dr brandon orr-walker - gp cme north/sat_plenary_1215_orr... · 2018-06-09 · side effects: glp-1...
TRANSCRIPT

Dr Brandon Orr-WalkerEndocrinologist
Clinical Head of Endocrinology and Diabetes
Middlemore
Auckland
12:15 - 12:40 What Can New Agents Offer Us?

Diabetes Management
What do the new agents offer us ?
Brandon Orr-Walker
June 2018

Outline
• Basic Premises and Assumptions
• Identifying the Opportunities
• Current state
• New treatment options, what new treatment options?

Basic Premises and Assumptions• Only worth making the diagnosis if we are going to change the progression of
disease
• Strong evidence base to reduce harm:
• Glycaemia
• BP
• Renal protection
• CVD risk
• Multifactorial management
• Early good control pays long term dividends
• We have people with diabetes at high risk of complications, and disparities exist
• Since 2003 majority of care for people with T2DM is to be in primary care
• Expertise in management is required to manage therapeutic challenge

Adapted from Stratton IM et al. on behalf of the UK Prospective Diabetes Study Group. BMJ 2000; 321:405–412.

Figure 5:DCCT-EDIC: Long-term Risk of Macrovascular
Complications
Years Since Entry*
DCCTEnd of
Randomized Treatment
*Diabetes Control and Complications Trial (DCCT) ended and Epidemiology of Diabetes Interventions and Complications (EDIC) began in year 10 (1993). Mean follow-up: 17 years.
EDICYear 1
EDICYear 7
12%
10%
8%
6%
Hem
oglo
bin
A1C
0.00
0.02
0.04
0.06
0.08
0.10
0.12
Conventional
Cum
ula
tive I
ncid
ence
Any Cardiovascular Outcome
P < 0.001 P < 0.001 P = 0.61
0 2 4 6 8 10
12
14
16
18
20
Conventional
Intensive 42% risk reduction P = 0.02
Intensive
DCCT/EDIC Research Group. JAMA. 2002;287:2563-2569. Copyright © 2002 American Medical Association. All rights reserved. | Nathan DM, et al. N Engl J Med. 2005;353:2643-2653. Copyright © 2005 Massachusetts Medical Society. All rights reserved.

IncreasedHepatic Glucose Production
Impaired Insulin Secretion
Hyperglycemia
Decreased GlucoseUptake
TZDsGLP-1 analoguesDPP-4 inhibitorsSulfonylureas Thiazolidinediones
Metformin
MetforminThiazolidinediones
_
Pathophysiologic Approach to Treatment of T2DM
DeFronzo RA. Diabetes. 2009;58:773-795.


Are we at goal?
Currently in CMDHB:
• Approximately 40,000 patients with diabetes
• 20% of patients with diabetes have HBA1c >= 75 mmol/mol
– 8316 patients (CPHAC minutes 20/01/16)
– (nationally 28% >= 64, Australia 22% >= 64)
– Growing faster than the denominator (10% over 2 years)
– Less than ½ as likely to be referred /seen in secondary care diabetes clinics than ADHB/WDHB (only 14%)
• Spending an additional $7 Million on retinal laser and Avastin
– Less than 20% patients commencing laser are referred to specialist diabetes teams in year prior or year after to help with diabetes care.

Clinical Inertia: Failure to advance therapy when recommended
Brown JB et al. Diabetes Care 2004; 27(7): 1535–40.

Treatment Inertia= clinical inertia
Two components:
• Clinician inertia
• Patient inertia– Lack of access– Health literacy– Non-adherence– Competing interests– Refusal of treatment
• Uninformed/misinformed• Well informed
– Lack of acceptable treatment options
– Many of the “patient inertia” factors can be clinician modified, and as healthcare professionals it is our role to do so to the best of our ability.

What does this have to do with diabetes?
Presentation title Date 12

What does this have to do with diabetes? Nothing!
Presentation title Date 13

Treatment options in clinical inertia
Two components:
• Clinician inertia • Patient inertia
– Lack of access– Health literacy– Non-adherence– Competing interests– Refusal of treatment
• Uninformed/misinformed• Well informed
– Lack of acceptable treatment options
– Many of the “patient inertia” factors can be clinician modified, and as healthcare professionals it is our role to do so to the best of our ability.
Acceptability of Treatment Options
Patient (acceptability)• Side effects• Misconceptions• Belief• Experience of success ( especially for uptitration)• Response of health care team
Healthcare team• Resource• Competency• Belief• Promotion
Treatment options per se• Funding• Advantages beyond “targeted indication” (external gains)• Cost


