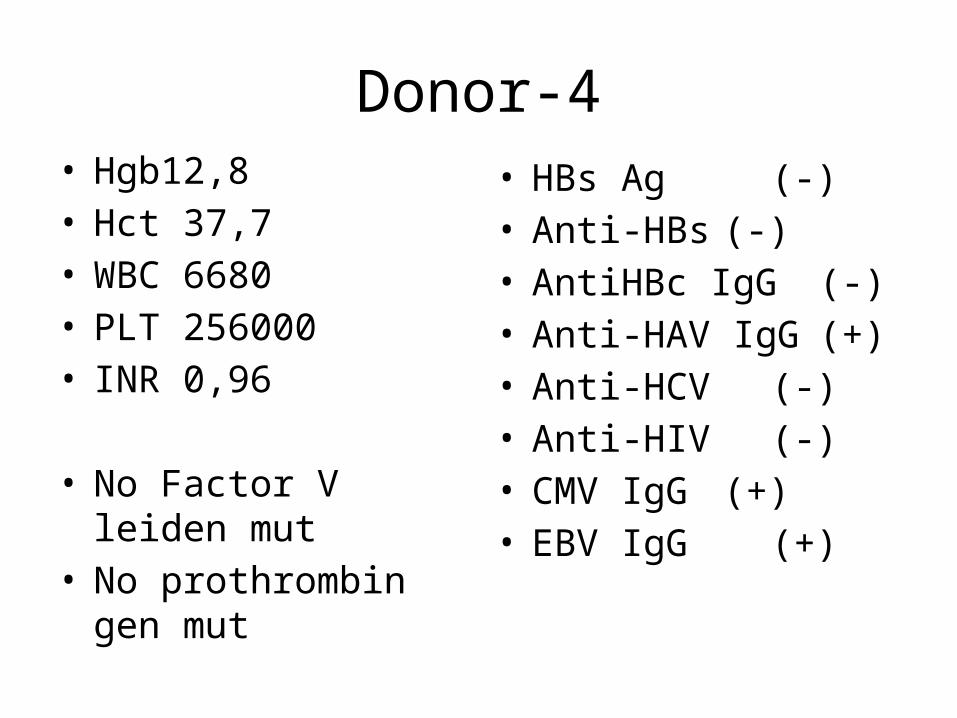
Donor-4• Hgb12,8• Hct 37,7• WBC 6680• PLT 256000• INR 0,96
• No Factor V leiden mut• No prothrombin gen
mut
• HBs Ag (-)• Anti-HBs (-)• AntiHBc IgG (-)• Anti-HAV IgG (+)• Anti-HCV (-)• Anti-HIV (-)• CMV IgG (+)• EBV IgG (+)
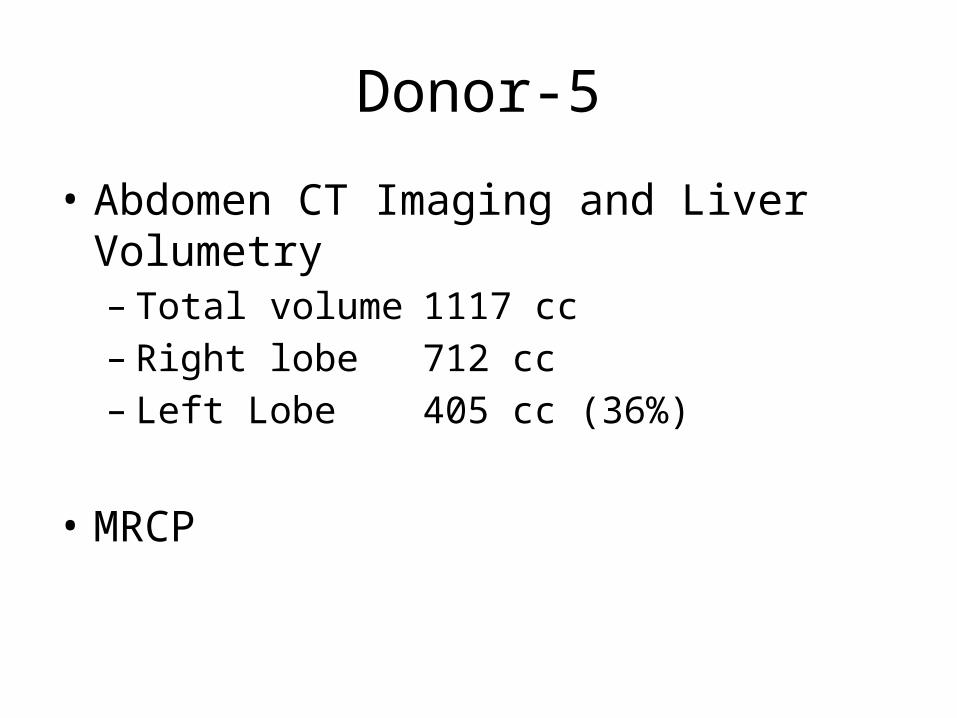
Donor-5