Management of glycaemic control (NZ)
Lifestyle modification
Food, physical activity and behavioural strategies
If measured HbA1c does not meet or closely approach agreed target within 3 months, or if patient is symptomatic, drug therapy should be considered
Gastrointestinal tolerance may be improved by gradual introduction Stop if eGFR <30 ml/min/1.73m2
Metformin
Educate the person on the possibility of hypoglycaemia
Sulphonylurea
First line drug therapy
Review medication adherence and dose optimisation
Acarbose therapy1
If metformin not tolerated or contraindicated
Second line drug therapy
If no congestive heart failureIf at significant risk of hypoglycaemiaConsider increased risk of fracture in women
Thiazolidinedione (pioglitazone)2, 3
If above target (HbA1c 50-55 mmol/mol [6.7 – 7.2%] or as individually agreed)
If above target >3 months
Sulphonylurea
Third line drug therapy
Insulin4
If above target >3 months
Guidance on the Management of Type 2 Diabetes 2011; available online at www.nzgg.org.nz
If above target
Review medication adherence and dose optimisation
Review medication adherence and dose optimisation

Presentation title Date 18

Presentation title Date 19

ADA 2018 Standards of Care
Presentation title Date 20

Presentation title Date 21

Psycho-
Bio-
-social
Patient-centred care
Individualising HbA1c goals
Inzucchi et al. Diabetes Care 2012;35:1364–79

Presentation title Date 23

CCM: Big Effort, Big Variation

• Incretin Pathway
• SGLT2 inhibitors
Newer agents
Presentation title Date 25

No new DKD-specific treatment in the last 15 years
26
1980 1990 2010 20152000
No new DKD-specific treatment in the last 15 years
High blood pressure
identified as DKD risk
factor
ß-blockers1
Hydralazine2
Captopril3
T1D
IDNT4, IRMA 25
IrbesartanT2D
RENAAL6
LosartanT2D
RAAS blockade

0
10
20
30
40
50
Brenner BM, et al. N Engl J Med. 2001;345(12):861-869.©2001 Massachusetts Medical Society. All rights reserved.
†In combination with open-label diuretic, calcium channel blocker, beta-blocker, alpha-blocker, and/or centrally acting agent
*doubling of serum creatinine, end stage renal disease, death
RENAAL Patients Reaching the Primary Composite Endpoint*
Cu
mu
lati
ve %
of
pati
en
ts w
ith
even
t
Months
240 12 36 48
554
583
Placebo
Losartan
Risk reduction=16%
P=0.02
762
751
689
692
295
329
36
52
Placebo† (n)
Losartan† (n)
www.hypertensiononline.org

RENAAL

RENAAL First Hospitalization for Heart Failure
0 12 24 36 48
Months
0
5
10
15
20
% o
f p
ati
en
ts
wit
h e
ven
t
32% Risk reductionP=0.005
Placebo* (n)
Losartan* (n)
762 685 616 375 53
751 701 637 388 74
Brenner BM, et al. N Engl J Med. 2001;345(12):861-869.©2001 Massachusetts Medical Society. All rights reserved.
www.hypertensiononline.org
*In combination with open-label diuretic, calcium channel blocker, beta-blocker, alpha-blocker, and/or centrally acting agent

Gila Monster Salivary product is GLP-1 agonist

Incretins Physiologically Regulate Insulin and Glucagon in a Glucose-dependent Manner
Physiologic
glucose
control
Ingestion
of Food
Active
GLP-1 & GIP
Release of
Incretin Gut
Hormones
GI tract
Glucose
uptake and
storage by
muscles and
other tissues
Glucose
output from
the liverGlucagon
from α-cells
(GLP-1)Glucose Dependent
Glucose Dependent
Insulin from β-cells
(GLP-1 and GIP)
Pancreas
α-cells
β-cells
Adapted from Kieffer TJ, Habener JF. Endocrine Reviews. 1999;20:876–913.; Ahrén B. Curr Diabetes Report. 2003;2:365-372. ; Drucker
DJ. Diabetes Care. 2003;26:2929-2940.; Holst JJ. Diabetes Metab Res Rev. 2002;18:430-441.; Drucker DJ. Expert Opin Investig Drugs.
2003;12:87-100.; Ahrén B et al. Horm Metab Res. 2004;36:867-876.

Insulin secretion
β-cell neogenesis
β-cell apoptosis
Glucagon secretionGlucose production
Heart
GI Tract
Liver
MuscleDrucker DJ. Cell Metab. 2006;3:153-165.
BrainAppetite
Cardioprotection
Cardiac output
StomachGastric emptying
Neuroprotection
Glucose Uptake
_
+
Stomach
GLP-1
GLP-1 Actions in Peripheral Tissue

Levels of Active Incretins GLP-1 and GIP Are Increased by DPP-4 Inhibition
*Refers to amino acid number. Deacon CF et al. Diabetes. 1995;44:1126–1131.
Meal
Intestinal
GIP and
GLP-1
release
GIP and GLP-1
Actions
DPP-4
Enzyme
GIP-(1-42*)
GLP-1(7-36)*
Active
GIP-(3-42)*
GLP-1(9-36)*
Inactive
Rapid
InactivationX
DPP-4
Inhibitor

Side Effects: GLP-1 Receptor Agonists and DPP-4 Inhibitors
GLP-1 Receptor Agonists DPP-4 Inhibitors
Side effects Gastrointestinal Well tolerated
Weight> 85% patients
lose weightWeight neutral
AdministrationTwice-daily
injectionOral, once daily
Other cardiac risk factors
↓ Triglycerides
↑ HDL
↓ Blood pressure
Unknown
Davidson JA. Cleve Clin J Med. 2009;76(suppl5):S28-S38.

Presentation title Date 35
Schnabel CA, et al. Vasc Health Risk Manag. 2006;2:69-77.
GLP-1 Receptor Agonists
• First-in-class (exenatide) approved in 2005
• Augment insulin secretion
• Inhibit glucagon secretion
• Lower fasting glucose and improve postprandial glucose profile

Exenatide Sustained A1c Reductions Over 82 Weeks
82-wk completer, N = 314; 82-wk ITT, N = 551; Mean ±SE.
Time (week)
Placebo-controlled Open-label extension
0 10 20 30 40 50 60 70 80 90-1.5
-1.0
-0.5
0.0
-1.1% ± 0.1%
-0.8% ± 0.1%
Ch
an
ge i
n A
1c (
%)
(All patients 10 mg BID)
8.3%8.4%
Mean Baseline A1c
82-Week ITT82-Week Completer
Blonde L, et al. Diabetes Obes Metab. 2006;8:436-447.
Blonde L, et al. Diabetes Obes Metab. 2006;8:436-447.

Blonde L, et al. Diabetes Obes Metab. 2006;8:436-447.
Durability of Exenatide: Weight
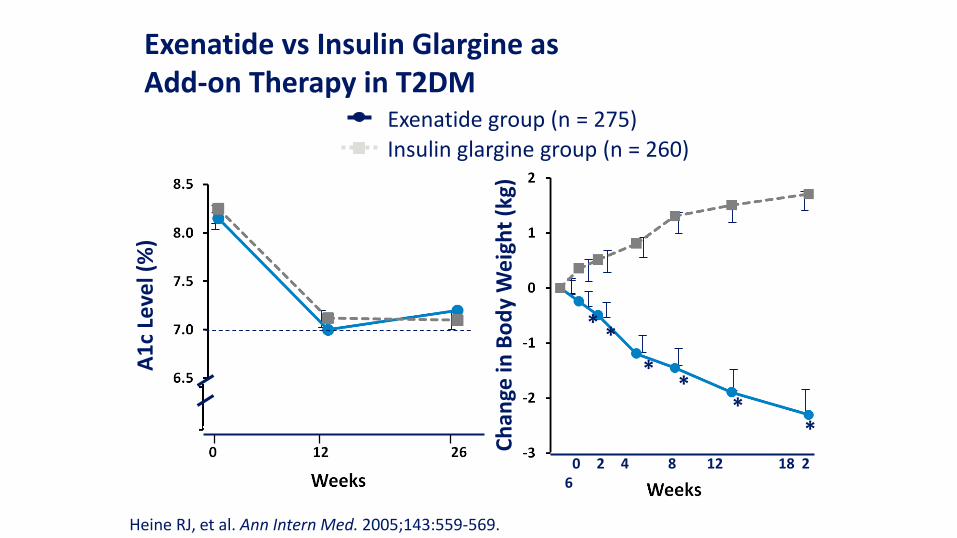
Exenatide vs Insulin Glargine as Add-on Therapy in T2DM
A1
c Le
vel (
%)
**
**
**
0 2 4 8 12 18 26
Ch
ange
in B
od
y W
eig
ht
(kg)
Heine RJ, et al. Ann Intern Med. 2005;143:559-569.
Exenatide group (n = 275)
Insulin glargine group (n = 260)