• Abdomen CT Imaging and Liver Volumetry– Total volume 1117 cc– Right lobe 712 cc– Left Lobe 405 cc (36%)
• MRCP
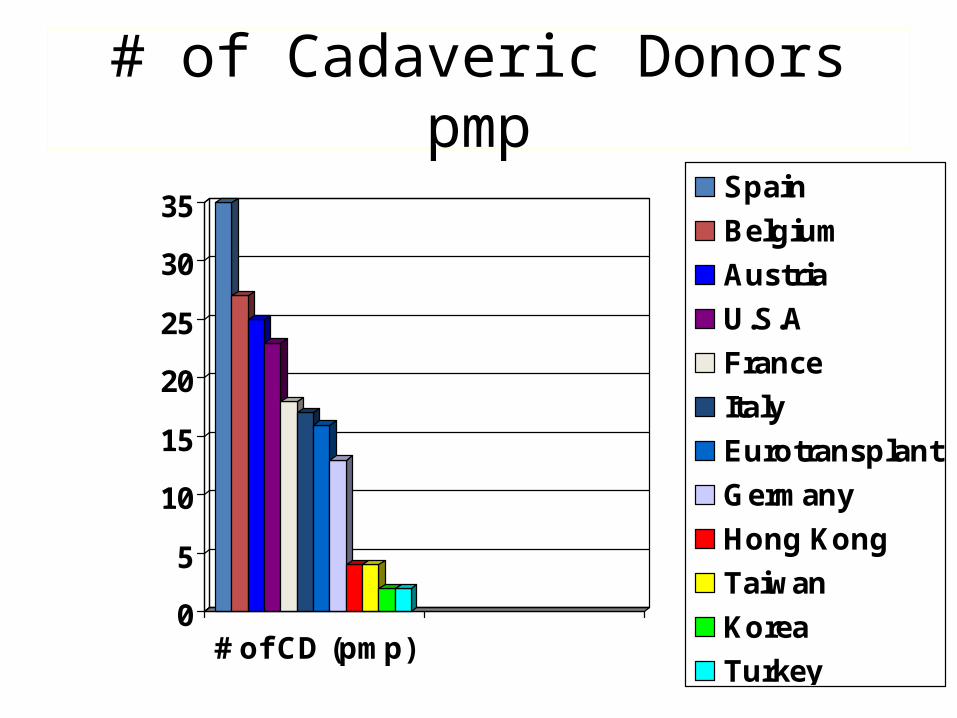
# of Cadaveric Donors pmp
0
5
10
15
20
25
30
35
# of CD (pmp)
Spain
Belgium
Austria
U.S.A
France
Italy
Eurotransplant
Germany
Hong Kong
Taiwan
Korea
Turkey
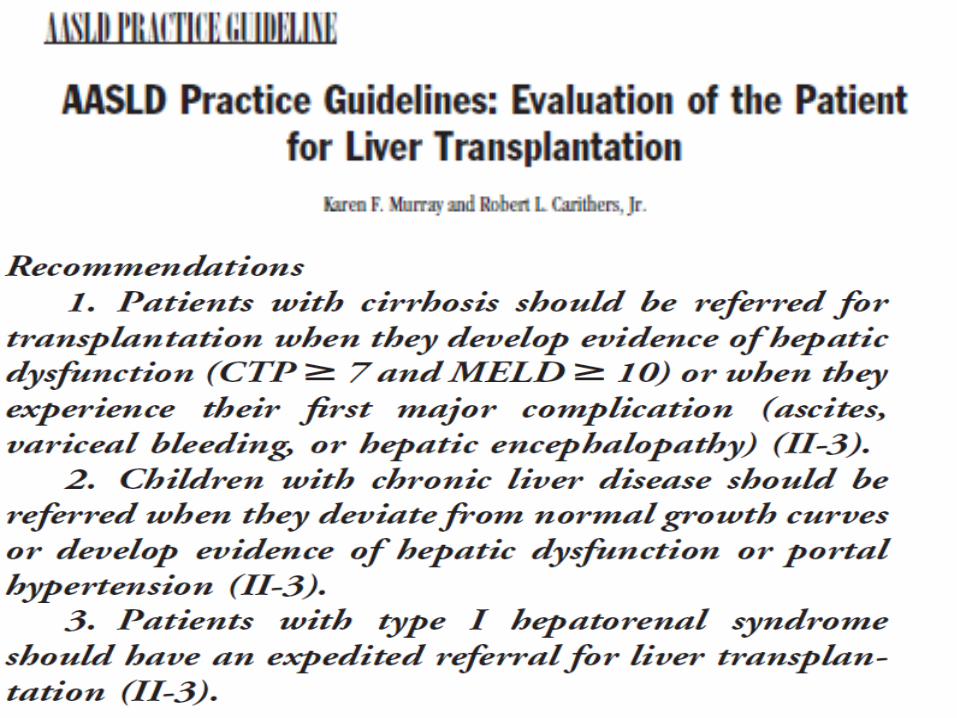
When and Who Should be Transplanted ?
• Acute liver failure
• Decompansated liver cirrhosis– Ascites– Encephalopathy– Icter– Esophageal variceal bleeding
• Systemic Complications of Liver Cirrhosis– Hepatopulmonary syndrome– Hepatorenal syndrome
• HCC
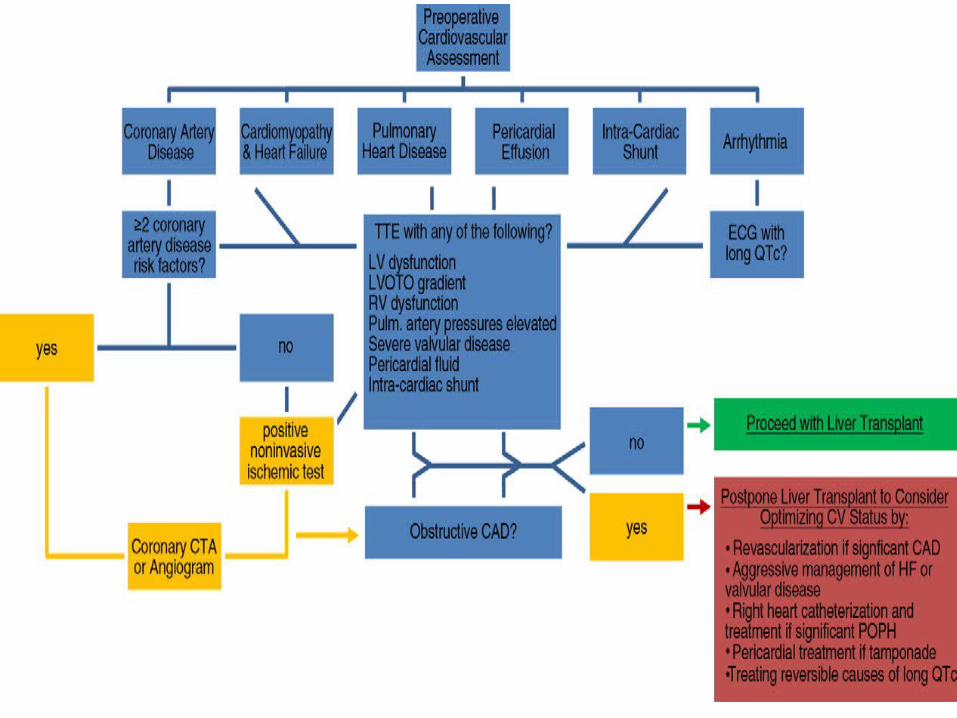
PREOPERATİVE ASSESMENT
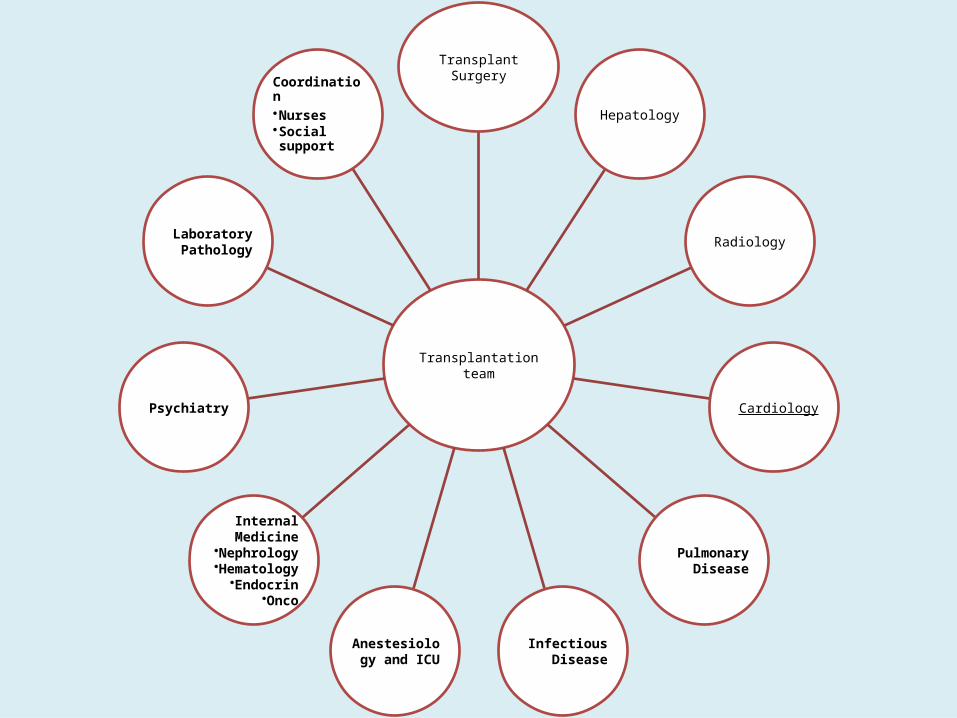
Transplantation team
Transplant Surgery
Hepatology
Radiology
Cardiology
Pulmonary Disease
Infectious Disease
Anestesiology and ICU
Internal Medicine
•Nephrology•Hematology
•Endocrin•Onco
Psychiatry
LaboratoryPathology
Coordination•Nurses•Social support
Evaluation of the recipients• A careful history and physical examination;
• Liver cirrhosis is a systemic disease • Cardiopulmonary assessment,
– Cardiac echocardiography, – pulmonary function tests, – Dobutamine stress testing, – cardiac catheterization in selected patients;
• Laboratory studies to confirm the etiology and severity of liver disease
• Creatinine clearance
Laboratory Studies-1• Biochemical analysis
– LFT
– RFT
– Alb/protein
– Tumor markers (AFP, Ca 19/9,..)
– Urinalysis-• urinary tract infection, proteinuria, hematuria,
Laboratory Studies-2• Laboratory studies to determine the status of
– current or previous hepatitis B virus (HBV), – hepatitis C virus, – Epstein-Barr virus, – cytomegalovirus, – human immunodeficiency virus (HIV) infections
Radiology• Abdominal imaging to determine
– hepatic artery – portal vein anatomy – presence of collaterals and shunts– presence of hepatocellular carcinoma (HCC).
• Doppler USG and CT angiography
• MRI should be performed, If creatinin level is not normal or history of hepatorenal syndrome or suspicion of HCC
Cardiac Evaluation-1 – Attention should be paid
• Over 50 years old• Male• Family history of CAD• Pre-TX diabetes• Alcoholic liver disease• Smoking• hyperlipidemia
– Echocardiography– Dobutamine stress test/dipyrimadole MPS– Angiography
Cardiac Evaluation-2 – Echocardiography
• EF• LV diastolic function• SPAP <45 no problem• SPAP 45-59 moderate PHT and over 60 mmHg is high
mortality right cardiac cateterization should be performed
– Patients who had severe PHT (SPAP>60 mmHg) is contraindication for LT since high perioperative mortality
– If the SPAP decreases after medical treatment with vasodilatator therapy, liver transplantation can be considered.
– PHT resolves within 4-6 months after LT and can be stopped.
Cardiac Evaluation-3– Most centers perform provacative tests since the
patients are too debilitated for exercise testing • Dobutamine stress test• Dipyridamole MPS
• In high risk patients coronary angiography– Risk of bleeding and renal failure!!!