Effects of GLP-1 Agonists on Cardiovascular Risk Factors
• A subset achieved 3.5 years of exenatide exposure and had serum lipids available for analysis (n = 151)
• Triglycerides decreased 12% (P = .0003)
• Total cholesterol decreased 5% (P = .0007)
• LDL-C decreased 6% (P < .0001)
• HDL-C increased 24% (P < .0001)
Klonoff DC, et al. Curr Med Res Opin. 2008;24:275-286.
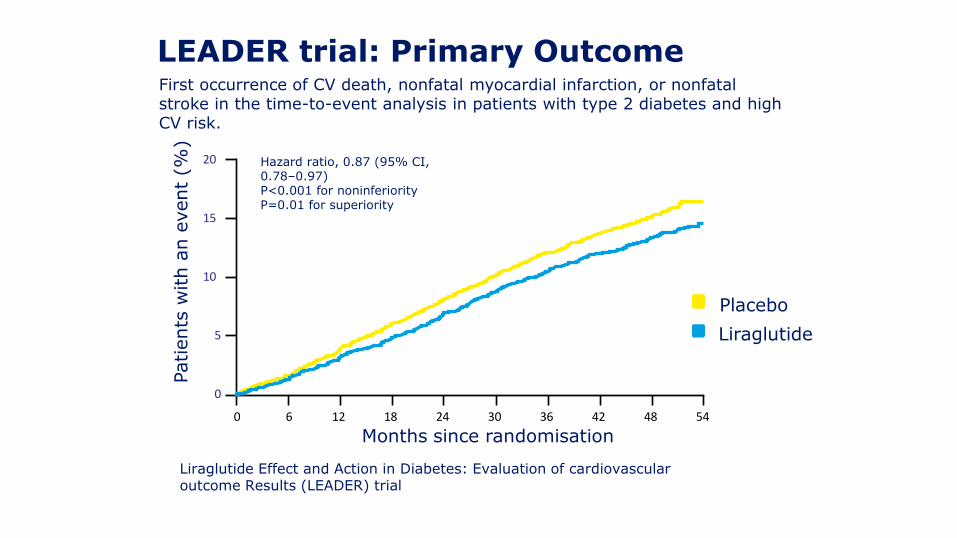
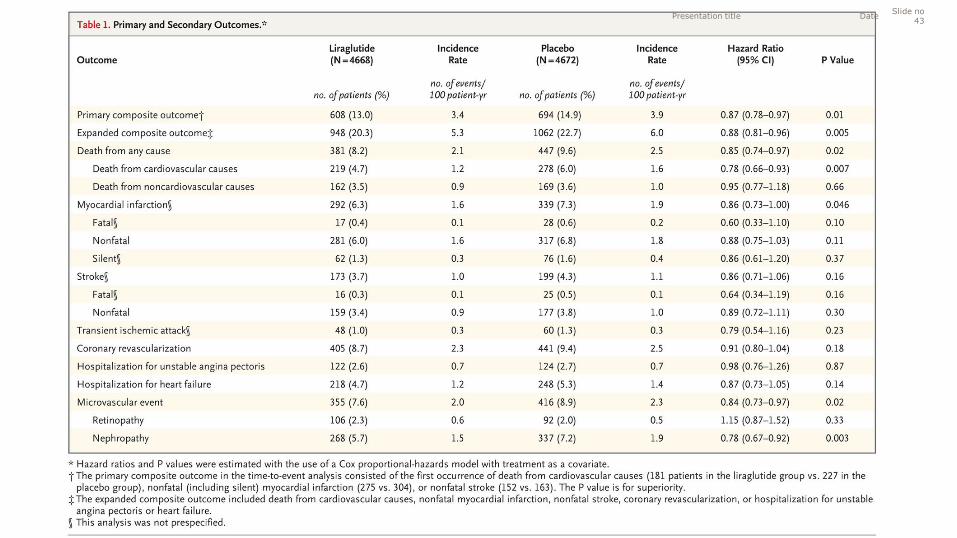
LEADER trial: Primary Outcome
15
10
20
5
0
0 6 12 18 24 30 36 42 48 54
Placebo
Liraglutide
Patients
with a
n e
vent
(%)
Months since randomisation
Hazard ratio, 0.87 (95% CI, 0.78–0.97)P<0.001 for noninferiorityP=0.01 for superiority
First occurrence of CV death, nonfatal myocardial infarction, or nonfatal stroke in the time-to-event analysis in patients with type 2 diabetes and high CV risk.
Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results (LEADER) trial
Adapted from: Marso SP et al., NEJM 2016

LEADER trial:
Death from Cardiovascular Causes
15
10
20
5
0
0 6 12 18 24 30 36 42 48 54
Placebo
Liraglutide
Patients
with a
n e
vent
(%)
Months since randomisation
Hazard ratio, 0.78 (95% CI, 0.66–0.93)P=0.007
Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results (LEADER) trial
Adapted from: Marso SP et al., NEJM 2016
Presentation titleSlide no
43Date