• There is poor correlation between the tests and angiographic findings
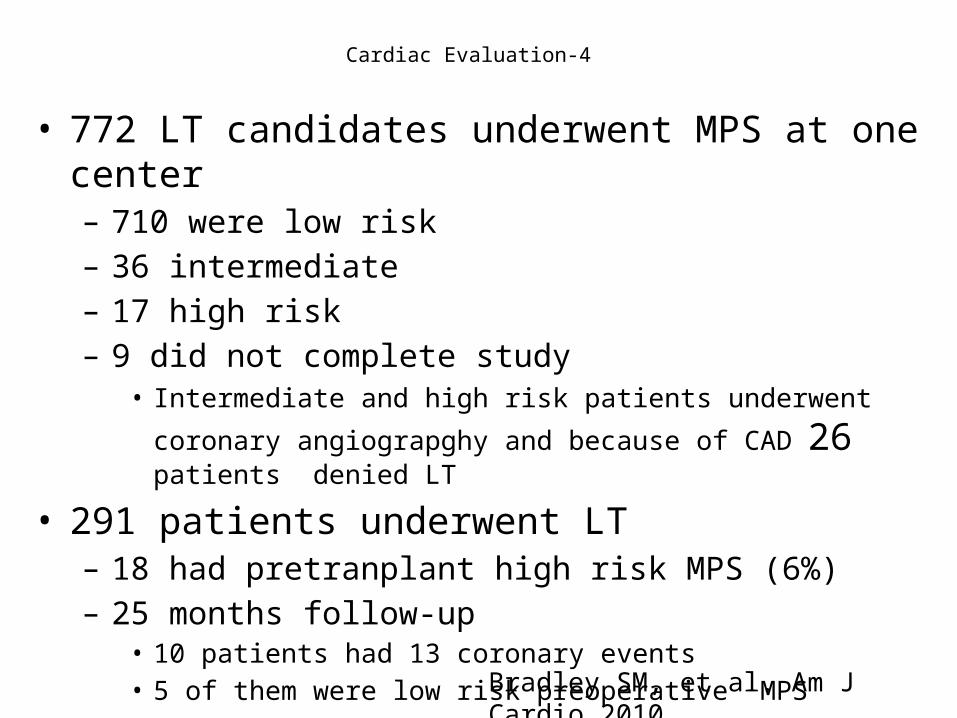
Cardiac Evaluation-4
• 772 LT candidates underwent MPS at one center– 710 were low risk– 36 intermediate– 17 high risk– 9 did not complete study
• Intermediate and high risk patients underwent coronary angiograpghy
and because of CAD 26 patients denied LT
• 291 patients underwent LT– 18 had pretranplant high risk MPS (6%)– 25 months follow-up
• 10 patients had 13 coronary events• 5 of them were low risk preoperative MPS
Bradley SM, et al. Am J Cardio 2010
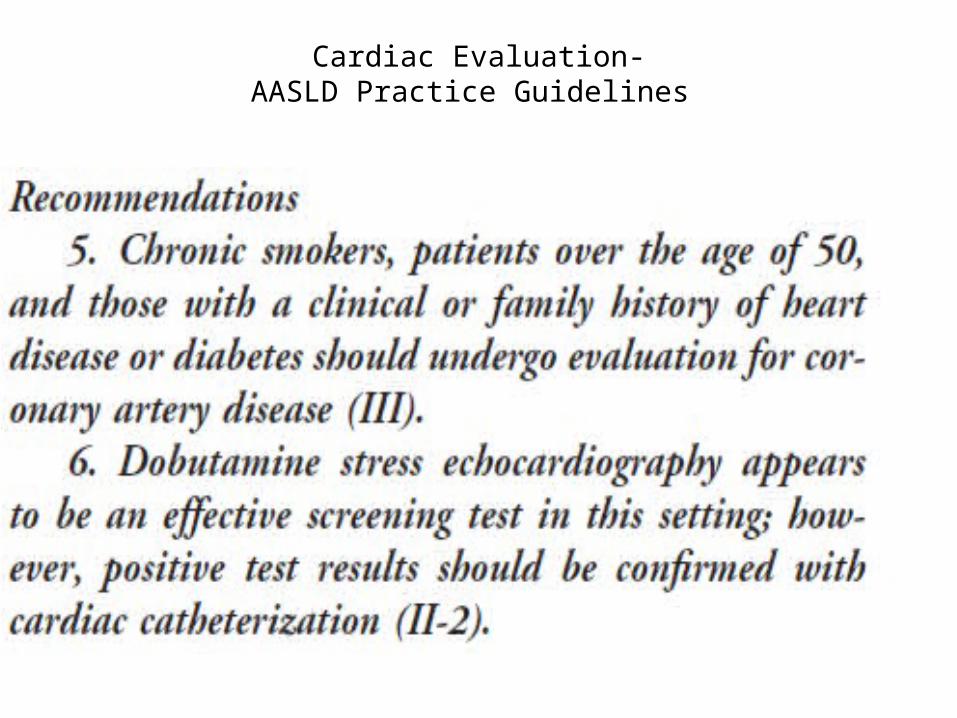
Cardiac Evaluation-AASLD Practice Guidelines
Pulmonary Evaluation• Pulmonary Evaluation
– X-ray– Pulse oxygen monitorization– Pulmonary function test– Thorax CT
• HCC• Smoking and family history of lung cancer