No new DKD-specific treatment in the last 15 years: SGLT2 inhibition
44
IDNT, Irbesartan Type 2 Diabetic Nephropathy Trial; RAAS, renin–angiotensin-aldosterone system; RENAAL, Reduction of
Endpoints in NIDDM with the Angiotensin II Antagonist Losartan.1. Mogensen CE et al. Br Med J (Clin Res Ed)1982;285:685; 2. Parving HH
et al. Lancet 1983;1:1175 3. Lewis EJ et al. N Engl J Med 1993;329:1456; 4. Lewis EJ et al. N Engl J
Med 2001;345:851; 5. Brenner BM et al. N Engl J Med 2001;345:861
1980 1990 2010 20152000
No new DKD-specific treatment in the last 15 years
High blood pressure
identified as DKD risk
factor
ß-blockers1
Hydralazine2
Captopril3
T1D
IDNT4, IRMA 25
IrbesartanT2D
RENAAL6
LosartanT2D
RAAS blockade

Renal glucose reabsorption in patients with hyperglycaemia
45SGLT, sodium glucose cotransporter.Gerich JE. Diabet Med 2010;27:136
Filtered glucose load >180 g/day
SGLT1
SGLT2 When blood
glucose increases above the
renal threshold
(>~10 mmol/L or
>180 mg/dL), the capacity of
SGLTs is exceeded,
resulting in urinary glucose
excretion

Empagliflozin increases urinary glucose excretion via SGLT2 inhibition
46
SGLT, sodium glucose cotransporter.*Loss of ~ 80 g of glucose per day = 240 cal/day.
Bakris GL et al. Kidney Int 2009;75;1272
Filtered glucose load >180 g/day
SGLT1
compensate
SGLT2
~90%SGLT2
inhibitors reduce glucose
reabsorption in the
proximal tubule,
leading to urinary glucose
excretion*and osmotic
diuresis
SGLT2inhibit
or
~ 80 g

Renal anatomy and physiology
GFR, glomerular filtration rateCherney D et al. Circulation 2014;129:587
47
KeyFlow of bloodFlow of filtrate
Afferent arteriole
Vasoconstriction decreases GFR
Efferent arteriole
Vasoconstriction increases GFR
Bowman’s capsule
Proximal convoluted tubule
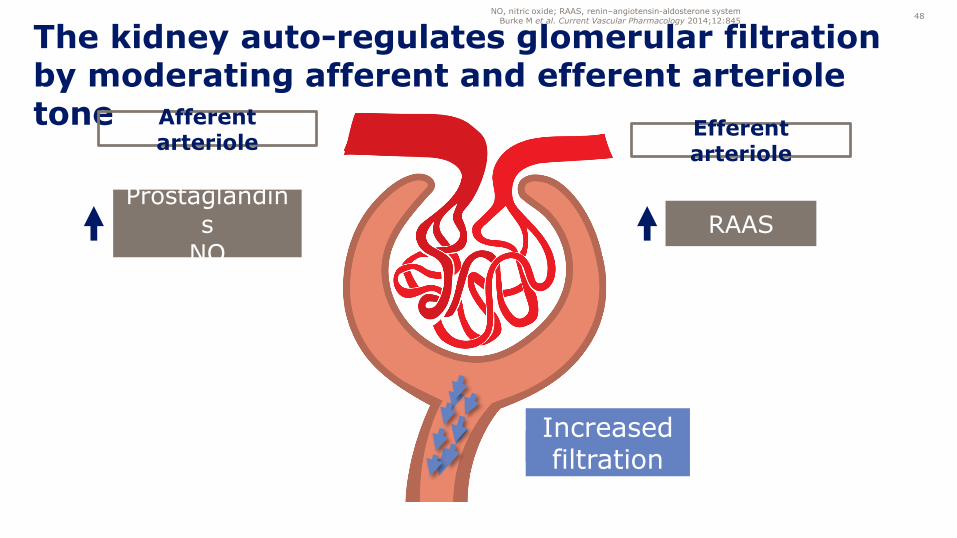
The kidney auto-regulates glomerular filtration by moderating afferent and efferent arteriole tone
NO, nitric oxide; RAAS, renin–angiotensin-aldosterone systemBurke M et al. Current Vascular Pharmacology 2014;12:845
48
Prostaglandins
NORAAS
Afferent arteriole
Efferent arteriole
Flow of filtrateIncreased filtration