• Hepatopulmonary syndrome-– clubbing and hypoxemia –arterial ortostatic
deoxygenataion • PPHT
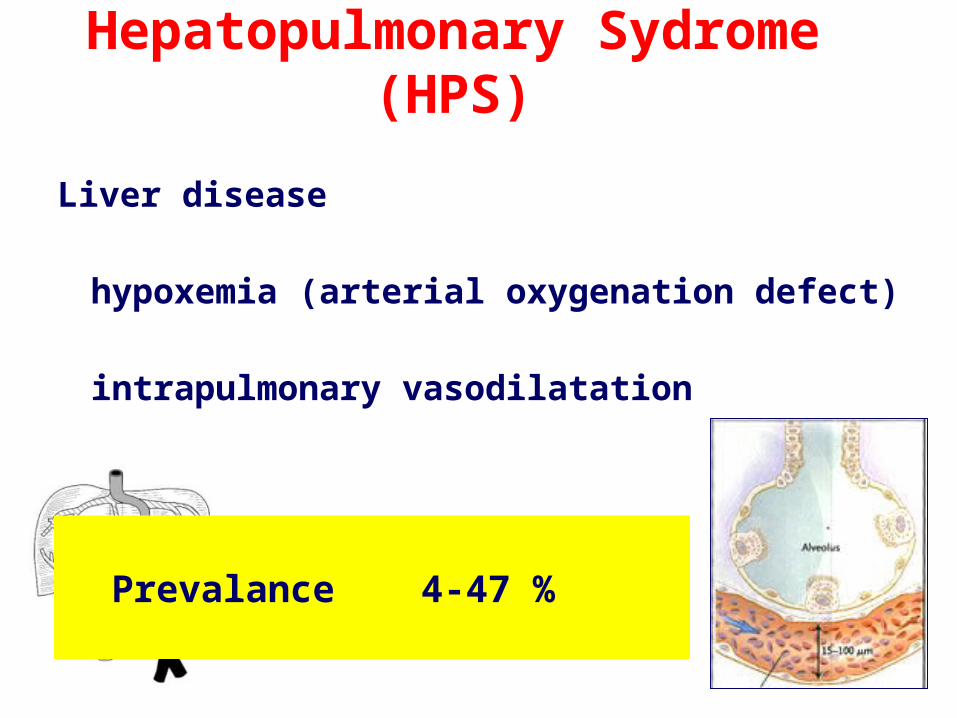
Hepatopulmonary Sydrome (HPS)
Liver disease
hypoxemia (arterial oxygenation defect)
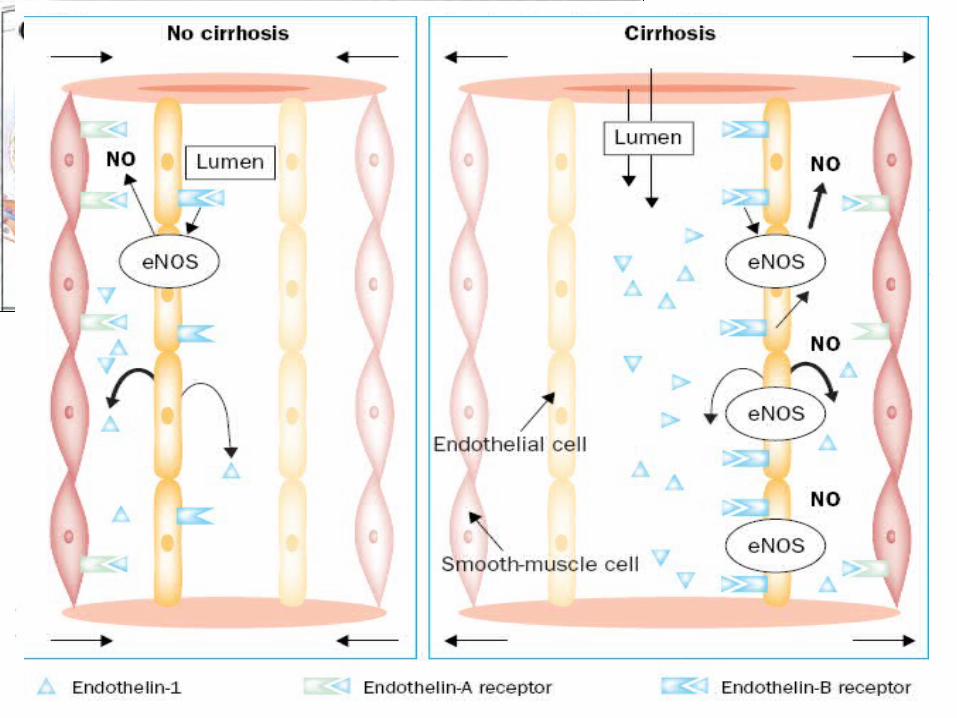
intrapulmonary vasodilatation
Prevalance 4-47 %

• Platipne
• Orthodeoksi
• hypoxemia during sleep
• siyanosis
• clubbing
• spider nevi
Clinic features
HPS-Diagnosis
• No biochemical marker Ø• Arterial blood gas analysis• Pulse oxymetry• Orto-deoxygenation test• TT ECHO• Scintigraphy• Pulmonary angiography
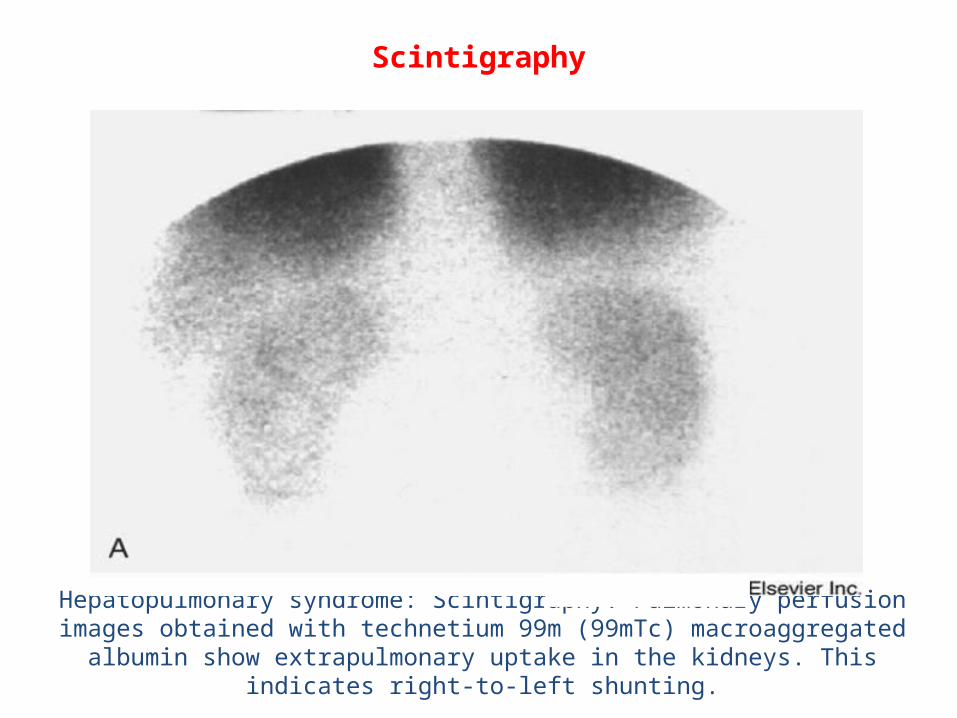
Scintigraphy
Hepatopulmonary syndrome: Scintigraphy. Pulmonary perfusion images obtained with technetium 99m (99mTc) macroaggregated albumin show extrapulmonary
uptake in the kidneys. This indicates right-to-left shunting.