Empagliflozin exerts a hemodynamic effect within the kidney
• By restoring the Tubulo-Glomerular Feedback (TGF), empagliflozin increases the afferent arteriole tone, thereby lowering glomerular hypertension
SGLT, sodium glucose cotransporter; GFR, glomerular filtration rate.Adapted from: Cherney D et al. Circulation 2014;129:587
Skrtic M et al. Diabetologia 2014;57:259949
Action: Clinical implications:
SGLT2 inhibition
Afferent arteriole narrowing
• Glomerular pressure decreases
• Early clinical marker:
– Initial dip in GFR
– Reduction of albuminuria
narrowing

Empagliflozin effect on glomerular hyperfiltrationshows similar magnitude as ACE inhibitor
177.7 172.0
142.8 139.0
0
20
40
60
80
100
120
140
160
180
200
ACEi Empagliflozin
Mean
GFR
(m
l/m
in/
1.7
3 m
2)
Note: Data from two different studies. ACEi, angiotensin-converting enzyme inhibitor; GFR, glomerular filtration rate.
1. Sochett E et al. J Am Soc Nephrol 2006;17:1703; 2. Cherney D et al. Circulation 2014;129:587
50
-33 ml/min-35 ml/min
Baseline ACEi Empagliflozin

Patients received JARDIANCE® or placebo on top of standard of care for CV and T2D management1
†Standard of care included antihypertensives, lipid-lowering agents, anticoagulants and glucose-lowering therapies.1
‡Data from both doses of JARDIANCE® were pooled for statistical analysis versus placebo. # JARDIANCE® can be used be used down to an eGFR of 45 mL/min/1.73m2.
1. Zinman B et al. N Engl J Med 2015;373:2117–28.
Standard of care + JARDIANCE®
10 mg (n=2345)
Standard of care + JARDIANCE®
25 mg (n=2342)
Standard of care† + Placebo(n=2333)
Randomised and treated(n=7020) Pooled‡
• Adults with T2D• Established CV disease (CAD,
PAD, MI or stroke)• HbA1c 7-10%• eGFR >30 mL/min/1.73m2#
• Glucose-lowering therapy was to remain unchanged for the first 12
weeks
• The trial was to continue until at least 691 patients experienced an
adjudicated primary outcome event
Slide 3 of 20

CV risk factor profile at study entry1
Data are mean or %. BMI, body mass index.
1. Zinman B et al. N Engl J Med 2015;373:2117–28.
Patient characteristics
57%Pt with T2Dduration >10 years
30.6BMI (kg/m2)
105Waist circumference (cm)
Previous CV events
76%Coronary artery disease
21%Peripheral artery disease
47%History of MI
23%History of stroke
10%Heart failure
63Age (years)
Slide 4 of 20
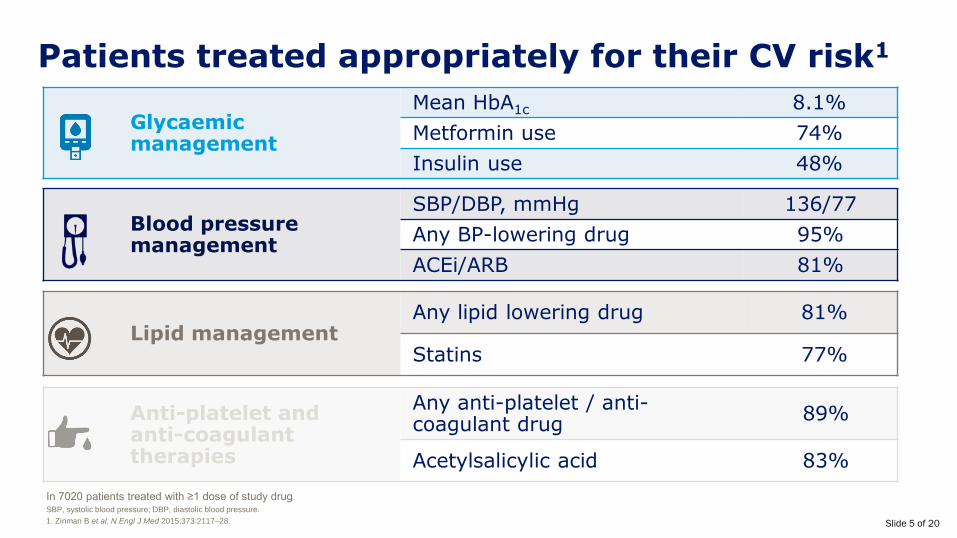
Glycaemicmanagement
Mean HbA1c 8.1%
Metformin use 74%
Insulin use 48%
Patients treated appropriately for their CV risk1
In 7020 patients treated with ≥1 dose of study drug.
SBP, systolic blood pressure; DBP, diastolic blood pressure.
1. Zinman B et al. N Engl J Med 2015;373:2117–28.
Blood pressure management
SBP/DBP, mmHg 136/77
Any BP-lowering drug 95%
ACEi/ARB 81%
Lipid managementAny lipid lowering drug 81%
Statins 77%
Anti-platelet and anti-coagulant therapies
Any anti-platelet / anti-coagulant drug
89%
Acetylsalicylic acid 83%
Slide 5 of 20

0
1
2
3
4
5
6
7
8
9
0 6 12 18 24 30 36 42 48Pati
en
ts w
ith
even
t
(%
)
Months
HR 0.62p<0.001
Adapted from Zinman B et al. 2015.1
*Within 6 months from start. #Up to 48 months from start.CV death was a pre-specified secondary endpoint. Cumulative incidence function. HR, hazard ratioThe absolute risk for CV death was 5.9% in patients receiving standard of care plus placebo and was reduced to 3.7% in patients receiving standard of care plus JARDIANCE® (p<0.001).1
1. Zinman B et al. N Engl J Med 2015;373:2117-28.
Standard of care +Placebo
Standard of care + JARDIANCE®
Early* and sustained# response
Results achieved on top of standard of care• Antihypertensives• Lipid lowering
agents• Anticoagulants• Glucose lowering
agents
CV deathJARDIANCE® reduced the relative risk of CV death by
38% vs placebo on top of standard of care in patients with T2D and established CV disease (CAD, PAD, MI or stroke)1
.
Slide 8 of 20
Standard of care +Placebo
Standard of care +JARDIANCE®
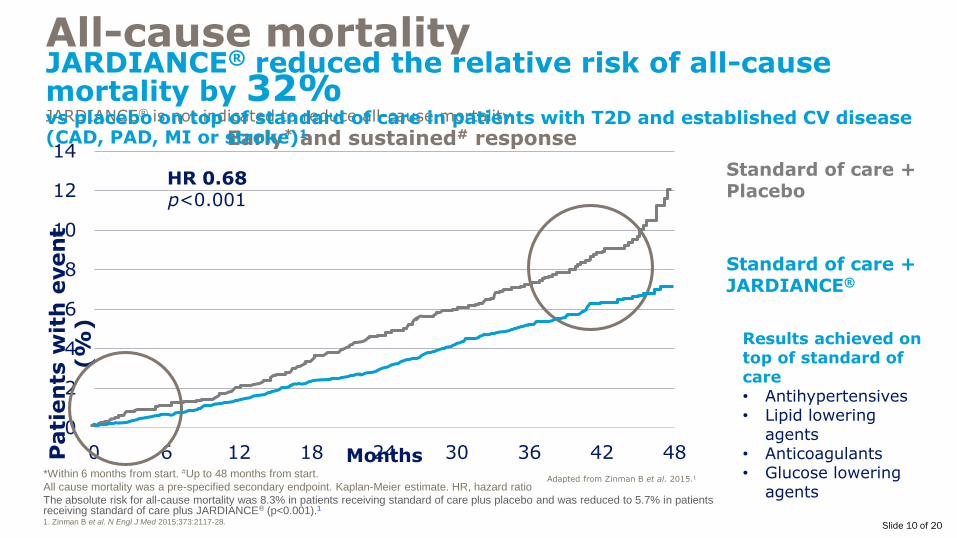
*Within 6 months from start. #Up to 48 months from start.
All cause mortality was a pre-specified secondary endpoint. Kaplan-Meier estimate. HR, hazard ratio
The absolute risk for all-cause mortality was 8.3% in patients receiving standard of care plus placebo and was reduced to 5.7% in patients receiving standard of care plus JARDIANCE® (p<0.001).1
1. Zinman B et al. N Engl J Med 2015;373:2117-28.
Adapted from Zinman B et al. 2015.1
0
2
4
6
8
10
12
14
0 6 12 18 24 30 36 42 48Pati
en
ts w
ith
even
t
(%
)
Months
HR 0.68p<0.001
Early* and sustained# responseJARDIANCE® is not indicated to reduce all-cause mortality
All-cause mortalityJARDIANCE® reduced the relative risk of all-cause mortality by 32% vs placebo on top of standard of care in patients with T2D and established CV disease (CAD, PAD, MI or stroke)1
Results achieved on top of standard of care• Antihypertensives• Lipid lowering
agents• Anticoagulants• Glucose lowering
agents
Slide 10 of 20