1. Medical treatment
2. TIPS?
coil for large AVM
3. Liver TX
pO2 < 50 high risk
100% O2 and no improvement------poor prognosis
HPS-Treatment
metilen blue
NOS inhibitors
Almitrine bimesylate
anti-TNF
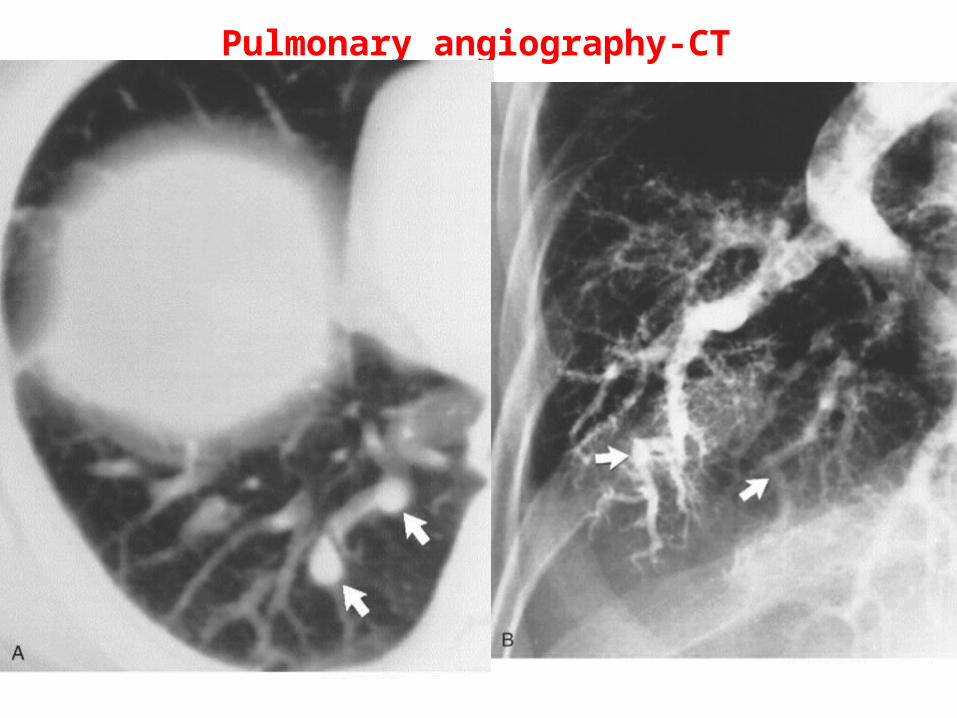
Pulmonary angiography-CT
PPHT• There should not be any primary cardiac and pulmonary disease and
– SPAP <45 mmHg --no problem– SPAP 45-59 mmHg-- moderate PHT – SPAP over 60 mmHg-- has high mortality and right cardiac
cateterization should be performedor
mean PAP >25 mmHg, at resting or 30 mmHg during exercise, increased pulmonary vasculare resistance PVR>240 dynes/s/cm)pulmonary arterial wedge pressure <15 mmHg .
– Patients who had severe PHT (SPAP>60 mmHg) is contraindication for LT since high perioperative mortality
– If the SPAP decreases after medical treatment with vasodilatator therapy, liver transplantation can be considered.
– PHT resolves within 4-6 months after LT and can be stopped.