0
1
2
3
4
5
6
7
0 6 12 18 24 30 36 42 48Pati
en
ts w
ith
even
t (%
)
Months
Standard of care + Placebo
Standard of care + JARDIANCE®
Hospitalisation for heart failureJARDIANCE® reduced the relative risk of hospitalisation for heart
failure by 35% vs placebo on top of standard of care in patients with T2D and established CV disease (CAD, PAD, MI or stroke)1
*Within 6 months from start. #Up to 48 months from start.
Hospitalisation for heart failure was a pre-specified secondary endpoint. Cumulative incidence function. HR, hazard ratioThe absolute risk for hospitalisation for heart failure was 4.1% in patients receiving standard of care plus placebo and was reduced to 2.7%in patients receiving standard of care plus JARDIANCE® (p<0.002).1
1. Zinman B et al. N Engl J Med 2015;373:2117–28.
HR 0.65p=0.002
Adapted from Zinman B et al. 2015.1
Early* and sustained# responseJARDIANCE® is not indicated to reduce hospitalisation for heart failure
Results achieved on top of standard of care• Antihypertensives• Lipid lowering
agents• Anticoagulants• Glucose lowering
agents
Slide 12 of 20

Pre-statin era <29% statin
Pre-ACEi/ARB era
Number needed to treat (NNT) to save 1 life
4S1 HOPE2
Standard of care included antihypertensives, lipid-lowering agents, anticoagulants and glucose-lowering therapies.3
ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blockers,1. 4S investigators. Lancet 1994;344:1383-89. 2. HOPE investigators, N Engl J Med 2000;342:145-53. 3. Zinman B et al. N Engl J Med 2015;373:2117-28.
Simvastatin1
for 5.4 years
30In high CV risk5% diabetes,
26% hypertension
Ramipril2
for 5 years
56
JARDIANCE®3
for 3.1 years
39
> 75% statin
> 80% ACEi/ARB
EMPA-REG OUTCOME®3
1994
2000 Now
In high CV risk38% diabetes,
46% hypertension
T2D with established CV disease (CAD, PAD, MI or stroke)
on top of standard of care
92% hypertension
Slide 14 of 20

*Incident or worsening nephropathy analysed in patients who did not have macroalbuminuria at baseline. Modified intention to treat analyses in patients who received ≥1 study drug.Defined as progression to macroalbuminuria (urinary albumin to-creatinine ratio, >300mg of albumin per gram of creatinine); a doubling of the serum creatinine level, accompanied by an eGFR of ≤45 ml/min/1.73m2,
as calculated by the Modification of Diet in Renal Disease (MDRD) formula; the initiation of renal-replacement therapy; or death from renal disease. Death due to renal disease: 3 events on JARDIANCE® and 0 on placebo.Standard of care included antihypertensives, lipid-lowering agents, anticoagulants and glucose-lowering agents.2
1. Wanner C et al. N Engl J Med 2016. 2. Zinman B et al. N Engl J Med 2015;373:2117–28.
JARDIANCE® slowed the progression of renal indicators in the EMPA-REG OUTCOME® study in patients with T2D and established CV disease (PAD, CAD, MI or stroke) on top of standard of care1*#
#JARDIANCE® is not indicated to prevent decline in renal function
Slide 15 of 20

SGLT2 inhibition and RAAS blockade
Afferent narrowing andEfferent widening
• Potential for normalisation of intraglomerular pressure
• Potential additive intraglomerularpressure reduction
• Potential for long-term renal protection
Future outlook – Dual SGLT2 and RAAS inhibition
Empagliflozin is not indicated for CV risk reduction or kidney diseaseAdapted from: Cherney D et al. Circulation 2014;129:587; Lewis et al. N
Engl J Med 2001;345:851; Kon V et al. Kidney Int 1993;44:545
59
Actions:SGLT2 inhibition
Afferent arteriole narrowing
Clinical implications:
• Decreased glomerular pressure
• Reduction in albuminuria
• Renal protection suggested
RAAS blockade
Efferent arteriole widening
• Decreased glomerular pressure
• Reduction in albuminuria
• Renal protection proven in clinical trials
CO
NCEPT

• Diabetes prevalence is growing
• Strong evidence base or reduced complications with optimal management
• There remain substantive numbers of people not at/near target for management
• Therapy needs to multifactorial and introduced progressively and incrementally to manage diabetes over time reflecting the progressive pathogenesis
• Newer therapies offer several advantages including convenience, side effect profile and are showing superiority in studied populations for renal and CVD endpoints above standard care
• Maori and Pacifica are at particularly high risk for CVD and renal harm from diabetes
• Cost is an issue, but largely because of the high numbers with diabetes with suboptimal control currently, thus cost is likely to come with substantive benefit.
Summary
Presentation title Date 60