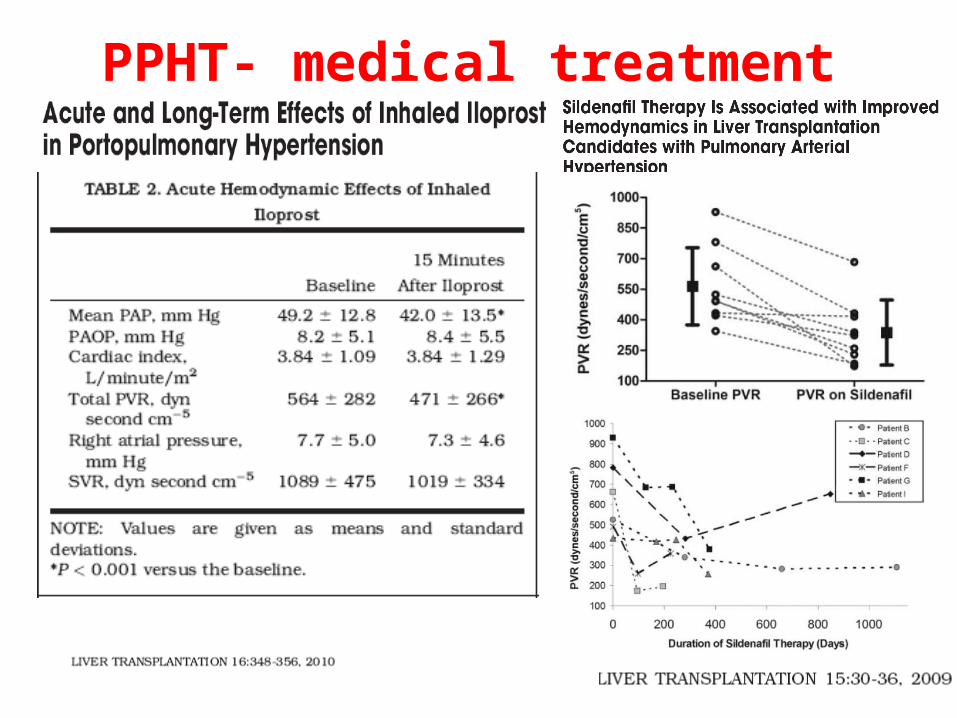
PPHT- medical treatment
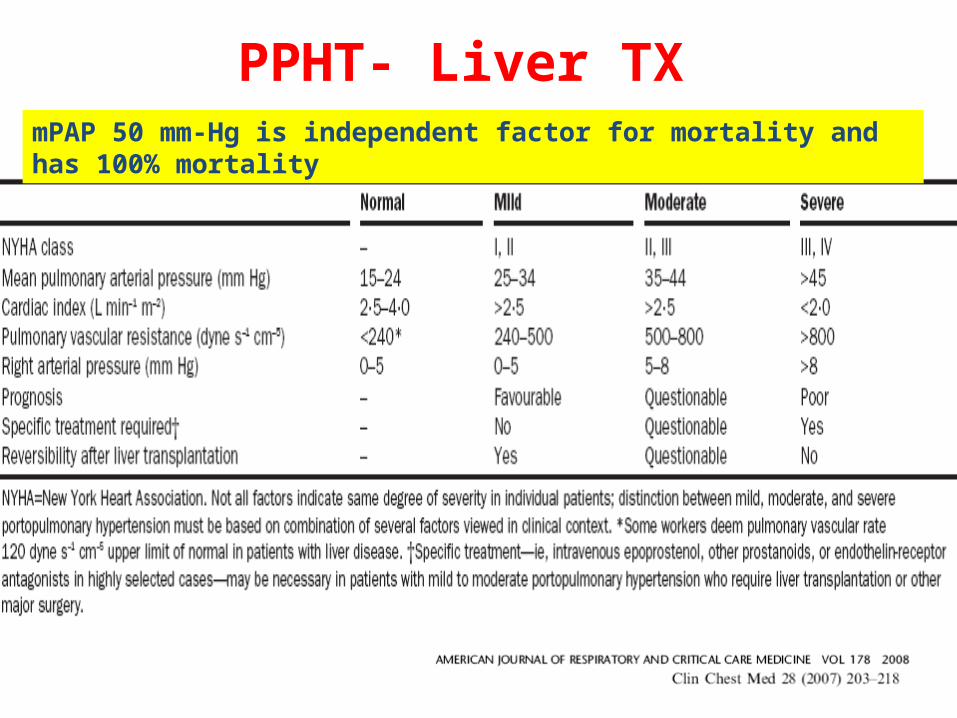
PPHT- Liver TXmPAP 50 mm-Hg is independent factor for mortality and has 100% mortality
Renal Functions
• Elevated serum creatinine level is an independent factor for RF and decreased survival after LT
• Patients preexisting primary renal disease has diminished survival and increased risk for posttransplant hemodialysis requirement
• Patients with chronic RF and liver disease should be considered for combined liver-kidney transplantation
• Hepatorenal syndrome that result in acute RF usually improves after LT
Murray KF and Carithers RL. Hepatology 2005
Renal Functions• In the presence of hepatorenal sydrome
– Albumin (1 g/kg/day) plus terlipressin– Stop diuretics– Avoid nephotoxic drugs– Stop propanolol – LT is the treatment choice and should be given high priority– Combined liver-kidney transplantation does not provide overall
results and should not be recommended for HRS.
• Preexisting renal disease– Nephrology consultation should be performed– Proteinuria, CrCl, baseline Cr level are important for
posttransplant period and survival– Combined liver-kidney transplantation
Recipient-screening• Screening
–Mamography–Colonoscopy
• Age• Family history of colon cancer• Primary sclerosing cholangitis• Ulcerative colitis
–Urology and Gynecology colsultations
Osteoporosis• It is a common complication of cirrhosis
– Postmenuoposal women– PBC– PSC– Auotimmune hapatitis that were given prolonged
steroids– Alcoholic patients
• Vitamin D and calcium support for osteopenic patients
• Bisphosphonates should be given carefully because of varices !!!!

Recipient with HCC
• Patients with HCC– Abdomen CT/MRI and angiography
– Thorax CT
– Bone scannig
– PET-CT ?
– AFP (higher than 400 ng/ml has poor prognosis)
Specific issues• Age
– There is no spesific age limitation– Older patients have lower long-term survival
• Obesity– Morbid obesity should be considered a contrindication for
LT– Patient with morbid obesity (BMI>40) and severe obesity
(BMI>35) has lower survival after LT– Bariatric surgery?
• Smoking– HAT is higher in chronic smokers– Increased malignancy and cardiac disease after LT
Disease Spesific Treatment-1• In patients with HBV
– Naïve patients• Entecavir• Tenofovir
– Under lamivudine therapy and DNA (-)• adding tenofovir at the posttransplant period
– Under LAM or entecavir and DNA (+) or viral breakthrough• Switch tenofovir or adding tenofovir on LAM or entecavir
• In decompansated HCV– If the patient has living donor, patient child B and well status
PEG-INF can be given with caution because of side effects and risk of progression of decompansation
– Child C patients, we do not give any spesific antiviral treatment
Recipient Evaluation-summary• Anamnesis and physical examination• Laboratory tests• Imaging• Preoperative treatment
– Renal functions, anti-viral treatment, diuretics, terlipressin plus albumin, lactulose, antibiotics, sildefanil, ….
• Consultations– Radiology: anotomy, mass, PVT, …– Cardiology– Pulmonary Evaluation– Infectious Disease– ICU and anestesiology– Gynecology/Urology– Psychiatric – Hematology/Nephrology/Endocrinology….
DONOR
EVALUATION
Living Donor-Step 1
• Age ->18, <50 years old
• Blood type and volunteering
• Interviewing for general information – should be lonely and without other relatives
– psychiatric evaluation should be performed • in the presence of suspicion of volunteering• suspicion of alcohol or drug abuse• psychiatric disease
• Anamnesis and physical examination– BMI– Systemic disease– Hepatobiliary disease– Thrombophila
Living Donor-Step-2
• Biochemical analysis– Liver FT– Renal FT– Fasting glucose– Lipid profiles– TSH– sT4– Protein electrophoresis– Seruloplasmin– Urinalysis– HOMA score– OGTT– HbA1c
• Hemogram• INR
• Serology– HBsAg– AntiHBC total– AntiHBs– AntiHAV IgG– Anti-HCV– Anti-HIV– VDRL
Living Donor-Step-2
• Hereditary tests for thrombosis– Factor V leiden mutation
– Protrombin gene mutation
• If the recipient has Wilson disease– 24 hour urinary copper– eye examination
• Autoimmune Tests– If the recipient disease is
autoimmune liver disease
• ANA• AMA• ASMA• LKM• SLA• HLA?

Living Donor-Step-3• Anotomical assessment
– Abdomen CT and CT angiography• GBWR should be 0.8 (lower limit 0.7, <0.7 SFSS)• Remnant volume should be 35%,
– sometimes could be 30% according to age and MHV satus
• Steatosis should be <10%• PV anotomy• HV anotomy
– MRCP
Living Donor-Step-4• Liver Bx
– BMI>28– Hyperlipidemia– >10 steatosis on CT evaluation– antiHBC (+) donors– metabolic or autoimmune liver disease
diagnosis of the recipient and primary relationship
Living Donation and Steatosis• Most patients has insulin resistance and
overweight• Exercise and dietetian consultation• Metformin• Omega-3 fish oil• Hyperlipidemia should be corrected• Donor who should not weight loss in 4-8
weeks probably unwillingness !!!
Living Donor-Consultations
– Phsychiatry
– Pulmonary
– Cardiology-
Living Donor-Step-5
weekly meeting of liver transplantation unit
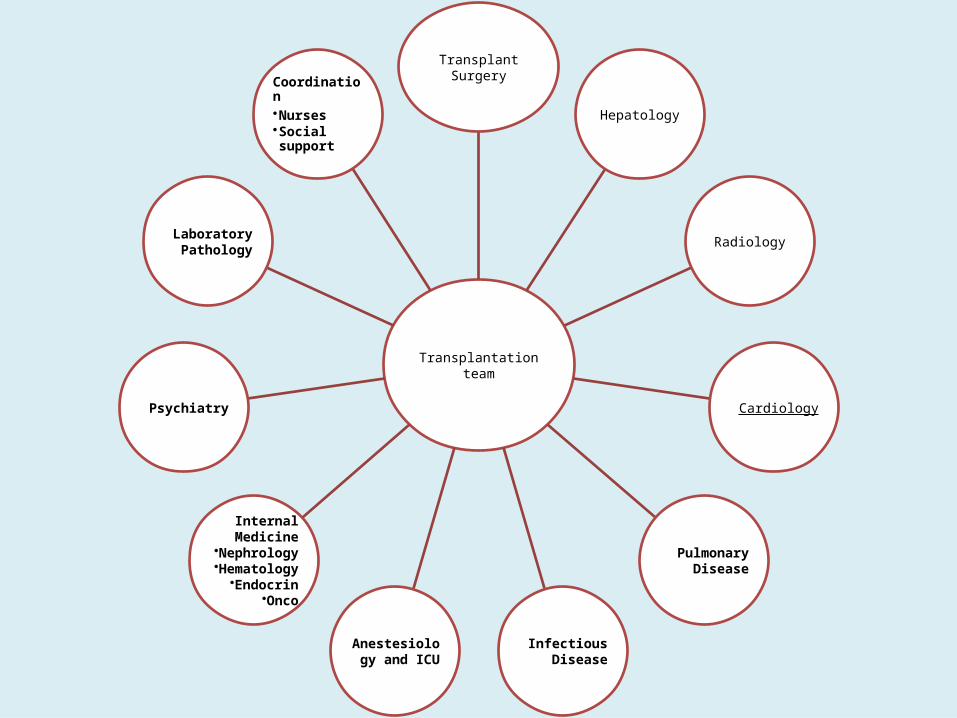
Transplantation team
Transplant Surgery
Hepatology
Radiology
Cardiology
Pulmonary Disease
Infectious Disease
Anestesiology and ICU
Internal Medicine
•Nephrology•Hematology
•Endocrin•Onco
Psychiatry
LaboratoryPathology
Coordination•Nurses•Social support
